

Introduction
Quality is never an accident; it is always the result of high intention, sincere effort, intelligent direction and skillful execution; it represents the wise choice of many alternatives, the cumulative experience of many masters of craftsmanship.
William A Foster
Nursing has a long history of high intention, sincere effort and skillful execution in the implementation of quality and patient safety efforts. The generation of new knowledge through empiric research and the development of practice-based evidence provide the foundation for these efforts. To support intelligent direction and wise choice several emerging areas in quality and safety research deserve greater emphasis over the next decade.
Improving quality involves assessing process and outcome measures of safety, effectiveness, patient-centredness, timeliness, efficiency and equity, as well as strengthening the capacity of health systems and clinical practices to create and sustain an organisational culture of quality and safety (Institute of Medicine, 2001). This Perspectives piece highlights several promising topic areas in quality and safety research, practice improvement and implementation science (IS). These perspectives are informed by my experiences as a researcher, advanced practice provider and leader of interprofessional healthcare teams. From 2010 to 2018, I was privileged to serve as a healthcare scientist and a division director at the Agency for Healthcare Research and Quality (AHRQ), an agency within the United States Department of Health and Human Services. AHRQ’s mission is to implement evidence and develop tools and strategies to help health systems and frontline healthcare workers deliver safe, high-quality, high-value healthcare that is also accessible, equitable and affordable. These experiences as a clinician and a scientist inspire my passion to develop methodologies, new knowledge and initiatives, and system-wide capacity designed to improve quality and safety in all healthcare settings.
Definitions of healthcare quality
Several published definitions of healthcare quality exist. Three frequently referenced definitions of healthcare quality are:
The extent to which healthcare services provided to individuals and patient populations improve desired health outcomes. In order to achieve this, healthcare must be safe, effective, timely, efficient, equitable and people-centred (Hanefeld et al., 2017).
The degree to which healthcare services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge (Institute of Medicine, 2001).
The degree to which the treatment dispensed increases the patient’s chances of achieving the desired results and diminishes the chances of undesirable results, having regard to the current state of knowledge (Busse et al., 2019).
All these definitions include a focus on individual and population health, the centrality of our evolving scientific evidence base and technical sophistication, the goal of improving outcomes, and the importance of the patient–provider relationship and shared decision-making.
IS and improvement science
Across the globe, practitioners, leaders and policy-makers struggle to ensure the uptake of rapidly evolving scientific knowledge, support the adoption of high value clinical procedures, technologies and organisational models, and discourage continued use of practices that do not or no longer have high value (Bauer and Kirchner, 2020; Leppin et al., 2019). These efforts are all designed to achieve optimal healthcare outcomes at the individual and population level. This growing field of research focused on how to improve healthcare practice is known under various names, including improvement science, dissemination and implementation research, and knowledge transfer or knowledge translation (KT) (Check et al., 2020; Granger, 2018).
Historically, patient safety and quality improvement efforts have largely focused on the detection and management of errors, improvement of a specific aspect of care quality (e.g. medication reconciliation) (Russ et al., 2020), and reduction of unwarranted variations in patient outcomes (e.g. diabetes management) (MacKay et al., 2020). As such, improvement science has emphasised measurement, feedback to decision-makers, and organisational change all in order to address a well-defined clinical problem or quality gap. Quality improvement efforts are often local, and typically are not studied to determine what works. Moreover, they may not be disseminated, and there is variable compliance with Standards for Quality Improvement Reporting Excellence (SQUIRE) guidelines (Goodman et al., 2016).
IS has a broader focus, and is defined as the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine care delivery, thereby improving quality and effectiveness (Eccles and Mittman, 2006). IS offers theory and methods to: (a) identify barriers and facilitators to implementation; (b) understand influences on professional and organisational behaviour; (c) select techniques to optimise implementation of practice improvements and anticipate and manage implementation failures; (d) evaluate effectiveness and efficiency of implementation; and (e) enhance sustainability (Bauer et al., 2015; Lasinski et al., 2021; Rapport et al., 2018).
