

Abstract
Robotics is a forward-looking discipline. Attention is focused on identifying the next grand challenges. In an applied field like medical robotics, however, it is important to plan the future based on a clear understanding of what the research community has recently accomplished and where this work stands with respect to clinical needs and commercialization. This Review article identifies and analyzes the eight key research themes in medical robotics over the last decade. These thematic areas were identified using search criteria that identified the most highly cited papers of the decade. Our goal for this Review article is to provide an accessible way for readers to quickly appreciate some of the most exciting accomplishments in medical robotics over the last decade, for this reason we have focused only on a small number of seminal papers in each thematic area. We hope that this article serves to foster an entrepreneurial spirit in researchers to reduce the widening gap between research and translation.
One-Sentence Summary:
Eighty percent of medical robotics papers have been published in the last decade – what has been accomplished?
INTRODUCTION
Just over three decades ago the first roboticists began to explore the use of robot manipulators for performing surgical procedures. Two decades ago, the first commercial systems were installed in hospitals. In the past decade, the field of medical robotics has gained momentum, and thousands of robotic surgical systems are now installed in clinics around the world, and many millions of procedures have been performed. As the acceptance of surgical robots by our healthcare systems has become clear, robotics researchers have increasingly focused their attention on what the next generation of medical robots might look like. Their attention is not limited to surgical robots, and other areas of medicine are also being investigated including robots to perform physical rehabilitation, telepresence robots for patient interaction with off-site healthcare workers, pharmacy automation, robots for disinfecting clinics, and more.
Medical robots were first developed to allow surgeons to operate remotely and / or with improved precision on their patients, and the history of the field is well documented in the literature (1–3). The earliest efforts can be traced back to applications in neurosurgery (4) and orthopaedic surgery (5). The first truly long-distance telesurgery was a transatlantic cholecystectomy performed twenty years ago (6). While early progress in the field was somewhat unsteady, as is to be expected with the introduction of any radically new technology, medical robotics has reached a level of maturity that has encouraged the healthcare industry to make substantial investments in development activities.
Researchers, however, generally look farther into the future and beyond commercial development activities. As we consider some of the key research activities in the past decade, we obtain a glimpse of where medical robotics will head in the coming decades. This article focuses on the last ten years and provides a retrospective assessment of the major accomplishments in medical robotics. We employ an inclusive definition for what constitutes a medical robot which is intended to cover all material that would be appropriate for inclusion in a major robotics research journal or conference. This encompasses single-and multi-degree-of-freedom motorized systems with motions that may be pre-programmed, joystick-prescribed, autonomous or some combination of the three. We define medical robotics research as the creation of new robots and robotic technologies for medical interventions. A large body of medical journal papers devoted to the evaluation of existing medical robots has also been published over the last decade. Since these robots largely represent technologies developed during prior decades, they are not discussed here.
In this paper, our goal was to identify the major research themes or “hot topics” in medical robotics over the decade and to summarize the seminal research papers that concisely highlight these themes.
HOT TOPICS OF THE DECADE
We identified eight hot topics by searching Web of Science for the most highly cited papers on medical robotics published in 2010–2020 (Table 1 and Fig. 1). These hot topics can be related to specific clinical applications (e.g. topic 1, robotic laparoscopy), or to enabling technologies that find broad applications in medicine (e.g. topic 7, soft robotics).
Table. 1.
Hot topics of the decade.
| Hot Topic | Seminal references |
|---|---|
| 1. Robotic laparoscopy | [7]–[18] |
| 2. Non-laparoscopic robots for minimally invasive surgery | [19]–[24] |
| 3. Assistive wearable robots | [25]–[33] |
| 4. Therapeutic rehabilitation robots | [34]–[41] |
| 5. Capsule robots | [42]–[48] |
| 6. Magnetic actuation | [49]–[52] |
| 7. Soft robotics | [53]–[61] |
| 8. Continuum robotics | [62]–[69] |
Fig. 1. Example clinical applications for the 8 hot topics of the decade.
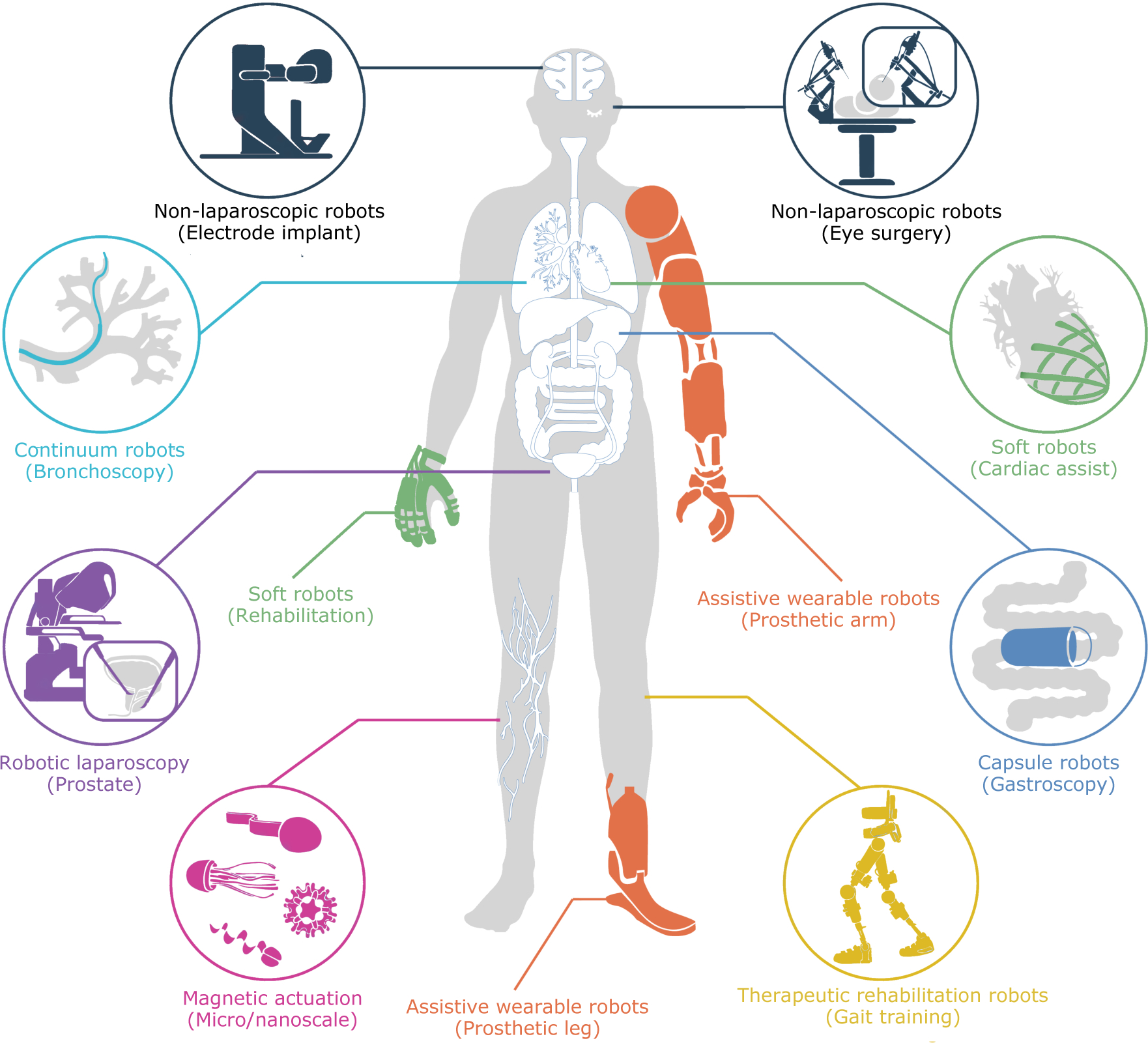
Starting at 8 o’clock and proceeding clockwise: Laparoscopic robots are the success story of medical robotics with applications including radical prostatectomy, radical cystectomy for bladder cancer, rectal cancer resection and hysterectomy. Continuum robots are robotic versions of manual medical instruments including catheters, bronchoscopes, uteroscopes and colonoscopes. Non-laparoscopic robots have been developed for varying applications including electrode implantation in the brain and microsurgery inside the eye. Soft robots have been used, e.g., to create soft sleeves to assist heart contraction and for hand rehabilitation of daily living tasks. Assistive wearable robots are used to augment or replace arm and leg motion in the cases of motion impairment or amputation. Capsule robots are pill-sized devices that are swallowed for endoscopic diagnosis and treatment of the alimentary canal. Therapeutic rehabilitation robots assist patients with neurological injuries in performing repetitive movements to relearn tasks such as walking and grasping. Magnetic actuation enables the wireless generation of forces and torques inside the body to actuate an untethered robot or to orient the tip of a catheter.
To illustrate how the number of publications in medical robotics has evolved over time, the total number of publications for engineering and medical journals is plotted in Fig. 2. The total number of publications for all but one of the hot topics is also reported in Figs. 2–3. (Total publications for non-laparoscopic robots for minimally invasive surgery are not reported since satisfactory search criteria could not be identified.) Note that the vertical scales for Figs. 2 and 3 differ by an order of magnitude.
Fig. 2. Medical robotics papers published in engineering and medical journal papers from 1990 to 2020.
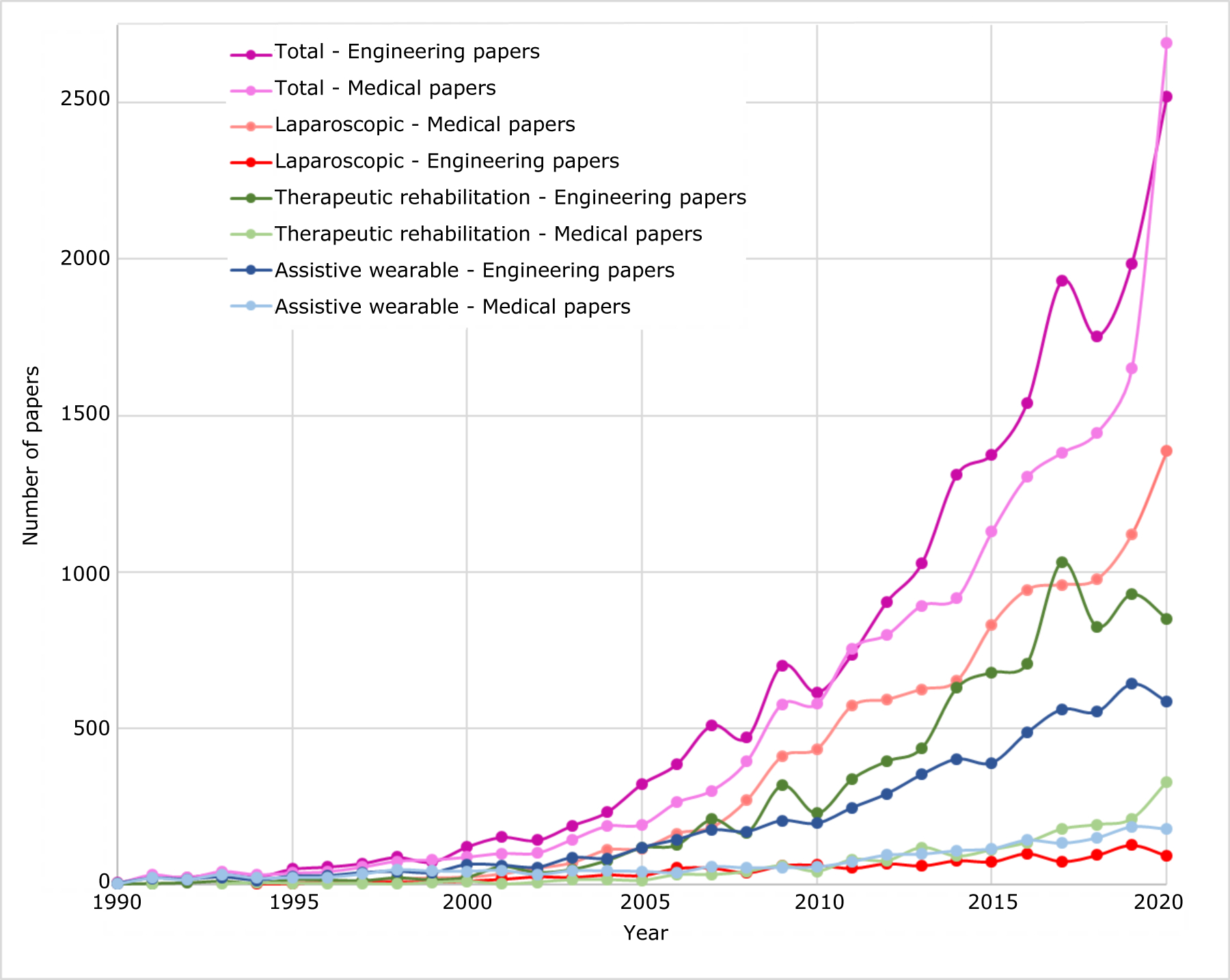
Curves report total numbers along with subsets corresponding to hot topics of laparoscopic robots, therapeutic rehabilitation robots and assistive wearable robots. Note that 2020 publications are potentially reduced by COVID-19 shutdowns. (Data from Web of Science: see Materials and Methods).
