

ABSTRACT
Objectives:
The aim of this article is to establish a comprehensive nation-wide prevalence of malocclusion traits on the sagittal, vertical, and transverse planes of space in Saudi Arabia.
Materials and Methods:
A systematic search was conducted in three databases (Medline via PubMed, Embase, and Web of Science) and complemented with a manual search of Google Scholar and the reference list of included studies. Original studies of Saudi Arabian healthy individuals at any age were included. The quality and the risk of bias of the included studies were assessed using the Joanna Briggs Institute’s appraisal tool. The data about the selected malocclusion traits on the sagittal, vertical, and transverse planes of space were extracted and pooled.
Results:
Out of 7163 identified titles, 11 studies were finally included. The risk of bias was high in two studies, moderate in eight studies, and low in one study. The studied age groups were from early childhood to late adulthood, with a total sample size of 19,169 participants. The majority of the studies recruited their sample from school/public sources, whereas the remaining three studies recruited their sample from dental (non-orthodontic) clinics.
Conclusions:
Within the limitations of this study, pooled prevalence of Angle’s Class I molar relation in Saudi Arabia was similar to other populations but Angle’s Class II and Class III molar relations were lower and higher, respectively. These differences could be attributed to population-related differences in craniofacial morphology. Teeth crowding, teeth spacing, and midline shift, along with increased overjet and overbite, were among the most common malocclusion traits occurring in Saudi Arabia.
KEYWORDS: Epidemiology, humans, malocclusion, overbite, prevalence, tooth
INTRODUCTION
Teeth misalignment (i.e., malocclusion) is a common dental abnormality that may deteriorate the occlusal harmony. The causes of malocclusion could be a complex mix of etiological causes, including hereditary and environmental factors (for review, see Fleming et al.[1]). Typically, malocclusion is evaluated within the three dimensions of space. This implies that it could vary in severity between different individuals. Additionally, the prevalence of malocclusion differs between different age groups, countries, and ethnicities. In the USA alone, it is estimated that around 45% of children (8–11 years) and 65% of adults have some form of malocclusion.[2] Whereas approximately 57–59% of the affected individuals require orthodontic treatment.
Indeed, malocclusion can impose different consequences on oral health-related quality of life.[3] Previous investigations elaborated on the impact of malocclusion on the individual’s aesthetic perception,[4,5] functional capability,[6] social,[7] and psychological well-being.[8] In a comprehensive systematic review, Dimberg et al.[9] showed strong evidence of the adverse effects of malocclusion on the oral health-related quality of life, especially on the emotional and social well-being. Therefore, it is necessary to treat individuals with malocclusion to avoid/minimize the associated health aberrations; however, the cost of orthodontic treatment is expensive. Thus, epidemiological assessment of a nation-wide prevalence of malocclusion in a specific country/ethnicity is crucial for research purposes to correlate with other countries/ethnicities. More importantly, knowing the malocclusion prevalence is essential for health providers to estimate the potential number of patients, thus preparing and allocating the necessary financial budget to cover the treatment costs. As far as the authors are aware, no studies have reported the nation-wide prevalence of malocclusion and other teeth-related anomalies in Saudi Arabia.
Thus, this systematic review was primarily aimed to establish comprehensive nation-wide reference data for the prevalence of different malocclusion traits in Saudi Arabia and pinpoint, if applicable, the age- and sex-related changes in the prevalence of malocclusion traits.
MATERIALS AND METHODS
The protocol for this systematic review was registered a priori in the Open Science Framework repository (https://osf.io/vjurk/) and adhered to the PRISMA-P (2021) guidelines.[10]
SEARCH STRATEGY
A systematic search was conducted from inception till July 1, 2020, in three databases [Medline (PubMed), Embase, and Web of Science Core Collection). The search strategy was built using relevant free-text terms and MeSH/Emtree terms extracted from relevant studies using PubReminer. The terms were, if appropriate, truncated/combined with proximity operators. Table 1 shows the implemented database search strategy. The database search was complemented with a manual search in Google Scholar and the forward/backward citation of the included studies. Major Saudi dental journals were also searched manually for any eligible studies. The included studies must be original and written in English, performed in non-orthodontic clinics, had a healthy Saudi Arabian population, and investigated any of the malocclusion categories of interest [Table 2]. The PECO question was: Population, non-orthodontic Saudi Arabian individuals at any age recruited in dental clinics or schools; Exposure, clinical assessment of selected malocclusion traits; Comparison, not applicable; Outcome, prevalence of the malocclusion traits.
Table 1.
