

Abstract
Introduction:
Amyotrophic lateral sclerosis (ALS) is a disease with high morbidity and mortality that adversely affects the activities of daily living. Disease progression in ALS is characterized by loss of function in bulbar, motor, and respiratory parameters. The revised amyotrophic lateral sclerosis functional rating scale (ALSFRS-R), which consists of 12 criteria, is used to determine disease effects on each of these functions. While each criterion is equally important when calculating the total ALSFRS-R score, the importance levels of the 12 criteria may vary in clinical practice. In this classical approach, the relationships among the parameters are not considered and the effects of bulbar, spinal, and respiratory dysfunctions on a patient’s activities of daily living may be different.
Methods:
In this study, we aimed to evaluate ALS cases with the ALSFRS-R fuzzy method. Although each subheading in the ALSFRS-R had the same score, the disease score was determined by the fuzzy ALSFRS-R method, based on whether a subheading had priority in management of the disease. While creating the functional rating scale ALSFRS-R approach, fuzzy ALSFRS-R score values were obtained by creating fuzzy models for each main group and integrating the fuzzy model results of each main group into a separate model.
Results:
In total, 50 patients with definite ALS according to the El Escorial criteria (33 men [66%] and 17 women [34%]; mean age, 58.49±10.01 years) were included in the study. When ALSFRS-R results and fuzzy ALSFRS-R results were compared, the prioritization order of 45 patients increased using the fuzzy ALSFRS-R score, while the prioritization order of five patients remained the same in both evaluations.
Conclusion:
The approach obtained by using fuzzy membership functions and decision rules, formed in accordance with expert opinion, was applied to the data of 50 patients from a large-scale hospital. In total, 90% of the patients had increased prioritization when using the fuzzy ALSFRS-R scoring method. Our results showed that the fuzzy approach provided more accurate information regarding a patient’s condition.
Keywords: Amyotrophic lateral sclerosis, functional rating scale, fuzzy
INTRODUCTION
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease with high morbidity and mortality, which adversely affects the activities of daily living. Disease progression in ALS involves bulbar, motor, and respiratory parameters. Neurological examinations or a number of clinical scales are used to demonstrate progressive deterioration in overall clinical presentation during patient follow-up. These methods include the revised amyotrophic lateral sclerosis functional rating scale (ALSFRS-R) (Appendix), which consists of questions that can be understood by the patient and can be easily applied to the patient (1, 2). In addition, the scale has been adapted for patients and caregivers to provide information by telephone administration, internet, and self-administration (3). The scale has been translated into various languages; the translated versions have been assessed for validity and reliability (4–8). The Turkish validation of ALSFRS-R was performed by Koç et al. (7).
Appendix.
ALSFRS-R Scale
| Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS) | |||
|---|---|---|---|
| The evaluated finding | Score | The evaluated finding | Score |
| 1- Speech | 7- Turning in bed | ||
| Normal speech processes | 4 | Normal | 4 |
| Detectable speech disturbance | 3 | Somewhat slow and clumsy, but no help needed | 3 |
| Intelligible with repeating | 2 | Can turn alone or adjust sheets, but with great difficulty | 2 |
| Speech combined with nonvocal communication | 1 | Can initiate, but not turn or adjust sheets alone | 1 |
| Loss of useful speech | 0 | Helpless | 0 |
| 2- Salivation | 8- Walking | ||
| Normal | 4 | Normal | 4 |
| Slight but definite excess of saliva in mouth; may have nighttime drooling | 3 | Early ambulation difficulties | 3 |
| Moderately excessive saliva; may have minimal drooling | 2 | Walks with assistance | 2 |
| Marked excess of saliva with some drooling | 1 | Non-ambulatory functional movement only | 1 |
| Marked drooling requires constant tissue or handkerchief | 0 | No purposeful leg movement | 0 |
| 3- Swallowing | 9- Climbing stairs | ||
| Normal | 4 | Normal | 4 |
| Early eating problems, occasional choking | 3 | Slow | 3 |
| Dietary consistency changes | 2 | Mild unsteadiness or fatigue | 2 |
| Needs supplemental tube feeding | 1 | Needs assistance | 1 |
| Exclusively parenteral or enteral feeding | 0 | Cannot do | 0 |
| 4- Handwriting | 10- Dyspnea | ||
| Normal | 4 | None | 4 |
| Slow or sloppy; all words are legible | 3 | Occurs when walking | 3 |
| Not all words are legible | 2 | Occurs with one or more of the following: eating, bathing, dressing | 2 |
| Able to grip pen but unable to write | 1 | Occurs at rest, difficulty in breathing when either sitting or lying | 1 |
| Unable to grip pen | 0 | Significant difficulty, considering using mechanical respiratory support | 0 |
| 5A- Cutting food without gastrostomy | 11- Orthopnea | ||
| Normal | 4 | None | 4 |
| Somewhat slow and clumsy, but no help needed | 3 | Some difficulty in sleeping at night due to shortness of breath. Does not routinely use more than two pillows | 3 |
| Can cut most foods, although clumsy and slow; some help needed | 2 | Needs extra pillow in order to sleep (more than 2) | 2 |
| Food must be cut by someone but can still feed slowly | 1 | Can only sleep sitting up | 1 |
| Needs to be fed | 0 | Unable to sleep | 0 |
