

Abstract
Intractable public health problems are influenced by interacting multi-level factors. Dynamic research approaches in which teams of scientists collaborate beyond traditional disciplinary, institutional, and geographic boundaries have emerged as promising strategies to address pressing public health priorities. However, little prior work has identified, defined, and characterized the outcomes of transdisciplinary (TD) research undertaken to address public health problems. Through a mixed methods approach, we identify, define, and characterize TD outcomes and their relevance to improving population health using the Transdisciplinary Research on Energetics and Cancer (TREC) II initiative as a case example. In Phase I, TREC II leadership (n = 10) identified nine initial TD outcomes. In Phase II (web-based survey; n = 23) and Phase III (interviews; n = 26; and focus groups, n = 23) TREC members defined and characterized each outcome. The resulting nine outcomes are described. The nine complementary TD outcomes can be used as a framework to evaluate progress toward impact on complex public health problems. Strategic investment in infrastructure that supports team development and collaboration, such as a coordination center, cross-center working groups, annual funded developmental projects, and face-to-face meetings, may foster achievement of these outcomes. This exploratory work provides a basis for the future investigation and development of quantitative measurement tools to assess the achievement of TD outcomes that are relevant to solving multifactorial public health problems.
Keywords: knowledge creation, transdisciplinary research evaluation, transdisciplinary outcomes, collaboration outcomes, team science
Introduction
Public health problems such as cancer, poor nutrition, cardiovascular disease, health disparities, and tobacco use have multifactorial causes and consequences that span interacting biological, behavioral, social, and environmental factors (Morgan et al., 2003; Warnecke et al., 2008; Lynch and Rebbeck, 2013; Adler et al., 2016). For example, in the USA, ~19% of cancer cases are attributable to high body mass index (Arnold et al., 2015). Observational studies have identified growth factor signaling pathways, inflammatory processes, adipose tissue hypoxia and insulin resistance, and shared genetic as biological mechanisms linking obesity and cancer (Basen-Engquist and Chang, 2011). Environmental and social factors, such as income inequality, neighbourhood designs that promote sedentary lifestyles and food systems that make energy dense, nutrient-poor foods inexpensive, and accessible fuel poor nutrition, limited physical activity, and subsequent poor health outcomes (Srinivasan et al., 2003; Swinburn et al., 2011). Despite significant progress over the last several decades, smoking continues to be the leading cause of preventable death worldwide (Centers for Disease Control and Prevention (CDC), 2009) and causes nearly half of all cancer deaths in the USA (Siegel et al., 2015). Biological mechanisms such as damage to DNA, inflammation, and oxidative stress from tobacco use cause a spectrum of adverse health outcomes (U.S. Department of Health and Human Services, 2010). Social and environmental factors such as advertising, cultural acceptability, peer influence, and public policies contribute to smoking behaviors (Morgan et al., 2003). Solutions that target only a single dimension of these intractable societal problems have not been sufficient for their resolution. For example, abundant evidence demonstrates that behavioral treatments that rely on individuals to make lifestyle changes but do not address contextual or biological factors do not result in sustained health improvements (Wooley and Garner, 1994; McTigue et al., 2003; Minian et al., 2020).
Transdisciplinary (TD) research approaches that break down disciplinary, institutional, and geographic barriers have emerged as promising strategies for addressing such problems (Rosenfield, 1992; Hiatt and Rimer, 1999; Turkkan et al., 2000; Pohl, 2008; Warnecke et al., 2008; Stokols et al., 2008b; McAneney et al., 2010; Hall et al., 2012b; Balsiger, 2015). Although a spectrum of definitions and characterizations exist, scholars agree that TD research differs from other cross-disciplinary approaches (i.e. multidisciplinary, interdisciplinary) based on the magnitude by which concepts from multiple disciplinary fields are mixed, or integrated, to form new theoretical, methodological, and analytic models and its explicit goal of addressing complex problems relevant to society (Rosenfield, 1992; Balsiger, 2004; Thompson Klein, 2004; Hessels and van Lente, 2008; Stokols et al., 2013). Stokols et al., whose definition guided the current study, proposed that TD research is:
… an integrative process whereby scholars and practitioners representing different disciplines work jointly to develop and use novel conceptual and methodological approaches that synthesize and extend discipline-specific theories, methods, and translational strategies to yield innovative solutions to a particular scientific and societal problem.
In the USA, public agencies have funded TD research programmes to address complex public health problems like cancer, nutrition and physical activity, health disparities and tobacco use and their relationships to chronic disease, including the Transdisciplinary Tobacco Research Centers (Morgan et al., 2003), The Transdisciplinary Research on Energetics and Cancer (TREC) (Patterson et al., 2013), Obesity-Related Behavioral Intervention Trials (Czajkowski et al., 2015), and Centers for Population Health and Health Disparities (Warnecke et al., 2008). Broadly, these multi-year, multi-site, multi-million-dollar initiatives aimed to integrate disciplinary approaches to address complex public health challenges. These efforts have contributed to a better understanding of the mechanisms underlying poor health outcomes and how and which interventions may improve population health. Evaluations of these TD initiatives conceptualize the TD research process as yielding expanded outcomes relative to traditional research models that are grounded in single disciplines (Rosenfield, 1992; Klein, 2014; Stokols et al., 2003; Walter et al., 2007; Carew and Wickson, 2010; Huutoniemi et al., 2010; Mitchell et al., 2015). However, in public health, the majority of approaches to describing and gauging TD research and its outcomes have focused on attitudes toward, process of conducting, and characteristics of TD research and the teams that implement the approach (Hall et al., 2008; Misra et al., 2009; Hall et al., 2012a; Misra et al., 2015; Lotrecchiano and Misra, 2018). Evaluations of public health initiatives that have focused specifically on TD outcomes largely describe single outcomes, such as increased quantity and degree of integration of peer-reviewed publications (Hall et al., 2012b), growth in researchers’ social networks (Okamoto and Centers for Population Health and Health Disparities Evaluation Working Group, 2015), and enhanced TD competencies and scholarly productivity among trainees (Vogel et al., 2012). However, no prior work to our knowledge characterizes a set of TD outcomes and describes their relevance to impacting public health problems. As research teams continue to implement TD research to solve public health problems, identifying and characterizing clearly defined outcomes is critical to guiding success of this approach. To address this gap, we use a multi-phase mixed methods approach (Creswell and Piano Clark, 2011) to identify and characterize outcomes of TD research and describe their relevance in addressing complex public health problems using the TREC II initiative as a case example.
Methods
Case example focus: the TREC initiative
TREC was a TD, cooperative center grant mechanism in energy balance and cancer funded by the National Cancer Institute (NCI) from 2005 to 2016. TREC’s mission was to integrate social, behavioral, clinical, and basic sciences to examine relationships among obesity, nutrition, physical activity, and cancer; the initiative aimed to propose, implement, and evaluate novel interventions to reduce the obesity burden (Patterson et al., 2013; Gehlert et al., 2014). The initiative was designed to promote TD research by providing funding for a coordination center, allowing for within- and cross-center pilot grants and coordinated initiative-wide working groups. Known as TREC I (2006–2010), NCI, four research centers, a centralized coordination center, and NCI programme staff comprised the initiative. The TREC II initiative, funded from 2011 to 2016, included four new research centers and the same coordination center at $15 million per year (2010) (Patterson et al., 2013; Gehlert et al., 2014; Schmitz et al., 2016) and is the focus of the current study (Figure 1). The TREC II Coordination Center included an evaluation core whose goal was to facilitate the integration and evaluation of the TD research conducted across the initiative (Hohl et al., 2019). The evaluation core sought to build on NCI evaluation efforts in the TREC I initiative (Hall et al., 2008; Vogel et al., 2012, 2013, 2014) by engaging TREC II members in the initiative’s evaluation. Qualitative and ethnographic approaches promote engagement (Rolfe et al., 2018); thus observations, qualitative interviews, and focus groups were central to the evaluation core’s goal to engage TREC membership. Engagement also occurred through interactive presentations and activities during TREC II scientific meetings and the convening of a cross-center Collaboration and Outcomes Working Group. A central goal of both the evaluation core and the working group was to determine, characterize, and ultimately measure TD research outcomes.