Fig. 3 – Medical robotics papers published in engineering and medical journal papers from 1990 to 2020.
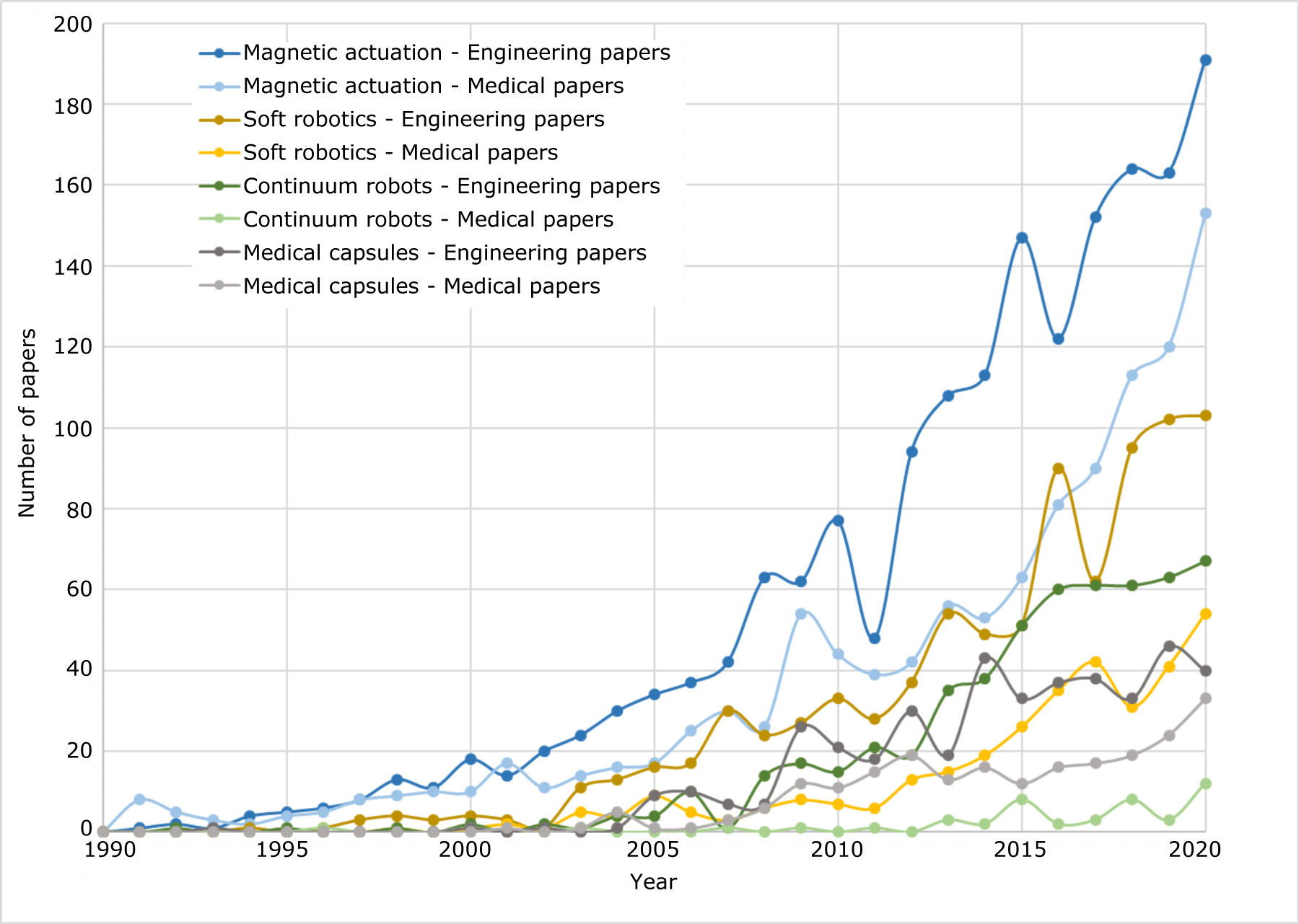
Curves report paper numbers for hot topics of soft robotics, magnetic actuation, capsule robots and continuum robots. Note that 2020 publications are potentially reduced by COVID-19 shutdowns. (Data from Web of Science: see Materials and Methods).
From Fig. 2, the number of publications on medical robotics in engineering and medical journals has grown exponentially from a total of 6 in 1990 to over 3500 in 2020. Medical journal papers are dominated by publications on laparoscopic robots (60–70% of total) with over 1300 published in 2020 owing to the success of Intuitive Surgical’s da Vinci robot. In line with the maturity of this technology, engineering papers on laparoscopy, in contrast, peak at 126 in 2019.
Engineering papers are dominated by therapeutic rehabilitation and assistive wearable robots. This pair of hot topics represents about 80% of the engineering-journal medical robotics papers published over the last decade. While these two topics entered the decade with an equal number of papers, therapeutic rehabilitation has subsequently notably outpaced assistive wearable robots. It is interesting to note, however, that the number of medical papers on these topics is less than 25% of the number of engineering papers. This is likely due to the fact that medical journal papers often report the results of clinical trials, which are much more costly and time consuming to perform than engineering studies.
The technologies plotted in Fig. 3 are less mature than those of Fig. 2 and consequently are the subject of fewer engineering and medical journal papers. Of these, magnetic actuation is the most mature and exponential growth in both engineering and medical papers can be observed with medical papers lagging engineering papers. Continued growth of this topic to some extent hinges on whether or not clinically viable applications of microrobots can be developed.
The plots of soft robotics papers show this topic to be early in its development cycle. It should be noted, however, that we excluded the large numbers of fundamental articles on soft actuators and sensors appearing in materials journals that suggest medical robotics as a potential application. The mapping of these broadly applicable technologies into medical robots over the next decade will likely produce the exponential growth suggested by the curves in Fig. 3.
Continuum robot technology is unusual in that manually actuated continuum-style medical instruments existed long before 1990. While new continuum robot architectures have been developed in recent decades, the critical advance to make these devices robotic was not one of mechanical design, but rather of mathematical modeling. This work is largely complete as described in its hot topic section below and future growth in engineering papers will likely describe clinical robot designs incorporating continuum components. Medical papers on this topic have been slow to take off because commercial efforts, e.g., Hansen Medical’s cardiac ablation catheters have been unsuccessful. New clinical systems, such as Intuitive Surgical’s Ion robot and Auris Healthcare’s Monarch platform (the latter based on Hansen Medical’s robotic catheter technology), both for performing distal lung biopsies, will lead to increasing numbers of medical papers in the coming decade.
Capsule robots are the least mature and perhaps the most specialized of the hot topic technologies. Their capabilities, as reported in the publications of Fig. 3, have improved substantially over the last decade. This technology may be at an inflection point. If the capabilities of these robots can be proven sufficient to displace current clinical approaches, interest in this topic will accelerate enabling its further development. There is some evidence that this is the case for soft capsule robots under magnetic actuation, an approach that has potential for noninvasive diagnosis and therapy inside the digestive tract.
The following sections describe each hot topic, provide a summary of the most important accomplishments over the decade and include insights on current and future research directions. As represented in Figs. 2 and 3, many papers have been published on each topic. With the goal of highlighting a focused reading list for readers who wish to most rapidly come up to speed on a topic only a few highly cited papers are provided as references. The bibliography at the end of the paper is divided into sections by hot topic. Each entry includes the number of times the paper was cited by other papers (Web of Science) and by patents (Lens.org) at the time this paper went to press.
Robotic Laparoscopy
Laparoscopic robotics is perhaps the most mature and certainly the most commercially successful subfield of medical robotics. Over the last decade, progress has been made on three fronts: clinical, commercial and academic. A rapidly growing majority of research in laparoscopic robots has been clinical. Many studies aim to compare the efficacy of the robot to standard (usually manual laparoscopic) techniques for different surgical procedures. Examples include studies on radical prostatectomy, radical cystectomy for bladder cancer, rectal cancer resection and hysterectomy.
Commercially, the decade has seen continuing evolutionary development of the da Vinci robot made by Intuitive Surgical. This system now offers the ability to mount endoscopic and laparoscopic instruments on any arm (earlier models had a specialized endoscope arm), semi-automated arm and patient cart positioning and improvements to the instrument coupling. Over the last decade, at least 50 different instruments have been released for the da Vinci. Furthermore, the da Vinci’s use has grown rapidly with over 1.2 million procedures completed in 2019 according to their annual report. At the same time, the initial patents which had given Intuitive Surgical a monopoly position in robotic laparoscopic surgery began to expire during the last decade resulting in several large medical device companies launching initiatives to develop their own robots which are currently being introduced.
Academic research progressed on two fronts over the decade. The first has used laparoscopic robots as a platform for developing enhanced capabilities. Major subtopics on this front include the introduction of open platform robots for research use, initial efforts into the development of surgical automation and continuing work on the integration of force sensing into laparoscopic tools. The second research direction in laparoscopic surgery has considered new robot architectures that might reduce procedural invasiveness. Single port systems have received the most attention, including a recently introduced commercial system from Intuitive, the da Vinci SP. There has also been some research into robots that are inserted into the body and then detached mechanically, powered by tethers or external fields. Each of these topics is described below.
Open platform laparoscopic robots.
New robot capabilities cannot typically be developed and tested in isolation. For results to be reproducible and comparable, it is important for such research to be performed on high-performance test platforms that are well characterized. It is a huge and duplicative undertaking for an individual research group to develop their own laparoscopic robot system. Recognizing this need, two groups introduced open-source robot platforms for the research community. The first was the Raven II, a non-clinical robotic surgery research platform which compactly supports two to four laparoscopic instruments (including daVinci SI instruments) in a work volume typical of abdominal laparoscopic surgery (7). Intuitive Surgical collaborated with several academic researchers to then introduce a research platform consisting of refurbished da Vinci Si patient and surgeon-side mechanisms, steroscopic display hardware with a custom electronics and a control package, the da Vinci Research Kit or dVRK (8). Neither system is certified for human use, but both have performed animal procedures with IACUC approval.
Surgical automation.
Laparoscopic robot systems are used to perform a wide range of standard surgical tasks. They also inherently provide complete actuation of instrument motion as well as high quality video and rich data sets describing instrument motion. As commercial offerings such as da Vinci have attained excellent levels of user-interface transparency, research focus has turned to use cases which might require supplementing teleoperated robotic surgery with automated assistance. Potential benefits of safe and effective automation of sub-tasks of a surgery include increased precision, fusion of non-visual or haptic sensor information, adherence to precise pre-operative plans, and amelioration of repetitive stress injury and other ergonomic hazards to surgeons. Barriers to safe and effective automation of selected surgical tasks are pronounced and include accurate 3D reconstruction of the (changing) surgical field, repeatable and accurate control of elongated and flexible endoscopic mechanisms, accurate situational awareness by the agent of the overall operation’s state, robustness of task plans to sensor errors, unusual tissue properties, and emergency events. Work on this topic extends from developing 2D and 3D computer vision techniques to detect and localize robotic tools (9) to learning from observation of surgical subtasks(10). It also includes semi-automated in vivo (11) suturing although the technologies in these studies required simplified visual environments. The development of autonomy remains a very active research frontier.