KT is a key component of IS. Grimshaw et al. (2012) define KT as ‘ensuring that stakeholders are aware of and use research evidence to inform their health and healthcare decision-making’(Grimshaw et al., 2012). This definition recognises that there is a wide range of stakeholders or target audiences for KT, including policy-makers, professionals (e.g. clinical providers), consumers (e.g. patients and informal caregivers) and researchers. KT emphasises approaches to synthesise knowledge and build awareness (e.g. systematic reviews, guidelines), dissemination of information in ways that are acceptable to busy practitioners (e.g. toolkits, clinical decision support (CDS)) and strategies that are designed to change practitioner behaviour (e.g. academic detailing, communities of practice).
Increasingly it is acknowledged that efforts to improve clinician capacity to access and use research will have only a limited effect unless organisational and system-wide barriers are simultaneously addressed (Bowen et al., 2009; Ellen et al., 2014). The models and theories of IS uniquely offer a set of methodological frameworks that can be applied to design and evaluate a multi-level approach to adoption, scale-up and sustainment of evidence-based practice change (Nilsen, 2015). IS methods are ideally suited to identify and manage organisational and system-wide enablers and barriers (Moullin et al., 2020). IS also offers measurement science to evaluate both implementation outcomes and patient-focused outcomes (Allen et al., 2020).
IS makes prominent use of theoretical approaches in order to understand better and explain how and why implementation succeeds or fails. More than 100 different IS models, frameworks and theories have been proposed, and there have been many narrative reviews describing their similarities and differences (Nilsen, 2015; Villalobos Dintrans et al., 2019). Most IS theory distinguishes individual, organisational, system-related and innovation-related determinants of implementation. Implementation theories can be used to inform the evaluation of barriers and facilitators, identify stakeholders and select implementation strategies and outcomes, at practitioner, team and organisational levels (Moullin et al., 2020). Notably, some IS frameworks are better suited than others for specific kinds of implementation contexts (e.g. sustainability) (Birken et al., 2020), and some may be more conducive to integration and dialogue across disciplinary boundaries (Harrison and Shortell, 2020; Mitchell et al., 2010).
IS complements and extends our traditional conceptual model of outcomes research, by explicating the link from evidence-based interventions to improved outcomes in heterogeneous patient populations and settings, many of which also have varying contextual influences. Proctor et al. distinguish three components of outcomes measurement. These are: (a) implementation outcomes (e.g. acceptability, adoption, feasibility, penetration or uptake and sustainability); (b) service outcomes (e.g. efficacy, safety, effectiveness); and (c) client outcomes (e.g. satisfaction, quality of life, mortality) (Proctor et al., 2011). Several recent reviews have summarised the domains and quantitative measurement properties of the available instruments to capture implementation outcomes (Allen et al., 2020; Khadjesari et al., 2020; Lewis et al., 2015). Qualitative methods are also essential in implementation research, because practice improvements must be feasible and acceptable in real-world conditions, which are inherently complex and shifting (Hamilton and Finley, 2019). Qualitative and mixed methods research designs allow for an in-depth consideration of the dynamic context of implementation – including institutional structures, stakeholder groups’ interests and interactions, human–technology interactions, and social, political, economic and legal conditions.
Information systems and technology
Towards the future, technology-enabled KT strategies will be increasingly important in achieving improved quality and safety. These include social media, email/text, electronic databases, electronic prompts and reminders, and web-supported training, dissemination and patient–provider and provider–provider interactions. These strategies may function as push strategies or pull strategies. With push strategies evidence is disseminated (e.g. via social media) to targeted groups of clinicians, patients and policy-makers to increase awareness. Pull strategies aim to increase the targeted users’ demand for and use of evidence (e.g. webinars to improve research literacy) (Brown et al., 2020).