Figure 1.
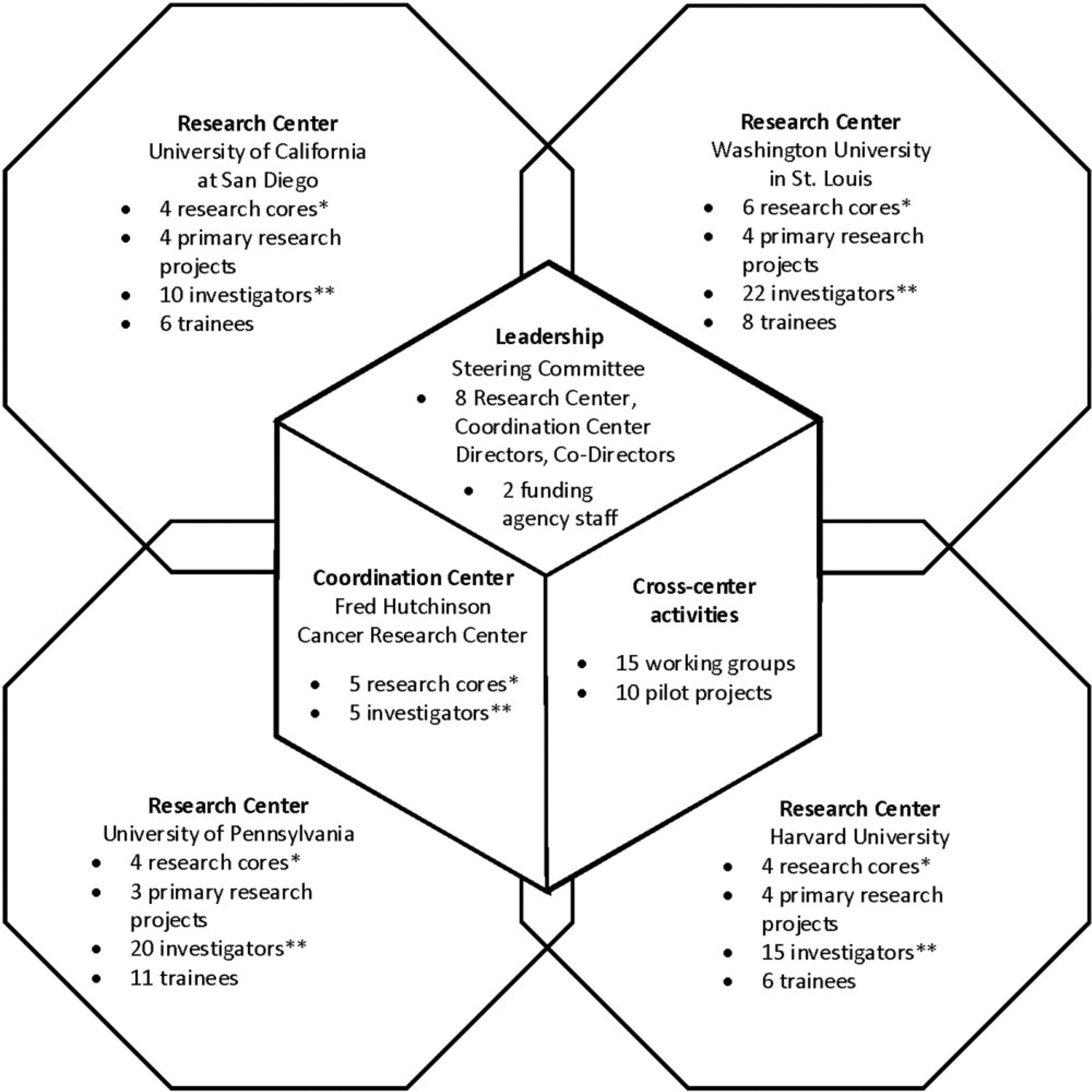
Overview of the TREC II structure (2010–2016).
Members of the TREC Coordination Center evaluation core collected data for the current study. The lead author and evaluation core manager, experienced in qualitative methods, traveled to research centers four times over the 5-year funding period to collect data and interacted with membership through cross-center working group and Steering Committee calls and at in-person TREC Scientific Meetings. We used a multi-phase mixed method framework, in which a problem is investigated through sequential qualitative and quantitative approaches; findings from one research phase are used to inform the next phase (Creswell and Piano Clark, 2011). This approach is appropriate for large-scale evaluations of initiatives like TREC, as its flexibility allows a set of unified research questions to be addressed and used to create a framework for subsequent evaluation (Creswell and Piano Clark, 2011).
Research Phase I: TREC II member engagement
Table 1 illustrates the study’s three phases. In Phase I, two members of the evaluation core team synthesized literature on TD research and conducted the content analysis of TREC II programme documentation (e.g. meeting notes, correspondence, grant proposals) to identify if and how documentation described processes, objectives, and TD outcomes, with the goal of creating a list of TD research outcomes. In May 2013, content analysis results were presented to the Steering Committee, which included TREC II Center Directors, the TREC II Coordination Center Director and Co-Director, and the TREC NCI programme staff—for discussion.
Table 1.
Study overview
| Phase | Purpose | Method | n | Analytic approach |
|---|---|---|---|---|
| I | Identify outcomes of TD research for public health | TREC steering committee session on evaluation | 10 | Content analysis of meeting notes |
| II | Refine outcomes of TD research for public health | Web-based survey among TREC investigators | 23 | Calculate basic descriptive statistics |
| III | Define and characterize TD outcomes in TREC, based on TREC member experiences | Semi-structured interviews among TREC investigators | 26 | Directed content analysis with axial coding of transcripts, |
| Focus groups among TREC trainees | 22 | iterative group discussion |
Research Phase II: web-based survey
We used the TD outcomes identified in Phase I to develop a brief web-based survey to refine the initial set of outcomes. The survey was administered to TREC investigators in January 2014 and included 14 yes/no questions to identify investigators’ perceived involvement in activities related to the nine TD outcomes identified in Phase I. To gather perspectives from a range of investigators who represented diverse disciplines and career stages, TREC II Center Directors were asked to identify a random stratified sample of investigators who represented project leaders, core leaders, and trainees (e.g. doctoral students and post-doctoral fellows) (n = 17) to complete the survey. In addition, all center directors and co-directors (n = 6) and project managers (n = 3) were invited to complete the survey. Survey data were uploaded into Excel to calculate summary statistics.