The search strategy implemented in Medline (PubMed), Embase, and Web of Science Core Collection databases
| No. | Query | Results |
|---|---|---|
| Medline via PubMed | ||
| 1 | (prevalence[MeSH Terms]) OR prevalence[Title/Abstract] | 696,024 |
| 2 | (malocclusion[MeSH Terms]) OR Malocclusion[Title/Abstract] | 36,050 |
| 3 | (((overbite[Title/Abstract] OR overjet[Title/Abstract] OR displacement[Title/Abstract] OR Spacing[Title/Abstract] OR crowding[Title/Abstract] OR open bite[Title/Abstract] OR crossbite[Title/Abstract] OR scissors bite).[Title/Abstract])) OR Malocclusion, Angle Class[Title/Abstract] | 37,820 |
| 4 | (((malocclusion[MeSH Terms]) OR Malocclusion[Title/Abstract])) OR ((((overbite[Title/Abstract] OR overjet[Title/Abstract] OR displacement[Title/Abstract] OR Spacing[Title/Abstract] OR crowding[Title/Abstract] OR open bite[Title/Abstract] OR crossbite[Title/Abstract] OR scissors bite).[Title/Abstract])) OR Malocclusion, Angle Class[Title/Abstract]) | 67,666 |
| 5 | (((((malocclusion[MeSH Terms]) OR Malocclusion[Title/Abstract])) OR ((((overbite[Title/Abstract] OR overjet[Title/Abstract] OR displacement[Title/Abstract] OR Spacing[Title/Abstract] OR crowding[Title/Abstract] OR open bite[Title/Abstract] OR crossbite[Title/Abstract] OR scissors bite).[Title/Abstract])) OR Malocclusion, Angle Class[Title/Abstract]))) AND ((prevalence[MeSH Terms]) OR prevalence[Title/Abstract]) | 2,498 |
| Embase | ||
| 1 | “prevalence”/exp OR “prevalence” | 1,051,315 |
| 2 | “malocclusion”/exp OR “malocclusion” | 34,247 |
| 3 | “overbite” OR “overjet” OR “displacement” OR “spacing” OR “crowding” OR “open bite” OR “crossbite” OR “scissors bite” OR “angle class” | 44,606 |
| 4 | (“malocclusion”/exp OR “malocclusion”) OR (“overbite” OR “overjet” OR “displacement” OR “spacing” OR “crowding” OR “open bite” OR “crossbite” OR “scissors bite” OR “angle class”) | 71,909 |
| 5 | (“prevalence”/exp OR “prevalence”) AND ((“malocclusion”/exp OR “malocclusion”) OR (“overbite” OR “overjet” OR “displacement” OR “spacing” OR “crowding” OR “open bite” OR “crossbite” OR “scissors bite” OR “angle class”)) | 3,054 |
| Web of Science Core Collection | ||
| TI=(malocclusion OR (crowd* or bite or tooth or teeth)) AND TI=(prevalence OR epidemiology OR distribution) Indexes=SCI-EXP`ANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, ESCI Timespan=All years | 1,593 | |
Table 2.
Included malocclusion categories/traits on the sagittal, vertical, and transverse planes as well as tooth space-related traits
| Malocclusion category | Included malocclusion traits |
|---|---|
| Traits in the sagittal plane | Primary and permanent molar relations, British Standards incisor classifications, anterior crossbite, and anterior overjet |
| Traits in the vertical plane | Anterior overbite and anterior and lateral open bite |
| Traits in the transverse plane | Buccal crossbite, scissors bite, midline shift, and diastema |
| Tooth space-related traits | Teeth crowding and spacing |
STUDY SELECTION
The database search result was exported to EndNote, where duplicates were removed by the built-in feature and manually checked for accuracy. The de-duplicated studies’ final list was then exported to Microsoft Excel, where the two authors independently screened the articles using a specific excel template. The screened studies were classified based on the titles and abstracts into either included, excluded, or undecided. Indecision in including any study was resolved by a mutual discussion, and exclusion of any study was based on a clearly stated reason. The full texts of the remaining undecided and potentially eligible studies were then carefully read. Studies that satisfy the inclusion criteria were included in the review. Again, any indecisions were resolved by a mutual discussion.
QUALITY ASSESSMENT AND DATA EXTRACTION
The Joanna Briggs Institute’s critical appraisal checklist for prevalence studies was used to assess the trustworthiness, relevance, and results of the included studies.[11] Two questions were removed from the original tool as they did not apply to the included studies. Each question was answered with one of the three options: yes, no, or unclear. One mark was given to each question answered with only “yes.” Thus, the sum of all “yes” answers for each study was counted. Based on the sum score, the quality of the studies was classified into low quality (a score <4), moderate quality (a score between 6 and 4), or high quality (full mark; 8 points score). The authors independently conducted the quality assessment, and any disagreements were resolved by a mutual discussion. Note that no study was excluded based on the used quality tool. The data obtained from the included studies were: author and date of publication, sample size, gender distribution, population age, population source, recorded malocclusion traits, and method of examination. The total sum of cases reported in each study for a particular malocclusion trait was divided by the total sample into those studies to obtain a pooled prevalence for this specific trait.
RESULTS
SEARCH STRATEGY AND STUDY QUALITY
The search strategy yielded 7163 studies. After the de-duplication process and the screening of the title/abstract of the included studies, 63 studies remained for the eligibility process in addition to 18 studies that were identified through the manual search. Further, the full texts of the 81 studies were carefully read, and a final list of 11 studies was deemed eligible for inclusion in the review [Figure 1].[12,13,14,15,16,17,18,19,20,21,22] Based on the critical appraisal tool [Table 3], one study was of low risk of bias,[18] eight studies showed a moderate risk of bias,[13,14,15,16,19,20,21,22] and two studies showed a high risk of bias.[12,17] Although most of the studies may have a sufficient sample size, they lack a power analysis to verify their sample size selection.
Figure 1.

PRISMA flowchart illustrates the included studies’ systematic screening/selection process
Table 3.