Navigation, Intraoperative Imaging and Visualization.
While surgical automation is often regarded as a novelty, some of the earliest medical robots, e.g., for milling cavities in bone in joint replacement, offered a level of automation comparable to machine tools [5]. Pre-operative CT or MR images were used to generate operative plans that were carried out under computer control while the clinician provided general supervision. As the field began to focus on soft tissue surgery, preprogrammed motions gave way to clinician-guided teleoperative control. Despite the change in control paradigm, the incorporation of image guidance, using either intraoperative or preoperative data, has become increasingly important for all types of robotic surgery – not just in laparoscopy. These techniques enable assessment of tissue perfusion as well as visualization of anatomical details below the tissue surface, minimizing the risks of damaging underlying vital structures such as nerves and blood vessels. For example, Intuitive Surgical has integrated near-infrared imaging with indocyanine green (ICG), allowing real-time assessment of microcirculation in vivo. ICG is a tricarbocyanine compound that is water-soluble and can be injected intravenously. This “firefly” technology absorbs near-infrared light and when injected remains intravascular and can be used to assess blood perfusion, allowing, for example, the detection of decreased blood perfusion at an intestinal anastomosis that may result in anastomotic dehiscence (12).
Contact force sensing and control.
Both manual and laparoscopic instruments remove the surgeon’s hand from tissues being manipulated and thus distort or completely suppress force and tactile sensations. To preserve safe handling of tissues in tasks such as retraction, interaction forces must be sensed and controlled. Furthermore, tactile sensing would allow the recreation of tissue palpation at the manipulator during robotic surgery. Technical barriers to such sensing include the small (5–10mm diameter) size of laparoscopic instruments, heat and corrosiveness of sterilization measures in re-usable instruments and cost in single-use instruments as well as the mechanics imposed between sensing point and the tool-tissue contact point or area. Progress to address this limitation has been made through the use of clever mechanical designs to separate pulling and grasping forces (13) as well as the introduction of new sensing technologies such as capacitive compliant polymer load cells (14).
Single Port Laparoscopic Robots.
As much as laparoscopic surgical approaches reduced invasiveness compared to standard open procedures, a typical manual or robotic procedure requires three or four incisions for individual instruments and the visualization endoscope. Combining multiple instrument controls, drives, and endoscopic visualization into a single access port require increased mechanical complexity and density. Notable innovative single-port prototypes include (15, 16).
Detached surgical robots.
The classic laparoscopic paradigm involves elongated instruments each inserted at a pivot point in the abdominal wall through a port/trocar. This geometry fundamentally constrains the motion by which a surgeon can approach the surgical task. Research to break this constraint faces the challenges of implementing all actuation and sensing inside the body itself, supplying suitable power and communication, and safe deployment and retrieval of an independently deployed robot from the surgical site. Prototypes demonstrating removal of the trocar-pivot constraint include endoscopes and robotic instruments inserted through a port and then attached to the abdominal wall using either magnetic forces (17) or a needle-sized puncture which is also used for power transmission (18).
Robots supporting laparoscopic surgery are the most advanced in terms of application to medicine with over 5 million people treated suggesting rapid momentum heading into the next decade. This volume allows medical innovations and the proliferation of new instruments which is expected to continue. New sensors, and better estimation and modeling data and algorithms will allow precise control of force. Gradual introduction of automation to support laparoscopic and other robotic surgeons will allow seamless integration of novel imaging and treatment modes increasing the surgeon’s role as a supervisor and monitor of advanced surgical instruments.
The most important advancements in laparoscopic robotics will be those with the most direct patient benefits including better treatment of tumor margins with less need to resect healthy tissue, detection and reduction of rare surgical errors, and reducing the trauma and risk of infection from surgical procedures.
Non-laparoscopic procedure-specific robots
Inspired by the success of the da Vinci robot for laparoscopic procedures, the past decade has also witnessed surgeons and engineers exploring new robotic solutions for non-laparoscopic procedures. Key areas of focus have included endoluminal and natural orifice interventions as well as robots for microsurgery.
Endoluminal and Natural Orifice Surgery.
Of the nascent applications of surgical robots explored in the past decade, we note works on endoluminal and endoscopic robots seeking to further reduce morbidity by eliminating the need for skin incisions to access internal anatomy and by offering solutions allowing for deeper access along tortuous anatomical passages. Shang et al. (19) presented a highly articulated endoscopic platform for endoluminal surgery and demonstrated peritoneal cavity and trans-vaginal access. Burgner et al. explored the potential use of concentric tube robots for transnasal pituitary gland surgery (20). Rivera-serrano et al. (21) presented the use of highly articulated robotic probe (HARP) for transoral access and delivery of manual tools.
New commercial systems focused on steerable catheters for natural orifice minimally invasive biopsy also have recently been launched. Perhaps the most notable of these systems are the Ion® system by Intuitive Surgical and the Monarch® system by Auris Healthcare. The Ion and Monarch systems employ dexterous catheter articulation to enable peripheral lung biopsy that would otherwise be very difficult to achieve safely. These systems leverage previously developed modeling and design technology of tendon-actuated continuum robots.
Micro-surgery.
Retinal micro-surgery poses unique challenges that exceed the capabilities of existing manual surgical systems. Researchers have taken three approaches to addressing these challenges. They have developed hand-held robots with tremor filtering. They have also created hand-on-hand (cooperative) robots. As a third approach, they have developed telemanipulated robots with a remote center of motion. Hand-held robots with active tremor cancellation have been refined for retinal surgery as in (22). In this approach, the surgeon-produced tremor in the handheld tool is sensed and a robot at the tip of the tool moves to oppose it such that most of the tremor is cancelled out.
Cooperative robots provide an alternative approach to tremor suppression while also offering additional capabilities. These robots hold the surgical tool together with the surgeon and operate under admittance control – producing motions based on the forces applied by the surgeon to the tool. The robot’s motions can be more precise than what the clinician can perform freehand and are also tremor free. Furthermore, assistive control laws, based on active constraints/virtual fixtures, can be implemented to help the surgeon follow a desired path, avoid dangerous tool excursions and to provide physiological relief from having to hold the surgical tool for extended periods of time. This approach has been applied to vitreoretinal microsurgery (23). It also being commercialized for tool stabilization in the upper airway where the length of needle drivers and graspers due to the trans-oral access makes it challenging to achieve precision manipulation (Galen Robotics, Inc.). The system has also been tested for applications involving use of image-guided barrier virtual fixtures for safe bone deburring during mastoidectomy where the risk of damaging the facial nerve is mitigated by the image-guided robotic system.
A third approach to robotic microsurgery is to use teleoperation. In this approach, the clinician does not need to hold the tool at all, but rather controls the robotic tool through an input device. This technology provides all of the advantages of cooperative robots with the addition of motion scaling and the potential for reduced inertial and frictional effects. Such a system for intraocular surgery has undergone first in human testing (24).
What the future holds:
There are several exciting developments that will enable a new wave of innovation of procedure-specific robotic platforms. In the past decade, we have seen some works in the area of electrode array steering and insertion for cochlear implants. These examples point to the potential of harnessing soft robotics and possibly magnetic actuation for creating new platforms for deep navigation. We also have seen some works on robotic systems that combine manipulation and sensing/diagnostics and imaging. We believe that there is still a need for solutions enabling in-vivo sensing and use of in-vivo sensing for improving surgeon performance. Systems that can use intraoperative sensing with adaptive assistive behaviors (virtual fixtures or shared control) will also allow surgeons to achieve rapid clinical deployability and improved perception and performance.
Assistive wearable robotics
Assistive wearable robotics focuses on the design and control of wearable robotic devices intended to improve the mobility or functionality of individuals with musculoskeletal or neuromuscular impairment. Areas of contribution in this field include the development of robotic limbs (also called powered prostheses) for individuals with upper and lower extremity amputation, and the development of exoskeletons (also called powered orthoses) for individuals with neuromuscular impairment, such as those with spinal cord injury, stroke, multiple sclerosis, or cerebral palsy. Although the field has historic roots dating at least to the early 1960s (see, for example, the Proceedings of the International Symposium on External Control of Human Extremities, 1963), the decade between 2010 and 2020 saw the fully-realized emergence of it.
Although an enumeration of research in the field is beyond the scope of this short summary, three major categories of research include: 1) powered lower limb prostheses; 2) neurally-controlled upper limb prostheses; and 3) lower limb exoskeletons. In the area of lower limb prosthetics, the state-of-the-art prior to (circa) 2010 were energetically-passive devices. The past decade saw the introduction of power into prosthetic knee and ankle joints. Since powered devices have volition, new control methods are required that ensure coordination between human and device. Approaches to doing so include piecewise passive impedance control, such as that described in (25) which provides assurances of locally passive behavior, and phase variable control, such as that described in (26), which supplants finite-state structures with a uniform control policy. Further, since powered devices substantially increased the range of activity-specific behaviors of such devices, methods of activity recognition are required to determine a current activity state, and intent to change activity state. Pattern recognition structures consisting of data reduction and classification methods were established, in which a given movement activity is inferred in real-time based on patterns of movement, such as the methods described by (27).
Unlike lower limb devices, the state-of-the-art prior to 2010 in upper limb prosthetics was powered (i.e., myoelectric prostheses). However, these devices typically employed single degree-of-freedom (DOF) hands and sequential myoelectric control. The past decade has seen the emergence of several multi-grasp hands and the development of corresponding multigrasp and/or multi-DOF hand and arm control methods. Such control methods include EMG-based pattern recognition approaches, in which multi-channel EMG is used as input to a pattern classifier, which in turn selects a corresponding desired grasp posture or arm movement, and subsequently executes the corresponding coordinated hand and/or arm movement (28). The decade also saw the use of implanted electrodes used for the efferent motor control of a multi-grasp arm prosthesis (29), and importantly, to provide meaningful neural sensory feedback corresponding to a hand prosthesis, such as the impressive work reported by (30) and (31).
Scholarly research and development in the area of lower limb exoskeletons (LLEs) over the decade has seen dramatic growth, particularly research associated with developing best practices for design and control of such systems, which varies depending on impairment and objective. Efforts describing exoskeletal designs emerged early in the decade, including methods of movement intent and control. A method of user intent that has gained widespread popularity is the use of body posture, as measured via IMUs, to infer intent to walk (or perform a different activity) (32). In addition to exoskeletons, soft “exosuits” were introduced during the decade (33). (See also the section Soft Robotics for Medicine.) Relative to exoskeletons that employ rigid links, soft exosuits employ low-modulus materials, often along with tendon actuation, to transmit movement assistance without imposing substantial movement constraint along non-actuated DOFs. Although methods for LLE control for non-ambulatory individuals became established during the decade, e.g., (32), the field has yet to fully establish corresponding best practices for providing gait assistance for poorly ambulatory individuals. In the case of non-ambulatory individuals, no joint-level cooperative control is required between human and machine, while assisting a user capable of movement generally entails a high degree of joint-level coordination between device and human. Presumably the field will, in the coming decade, establish methods for assisting poorly-ambulatory individuals without jeopardizing the user’s agency or ability to maintain balance, particularly in the absence of a stability aid, with the aspirational objective of also improving balance.
Therapeutic rehabilitation Robots
While assistive exoskeletons and prosthetic limbs are intended to replace lost function, rehabilitation robots are designed to deliver repetitive movement therapy to the limbs following neurological injuries, most commonly stroke and spinal cord injury, so that the individual’s capabilities are restored. These robotic devices enable the execution of reaching, grasping, walking, and ankle movements in a manner that induces or facilitates neuroplasticity, which can result in recovery of range of motion and movement coordination. When these gains are realized, the patient experiences restored limb function and, in some cases, is able to provide self-care, live independently, and even return to the workforce following their injury without the support of the robotic device.