Research Phase III: interviews and focus groups
We further explored the results of the web-based survey using semi-structured interviews with TREC II investigators and focus groups with trainees. The lead author conducted interviews and focus groups face to face in January and February 2014. All TREC II investigators and trainees who were invited to complete the web-based survey were also invited to participate in an interview. Specifically, we developed a semi-structured interview guide containing a bank of 30 questions. Questions aimed to prompt respondents to (1) define and characterize each TD outcome; (2) describe how the outcome was relevant to addressing complex public health problems; and (3) what, if any, additional outcomes might result from TD research approaches. We used individual interviewees’ responses to the web-based survey to select specific questions from the question bank for each interview. For example, if a participant had responded positively to having contributed to an outcome in the survey, she or he received directed questions to probe for deeper description of that outcome.
Focus groups with TREC trainees aimed to complement Phase II data and to investigate the identified TD outcome ‘training’ in-depth among investigators in the early stages of their research career. A focus group methodology was selected to collect a range of experiences and perceptions of each TREC center’s respective training programme and that of training opportunities offered across the initiative. We designed the focus group guide to determine TREC II trainees’ goals and expectations for participation in a TD initiative, what they perceived as unique aspects of mentorship in a TD initiative, and their perceived competence at addressing societal problems using TD research approaches. All participants were recruited via email, provided written consent, agreed to be audio-recorded, and received a $20 gift card for their time. Study procedures were approved by the Fred Hutchinson Cancer Research Center Institutional Review Board.
Analysis
Individual and focus group interviews were professionally transcribed. Each transcription was checked for accuracy, de-identified, and uploaded into Atlas.ti (Version 8) for coding and analysis. Three members of the study team first reviewed all transcripts and then applied a directed content analysis to characterize, summarize examples, and determine the relevance of the proposed TD outcomes to solving complex public health problems (Hsieh and Shannon, 2005). We sought to determine if and where revision of the proposed outcomes—and their conceptualization—was necessary by developing a list of pre-determined codes that included each of the nine proposed TD outcomes and a general code ‘relevance’ to describe the outcome’s relevance to solving public health problems. Two coders performed axial coding (Saldana, 2009), in which they first applied the initial set of codes to the same five interviews and then met to discuss interpretations, assess inter-coder reliability, add sub-codes, and refine the codes as needed. Coders consulted with the larger study team throughout the coding process, resolved issues of disagreement through group discussion, and built consensus on quote interpretation and emergent themes. This process clarified the ‘new research methods and models’ outcome and led to two new codes reflecting ‘integrated theoretical framework development’ and ‘development and adaptation of new statistical models’. In addition, a new code was created to reflect the outcome ‘new transdisciplinary team and consortia formation’, which encompassed the original ‘new cross- and within-center collaborations’ and ‘building awareness of the transdisciplinary approach’. Finally, all participants received a report of findings from interviews and focus groups conducted at their center. Participants were invited to provide feedback, such as additional interpretations. Members of the TREC II Steering Committee and Collaboration and Outcomes Working Group also had the opportunity to discuss qualitative findings and provide alternative explanations and interpretations.
Results
All TREC Steering Committee members (n = 10) participated in Phase I; 23 (88%) invited TREC II members completed the web-based survey in Phase II; and 26 (100%) invited members participated in a one-on-one interview; and 23 (74%) invited TREC II trainees participated in one of the four focus groups in Phase III (Table 2). Interviews and focus groups lasted ~1 hour (interviews range: 48–75 min; focus groups range: 52–65 min). Based on survey results, directed content analysis, and study team review, we refined the original outcomes resulting in the nine described in Table 3. Table 4 provides additional quotes from study participants representative of each outcome. Below, we describe how investigators defined and characterized the nine outcomes.
Table 2.
TREC II research center interview and focus group respondents; n = 49 (January–February 2014)
| Interviewees | n |
|---|---|
| Center Directors/Co-Director | 5 |
| Project Manager/Administrative Role | 4 |
| Primary Project Investigator or Co-I | 11 |
| Pilot Project Investigator | 12 |
| Core Leader | 6 |
| Early Career Investigator (postdoc or junior faculty) | 7 |
| Total interviewees | 26a |
| Focus groups (n = 4) | |
| Traineesb | 23 |
Some individuals interviewed hold multiple roles in the TREC initiative. This number reflects the total number of TREC individuals interviewed.
TREC members who participated in focus groups self-identified as TREC trainees.
Table 3.
Relevance and examples of TREC transdisciplinary outcomes
| Outcome | Relevance for solving complex societal problems | Examples of TREC members’ achievement of transdisciplinary outcomesa | |
|---|---|---|---|
| 1 | New transdisciplinary team and consortia formation | Forming consortia that bridge academic disciplines, political stakeholders, and community partners can lead to long-term collaborations that foster innovation, creativity, and sustainable public health impact. Venues for consortium building may include but are not limited to conferences, symposia, or town hall meetings |
|
| 2 | Integrated theoretical framework development | Frameworks that combine concepts and draw on expertise from more than one discipline guide transdisciplinary research by helping to ensure that multiple perspectives are considered and that the optimal combination of expertise is incorporated throughout the research process. Along with team and consortia formation, these frameworks form the foundation for subsequent transdisciplinary research outcomes |
|
| 3 | Multi-Level intervention model development and testing | Multi-level interventions aim to simultaneously address a range of individual-, interpersonal-, organizational-, community-, and policy-level factors that influence complex public health problems. Such models follow naturally from a transdisciplinary approach in that they cover many of the diverse levels of analysis to understand and intervene upon the interaction between biological, behavioral, and socio-environmental factors |
|
| 4 | Development and adaptation of relevant statistical models | New statistical methods and new uses for existing statistical methods are required to determine associations, interrelationships, and mutual influence that biological, genetic, environmental, social, and behavioral dimensions have on each other and on public health overall |
|
| 5 | Translation of findings across levels of science | Transdisciplinary teams comprise investigators and stakeholders who aim to integrate findings from across levels of influence to speed translation from basic science to clinical practice and policy |
|
| 6 | Public policy influence | Transdisciplinary research approaches champion scientific innovation and discovery. By involving academic and community, and government stakeholders, transdisciplinary teams apply these discoveries through policy changes that impact the public health challenges of concern |
|
| 7 | Transdisciplinary manuscript publication | Transdisciplinary research is conducted by teams of investigators, which can result in higher publication rates compared to single investigator-initiated research. Publications and grants representative of the transdisciplinary approach exhibit high degree of disciplinary integration. Publications that highlight findings from transdisciplinary approaches raise awareness among the academic community and can lead to greater interest and investment in transdisciplinary research |
|
| 8 | Transdisciplinary grant awards |
|
|
| 9 | Training the next generation of transdisciplinary researchers | Complex public health problems such as the relationships between diet, physical activity, and cancer require innovative, integrated scientific solutions. Thus, efforts must be made to train investigators from diverse disciplines to communicate, collaborate, develop novel conceptual models and research methodologies, and translate and integrate findings across levels of influence |
|
Examples provided are representative but not exhaustive of those across the TREC II initiative.
Table 4.
