

This secondary analysis of a randomized clinical trial evaluates longitudinal arterial spin labeled data to test the hypothesis that long-term intensive treatment does not reduce cerebral blood flow compared with standard treatment.
Key Points
Question
Is intensive antihypertensive treatment associated with increased risk of cerebral hypoperfusion compared with standard treatment?
Findings
In a magnetic resonance imaging substudy within SPRINT of 547 patients, at 4-year follow-up, an intensive systolic blood pressure target of less than 120 mm Hg was associated with a significantly larger increase in cerebral blood flow compared with a standard blood pressure target of less than 140 mm Hg among adults with hypertension. This association was most pronounced among participants with a history of cardiovascular disease.
Meaning
Compared with a standard blood pressure target, an intensive blood pressure target was associated with increased, rather than decreased, cerebral perfusion in this study.
Abstract
Importance
Antihypertensive treatments benefit cerebrovascular health and cognitive function in patients with hypertension, but it is uncertain whether an intensive blood pressure target leads to potentially harmful cerebral hypoperfusion.
Objective
To investigate the association of intensive systolic blood pressure (SBP) control vs standard control with whole-brain cerebral blood flow (CBF).
Design, Setting, and Participants
This substudy of the Systolic Blood Pressure Intervention Trial (SPRINT) randomized clinical trial compared the efficacy of 2 different blood pressure–lowering strategies with longitudinal brain magnetic resonance imaging (MRI) including arterial spin labeled perfusion imaging to quantify CBF. A total of 1267 adults 50 years or older with hypertension and increased cardiovascular risk but free of diabetes or dementia were screened for the SPRINT substudy from 6 sites in the US. Randomization began in November 2010 with final follow-up MRI in July 2016. Analyses were performed from September 2020 through December 2021.
Interventions
Study participants with baseline CBF measures were randomized to an intensive SBP target less than 120 mm Hg or standard SBP target less than 140 mm Hg.
Main Outcomes and Measures
The primary outcome was change in whole-brain CBF from baseline. Secondary outcomes were change in gray matter, white matter, and periventricular white matter CBF.
Results
Among 547 participants with CBF measured at baseline, the mean (SD) age was 67.5 (8.1) years and 219 (40.0%) were women; 315 completed follow-up MRI at a median (IQR) of 4.0 (3.7-4.1) years after randomization. Mean whole-brain CBF increased from 38.90 to 40.36 (difference, 1.46 [95% CI, 0.08-2.83]) mL/100 g/min in the intensive treatment group, with no mean increase in the standard treatment group (37.96 to 37.12; difference, –0.84 [95% CI, –2.30 to 0.61] mL/100 g/min; between-group difference, 2.30 [95% CI, 0.30-4.30; P = .02]). Gray, white, and periventricular white matter CBF showed similar changes. The association of intensive vs standard treatment with CBF was generally similar across subgroups defined by age, sex, race, chronic kidney disease, SBP, orthostatic hypotension, and frailty, with the exception of an indication of larger mean increases in CBF associated with intensive treatment among participants with a history of cardiovascular disease (interaction P = .05).
Conclusions and Relevance
Intensive vs standard antihypertensive treatment was associated with increased, rather than decreased, cerebral perfusion, most notably in participants with a history of cardiovascular disease.
Trial Registration
ClinicalTrials.gov Identifier: NCT01206062
Introduction
Hypertension is a major risk factor for cardiovascular and cerebrovascular diseases including stroke, small vessel disease, and dementia.1,2,3 While stroke occurs in the setting of acute and severe hypoperfusion, chronic hypoperfusion of lower severity underlies small vessel ischemic disease and contributes to cognitive decline.4,5,6 Antihypertensive therapies to lower elevated blood pressure (BP) are a key management strategy to prevent cardiovascular and cerebrovascular disease, but there is uncertainty concerning the optimal target BP, primarily owing to concerns that aggressive BP reduction could cause organ hypoperfusion, including in the brain.7,8 The Systolic Blood Pressure Intervention Trial (SPRINT) was a multicenter randomized clinical trial comparing intensive BP control, targeting a systolic BP (SBP) less than 120 mm Hg, to a standard treatment target (SBP <140 mm Hg). The trial showed an overall benefit for intensive treatment on cardiovascular morbidity and mortality9 and cerebrovascular health, including a reduced incidence of adjudicated cognitive impairment.3 Additionally, among a subset of trial participants who underwent brain magnetic resonance imaging (MRI), participants randomized to the intensive SBP target had a smaller increase in white matter lesions (WMLs) but greater reduction in total brain volume over approximately a median of 4 years’ follow-up.10
Cerebral blood flow (CBF) is the volume of blood flowing through brain parenchyma per unit time. CBF is relatively stable over a wide range of perfusion pressure changes through the constriction and dilation of blood vessels, a physiological phenomenon known as cerebral autoregulation.11 Below and above this range cerebral autoregulation is thought to fail and expose the brain to ischemia or hypoperfusion injury. Untreated or poorly controlled hypertension shifts the range of CBF autoregulation toward higher BP12 and causes reduced CBF.13,14,15,16 Standard antihypertensive treatments have been shown to lower the autoregulatory BP limits, coupled with increased CBF17,18,19; however, there has been concern that more aggressive treatment may lower BP below the lower autoregulatory limit and lead to cerebral ischemic injury.20 Two prior studies with small sample sizes and short duration (approximately 3 months) suggest a stable CBF in response to intensive treatment (SBP <125 mm Hg),21,22 although long-term effects are unknown.