Some rehabilitation robots take the form of exoskeletons that fit around the leg, arm, or hand, while others are end-effector type robots that interface with the human body through a handle or foot platform. Devices target either lower limbs, with the primary objective being the restoration of mobility, or the upper limb, with the objective being the restoration of dexterity. The robot becomes a reliable tool for the physical therapist, providing precise and repeatable movement support to the patient with a level of intensity that can be modulated either through variable resistance, assistance, or number of repetitions. Integrating robotic devices in a rehabilitation regimen can reduce personnel costs, minimize work-related injuries, and improve the consistency by which training is delivered. Robots for rehabilitation can serve both as the means to deliver therapy and as a tool for assessment, since on-board sensors can measure features of movements over the course of the therapeutic intervention, providing a fine-grained view of the progress in movement capability that traditional clinical assessment scales, which are coarse and focused on functional ability, fail to capture.
Since the introduction of rehabilitation robots in the early 1990s as a means to provide precise, repetitive movement therapy, there have been important advances made in their design, fabrication, control, and clinical translation. In the decade prior to 2010, the major research accomplishments included the clinical assessment and commercialization of the first generation of robotic devices developed for neurorehabilitation, including treadmill-based exoskeletons for gait rehabilitation, such as the Lokomat, and end-effector type robots for upper limb rehabilitation, such as the InMotionARM robot. Since these initial developments, in the early 2000s, researchers began to develop new exoskeleton-type robots for the upper limb that could target specific joint movements distal to elbow and shoulder, while lower-limb exoskeletons that could facilitate over ground walking were introduced. This decade saw foundational work in the development of control algorithms that were designed to enable better coordination of movement between robot and patient.
During the decade 2010–2020, rehabilitation robotics research was primarily focused on four areas. The first was novel device design, increasingly of the exoskeleton form and focused on the distal joints of the upper limb and incorporating compliance and soft materials for both actuation and structure. The second was the development of new control algorithms to modulate the interaction between human and robot to elicit maximum participation from the human. The third was the creation of methods of intent detection to infer and support the patient’s desired movements, rather than prescribed or preprogrammed trajectories. The fourth was the expanded use of robotic devices for objective and quantitative assessment of neurorecovery, not just the delivery of therapy.
In the last ten years, researchers have increasingly focused on the design of rehabilitation robots for the hand and wrist, since the ability to self-feed, groom, and care necessitates recovery of hand function and dexterity. In contrast to the periodic nature of walking, upper limb and hand movements involve dozens of degrees-of-freedom, leading to complex kinematic designs of rigid arm and hand exoskeletons and tendon or cable-based actuation schemes that attempt to reduce device weight and inertia by remotely locating the actuators (34). Some groups have embraced soft robotic technologies for glove-based designs that focus on functional grasps, using pneumatic actuation that may even facilitate home-based rehabilitation (35).
There have been impressive advances in control methods for rehabilitation robots in the past decade, predominantly those that facilitate cooperation between robot and patient. Increasingly advanced methods to estimate the capability of the patient to initiate or execute reaching movements or gait trajectories have been proposed, which are coupled to adaptive control schemes for the robotic device to automatically adjust the amount of robot support on the fly, maximizing the patient’s contribution to movement execution (see (36) for an example in upper limb rehabilitation, and (37) for lower limb rehabilitation). This strategy is known to promote neuroplasticity, which is critical to recovery of movement coordination (38)
Patient engagement, both cognitive and physical, is another factor known to promote neuroplasticity during rehabilitation (39). In the past decade, researchers have developed new methods to detect movement intent from patients using surface electromyography (EMG) to measure electrical activity of the muscles themselves, or electroencephalography (EEG) to infer intent from changes in the electrical potentials recorded from the surface of the scalp. Clinical evaluation of these techniques is in the early stages, though some initial findings show that outcomes for EEG-based intent detection are comparable to robotic therapy without intent detection (see, for example,(40)). While this may at first seem to be a disappointing outcome, the number of movement repetitions achieved in a single therapy session using this technology is substantially lower than robotic rehabilitation alone given the complexity of the experimental set-up and computational overhead. Despite this, the clinical gains are comparable, meaning that such technologies may enable more severely impaired individuals who cannot initiate movement to benefit from robotic rehabilitation.
A final area of advancement in the past decade is in the application of robotic rehabilitation devices as assessment tools. Clinical assessment scales are known to be relatively coarse in their ability to detect improvements in motor function. Robotic devices, outfitted with high resolution sensors, can be used to assess range of motion, intra- and inter-limb coordination, and movement smoothness, among other features (41). Additionally, these devices can track recovery over higher-resolution time scales, since data can be collected at each treatment session. There is great potential for robotic assessment of neurorecovery to influence the intervention itself, which gives promise to the potential for robotic devices to appreciably improve rehabilitation outcomes in the future.
The developments of the past decade are starting to be assessed clinically, using both research grade devices and those that have been commercialized. Clinical studies aimed at the evaluation of efficacy of novel devices, controllers, and methods for detecting user intent for stroke and spinal cord injury rehabilitation are in some cases actively recruiting participants, while other studies are listed in the clinical trials database but are not yet recruiting. Example clinical studies include investigations of soft robotic gloves, interactive exoskeletons for gait rehabilitation, and the potential for using EMG or EEG to control a rehabilitation exoskeleton. Although not directly related to advances in robotics, there are additional clinical studies that aim to determine the efficacy of existing devices for treatment of different neurological impairments. For example, devices developed to treat stroke populations are being evaluated on spinal cord injury populations. Another notable ongoing effort is the evaluation of the efficacy of combining robotic rehabilitation with other therapeutic interventions, such as spinal stimulation or pharmacological treatments.
While robotic devices have been shown to effectively deliver therapy to both the upper and lower limbs following stroke and spinal cord injury, the improvements in clinical outcome measures of function to date have been modest when compared to traditional therapy (38). Future research efforts are increasingly focused on gaining a better understanding of the mechanisms of neuroplasticity, including how it can be reliably induced and exploited to maximize therapeutic outcomes. Such efforts are increasingly dependent on advances in neuroscience, including new techniques for recording neuronal activity. Advances in robotic technologies are also vital to achieving these goals, including the development of better fitting devices and more precise sensing and actuation embedded in devices to target the distal degrees of freedom of the upper and lower limbs that are most likely to facilitate a return of function and independence. Finally, advanced control algorithms that can more precisely characterize the patient’s capabilities in real-time and adjust not only the level of support needed to complete movements, but also impose appropriate resistance or challenge are needed.
Capsule robots
At the dawn of the new millennia, Given Imaging (now Medtronic) introduced wireless capsule endoscopy as a minimally invasive method of inspecting the gastrointestinal tract. The possibility of collecting images deep inside the bowel just by swallowing a “pill” revolutionized the field of gastrointestinal endoscopy and sparked a brand-new field of research: medical capsule robots.
It was quickly understood that conventional capsule endoscopes – which move passively through the gastrointestinal tract – were limited in their inability to interact with the bowel and carry-out interventions. A natural first approach to address this was to adopt “on-board actuation”: actively controlling the capsule using internal, miniature locomotion mechanisms (e.g. legs) (42).
However, enthusiasm for this approach declined rapidly as the research community realized a major challenge: integrating complex mechanisms, including an adequate power supply, into a “pill-sized” device (typically 24mm length, 11mm diameter) was an impractical solution using available technology.
The alternative approach of magnetic actuation was explored to solve this limitation. The use of magnetic coupling bypasses the need for intricate mechanisms, reduces on-board power needs and hence the overall size and complexity of the device. This form of actuation manipulates the capsule (containing an embedded magnet) via an externally generated magnetic field. This mechanically simple arrangement can precisely control capsule orientation and induce relative motion. The field may be generated by permanent magnets or electromagnets. In comparing the two: electromagnets provide an additional degree of control in varying the magnitude of magnetic field, though the volumetric magnetic flux density generated is lower than that of permanent magnets. Medical capsule robots are now a clinically viable alternative to standard interventional endoscopy.
While offering an elegant mechanical solution, researchers in the area were faced with the challenge of developing reliable control strategies – a complex task owing to the highly nonlinear properties of magnetic fields. These evolved from manual manipulation of a hand-held external permanent magnet, to robotic control of the magnetic field (43, 44). This was shown to be both clinically and commercially effective for the exploration of the stomach and is now available in hospitals (NaviCam, Ankon).
Effective interventional capabilities using magnetic actuation were successfully demonstrated in pill-size robots by combining it with soft robotics. A smart, compliant device operated by external magnetic fields showed the feasibility of actively moving to a site of interest and delivering a drug (45) or collecting tissue biopsies (46).
With a market pressure towards ease-of-use, combined with the complexities of magnetic actuation, the role of robot assistance in magnetic control of capsule endoscopes increased substantially. A key enabler for this was the introduction of real-time localization techniques. Knowing position and orientation (i.e. pose) of the capsule is crucial to plan the application of magnetic force and torque for the desired motion (47). Clinically-viable examples of localization are mainly based on magnetic localization (48). This is now enabling researchers to explore different levels of computer assistance, moving towards the ultimate goal of making endoscopy as intuitive as driving a car in a videogame.
As we begin the next decade, intelligent magnetic control of pill-sized robots may offer unprecedented diagnostic and therapeutic capabilities when combined with multimodal imaging (e.g. multi-spectral, auto-fluorescence, micro-ultrasound) and micro/nano-robotics. Aside from the clinical uses, this could provide a research platform to reach deeper into the human body to address other scientific questions related to, for example, our microbiome.
The future may also hold exciting advances in energy storage or wireless power transfer, which revive on-board actuation approaches, or “multi-scale operation”, as suggested in (46), where a pill-sized robot deploys an army of interventional micro-robots. Whatever lies ahead, medical capsule robotics remains an exciting, fast-moving and highly influential field of research.
Magnetic actuation for medicine
Long before magnetic fields were used to create images of the inside of the body, they were used to perform surgery. Evidence of the use of magnetic fields for extracting iron shavings accidently embedded within the eye dates back to at least the 17th century and also during the industrial revolution. In the 1950’s, the first research into their use for guiding catheters with magnets mounted on the tip began. However, a commercially available system did not appear until 2003 with Stereotaxis’ Niobe robotic magnetic navigation system, which uses two moving permanent magnets to generate changing magnetic fields for guiding endocardial ablation catheters to treat cardiac arrhythmias (Electrophysiology (EP) procedures). While the market penetration of this magnetically-guided catheter system has been slow, the past decade has seen increasing interest from researchers as well as medical device companies, and we see a linear increase in the number of papers published on the topic and an exponential increase in citations.
Modeling multi-DOF electromagnetic navigation systems.
One important breakthrough in magnetic actuation from the past decade, and the most highly cited paper in the field of magnetic actuation and microrobotics, is (49). This work generalized the physics and mathematics of an arbitrary number of geometrically arranged electromagnetics to exert a magnetic force and torque on a given magnetic body. This led the way for the robotics community to bring over fifty years of work in robotic manipulator control and design to bear onto the magnetic actuation problem. The patents that were generated from this work formed the basis for one company to develop a seven-electromagnet system that has been used to perform endocardial catheter ablations on several patients.
Magnetically guided microrobots.
As discussed in the previous section, capsule robots are relatively large devices enabling larger permanent magnets to be mounted in them allowing for magnetic field gradients to provide appreciable actuation force (43). As free-swimming devices become less than a millimeter in size, the amount of magnetic material that can be affixed to them makes field-gradient approaches challenging, and new magnetic actuation strategies are required. Inspired by the helical motion of flagellated bacteria as well as the traveling wave motion of flagellated eukaryotes such as spermatozoa, the first microrobots appeared prior to 2010. Helical structures, in particular, are well suited to magnetic actuation as rotation fields generated torque, which scales well with fluidic drag torques. In the past decade, robust fabrication techniques and effective models have been developed that have created opportunities for developing microrobots capable of performing useful medical tasks (50). A number of efforts continue in this direction with new impetus on using materials that will eventually biodegrade in the body without harm to the patient, or on developing magnetic tools for retrieving magnetic microrobots from the body after use.
Magnetic locomotion strategies at millimeter scales.
