

Abstract
Introduction:
Patients with bipolar disorder have motor skill deficiency and cognitive dysfunction. It is suggested that these deficiencies are related to the neurodevelopmental course of the disease. The aim of this study was to examine whether or not there was a change in the handwriting of patients with bipolar disorder in periods of mania and remission.
Method:
Two samples of handwriting and signature were taken from the cases, one on admission before treatment and one just after discharge. The first sample was taken in the period when the patients hospitalised with manic episode before medications and the second sample was taken in remission when the decision for discharge was made. The handwriting changes betwen the manic episode and the remission period were examined.
Results:
In the examination of the handwriting between the two periods, there was an increase in the size of the writing, pen pressure, the length of words, the spaces between words, and missing and incorrect punctuation marks in the manic episode. There were no differences in any handwriting measure on function of the specific diagnosis or the antipsychotic dose but tremor count was higher in patients using antipsychotics (p<0.05). Most of the parameters showing a change were found to be related to the Young Mania Rating Scale (YMRS) scores.
Conclusion:
The results of this study determined severe changes in the handwriting of patients with bipolar disorder in a period of mania. Handwriting features can be used to screen patients for discharge and can be used for prediction when a patient might switch into manic episode. Also intake YMRS scores were found as the most important feature that affect handwriting parameters in manic patients.
Keywords: Handwriting, mania, bipolar affective disorder
INTRODUCTION
The action of writing is a process undertaken by several regions of the brain working together. Writing requires the collaboration of attention, memory, imagination, verbal thought, speaking and reading centres. In addition to these brain activities, the muscle and bone structures must be co-ordinated (1, 2). The motor cortex, which provides the primary motor activity of the brain, the supplementary motor area (SMA), and the writing and talking centres of the Wernicke and Broca areas are important centres playing a role in this process. The activities of writing occur through transmission to the hands of signals emerging from the motor cortex (3). If there is any brain damage or functional impairment for any reason in these areas, serious changes may be seen in the handwriting. In addition, previous studies have shown that neurochemical factors (serotonin, dopamine etc) and basal ganglion dysfunction that have a role in the pathogenesis of psychiatric (depression, schizophrenia) and neurological diseases (Parkinson’s disease) are effective in the changes in handwriting (2).
Bipolar Disorder (BD) is a severe psychiatric disease characterised by periods of mania, depression and remission. In the manic episode, the mood is excessively elevated. In this period, the patient has exaggerated thoughts and engages in exciting and dangerous projects and tasks (4). These activities lead to unwanted results. The patient may find themselves in the forensic process in this period because of excessive spending, taking out loans or signing cheques or promissory notes (5, 6). Many studies have shown that patients with bipolar disorder have motor skill deficiency and cognitive dysfunction. It is suggesting that these deficiencies are related to the neurodevelopmental course of the disease and related with increased extrapyramidal symptoms (7). Lohr and Caligiuri reported that patients with bipolar disorder performed worse on some measures of motor function [force steadiness and velocity scaling] than healthy participants (8). Also motor abnormalities can occur in these patients that can cause handwriting changes.
Highlights
There are changes in handwriting in bipolar disorder.
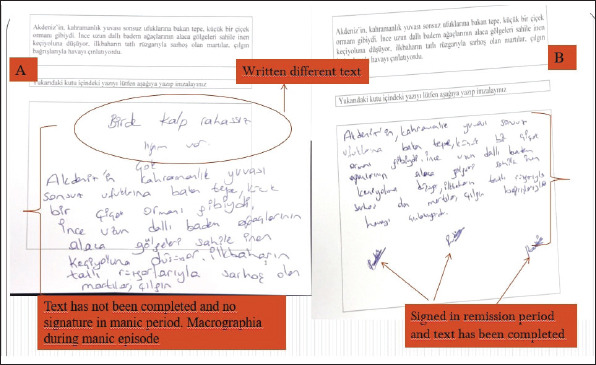
Macrographia has been detected during the manic episode.
Handwriting features can be used as a screening tool for remission in bipolar disoder.
Handwriting can be used for prediction of a switch into mania.
We thought that when these patients’ motor skills and cognitive functions were impaired, there would be serious changes in the handwriting. And we aimed to investigate whether or not there was a change in the handwriting of patients with BD by comparing examples in the manic and euthymic periods, and if a significant change emerged, to find out whether “Handwriting changes can be used for monitoring and management of bipolar patients”.
METHODS
Case Selection
The cases to be evaluated in the study were selected from patients who presented at the Psychiatry Clinic of Inonu University Medical Faculty Turgut Özal Medical Centre between 1 June 2016 and 1 June 2017, and were diagnosed with a BD manic episode according to the DSM-V diagnostic criteria and hospitalised.
Approval for the study was granted by the Local Clinical Research Ethics Committee (decision no: 2016/104, dated: 11/05/2016).
The Young Mania Rating Scale (YMRS) was applied to all patients at both instances: at admission and after discharge. Two samples of handwriting and signature were taken from the cases, one on admission before treatment and one just after discharge. The first sample was taken in the period when the patients hospitalised with manic episode before medications and the second sample was taken when the decision for discharge was made and was evaluated as the remission period after treatment. The Extrapyramidal Symptom Rating Scale (ESRS) was applied to all patients to control for side effect of medication.