The MRI substudy in SPRINT included arterial spin labeled (ASL) perfusion MRI, which provides noninvasive quantification of regional CBF, to assess the association of intensive SBP lowering with cerebral perfusion. In this study, we evaluated longitudinal ASL data to test the hypothesis that long-term intensive treatment does not reduce CBF compared with standard treatment.
Methods
Study Participants
The trial design and the primary outcomes have been described previously,3and the trial protocol is available in Supplement 1. Briefly, 9361 participants with hypertension who were 50 years or older with SBP of 130 to 180 mm Hg were randomized in a 1:1 ratio by the SPRINT coordinating center to an SBP goal of less than 120 or less than 140 mm Hg between November 2010 and March 2013. Trial participants were recruited from a variety of clinic settings (eg, primary care, nephrology/hypertension, geriatrics) or from the local community. Participants also had at least 1 risk factor for heart disease: prior cardiovascular disease, chronic kidney disease (defined by estimated glomerular filtration rate of <60 mL/min/1.73 m2), a 10-year Framingham cardiovascular disease risk of 15% or more, or 75 years or older. Individuals with diabetes, with history of stroke, residing in a nursing home, or carrying a diagnosis of dementia or treated with medications primarily used for dementia were excluded. The trial and the MRI substudy were approved by the institutional review board at each study site and each participant provided written informed consent.
Brain MRIs were obtained at 7 MRI sites using 3T scanners (3 Philips and 4 Siemens). Exclusion criteria for the MRI substudy included presence of an implanted electrical device, ferromagnetic or unknown cerebral aneurysm clip, otologic implant, unknown metallic foreign bodies, exposure to metal fragments in or around the eyes, or severe claustrophobia. Of 1267 individuals screened for the MRI substudy, 793 were eligible and 622 had a baseline ASL scan that passed quality control (Figure 1). ASL data from 1 Siemens site were excluded owing to a technical issue at the follow-up scan.
Figure 1. Eligibility, Randomization, and Follow-up for Participants in the Magnetic Resonance Imaging (MRI) Substudy.

The total randomization number indicates the number of participants in the Systolic Blood Pressure Intervention Trial (SPRINT) magnetic resonance imaging substudy who were located in proximity to a study MRI scanner. ASL indicates arterial spin labeling.
MRI Study and Acquisition
Multimodal MRI scans were obtained at baseline and planned at 48 months postrandomization. Each participant was scanned on the same scanner at both time points. The MRI protocol included ASL to measure CBF, fluid-attenuated inversion recovery T2-weighted MRI to measure WML volumes and T1-weighted structural MRI to measure brain volume and segment regions of interest (ROIs). ASL data were obtained using pseudo-continuous labeling with 1.5/1.5-second labeling/postlabeling delay at 90 mm below the center of the imaging volume or 30.5 mm below the inferior slice in Siemens and Philips scanners respectively. Forty label/control image pairs were obtained using 2-dimensional echo-planar imaging with repetition time of 4000 milliseconds; echo time, 11 milliseconds; field of view, 220 mm; and voxel size, 3.4 × 3.4 × 5 mm3 with a 20% distance factor, 20 slices. Fluid-attenuated inversion recovery acquisitions had repetition time/echo time of 6000/285 milliseconds; inversion time, 2200 milliseconds; field of view, 258 mm; slices, 160; and native resolution, 1 mm isotropic. T1-weighted magnetization-prepared rapid acquisition with gradient echo images were obtained using repetition time/echo time of 1900/2.89 milliseconds; field of view, 250 mm; slices, 176; and native resolution, 1 mm isotropic.