| 5B- Cutting food with gastrostomy | 12- Respiratory insufficiency | ||
| Normal | 4 | None | 4 |
| Clumsy but able to perform all manipulations independently | 3 | Intermittent use of BiPAP | 3 |
| Some help needed with closures and fasteners | 2 | Continuous use of BiPAP during the night | 2 |
| Provides minimal assistance to caregiver | 1 | Continuous use of BiPAP during the night and day | 1 |
| Unable to perform any aspect of task | 0 | Invasive mechanical ventilation by intubation or tracheostomy | 0 |
| 6- Dressing and hygiene | Total Score | …/48 | |
| Normal | 4 | ||
| Independent and complete self-care with effort or decreased efficiency | 3 | ||
| Intermittent assistance or substitute methods | 2 | ||
| Needs attendant for self-care | 1 | ||
| Total dependence | 0 | ||
The ALSFRS-R scoring system is a frequently used scale consisting of 12 sub-parameters that assess the functional status of patients during the follow-up period. Each parameter has a score of 0–4. An ALSFRS-R score of 0 indicates the worst functional status and a score of 48 indicates the best functional status (1, 2). Life-threatening respiratory insufficiency and non-life-threatening factors that affect the quality of life (e.g., pencil holding, climbing stairs, and salivating) are evaluated with similarly weighted scores. This means that a patient with a higher score on the ALSFRS-R may have a worse status or better status than that represented by their numerical value. Therefore, other methods are needed to evaluate the actual clinical presentation by appropriate weighting of life-threatening factors (9). Rooney, discussed this issue in their article entitled, “Does ALSFRS-R measure the patient’s current picture?”, and stated that the ALSFRS-R score does not fully reflect the severity and course of the disease (9). Although the classical ALSFRS-R scoring system is widely used, it has the following limitations:
Highlights
In daily practice, ALSFRS-R is a Turkish validated scale used to evaluate the functional status of patients with amyotrophic lateral sclerosis. Parameters consisting of 12 main headings in this scale are collected numerically, but in this classical approach, the relations of these parameters with each other are not taken into account.
In the classical evaluation, the uncertainties between the parameters are ignored.
Although the effects of each parameter on the patient’s activities of daily living and prognosis are different, they have the same score weight.
From this point of view, it is aimed to evaluate the ALSFRS-R scale with fuzzy logic method, to reveal the constraints and to develop the scale in line with the data obtained. This method was used for the first time in the literature for the evaluation of ALSFRS-R.
The same ALSFRS-R score can be obtained with different combinations of the 12 parameters included in the scoring. Functional differences between patients with different combinations and the same ALSFRS-R score are neglected in the numerical representation.
It is accepted that the 12 parameters contribute to the activities of daily living of patients at the same level. However, in practice, the approach and priority order with the same score may be different between physicians performing research on the subject and those following patients in the clinic.
In clinical practice, 12 parameters in the ALSFRS-R are collected numerically. Relationships among these parameters are not considered in the classical approach. In the classical assessment, uncertainties between parameters are ignored.
Therefore, the present study aimed to present the current status of patients more accurately by using fuzzy logic (9). Fuzzy logic was introduced by Lutfi Ali Askerzade (1921), who was also known as Zadeh (1990) (10). This method has been successfully used in various disciplines in the health sector and in many other sectors. The most important step in patient treatment is determining the correct diagnosis. This stage of complex clinical decision-making is often accompanied by a degree of uncertainty, which is a challenge for both physician and patient; fuzzy logic is one of the methods to reduce this uncertainty. There are only two important studies in the literature using fuzzy logic in neurodegenerative diseases, such as Huntington’s disease, Parkinson’s disease, and ALS. These studies aimed to analyze the walking disorder observed in patients with neurodegenerative disease by using fuzzy logic, to develop a new gait scale and to predict prognosis (11–15).
THE APPROACH DEVELOPED IN THE STUDY
The developed approach consists of the following steps.
Calculation of ALSFRS-R Scores of Patients
In the first step of the study, ALSFRS-R scores of patients were calculated using the classical scoring system. In the classical evaluation, the scores obtained by the patient from each sub-parameter of the scale are aggregated and the patient’s score value is obtained.
Establishment of a Fuzzy-ALSFRS-R Scoring System
The 12 parameters in the ALSFRS-R scoring system can be classified into three main headings (bulbar, spinal, and respiratory), as shown in Figure 1 (2). In the classical scoring system, the functional status of the patients is evaluated according to the total score obtained from ANNEX-1 and no classification is used. In this study, considering the effects of bulbar, spinal, and respiratory dysfunctions on the activities of daily living of the patients, ALSFRS-R components were considered using the classification shown in Figure 1 (2).
Figure 1.
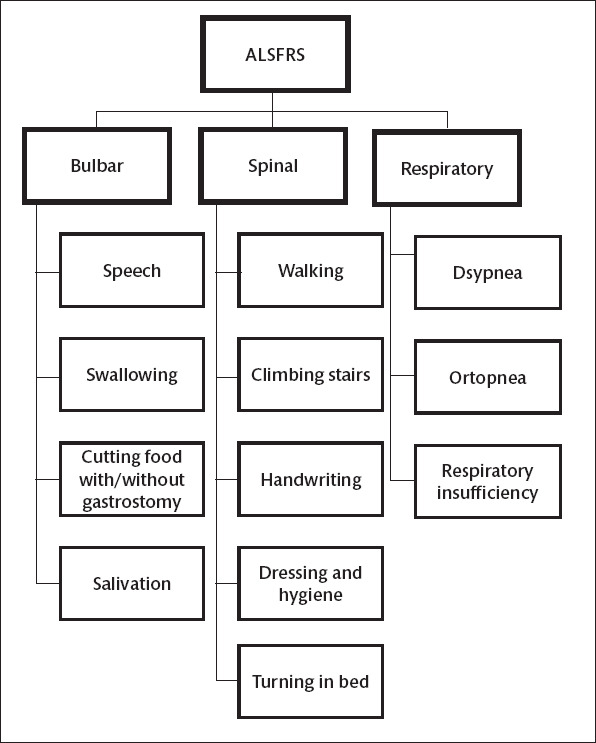
ALSFRS-R classification (2).