The cases selected were restricted to the age range of 18–56 years to ensure that the handwriting characteristic properties were fully developed and to prevent the effect of any age-related impairment in writing. Patients were pre-screened for neuro-psychiatric diseases and were excluded if they were illiterate, if they had any additional neuro-psychiatric disorder, or had any congenital or acquired disability that could affect the handwriting. Patients were also excluded if they were discharged early for any reason with only partial recovery, or if a second sample could not be obtained for reasons such as the patient’s refusal to provide a sample. The study included 36 cases only diagnosed with BAD manic episode.
Data Collection
A record was made for each of the cases in the study of age, gender, educational status, work and professional status, marital status, dominant hand, duration of disease, number of previous manic and total episode, family history, medications used and comorbidities. A standard text was prepared for the participants to copy as the handwriting sample: “Akdeniz’in, kahramanlık yuvası sonsuz ufuklarına bakan tepe, küçük bir çiçek ormanı gibiydi. İnce uzun dallı badem ağaçlarının alaca gölgeleri sahile inen keçiyoluna düşüyor, ilkbaharın tatlı rüzgarıyla sarhoş olan martılar, çılgın bağırışlarıyla havayı çınlatıyordu” (The hill overlooking the endless horizons of the heroic home of the Mediterranean was like a small flower forest. The dappled shadows of the slender and branched almond trees were falling on the path leading down to the beach, and the seagulls, intoxicated by the sweet breeze of spring, were ringing in the air with their wild cries). The participants were instructed to write the text in the space left below the printed version and then to sign the paper.
The text was printed on a standard HP Laserjet 1018 printer on A4 photocopy paper of 80 gr/m2 quality. The same physical conditions were provided for all the participants at the stage of writing the text. All were given a blue 1.0 ballpoint pen of the same series. A flat-surfaced table and a chair at a height at which the individual could comfortably write were provided in a well-lit room. Care was taken to avoid any physical, visual or auditory distractions while writing.
Determination of the Parameters To Be Examined
Some of the parameters to be examined in the writing, such as level of the lines, degree of pressure, space between words, the height of ascending and descending letters, spelling and punctuation mistakes, were determined by examining previous studies conducted in this area (9–12).
Evaluation of the Data
The data collected were scanned with a standard OKI MB451 multi-function colour scanner and transferred to a computer program in pdf format. Measurement of the data in the PDF format was made using the ruler function in the Adobe Acrobat Reader DC program (Figure 1). In the data examination, direct and oblique-angled light sources, a microscope, a magnifier and HS 525 document detector were used. Measurements of collected data were evaluated by three examiners who were blinded to clinical status.
Figure 1.
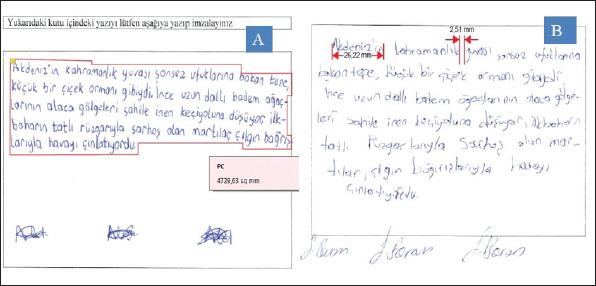
Measurement of some parameters; A: Area covered by the writing (mm2), B: Word length and space between words (mm).
Statistical Analysis
Statistical evaluations of the data obtained in the study were made using the Statistical Package for the Social Sciences (SPSS) for Windows v22.0 software. Quantitative variables were stated as mean ± standard deviation (SD), median, minimum and maximum values. Categorical variables were stated as number (n) and percentage (%). Handwriting scores of different examiners evaluated by using Friedman’s analysis of variance by rank and intraclass correlation coefficients were also calculated.
The quantitative data did not conform to normal distribution as determined by the Shapiro-Wilk test (p<0.05). Changes in the parameters between the mania and remission periods were evaluated with Pearson correlation analysis, the Pearson Chi square test, the Students’ t test, the Wilcoxon test and the McNemar test. A value of p<0.05 was accepted as statistically significant. Multiple linear regression analysis (with stepwise selection method) was used for determining significant factors related with YMRS scores.
RESULTS
A total of 36 cases were included in the study (Female 22, Male 14). Education level of 23 participants (% 63.9) were high school or lower. 32 participants (% 88.9) were right handed. All patients were taking different combinations of mood stabilizers, antipsychotics or benzodiazepines. We evaluated reliability of the handwriting scores for the three different examiners (Table 1). YMRS score means were 26.61±8.40 (minimum 7.0, maximum 46.0). It was determined that patients writing in the manic period took up more space, had more missing or incorrect punctuation marks and wrote more lines (Table 2) (Figure 2). More mistakes were made in the general rules of writing in the manic episode [slope of writing, inappropriate use of capital and lower letters (t (22)=2.837, p<0.05), writing outside the text (t (17)=2.773, p<0.05) and writing in more lines (t (12)=5.366, p<0.05)] (Figure 2, 3). As seen in Table 3, a statistically significant difference was determined in the length of words and the spaces between words.
Table 1.