MRI Processing
MRI data were processed at the University of Pennsylvania using automated pipelines. All image analysts were blinded to treatment group and other nonimaging study data. ASL data processing pipeline was developed in-house in MATLAB version 2016b (MathWorks) with Statistical Parametric Mapping 12 and FSL following the recommendation by Alsop et al23 and consisted of motion correction of raw label/control time series, CBF quantification using a single compartment model, and subsequent denoising based on a structural correlation with robust bayesian criteria.24,25,26 The quality of the CBF maps for each participant was evaluated using an automated quality evaluation metric,27 which outputs a numerical score with range (0, 1) where higher values indicate a better CBF map. CBF maps with quality evaluation metric less than 0.35, a predefined threshold for global CBF measures, were excluded from the analysis. The remaining CBF maps were coregistered to participants’ T1 space using a transform obtained with a boundary-based approach. Gray matter (GM) and white matter (WM) were segmented from T1-weighted images using a multi-atlas label fusion method,28 with the sum of the 2 tissue types defining the whole brain (WB) ROI. Mean CBF in WB, GM, and WM were extracted and used for analysis. Additionally, we considered the mean CBF in a functionally defined periventricular WM ROI, which was constructed based on subthreshold CBF in a group mean CBF map generated from middle-aged healthy participants in the Coronary Artery Risk Development in Young Adults study.24,29 The periventricular WM ROI is a small portion of the WM ROI that includes the most weakly perfused brain parenchyma supplied exclusively by the terminal distributions of long arterioles less than 100 microns in diameter30 and represents the region where the earliest age-associated WMLs occur.24 WMLs were segmented from fluid-attenuated inversion recovery T2-weighted images using a previously described deep-learning–based segmentation method.31
Clinical Measures
BP measurements were obtained with Professional Digital Blood Pressure Monitor (Omron Healthcare; model 907XL). Visit BP was recorded as the mean of 3 seated measurements after 5-minute rest periods. During the rest and BP measurement periods, participants were prohibited from completing questionnaires, talking, or texting. Blood and urine samples were analyzed at a central laboratory located in Minneapolis, Minnesota.
Duration of Follow-up
On August 20, 2015, based on a recommendation by the data and safety monitoring board to inform the investigators and participants of the favorable cardiovascular outcome results with intensive treatment, the process to end the trial intervention was initiated early. As a result, most of the follow-up MRI scans used in this study (298 [94.6%]) occurred during a closeout period (from August 20, 2015, to July 1, 2016) when the participants were transitioning to having their hypertension managed by their primary care clinician, although the study still provided antihypertensive medications. The median (IQR) interval between August 20, 2015, and the follow-up MRI scans completed during the closeout period was 192 (124-245) days, which was 4.0 (3.7-4.1) years after randomization.
Outcomes
The primary outcome of this substudy was the change in mean WB CBF from baseline to follow-up. Secondary outcomes included the mean CBF in GM, WM, and the periventricular WM.
Subgroups of Interest
Prespecified subgroups for the trial’s primary outcomes included age (<75 years vs ≥75 years), sex, race (not Black [ie, those who reported being American Indian/Alaskan Native; Asian; Native Hawaiian/Pacific Islander; Spanish, Hispanic, or Latino origin but not Black; White; or other] vs Black), chronic kidney disease (estimated glomerular filtration rate <60 vs ≥60 mL/min/1.73 m2), history of cardiovascular disease,32 baseline tertiles of SBP (≤129, 129 to <143, ≥143 mm Hg), and presence of orthostatic hypotension. We also examined subgroups based on frailty status using a previously developed frailty index.33 Participants self-reported age, sex, cardiovascular disease, and education. Race and ethnicity were collected via self-report using fixed categories to satisfy the National Institutes of Health Policy and Guidelines on the Inclusion of Women and Minorities as Subjects in Clinical Research.