Representative quotes characterizing TREC transdisciplinary outcomes (January–February 2014)
| Outcome | Representative quotes | |
|---|---|---|
| 1 | New transdisciplinary team and consortia formation | It is important to showcase the contributions of transdisciplinary projects to other investigators. I’ve been in so many different venues where I present on the really consistent evidence that we are finding in TREC around sleep and obesity. There are so many different ways that it then triggers another investigator in the room to come up to me and say, ‘I’m just beginning a cohort. I hadn’t thought about including sleep or including questions about sleep.’ And I see that as a direct result of presenting in these national forums and kind of getting the word out, to then have someone in the room, or other researchers in the room, consider adding sleep into their studies. (Participant 4220) |
| 2 | Integrated theoretical framework development | [The] unified framework […] is bridging basic science, epidemiology, and clinical research. That’s [Investigator]’s project on animal models for healthy aging. […] We have also developed statistical approaches to analyze predictors of healthy aging in large cohort studies. We wanted to identify dietary factors, lifestyle factors and genetic factors for healthy aging. For a clinical component we have a project to look at the effects of physical activity and metformin among cancer survivors, […] We want to prolong the life of the cancer survivors and improve both the quality and the quantity of their lifespan. […] This is a relatively novel area that we have developed. (Participant 4200) Sometimes in pediatrics we borrow a lot from adult medicine. […] But I am interested in innovating from within pediatrics. There’s a lot of work showing that insufficient sleep in adults is associated with obesity or adiposity gained through different mechanisms, such as hormonal influences, physical activity, or lack of physical activity. But what’s never discussed in adults is that insufficient sleep might actually affect executive function. In children, behavior and impulsivity [are] things that as pediatricians, we know. We know behavior. We know cognition. It’s our language. It doesn’t come up as often in some of the adult mechanisms, but in children it’s incredibly plausible that sleep deprivation in a child affects their impulsivity, their behavior, their ability to make appropriate decisions. That kind of executive function and control has never been studied or proposed as a mechanism for why sleep is associated with obesity. There are many different examples where I also bring in that conceptual framework to broaden our sense of what are some mechanistic pathways [between sleep and obesity]. (Participant 4220) |
| 3 | Multi-Level intervention model development and testing | The statistical work that was done on our main TREC project [an exercise/weight loss intervention] data previously was done by exercise scientists [with participants] in the lab. […] As an interventionist, a behavior scientist, I think about the data in such a different way […] How might GPS data-the data that puts you in an environment-affect the algorithms and the whole picture? […] So in that way, the neighborhood piece comes into it. [We] have applied machine learning algorithms to free living data, not lab data. The computer scientists [are] not public health people so they haven’t thought about collecting free living data either. […] They might have developed algorithms to be able to detect X, Y, Z, but not with a purpose in mind. [We think about how] this algorithm can help somebody do X, Y. (Participant 4330) |
| 4 | Development and adaptation of relevant statistical models | You have a surrogate measure and gold standard measure of diet, and you have a biomarker, the method of triads. There’s a mathematical way of using those three pieces of data to come up with a measurement error correction, even if there is correlated error… So what we’ve done is take that general concept of the method of triads and find new applications for them. So the fact that it has an application with nutritional epidemiology doesn’t mean that there’s other areas where it cannot be used. And as long as the statistical principles of the method applies to any other problem, this can be used for any other problem. (Participant 4220) |
| 5 | Translation of findings across levels of science | Transdisciplinary teams ‘should be mentoring basic scientists in a way that helps us to translate to humans…mentoring human researchers in a way that helps them to understand animal models…-training both of those sets of scientists in understanding health policy and changing policy, dissemination science.’ (Participant 4400) |
| 6 | Public policy influence | It is a dilemma. When I first started talking about [engaging in policy work], I had very traditional researchers in this university saying, ‘that’s not for you to do. You’re too junior to be thinking about affecting policy. You should be very focused and that’s a distraction. |
| 7 and 8 | Transdisciplinary manuscript publication and transdisciplinary grant awards | We’ve already talked with NIH and NCI about looking at the community, neighborhood characteristics, and cancer outcomes and how they might be related. We’re applying for a cross-TREC pilot grant [to gather] preliminary information to look at this. […] The luxury of working with the two different sites [is that] we can look in Philadelphia and in St. Louis and compare across populations to see if there are similarities or not, then move forward into intervention work. (Participant 4440) |
| 9 | Training the next generation of transdisciplinary researchers | My expectations were to learn about other objective measures of energetics. [I’ve learned] a lot about accelerometry and GPS from other TREC center [investigators]. I don’t know if that was my goal at the outset, but through TREC, my goals have become to build that expertise. It’s definitely new frameworks. It’s new technology, it’s new kind of analytical approaches, too. And it’s not kind of the traditional Epi that I was taught here. So I’m trying to incorporate what I know in this new technology, new approach. (Focus Group 4200) Most innovation happens at the intersections—not in the center—of disciplines. In the center of disciplines is repetition. You do what you know, what your mentor did. If you really want innovation, you have to be at an intersection, an interface. These days, doing what you did just isn’t sufficient. You just cannot come in with incremental science anymore. You’ve got to come in with something new. […] There’s not a good future for very, very generally unidisciplinary research, especially in human research. (Participant 4300) |
Outcome 1: new TD team and consortia formation
Respondents said that one critical outcome of funded TD teams is that connections formed have led to long-term collaborations between researchers representing multiple and often disparate disciplines that otherwise would not have occurred. They said TD teamwork fosters innovation and creativity from study design to implementation, analysis, and dissemination that has implications for real-world application, such as in the case of investigators whose research contributed to changes in clinical guidelines to prioritize sleep to reduce obesity risk. A human behavior researcher reported that adopting TD approaches to science:
makes you think about things in a way you normally wouldn’t. I find when I talk to basic scientists or investigators who work with mice that [we] approach the question in different ways and I think it helps for a better outcome in terms of a research question.
(Participant 4103)
Investigators reported that TD team science has the capacity to extend to a much wider audience than does monodisciplinary teams. They reported utilizing opportunities to present in new settings, where they were able to share results from their disciplinarily integrated studies and develop connections with investigators outside of the initiative (see Table 4). Senior investigators related that for TD consortia ‘to be relevant to the community’, institutions—not necessarily individuals—should engage those outside the research institution in their work, and specifically have an ‘obligation to communicate results and broader implications back to stakeholders, which at some level are the taxpayers’ (Participant 4100) Another investigator described their center’s commitment to that engagement:
We’re again bringing in other [researchers, community organizations, worksites, and policy makers] who have not thought about interacting with other investigators the way we’re doing now. We’re [also] disseminating the work by research papers, editorials, and other kinds of writing that leads to transdisciplinary thinking and trying to inform the [research] community about different ways they could have an impact, you know, giving them examples of how we’ve done it, how they can have an impact that might be larger than what their individual discipline is giving them.
(Participant 4450)
Outcome 2: integrated theoretical frameworks
Although ‘integrated theoretical frameworks’ was not an item in the quantitative survey, it emerged as an outcome through the qualitative phase as investigators described their work across TREC II research studies. The teams and consortia formed as a consequence of TREC II provided investigators with the diverse expertise to think about public health problems in new ways. Participants reported that these teams propelled them to develop new theoretical frameworks that bridged multiple conceptual domains. For example, this investigator described experiences in cross-center development projects, in which each site contributed uniquely to the success of the project, advanced team members’ ability to assess interacting influences on energy balance and cancer risk:
Our site’s expertise is that we had an ongoing cohort study [with…] participants who were very likely to adhere to study protocols […and…] expertise in the GIS side, in terms of layering on spatial information. At [another institution] they had a lot more experience with accelerometry and GPS in very small studies and cleaning that data. [Investigator] at [institution] is a world expert in physical activity research. And then, [institution] has a lot of expertise in GIS and other kind of novel objective measures too. So [this team] definitely expanded our reach in terms of measures into areas that were not within the expertise at this site.