Technologies that hold promise to improve quality and safety include telehealth, mobile health and CDS. Telehealth use, particularly in ambulatory settings, has been widely adopted during the coronavirus disease (covid-19) pandemic and has the potential to improve patient–provider engagement and access, particularly in rural and underserved areas (Batsis et al., 2019). Mobile health technologies including patient portals, wearables and other patient-facing applications (Llorens-Vernet and Miró, 2020; Lu et al., 2020) can be leveraged to transfer knowledge to patients and informal caregivers, thereby optimising adherence, healthy behaviours and self-management (Abbasgholizadeh Rahimi et al., 2017; Chapman et al., 2020; Obro et al., 2020). Finally, CDS holds promise in improving care quality and safety. A meta-analysis of controlled trials examining the effects of CDS on quality confirms that it improves the delivery of guideline-concordant care, reduces ordering errors for diagnostic tests and medications and encourages de-implementation of ineffective or harmful care practices (Kwan et al., 2020).
Evidentiary sources for quality whole person care
A proactive engagement among interprofessional teams, QI programmes and embedded implementation scientists is essential to identify gaps in quality and safety, define key metrics and data that should be collected and presented to stakeholders on a regular basis, and support the generation of both QI initiatives and implementation research. A proposed model of the evidentiary data sources essential for person-centred, evidence-based clinical decision-making is depicted in Figure 1. Exogenous evidence is supplied by published research, evidence-based guidelines, benchmarking based on other health systems and patient registries. Endogenous evidence is derived from health system population data, organisational quality monitoring systems, focused implementation and practice improvement efforts and public health data. Patients’ electronic health records and the quality metrics routinely reported to individual providers and teams offer essential contextual information. Application of this framework can serve to strengthen quality and safety initiatives and focus improvement science efforts throughout all levels of the organisation.
Figure 1.
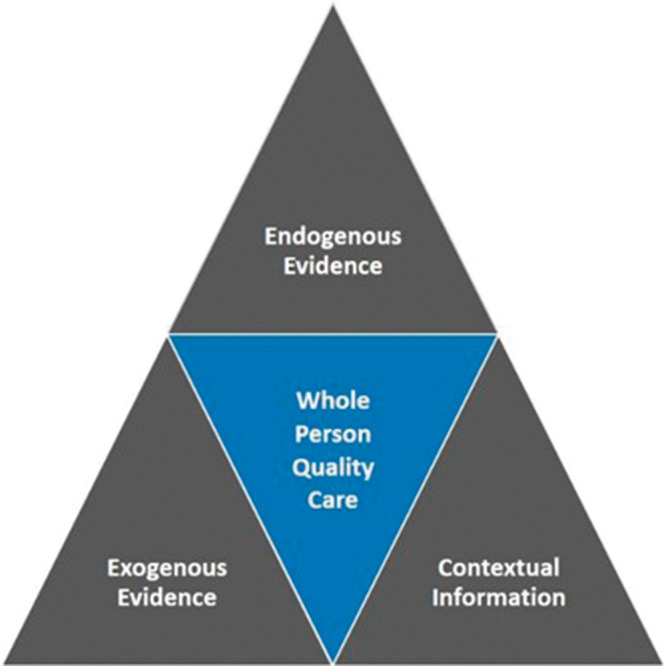
Evidentiary sources for quality care.
New and emerging approaches to improving quality and safety
Over the past decade, leaders of healthcare organisations have embraced the principles of high reliability organisations (HROs) to reduce practice variation and mitigate safety risks (Cochrane et al., 2017). Principles of HROs derive from industries that include nuclear power plants and aviation. These industries, like healthcare, have a high potential for risk, may be dynamic and unpredictable, and are heavily reliant on people rather than technology to prevent errors and harm. HRO principles emphasise finding and fixing problems and operational failures, identifying and preventing errors and near misses, and strengthening situational awareness among all staff involved in processes in which there is potential for harm. HRO-focused health systems emphasise the importance of understanding how all the parts of the system work together to prevent errors, and they prioritise frontline staff as experts in the decision-making and problem-solving process (Davenport et al., 2018). Evidence is now emerging that frontline healthcare staff are highly attuned to macro and microsystem problems, and are thus uniquely qualified to address small operational failures, thereby reducing errors and near misses in clinical practice settings (Stevens et al., 2017).