Handwriting scores of different measurers and analysis results
| Mean | S. D. | ICC (95% CI) | p value | ||
|---|---|---|---|---|---|
| Area covered by the writing (mm2) (mania) | 1st measurer | 8203.21 | 2587.11 | 0.829 (0.703–0.907) | 0.017* |
| 2nd measurer | 9461.38 | 2350.60 | |||
| 3rd measurer | 8839.06 | 2318.91 | |||
| Area covered by the writing (mm2) (remission) | 1st measurer | 7335.61 | 2689.03 | 0.954 (0.919–0.975) | 0.264 |
| 2nd measurer | 7276.46 | 2885.36 | |||
| 3rd measurer | 7483.71 | 2492.65 | |||
| Akdeniz’in (mania) | 1st measurer | 30.47 | 5.78 | 0.908 (0.838–0.950) | 0.358 |
| 2nd measurer | 29.20 | 6.21 | |||
| 3rd measurer | 29.71 | 5.62 | |||
| Akdeniz’in (remission) | 1st measurer | 30.23 | 7.18 | 0.426 (0.001–0.688) | 0.779 |
| 2nd measurer | 29.59 | 6.93 | |||
| 3rd measurer | 29.35 | 7.87 | |||
| ağaçlarının (mania) | 1st measurer | 29.94 | 6.45 | 0.750 (0.558–0.867) | <0.001* |
| 2nd measurer | 29.35 | 6.36 | |||
| 3rd measurer | 28.95 | 6.36 | |||
| ağaçlarının (remission) | 1st measurer | 28.74 | 6.92 | 0.862 (0.760–0.925) | 0.590 |
| 2nd measurer | 27.36 | 5.30 | |||
| 3rd measurer | 27.82 | 5.68 | |||
| keçiyoluna (mania) | 1st measurer | 30.44 | 6.44 | 0.977 (0.959–0.988) | 0.529 |
| 2nd measurer | 30.35 | 6.45 | |||
| 3rd measurer | 30.17 | 6.27 | |||
| keçiyoluna (remission) | 1st measurer | 28.79 | 8.27 | 0.957 (0.926–0.977) | 0.205 |
| 2nd measurer | 28.62 | 7.85 | |||
| 3rd measurer | 27.85 | 7.97 | |||
| rüzgarıyla (mania) | 1st measurer | 30.85 | 6.95 | 0.946 (0.905–0.971) | 0.402 |
| 2nd measurer | 30.34 | 6.86 | |||
| 3rd measurer | 30.82 | 6.80 | |||
| rüzgarıyla (remission) | 1st measurer | 28.55 | 7.42 | 0.958 (0.926–0.977) | 0.155 |
| 2nd measurer | 28.38 | 5.86 | |||
| 3rd measurer | 27.55 | 6.64 | |||
| çınlatıyordu (mania) | 1st measurer | 35.08 | 6.55 | 0.914 (0.846–0.954) | 0.034* |
| 2nd measurer | 34.95 | 6.53 | |||
| 3rd measurer | 33.46 | 6.66 | |||
| çınlatıyordu (remission) | 1st measurer | 33.70 | 8.31 | 0.960 (0.930–0.978) | 0.174 |
| 2nd measurer | 33.91 | 7.63 | |||
| 3rd measurer | 32.86 | 8.23 | |||
| kahramanlık yuvası (mania) | 1st measurer | 4.82 | 2.06 | 0.836 (0.710–0.912) | 0.682 |
| 2nd measurer | 4.92 | 1.85 | |||
| 3rd measurer | 4.79 | 2.03 | |||
| kahramanlık yuvası (remission) | 1st measurer | 4.53 | 1.61 | 0.806 (0.663–0.895) | 0.590 |
| 2nd measurer | 4.55 | 1.57 | |||
| 3rd measurer | 4.62 | 1.69 | |||
| çiçek ormanı (mania) | 1st measurer | 5.59 | 3.60 | 0.902 (0.826–0.948) | 0.007* |
| 2nd measurer | 5.60 | 3.64 | |||
| 3rd measurer | 6.01 | 3.65 | |||
| çiçek ormanı (remission) | 1st measurer | 4.11 | 2.78 | 0.945 (0.903–0.970) | 0.814 |
| 2nd measurer | 4.13 | 2.65 | |||
| 3rd measurer | 4.43 | 2.86 | |||
| küçük “k” (mania) | 1st measurer | 4.94 | 1.23 | 0.955 (0.920–0.976) | 0.889 |
| 2nd measurer | 4.96 | 1.21 | |||
| 3rd measurer | 5.05 | 1.15 | |||
| küçük “k” (remission) | 1st measurer | 4.47 | 1.03 | 0.843 (0.725–0.916) | 0.124 |
| 2nd measurer | 4.51 | 0.95 | |||
| 3rd measurer | 4.35 | 1.03 |
p values were obtained by Friedman’s analysis of variance by ranks;
p<0.05.
ICC, intraclass correlation coefficient; CI, confidence interval; S. D., standard deviation; mm, milimeter.
Table 2.