(Participant 4240)
Such integrated frameworks guided and unified individual research projects as part of each TREC II center. A senior investigator commented that center’s framework, ‘gets us to integrate all the projects across the whole of our center. And that has everyone thinking at new levels [about how to] model obesity and cancer risk and outcomes across a life course’ (Participant 4100) Another investigator described his center’s multidimensional framework that was designed to ‘have direct public health and clinical relevance’ on healthy aging. He explained, ‘[The] unified framework […] is bridging basic science, epidemiology, and clinical research’ (see Table 4 for full quote). A trainee who participated in a cross site pilot project described a framework the team developed to ‘integrate measures of physical activity, sedentary behavior, sleep, [and] location’, anticipating that subsequent frameworks could ‘layer on other spatial data, [like] air pollution, so that we can build more personal measures of air pollution […] green space […] and land use data’ (Participant 4240).
Outcome 3: multi-level intervention model development and testing
One approach by which TREC II researchers addressed energetics and cancer was by developing, implementing, and evaluating multi-level intervention models. Such models consider a range of individual, interpersonal, organizational, community, and policy-level influences on health outcomes (Warnecke et al., 2008; Taplin et al., 2012). To that end, investigator teams across centers had obtained both internal and external funding to translate findings from TREC II observational studies into the development of interventions that aimed to reduce obesity-related cancer morbidity and mortality. They noted that development of multi-level intervention models and their implementation arose from projects within their individual centers and through cross-center pilot projects and working groups. At one center, investigators developed an intervention to determine the extent to which exercise and/or weight loss affects breast cancer-related lymphedema outcomes among survivors, and what economic benefit resulted. A basic scientist, a behavioral interventionist, and an expert in emerging technology who had met through TREC proposed a project to reduce extended sitting time among older adults, a serious risk factor for cancer and chronic disease. Their multi-level intervention model addressed individual factors such as behavior change and community-level factors such as altering work environments. Representing what one investigator described as ‘a whole other area of new interactions of interdisciplinary work’, they planned to assess biomarker response, racial/ethnic differences, and objective measures of movement based on tracking device data.
Outcome 4: development and adaptation of relevant statistical models
About three quarters of investigators reported using or developing new statistical models in their work. These investigators said their involvement in TD research projects propelled them to consider the value of developing and adapting statistical models to analyze associations, interrelationships, and mutual influence between biological, genetic, environmental, social, and behavioral factors and consequent health outcomes. TREC members reported that statisticians within and across TREC II research centers challenged investigators to apply statistical models in new ways. Statisticians reported that having access to statisticians from other disciplines working on similar topics of cancer and energy balance was a new experience attributable to the collaborative structure of TREC. Sharing ideas with statisticians across TREC II centers prompted a deeper understanding of measurement of complex variables. Investigators recognized the application of statistical approaches in the realm of cancer and energetics research was unique; thus, an investigator reported ‘I’m not sure they’re novel statistical designs, but they’re new for us, which is exciting’ (Participant 4306). As an example, in a primary research project conducted within one TREC center, statisticians developed a bio bridge design in which multiple imputations were used to examine biomarkers as intermediate endpoints for a randomized controlled trial to predict and prevent breast cancer recurrence. A statistician advising trainees on a pilot project that spanned multiple TREC centers described that team’s approach to addressing the correlated error inherent with diet self-report and the lack of biomarkers for puberty (see Table 4). At another TREC center, a clinician investigating the effect of maternal diet on prostate tumor proliferation in male mice teamed with a population health biostatistician who was:
shocked that we had so few animals […] so he came up with this new Bayesian model to look at our data. […] When he looked at the different variables, obviously, maternal diet made a big difference on proliferation, but the second most important thing was the number of male mice in the cage. The more mice that were in the cage, the more likely the mice were to get the hyper proliferation as opposed to the mice that were either housed singly or just with one other mouse.
(Participant 4120)
Outcome 5: translation of findings across levels of science
Although few investigators (32%) reported having participated in research to translate animal studies into human studies and vice versa, many interviewees identified evaluating and applying findings from biomedical to clinical to policy as an essential outcome of TD research. At one TREC II center, investigators in psychology, animal research, biomarkers, exercise science, behavioral interventions, health disparities, and endocrinology at all career levels proposed a project to translate findings about fasting, circadian rhythm, and breast cancer risk from a mouse model into a human observational study. They sought to determine if nightly fasting among Latinas and non-Latina white women may predict similar outcomes of inflammation and insulin resistance, which are associated with increased breast cancer risk. One investigator noted that this work:
could translate immediately into public health guidelines. You should have a fasting period at night […] so you don’t disrupt your circadian clock. Right now, we really have no evidence-based guidelines for like meal frequency or timing. […] Assuming it is replicable, it’s straight to guidelines.
(Participant 4300)
A senior investigator described the primary research projects and ancillary projects at their TREC II center as part of a systems science modeling approach. Biological data from animal and human models, data from intervention studies, and data from studies of the built environment would contribute to a broader exploration of how to intervene to reduce cancer risk.
Outcome 6: public policy influence
Respondents agreed unanimously that a central role of research is to build the evidence base to inform changes in policy to promote population health. They said the nature of TD collaboration specifically in TREC facilitated a drive to make systematic, structural policy changes. This investigator illustrated this concept, stating:
There’s this hole in the middle of our efforts to try to actually change things. The investigators who are building the evidence base build the evidence base and stop. The public health people focus on changing policy and stop. The physicians focus on applying the best evidence that they can without actually changing their infrastructure and stop. The health services people are focused on high level changes. Transdisciplinary researchers say, ‘We have a new evidence base. How do we change the clinical infrastructure?’
(Participant 4100)
Participants were cognizant of the ethical challenges of using preliminary evidence to inform policy, citing the amount of time it takes to conduct studies and test evidence as one challenge to influencing public policy. They noted that their exposure through TREC II to diverse research, community, and government stakeholders who had expertise in dissemination and implementation propelled them to think critically about the societal implications of their work and specifically, ‘how public policy works […] so we are not overclaiming what we might be able to do with what we’ve discovered in our work’ (Participant 4330). At one TREC center, investigators developed guidelines and public policies ranging from removing sugar-sweetened beverages from school cafeterias, informing school start times based on children’s need for sleep, and developing a federal policy on affordable housing, all determinants of obesity and cancer demonstrated through their TD research. Trainees and junior investigators recognized the importance of engaging with those outside of research and academic institutions, ideally during study design, to ‘understand what challenges they face, and what’s realistic, so that my research can be as applied as possible’ (Participant 4102). Investigators across disciplines and career stages acknowledged the relevance of their role as researchers in policy, as this investigator expressed, ‘…the research and the policy […] is all part of a continuum. You can’t have the policy changes responsibly without the research behind it’ (Participant 4421). These stakeholders were seen as critical to developing appropriate conceptual frameworks whose application could eventually guide policy efforts. Investigators described multiple challenges of engaging in policy work as academic researchers, such as conflicting expectations of TD researchers and university policies. Some investigators noted that while policy work is inherent in TD research, it is seldom rewarded in academic institutions and not emphasized in many degree programs; thus, investigators are not equipped with the tools to translate the relevance of their work to audiences outside of research institutions.