Although each subheading in ALSFRS-R has the same score, the disease score can be determined by the fuzzy ALSFRS-R method based on whether it has priority in the management of the disease. When creating the fuzzy ALSFRS-R approach, individual fuzzy models can be created for each main group. The fuzzy ALSFRS-R score value can then be obtained by integrating the fuzzy model results of each main group into a separate model. In our study, a fuzzy ALSFRS-R scale was constructed based on the classical ALSFRS-R scale and was coded using the Fuzzy Logic Designer Tool in Matlab 16a. The models created by the fuzzy ALSFRS-R approach are described below.
Creating a fuzzy model of bulbar functions
Speech, swallowing, feeding (with or without gastrostomy), and salivating are the parameters that reflect bulbar function. These parameters are taken as input and bulbar function values are taken as an output; the decision rules are formed accordingly. Considering that each item in the ALSFRS-R score ranges from 0 to 4, the minimum and maximum scores of these four parameters vary from 0 to 16. The bulbar function fuzzy logic design developed in this study is shown in Figure 2a, including the inputs and single output. As shown in Figure 2a, the “Mamdani min max” method was used.
Figure 2.

a–d. Design of bulbar (a), spinal (b), respiratory (c) and fuzzy ALSFRS-R (d) function fuzzy logic.
The input parameters that are considered when constructing the fuzzy bulbar approach consist of three levels and the single output parameter consists of five levels. Table 1 shows the membership functions determined for the input and output parameters, based on expert opinion. The triangular, smf, and zmf membership functions were used; the membership functions prepared for input and output are provided in Figures 3 and 4, respectively.
Table 1.
Bulbar, spinal and respiratory membership function values
| Parameter | Assessment | Fuzzy number | |
|---|---|---|---|
| Bulber | |||
| Input | Speech Swallowing Cutting food with or without gastrostomy Salivation |
Good Medium Poor |
Smf (2, 4) Tria (1, 2, 3) Zmf (0, 2) |
| Output | --Bulbar Value | Excellent Good Medium Poor Very Poor |
Smf (12, 16) Tria (9, 12, 15) Tria (6, 9, 12) Tria (3, 6, 9) Zmf (0, 6) |
| Spinal | |||
| Input | Walking Climbing stairs Handwriting Dressing and hygiene Turning in bed |
Good Medium Poor |
Smf (2, 4) Tria (1, 2, 3) Zmf (0, 2) |
| Output | Spinal Value | Excellent Good Medium Poor Very Poor |
Smf (12, 20) Tria (9, 12, 15) Tria (6, 9, 12) Tria (3, 6, 9) Zmf (0, 6) |
| Respiratory | |||
| Input | Dyspnea Orthopnea Respiratory insufficiency |
Good Medium Poor |
Smf (2, 4) Tria (1, 2, 3) Zmf (0, 2) |
| Output | Respiratory Values | Excellent Good Medium Poor Very Poor |
Zmf (0, 2) Smf (8, 12) Tria (6, 8, 10) Tria (2, 4, 6) Zmf (0, 4) |
Figure 3.
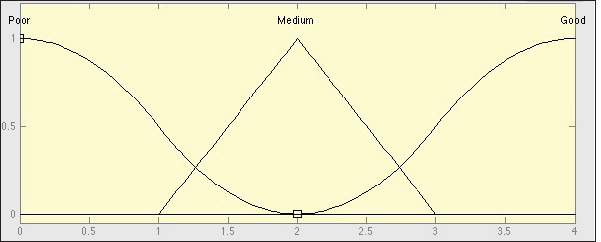
Membership function plots of input variables.
Figure 4.
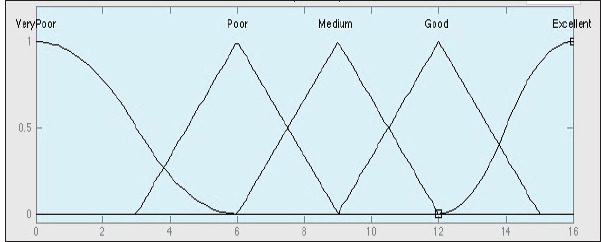
Membership function plots of bulbar output function.
Creating a fuzzy model of spinal functions
Handwriting, self-care and dressing, walking, climbing stairs and turning in bed and covering are parameters that reflect spinal function. These parameters are taken as input and spinal function values are taken as an output; the decision rules are formed accordingly. Considering that in the ALSFRS-R score ranges from 0 to 4, the minimum and maximum scores of these five parameters vary from 0 to 20. The spinal function fuzzy logic design developed in this study is shown in Figure 2b, including the inputs and single output. As shown in Figure 2b the “Mamdani min max” method was used.
The fuzzy spinal approach, input parameters consist of 3 levels and the output parameters consists of 5 levels. Table 1 shows the triangular, smf and zmf membership functions determined for the input and output parameters according to expert opinion.
Creating a fuzzy model of respiratory functions
Respiratory complaints are the most important parameters affecting mortality and consist of three parameters: dyspnea, orthopnea and respiratory failure. These parameters are taken as input and respiratory function values are taken as an output; the decision rules are formed accordingly. Considering that each item in the ALSFRS-R score ranges from 0 to 4, the minimum and maximum scores of these three parameters vary from 0 to 12. The respiratory function fuzzy logic design developed in this study is shown in Figure 2 c, including the inputs and single output. As shown in Figure 2 c, the “Mamdani min-max” method was used.