Analysis of the form of the written text
| Mania | Remission | |||||
|---|---|---|---|---|---|---|
| Mean | S. D. | Mean | S. D. | p value | d | |
| Space left at the top (T) of the paper (mm) | 3.10 | 1.95 | 2.84 | 1.41 | 0.78 | 0.13 |
| Space left at the bottom (B) of the paper (mm) | 30.14 | 17.26 | 35.79 | 15.68 | 0.02* | 0.34 |
| Space left at the right side (R) of the paper (mm) | 5.78 | 6.13 | 4.17 | 4.52 | 0.27 | 0.29 |
| Space left at the left side (L) of the paper (mm) | 5.54 | 10.38 | 3.30 | 1.87 | 0.94 | 0.30 |
| Space between two lines (mm) | 4.30 | 1.14 | 4.11 | 1.42 | 0.23 | 0.14 |
| Area covered by the writing (mm2) | 8203.20 | 2587.10 | 7046.18 | 2898.96 | 0.01* | 0.42 |
| Number of lines in which the text was written | 7.0 | 1.38 | 6.0 | 0.85 | 0.0001* | 0.87 |
| Number of angularity | 2.65 | 2.42 | 1.95 | 1.25 | 0.005* | 0.36 |
| Tremor count | 4.54 | 4.96 | 2.36 | 2.18 | 0.003* | 0.56 |
| Number of tapered ends | 44.15 | 24.57 | 28.58 | 18.54 | 0.005* | 0.71 |
| Missing punctuation (number) | 1.89 | 0.73 | 0.92 | 1.25 | 0.01* | 0.94 |
| Incorrect punctuation (number) | 0.61 | 0.73 | 0.06 | 0.33 | 0.0001* | 0.97 |
p<0.05.
S. D., standard deviation; mm, millimeter; d, effect size (Cohen’s d).
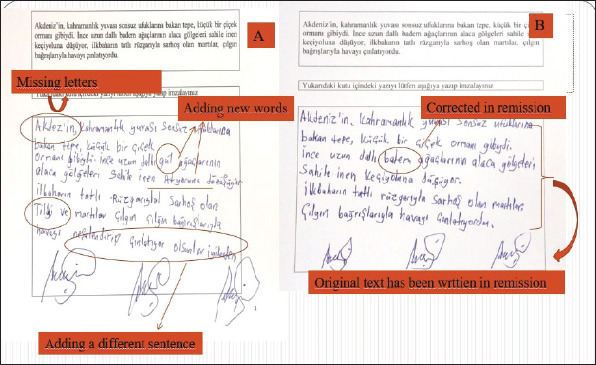
Figure 2.
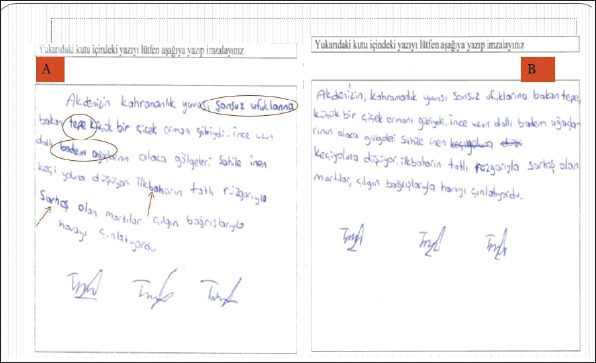
Handwriting of a thirty-year-old male; A: Handwriting in mania, there are many mistakes, B: In remission, original text has been written, and corrected mistakes (Irregularity in rhythm is significant, especially in character size during mania).
Figure 3.
Handwriting of a twenty-year-old female, showing differences between mania and remission; A: Manic period, B: Remission period. Enlargement of writing and decrease in writing quality are determined.
Table 3.
Measurements of word lengths and spaces between words
| Word length | Mania | Remission | ||||
|---|---|---|---|---|---|---|
| Mean | S. D. | Mean | S. D. | p value | d | |
| Akdeniz’in | 30.47 | 5.77 | 30.22 | 7.18 | 0.68 | 0.03 |
| ağaçlarının | 29.94 | 6.45 | 28.96 | 7.26 | 0.03* | 0.14 |
| keçiyoluna | 30.44 | 6.44 | 28.78 | 8.26 | 0.23 | 0.22 |
| rüzgarıyla | 30.85 | 6.94 | 28.54 | 7.42 | 0.03* | 0.32 |
| çınlatıyordu | 35.08 | 6.55 | 33.70 | 8.31 | 0.13 | 0.18 |
| Space between words | ||||||
| kahramanlık yuvası | 4.81 | 2.05 | 4.52 | 1.61 | 0.20 | 0.15 |
| çiçek ormanı | 7.17 | 9.98 | 4.10 | 2.78 | 0.03* | 0.41 |
| alaca gölgeleri | 6.54 | 3.15 | 5.89 | 3.15 | 0.15 | 0.26 |
| ilkbaharın tatlı | 5.33 | 6.04 | 4.96 | 1.96 | 0.49 | 0.08 |
| sahile inen | 5.04 | 1.65 | 4.64 | 2.32 | 0.01* | 0.19 |
p<0.05.
S. D., standard deviation; mm, millimeter; d, effect size (Cohen’s d).
A significant increase was determined in the manic episode in the width and height of the letters ‘n’ and ‘r’ located in the mid-zone and final zone (t (6)=5.052, p<0.05). In the examination of the capital letters, the letter ‘A’ was seen to be written larger in the manic episode (t (18)=3.531, p<0.05). Similarly, the size of ascending and descending letters was determined to be increased in the manic episode (Table 4). Repeated letters and the degree of pen pressure applied when writing were significantly higher in mania (p<0.05) (Figure 4, 5).
Table 4.
