

Abstract
In-office needle tendoscopy (IONT) can be used for the diagnosis and treatment of several peroneal tendon pathologies including peroneal tendon tendinopathy, tears, and instability. Benefits of IONT for peroneal tendon disorders include the ability to dynamically evaluate peroneal tendon stability, quicker patient recovery, reduced cost, and improved patient satisfaction. Several studies have suggested that tendoscopic treatment may avoid several complications related to open treatment of peroneal tendon pathologies, including scar formation and groove stenosis. The purpose of the present report is to describe the technique for performing IONT for common peroneal tendon pathologies. This Technical Note describes the techniques for obtaining adequate anesthesia and performing IONT, indications, and advantages of performing these procedures in the office rather than in the operating room.
Technique Video
Operative technique demonstrating needle tendoscopy of the peroneal tendons.
Peroneal tendon pathologies, which include tendinopathies, tears, and instability (i.e., tendon subluxation or dislocation), are increasingly recognized sources of lateral ankle pain and instability but have been underdiagnosed.1 Surgical treatment for peroneal tendon disorders historically involved open exploration of the peroneal tendons, but several authors have recently expressed concerns with the traditional open procedure. These include reported complications such as increased scar formation, adhesions, groove stenosis, sural nerve injury, and prolonged postoperative immobilization, all of which can generate postoperative pain.2,3 Consequently, there has been a recent trend toward the use of peroneal tendoscopy as a less-invasive treatment that may improve outcomes compared to traditional open management of peroneal disorders.4, 5, 6, 7
Although peroneal tendoscopy was traditionally performed in the operating room with the patient under general or regional anesthesia with sedation, this technique is particularly amenable to in-office needle tendoscopy (IONT) for several reasons. IONT allows for dynamic assessment of peroneal tendon instability and live visualization of peroneal tendon sliding within the sheath and groove. Although this can be performed by manually circumducting the ankle during surgery in the sedated patient, it can be valuable to assess peroneal tendon gliding in the awake patient who can perform provocative ankle motions to elicit instability. Given the difficulties of assessing peroneal tendon pathologies and anatomic variants on magnetic resonance imaging (MRI), IONT can also be a valuable adjunct or even cost-saving replacement to MRI for the evaluation of lateral-sided ankle pain or instability.8, 9, 10, 11, 12
Wide-awake local anesthesia no tourniquet (WALANT) surgery is well established in hand surgery and is now becoming increasingly used in foot and ankle surgery; however, the indications and techniques for WALANT in foot and ankle surgery are still being defined.13, 14, 15, 16, 17, 18 The purpose of the present report is to describe the surgical technique for performing IONT with the Arthrex (Naples, Florida, US) Nanoscope nano tendoscopy system for the diagnosis and treatment of common peroneal tendon pathologies. Attention is paid to techniques for obtaining adequate local anesthesia and performing in-office peroneal tendoscopy, indications, and the advantages of performing these procedures in the office rather than the operating room (Video 1).
Surgical technique
Preoperative Planning/Positioning
Before the procedure, the planned distal and proximal lateral portal sites (Fig 1) are injected with 1% lidocaine. After 5 to 10 minutes, the needle is then advanced into the peroneal tendon sheath through the distal portal, and 5 mL of 1:1 ratio 0.5% bupivacaine with epinephrine and 1% lidocaine with epinephrine is injected (Fig 2). The use of epinephrine improves hemostasis and obviates the need for a tourniquet. The “blow slow before you go” technique19 is used wherein the anesthetic is injected slowly, and there is a pause in between injecting the skin and subcutaneous tissue before proceeding deeper. In case a groove deepening is required, an effort is made to inject the periosteum and fibrocartilage of the retrofibular groove and posterior fibula after the initial injection is given. The patient lies on their nonoperative side in the lateral decubitus position so that the lateral side of the operative extremity is facing up. Soft padding is placed beneath the patient’s nonoperative knee for comfort. The surgeon and assistant then don sterile masks, gloves, and gowns, and the patient’s extremity is prepped and draped in the typical sterile fashion.
Fig 1.

The patient is placed in the lateral decubitus position such that the lateral surface of the operative ankle is exposed. This is a lateral surface view of the left ankle. Surface markings are labeled and listed as follows: LM, lateral malleolus; PP, proximal portal; PT, peroneal tendon; SPR, superior peroneal retinaculum; DP, distal portal. The location of portal sites can be adjusted based on the area of pathology.
Fig 2.