Quality assessment of the included studies using an adapted version of the JBI critical appraisal checklist
| Question | Farsi and Salama (1996) | Asiry (2015) | Wyne et al. (2001) | Murshid et al. (2010) | Alamoudi (1999) | Ghaznawi et al. (1999) | Alajlan et al. (2019) | Gudipaneni et al. (2018) | Zakirulla (2012) | Alogaibi et al. (2020) | Asiry and AlShahrani (2019) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Was the sample frame appropriate to address the target population? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes |
| Were study participants sampled in an appropriate way? | Yes | Yes | No | Yes | Yes | No | Unclear | Yes | Unclear | Unclear | Yes |
| Was the sample size adequate? | No | No | No | No | No | No | Yes | Yes | No | Yes | Yes |
| Were the study subjects and the setting described in detail? | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No | No | No |
| Were valid methods used for the identification of the condition? | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes |
| Was the condition measured in a standard, reliable way for all participants? | Yes | Yes | No | Yes | Yes | Yes | No | Yes | No | Yes | No |
| Was there appropriate statistical analysis? | Yes | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | No | Yes | Yes |
| Risk of bias | Moderate | Moderate | High | Moderate | Moderate | Moderate | Moderate | Low | High | Moderate | Moderate |
STUDY CHARACTERISTICS
The included studies had diverse age groups ranging from 3 to 5 years to late adulthood, with a total sample size of 19,169 participants. The majority of the studies recruited their sample from school/public sources,[12,13,14,15,16,19,20,21] whereas the remaining three studies recruited their sample from dental (non-orthodontic) clinics.[17,18,22]Table 4 presents a detailed summary of the main characteristics of each included study.
Table 4.
Main characteristics of the included studies
| Study | Year | Sample size; gender | Age (years) | Sample source | Malocclusion traits, n of cases | Defined I/E criteria | Exam method | Study quality |
|---|---|---|---|---|---|---|---|---|
| Alamoudi (1999) | 1990 | 502; 244 F: 258 M | 4–6 | School | V: LOB = 1; T: MS = 2, SB = 1; O: CR = 94 |
Yes | Clinical | Moderate |
| Farsi and Salama (1996) | 1996 | 520; NA | 3–5 | School | S: MR (Cl 1 = 416, Cl 2 = 42, Cl 3 = 62), IR (Cl 1 = 445, Cl 2 = 57, Cl 3 = 18), OJ (0–1 mm = 283, 2–3 mm = 172, ≥4 mm = 65), ACB = 15; V: OVB (0–4 mm = 295, >4 mm = 140), AOB = 85; T: BCB = 21, SB = 1 |
Yes | Clinical | Moderate |
| Ghaznawi et al. (1999) | 1999 | 1010; 478 F: 532 M | 12–40 | Dental clinic | T: DT = 45 | — | Clinical and X-ray | Moderate |
| Wyne et al. (2001) | 2001 | Primary dentition: 77; 38 F: 39 M Mixed dentition: 76; 9 F: 67 M |
4 ± 1.4 9.7 ± 2.9 |
Public | S: MR (Cl 1 = 151, Cl 2 = 2, Cl 3 = 0), ACB = 1; V: AOB = 1; T: BCB = 1 |
— | Clinical | Low |
| Murshid et al. (2010) | 2010 | 1024; 416 F: 608 M | 13–15 | School | S: MR (Cl 1 = 92, Cl 2 = 214, Cl 3 = 140), OJ (>4 mm = 294); V: OVB (>4 mm = 408); T: MS = 246; O: CR = NA |
Yes | Clinical and study casts | Moderate |
| Zakirulla (2012) | 2012 | 700; 294 F: 406 M | 2–6 | Dental clinic | S: MR (Cl 1 =389, Cl 2 = 23, Cl 3 = 288), ACB = 5; V: AOB = 2; O: CR = 42, SP = 565 |
Yes | Clinical | Low |
| Asiry (2015) | 2015 | 1825; 818 F: 1007 M | 12–16 | School | S: MR (Cl 1 = 1097, Cl 2 = 130, Cl 3 = 185), IR (Cl 1 = 988, Cl 2 = 227, Cl 3 = 206), OJ (≤0 mm = 183, 1–3 mm = 1223, 4–6 mm = 278, >6 mm = 22), ACB = 153; V: OVB (1–3 mm = 1398, 4–6 mm = 119, >6 mm = 3); T: BCB = 164; O: CR = 822, SP = 492 |
Yes | Clinical | Moderate |
| Gudipaneni et al. (2018) | 2018 | 500; 223 F: 277 M | 16 ± 1 | Dental clinic | S: MR (Cl 1 = 264, Cl 2 = 159, Cl 3 = 77), OJ (≤0 mm = 57, 2-4 mm = 332, >4mm = 111), ACB = 24; V: OVB (1-2 mm = 61, 2-4 mm = 322, >4 mm = 117), AOB = 23; T: BCB = 47; O: CR = 236, SP = 136 |
Yes | Clinical | High |
| Alajlan et al. (2019) | 2019 | 520; 273 F: 247 M | 7–12 | School | S: MR (Cl 1 = 366, Cl 2 = 111, Cl 3 = 43), IR (Cl 1 = 377, Cl 2 = 103, Cl 3 = 40), OJ (≤0 mm = 49, 0–4 mm = 396, >4 mm = 75), ACB = 27; V: OVB (2–4 mm = 436, 4–7 mm = 57, >8 mm = 27), AOB = 40, LOB = 3; T: BCB = 69, SB = 21 |
Yes | Clinical | Moderate |