Measurement of ascending and descending letters
| Ascending Letters | Mania | Remission | ||||
|---|---|---|---|---|---|---|
| Mean | S. D. | Mean | S. D. | p value | d | |
| kahramanlık “h” | 4.95 | 1.10 | 4.40 | 1.28 | 0.0001* | 0.46 |
| dallı “d” | 4.86 | 1.08 | 4.61 | 1.05 | 0.09 | 0.23 |
| martılar “t” | 4.51 | 1.11 | 4.70 | 1.52 | 0.56 | 0.14 |
| ufuklarına “f” | 5.76 | 1.63 | 5.39 | 1.24 | 0.02* | 0.25 |
| küçük “k” | 4.94 | 1.22 | 4.46 | 1.02 | 0.0001* | 0.42 |
| Descending Letters | ||||||
| tepe “p” | 4.19 | 0.85 | 4.21 | 1.23 | 0.78 | |
| gibiydi “g” | 5.10 | 1.39 | 4.74 | 1.07 | 0.03* | |
| havayı “y” | 4.86 | 1.2 | 4.31 | 1.05 | 0.01* | |
p<0.05.
S. D., standard deviation; mm, millimeter; d, effect size (Cohen’s d).
Figure 4.
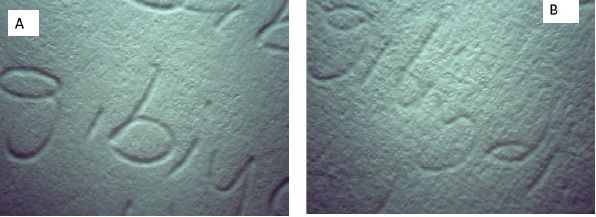
Pen pressure of handwriting evaluated with HS 525 document detector (30× magnified); A: pen pressure is much more during manic episode, B: pen pressure is less during remission.
Figure 5.
Samples of a 43-year-old housewife, shown overwritten words and letters in mania (A), overwritten words and letters are diminished in remission (B).
In order to research the effect of antipsychotics on handwriting features, patients were divided in two groups depending on whether they were taking or not antipsychotics. Students’ t test was performed and results are shown in Table 5. Number of tremor and “f” in “ufuklarına” were found significantly different. No significant differences between groups were observed in other handwriting features. To study the putative effect of antipsychotic dose on the handwriting variables, medication dose was classified as high or low, and t-tests were performed on each handwriting features. Categorization of treatments in high or low was based on clinical guidelines (13). No significant differences between groups were observed in none of the handwriting features.
Table 5.
Handwriting features and their mean values and standard deviations (between parenthesis) for each group (antipsychotics users vs. no antipsychotics)
| Features | Antipsychotics (n=24) | No Antipsychotics (n=12) | Student’s t |
|---|---|---|---|
| Area covered by the writing (mm2) | 8183.20 (2703.0) | 8243.30 (2452.9) | t <1 |
| Missing punctuation (number) | 2.16 (2.11) | 1.33 (2.10) | t=1.11, p=0.273 |
| ağaçlarının (mm) | 29.03 (6.18) | 31.58 (6.88) | t=-1.10, p=0.279 |
| rüzgarıyla (mm) | 30.30 (7.13) | 31.84 (6.78) | t <1 |
| kahramanlık “h” (mm) | 4.77 (1.06) | 5.26 (1.15) | t=-1.21, p=0.233 |
| ufuklarına “f” | 5.53 (1.39) | 6.51 (2.16) | t=-2.08, p=0.045* |
| Number of tremor | 4.80 (4.36) | 2.26 (2.12) | t=2.57, p=0.01* |
p<0.05
We performed multiple linear regression analysis with YMRS change scores as dependent variable. The variance inflation factor (VIF) was found less than ten, and residual terms showed homoscedasticity. We found that missing punctuation number change (p=0.015), education (p=0.038) and “çiçek ormanı” space between words change (p=0.004) were the most related factors with YMRS change scores by controlling gender effect (p=0.005) (Table 6). On the other hand, age (p=0.485) and medication (p=0.492) were not found as significant factors on YMRS change scores. The final model was; “YMRS Change Score=7.122+3.660* Gender+5.714 * Education+0.862* Missing punctuation (number) change+0.192* “çiçek ormanı” (Space between words) change”.
Table 6.
Significant related factors with the YMRS Scores. Multiple linear regression analysis
| Unstandardized β | Standard Error | Standardized β | t | p | 95.0% Confidence Interval for β | ||
|---|---|---|---|---|---|---|---|
| (Constant) | 7.122 | 0.771 | 9.234 | <0.001 | 5.547 | 8.697 | |
| Gender (Male) | 3.660 | 1.198 | 0.400 | 3.055 | 0.005 | 1.213 | 6.108 |
| Education | 5.714 | 2.581 | 0.385 | 2.214 | 0.038 | 2.791 | 4.325 |
| Missing punctuation (number) change | 0.862 | 0.334 | 0.328 | 2.582 | 0.015 | 0.180 | 1.544 |
| çiçek ormanı (Space between words) change | 0.192 | 0.062 | 0.408 | 3.087 | 0.004 | 0.065 | 0.318 |
Dependent variable: YMRS change score.