The input parameters that are considered when constructing the fuzzy respiratory approach consist of three levels and the single output parameter consists of five levels. Table 1 shows the triangular, smf, and zmf membership functions determined for the input and output parameters, based on expert opinion.
Forming the ALSFRS-R scale fuzzy model
Output parameters obtained by fuzzy models in bulbar, spinal, and respiratory functions are taken as input in the Fuzzy ALSFRS-R scale; the total score obtained from the ALSFRS-R scale is taken as an output. The ALSFRS-R function fuzzy design developed in this study is shown in Figure 2 d, including the inputs and single output. As shown in Figure 2 d, the “Mamdani min max” method was used.
The bulbar, spinal, and respiratory fuzzy models are used as input parameters; thus, membership functions consist of five levels (Table 1). The membership function of the ALSFRS-R score value, which is the output parameter, consists of five levels based on expert opinion (Table 2). Classical ALSFRS-R values were considered when determining membership function values, based on expert opinion.
Table 2.
ALSFRS-R membership function values
| Assessment | Fuzzy Number |
|---|---|
| Excellent | Smf (32, 48) |
| Good | Tria (20, 30, 40) |
| Medium | Tria (15, 20, 30) |
| Poor | Tria (7, 10, 20) |
| Very poor | Zmf (0, 10) |
RESULTS
Data Collection
Our study was conducted in Çukurova University Medical Faculty (8 September 2017; meeting 68, decision 22) after being approved by our ethics committee. All steps performed in our study were coherent with Declaration of Helsinki. Between September 2017 and April 2019, 50 patients with definite ALS diagnosis according to El-Escorial diagnostic criteria were included in this study (33 men [66%] and 17 women [34%]; mean age, 58.49±10.01 years); this number excluded patients with unclear diagnosis and those whose files were missing data. The age range was not determined to allow randomization during patient selection. Sex, age, age of onset, and duration of illness of the patients are shown in Table 3.
Table 3.
Patients’ demographic characteristics
| Sex | Age, year | Age of onset, year | Duration of disease until the study date, year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Min | Avg | Max | SD | Min | Avg | Max | SD | Min | Avg | Max | SD | |
| Female | 38 | 59.83 | 76 | 11.17 | 33 | 58.06 | 74 | 11.46 | 1 | 3.06 | 7 | 1.30 |
| Male | 37 | 57.70 | 76 | 9.43 | 35 | 54.64 | 74 | 9.60 | 1 | 3.18 | 12 | 2.02 |
| Total | 37 | 58.45 | 76 | 10.02 | 33 | 55.84 | 74 | 10.31 | 1 | 3.14 | 12 | 1.79 |
Min, minimum; Max, maximum; Avg, average; SD, standard deviation.
Calculation of ALSFRS-R Scores of Patients
The total values of the scores of the 50 patients included in the ALSFRS-R scale from each parameter forming the ALSFRS-R scale are listed in Table 4. Scoring was performed by a neurologist who was responsible for the neuromuscular outpatient clinic and who had 20 years of experience in treatment of ALS patients.
Table 4.
ALSFRS-R scores of patients
| Bulbar | Spinal | Respiratory | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Speech | Swallowing | Cutting food with/without gastrostomy | Salivation | Walking | Climbing stairs | Handwriting | Turning in bed | Dressing and hygiene | Dyspnea | Orthopnea | Respiratory insufficiency | Total Score | ||
| 5a | 5b | |||||||||||||
| 1 | 4 | 4 | 4 | 0 | 4 | 3 | 2 | 4 | 3 | 4 | 4 | 4 | 4 | 44 |
| 2 | 4 | 3 | 4 | 0 | 4 | 3 | 2 | 4 | 3 | 3 | 4 | 4 | 4 | 43 |
| 3 | 3 | 4 | 4 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 4 | 4 | 4 | 40 |
| 4 | 4 | 4 | 4 | 0 | 4 | 3 | 2 | 4 | 3 | 3 | 4 | 4 | 4 | 44 |
| 5 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| 6 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| 7 | 4 | 4 | 4 | 0 | 3 | 3 | 4 | 3 | 3 | 3 | 3 | 4 | 4 | 42 |
| 8 | 3 | 3 | 3 | 0 | 3 | 0 | 0 | 2 | 2 | 2 | 1 | 3 | 4 | 30 |
| 9 | 3 | 3 | 3 | 0 | 3 | 3 | 2 | 2 | 3 | 3 | 3 | 4 | 4 | 36 |
| 10 | 1 | 2 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 2 | 3 | 4 | 18 |
| 11 | 1 | 3 | 3 | 0 | 2 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 3 | 34 |