| Asiry and AlShahrani (2019) | 2019 | 1998; 1000 F: 998 M | 14.13 ± 0.99 | School | S: MR (Cl 1 = 1219, Cl 2 = 326, Cl 3 = 154), IR (Cl 1 = 1255, Cl 2 = 231, Cl 3 = 112), OJ (≤0 mm = 94, 1–3 mm = 1515, 4–6 mm = 328, >6 mm = 61), ACB = 109; V: OVB (1–3 mm = 1490, 4–6 mm = 321, >6 mm = 65), AOB (1–3 mm = 99, 4–6 mm = 20, >6 mm = 3); T: BCB = 169, SB = 21; O: CR = 532, SP = 411 |
Yes | Clinical | Moderate |
| Alogaibi et al. (2020) | 2020 | 3016; 1507 F: 1509 M | 14–18 | School | S: MR (Cl 1 = 1718, Cl 2 = 510, Cl 3 = 422), OJ (≤0 mm = 114, 0–4 mm = 2400, 4–6 mm = 430, >6 mm = 72); ACB = 178; V: OVB (0–4 mm = 1857, 4–6 mm = 805, >6 mm = 46), AOB (4–6 mm = 181, >6 mm = 127); T: MS = 1571, BCB =764, SB = 47; O: CR = NA, SP = 795 |
Yes | Clinical | Moderate |
ACB = anterior crossbite; AOB = anterior open bite; BCB = buccal crossbite; Cl = molar/incisor classification; CR = crowding; DT = diastema; F = female; IR = incisal relation; LOB = lateral open bite; MR = molar relation; MS = midline shift; n = number; NA = not applicable; O = tooth space malocclusion traits; OJ = overjet; OVB = overbite; S = sagittal; SB = scissors bite; SP = spacing; T = transverse; V = vertical
PREVALENCE PER MALOCCLUSION TRAIT
The malocclusion traits obtained from the included studies in the sagittal, vertical, and transverse dimensions and other traits related to tooth space are summarized subsequently.
MOLAR AND INCISOR RELATIONS
The pooled prevalence of Angle’s classifications in Saudi Arabia was 69.66% for Class I, 17.84% for Class II, and 12.5% for Class III classifications [Figure 2].[12,13,15,16,17,18,19,20,21] Among the studies, conflicting results were reported on the sex differences in the three Angle’s classifications.[16,19,20,21] In contrast, the majority of the children in the primary dentition had a flush-terminal molar relation (69.63%),[12,13,17] followed by mesial-step (25.49%) and distal-step molar relations (4.88%).
Figure 2.
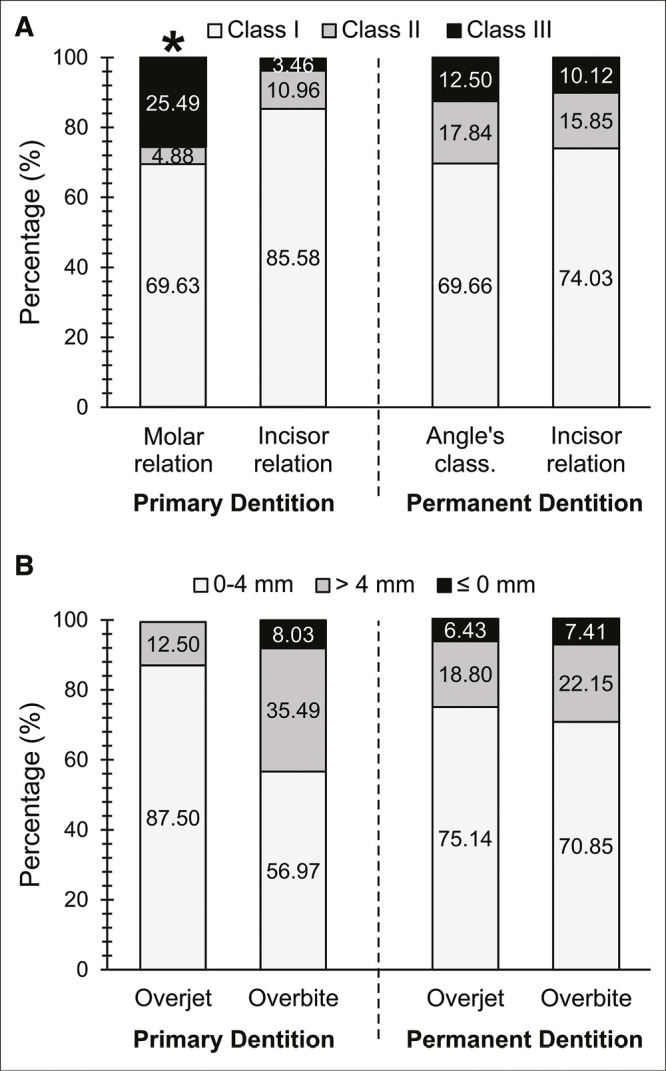
(A) The pooled prevalence of molar and incisor relations and (B) the pooled prevalence of overjet and overbite classifications during primary and permanent dentitions. *Charts represent the molar relationship in the primary dentition, which were classified as follows: flush-terminal (light gray), distal-step (dark gray), and mesial-step (black) relations
In a close relationship to the pooled Angle’s classifications, the British Standards incisor classifications in the permanent dentition were reported in 74.03%, 15.9%, and 10.12%, for Classes I, II, and III, respectively.[15,19,21] It was observed that Class I incisor relation was higher in children with primary dentition (85.6%) when compared with permanent dentition.[13] An opposite trend was observed for Class II and Class III incisor relations (11% and 3.5%, respectively).[13]
OVERJET
The anterior–posterior relationship of anterior maxillary teeth to the mandibular anterior teeth (i.e., overjet) obtained from the studies was categorized into three main classifications of overjet: normal overjet (0–4 mm), increased overjet (˃4 mm), and reduced overjet (≤0 mm). The majority of the studied individuals in the permanent dentition had normal overjet (75.14%), whereas increased overjet of more than 4 mm was found in 18.8% of the individuals.[13,15,16,18,19,20,21,23] However, a lower prevalence was reported for the reduced overjet (≤0 mm) of about 6.43% [Figure 2]. The prevalence of the different overjet classes in children with primary dentition was reported in only one study.[13] The majority of the studied 520 children had normal overjet (87.5%), whereas increased overjet was reported in 12.5% of the studied children, and none was reported to have a reduced overjet. Only two studies have reported the sex differences in the different classes of overjet.[19,20] One study showed that males commonly have normal overjet, whereas females commonly have increased overjet but with no sex differences for the reduced overjet.[19] Another study reported male predominance for increased overjet than females.[20]
ANTERIOR CROSSBITE
Anterior crossbite can be defined as the lingual positioning of one or more maxillary anterior teeth in relation to the mandibular teeth. The pooled prevalence of anterior crossbite in the permanent dentition was 6.25% [Figure 3].[12,13,15,17,18,19,20,21] However, the prevalence was lower for children with primary dentition (1.09%).[12,13,17] The sex difference on anterior crossbite was reported in two studies, in which they showed males were more commonly affected than females.[19,20]
Figure 3.