R2=0.549; F=12.160; p<0.001
DISCUSSION
The results of the current study demonstrated that the period of mania in bipolar disorder features objective measurable changes in handwriting. During handwriting process besides motor cortex, basal ganglia, extrapyramidal system and neurotransmitters take part. The basal ganglia, the subthalamic nucleus (STN), the substantia nigra pars compacta (SN), and thalamus play a key role in the maintenance and stabilization of voluntary movements, regulation of muscle tone, and integration of afferent information from the periphery (2). Basal ganglia dysfunction in patients with BD causes changes in handwriting due to involuntary movements. Neurotransmitters are released at nerve junctions and provide electrical impulses to pass from one neuron to another (3). Increasing or decreasing of these endogenous chemicals cause disrupted of transmission system (3, 8). Consequently, cognitive and motor functions of patients with BD are affected (1, 7).
The handwriting of the study participants was seen to be larger and occupy a larger space in the manic period. Micrography is observed in Parkinson’s disease and several authors accept micrography as an important finding in early diagnosis (14, 15). A reduced level of dopamine is known to have a role in the pathogenesis of Parkinson’s disease (16). While a reduced dopamine level leads to micrography (17), we suggest that the increased level of dopamine seen in mania could cause macrography.
When the handwriting samples were examined in general, the rate of starting new lines was determined to be low in the manic episode and high in the remission period. Furthermore, in the manic episode the writing exceeded the defined space and there were more missing or incorrect punctuation marks. In a similar study of schizophrenia patients by Kömür et al (12), more punctuation errors were made compared to the control group. Gawda (18) also stated that the dots on the letters ‘i’ and ‘j’ were missed more often by those with schizophrenia than by a control group. This can be considered to be due to concentration problems in manic episode (19).
In the current study, the slope of the writing was determined to be more irregular in the manic episode, with more regular handwriting seen during remission. There was also determined to be more incorrect use of capital and lower case letters in the manic period, as well as a greater rate of incorrect or missing letters. These findings are not specific to the manic episode of BD and can be seen in several neuro-psychiatric diseases (18, 20).
In a study by Aşicioglu and Turan (9) investigating the effects of alcohol on handwriting, a severe change was seen in the handwriting under the effect of alcohol, and it was determined that the writing and character size were increased, the slope of the writing deteriorated and there was irregular rhythm. Phillips and colleagues (21) reported that alcohol led to cerebellar dysfunction. There was seen to be motor slowing down with the effect of alcohol, writing was slower, pressure on the pen was reduced, tremor was increased and horizontal lines could not be maintained (21).
Similar findings were determined in a study of 87 patients with Parkinson’s disease (22). These changes seen in the handwriting were said to be related to basal ganglion strial dopamine levels and fine motor skills were impaired (22). In the current study, it was determined that in the manic period the size of the writing increased, the rate of writing was irregular and there were spelling and punctuation mistakes. This can be considered to be associated with basal ganglion dysfunction and fine motor skills impairment in the manic period (19).
Gawda (20) examined the change in handwriting in a study of psychiatric patients and investigated whether the findings were disease-specific. Similar results have been found in studies made according to personality characteristics and in patients with schizophrenia, depression and anti-social disorder. The results demonstrated that there was in increase in irregular writing forms, impaired letter forms, inability to maintain a horizontal line, slow writing speed and tremor. It has been reported that none of these findings are disease-specific (18, 20, 23). In patients with depression, which deteriorates mood, there has been reported to be less pen pressure in the handwriting (23). This finding can be evaluated as a slowing down of motor activity by reduced serotonin levels which play a role in the pathogenesis of depression, thereby leading to reduced pressure when writing. In the current study, the pen pressure in the handwriting was increased in the manic period. The dopamine level leading to the increase in expansive mood in mania can be considered to lead to the degree of pen pressure.
Another important finding of the current study was the changes seen in the letters in the mid-zone and at the end of words. The size of the letters in these sections and the length of words were increased. This is thought to be due to the inability to maintain attention and concentration during the manic episode. In addition, some patients in the manic episode wrote phrases that were not in the text and 3 patients had written a completely different text. This can be attributed to reduced cognitive functions, and flight of ideas in patients in this period (24, 25).
In addition, it was determined that in remission the patients made efforts to correct mistakes they had made when writing in the manic period. In particular, there was not seen to be any text written other than what was in the text in the remission period and there was a significant decrease in crossings out, the text exceeding the defined space, and spelling and punctuation mistakes. In a previous study in literature of patients with schizophrenia, there was a similar reduction in writing mistakes following treatment of the patients (12). These improvements can be considered to be associated with the correction of mood after treatment of these patients.
Psychotropic drugs may also alter handwriting features. Gerken and colleagues checked whether handwriting movement size (i. e, area encompassed by handwriting) could predict the treatment response in patients with schizophrenia (26). The researchers reported that treatment with antipsychotics resulted in a reduction in the overall size of the handwriting samples (defined as a 13% reduction in the overall size, or area, of 50% or more of the handwriting samples) in about one-third of the treatment responders. Nevertheless, most of the treatment non-responders also showed reduction in handwriting area, suggesting that handwriting may not be an effective predictor of treatment response. The authors concluded that handwriting parameters might be better suited for evaluating neurological side effects of neuroleptic medications rather than predicting treatment response using standard observer rating scales (26). In addition, these drugs can affect fine motor control of hand presented with parkinsonism and dyskinesia.