| 12 | 3 | 3 | 4 | 0 | 3 | 2 | 0 | 1 | 1 | 0 | 3 | 4 | 4 | 28 |
| 13 | 0 | 1 | 0 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 2 | 3 | 4 | 19 |
| 14 | 3 | 3 | 4 | 0 | 3 | 2 | 2 | 3 | 3 | 3 | 3 | 4 | 4 | 37 |
| 15 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 4 |
| 16 | 4 | 4 | 4 | 0 | 3 | 3 | 2 | 3 | 3 | 3 | 3 | 4 | 4 | 40 |
| 17 | 1 | 1 | 1 | 0 | 2 | 1 | 0 | 1 | 1 | 0 | 2 | 2 | 3 | 15 |
| 18 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | 2 | 1 | 1 | 1 | 2 | 3 | 19 |
| 19 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 2 | 8 |
| 20 | 2 | 1 | 3 | 0 | 3 | 2 | 0 | 3 | 2 | 2 | 1 | 2 | 3 | 21 |
| 21 | 4 | 3 | 4 | 0 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 3 | 4 | 38 |
| 22 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 2 | 3 | 11 |
| 23 | 3 | 3 | 3 | 0 | 3 | 4 | 4 | 3 | 3 | 3 | 2 | 3 | 4 | 38 |
| 24 | 4 | 4 | 4 | 0 | 4 | 3 | 2 | 4 | 4 | 4 | 4 | 4 | 4 | 46 |
| 25 | 4 | 3 | 3 | 0 | 4 | 4 | 4 | 2 | 4 | 4 | 4 | 4 | 4 | 45 |
| 26 | 2 | 2 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 2 | 3 | 4 | 16 |
| 27 | 3 | 3 | 3 | 0 | 4 | 3 | 4 | 1 | 3 | 3 | 3 | 4 | 4 | 38 |
| 28 | 2 | 3 | 2 | 0 | 2 | 4 | 4 | 2 | 4 | 4 | 2 | 3 | 4 | 36 |
| 29 | 4 | 4 | 4 | 0 | 4 | 3 | 2 | 4 | 4 | 4 | 4 | 4 | 4 | 46 |
| 30 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 2 | 6 |
| 31 | 3 | 3 | 4 | 0 | 3 | 3 | 2 | 4 | 4 | 4 | 2 | 4 | 4 | 39 |
| 32 | 2 | 2 | 2 | 0 | 3 | 3 | 3 | 2 | 4 | 4 | 4 | 4 | 4 | 39 |
| 33 | 3 | 3 | 4 | 0 | 3 | 3 | 3 | 2 | 4 | 3 | 3 | 4 | 4 | 39 |
| 34 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| 35 | 2 | 2 | 3 | 0 | 3 | 4 | 3 | 3 | 3 | 3 | 2 | 3 | 3 | 36 |
| 36 | 2 | 2 | 0 | 0 | 2 | 2 | 0 | 0 | 2 | 1 | 2 | 3 | 4 | 20 |
| 37 | 2 | 2 | 4 | 0 | 1 | 4 | 4 | 4 | 4 | 3 | 2 | 4 | 4 | 38 |
| 38 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 1 | 2 | 3 | 9 |
| 39 | 4 | 4 | 4 | 0 | 4 | 3 | 2 | 4 | 4 | 4 | 4 | 4 | 4 | 45 |
| 40 | 2 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 1 | 0 | 3 | 4 | 4 | 25 |
| 41 | 2 | 2 | 1 | 0 | 2 | 4 | 4 | 2 | 4 | 2 | 4 | 4 | 4 | 35 |
| 42 | 3 | 3 | 4 | 0 | 4 | 4 | 3 | 4 | 4 | 4 | 3 | 4 | 4 | 44 |
| 43 | 4 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 |
| 44 | 3 | 3 | 0 | 0 | 4 | 2 | 0 | 0 | 0 | 0 | 2 | 4 | 4 | 22 |
| 45 | 0 | 2 | 1 | 0 | 2 | 2 | 0 | 3 | 0 | 0 | 3 | 3 | 4 | 20 |
| 46 | 2 | 2 | 2 | 0 | 2 | 1 | 0 | 2 | 1 | 1 | 2 | 3 | 4 | 22 |
| 47 | 2 | 2 | 3 | 0 | 1 | 3 | 2 | 3 | 3 | 3 | 2 | 3 | 3 | 31 |
| 48 | 4 | 3 | 4 | 0 | 4 | 3 | 3 | 4 | 3 | 2 | 3 | 3 | 4 | 40 |
| 49 | 1 | 0 | 0 | 0 | 2 | 1 | 0 | 2 | 1 | 2 | 1 | 2 | 0 | 12 |
| 50 | 3 | 3 | 3 | 0 | 4 | 4 | 2 | 4 | 4 | 3 | 4 | 4 | 4 | 42 |
One of the most important problems in the management of the disease is the development of feeding complications due to swallowing difficulty. Because nutrition positively affects the quality and duration of the patient’s life, gastrostomy is performed in patients with swallowing difficulties. In this study, patients were evaluated based on their spinal, bulbar, and respiratory parameters, as well as their nutritional status (i. e., whether a feeding tube was inserted into the stomach). The ALSFRS-R scores of the 50 patients are shown in Table 4.
Table 4 shows that more than one patient has the same ALSFRS-R score, but these scores are achieved based on different combinations of parameters. Indeed, patients 13 and 18 had ALSFRS-R scores of 19; patients 31, 32, 33, and 34 had ALSFRS-R scores of 38. Achieving the same ALSFRS-R score with different combinations of parameters may discount the significance of the parameters and lead to insufficient treatment of a patient with a more critical health status. In this study, the fuzzy ALSFRS-R approach was applied based on the effects of the parameters with different weights on the ALSFRS-R scores.
Application of Fuzzy-ALSFRS-R Scoring System
The results of the fuzzy ALSFRS-R approach developed for the 50 patients included in the study are shown in Table 5. These results for each patient were based on membership functions obtained from the fuzzy bulbar, fuzzy spinal, and fuzzy respiratory models.
Table 5.