If the constraints on magnetic material selection are relaxed such that toxic hard magnetic particles are incorporated into flexible polymeric structures, millimeter-scale robot designs can be created that exhibit a number of new and exciting locomotion strategies. Many of these techniques culminated in recent work from Sitti’s group on a single device capable of multi-modal locomotion enabled by using a variety of dynamically varying magnetic fields (51). An impressive number of rolling, walking, jumping, and crawling motions were experimentally demonstrated in the paper.
Magnetically guided catheters.
Current trends in magnetic actuation show a return to its roots in which magnetically tipped catheters and endoscopes are being increasingly investigated. Zhao’s recent work (52) demonstrates the potential for magnetic actuation to be used to guide sub-millimeter hydrogel-covered catheters with embedded hard magnetic particles. This work identifies a number of medical procedures that could be performed with such devices in the future. Undoubtedly, the reason for this increasing interest is the promise for more maneuverable medical devices, at smaller scales, that can be manufactured more economically than complex pull-wire or motor-based devices.
The past decade has seen a number of advances in magnetic actuation for medicine. We have gained a deeper understanding of how to generate dynamically varying magnetic fields and field gradients that can harmlessly penetrate the entire human body. We have seen an increase in the use of soft polymeric materials, following the trends we see in Soft Robotics, with the goal of creating safer more maneuverable magnetic medical devices (48,49). Finally, we have also seen many of these efforts move to in vivo trials and even into humans. Certainly, the next decade will see more efficacious medical therapies realized using this technology, resulting in the rapid acceleration of commercial efforts.
Soft robotics for medicine
Defining which achievement in robotics launched the field of soft robotics for medicine is not trivial. Robotics based on soft concepts, intrinsically compliant structures, and smart materials was strictly joined to biomimetics and bioinspiration, from the beginning. On the other hand, the growing interest for bioinspired robots with compliant bodies has promoted the research on smart materials which could be adopted for fabricating soft robots or for providing soft robots with sensing and actuation capabilities, from the macroscale down to the nanoscale (53). Just to make an example, most works on artificial skins with sensing capabilities can be found in literature with application into soft robots and soft devices.
Looking at the literature of the last 10 years, there are many fundamental review or survey papers about soft and bioinspired robotics for a lot of applications (including medicine, where the issue of intrinsic safety is extremely relevant), and many material-science papers and reviews on novel smart materials, where traditional silicon-based technologies for sensing are replaced by silicone-based technologies with smart behavior.
Considering the most highly cited papers of the last decade and excluding materials papers and survey papers, two types of works related to medicine can be identified: one includes wearable soft robots for rehabilitation or human augmentation which have been covered in the previous sections. The second includes robots for intervention and surgery, or components for intervention and surgical robotics. Concerning the field of surgery and intervention, three parallel subtopics can be identified: i) soft devices for surgery or intervention, where the entire traditional device is replaced by a soft robotic design, both at the macro and miniature scale (54), and (45); ii) soft, bioinspired or compliant components, which can work as standalone devices or can be integrated into more traditional systems (55, 56); iii) soft components and systems for advanced simulators, both for training and for studying specific physiological functions (57–59), between robotics and bioartificial organs.
In the first category, some interesting designs of modular and tunable stiffness devices for surgery and endoscopy have been developed and have reached the pre-clinical or the cadaver test level (54). The main idea is transforming surgical manipulators into elephant trunks or octopus arms with the ability to do more tasks with the same arm, by simply changing the stiffness of the different segments. Relevant results have been achieved also applying soft robotics technology to gastrointestinal capsule endoscopy, with the development of soft-body capsules for performing targeted drug delivery, as already mentioned above(44, 54).
For the second category, bioinspired components – in some cases with a soft body or with a biomimetic safe interaction with the environment – have demonstrated superior capabilities in comparison with traditional devices (55, 60), e.g. in biopsy. But a soft and bioinspired design was already explored more than 20 years ago for advanced endoscopes with the attempt to adapt the shape of the medical tool to the features of the explored human environment (as in (45, 46) mentioned above).
Finally, there is a recent research direction, not easily falling into any categories, where soft robots are used for in vivo assistive or therapeutic devices (59, 61).
With the exception of some studies at the intersection between magnetic micro robotics and soft robotics, which have already reached the clinical stage, most of the presented technologies still need an extensive pre-clinical and clinical validation.
The field of soft robotics, even if it has not produced paradigmatic examples of medical robotic systems yet, is steering the design and development of most medical instrumentation. In parallel, soft robotics is also nurturing the research in soft materials and novel fabrication technologies, which can open unexpected avenues in biomedical applications.
Continuum robots for medicine
Continuum robots change shape through flexural deformation rather than through discrete joints. Their ability to take the shape of three-dimensional curves enables this type of robot to perform procedures through smaller surgical corridors than would be required by traditional robotic mechanisms. They can enter the body through natural orifices, navigate through body lumens and steer around critical structures when passing through solid tissue. The flexural compliance of continuum robots in contrast to conventional designs also enhances their safety.
Continuum robots can be characterized by the actuation method used to produce flexural shape change. The most common approach to shape control is by varying the displacement or tension force applied to one or more tendons arranged around a central flexible backbone. A variation on this technique, called multibackbone designs, replaces the tendon strings with rods which can apply both tensile and compressive forces. A third type, concentric tube robots, blurs the roles of the actuation elements and backbone by using the relative translation and rotation of pre-curved concentrically-combined superelastic tubes to effect shape changes. Magnetic actuation, discussed in detail in another section of this paper, is a fourth technique in which external magnets positioned around the patient are used to produce the desired deflection of a magnetically-tipped flexible tube.
In the decade preceding 2010, the major research progress involved the development of design principles and mechanics-based kinematic models for tendon- and multibackbone-actuated continuum robot architectures. This work led to important medical robot commercialization efforts such as Hansen Medical’s tendon-actuated cardiac catheter. In addition, a tendon-actuated design was proposed in which the flexible backbone was replaced by a series of short cylindrical links connected by spherical joints. This design became the basis of the surgical robot currently being commercialized by Medrobotics. During this decade, the concept of concentric tube robots was first introduced, but a more complete description of the design principles and kinematic model for this architecture only became complete in 2010 (62).
During the decade 2010–2020, continuum robot research was focused in four areas: (1) incorporating external contacts and loads in robot modeling and control, (2) developing methods to control robot stiffness, (3) creating “soft” continuum robots, and (4) the design of continuum robots for specific clinical applications. Each is described below.
Extending kinematic models to consider external contacts and loads.
In many medical applications, a robot will contact tissue not only at its tip, but also at many locations along its length. Unlike rigid robots, these contact forces can produce appreciable deformation of a continuum robot leading to large errors in the kinematic map relating, e.g., tendon tension to tip position and orientation. An important research thrust has been to include external loading in the kinematic model (63) as well as to infer external loads from the kinematic input variables, e.g., tendon tension forces (64). Alternatively, a model-free approach has been proposed in which the contact-constrained kinematic model is estimated during task execution (65). For model-based control methods, an alternative to inferring external loads from kinematic inputs is to directly sense them. While the creation of a distributed sensing skin at the size scale and price point appropriate for medical interventions remains an open problem, noteworthy effort over the decade has gone into the development of sensors that can estimate robot shape (66).
Stiffness control.
In contrast to rigid robots, the inherent flexibility of continuum robots enhances their safety during navigation through the body to a surgical site. Surgical tasks, however, involve applying forces to tissue and the lower tip stiffness of continuum robots require larger robot displacements to produce a given force. The task-based force level together with limited volume available to maneuver the robot define a minimum tip stiffness needed to perform the task. Important work over the decade has developed mechanical design methods for enhancing and controlling continuum robot stiffness, e.g., by incorporating layer jamming in the flexural components (67). For those situations when the inherent stiffness is sufficient, control algorithms have been developed which modify the kinematic inputs to achieve a desired tip stiffness (68).
Soft continuum robots.
Continuum robots are often fabricated from compliant polymeric materials and some of the earliest examples were actuated pneumatically or hydraulically – the two features typically used to define “soft” robots. With a few exceptions, however, medical continuum robots have eschewed gas or fluid actuation which tend to increase modeling complexity and response time. With the explosive growth in soft robotics over the last decade, however, these actuation methods as well as the use of even more compliant materials are now being explored for medical applications (69).
Application-specific continuum robot design.
In addition to deepening the technological toolbox, researchers have also collaborated with clinicians to create robotic systems designed to perform specific procedures. For example, (16) produced a single-port system for abdominal surgery. Once inserted into the abdomen, two multibackbone continuum arms along with a conventionally-jointed stereo endoscopic arm extend from a single sheath to create an anthropomorphic representation of the surgeon’s head and arms. This technology was licensed for commercialization by Titan Medical. As a second example, the system of (20) explores the use of two concentric tube robots together with a separate passive endoscope for transnasal skull-base surgery. This system was an important early demonstration of how the concentric tube architecture, along with the theoretical modeling developed to support it, could provide the workspace, stiffness and manipulability necessary to perform actual neurosurgical tasks.
The last decade has provided a maturation of the fundamental techniques for designing and modeling the various continuum robot architectures. Although this research is largely complete, the availability of new sensing technologies will likely spur the development of improved sensor-based control techniques. For example, Fiber Bragg Gratings (FBGs), a very expensive technology, is the main shape-sensing modality that has been investigated (66). An inexpensive alternative technology would likely result in a new generation of control algorithms. Furthermore, we will likely see continued interest in applying soft robotics to produce alternative robot designs as well as learning / AI applied to robot navigation and control. While this work will largely be driven by research novelty rather than clinical need, it will add to the technological toolbox.
While early validation experiments were academic in nature with little attention paid to eventual medical applications, there was a growing emphasis over the decade toward creating prototype systems such as those noted above that could perform actual medical procedures. For continuum robots to reach the clinic, this line of research will be increasingly important in the years ahead. There are several reasons for this. First, the creation and demonstration of a procedure-specific prototype is the fundamental step required to de-risk the technology for commercialization. It also enables a first-cut cost-benefit comparison with current clinical practice. Thus, these technology demonstration projects can directly lead to commercialization efforts. Equally important, procedure-specific prototypes serve to identify critical knowledge gaps that spur future fundamental research.
DISCUSSION
The number of papers on medical robotics has grown exponentially from less than 10 published in 1990 to more than 5200 in 2020. Consequently, the fraction of papers published during the last decade is over 80% of the total. These publications span the entire range of the research pipeline. Engineering journal publications have covered the creation of new robotic technologies for medical applications as well as the design of new medical robots. Medical journal publications have completed the research process by evaluating existing robot designs in human patients.
While the field cannot yet point to comprehensive clinical trials which show that robotic surgical procedures provide improved procedural outcomes for patients (70), or reduced procedure cost compared to non-robotic surgery (71), a number of patient benefits have been demonstrated. These include shorter hospital stays, faster recuperation, fewer reoperations and reduced blood transfusions (71). For surgeons, robots provide improved ergonomics, leading to reductions in neck and back pain (72) as well as hand and wrist numbness (73) with less physical and mental stress compared to direct hand-controlled procedures (74). These factors increase a surgeon’s quality of life and could potentially lengthen their career. Studies have also shown that robotics can dramatically reduce radiation exposure to both the surgeon and the patient (75).
To further this progress, it would be beneficial to channel future engineering research efforts in the most promising directions. This requires developing an understanding of how robots and their underlying technologies add value in medicine. While in almost all other industries, robots are employed as autonomous agents to reduce human labor costs, medical robots, at least to date, have been developed to add value in other application-dependent ways.
For example, all the benefits mentioned in the preceding paragraph arise in laparoscopic surgery except for reduced radiation exposure which applies to cardiac catheterization procedures. In therapeutic rehabilitation, it can be argued that the value currently added is in providing a larger number of repetitions rather than in improving the quality of the repetitions. On the other hand, energy-delivery robots, e.g., for radiotherapy, provide a combination of precision, repeatability and speed that is hard to match by other means. Similarly, a powered prosthesis can directly improve patient outcomes by expanding both the number and quality of daily living tasks that can be performed compared to a non-robotic device. In the same way, capsule robots may eventually replace some open bowel procedures, improving the diagnostic possibilities in hard-to-reach body regions and reducing the discomfort of existing endoluminal bowel procedures.