There are no patients without medications in our study. In clinical practice, it is difficult to find individuals with a severe mental disorder who are not under the effect of medication. We did not find significant differences between participants with low and high doses of antipsychotics in any of the handwriting features evaluated. These results are similar with other studies that detected motor abnormality in antipsychotic treatment (27, 28). On the other hand, another important finding in this study was that tremor was noticed in the handwriting of antipsychotic users without developing clinical side effects. This can help to notice motor side effects of antipsychotics in the early period. In the literature it has been reported that gender had also effect on handwriting (29, 30). Females had advantage in various handwriting tasks, including written composing and written fluency. In a current study, it was found that gender had an effect on handwriting.
There are some limitations in our study. In daily life, these patients use handwriting in commercial, judicial and official procedures. We also collected samples using pen and paper in our study, we thought it would be more appropriate to examine the handwriting and signatures on the document. Therefore, we did not use a digitizing tablet with appropriate software and did not examine the kinematic values features such as velocity, stroke and jerk. In addition, the limited time between the first examination and the second examination is another limitation of our study. This study was done according to the Turkish alphabet and our results may be a guide for languages that use the Latin alphabet, but it may be difficult to generalize to languages that differ in their grammatic structure and orthographic features. For this purpose, further studies are needed.
CONCLUSION
Writing is understood as a psycho-neuro-motor process affected by several factors. When one of these in the processes are affected, serious changes can occur in handwriting. As a result, in our study; inital YMRS scores were one of the most important factors affecting handwriting change parameters. Handwriting features can be used to screen patients for discharge and can be helpful for predicting when a patient with BD might switch into manic episode. Also we suggest that, handwriting can be used to detect the motor side effects of antipsychotics in the early period.
Footnotes
Ethics Committee Approval: Ethics Committee approval was obtained from the Faculty of Medicine Inonu University (decision no:2016/104, dated:11/05/2016).
Informed Consent: Written informed consent forms were obtained from the all participants.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept- NA, OC; Design- NA, OC, EPZ; Supervision- OC, RK, NA; Resource- RK, EPZ, BSÖ; Materials- NA, EPZ; Data Collection and/or Processing- NA, BSÖ, EPZ; Analysis and/or Interpretation- NA, ÖC, RK; Literature Search- NA, EPZ, BSÖ; Writing- NA, ÖC; Critical Reviews- ÖC, RK.
Conflict of Interest: No.
Financial Disclosure: The authors declared that this study has received no financial support
REFERENCES
- 1.Saudek R. Factors that cause changes in handwriting. In: Koppenhaver KM, editor. Forensic Document Examination Principles and Practice. Totowa: Humana Press Inc; 2007. pp. 27–36. [Google Scholar]
- 2.Caligiuri MP, Mohammed LA. The Neuroscience of Handwriting:Applications for Forensic Document Examination. Boca Raton: CRC Press; 2012. [Google Scholar]
- 3.Hall JE, Guyton AC. Textbook of medical physiology. 12th ed. Philadelphia, PA: Saunders Elsevier; 2011. https: //bujhansi.ac.in/econtent/pages/shortcodes/biomedical/Guyton-and-Hall-Textbook-of-Medical-Physiology-12th-Ed.pdf . [Google Scholar]
- 4.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Pub; 2013. (DSM-5®) https: //www.psychiatry.org/psychiatrists/practice/dsm . [Google Scholar]
- 5.Fovet T, Geoffroy PA, Vaiva G, Adins C, Thomas P, Amad A. Individuals with bipolar disorder and their relationship with the criminal justice system:a critical review. Psychiatric Serv. 2015;66:348–353. doi: 10.1176/appi.ps.201400104. [DOI] [PubMed] [Google Scholar]
- 6.Pondé MP, Caron J, Mendonça MS, Freire AC, Moreau N. The relationship between mental disorders and types of crime in inmates in a Brazilian prison. J Forensic Sci. 2014;59:1307–1314. doi: 10.1111/1556-4029.12462. [DOI] [PubMed] [Google Scholar]
- 7.Arango C, Fraguas D, Parellada M. Differential Neurodevelopmental Trajectories in patients with early-onset bipolar and schizophrenia disorders. Schizophr Bull. 2014;40(Suppl 2):S138–S146. doi: 10.1093/schbul/sbt198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lohr JB, Caligiuri MP. Abnormalities in motor physiology in bipolar disorder. J Neuropsychiatr. 2006;18:342–349. doi: 10.1176/jnp.2006.18.3.342. [DOI] [PubMed] [Google Scholar]
- 9.Aşıcıoğlu F, Turan N. Handwriting changes under the effect of alcohol. Forensic Sci Int. 2003;132:201–210. doi: 10.1016/s0379-0738(03)00020-3. [DOI] [PubMed] [Google Scholar]