Statistical Analysis
Baseline correlations between structural brain MRI measures and CBF were estimated using partial correlation coefficients adjusting for age, sex, and MRI facility, along with treatment group in some analyses.34 Linear mixed models, including random effects for participant and MRI facility, were used to estimate the mean change in CBF between the treatment groups, including age, sex, and time since randomization as covariates. We also conducted sensitivity analyses to address the influence of missing follow-up data using multiple imputation (eMethods and eTable 1 in Supplement 2). Next, because a growing body of evidence suggests that certain antihypertensive medication classes may have specific direct associations with the brain independent of their BP-lowering effects, we conducted sensitivity analyses to examine whether certain classes of antihypertensive medications modified the estimated association of intensive vs standard treatment with CBF. For example, antihypertensive medications that stimulate type 2 and 4 angiotensin II receptors, including angiotensin receptor blockers, dihydropyridine calcium channel blockers, and thiazide diuretics, may have beneficial effects on the brain, possibly through reduced inflammation, hypoxia, and fibrosis.35,36,37,38,39,40,41 For this sensitivity analysis, we repeated the main analysis estimating the association of intensive vs standard treatment with CBF after adjusting for medication use at the visit closest to the MRI follow-up visit (the number and total dosage of antihypertensive medications did not change substantially after 6 months of follow-up in most participants; eFigure 1 in Supplement 2). We adjusted for the use of the following medications in separate models: (1) angiotensin II stimulating vs inhibiting vs mixed regimen, (2) angiotensin-converting enzyme inhibitors vs angiotensin receptor blocker, (3) angiotensin-converting enzyme inhibitors vs others, (4) angiotensin receptor blockers vs others, (5) β-blockers vs others, (6) calcium channel blocker vs others, and (7) thiazide vs others. All analyses were performed using SAS statistical software version 9.4 (SAS Institute) and R version 3.4.2 (R Project for Statistical Computing). All hypothesis tests were 2-sided, and P values less than .05 were considered statistically significant. No adjustments for multiple comparisons were made. Analyses were performed from September 2020 through December 2021.
Results
Of the 547 participants having ASL scans passing the automated quality control at baseline, 315 participants had follow-up scans that also passed quality control. The demographics and clinical characteristics of the participants who completed the baseline and follow-up MRI scans are shown in Table 1. At baseline, the mean (SD) age of the overall sample was 67.5 (8.1) years, 219 (40.0%) were women, 176 (32.2%) were African American, and 35 (6.4%) were Hispanic. The mean (SD) SBP was 137.8 (15.2) mm Hg at baseline. Figure 2 shows the baseline association between WB CBF, total brain volume, and WML volume. Mean WB CBF was weakly correlated with the total brain volume adjusted for intracranial volume but not with the burden of WM lesions.
Table 1. Baseline Characteristics of Participants in the Magnetic Resonance Imaging Substudy With a Baseline Assessment of Cerebral Blood Flow.
| Variable | No. (%) | |||
|---|---|---|---|---|
| Completed baseline scan | Completed follow-up scan | |||
| Intensive (n = 286) | Standard (n = 261) | Intensive (n = 168) | Standard (n = 147) | |
| Age, mean (SD), y | 67.9 (7.9) | 67.1 (8.4) | 68.2 (7.6) | 66.6 (7.7) |
| Age ≥75 y | 70 (24.5) | 58 (22.2) | 39 (23.2) | 27 (18.4) |
| Female | 119 (41.6) | 100 (38.3) | 69 (41.1) | 52 (35.4) |
| Male | 167 (58.4) | 161 (61.7) | 99 (58.9) | 95 (64.6) |
| Race and ethnicity | ||||
| Black | 93 (32.5) | 83 (31.8) | 49 (29.2) | 44 (29.9) |
| Hispanic | 14 (4.9) | 21 (8.0) | 9 (5.4) | 13 (8.8) |
| White | 174 (60.8) | 152 (58.2) | 108 (64.3) | 86 (58.5) |
| Other | 5 (1.7) | 5 (1.9) | 2 (1.2) | 4 (2.7) |
| History of cardiovascular disease | 41 (14.3) | 42 (16.1) | 18 (12.2) | 19 (11.3) |
| Systolic blood pressure, mm Hg | ||||
| Mean (SD) | 138.0 (17.9) | 137.8 (15.2) | 136.0 (17.9) | 138.2 (15.5) |