Outcomes 7 and 8, scholarly productivity: TD manuscript publication and TD grant awards
Respondents recognized that publications and independent research funding, while not unique to TD research, are the accepted benchmarks of successful research. Accordingly, the majority (78%) reported applying for new non-TREC grants with other TREC investigators and considered 30 of their grants and 24 of their publications to be TD. Investigators did, however, describe two major challenges: first, identifying journals that would favorably review and accept TD publications (i.e. those reflecting multiple disciplines), and second, finding the additional time required to collaborate across disciplines, departments and institutions to develop integrated frameworks and implement projects, analyze results, and disseminate and translate findings. Investigators described a collaboration across TREC II centers to develop new grant applications that addressed multi-level components of the impact of exercise and weight loss on breast cancer co-morbidities like lymphedema. This cross-center team designed a study to examine whether racial/ethnic disparities in severity and progression of lymphedema result in higher costs for minority group members. This effort relied on a framework that integrated biological, community, and economic theory that investigators said was made possible through TREC II collaborations. One investigator described the process of convening researchers with diverse expertise and a unifying interest and developing a grant application to address health disparities in breast cancer. This investigator perceived this practice as different from non-TD approaches based on the project’s focus to create a framework that linked theories and expertise from multiple disciplines. The framework could inform a multi-level intervention to improve disparate breast cancer outcomes.
Outcome 9: training the next generation of TD researchers
Nearly two-thirds (61%) of respondents reported participating in TREC-specific training activities, and three quarters (74%) of those surveyed identified themselves as a mentor to trainees. Each TREC II research center was required to support an Education and Training Core with the goal to train investigators to integrate disciplines to investigate and address multiple influences on energy balance and cancer. In addition, TREC II supported a cross-center Training and Education Working Group a Coordination Center investigator. Trainees said these opportunities facilitated their career development and built a sense of community across investigators from different departments and disciplines at their institutions. These relationships led to productive research and mentorship collaborations that trainees said positioned them to both understand multiple levels of influence on obesity and cancer and determine where to intervene to improve population health. One trainee commented, ‘Every project that I work on is a team approach. It’s not just me and my mentor working on something, but we involve people from all different levels [of science] that are like a mini group of experts’ (FG4300). Trainees said that TD research requires new skills, such as working in cross-disciplinary, often dispersed teams, and developing novel conceptual models and analytic approaches with an overall goal to yield public health impact. Thus, they underscored the importance of gaining cross-disciplinary training to prepare them to conduct this type of work. An epidemiologist with expertise in the built environment said as a TREC trainee, he expected to learn to apply ‘new frameworks […] new technology […] new analytical approaches [beyond the] traditional Epi I was taught here’ to address the burden of obesity and cancer (see Table 4 for full quote).
Senior investigators emphasized the importance of leveraging TREC II human and financial resources to facilitate growth among trainees. To that end, proposals involving trainees were prioritized for pilot project funds. Trainees across all four centers recognized the value of having access to those funds and their corresponding research opportunities. One trainee reported, ‘If you have an idea, if somebody’s excited about a new project, it’s actually feasible to figure out how to make it happen. […] There are funds specifically dedicated to our development and developing new ideas’ (FG4400). Another participant reflected on the value of having access to data from multiple projects across the TREC II research centers, saying, ‘Since TREC has been going on for some time now there’s data available across sites that as a trainee you have access to. If we’re interested, we’re welcome to join in [analysis and manuscript writing]’ (FG4200). Trainees said that as TREC II members, they benefited from mentorship with experts that spanned institutions and disciplines, from basic science to population health. This trainee said that through:
cross-TREC projects and also our working group, we’ve really been able to bring in a very diverse set of spatial measures. […] There are investigators who have much more of a focus on objective real-time measures, and then others who understand geography. [The TREC collaborations have] really helped me to learn a lot of new approaches and nuance into the field that I thought I was really good in. […] Oftentimes in Epi we’re taught one concept. And then in Geography they have a very, very different approach. […] [I learned] new terminology and new concepts that I just took for granted.
A mentor summarized the importance of training scholars to pursue TD research, despite the difficulties such training may present: ‘Most innovation happens at the intersections—not in the center—of disciplines. In the center of disciplines is repetition. […]. If you really want innovation, you have to be at an intersection, an interface’ (Participant 4300; see Table 4 for full quote).
Discussion
In this study, we applied a multi-phase, mixed method approach to establish, define, and characterize nine complementary outcomes of the TD approach based on TREC II member perspectives. This work advances our understanding of TD research for public health problems in three ways. First, it offers an outcome framework inclusive of characterizations and tangible examples of ways in which investigators in a national, multi-site TD initiative worked to impact public health challenges at the intersection of energy balance and cancer. Second, this work identifies two new TD outcomes that have not been characterized in previous evaluations of TD public health initiatives, consortium building and public policy influence. Third, this work draws connections between these outcomes and their relevance to the goal of a national initiative to reduce the obesity burden and improve population health. Collectively, outcomes identified in this study can be characterized as the conceptual, intellectual, institutional, and societal products that resulted from application of a transdisciplinary research approach. Although the TD outcomes identified overlap somewhat with those expected in non-TD approaches, they are distinguished by the involvement of team members who represent diverse disciplines, reliance on new and integrated theoretical frameworks, and the explicit goal to address a societal problem of interest. These nine TD outcomes can serve as a starting point for assessing the value added by TD research approaches.
Two outcomes identified by TREC investigators that are distinct from other TD outcome investigations were forming consortia and influencing public policy. Investigators emphasized the importance of bridging academic disciplines, political stakeholders, and community partners as a means of sustaining programmes that aim to improve public health outcomes. This conceptualization of TD research aligns with European conceptualizations, which call for knowledge integration from both scientific and nonscientific stakeholders (Flinterman et al., 2001; Hadorn et al., 2010). Because this work is time consuming and can potentially rely on extensive resources, TD investigators must be appropriately trained to partner and collaborate across both academic disciplines and community sectors and be supported by their universities’ administrations. Evidence demonstrates that context and environment (e.g. institutional resources, geographic proximity) and individual-level factors (e.g. disciplines represented, personality) influence team development, success, and TD orientation (Hall et al., 2008; Stokols et al., 2008a; Olson et al., 2009; Misra et al., 2015). The collaboration of TREC II’s four research centers, a coordination center, and NCI enabled investigators to draw upon resources and expertise across and beyond the initiative. TREC II participants cited cross-center pilot projects, cross-center scientific working groups, and center-level cores as specific TREC programme infrastructure components that were critical to supporting teams and fostering achievement of TD outcomes for public health impact.
Investigators from all career stages said that replicable, repeated evidence generated from TD research should necessarily inform policies and that TD research teams are ideally equipped to become engaged in policy processes. However, while some mid-stage investigators reported that they were experienced in translating evidence into practice, they were unsure which avenues to take to translate such findings into public policy. Early career investigators particularly reported not having the support, training, or skills to engage in policy work, representing an area of further consideration for incorporation into TD training programmes. A similar concept was highlighted in an evaluation of TD doctoral programmes, wherein more than half of dissertations did not aim to translate results into ‘community problem solving’ efforts. These findings have implications for both the design of future TD training programs that endeavor to prepare scholars to integrate disciplines in service of addressing public health problems and university practices, policies, and reward systems. If policy work is a valued and necessary component for speeding research translation, training programs should provide opportunities for investigators to better understand and become engaged in this work, and university practices should reward efforts toward translating evidence into policy (Mitrany and Stokols, 2005; Neuhauser et al., 2007; Giles-Corti et al., 2015). Our work supports findings that engaging stakeholders outside of academia, such as community members and policy experts, are be critical to efficiently and effectively translating basic science findings to public policies that improve population health (Rashid et al., 2009; Ramanadhan et al., 2018).
A central discussion among TREC investigators in this study was the relevance of their work and these outcomes to the initiative’s ultimate goal of understanding and addressing cancer and energy balance and improving population health. Future research is needed to examine the temporality and sequencing of each of TD outcome identified here. Such studies may qualitatively explore and quantitatively measure the interacting influence of each of these outcomes on sustained population health improvements.