This is a lateral surface view of the left ankle. (A) To create the distal portal, a stab is made through the skin with a no. 15 blade. (B) Blunt dissection with a hemostat is used to safely open the portal site. (C) The trocar is inserted into the distal portal site in line with peroneal tendon sheath. You may feel a popping sensation when the peroneal tendon sheath is pierced through with the trocar. The posterolateral fibula cortex can be palpated to help orient the direction of trocar placement. The camera is inserted, and diagnostic tendoscopy can be performed
Portal Placement
A 22-gauge needle is used to identify the peroneal sheath about 1 cm distal to the tip of the lateral malleolus, and 5.0 mL of saline solution is injected into the sheath to confirm correct placement. A 2 mm skin incision is then made with an 11-blade, and a blunt trocar is then used to enter the peroneal tendon sheath. The camera is exchanged over the trocar and connected to water inflow, typically at a pressure of 20 mm Hg (Fig 2).
Operative Technique
A diagnostic tendoscopy is performed on all 3 zones of pathology starting proximally at the musculotendinous junction where the muscle belly of the peroneus brevis along with the peroneus longus tendon can both be visualized, and then proceeding distally into the retrofibular groove (Fig 3, Fig 4, Fig 5). The surgeon can passively range the ankle to assess peroneal tendon gliding, and the patient can also be asked to circumduct their ankle or to perform provocative motions to evaluate for tendon instability (Fig 6).
Fig 3.
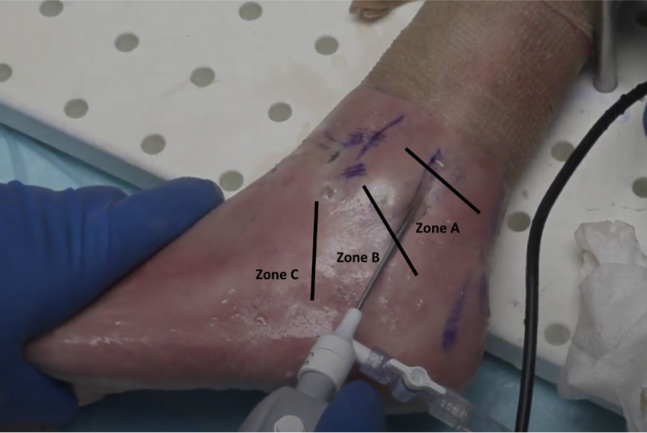
Zones of peroneal tendon pathology. Areas of peroneal tendon pathology are traditionally classified into zones. These zones were initially described by Brandes and Smith for peroneus longus tendinopathies but have since been used to describe both peroneus longus and brevis pathology. Zone A represents the area under the superior peroneal retinaculum, zone B the area under the inferior retinaculum, and zone C the cuboid notch.
Fig 4.

This is a tendoscopic view from the distal tendoscopy portal site on the lateral side of the left ankle. The peroneus brevis tendon can be seen and is recognizable by its relatively flat shape. The retrofibular groove is also visible. In this view, the patient’s ankle can be circumducted to visualize tendon gliding and any evidence of tendon subluxation. The patient may also be instructed to range their ankle to recreate their subjective instability.
Fig 5.

This is a tendoscopic view from the distal tendoscopy portal site of the left ankle. As the camera is pointed slightly more posteriorly, you can visualize the peroneus longus tendon, recognizable by its relatively round shape.
Fig 6.

This is an intraoperative image of a tendoscopic view from the distal portal site of the left ankle. This patient underwent in-office peroneal tendoscopy and fibular groove deepening for peroneal tendon subluxation. The structures visible are the superior peroneal retinaculum, peroneus longus and peroneus brevis tendon. In this patient there is noticeably less space in the peroneal tendon sheath, as well as overcrowding in the retrofibular groove, which are both contributing factors to peroneal tendon instability.
If the decision is made to perform a concomitant therapeutic procedure, a second portal can be made under direct visualization using a 25-gauge needle based on the location of the pathology. This portal is typically at least 3 cm proximal to the distal portal to leave a skin bridge of at least 30 mm. Once the proper portal location is confirmed, an 11-blade is used to make a 2 mm skin incision and then to enter the peroneal tendon sheath, taking care to avoid the peroneal tendons.