| Tertile | ||||
| ≤129 | 107 (37.4) | 79 (30.3) | 65 (38.7) | 44 (29.9) |
| >129 to <143 | 82 (28.7) | 91 (34.9) | 53 (31.5) | 55 (37.4) |
| ≥143 | 97 (33.9) | 91 (34.9) | 50 (29.8) | 48 (32.7) |
| Diastolic blood pressure, mean (SD), mm Hg | 76.9 (11.0) | 78.1 (11.6) | 76.1 (11.2) | 78.7 (11.4) |
| Orthostatic hypotension | 24 (8.4) | 11 (4.2) | 17 (10.1) | 8 (5.4) |
| eGFR, mL/min/1.73 m2a | ||||
| Mean (SD) | 72.2 (19.7) | 73.8 (19.9) | 71.5 (18.6) | 74.9 (19.5) |
| <60a | 78 (27.4) | 71 (27.3) | 49 (29.2) | 36 (24.5) |
| PHQ-9 score ≥10b | 18 (6.3) | 17 (6.5) | 8 (4.8) | 8 (5.4) |
| Montreal Cognitive Assessment, median (IQR)c | 24 (21-26) | 24 (22-27) | 24 (21-27) | 25 (22-27) |
| Frailty statusd | ||||
| Fit (score ≤0.10) | 56 (19.6) | 47 (18.0) | 38 (22.6) | 29 (19.7) |
| Prefrail (0.10< score ≤0.21) | 147 (51.4) | 145 (55.6) | 87 (51.8) | 86 (58.5) |
| Frail (score >0.21) | 83 (29.0) | 69 (26.4) | 43 (25.6) | 32 (21.8) |
| Intracranial volume, mean (SD), cm3 | 1371.8 (149.6) | 1384.9 (145.2) | 1375.0 (141.9) | 1393.6 (149.4) |
| Total brain volume, mean (SD), cm3 | 1124.5 (114.0) | 1133.4 (115.7) | 1128.2 (110.7) | 1141.4 (115.4) |
| WML volume, median (IQR), cm3 | 3.0 (1.5 to 6.2) | 3.2 (1.6 to 6.0) | 2.7 (1.4 to 5.9) | 3.0 (1.6 to 6.1) |
| CBF, mean (SD), mL/100 g/min | ||||
| WB | 38.6 (10.8) | 37.5 (9.3) | 39.0 (9.8) | 37.6 (9.2) |
| GM | 50.2 (13.3) | 48.5 (11.4) | 50.4 (12.1) | 48.7 (11.1) |
| WM | 19.9 (7.2) | 19.4 (6.4) | 20.5 (6.6) | 19.4 (6.3) |
| Periventricular WM | 15.9 (6.6) | 15.5 (5.9) | 16.6 (6.1) | 15.5 (5.7) |
Abbreviations: CBF, cerebral blood flow; eGFR, estimated glomerular filtration rate; GM, gray matter; PHQ-9, Patient Health Questionnaire 9-item depression scale; WB, whole brain; WM, white matter; WML, white matter lesion.
eGFR is based on the Chronic Kidney Disease–Epidemiology study equation.
Scores range from 0 to 27. Higher scores denote greater severity of depressive symptoms, with ≥10 indicating moderate to severe depressive symptoms.
Scores range from 0 to 30, with higher scores denoting better cognitive function.
Scores range from 0 to 1, with higher scores indicating a higher likelihood of frailty.
Figure 2. Baseline and Longitudinal Associations Between Whole-Brain Cerebral Blood Flow (CBF), Total Brain Volume, and Cerebral White Matter Lesions (WML).

Rho denotes partial rank correlation coefficient adjusting for age, sex, and magnetic resonance imaging facility. Lines denote estimated least-squares regression line with corresponding 95% CI. WML volumes presented using inverse hyperbolic sine transformation, f(x) = log(x + [x2 + 1]0.5). ICV indicates intracranial volume.
Change in BP and Cerebral Perfusion During Follow-up
Consistent with the larger cohort of participants in the MRI substudy10 and SPRINT overall, there was a sustained between-group difference in SBP among this subgroup of participants with a measured baseline CBF. The mean SBP through the end of active intervention was 120.5 mm Hg in the intensive treatment group vs 134.4 mm Hg in the standard treatment group (difference, 13.9 mm Hg [95% CI, 12.4-15.3 mm Hg]). During the transitional closeout period during which the majority of the follow-up MRI scans occurred, the mean (SD) SBP in the intensive treatment group increased to 126.9 mm Hg (95% CI, 124.2-129.6 mm Hg), whereas the standard treatment group increased to 138.2 mm Hg (95% CI, 135.5-140.9 mm Hg) (difference, 11.3 mm Hg [95% CI, 7.7-14.9 mm Hg]). At 4 years of follow-up, mean (SD) WB CBF in the intensive treatment group increased by 1.46 mL/100 g/min (95% CI, 0.08-2.83), while WB CBF decreased in the standard treatment group, with mean change from baseline of –0.84 mL/100 g/min (95% CI, –2.30 to 0.61) (Table 2). Following adjustment for age, sex, and days since randomization, the increase in mean WB CBF in the intensive treatment group was significantly greater than in the standard treatment (mean between-group difference: 2.30 mL/100 g/min [95% CI, 0.30-4.30]). Figure 3 shows the longitudinal change in mean WB CBF by age and treatment group. Mean WM CBF also increased significantly among participants randomized to intensive compared with standard treatment, while there were not significant differences in GM and periventricular WM CBF.