Towards the future, methods for engaging a diverse group of stakeholders at all levels of the healthcare system must be better quantified and tested in empirical research (Wensing and Grol, 2019). Frontline staff is a group that typically has many demands on their time. One potential solution is to expand the use of researchers embedded within health systems (Cheetham et al., 2018; Gould et al., 2020; Robinson et al., 2017). Nurse researchers, with our expertise in clinical care delivery and knowledge of improvement science, are uniquely positioned to fulfill this role (Carter et al., 2020). One important advantage of embedded nurse researchers is the enhanced capacity for relationship building and establishing collaborations with all stakeholders (Vindrola-Padros et al., 2017); both are critical elements for leading successful quality improvement and implementation efforts.
Capacity building
The scientific infrastructure for research on how to improve healthcare has developed significantly over the past two decades (Davis and D’Lima, 2020). Major funders, including the National Institute for Health Research in the UK, the National Institutes of Health in the USA, have provided substantial funding. Scientific journals dedicated to this field, including BMJ Quality and Safety and Implementation Science have emerged, and there is a variety of annual scientific conferences focused on health improvement and IS, including those organised by the Society for Implementation Research Collaboration (SIRC). International standards for reporting implementation studies (StaRI) have been developed (Pinnock et al., 2017). There are also many training opportunities in quality improvement and IS, including those offered by the NIH (Boehm et al., 2020). These resources can enhance the capacity of nurse researchers to lead translational research teams focused on implementing best evidence in practice and improving healthcare quality.
Conclusion
To foster the translation of new research findings, close gaps in care quality and safety, and optimise health outcomes, we must strengthen the integration of QI efforts and IS methods (theories, strategies and outcomes). To date, many efforts in QI have been siloed, not fully leveraging IS theory and methods. QI programmes are well positioned to identify gaps in quality and safety, and to generate ideas for implementation studies. At the same time, IS incorporates a focus on success factors (facilitators or enablers) to enact and sustain practice change and offers tools to characterise the proximal and distal effects of practice change on a wide range of outcomes. QI and IS represent synergistic approaches to achieve continuous improvements in quality and safety in healthcare settings. Together they provide the intelligent direction for improvement science, complementing intention, effort and skillful execution.
Biography
Richard Ricciardi is a Professor and Director of Strategic Partnerships for the Center for Health Policy and Media Engagement at the George Washington University School of Nursing.
References
- Abbasgholizadeh Rahimi S, Menear M, Robitaille H, et al. (2017) Are mobile health applications useful for supporting shared decision making in diagnostic and treatment decisions? Global Health Action 10: 1332259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allen P, Pilar M, Walsh-Bailey C, et al. (2020) Quantitative measures of health policy implementation determinants and outcomes: a systematic review. Implementation Science 15: 47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Batsis JA, DiMilia PR, Seo LM, et al. (2019) Effectiveness of ambulatory telemedicine care in older adults: a systematic review. Journal of the American Geriatrics Society 67: 1737–1749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bauer MS, Damschroder L, Hagedorn H, et al. (2015) An introduction to implementation science for the non-specialist. BMC Psychology 3: 32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bauer MS, Kirchner J. (2020) Implementation science: what is it and why should I care? Psychiatry Research 283: 112376. [DOI] [PubMed] [Google Scholar]
- Birken SA, Haines ER, Hwang S, et al. (2020) Advancing understanding and identifying strategies for sustaining evidence-based practices: a review of reviews. Implementation Science 15: 88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boehm LM, Stolldorf DP, Jeffery AD. (2020) Implementation science training and resources for nurses and nurse scientists. Journal of Nursing Scholarship: An official publication of Sigma Theta Tau International Honor Society of Nursing 52: 47–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowen S, Erickson T, Martens PJ, et al. (2009) More than “using research”: the real challenges in promoting evidence-informed decision-making. Healthcare Policy 4: 87–102. [PMC free article] [PubMed] [Google Scholar]