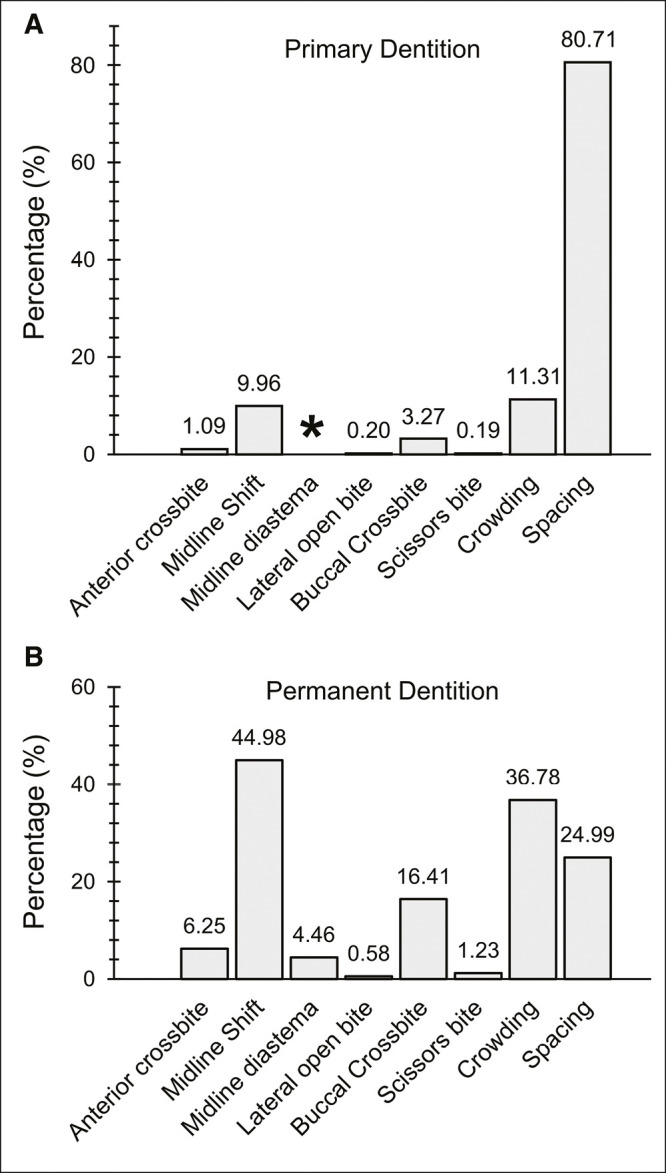
The pooled prevalence of anterior crossbite, transverse, vertical, and tooth space-related malocclusion traits across Saudi Arabia during primary (A) and permanent (B) dentitions. *No data were reported concerning midline diastema in the primary dentition
OVERBITE
The included studies varied a lot in their overbite classifications. Thus an effort was made to categorize them into a generalizable classification: normal overbite between 0 and 4 mm, an excessive bite of more than 4 mm (i.e., deep bite), or reduced overbite of equal to or less than 0 mm.[12,13,15,16,17,18,19,20,21] The pooled prevalence of overbite in the permanent dentition was similar to the pooled prevalence of overjet. The normal overbite was present in 70.85% of the pooled individuals, whereas 22.15% of them had an excessive bite (> 4 mm), and the remaining 7.41% had a reduced overbite [Figure 2]. For children in the primary dentition, it was observed that 56.97% of them had a normal overbite, 35.49% had an excessive overbite, and the remaining 8.03% had a reduced overbite.[12,13,17] Further, no sex differences were reported for any of the different overbite classifications.
LATERAL OPEN BITE
The pooled prevalence of the lateral open bite in the permanent dentition was 0.58% [Figure 3].[14,19] A much lower prevalence was reported for the children in the primary dentition (0.2%).[14] However, no sex differences were reported for the prevalence of lateral open bite.