Table 2. Changes in Cerebral Blood Flow by Treatment Group.
| Outcome | Cerebral blood flow, (95% CI), mL/100 g/mina | Difference in change (95% CI) | P value | |||||
|---|---|---|---|---|---|---|---|---|
| Intensive treatment | Standard treatment | |||||||
| Baseline | Follow-up | Change | Baseline | Follow-up | Change | |||
| Whole brain | 38.90 (36.64 to 41.17) | 40.36 (37.95 to 42.77) | 1.46 (0.08 to 2.83) | 37.96 (35.67 to 40.26) | 37.12 (34.66 to 39.58) | –0.84 (–2.30 to 0.61) | 2.30 (0.30 to 4.30) | .02 |
| Gray matter | 50.76 (47.01 to 54.52) | 52.91 (49.01 to 56.80) | 2.14 (0.41 to 3.87) | 49.40 (45.61 to 53.19) | 49.06 (45.11 to 53.00) | –0.34 (–2.17 to 1.48) | 2.49 (–0.03 to 5.00) | .05 |
| White matter | 19.86 (18.85 to 20.88) | 20.51 (19.35 to 21.67) | 0.65 (–0.32 to 1.61) | 19.41 (18.36 to 20.46) | 18.57 (17.36 to 19.79) | –0.83 (–1.85 to 0.18) | 1.48 (0.08 to 2.88) | .04 |
| Periventricular white matter | 15.79 (14.81 to 16.78) | 16.11 (15.01 to 17.21) | 0.32 (–0.54 to 1.17) | 15.48 (14.47 to 16.50) | 14.60 (13.45 to 15.76) | –0.88 (–1.80 to 0.04) | 1.20 (–0.06 to 2.45) | .06 |
Estimates based on a linear mixed model, adjusting for age, sex, and days since randomization, with random effects for participant and magnetic resonance imaging facility. Estimates represent least-square means, with follow-up estimates computed at 1452 days (4.0 years) postrandomization, which was the median follow-up in both treatment groups. For change estimates, negative values denote decreases from baseline, while positive values indicate increases from baseline. Difference in change represents intensive treatment group minus standard treatment.
Figure 3. Longitudinal Change in Whole-Brain Cerebral Blood Flow (CBF) by Age and Treatment Group.
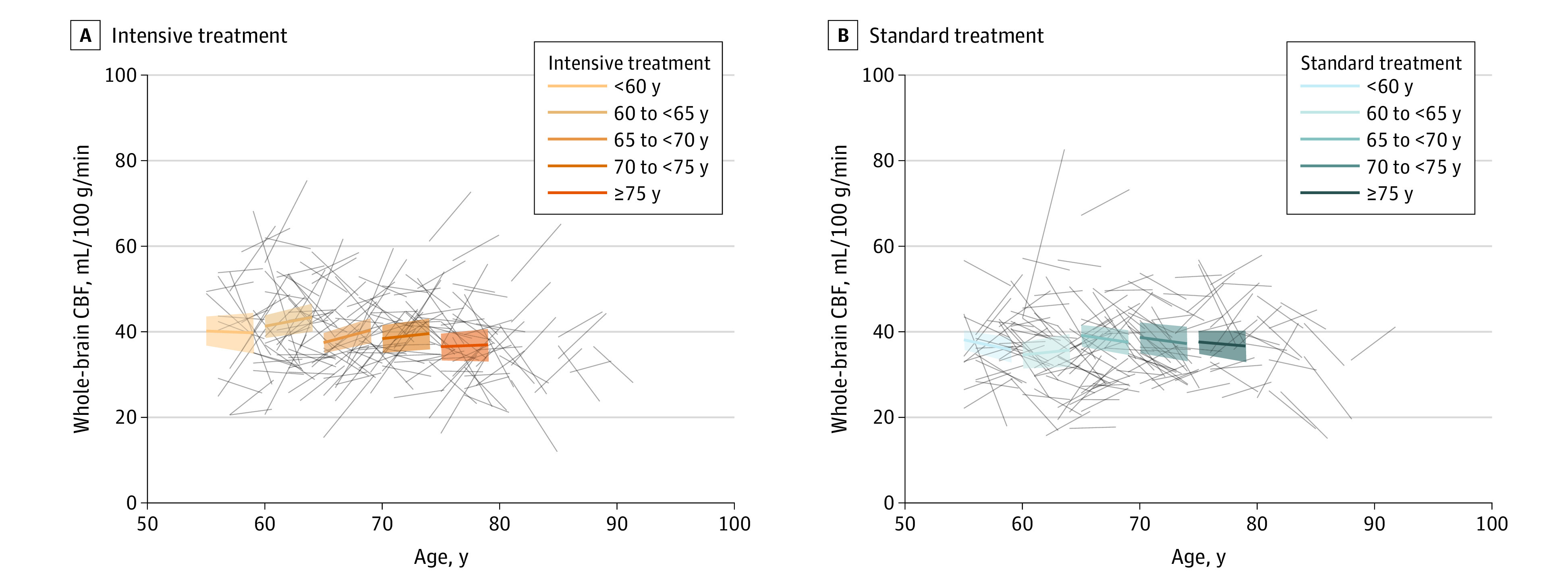
Bold colored lines represent age-specific change in whole-brain CBF estimated from a treatment group–specific linear mixed model, with associated 95% CIs. Gray lines represent individual participant trajectories.
Annualized changes in WB CBF and intracranial volume–adjusted total brain volume were not correlated in either treatment group (Figure 2). The annualized CBF change was correlated (ρ = −0.205; P = .01) with the change in WML volume in the intensive treatment group but not in the standard treatment arm (Figure 2). Pooling across treatment groups, CBF changes in GM, WM, and the periventricular WM were correlated with changes in WML volume (eFigure 2 in Supplement 2).
In subgroup analysis, there was a significant interaction between treatment group and baseline history of cardiovascular disease for the change in mean WB CBF (eTable 2 in Supplement 2). Participants with history of cardiovascular disease had a larger increase in CBF with intensive treatment than with standard treatment compared with those without baseline cardiovascular disease. There was no other significant subgroup interaction (eTable 2 in Supplement 2).
Sensitivity Analyses