Fuzzy ALSFRS-R assessment results and comparison with Classical ALSFRS-R
| Patient no | Fuzzy Bulbar | Fuzzy Spinal | Fuzzy Respiratory | Fuzzy ALSFRS-R | Classical ALSFRS-R | Patient No | Fuzzy Bulbar | Fuzzy Spinal | Fuzzy Respiratory | Fuzzy ALSFRS-R | Classical ALSFRS-R | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Score | Rank | Score | Rank | Score | Rank | Score | Rank | ||||||||
| 1 | 14.90 | 12 | 10.9 | 43.30 | 23 | 44 | 29 | 26 | 5.07 | 1.69 | 8 | 12.50 | 4 | 16 | 10 |
| 2 | 14.40 | 12.8 | 10.9 | 43.00 | 20 | 43 | 28 | 27 | 13.50 | 12 | 10.7 | 42.60 | 16 | 38 | 24 |
| 3 | 14.10 | 17.3 | 10.9 | 42.70 | 17 | 40 | 26 | 28 | 8.70 | 17.7 | 8 | 29.40 | 12 | 36 | 22 |
| 4 | 14.90 | 12.8 | 10.9 | 43.10 | 21 | 44 | 29 | 29 | 14.90 | 12 | 10.9 | 43.30 | 23 | 46 | 31 |
| 5 | 1.72 | 1.69 | 1.13 | 2.91 | 1 | 2 | 1 | 30 | 1.70 | 1.69 | 6 | 12.40 | 3 | 6 | 4 |
| 6 | 1.72 | 1.69 | 1.13 | 2.91 | 1 | 2 | 1 | 31 | 13.30 | 12 | 8 | 30.00 | 14 | 39 | 25 |
| 7 | 14.90 | 17.3 | 10.7 | 43.20 | 22 | 42 | 27 | 32 | 5.07 | 17.3 | 10.9 | 29.70 | 13 | 39 | 25 |
| 8 | 13.30 | 9 | 6 | 28.50 | 11 | 30 | 18 | 33 | 13.30 | 16.7 | 10.7 | 42.80 | 19 | 39 | 25 |
| 9 | 13.30 | 16.7 | 10.7 | 42.80 | 18 | 36 | 22 | 34 | 1.72 | 1.69 | 1.13 | 2.91 | 1 | 2 | 1 |
| 10 | 2.30 | 1.96 | 8 | 12.50 | 4 | 18 | 11 | 35 | 8.21 | 17.3 | 8 | 28.40 | 10 | 36 | 22 |
| 11 | 6.00 | 17.3 | 8 | 21.70 | 8 | 34 | 20 | 36 | 5.07 | 5.94 | 8 | 21.80 | 9 | 20 | 13 |
| 12 | 13.30 | 2.81 | 10.7 | 12.60 | 5 | 28 | 17 | 37 | 5.07 | 17.3 | 8 | 21.80 | 9 | 38 | 24 |
| 13 | 6.00 | 6 | 8 | 21.70 | 8 | 19 | 12 | 38 | 1.72 | 2.01 | 6 | 12.40 | 3 | 9 | 6 |
| 14 | 13.30 | 17.3 | 10.7 | 42.80 | 19 | 37 | 23 | 39 | 14.90 | 12 | 10.9 | 43.30 | 23 | 45 | 30 |
| 15 | 1.70 | 1.69 | 4 | 12.40 | 3 | 4 | 3 | 40 | 5.07 | 2.81 | 10.7 | 12.60 | 5 | 25 | 16 |
| 16 | 14.90 | 12.8 | 10.7 | 43.10 | 21 | 40 | 26 | 41 | 5.07 | 12 | 10.9 | 29.70 | 13 | 35 | 21 |
| 17 | 1.72 | 2.01 | 8 | 12.40 | 3 | 15 | 9 | 42 | 14.00 | 17.3 | 10.7 | 42.60 | 16 | 44 | 29 |
| 18 | 5.07 | 2.01 | 6 | 12.50 | 4 | 19 | 12 | 43 | 8.00 | 1.69 | 1.13 | 3.10 | 2 | 3 | 2 |
| 19 | 1.71 | 1.69 | 6 | 12.40 | 3 | 8 | 5 | 44 | 7.50 | 2.81 | 8 | 12.70 | 6 | 22 | 15 |
| 20 | 3.48 | 9 | 6 | 16.30 | 7 | 21 | 14 | 45 | 2.30 | 10 | 10.7 | 21.80 | 9 | 20 | 13 |
| 21 | 13.90 | 17.3 | 8 | 42.50 | 15 | 38 | 24 | 46 | 5.07 | 2.01 | 8 | 12.50 | 4 | 22 | 15 |
| 22 | 1.70 | 2.01 | 6 | 12.40 | 3 | 11 | 7 | 47 | 5.07 | 12.8 | 8 | 21.80 | 9 | 31 | 19 |
| 23 | 13.30 | 17.3 | 8 | 42.80 | 19 | 38 | 24 | 48 | 14.40 | 17.3 | 10.7 | 43.00 | 20 | 40 | 26 |
| 24 | 14.90 | 12 | 10.9 | 43.30 | 23 | 46 | 31 | 49 | 1.72 | 10 | 6 | 12.50 | 4 | 12 | 8 |
| 25 | 14.40 | 17.7 | 10.9 | 43.00 | 20 | 45 | 30 | 50 | 13.50 | 12.8 | 10.9 | 42.60 | 16 | 42 | 27 |
Application of ALSFRS-R Fuzzy Method
Comparison of classical ALSFRS-R results (Table 4) and fuzzy ALSFRS-R results is shown in Table 5. Based on ALSFRS-R values, the priority rankings of 45 patients increased, while the priority rankings of five patients remained identical between evaluations. When Table 5 was reviewed, it was determined that the classical ALSFRS-R and fuzzy ALSFRS-R scores of some patients (patients 5, 6, 34 etc.) were similar, because all of them obtained the same scores from each parameter. On the other hand, it was noticed that some patients (patients 13 and 18, patient 44 and 46, patients 9.28 and 35 etc.) had lower fuzzy ALSFRS-R scores even though classical ALSFRS-R scores were similar Table 5). This is due to the fact that the effects of bulbar and/or respiratory parameters are more prominent in cases with low fuzzy ALSFRS-R scores.