MIDLINE SHIFT
The pooled prevalence of the midline shift in the permanent dentition across Saudi Arabia was 44.98% [Figure 3].[14,16,20] However, the prevalence of the midline shift in children with primary dentition was only 9.96%.[14] This anomaly was more prevalent in the mandibular arch (41.49%) than the maxillary arch.[20] Conflicting results concerning the sex differences in midline shift prevalence were reported in the included studies. Whereas two studies reported that females were more likely to have a midline shift than males,[14,16] one study reported an opposite trend of males being more affected than females.[20]
MIDLINE DIASTEMA
Only one study reported the prevalence of midline diastema in Saudi Arabia[22] (4.46%) [Figure 3]. This malocclusion trait was reported to occur in both sexes equally.[22]
BUCCAL CROSSBITE
Buccal crossbite occurs when the buccal cusp of one or more of the maxillary posterior teeth occludes lingually to the buccal cusp of the opposing mandibular posterior teeth.[24] The pooled prevalence of buccal crossbite in the permanent dentition across Saudi Arabia was 16.41% [Figure 3].[12,13,15,18,19,20,21] In contrast, the pooled prevalence of buccal crossbite in children with primary dentition was 3.27%.[12,13] Unilateral buccal crossbite affected almost three quarters of the individuals with buccal crossbite (73.45%), whereas bilateral buccal crossbite constitutes the remaining cases (26.55%). Further, females were reported to be more likely to have buccal crossbite than males.[19,20]
SCISSORS BITE
The pooled prevalence of scissors bite in the mixed/permanent dentition was 1.23% [Figure 3].[13,14,19,20,21] However, it was pretty rare in children with primary dentition (0.19%; pooled).[13,14] Whereas one study reported females to be more likely to have scissors bite than males,[19] another study reported an opposite trend of males being more affected than females.[20]
TEETH CROWDING (MORE THAN 2 MM)
The pooled prevalence of teeth crowding in the permanent dentition across Saudi Arabia was 36.78% [Figure 3],[14,15,16,17,18,20,21] approximately three times higher than what is reported for children with primary dentition (11.31%; pooled).[14,17] Overall, the teeth crowding prevalence was equally present in the maxillary and mandibular arches (48.3% and 51.7%, respectively). Moreover, conflicting results were presented about the sex differences in the prevalence of teeth crowding. One study found an equal sex predisposition to teeth crowding,[17] whereas one study showed males to be affected with teeth crowding than females,[20] another found that females were likely to be affected than males.[16]
TEETH SPACING
The pooled prevalence of permanent teeth spacing was 24.99% [Figure 3].[15,17,18,20,21] It was majorly present in the maxillary arch (63.68%) than in the mandibular arch. Teeth spacing was normally present in 80.71% of the children with primary dentition.[17] None of the studies reported any sex differences in teeth spacing.
DISCUSSION
Malocclusion could impose hazardous implications on people’s psychosocial well-being[9] and oral functional capabilities.[6] Therefore, assessing the malocclusion prevalence is essential to plan and prioritize the financial budget and skillful human resources to overcome the associated health aberrations. As no studies have reported the nation-wide prevalence of malocclusion and other teeth-related anomalies in Saudi Arabia, the current comprehensive systematic review adds essential knowledge on the topic. It was concluded from the pooled data that a larger percentage of the included samples was affected by different forms of malocclusion traits. As such, Class I malocclusion was shown to affect approximately 70% of the individuals, followed by midline shift (45%), teeth crowding (36.8%), and teeth spacing (25%).
The pooled prevalence of Class I and Class II Angle’s classifications obtained from the included studies was comparable to other studies.[25,26,27,28] The pooled prevalence of Angle’s Class III classification in Saudi Arabia was considerably high. A significant association was reported previously between the etiology of malocclusion and genetic predisposition and environmental factors.[1] Indeed, the significantly higher prevalence of Class III malocclusion in Saudi Arabia than other populations could be attributed to the ethnic differences in craniofacial morphology.[29] Moreover, the higher Class III malocclusion prevalence in Saudi Arabia could be related to methodological variations such as the included samples’ age and size.
In the current review, the increased overjet prevalence was closely related to the prevalence of Angle’s Class II molar relation. Similarly, a lesser relation was observed between the decreased overjet and the pooled prevalence of Angle’s Class III molar relation. This indicates that when there is a discrepancy between the maxillary and mandibular jaws, this results in a discrepancy in teeth relationship, resulting in an increased or decreased overjet, respectively. However, the teeth can compensate for such skeletal discrepancy, often observed in Class III patients, which may mask the extent of the overjet.