Results of analyses based on multiple imputation to address missing follow-up measurements of CBF are reported in eTable 3 in Supplement 2. Results were generally unchanged, showing significant increases in WB and WM CBF associated with intensive treatment. We also examined if use of certain classes of antihypertensive medications during the trial potentially explained the association of intensive treatment with WB CBF. The association of intensive treatment with WB CBF was generally unchanged after adjustment for use of various classes of antihypertensive medications at the visit prior to the follow-up MRI (eTable 4 in Supplement 2).
Discussion
Using perfusion MRI data acquired in the neuroimaging substudy of a randomized clinical trial, we found that intensive treatment was not associated with hypoperfusion, but rather with a small but significant increase in WB and WM CBF compared with a standard treatment over approximately 4 years of follow-up. In subgroup analyses, participants with a history of cardiovascular disease randomized to intensive treatment exhibited the largest increases in WB CBF. Prior reports have suggested that intensive antihypertensive therapy was well tolerated in the short term,21,22 with this study demonstrating that targeting longer-term intensive BP control may be associated with a subtle but significant increase in CBF.
The mechanistic basis for the observed increase in CBF associated with intensive treatment remains uncertain but suggests a complex relationship between BP and CBF, beyond simply static cerebral perfusion pressure and cerebrovascular autoregulation. One key barrier to implementation of intensive treatment was a concern that intensive treatment might reduce the BP below the cerebral autoregulatory limit, leading to cerebral hypoperfusion. Our findings suggest that this does not occur, at least on a chronic basis. Note that this relates to static cerebral autoregulation rather than dynamic autoregulation, which describes CBF changes in response to a more rapid change in BP. CBF is measured supine, not while standing, and it remains possible that the CBF changes when transitioning from sitting to standing pertaining to dynamic autoregulation with intensive therapy can be lower. The association of intensive treatment with brain perfusion stand somewhat in contrast with association with the kidney, where intensive treatment resulted in a greater incidence of acute kidney injury speculated to reflect hemodynamic changes in kidney perfusion.42,43 This difference may reflect a greater adaptability of cerebrovascular autoregulation to chronic systemic changes or greater tolerance to episodic hypotension relative to the kidney vascular system. There were no appreciable associations of medication class with the estimated association of intensive treatment with CBF outcomes, suggesting that our results were more likely driven by achieved BP rather than any specific medication effect independent of BP change.