ALSFRS-R is a physician-approved tool for assessing coarse and fine motor function, bulbar symptoms, and respiratory involvement in patients with ALS (1). Importantly, the scale has some limitations in evaluating the patient’s clinical condition.
The scale only reflects the patient’s actual status in the later stages of the disease. It may have lower sensitivity in determining disease severity based on the affected area (16, 17). The score of a patient is based on the examination findings of the physician, as well as the explanations by the patient and their caregivers. The patient’s clinical condition may sometimes be exaggerated by patients and caregivers, or may be minimized to show their resilience against disease and to appear stronger for their relatives (1). In some studies, because of the patient’s limited movement, the scale is completed based on information received by telephone. In this case, physician observation is excluded from the assessment. The scale was developed mainly to evaluate the results of pharmaceutical clinical research.
Equal weighting of each parameter during scoring and disregard for the importance of particular factors relating to the health status of a patient is problematic when prioritizing patient treatment. For example, respiratory failure, writing, swallowing, and climbing stairs are weighted equally. This may cause insufficient assessment of the severity of the disease level and result in delayed treatment of urgent conditions. Therefore, the inappropriate weighting of parameters that are not significantly correlated is the greatest limitation of the scale; our findings support this perspective.
Table 6.
Classic ALSFRS-R and Fuzzy ALSFRS comparison
| Patient No | Classic ALSFRS-R | Fuzzy ALSFRS-R | Patient No | Classic ALSFRS-R | Fuzzy ALSFRS-R | ||||
|---|---|---|---|---|---|---|---|---|---|
| Score | Rank | Score | Rank | Score | Rank | Score | Rank | ||
| 1 | 44 | 29 | 43.30 | 23 | 26 | 16 | 10 | 12.50 | 4 |
| 2 | 43 | 28 | 43.00 | 20 | 27 | 38 | 24 | 42.60 | 16 |
| 3 | 40 | 26 | 42.70 | 17 | 28 | 36 | 22 | 29.40 | 12 |
| 4 | 44 | 29 | 43.10 | 21 | 29 | 46 | 31 | 43.30 | 23 |
| 5 | 2 | 1 | 2.91 | 1 | 30 | 6 | 4 | 12.40 | 3 |
| 6 | 2 | 1 | 2.91 | 1 | 31 | 39 | 25 | 30.00 | 14 |
| 7 | 42 | 27 | 43.20 | 22 | 32 | 39 | 25 | 29.70 | 13 |
| 8 | 30 | 18 | 28.50 | 11 | 33 | 39 | 25 | 42.80 | 19 |
| 9 | 36 | 22 | 42.80 | 18 | 34 | 2 | 1 | 2.91 | 1 |
| 10 | 18 | 11 | 12.50 | 4 | 35 | 36 | 22 | 28.40 | 10 |
| 11 | 34 | 20 | 21.70 | 8 | 36 | 20 | 13 | 21.80 | 9 |
| 12 | 28 | 17 | 12.60 | 5 | 37 | 38 | 24 | 21.80 | 9 |
| 13 | 19 | 12 | 21.70 | 8 | 38 | 9 | 6 | 12.40 | 3 |
| 14 | 37 | 23 | 42.80 | 19 | 39 | 45 | 30 | 43.30 | 23 |
| 15 | 4 | 3 | 12.40 | 3 | 40 | 25 | 16 | 12.60 | 5 |
| 16 | 40 | 26 | 43.10 | 21 | 41 | 35 | 21 | 29.70 | 13 |
| 17 | 15 | 9 | 12.40 | 3 | 42 | 44 | 29 | 42.60 | 16 |
| 18 | 19 | 12 | 12.50 | 4 | 43 | 3 | 2 | 3.10 | 2 |
| 19 | 8 | 5 | 12.40 | 3 | 44 | 22 | 15 | 12.70 | 6 |
| 20 | 21 | 14 | 16.30 | 7 | 45 | 20 | 13 | 21.80 | 9 |
| 21 | 38 | 24 | 42.50 | 15 | 46 | 22 | 15 | 12.50 | 4 |
| 22 | 11 | 7 | 12.40 | 3 | 47 | 31 | 19 | 21.80 | 9 |
| 23 | 38 | 24 | 42.80 | 19 | 48 | 40 | 26 | 43.00 | 20 |
| 24 | 46 | 31 | 43.30 | 23 | 49 | 12 | 8 | 12.50 | 4 |
| 25 | 45 | 30 | 43.00 | 20 | 50 | 42 | 27 | 42.60 | 16 |
In this study, a fuzzy ALSFRS-R scoring approach was developed based on the parameters used in the classical ALSFRS-R scoring system. The resulting approach, obtained through fuzzy membership functions and decision rules developed on the basis of expert opinion, was applied to the data of 50 patients from a large-scale hospital. These assessments showed that the fuzzy ALSFRS-R scoring approach provided more accurate information about a patient’s condition.
Limited budget, personnel, and material problems are encountered in hospitals. For ALSFRS-R patients, the effectiveness of scarce resources can be improved by correctly determining the patient’s importance ranking.
CONCLUSION
Interface software can be created for fuzzy rules developed in future studies. Fuzzy ALSFRS-R evaluation results can be demonstrated and the actions that should be taken, based on results according to ALSFRS-R scores, can be determined by physicians using the interface software.
Footnotes
Ethics Committee Approval: Our study was conducted in Çukurova University Medical Faculty (8 September 2017; meeting 68, decision 22) after being approved by our ethics committee.