A 2.0 mm shaver can be inserted through this proximal portal to debride tendon tears, accessory peroneal muscles or low-lying peroneus brevis muscle belly. Either a 2.0 mm shaver or 3 mm burr can also be used to perform a fibular groove deepening (Fig 7). Other tendoscopic procedures that can be done in the office include superior peroneal retinaculum (SPR) scar resection, excision of a hypertrophic peroneal tubercle, release of the inferior peroneal retinaculum, debridement of calcaneofibular impingement, and debridement of synovitis or adhesions after prior open peroneal tendon surgery. SPR repair can also be achieved with a mini 1 cm incision under tendoscopic visualization. Patients typically feel a sensation of vibration with either the shaver or the burr but do not feel pain as long as adequate time has elapsed between anesthetic injection and beginning the procedure. Additional local anesthesia can also be provided as necessary.
Fig 7.

Example of retrofibular groove deepening. The retrofibular groove (∗) with the peroneus brevis tendon (PB) are shown in (A). An example of tendoscopic groove deepening is shown in (B). Examples of the retrofibular groove after deepening with increased space for tendon gliding is shown in (C), and the groove is shown more clearly in (D) with the tendon retracted.
At the conclusion of the procedure, patients are asked to dorsiflex, plantarflex, and circumduct their ankle to ensure satisfactory tendon gliding and stability. Suction is used to remove any remaining fluid from the ankle joint, and Steri-Strips are used to close the portals. Patients are fully awake during the entire procedure and can view the needle-arthroscopy on the viewing monitor with the surgical team. Patients are encouraged to be actively engaged and ask questions during the procedure. For patients who undergo a peroneal tear debridement, with or without groove deepening, a sterile soft dressing is applied that permits early range of motion. A short leg splint is applied in cases involving soft tissue repair, such as an SPR repair or reconstruction. A step-by-step guide to the performance of this procedure can be found in Table 1.
Table 1.
Step-by-step Guide to Performing In-Office Needle Tendoscopy
| Step 1. Inject proximal and distal tendoscopy portal sites. After 5 to 10 minutes, inject deeper into soft tissues, retrofibular groove and posterior fibula, and any other desired sites (e.g., peroneal tubercle) |
| Step 2. Make 2 mm incision in distal portal. Use blunt trocar to enter peroneal sheath. Before incision, can localize with 25-gauge needle if desired. |
| Step 3. Perform diagnostic tendoscopy, examining all three zones of pathology. Ask patient to perform provocative maneuvers and also manually circumduct ankle to identify instability |
| Step 4. Perform debridement or groove deepening as indicated. Be aware of anatomic variants that can contribute to retrofibular groove overcrowding. Actively engage patient during procedure. |
| Step 5. Ask patient to plantarflex, dorsiflex, and circumduct ankle, and re-examine tendon sliding and stability. |
| Step 6. Apply Steri-Strips for portals and soft dressing or splint as indicated. |
Postoperative Protocol
After surgery, patients advance their weightbearing as tolerated. Formal physical therapy consisting of phased muscle firing, balance, and proprioceptive training is begun immediately, and patients are advanced to sport-specific therapy once they demonstrate competence with the aforementioned early protocol, typically 2 weeks after the procedure. Ice and elevation are encouraged when not ambulating. Pain medication is prescribed for 4 days after the procedure, and patients return on day 5 after the procedure.
Discussion
The use of IONT is particularly suited to the diagnosis and treatment of common peroneal conditions for a variety of reasons. Many of the anatomic variants that can contribute to an overcrowded retrofibular groove and peroneal pathology can be difficult to assess on MRI, and IONT provides clinicians the ability to diagnose these in the office. The use of IONT can also provide a dynamic evaluation of peroneal tendon gliding and stability in addition to being used to assess tear size and intrasheath subluxation. There is a small but growing body of evidence that tendoscopic treatment of peroneal disorders are associated with improved outcomes and quicker recovery compared to their traditional open counterparts.6 We do recommend keeping in mind the advantages, disadvantages and potential downsides when considering needle arthroscopy for a patient (Tables 2 and 3).
Table 2.
Advantages and Disadvantages of the Proposed Technique
| Advantages |
| Dynamic assessment of peroneal tendon gliding |
| Reduced cost and resource utilization |
| Potential for improved patient satisfaction |
| Improved ability to diagnose anatomic variants compared to magnetic resonance imaging |
| Disadvantages |
| More difficult to convert to open procedure |
| Potential for patient pain or discomfort |
| Learning curve |
Table 3.