In directing robotic technology research to maximize value added, the most important technology targets are those that will enable new types of interventions that are either currently impossible or impractical based on current technology. Magnetic actuation is an example of such a technology that is enabling for capsule robots and medical microrobots. This technique has allowed miniaturization by moving actuation and power supplies outside the body. Soft robotics is likely to be a very important enabling technology over the next decade. Much of the most promising work is currently being performed in the materials community and relates to the creation of thin polymer layers with embedded sensors and actuators. While this work seems far from medical application now, these capabilities will likely have a large influence on interventional, rehabilitative and assistive robots. Other enabling technologies in sensing, imaging, actuation and energy storage may arise as crossovers from consumer electronics.
As an alternative to enabling new procedures, a technology can have a major influence if it provides a new way for a medical robot to add value. The effective synergy of pre-operative and intra-operative imaging integrated with flexible, ergonomically enhanced surgical tools is an important example of this approach which represents a substantial contribution over the last decade. The value of this approach will likely continue in the future. Translating cellular and molecular imaging modalities from the laboratory to an in vivo - in situ surgical setting will further expand the functional capabilities of surgical interventions by providing improved tissue detection, labelling, and targeting for both macroscopic and cell-based therapies. This approach can fundamentally alter the planned surgical pathways by streamlining intraoperative surgical decision making and optimization with increased consistency and accuracy, circumventing potential post-operative complications and revisions.
Another way for robots to add value is through autonomy. While the development of autonomous automotive driving capabilities has been perhaps the hottest topic in all of robotics over the decade, its use in medical robots is currently limited. Examples include assistive wearable robots and rehabilitation robots. These systems produce preprogrammed motions that can be switched between and altered based on user inputs. Similarly, orthopedic robots mill out preprogrammed cavities in bone and radiosurgery robots play back preprogrammed trajectories to produce the desired x-ray exposures of internal lesions. While these preprogrammed motions represent a very simple form of autonomy, they are enabling for these applications. For example, an assistive lower leg prosthesis would be useless if the operator had to actively control the ankle motion during walking.
The technological frontier in medical robot autonomy corresponds to endowing the robot with the capability to formulate and alter its plans and motions based on real-time sensor data. Examples could include autonomous laparoscopic surgery to remove cancerous lesions or autonomous transcatheter repair of a heart valve. This level of autonomy brings with it not only technical challenges, but also regulatory, ethical and legal challenges – which have yet to be fully resolved and will raise commercialization costs. Consequently, it will be much easier to incrementally add such autonomous functionality to pre-existing medical robots whose value can be justified without consideration of autonomous functionality. Examples include automated suturing for laparoscopic surgery, autonomous navigation of flexible endoscopes or autonomous electrophysiological catheter mapping inside the heart.
An evolutionary trend toward progressive automation as suggested by Fig. 4 will provide time for the necessary technological developments in algorithms and sensors while allowing stakeholders time to progressively construct an appropriate regulatory and legal framework. Medical applications for which autonomy is necessary to justify the robot will be more challenging to commercialize in the short term but may be of highest value in the long term. Lower hanging fruit of this type could include simple time-critical endoluminal interventions while bionic implants represent a more complicated class of devices.
Fig. 4. Application-specific trend toward increasing medical robot autonomy.
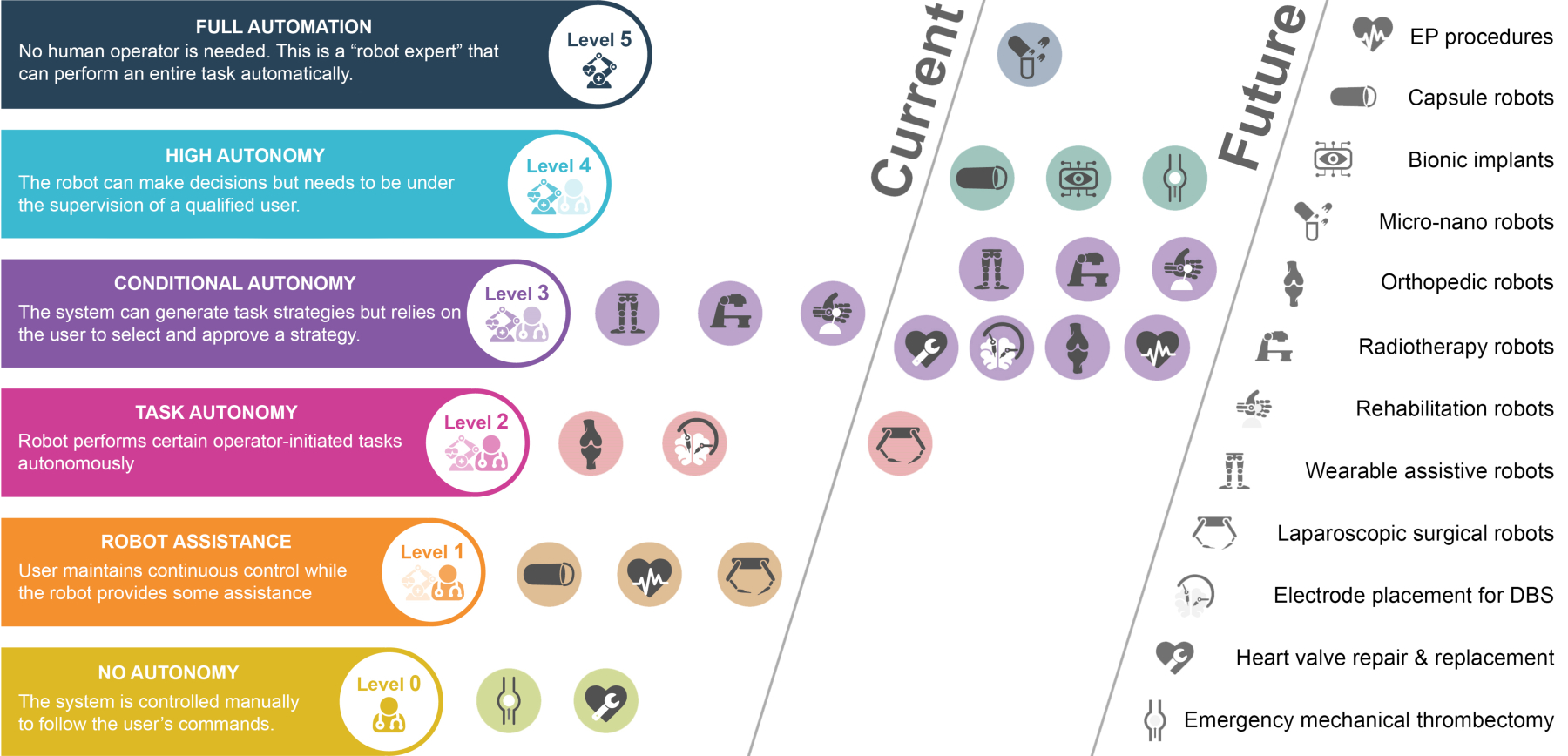
In current use, the level of autonomy is typically the minimum needed to be clinically useful. For example, radiotherapy robots operate at a level of conditional autonomy computing and executing a radiation exposure trajectory to provide the desired radiation dose inside a patient while minimizing exposure of surrounding tissues. Orthopedic robots are capable of autonomously milling out a prescribed cavity for knee and hip implants. In contrast, laparoscopic surgical robots have proven successful under continuous operator control and so currently offer only limited robotic assistance. Transcatheter mechanical thrombectomy and heart valve repair are examples of clinical applications for which robotic solutions have yet to be developed although both could potentially benefit from robotic solutions. In the future, it is anticipated that the level of autonomy of current robotic systems will increase. The biggest increases will be for those applications for which autonomy is vital to their function. For example, highly autonomous systems for remotely performing emergency mechanical thrombectomies to treat stroke would significantly increase the accessibility of this treatment while also decreasing the time to treatment. As a second example, bionic implants which improve or restore body functions will be sufficiently integrated with their host to not require continuous conscious control.
Of the more than 19,000 engineering papers published on medical robotics since 1990, only a handful can be considered enabling for existing commercial medical robots. Even the papers of high technological influence comprising the bibliography have modest numbers of patent citations. In part, this may be due to the substantial lag that can occur between technology development and its commercial application. Perhaps an equally important contributor is the mismatch between technology research and the realities of medical device commercialization.
Bringing robotic technology to clinical use requires much more than simply well-cited research articles. A genuine clinical need must be identified. A relevant technology must be developed to address this need that considers the specifics of how the robot adds value for the clinician and for the patient. Medical doctors must be convinced of this value proposition. The technology must also be developed with hospital administrative and financial constraints well-considered, and without hindering well established clinical workflows. Potential risks must be identified early on so that ethical approvals can be obtained. Finally, attractive business models must be developed to ensure that sufficient investment can be obtained to bring the technology through the complex pathways that must be navigated for any medical device to make it to commercial success. Maximizing the chance of success suggests that technology researchers stray from their ivory towers to form deep collaborations with clinicians, regulators, investors and the business community.
MATERIALS AND METHODS
The manuscript is not intended to be a traditional survey that provides sweeping coverage of medical robotics over the decade nor to provide an exhaustive bibliography of the field. Instead, our goal was to provide a focused view of the most important research advances of the decade and to point the reader to a small set of papers that are seminal with respect to these advances. Research was defined as the development of new robots and robotic technology. Clinical evaluation papers using existing robots were excluded unless they conveyed an important translational result.
This approach, by its nature, injects some subjectivity into the paper, however, we attempted to be as objective as possible. Our approach was as follows. We first developed an initial list of prospective hot topics based on author consensus. This list of topics was then validated and refined by performing a broad search of medical / surgical robotics using Web of Science and then grouping the results by topic. This resulted in dropping some candidate topics while subdividing others into multiple topics. For example, while there has been important work in orthopedic and spinal procedure robots, the highly cited papers were published prior to 2010. Furthermore, we observed that there was important research on procedure-specific robots that did not fit into any of the hot topics. This included robots developed for endoluminal and NOTES procedures along with robots for microsurgery. To include this work, we added a final hot topic on non-laparoscopic procedure-specific robots.
Given this list of hot topics, we then sought to identify topic-specific search terms for use with Web of Science that would provide comprehensive coverage for that topic. Our goal was two-fold. First, we wished to identify the total number of papers published on each hot topic as reported in Figures 2 and 3. Second, for inclusion in our bibliography, we wished to identify the most influential papers for each topic based on citation count.
Identification of the topic-specific search terms meeting these two goals was an iterative process. Initially, each search was formulated by building a set of common terms related to medical robots that returned the most comprehensive set of relevant references:
(medical* OR medicine OR surgical OR surgery OR surgeon (in TOPIC) AND robot* OR manipulator (in TOPIC)).
This search was then further constrained using keywords for each hot topic. The keywords were tested and revised by reviewing the search results based on the authors’ knowledge of the field to ensure that the results for the top 100 cited papers returned by the search were both relevant and comprehensive. This approach worked well for 4 out of the 8 topics. For the remaining 4 topics, it was also necessary to adapt the common search terms along with topic-specific keywords in order to identify a search that yielded relevant and comprehensive results.
Each section of the paper was then composed based on the authors’ knowledge of the topic as supported by the search results. For each hot topic, a small number of the most highly cited research papers were selected to support the major concepts. These are the papers included in the bibliography. While in some cases, papers had similar numbers of citations and subjective decisions were made to pick one over another, the overall selection process was objective. Survey papers were excluded.
Paper citation counts included in the bibliography are from Web of Science. Patent citation counts are from Lens.org. Data was collected on October 11, 2021.
Data within Figs. 2 and 3
Figs. 2 and 3 report the year-by-year numbers of publications resulting from the Web of Science searches for the individual and combined hot topic searches. The results are further broken down by publication type (engineering vs. medical journals). Searches were performed on October 11, 2021.
Web of Science search terms
The sets of search terms for each hot topic which are listed below were used with Web of Science to identify the most highly cited papers for each topic.