Teeth spacing in the permanent dentition was also among the common types of malocclusion traits. The presence of teeth spacing in the primary dentition is a preferable prerequisite for a favorable permanent teeth eruption and alignment.[24] In the current review, teeth spacing was normally present in 80.71% of the children with primary teeth. However, it affected approximately 25% of the pooled individuals with permanent dentition, which agrees with other studies.[30,31] In contrast, when there is a lack of space in the arch, teeth crowding is an inevitable sequela.[24] In the current study, anterior teeth crowding was observed to affect approximately one-tenth of the pooled children with primary dentition, which worsens with age to affect more than one-third of the pooled individuals in the mixed/permanent dentitions, which is in agreement with previous studies.[2,32] Several reasons can explain the increased prevalence of teeth crowding during permanent dentition. During early childhood, primary dentition acts as natural space maintainers to the erupting permanent teeth. However, when the primary teeth are lost immaturely or persist until the permanent teeth eruption, this will eventually displace the erupting permanent teeth causing teeth crowding.[24] During adulthood, in addition to variations in tooth/arch size discrepancy, the permanent teeth mesially drift with aging, which may lead to late anterior teeth crowding.[33] On the contrary, midline shift was observed in the current review to occur in 45% of the cases. Several possible causes of midline shift have been reported in the literature. Functional lateral shift of the mandible, anterior teeth crowding, asymmetric morphology of anterior teeth, or combinations of these factors were proposed to lead to midline shift.[34]
It should be acknowledged that there are known methodological limitations that commonly contaminate studies of malocclusion prevalence. These include differences in participant’s age and number, sample recruitment source, and malocclusion trait registration method.[35] Conducting studies on gender-specific samples or orthodontic patients may not reflect the actual prevalence of malocclusion for a given community as they are more likely to overestimate the presence of malocclusion, thus weakening the data’s generalizability. In the current review, a rigorous screening process was implemented. Studies of orthodontic patients or gender-specific samples were excluded. Further, studies of malocclusion prevalence should acknowledge that different types of malocclusions are transitionary and may be resolved or even worsen with age. A clear example of such traits is the presence of midline diastema on the ugly-duckling stage of dentition, where the diastema may resolve with the help of the eruption of permanent canines. Therefore, a careful selection of a target age group is needed to avoid under- or over-representing any malocclusion trait. Thus, to minimize any unintentional biases in pooling the data, a cautious scrutinization process of the included studies was implemented.
CONCLUSION
Similar to other populations, Angle’s Class I molar relation was commonly observed in Saudi Arabia. In contrast, Angle’s Class II molar relation was lower, whereas Angle’s Class III molar relation was considerably higher than other populations, which could be attributed to population-related differences in craniofacial morphology. Teeth crowding, teeth spacing, midline shift, and increased overjet and overbite were the most common traits of malocclusion occurring in Saudi Arabia. Limited gender differences were displayed on the selected malocclusion traits.
ACKNOWLEDGEMENTS
The researchers would like to thank the Deanship of Scientific Research, Qassim University, Saudi Arabia for the support of this project. Protocol registration url: https://osf.io/vjurk/.
FINANCIAL SUPPORT AND SPONSORSHIP
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
CONFLICTS OF INTEREST
All authors declare that there are no conflicts of interest.
AUTHORS’ CONTRIBUTION
NA: conceptualization, methodology, validation, formal analysis, investigation, visualization, data curation, writing—review and editing, supervision, project administration. FA: methodology, validation, data curation, writing—original draft.
ETHICAL POLICY AND INSTITUTIONAL REVIEW BOARD STATEMENT
Not applicable.
PATIENT DECLARATION OF CONSENT
Not applicable.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- 1.Fleming PS, DiBiase AT, Cobourne MT. The aetiology of malocclusion: A contemporary view. Orthod Updat. 2008;1:16–21. [Google Scholar]
- 2.Proffit WR, Fields HW, Jr, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97–106. [PubMed] [Google Scholar]
- 3.Liu Z, McGrath C, Hägg U. The impact of malocclusion/orthodontic treatment need on the quality of life. A systematic review. Angle Orthod. 2009;79:585–91. doi: 10.2319/042108-224.1. [DOI] [PubMed] [Google Scholar]
- 4.Van der Geld P, Oosterveld P, Van Heck G, Kuijpers-Jagtman AM. Smile attractiveness. Self-perception and influence on personality. Angle Orthod. 2007;77:759–65. doi: 10.2319/082606-349. [DOI] [PubMed] [Google Scholar]
- 5.Janson G, Branco NC, Fernandes TM, Sathler R, Garib D, Lauris JR. Influence of orthodontic treatment, midline position, buccal corridor and smile arc on smile attractiveness. Angle Orthod. 2011;81:153–61. doi: 10.2319/040710-195.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Magalhães IB, Pereira LJ, Marques LS, Gameiro GH. The influence of malocclusion on masticatory performance. A systematic review. Angle Orthod. 2010;80:981–7. doi: 10.2319/011910-33.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Henson ST, Lindauer SJ, Gardner WG, Shroff B, Tufekci E, Best AM. Influence of dental esthetics on social perceptions of adolescents judged by peers. Am J Orthod Dentofacial Orthop. 2011;140:389–95. doi: 10.1016/j.ajodo.2010.07.026. [DOI] [PubMed] [Google Scholar]