Pearls and Pitfalls of the Proposed Technique
| Pearls |
| Patient selection is critical |
| When injecting local anesthetic, use “blow slow before you go” technique |
| Encourage patients to ask questions and engage them as active participant during procedure |
| Before making proximal portal, perform full diagnostic tendoscopy. Can place portal more proximal or distal depending on pathology (debriding accessory muscle or tendon tear proximally versus groove deepening distally |
| If needed, can give additional anesthetic to facilitate conversion to open procedure |
| Pitfalls |
| No anesthesia backup available in office (can consider performing in operating room to begin with to have anesthesia available in case general anesthesia induction required) |
| Not giving local anesthetic enough time to work |
| Risk of tissue necrosis with epinephrine (can keep phentolamine available) |
| Failure to fully evaluate for anatomic variants and sources of retrofibular groove overcrowding |
Since it was first described in 1998, the indications for peroneal tendoscopy have expanded significantly in the past few years. The use of IONT has further improved patient satisfaction and outcomes after peroneal tendoscopy while also reducing costs. Although WALANT surgery is well established in hand surgery, there has been a recent trend toward the use of WALANT in other areas, particularly foot and ankle surgery.13, 14, 15, 16, 17, 18 One study examining the use of WALANT in 30 patients who underwent foot and ankle surgery surveyed the patients after surgery and found that 87% would undergo their surgery under WALANT again and would recommend it to someone else.13 Another prospective comparative study of general anesthesia versus WALANT found decreased postoperative pain and improved postoperative patient experience with WALANT compared to general anesthesia.14 There are numerous benefits of WALANT including savings in cost and scarce operating room resources, the ability to avoid preoperative medical clearance, as well as insurance precertification for surgery, and obviating the need for an anesthesiologist.12 The smaller 2 mm incisions also cause less damage to the skin and subcutaneous tissue, which minimizes the potential for bacterial entry and infection.20 Beyond the material benefits, however, a major advantage of wide-awake IONT is the unique opportunity for surgeons to connect with and engage their patients, which can potentially improve patient satisfaction and participation in post-operative rehabilitation. Patients can move their ankle in real time and observe their peroneal tendon gliding smoothly and without subluxation and then be reassured that their tendons are now stable. They can see how their retrofibular groove is less crowded after debridement of an accessory muscle. This could have numerous tangible benefits in the form of increased patient satisfaction, greater compliance increased participation in postoperative rehabilitation, and greater patient involvement in the therapeutic relationship.
We have found that our cohort of patients has been interested in this procedure and have reported that watching the tendoscopy live, being able to ask questions, and being asked to participate by moving their ankle have all been positive experiences for them. Further studies are needed and planned to evaluate clinical outcomes after IONT of the peroneal tendons. Nevertheless, this remains an exciting new development within foot and ankle surgery that could become a significant portion of daily clinical practice which could provide orthopaedic surgeons with a unique opportunity to improve patient satisfaction and build rapport with their patients.
Footnotes
The authors report the following potential conflicts of interest or sources of funding: The authors report the following potential conflicts of interest or sources of funding: J.G.K. received support from the Ohnell Family Foundation and Mr. and Mrs. Michael J. Levitt; he is a consultant for Arteriocyte Industries (Isto Biologics) and Arthrex. J.W.S. reports Arthroscopy Association of North American board or committee membership. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
Operative technique demonstrating needle tendoscopy of the peroneal tendons.
References
- 1.Dombek M.F., Lamm B.M., Saltrick K., Mendicino R.W., Catanzariti A.R. Peroneal tendon tears: A retrospective review. J Foot Ankle Surg. 2003;42:250–258. doi: 10.1016/s1067-2516(03)00314-4. [DOI] [PubMed] [Google Scholar]
- 2.Steel M.W., DeOrio J.K. Peroneal tendon tears: Return to sports after operative treatment. Foot Ankle Int. 2007;28:49–54. doi: 10.3113/FAI.2007.0009. [DOI] [PubMed] [Google Scholar]