Limitations
We made multiple and diverse attempts to characterize the experience and perspectives of TREC II investigators at all levels and corroborate findings regarding TD outcomes. However, the data only represent those who participated in the study and may not be representative of the entire TREC II initiative. The tools developed for this study were a result of multiple engagement efforts and thus customized to TREC and may not generalize widely. However, the initiative spanned multiple schools and departments within five geographically dispersed research institutions and a prominent federal funding agency, which lends to inferential transferability to other similarly structured initiatives (Teddlie and Tashakkori, 2003). The quantitative survey was only administered to a subset of TREC investigators (n = 23) and did not include questions about TREC members involvement in influencing policy or forming new collaborations. Due to the timing of the decision to include a larger sample of TREC trainees in focus group discussions, the survey had been rolled out and fewer trainees contributed to the survey than those who participated in focus groups. Future studies should investigate in more depth the complexities and outcomes of TD training programmes to build on work conducted in previous initiatives (Mitrany and Stokols, 2005; Vogel et al., 2012). Finally, these results were influenced by the TD context within which TREC investigators worked. Thus, further research should investigate if and how such outcomes may pertain to other TD initiatives, and which factors may constrain or facilitate their achievement.
Conclusion
This work identifies and characterizes nine complementary TD outcomes that can be used to evaluate progress toward impact on complex public health problems. Strategic investment in infrastructure that supports team development and collaboration, such as a coordination center, cross-center working groups, annual funded developmental projects, and face-to-face meetings, may foster the achievement of these outcomes. This exploratory work provides a basis for the future investigation and development of quantitative measurement tools to assess the achievement of TD outcomes that are relevant to solving multifactorial public health problems.
Acknowledgements
The authors would like to thank all TREC II members who participated in this study, with particular gratitude to programme administration staff Diana Lowry, Lori Schumacher, Christine Marx, Renee Miciek, and Bilge Pakiz. This work was supported by National Cancer Institute (NCI) grant U01 CA116850. Sarah Hohl was also supported by NCI grant T32 CA092408, Biobehavioral Cancer Prevention and Control Training Grant.
Footnotes
Conflict of interest statement. None declared.
References
- Adler NE, Glymour MM, and Fielding J (2016) ‘Addressing Social Determinants of Health and Health Inequalities’, JAMA: The Journal of the American Medical Association, 316: 1641–2. [DOI] [PubMed] [Google Scholar]
- Arnold M et al. (2015) ‘Global Burden of Cancer Attributable to High Body-Mass Index in 2012: A Population-Based Study’, The Lancet Oncology, 16: 36–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Balsiger J (2015) ‘Transdisciplinarity in the Class Room? Simulating the co-Production of Sustainability Knowledge’, Futures, 65: 185–94. [Google Scholar]
- Balsiger PW (2004) ‘Supradisciplinary Research Practices: History, Objectives and Rationale’, Futures, 36: 407–21. [Google Scholar]
- Basen-Engquist K, and Chang M (2011) ‘Obesity and Cancer Risk: Recent Review and Evidence’, Current Oncology Reports, 13: 71–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carew AL, and Wickson F (2010) ‘The TD Wheel: A Heuristic to Shape, Support and Evaluate Transdisciplinary Research’, Futures, 42: 1146–55. [Google Scholar]
- Centers for Disease Control and Prevention (CDC) (2009) ‘Cigarette Smoking among Adults and Trends in Smoking cessation—United States, 2008’, Morbidity and Mortality Weekly Report, 58: 1227–32. [PubMed] [Google Scholar]
- Creswell JW, and Piano Clark VL (2011) Designing and Conducting Mixed Methods Research, 2nd edn. Thousand Oaks, CA: Sage Publications. [Google Scholar]
- Czajkowski SM et al. (2015) ‘From Ideas to Efficacy: The ORBIT Model for Developing Behavioral Treatments for Chronic Diseases’, Health Psychology, 34: 971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flinterman JF et al. (2001) ‘Transdisciplinarity: The New Challenge for Biomedical Research’, Bulletin of Science, Technology & Society, 21: 253–66. [Google Scholar]
- Gehlert S et al. (2014) ‘Advancing Transdisciplinary Research: The Transdisciplinary Research on Energetics and Cancer Initiative’, Journal of Translational Medicine & Epidemiology, 2: 1032. [PMC free article] [PubMed] [Google Scholar]
- Giles-Corti B et al. (2015) ‘Translating Active Living Research into Policy and Practice: One Important Pathway to Chronic Disease Prevention’, Journal of Public Health Policy, 36: 231–43. [DOI] [PubMed] [Google Scholar]
- Hadorn GH, Pohl C, and Bammer G (2010) Solving Problems through Transdisciplinary Research and Integration’, in Robert F, Klein JT and Pacheco RCDS (eds) The Oxford Handbook of Interdisciplinarity, pp. 431–52. New York: Oxford University Press. [Google Scholar]
- Hall KL et al. (2008) ‘The Collaboration Readiness of Transdisciplinary Research Teams and Centers Findings from the National Cancer Institute’s TREC Year-One Evaluation Study’, American Journal of Preventive Medicine, 35 (2 Suppl): S161–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall KL et al. (2012a) ‘A Four-Phase Model of Transdisciplinary Team-Based Research: Goals, Team Processes, and Strategies’, Translational Behavioral Medicine, 2: 415–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall KL et al. (2012b) ‘Assessing the Value of Team Science: A Study Comparing Center- and Investigator-Initiated Grants’, American Journal of Preventive Medicine, 42: 157–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hessels LK, and van Lente H (2008) ‘Re-Thinking New Knowledge Production: A Literature Review and a Research Agenda’, Research Policy, 37: 740–60. [Google Scholar]
- Hiatt RA, and Rimer BK (1999) ‘A New Strategy for Cancer Control Research’, Cancer Epidemiology Biomarkers & Prevention, 8: 957–64. [PubMed] [Google Scholar]
- Hohl SD, Knerr S, and Thompson B (2019) ‘A Framework for Coordination Center Responsibilities and Performance in a Multi-Site, Transdisciplinary Public Health Research Initiative’, Research Evaluation, 28: 279–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hsieh H-F, and Shannon SE (2005) ‘Three Approaches to Qualitative Content Analysis’, Qualitative Health Research, 15: 1277–88. [DOI] [PubMed] [Google Scholar]
- Huutoniemi K et al. (2010) ‘Analyzing Interdisciplinarity: Typology and Indicators’, Research Policy, 39: 79–88. [Google Scholar]
- Klein JT (2014) ‘Discourses of transdisciplinarity: Looking Back to the Future’, Futures, 63: 68–74. [Google Scholar]
- Lotrecchiano GR, and Misra S (2018) Transdisciplinary Knowledge Producing Teams: Toward a Complex Systems Perspective. Informing Science, 21: 52–74. [Google Scholar]
- Lynch SM, and Rebbeck TR (2013) Bridging the Gap between Biologic, Individual, and Macroenvironmental Factors in Cancer: A Multilevel Approach. Cancer Epidemiology, Biomarkers & Prevention: a Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology, 22: 485–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McAneney H et al. (2010) ‘Translating Evidence into Practice: A Shared Priority in Public Health?’, Social Science & Medicine, 70: 1492–500. [DOI] [PubMed] [Google Scholar]