- 8.de Paula Júnior DF, Santos NC, da Silva ET, Nunes MF, Leles CR. Psychosocial impact of dental esthetics on quality of life in adolescents. Angle Orthod. 2009;79:1188–93. doi: 10.2319/082608-452R.1. [DOI] [PubMed] [Google Scholar]
- 9.Dimberg L, Arnrup K, Bondemark L. The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur J Orthod. 2015;37:238–47. doi: 10.1093/ejo/cju046. [DOI] [PubMed] [Google Scholar]
- 10.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br Med J. 2022;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015;13:147–53. doi: 10.1097/XEB.0000000000000054. [DOI] [PubMed] [Google Scholar]
- 12.Wyne A, Al-Dlaigan Y, Khan N. Caries prevalence, oral hygiene and orthodontic status of Saudi Bedouin children. Indian J Dent Res. 2001;12:194–8. [PubMed] [Google Scholar]
- 13.Farsi NM, Salama FS. Characteristics of primary dentition occlusion in a group of Saudi children. Int J Paediatr Dent. 1996;6:253–9. doi: 10.1111/j.1365-263x.1996.tb00254.x. [DOI] [PubMed] [Google Scholar]
- 14.Alamoudi N. The prevalence of crowding, attrition, midline discrepancies and premature tooth loss in the primary dentition of children in Jeddah, Saudi Arabia. J Clin Pediatr Dent. 1999;24:53–8. [PubMed] [Google Scholar]
- 15.Asiry MA. Occlusal status among 12–16 year-old school children in Riyadh, Saudi Arabia. J Int Oral Health. 2015;7:20–3. [PMC free article] [PubMed] [Google Scholar]
- 16.Murshid ZA, Amin HE, Al-Nowaiser AM. Distribution of certain types of occlusal anomalies among Saudi Arabian adolescents in Jeddah city. Community Dent Health. 2010;27:238–41. [PubMed] [Google Scholar]
- 17.Zakirulla M. Malocclusion in deciduous dentition of Saudi children: A cross-sectional study. Bang J Med Sci. 2012;11:343–6. [Google Scholar]
- 18.Gudipaneni RK, Aldahmeshi RF, Patil SR, Alam MK. The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the Northern border region of Saudi Arabia: An epidemiological study. BMC Oral Health. 2018;18:16. doi: 10.1186/s12903-018-0476-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Alajlan SS, Alsaleh MK, Alshammari AF, Alharbi SM, Alshammari AK, Alshammari RR. The prevalence of malocclusion and orthodontic treatment need of school children in Northern Saudi Arabia. J Orthod Sci. 2019;8:10. doi: 10.4103/jos.JOS_104_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Alogaibi YA, Murshid ZA, Alsulimani FF, Linjawi AI, Almotairi M, Alghamdi M, et al. Prevalence of malocclusion and orthodontic treatment needs among young adults in Jeddah city. J Orthod Sci. 2020;9:3. doi: 10.4103/jos.JOS_44_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Asiry MA, AlShahrani I. Prevalence of malocclusion among school children of Southern Saudi Arabia. J Orthod Sci. 2019;8:2. doi: 10.4103/jos.JOS_83_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ghaznawi H, Daas H, Salakon O. A clinical and radiographic survey of selected dental anomalies and conditions in a Saudi Arabian population. Saudi Dent J. 1999;11:8–13. [Google Scholar]
- 23.Learreta JA, Moses AJ. Cephalometric variation in patients with and without intraoral neuromuscular repositioning appliance. J Gen Orthod. 1999;10:14–21. [PubMed] [Google Scholar]
- 24.Koch G, Poulsen S, Espelid I, Haubek D. In: Koch G, editor. Wiley-Blackwell; 2017. p. 408. [Google Scholar]
- 25.El-Mangoury NH, Mostafa YA. Epidemiologic panorama of dental occlusion. Angle Orthod. 1990;60:207–14. doi: 10.1043/0003-3219(1990)060<0207:EPODO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Gardiner JH. An orthodontic survey of Libyan schoolchildren. Br J Orthod. 1982;9:59–61. doi: 10.1179/bjo.9.1.59. [DOI] [PubMed] [Google Scholar]
- 27.Onyeaso CO. Prevalence of malocclusion among adolescents in Ibadan, Nigeria. Am J Orthod Dentofacial Orthop. 2004;126:604–7. doi: 10.1016/j.ajodo.2003.07.012. [DOI] [PubMed] [Google Scholar]
- 28.Burgersdijk R, Truin GJ, Frankenmolen F, Kalsbeek H, van’t Hof M, Mulder J. Malocclusion and orthodontic treatment need of 15-74-year-old Dutch adults. Community Dent Oral Epidemiol. 1991;19:64–7. doi: 10.1111/j.1600-0528.1991.tb00111.x. [DOI] [PubMed] [Google Scholar]
- 29.Aldrees AM. Lateral cephalometric norms for Saudi adults: A meta-analysis. Saudi Dent J. 2011;23:3–7. doi: 10.1016/j.sdentj.2010.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Abu Alhaija ES, Al-Khateeb SN, Al-Nimri KS. Prevalence of malocclusion in 13-15 year-old North Jordanian school children. Community Dent Health. 2005;22:266–71. [PubMed] [Google Scholar]
- 31.Gelgör IE, Karaman AI, Ercan E. Prevalence of malocclusion among adolescents in Central Anatolia. Eur J Dent. 2007;1:125–31. [PMC free article] [PubMed] [Google Scholar]
- 32.Dimberg L, Lennartsson B, Arnrup K, Bondemark L. Prevalence and change of malocclusions from primary to early permanent dentition: A longitudinal study. Angle Orthod. 2015;85:728–34. doi: 10.2319/080414-542.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jonsson T, Arnlaugsson S, Saemundsson SR, Magnusson TE. Development of occlusal traits and dental arch space from adolescence to adulthood: A 25-year follow-up study of 245 untreated subjects. Am J Orthod Dentofacial Orthop. 2009;135:456–62. doi: 10.1016/j.ajodo.2007.04.047. [DOI] [PubMed] [Google Scholar]
- 34.Lewis PD. The deviated midline. Am J Orthod. 1976;70:601–16. doi: 10.1016/0002-9416(76)90223-2. [DOI] [PubMed] [Google Scholar]
- 35.Rakhshan V. Meta-analysis and systematic review of factors biasing the observed prevalence of congenitally missing teeth in permanent dentition excluding third molars. Prog Orthod. 2013;14:33. doi: 10.1186/2196-1042-14-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.