- 3.Sammarco G., Mangone P. Diagnosis and treatment of peroneal tendon injuries. Foot Ankle Surg. 2000;6:197–205. [Google Scholar]
- 4.Kennedy J.G., van Dijk P.A., Murawski C.D., Duke G., Newman H., DiGiovanni C.W., et al. Functional outcomes after peroneal tendoscopy in the treatment of peroneal tendon disorders. Knee Surg Sports Traumatol Arthrosc. 2016;24:1148–1154. doi: 10.1007/s00167-016-4012-6. [DOI] [PubMed] [Google Scholar]
- 5.Vega J., Batista J.P., Golanó P., Dalmau A., Viladot R. Tendoscopic groove deepening for chronic subluxation of the peroneal tendons. Foot Ankle Int. 2013;34:832–840. doi: 10.1177/1071100713483098. [DOI] [PubMed] [Google Scholar]
- 6.Nishimura A., Kato K., Nakazora S., Senga Y., Fukuda A., Sudo A. Tendoscopic peroneal retinaculum repair for recurrent peroneal tendon dislocation enables earlier return to sports than the open procedure. Knee Surg Sports Traumatol Arthrosc. 2020;28:3318–3323. doi: 10.1007/s00167-020-05877-x. [DOI] [PubMed] [Google Scholar]
- 7.Stornebrink T., Emanuel K.S., Shimozono Y., Karlsson J., Kennedy J.G., Kerkhoffs G.M. A change in scope: Redefining minimally invasive. Knee Surg Sports Traumatol Arthrosc. 2020;28:3064–3065. doi: 10.1007/s00167-020-05898-6. [DOI] [PubMed] [Google Scholar]
- 8.Park H.J., Cha S.D., Kim H.S., Chung S.T., Park N.H., Yoo J.H., et al. Reliability of MRI findings of peroneal tendinopathy in patients with lateral chronic ankle instability. Clin Orthop Surg. 2010;2:237–243. doi: 10.4055/cios.2010.2.4.237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Adler R.S., Finzel K.C. The complementary roles of MR imaging and ultrasound of tendons. Radiol Clin. 2005;43:771–807. doi: 10.1016/j.rcl.2005.02.011. [DOI] [PubMed] [Google Scholar]
- 10.Giza E., Mak W., Wong S.E., Roper G., Campanelli V., Hunter J.C. A clinical and radiological study of peroneal tendon pathology. Foot Ankle Spec. 2013;6:417–421. doi: 10.1177/1938640013501544. [DOI] [PubMed] [Google Scholar]
- 11.Voigt J.D., Mosier M., Huber B. Diagnostic needle arthroscopy and the economics of improved diagnostic accuracy: A cost analysis. Appl Health Econ Health Policy. 2014;12:523–535. doi: 10.1007/s40258-014-0109-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McMillan S., Schwartz M., Jennings B., Faucett S., Owens T., Ford E. In-office diagnostic needle arthroscopy: Understanding the potential value for the US healthcare system. Am J Orthop. 2017;46:252–256. [PubMed] [Google Scholar]
- 13.MacNeill A.L., Mayich D.J. Wide-awake foot and ankle surgery: A retrospective analysis. Foot Ankle Surg. 2017;23(4):307–310. doi: 10.1016/j.fas.2016.09.004. [DOI] [PubMed] [Google Scholar]
- 14.Wright J., MacNeill A.L., Mayich D.J. A prospective comparison of wide-awake local anesthesia and general anesthesia for forefoot surgery. Foot Ankle Surg. 2019;25:211–214. doi: 10.1016/j.fas.2017.10.015. [DOI] [PubMed] [Google Scholar]
- 15.MacNeill A.L., Wright J., Mayich D.J. Qualitative aspects of patient pain during surgery with wide-awake local anesthesia. J Orthop. 2019;16:105–108. doi: 10.1016/j.jor.2018.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bilgetekin Y.G., Kuzucu Y., Öztürk A., Yüksel S., Atilla H.A., Ersan Ö. The use of the wide-awake local anesthesia no tourniquet technique in foot and ankle injuries. Foot Ankle Surg. 2021;27:535–538. doi: 10.1016/j.fas.2020.07.002. [DOI] [PubMed] [Google Scholar]
- 17.MacNeill A.L., Mayich D.J. A physiological assessment of patient pain during surgery with wide-awake local anesthesia. J Orthop. 2020;19:158–161. doi: 10.1016/j.jor.2019.11.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Turcotte J.J., Petre B.M., Jones C.M., Gelfand J.M. Maintaining access to orthopaedic surgery during periods of operating room resource constraint: Expanded use of wide-awake surgery during the COVID-19 pandemic. J Am Acad Orthop Surg Glob Res Rev. 2020;4(12):e20.00100. doi: 10.5435/JAAOSGlobal-D-20-00100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Strazar A.R., Leynes P.G., Lalonde D.H. Minimizing the pain of local anesthesia injection. Plast Reconstr Surg. 2013;132:675–684. doi: 10.1097/PRS.0b013e31829ad1e2. [DOI] [PubMed] [Google Scholar]
- 20.Zengerink M., van Dijk C.N. Complications in ankle arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2012;20:1420–1431. doi: 10.1007/s00167-012-2063-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Operative technique demonstrating needle tendoscopy of the peroneal tendons.
Operative technique demonstrating needle tendoscopy of the peroneal tendons.