- McTigue KM et al. (2003) ‘Screening and Interventions for Obesity in Adults: Summary of the Evidence for the US Preventive Services Task Force’, Annals of Internal Medicine, 139: 933–49. [DOI] [PubMed] [Google Scholar]
- Minian N et al. (2020) ‘Identifying Contexts and Mechanisms in Multiple Behavior Change Interventions Affecting Smoking Cessation Success: A Rapid Realist Review’, BMC Public Health, 20: 918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Misra S et al. (2009) ‘Evaluating an Interdisciplinary Undergraduate Training Program in Health Promotion Research’, American Journal of Preventive Medicine, 36: 358–65. [DOI] [PubMed] [Google Scholar]
- Misra S, Stokols D, and Cheng L (2015) ‘The Transdisciplinary Orientation Scale: Factor Structure and Relation to the Integrative Quality and Scope of Scientific Publications’, Journal of Translational Medicine & Epidemiology, 3: 1042. [Google Scholar]
- Mitchell C, Cordell D, and Fam D (2015) ‘Beginning at the End: The Outcome Spaces Framework to Guide Purposive Transdisciplinary Research’, Futures, 65: 86–96. [Google Scholar]
- Mitrany M, and Stokols D (2005) ‘Gauging the Transdisciplinary Qualities and Outcomes of Doctoral Training Programs’, Journal of Planning Education and Research, 24: 437–49. [Google Scholar]
- Morgan GD et al. (2003) ‘Facilitating Transdisciplinary Research: The Experience of the Transdisciplinary Tobacco Use Research Centers’, Nicotine & Tobacco Research, 5 (Suppl_1): S11–S9. [DOI] [PubMed] [Google Scholar]
- Neuhauser L et al. (2007) ‘Advancing Transdisciplinary and Translational Research Practice: Issues and Models of Doctoral Education in Public Health’, Journal of Research Practice, 3: 19. [Google Scholar]
- Okamoto J and Centers for Population Health and Health Disparities Evaluation Working Group (2015) ‘Scientific Collaboration and Team Science: A Social Network Analysis of the Centers for Population Health and Health Disparities’, Translational Behavioral Medicine, 5: 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson GM, Olson JS, and Venolia G (2009) ‘What Still Matters about Distance?’, in Proceedings of HCIC 2009. [Google Scholar]
- Patterson RE et al. (2013) ‘The 2011–2016 Transdisciplinary Research on Energetics and Cancer (TREC) Initiative: Rationale and Design’, Cancer Causes & Control, 24: 695–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pohl C (2008) ‘From Science to Policy through Transdisciplinary Research’, Environmental Science & Policy, 11: 46–53. [Google Scholar]
- Ramanadhan S et al. (2018) ‘Participatory Implementation Science to Increase the Impact of Evidence-Based Cancer Prevention and Control’, Cancer Causes & Control, 29: 363–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rashid JR et al. (2009) ‘Eliminating Health Disparities through Transdisciplinary Research, Cross-Agency Collaboration, and Public Participation’, American Journal of Public Health, 99: 1955–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rolfe DE et al. (2018) ‘Using Qualitative Health Research Methods to Improve Patient and Public Involvement and Engagement in Research’, Research Involvement and Engagement, 4: 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenfield PL (1992) ‘The Potential of Transdisciplinary Research for Sustaining and Extending Linkages between the Health and Social Sciences’, Social Science & Medicine, 35: 1343–57. [DOI] [PubMed] [Google Scholar]
- Saldana J (2009) The Coding Manual for Qualitative Researchers. Thousand Oaks, CA: Sage. [Google Scholar]
- Schmitz KH et al. (2016) ‘TREC to WHERE? Transdisciplinary Research on Energetics and Cancer’, Clinical Cancer Research, 22: 1565–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siegel RL et al. (2015) ‘Deaths Due to Cigarette Smoking for 12 Smoking-Related Cancers in the United States’, JAMA Internal Medicine, 175: 1574–6. [DOI] [PubMed] [Google Scholar]
- Srinivasan S, O’fallon LR, and Dearry A (2003) ‘Creating Healthy Communities, Healthy Homes, Healthy People: Initiating a Research Agenda on the Built Environment and Public Health’, American Journal of Public Health, 93: 1446–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokols D et al. (2003) ‘Evaluating Transdisciplinary Science’, Nicotine & Tobacco Research, 5(Suppl 1): S21–S39. [DOI] [PubMed] [Google Scholar]
- Stokols D et al. (2008a) ‘The Ecology of Team Science: Understanding Contextual Influences on Transdisciplinary Collaboration’, American Journal of Preventive Medicine, 35: S96–S115. [DOI] [PubMed] [Google Scholar]
- Stokols D et al. (2008b) ‘The Science of Team Science: Overview of the Field and Introduction to the Supplement’, American Journal of Preventive Medicine, 35: S77–S89. [DOI] [PubMed] [Google Scholar]
- Stokols D, Hall KL and Vogel AL (2013) ‘Transdisciplinary Public Health: Definitions, Core Characteristics, and Strategies for Success’, in Haire-Joshu D, McBride TD (eds.) Transdisciplinary Public Health: Research, Methods, and Practice, pp. 3–30. San Francisco: Jossey-Bass. [Google Scholar]
- Swinburn BA et al. (2011) ‘The Global Obesity Pandemic: Shaped by Global Drivers and Local Environments’, The Lancet, 378: 804–14. [DOI] [PubMed] [Google Scholar]
- Taplin SH et al. (2012) ‘Introduction: Understanding and Influencing Multilevel Factors across the Cancer Care Continuum’, Journal of the National Cancer Institute Monographs, 2012: 2–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teddlie C, and Tashakkori A (2003) ‘Major Issues and Controveries in the Use of Mixed Methods in the Social and Behavioral Sciences’, Handbook of Mixed Methods in Social & Behavioral Research, 1: 3–50. [Google Scholar]
- Thompson Klein J (2004) ‘Prospects for Transdisciplinarity’, Futures, 36: 515–26. [Google Scholar]
- Turkkan JS, Kaufman NJ, and Rimer BK (2000) ‘Transdisciplinary Tobacco Use Research Centers: A Model Collaboration between Public and Private Sectors’, Nicotine & Tobacco Research, 2: 9–13. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services (2010) How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. [Google Scholar]
- Vogel AL et al. (2012) ‘Influence of a National Cancer Institute Transdisciplinary Research and Training Initiative on Trainees’ Transdisciplinary Research Competencies and Scholarly Productivity’, Translational Behavioral Medicine, 2: 459–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel AL et al. (2013) ‘The Team Science Toolkit: Enhancing Research Collaboration through Online Knowledge Sharing’, American Journal of Preventive Medicine, 45: 787–9. [DOI] [PubMed] [Google Scholar]
- Vogel AL et al. (2014) ‘Pioneering the Transdisciplinary Team Science Approach: Lessons Learned from National Cancer Institute Grantees’, Journal of Translational Medicine & Epidemiology, 2(2). [PMC free article] [PubMed] [Google Scholar]
- Walter AI et al. (2007) ‘Measuring Societal Effects of Transdisciplinary Research Projects: Design and Application of an Evaluation Method’, Evaluation and Program Planning, 30: 325–38. [DOI] [PubMed] [Google Scholar]
- Warnecke RB et al. (2008) ‘Approaching Health Disparities from a Population Perspective: The National Institutes of Health Centers for Population Health and Health Disparities’, American Journal of Public Health, 98: 1608–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wooley SC, and Garner DM (1994) ‘Dietary Treatments for Obesity Are Ineffective’, British Medical Journal, 309: 655. [DOI] [PMC free article] [PubMed] [Google Scholar]