Robots for laparoscopic surgery
medical* OR medicine OR surgical OR surgery OR surgeon (in TOPIC) AND robot* OR manipulator (in TOPIC) AND laparoscop* (in TOPIC and TITLE)
Non-laparoscopic procedure-specific robots
medical* OR medicine OR surgical OR surgery OR surgeon (in TOPIC) AND robot* OR manipulator (in TOPIC) NOT laparoscop* (in TOPIC and TITLE)
Assistive wearable robotics
(prosthe* OR orthos* OR orthot* OR exoskelet* OR exosuit*) AND (robotic OR powered), all in TOPIC 2010–2020 Figure search: (prosthe* OR orthos* OR orthot* OR exoskelet* OR exosuit*) AND (robotic OR powered), NOT (rehab*), all in TOPIC 2010–2020
Therapeutic rehabilitation robots
(robot* OR exoskelet*) AND (rehab*)), all TOPIC 2010 – 2020
Medical capsule robots
(robot* ) AND (pill OR capsul*) AND (medic* OR endoscop* OR intestin* OR surg*) all TOPIC 2010 – 2020
Magnetic actuation for medicine
(robot* OR microrobot* OR nanorobot* OR manipulat* OR actuat*) AND (magnet* OR micromagnet* OR nanomagnet*) AND (medical* OR medicine* OR surgical* OR surgeon* OR surgery*) all in TOPIC 2010 – 2020
Soft robotics for medicine
(medical* OR medicine OR surgical OR surgery OR surgeon) AND (robot OR robotics) AND (soft) NOT (materials OR material) NOT (rehabilitation), all in TOPIC 2010 – 2020
Continuum robots for medicine
WoS Search: (medical* OR medicine OR surgical OR surgery OR surgeon) AND (robot* OR manipulator) AND (continuum OR snake) all in TOPIC 2010 – 2020
Supplementary Material
Acknowledgements:
We thank Dr. Margherita Mencattelli for her assistance with the figures and references.
Funding:
Partial support for PED was provided by the National Institutes of Health under grants R01NS099207 and R01HL124020.
Footnotes
Competing interests: None specific to the content of the paper.
Data and materials availability:
All data presented in the paper can be reproduced as described in the Materials and Methods section.
Bibliography and References Cited
- 1.Howe RD, Matsuoka Y, Robotics for surgery. Annual review of biomedical engineering 1, 211–240 (1999). Citations: 160 papers; 65 patents. [DOI] [PubMed] [Google Scholar]
- 2.Satava RM, Surgical robotics: the early chronicles: a personal historical perspective. Surgical Laparoscopy Endoscopy & Percutaneous Techniques 12, 6–16 (2002). Citations: 121 papers; 40 patents. [DOI] [PubMed] [Google Scholar]
- 3.Simaan N, Yasin RM, Wang L, Medical technologies and challenges of robot-assisted minimally invasive intervention and diagnostics. Annual Review of Control, Robotics, and Autonomous Systems 1, 465–490 (2018). Citations: 37 papers; 0 patents. [Google Scholar]
- 4.Kwoh YS, Hou J, Jonckheere EA, Hayati S, A robot with improved absolute positioning accuracy for CT guided stereotactic brain surgery. IEEE Transactions on Biomedical Engineering 35, 153–160 (1988). Citations: 491 papers; 99 patents. [DOI] [PubMed] [Google Scholar]
- 5.Taylor RH, Mittelstadt BD, Paul HA, Hanson W, Kazanzides P, Zuhars JF, Williamson B, Musits BL, Glassman E, Bargar WL, An image-directed robotic system for precise orthopaedic surgery. IEEE Transactions on Robotics and Automation 10, 261–275 (1994). Citations: 156 papers, 46 patents. [Google Scholar]
- 6.Marescaux J, Leroy J, Gagner M, Rubino F, Mutter D, Vix M, Butner SE, Smith MK, Transatlantic robot-assisted telesurgery. Nature 413, 379–380 (2001). Citations: 512 papers; 2 patents. [DOI] [PubMed] [Google Scholar]
- 7.Hannaford B, Rosen J, Friedman DW, King H, Roan P, Cheng L, Glozman D, Ma J, Kosari SN, White L, Raven-II: an open platform for surgical robotics research. IEEE Transactions on Biomedical Engineering 60, 954–959 (2012). Citations: 184 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 8.Kazanzides P, Chen Z, Deguet A, Fischer GS, Taylor RH, DiMaio SP, An open-source research kit for the da Vinci® Surgical System. paper presented at the 2014 IEEE international conference on robotics and automation (ICRA), 2014. Citations: 145 papers; 0 patents. [Google Scholar]
- 9.Sarikaya D, Corso JJ, Guru KA, Detection and localization of robotic tools in robot-assisted surgery videos using deep neural networks for region proposal and detection. IEEE transactions on medical imaging 36, 1542–1549 (2017). Citations: 75 papers; 5 patents. [DOI] [PubMed] [Google Scholar]
- 10.Murali A, Sen S, Kehoe B, Garg A, McFarland S, Patil S, Boyd WD, Lim S, Abbeel P, Goldberg K, Learning by observation for surgical subtasks: Multilateral cutting of 3d viscoelastic and 2d orthotropic tissue phantoms. paper presented at the 2015 IEEE International Conference on Robotics and Automation (ICRA), 2015. Citations: 54 papers; 0 patents. [Google Scholar]
- 11.Shademan A, Decker RS, Opfermann JD, Leonard S, Krieger A, Kim PC, Supervised autonomous robotic soft tissue surgery. Science translational medicine 8, 337ra364–337ra364 (2016). Citations: 176 papers; 1 patents. [DOI] [PubMed] [Google Scholar]
- 12.Jafari MD, Lee KH, Halabi WJ, Mills SD, Carmichael JC, Stamos MJ, Pigazzi A, The use of indocyanine green fluorescence to assess anastomotic perfusion during robotic assisted laparoscopic rectal surgery. Surgical endoscopy 27, 3003–3008 (2013). Citations: 188 papers. [DOI] [PubMed] [Google Scholar]
- 13.Hong MB, Jo Y-H, Design and evaluation of 2-DOF compliant forceps with force-sensing capability for minimally invasive robot surgery. IEEE Transactions on Robotics 28, 932–941 (2012). Citations: 51 papers; 0 patents. [Google Scholar]
- 14.Kim U, Lee D-H, Yoon WJ, Hannaford B, Choi HR, Force sensor integrated surgical forceps for minimally invasive robotic surgery. IEEE Transactions on Robotics 31, 1214–1224 (2015). Citations: 89 papers; 0 patents. [Google Scholar]
- 15.Piccigallo M, Scarfogliero U, Quaglia C, Petroni G, Valdastri P, Menciassi A, Dario P, Design of a novel bimanual robotic system for single-port laparoscopy. IEEE/ASME Transactions on mechatronics 15, 871–878 (2010). Citations: 125 papers; 23 patents. [Google Scholar]
- 16.Ding J, Goldman RE, Xu K, Allen PK, Fowler DL, Simaan N, Design and coordination kinematics of an insertable robotic effectors platform for single-port access surgery. IEEE/ASME transactions on mechatronics 18, 1612–1624 (2012). Citations: 98 papers; 6 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tortora G, Dario P, Menciassi A, Array of robots augmenting the kinematics of endocavitary surgery. IEEE/ASME transactions on mechatronics 19, 1821–1829 (2014). Citations: 33 papers; 0 patents. [Google Scholar]
- 18.Castro CA, Alqassis A, Smith S, Ketterl T, Sun Y, Ross S, Rosemurgy A, Savage PP, Gitlin RD, A wireless robot for networked laparoscopy. IEEE Transactions on Biomedical Engineering 60, 930–936 (2012). Citations: 37 papers; 1 patents. [DOI] [PubMed] [Google Scholar]
- 19.Shang J, Noonan DP, Payne C, Clark J, Sodergren MH, Darzi A, Yang G-Z, An articulated universal joint based flexible access robot for minimally invasive surgery. paper presented at the 2011 IEEE international conference on robotics and automation, 2011. Citations: 102 papers; 11 patents. [Google Scholar]
- 20.Burgner J, Rucker DC, Gilbert HB, Swaney PJ, Russell PT, Weaver KD, Webster RJ, A telerobotic system for transnasal surgery. IEEE/ASME Transactions on Mechatronics 19, 996–1006 (2013). Citations: 151 papers; 5 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rivera-Serrano CM, Johnson P, Zubiate B, Kuenzler R, Choset H, Zenati M, Tully S, Duvvuri U, A transoral highly flexible robot: novel technology and application. The Laryngoscope 122, 1067–1071 (2012). Citations: 47 papers; 6 patents. [DOI] [PubMed] [Google Scholar]
- 22.MacLachlan RA, Becker BC, Tabarés JC, Podnar GW, Lobes LA, Riviere CN, Micron: an actively stabilized handheld tool for microsurgery. IEEE Transactions on Robotics 28, 195–212 (2011). Citations: 141 papers; 7 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Üneri A, Balicki MA, Handa J, Gehlbach P, Taylor RH, Iordachita I, New steady-hand eye robot with micro-force sensing for vitreoretinal surgery. paper presented at the 2010 3rd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, 2010. Citations: 139 papers; 18 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Edwards TL, Xue K, Meenink HCM, Beelen MJ, Naus GJL, Simunovic MP, Latasiewicz M, Farmery AD, de Smet MD, MacLaren RE, First-in-human study of the safety and viability of intraocular robotic surgery. Nature Biomedical Engineering 2, 649–656 (2018). Citations: 48 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sup F, Varol HA, Goldfarb M, Upslope walking with a powered knee and ankle prosthesis: initial results with an amputee subject. IEEE transactions on neural systems and rehabilitation engineering 19, 71–78 (2010). Citations: 161 papers; 5 patents. [DOI] [PubMed] [Google Scholar]
- 26.Gregg RD, Lenzi T, Hargrove LJ, Sensinger JW, Virtual constraint control of a powered prosthetic leg: From simulation to experiments with transfemoral amputees. IEEE Transactions on Robotics 30, 1455–1471 (2014). Citations: 98 papers; 5 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Young A, Kuiken T, Hargrove L, Analysis of using EMG and mechanical sensors to enhance intent recognition in powered lower limb prostheses. Journal of neural engineering 11, 056021 (2014). Citations: 90 papers; 1 patents. [DOI] [PubMed] [Google Scholar]
- 28.Hargrove LJ, Miller LA, Turner K, Kuiken TA, Myoelectric pattern recognition outperforms direct control for transhumeral amputees with targeted muscle reinnervation: a randomized clinical trial. Scientific reports 7, 1–9 (2017). Citations: 67 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rossini PM, Micera S, Benvenuto A, Carpaneto J, Cavallo G, Citi L, Cipriani C, Denaro L, Denaro V, Di Pino G, Ferreri F, Guglielmelli E, Hoffmann K-P, Raspopovic S, Rigosa J, Rossini L, Tombini M, Dario P, Double nerve intraneural interface implant on a human amputee for robotic hand control. Clinical neurophysiology 121, 777–783 (2010). Citations: 243 papers; 3 patents. [DOI] [PubMed] [Google Scholar]
- 30.Raspopovic S, Capogrosso M, Petrini FM, Bonizzato M, Rigosa J, Di Pino G, Carpaneto J, Controzzi M, Boretius T, Fernandez E, Granata G, Oddo CM, Citi L, Ciancio AL, Cipriani C, Carrozza MC, Jensen W, Guglielmelli E, Stieglitz T, Rossini PM, Micera S, Restoring natural sensory feedback in real-time bidirectional hand prostheses. Science translational medicine 6, 222ra219–222ra219 (2014). Citations: 484 papers, 11 patents. [DOI] [PubMed] [Google Scholar]
- 31.Tan DW, Schiefer MA, Keith MW, Anderson JR, Tyler J, Tyler DJ, A neural interface provides long-term stable natural touch perception. Science translational medicine 6, 257ra138–257ra138 (2014). Citations: 372 papers; 17 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Farris RJ, Quintero HA, Murray SA, Ha KH, Hartigan C, Goldfarb M, A preliminary assessment of legged mobility provided by a lower limb exoskeleton for persons with paraplegia. IEEE Transactions on neural systems and rehabilitation engineering 22, 482–490 (2013). Citations: 101 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Awad LN, Bae J, O’donnell K, De Rossi SM, Hendron K, Sloot LH, Kudzia P, Allen S, Holt KG, Ellis TD, A soft robotic exosuit improves walking in patients after stroke. Science translational medicine 9, (2017). Citations: 196 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 34.Mao Y, Agrawal SK, Design of a cable-driven arm exoskeleton (CAREX) for neural rehabilitation. IEEE Transactions on Robotics 28, 922–931 (2012). Citations: 217 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 35.Polygerinos P, Wang Z, Galloway KC, Wood RJ, Walsh CJ, Soft robotic glove for combined assistance and at-home rehabilitation. Robotics and Autonomous Systems 73, 135–143 (2015). Citations: 619 papers; 10 patents. [Google Scholar]