Informed Consent: Written informed consent forms were obtained from the legalguardians of all cases.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept- GGÇ, AK, CD; Design- FK; Supervision- GGK; Resource- FK; Materials- GGK; Data Collection and/or Processing- GGK; Analysis and/or Interpretation- GGK, AK, CD, FK; Literature Search- GGK; Writing- GGK, CD, FK, AK; Critical Reviews- FK, AK.
Conflict of Interest: The authors declare that there is no conflict of interest.
Financial Disclosure: No funding.
REFERENCES
- 1.The ALS CNTF treatment study (ACTS) phase I-II Study Group. The Amyotrophic Lateral Sclerosis Functional Rating Scale. Assessment of activities of daily living in patients with amyotrophic lateral sclerosis. Arch Neurol. 1996;53:141–147. https: //jamanetwork.com/journals/jamaneurology/article-abstract/593848 . [PubMed] [Google Scholar]
- 2.Cedarbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, Nakanishi A BDNF ALS Study Group (Phase III) The ALSFRS-R. a revised ALS functional rating scale that incorporates assessments of respiratory function. J Neurol Sci. 1999;169:13–21. doi: 10.1016/s0022-510x(99)00210-5. [DOI] [PubMed] [Google Scholar]
- 3.Bakker LA, Schröder CD, van Es MA. Assessment of the factorial validity and reliability of the ALSFRS-R. a revision of its measurement model. J Neurol. 2017;264:1413–1420. doi: 10.1007/s00415-017-8538-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abdulla S, Vielhaber S, Körner S, Machts J, Heinze HJ, Dengler R, Petri S. Validation of the German version of the extended ALS functional rating scale as a patient-reported outcome measure. J Neurol. 2013;260:2242–55. doi: 10.1007/s00415-013-6955-6. [DOI] [PubMed] [Google Scholar]
- 5.Campos TS, Rodríguez-Santos F, Esteban J, Vázquez PC, Mora Pardina JS, Carmona AC. Spanish adaptation of the revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R) Amyotroph Lateral Scler. 2010;11:475–477. doi: 10.3109/17482968.2010.489115. [DOI] [PubMed] [Google Scholar]
- 6.Guedes K, Pereira C, Pavan K, Valério BC. Cross-cultural adaptation and validation of ALS functional rating scale-revised in Portuguese language. Arq Neuropsiquiatr. 2010;68:44–47. doi: 10.1590/s0004-282x2010000100010. [DOI] [PubMed] [Google Scholar]
- 7.Koç F, Balal M, Demir T, Alparslan ZN, Sarica Y. Adaptation to Turkish and reliability study of the revised Amyotrophic Lateral Sclerosis Functional Rating Scale (ALSFRS-R) Arch Neuropsychiatr. 2016;53:229–233. doi: 10.5152/npa.2016.11334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ohashi Y, Tashiro K, Itoyama Y, Nakano I, Sobue G, Nakamura S, Sumino S, Yanagisawa N. Study of functional rating scale for amyotrophic lateral sclerosis: revised ALSFRS (ALSFRS-R) Japanese version. No To Shinkei. 2001;53:346–355. https: //pubmed.ncbi.nlm.nih.gov/11360474/ [PubMed] [Google Scholar]
- 9.Rooney J, Burke T, Vajda A, Heverin M, Hardiman O. What does the ALSFRS-R really measure?A longitudinal and survival analysis of functional dimension subscores in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2017;88:381–385. doi: 10.1136/jnnp-2016-314661. [DOI] [PubMed] [Google Scholar]
- 10.Zadeh LA. The birth and evolution of fuzzy logic. Int J Gen Syst. 1990;17:95–105. [Google Scholar]
- 11.Aziz W, Arif M. Complexity analysis of stride interval time series by threshold dependent symbolic entropy. Eur J Appl Physiol. 2006;98:30–40. doi: 10.1007/s00421-006-0226-5. [DOI] [PubMed] [Google Scholar]
- 12.Klomsae A, Auephanwiriyakul S, Theera-Umpon N. String grammar unsupervised possibilistic fuzzy c-medians for gait pattern classification in patients with neurodegenerative diseases. Comput Intell Neurosci. 2018;1869565 doi: 10.1155/2018/1869565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wu Y, Krishnan S. Computer-aided analysis of gait rhythm fluctuations in amyotrophic lateral sclerosis. Med Biol Eng Comput. 2009;47:1165–1171. doi: 10.1007/s11517-009-0527-z. [DOI] [PubMed] [Google Scholar]
- 14.Ye Q, Xia Y, Yao Z. Classification of gait patterns in patients with neurodegenerative disease using adaptive neuro-fuzzy inference system. Comput Math Methods Med. 2018;2018:9831252. doi: 10.1155/2018/9831252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pham TD. Texture classification and visualization of time series of gait dynamics in patients with neuro-degenerative diseases. IEEE Trans Neural Syst Rehabil Eng. 2018;26:188–196. doi: 10.1109/TNSRE.2017.2732448. [DOI] [PubMed] [Google Scholar]
- 16.Voustianiouk A, Seidel G, Panchal J, Sivak M, Czaplinski A, Yen A, Appel SH, Lange DJ. ALSFRS and Appel ALS scores: discordance with disease progression. Muscle Nerve. 2008;37:668–772. doi: 10.1002/mus.20977. [DOI] [PubMed] [Google Scholar]
- 17.Wicks P, Massagli MP, Wolf C, Heywood J. Measuring function in advanced ALS. validation of ALSFRS-EX extension items. Eur J Neurol. 2009;16:353–359. doi: 10.1111/j.1468-1331.2008.02434.x. [DOI] [PubMed] [Google Scholar]