- 10.Bancila VG. The forensic importance of handwriting pathology in major psychiatric disorders. Int J of Cri Invest. 2012;2:209–219. http: //docs.manupatra.in/newsline/articles/Upload/5A4494DF-64C5-4A2D-B833-D288E622DD60.pdf . [Google Scholar]
- 11.Mergl R, Juckel G, Rihl J, Henkel V, Karner M, Tigges P, et al. Kinematical analysis of handwriting movements in depressed patients. Acta Psychiatr Scand. 2004;109:383–391. doi: 10.1046/j.1600-0447.2003.00262.x. [DOI] [PubMed] [Google Scholar]
- 12.Kömür İ, Gürler AS, Başpınar B, Şahin E, Kantarcı MN, Emül M, et al. Differences in handwritings of schizophrenia patients and examination of the change after treatment. J Forensic Sci. 2015;60:1613–1619. doi: 10.1111/1556-4029.12858. [DOI] [PubMed] [Google Scholar]
- 13.Andreasen NC, Pressler M, Nopoulos P, Miller D, Ho B-C. Antipsychotic Dose Equivalents and Dose-years:A Standardized Method for Comparing Exposure to Different Drugs. Biol Psychiatry. 2010;67:255–262. doi: 10.1016/j.biopsych.2009.08.040. https: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Van Gemmert AWA, Adler CH, Stelmach GE. Parkinson's disease patients undershoot target size in handwriting and similar tasks. J Neurol Neurosurg Psychiatry. 2003;74:1502–1508. doi: 10.1136/jnnp.74.11.1502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Becker G, Müller A, Braune S, Büttner T, Benecke R, Greulich W, et al. Early diagnosis of Parkinson's disease. J Neurol. 2002;249(Suppl 3:III):40–48. doi: 10.1007/s00415-002-1309-9. [DOI] [PubMed] [Google Scholar]
- 16.McLennan JE, Nakano K, Tyler HR, Schwab RS. Micrographia in Parkinson's disease. J Neurol Sci. 1972;15:141–152. doi: 10.1016/0022-510x(72)90002-0. [DOI] [PubMed] [Google Scholar]
- 17.Muneer A. Mixed States in Bipolar Disorder:Etiology, Pathogenesis and Treatment. Chonnam Med J. 2017;53:1–13. doi: 10.4068/cmj.2017.53.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gawda B. Dysfluent Handwriting in Schizophrenic Outpatients. Percept Mot Skills. 2016;122:560–577. doi: 10.1177/0031512516637019. [DOI] [PubMed] [Google Scholar]
- 19.Dubovsky SL. Mania. Continuum. 2015;21:737–755. doi: 10.1212/01.CON.0000466663.28026.6f. [DOI] [PubMed] [Google Scholar]
- 20.Gawda B. Lack of evidence for the assessment of personality traits using handwriting analysis. Polish Psychol Bull. 2014;45:73–79. [Google Scholar]
- 21.Phillips JG, Ogeil RP, Müller F. Alcohol consumption and handwriting:A kinematic analysis. Hum Mov Sci. 2009;28:619–632. doi: 10.1016/j.humov.2009.01.006. [DOI] [PubMed] [Google Scholar]
- 22.Nackaerts E, Heremans E, Smits-Engelsman BCM, Broeder S, Vandenberghe W, Bergmans B, et al. Validity and reliability of a new tool to evaluate handwriting difficulties in Parkinson's disease. PLoS One. 2017;12:e0173157. doi: 10.1371/journal.pone.0173157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gawda B. Little Evidence for the graphical markers of depression. Percept Mot Skills. 2013;117:304–318. doi: 10.2466/03.10.pms.117x15z8. [DOI] [PubMed] [Google Scholar]
- 24.Harvey PD, Wingo AP, Burdick KE, Baldessarini RJ. Cognition and disability in bipolar disorder:lessons from schizophrenia research. Bipolar Disord. 2010;12:364–375. doi: 10.1111/j.1399-5618.2010.00831.x. [DOI] [PubMed] [Google Scholar]
- 25.Palmis S, Danna J, Velay J-L, Longcamp M. Motor control of handwriting in the developing brain:A review Motor control of handwriting in the developing brain:A review. Cogn Neuropsychol. 2017;34:187–204. doi: 10.1080/02643294.2017.1367654. https: [DOI] [PubMed] [Google Scholar]
- 26.Gerken A, Wetzel H, Benkert O. Extrapyramidal symptoms and their relationship to clinical efficacy under perphenazine treatment. A controlled prospective handwriting-test study in 22 acutely ill schizophrenic patients. Pharmacopsychiatry. 1991;24:132–137. doi: 10.1055/s-2007-1014456. [DOI] [PubMed] [Google Scholar]
- 27.Dean DJ, Teulings H-L, Caligiuri M, Mittal VA. Handwriting analysis indicates spontaneous dyskinesias in neuroleptic naïve adolescents at high risk for psychosis. J Vis Exp. 2013;81:e50852. doi: 10.3791/50852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Crespo Y, Ibañez A, Soriano MF, Iglesias S, Aznarte JI. Handwriting movements for assessment of motor symptoms in schizophrenia spectrum disorders and bipolar disorder. PLoS One. 2019;14:e0213657. doi: 10.1371/journal.pone.0213657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Reilly D, Neumann DL, Andrews G. Gender differences in reading and writing achievement:Evidence from the National Assessment of Educational Progress (NAEP) Am Psychol. 2019;74:445–458. doi: 10.1037/amp0000356. [DOI] [PubMed] [Google Scholar]
- 30.Reynolds MR, Scheiber C, Hajovsky DB, Schwartz B, Kaufman AS. Gender Differences in Academic Achievement:Is Writing an Exception to the Gender Similarities Hypothesis? J Genet Psychol. 2015;176:211–234. doi: 10.1080/00221325.2015.1036833. https: [DOI] [PubMed] [Google Scholar]