- 36.Pehlivan AU, Losey DP, O’Malley MK, Minimal assist-as-needed controller for upper limb robotic rehabilitation. IEEE Transactions on Robotics 32, 113–124 (2015). Citations: 95 papers; 0 patents. [Google Scholar]
- 37.Duschau-Wicke A, Caprez A, Riener R, Patient-cooperative control increases active participation of individuals with SCI during robot-aided gait training. Journal of neuroengineering and rehabilitation 7, 1–13 (2010). Citations: 104 papers; 18 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cramer SC, Sur M, Dobkin BH, O’brien C, Sanger TD, Trojanowski JQ, Rumsey JM, Hicks R, Cameron J, Chen D, Harnessing neuroplasticity for clinical applications. Brain 134, 1591–1609 (2011). Citations: 491 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Krebs HI, Palazzolo JJ, Dipietro L, Ferraro M, Krol J, Rannekleiv K, Volpe BT, Hogan N, Rehabilitation robotics: Performance-based progressive robot-assisted therapy. Autonomous robots 15, 7–20 (2003). Citations: 450 papers; 4 patents. [Google Scholar]
- 40.Ang KK, Chua KSG, Phua KS, Wang C, Chin ZY, Kuah CWK, Low W, Guan C, A randomized controlled trial of EEG-based motor imagery brain-computer interface robotic rehabilitation for stroke. Clinical EEG and neuroscience 46, 310–320 (2015). Citations: 198 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 41.Scott SH, Dukelow SP, Potential of robots as next-generation technology for clinical assessment of neurological disorders and upper-limb therapy. Journal of Rehabilitation Research & Development 48, (2011). Citations: 103 papers; 2 patents. [DOI] [PubMed] [Google Scholar]
- 42.Valdastri P, Webster RJ III, Quaglia C, Quirini M, Menciassi A, Dario P, A new mechanism for mesoscale legged locomotion in compliant tubular environments. IEEE Transactions on Robotics 25, 1047–1057 (2009). Citations: 147 papers; 5 patents. [Google Scholar]
- 43.Ciuti G, Valdastri P, Menciassi A, Dario P, Robotic magnetic steering and locomotion of capsule endoscope for diagnostic and surgical endoluminal procedures. Robotica 28, 199–207 (2010). Citations: 167 papers; 7 patents. [Google Scholar]
- 44.Carpi F, Kastelein N, Talcott M, Pappone C, Magnetically controllable gastrointestinal steering of video capsules. IEEE Transactions on Biomedical Engineering 58, 231–234 (2010). Citations: 119 papers; 5 patents. [DOI] [PubMed] [Google Scholar]
- 45.Yim S, Sitti M, Design and rolling locomotion of a magnetically actuated soft capsule endoscope. IEEE Transactions on Robotics 28, 183–194 (2011). Citations: 183 papers; 2 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Yim S, Gultepe E, Gracias DH, Sitti M, Biopsy using a magnetic capsule endoscope carrying, releasing, and retrieving untethered microgrippers. IEEE Transactions on Biomedical Engineering 61, 513–521 (2013). Citations: 120 papers; 3 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mahoney AW, Abbott JJ, Five-degree-of-freedom manipulation of an untethered magnetic device in fluid using a single permanent magnet with application in stomach capsule endoscopy. The International Journal of Robotics Research 35, 129–147 (2016). Citations: 90 papers; 0 patents. [Google Scholar]
- 48.Di Natali C, Beccani M, Valdastri P, Real-time pose detection for magnetic medical devices. IEEE Transactions on Magnetics 49, 3524–3527 (2013). Citations: 59 papers; 5 patents. [Google Scholar]
- 49.Kummer MP, Abbott JJ, Kratochvil BE, Borer R, Sengul A, Nelson BJ, OctoMag: An electromagnetic system for 5-DOF wireless micromanipulation. IEEE Transactions on Robotics 26, 1006–1017 (2010). Citations: 531 papers; 5 patents. [Google Scholar]
- 50.Tottori S, Zhang L, Qiu F, Krawczyk KK, Franco-Obregón A, Nelson BJ, Magnetic helical micromachines: fabrication, controlled swimming, and cargo transport. Advanced materials 24, 811–816 (2012). Citations: 683 papers; 3 patents. [DOI] [PubMed] [Google Scholar]
- 51.Hu W, Lum GZ, Mastrangeli M, Sitti M, Small-scale soft-bodied robot with multimodal locomotion. Nature 554, 81–85 (2018). Citations: 607 papers; 4 patents. [DOI] [PubMed] [Google Scholar]
- 52.Kim Y, Parada GA, Liu S, Zhao X, Ferromagnetic soft continuum robots. Science Robotics 4, (2019). Citations: 180 papers; 1 patents. [DOI] [PubMed] [Google Scholar]
- 53.Cangialosi A, Yoon C, Liu J, Huang Q, Guo J, Nguyen TD, Gracias DH, Schulman R, DNA sequence–directed shape change of photopatterned hydrogels via high-degree swelling. Science 357, 1126–1130 (2017). Citations: 174 papers; 2 patents. [DOI] [PubMed] [Google Scholar]
- 54.Abidi H, Gerboni G, Brancadoro M, Fras J, Diodato A, Cianchetti M, Wurdemann H, Althoefer K, Menciassi A, Highly dexterous 2-module soft robot for intra-organ navigation in minimally invasive surgery. The International Journal of Medical Robotics and Computer Assisted Surgery 14, e1875 (2018). Citations: 28 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 55.Ko SY, Frasson L, y Baena FR, Closed-loop planar motion control of a steerable probe with a “programmable bevel” inspired by nature. IEEE Transactions on Robotics 27, 970–983 (2011). Citations: 64 papers; 0 patents. [Google Scholar]
- 56.Levering V, Wang Q, Shivapooja P, Zhao X, López GP, Soft Robotic Concepts in Catheter Design: an On-Demand Fouling-Release Urinary Catheter. Advanced healthcare materials 3, 1588–1596 (2014). Citations: 33 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Roche ET, Horvath MA, Wamala I, Alazmani A, Song S-E, Whyte W, Machaidze Z, Payne CJ, Weaver JC, Fishbein G, Kuebler JD, Vasilyev NV, Mooney DJ, Pigula FA, Walsh CJ, Soft robotic sleeve supports heart function. Science translational medicine 9, (2017). Citations: 147 papers; 3 patents. [DOI] [PubMed] [Google Scholar]
- 58.Chen F, Dirven S, Xu W, Li X, Soft actuator mimicking human esophageal peristalsis for a swallowing robot. IEEE/ASME Transactions on Mechatronics 19, 1300–1308 (2013). Citations: 34 papers; o patents. [Google Scholar]
- 59.Payne CJ, Wamala I, Abah C, Thalhofer T, Saeed M, Bautista-Salinas D, Horvath MA, Vasilyev NV, Roche ET, Pigula FA, An implantable extracardiac soft robotic device for the failing heart: mechanical coupling and synchronization. Soft robotics 4, 241–250 (2017). Citations: 28 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 60.Liu H, Li J, Song X, Seneviratne LD, Althoefer K, Rolling indentation probe for tissue abnormality identification during minimally invasive surgery. IEEE Transactions on Robotics 27, 450–460 (2011). Citations: 64 papers; 2 patents. [Google Scholar]
- 61.Damian DD, Price K, Arabagi S, Berra I, Machaidze Z, Manjila S, Shimada S, Fabozzo A, Arnal G, Van Story D, In vivo tissue regeneration with robotic implants. Science Robotics 3, (2018). Citations: 14 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 62.Dupont PE, Lock J, Itkowitz B, Butler E, Design and control of concentric-tube robots. IEEE Transactions on Robotics 26, 209–225 (2009). Citations: 412 papers; 16 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rucker DC, Jones BA, Webster III RJ, A geometrically exact model for externally loaded concentric-tube continuum robots. IEEE transactions on robotics 26, 769–780 (2010). Citations: 218 papers; 14 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Xu K, Simaan N, Intrinsic wrench estimation and its performance index for multisegment continuum robots. IEEE Transactions on Robotics 26, 555–561 (2010). Citations: 76 papers; 7 patents. [Google Scholar]
- 65.Yip MC, Camarillo DB, Model-less feedback control of continuum manipulators in constrained environments. IEEE Transactions on Robotics 30, 880–889 (2014). Citations: 103 papers; 0 patents. [Google Scholar]
- 66.Xu R, Yurkewich A, Patel RV, Curvature, torsion, and force sensing in continuum robots using helically wrapped FBG sensors. IEEE Robotics and Automation Letters 1, 1052–1059 (2016). Citations: 99 papers; 1 patents. [Google Scholar]
- 67.Kim Y-J, Cheng S, Kim S, Iagnemma K, A novel layer jamming mechanism with tunable stiffness capability for minimally invasive surgery. IEEE Transactions on Robotics 29, 1031–1042 (2013). Citations: 174 papers; 5 patents. [Google Scholar]
- 68.Mahvash M, Dupont PE, Stiffness control of surgical continuum manipulators. IEEE Transactions on Robotics 27, 334–345 (2011). Citations: 144 papers; 9 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Cianchetti M, Ranzani T, Gerboni G, Nanayakkara T, Althoefer K, Dasgupta P, Menciassi A, Soft robotics technologies to address shortcomings in today’s minimally invasive surgery: the STIFF-FLOP approach. Soft robotics 1, 122–131 (2014). Citations: 237 papers; 1 patents. [Google Scholar]
- 70.Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderäng U, Thorsteinsdottir T, Lagerkvist M, Damber J-E, Bjartell A, Hugosson J, Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: a prospective, controlled, nonrandomised trial. European urology 68, 216–225 (2015). Citations: 216 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 71.Forsmark A, Gehrman J, Angenete E, Bjartell A, Björholt I, Carlsson S, Hugosson J, Marlow T, Stinesen-Kollberg K, Stranne J, Health economic analysis of open and robot-assisted laparoscopic surgery for prostate cancer within the prospective multicentre LAPPRO trial. European urology 74, 816–824 (2018). Citations: 22 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 72.Bagrodia A, Raman JD, Ergonomic considerations of radical prostatectomy: physician perspective of open, laparoscopic, and robot-assisted techniques. Journal of endourology 23, 627–633 (2009). [DOI] [PubMed] [Google Scholar]
- 73.Gofrit ON, Mikahail AA, Zorn KC, Zagaja GP, Steinberg GD, Shalhav AL, Surgeons’ perceptions and injuries during and after urologic laparoscopic surgery. Urology 71, 404–407 (2008). Citations: 59 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
- 74.van der Schatte Olivier R. v., van’t Hullenaar C, Ruurda J, Broeders I, Ergonomics, user comfort, and performance in standard and robot-assisted laparoscopic surgery. Surgical endoscopy 23, 1365–1371 (2009). Citations: 90 papers; 0 patents. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Patel TM, Shah SC, Soni YY, Radadiya RC, Patel GA, Tiwari PO, Pancholy SB, Comparison of Robotic Percutaneous Coronary Intervention With Traditional Percutaneous Coronary Intervention: A Propensity Score–Matched Analysis of a Large Cohort. Circulation: Cardiovascular Interventions 13, e008888 (2020). Citations: 9 papers; 0 patents. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
All data presented in the paper can be reproduced as described in the Materials and Methods section.