- Brown A, Barnes C, Byaruhanga J, et al. (2020) Effectiveness of technology-enabled knowledge translation strategies in improving the use of research in public health: systematic review. Journal of Medical Internet Research 22: e17274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Busse R, Klazinga N, Panteli D, et al. (2019) Improving Healthcare Quality in Europe: Characteristics, Effectiveness and Implementation of Different Strategies, Copenhagen: European Observatory on Health Systems and Policies. [PubMed] [Google Scholar]
- Carter EJ, Hessels A, Cato K, et al. (2020) Evaluation of the joint nurse scientist role across academia and practice. Nursing Outlook 68: 261–269. [DOI] [PubMed] [Google Scholar]
- Chapman E, Haby MM, Toma TS, et al. (2020) Knowledge translation strategies for dissemination with a focus on healthcare recipients: an overview of systematic reviews. Implementation Science 15: 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Check DK, Zullig LL, Davis MM, et al. (2020) Improvement science and implementation science in cancer care: identifying areas of synergy and opportunities for further integration. Journal of General Internal Medicine. DOI: 10.1007/s11606-020-06138-w. Epub ahead of print 31 Aug 2020. PMID: 32869193. [DOI] [PMC free article] [PubMed]
- Cheetham M, Wiseman A, Khazaeli B, et al. (2018) Embedded research: a promising way to create evidence-informed impact in public health? Journal of Public Health (Oxford) 40: i64–i70. [DOI] [PubMed] [Google Scholar]
- Cochrane BS, Hagins M, Jr, Picciano G, et al. (2017) High reliability in healthcare: creating the culture and mindset for patient safety. Healthcare Management Forum 30: 61–68. [DOI] [PubMed] [Google Scholar]
- Davenport PB, Carter KF, Echternach JM, et al. (2018) Integrating high-reliability principles to transform access and throughput by creating a centralized operations center. The Journal of Nursing Administration 48: 93–99. [DOI] [PubMed] [Google Scholar]
- Davis R, D’Lima D. (2020) Building capacity in dissemination and implementation science: a systematic review of the academic literature on teaching and training initiatives. Implementation Science 15: 97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eccles MP, Mittman BS. (2006) Welcome to implementation science. Implementation Science 1: 1. [Google Scholar]
- Ellen ME, Léon G, Bouchard G, et al. (2014) Barriers, facilitators and views about next steps to implementing supports for evidence-informed decision-making in health systems: a qualitative study. Implementation Science 9: 179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodman D, Ogrinc G, Davies L, et al. (2016) Explanation and elaboration of the SQUIRE (Standards for Quality Improvement Reporting Excellence) guidelines, V.2.0: examples of SQUIRE elements in the healthcare improvement literature. BMJ Quality & Safety 25: e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gould MK, Sharp AL, Nguyen HQ, et al. (2020) Embedded research in the learning healthcare system: ongoing challenges and recommendations for researchers, clinicians, and health system leaders. Journal of General Internal Medicine 35: 3675–3680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granger BB. (2018) Science of improvement versus science of implementation: integrating both into clinical inquiry. AACN Advanced Critical Care 29: 208–212. [DOI] [PubMed] [Google Scholar]
- Grimshaw JM, Eccles MP, Lavis JN, et al. (2012) Knowledge translation of research findings. Implementation Science 7(50): 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton AB, Finley EP. (2019) Qualitative methods in implementation research: an introduction. Psychiatry Research 280: 112516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanefeld J, Powell-Jackson T, Balabanova D. (2017) Understanding and measuring quality of care: dealing with complexity. Bulletin of the World Health Organization 95: 368–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrison MI and Shortell SM. (2020) Multi-level analysis of the learning health system: integrating contributions from research on organizations and implementation. Learning Health Systems e10226. [DOI] [PMC free article] [PubMed]
- Institute of Medicine (2001) Crossing the Quality Chasm: A New Health System for the 21st Century, Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Khadjesari Z, Boufkhed S, Vitoratou S, et al. (2020) Implementation outcome instruments for use in physical healthcare settings: a systematic review. Implementation Science 15: 66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwan JL, Lo L, Ferguson J, et al. (2020) Computerised clinical decision support systems and absolute improvements in care: meta-analysis of controlled clinical trials. BMJ (Clinical Research ed.) 370: m3216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lasinski AM, Ladha P, Ho VP. (2021) Provision of Defect-free care: implementation science in surgical patient safety. Surgical Clinics of North America 101: 81–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leppin AL, Mahoney JE, Stevens KR, et al. (2019) Situating dissemination and implementation sciences within and across the translational research spectrum. Journal of Clinical Translational Science 4: 152–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis CC, Fischer S, Weiner BJ, et al. (2015) Outcomes for implementation science: an enhanced systematic review of instruments using evidence-based rating criteria. Implementation Science 10: 155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Llorens-Vernet P, Miró J. (2020) Standards for mobile health-related apps: systematic review and development of a guide. JMIR Mhealth Uhealth 8: e13057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu L, Zhang J, Xie Y, et al. (2020) Wearable health devices in health care: narrative systematic review. JMIR Mhealth Uhealth 8: e18907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKay D, Kirkham R, Freeman N, et al. (2020) Improving systems of care during and after a pregnancy complicated by hyperglycaemia: a protocol for a complex health systems intervention. BMC Health Services Research 20: 814–x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell SA, Fisher CA, Hastings CE, et al. (2010) A thematic analysis of theoretical models for translational science in nursing: mapping the field. Nursing Outlook 58: 287–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moullin JC, Dickson KS, Stadnick NA, et al. (2020) Ten recommendations for using implementation frameworks in research and practice. Implementation Science Community 1: 42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nilsen P. (2015) Making sense of implementation theories, models and frameworks. Implementation Science 10: 53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Obro LF, Heiselberg K, Krogh PG, et al. (2020) Combining mHealth and health-coaching for improving self-management in chronic care. A scoping review. Patient Education and Counseling. S0738-3991(20)30563-2. DOI: 10.1016/j.pec.2020.10.026. Epub ahead of print 21 Oct 2020. PMID: 33143907. [DOI] [PubMed]
- Pinnock H, Barwick M, Carpenter CR, et al. (2017) Standards for reporting implementation studies (StaRI): explanation and elaboration document. BMJ Open 7: e013318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Proctor E, Silmere H, Raghavan R, et al. (2011) Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Administration in Policy and Mental Health 38: 65–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rapport F, Clay-Williams R, Churruca K, et al. (2018) The struggle of translating science into action: foundational concepts of implementation science. Journal of Evaluation in Clinical Practice 24: 117–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson TE, Janssen A, Harnett P, et al. (2017) Embedding continuous quality improvement processes in multidisciplinary teams in cancer care: exploring the boundaries between quality and implementation science. Australian Health Review 41: 291–296. [DOI] [PubMed] [Google Scholar]
- Russ CM, Stone S, Treseler J, et al. (2020) Quality improvement incorporating a feedback loop for accurate medication reconciliation. Pediatrics. Epub ahead of print November 2019. 146: e20192464. DOI: 20192410.20191542/peds.20192019-20192464. [DOI] [PubMed]
- Stevens KR, Engh EP, Tubbs-Cooley H, et al. (2017) Operational failures detected by frontline acute care nurses. Research in Nursing & Health 40: 197–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Villalobos Dintrans P, Bossert TJ, Sherry J, et al. (2019) A synthesis of implementation science frameworks and application to global health gaps. Global Health Research Policy 4: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vindrola-Padros C, Pape T, Utley M, et al. (2017) The role of embedded research in quality improvement: a narrative review. BMJ Quality & Safety 26: 70–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wensing M, Grol R. (2019) Knowledge translation in health: how implementation science could contribute more. BMC Medicine 17: 88. [DOI] [PMC free article] [PubMed] [Google Scholar]