To the extent that increased CBF is beneficial to cerebrovascular health,44 intensive treatment seems to be advantageous, adding to the other beneficial effects of intensive treatment detailed in SPRINT. Previously, structural MRI showed smaller increases in WML volumes but greater decreases in total brain volume associated with intensive treatment.10 While the increase in CBF in the intensive treatment group is consistent with the favorable effect on the progression of WM lesions, we observed generally weak correlations between the changes in CBF and WM lesion volumes. Although CBF is believed to be one factor affecting WML change,45,46,47 it is possible that other hypertension-related factors affecting WML change, such as vascular remodeling, have contributed. Additionally, with the known individual variability in CBF measures29 and the slow process of WML progression, it is possible that the trial did not have sufficient sensitivity to detect a more direct association between these measures. Although baseline CBF and total brain volume were correlated, there was also no association between changes in these measures during follow-up. In fact, the absolute change for these measures at the group level were in opposite directions, suggesting that hypoperfusion was not likely a factor in the larger declines in total brain volume associated with intensive treatment.
Limitations
The current study has several limitations. First, the sample size of the imaging substudy was much smaller than the overall trial and may not be fully representative of the overall cohort.10 The completion rate of follow-up MRIs was lower than expected and it was further reduced in the current study owing to technical issues at 1 site. Second, the trial design incorporated MRI scanning including ASL at only 2 time points, so the trajectory and stability of CBF changes could not be assessed. Third, the study did not use current state-of-art 3-dimensional pseudocontinuous ASL with background suppression, which can provide more reliable CBF measures, although it used pseudocontinuous labeling, which is the currently recommended labeling strategy.23 Moreover, the ASL MRI protocol used in the trial has been extensively used in a number of prior studies, including longitudinal studies and in different patient populations.48,49,50,51,52
Conclusions
Intensive BP control to a target of less than 120 mm Hg compared with a standard target of less than 140 mm Hg was associated with increased CBF in WB and WM. Increases in CBF associated with intensive treatment were more pronounced in participants with a history of cardiovascular disease.
Trial Protocol
eMethods.
eTable 1. Multiple Imputation Conditional Model Specification for Sensitivity Analyses
eTable 2. Changes in Whole Brain Cerebral Blood Flow by Treatment Group and Subgroup
eTable 3. Sensitivity Analyses of the Association of Treatment Group with Cerebral Blood Flow based on Multiple Imputation
eTable 4. The effect of intensive vs. standard BP control on mean Whole Brain CBF within medication use subgroups at the most recent visit prior to the follow-up MRI assessment (N = 315)
eFigure 1. Modified therapeutic intensity score in the two treatment groups over the course of follow-up
eFigure 2. Adjusted Associations between Changes in Cerebral Blood Flow, Total Brain Volume, and White Matter Lesions Volume across the entire cohort with longitudinal CBF
eReferences
Data Sharing Statement
References
- 1.Faraco G, Iadecola C. Hypertension: a harbinger of stroke and dementia. Hypertension. 2013;62(5):810-817. doi: 10.1161/HYPERTENSIONAHA.113.01063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lawes CMM, Bennett DA, Feigin VL, Rodgers A. Blood pressure and stroke: an overview of published reviews. Stroke. 2004;35(3):776-785. doi: 10.1161/01.STR.0000116869.64771.5A [DOI] [PubMed] [Google Scholar]
- 3.Williamson JD, Pajewski NM, Auchus AP, et al. ; SPRINT MIND Investigators for the SPRINT Research Group . Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553-561. doi: 10.1001/jama.2018.21442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Park JH, Hong JH, Lee SW, et al. The effect of chronic cerebral hypoperfusion on the pathology of Alzheimer’s disease: a positron emission tomography study in rats. Sci Rep. 2019;9(1):14102. doi: 10.1038/s41598-019-50681-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wolters FJ, Zonneveld HI, Hofman A, et al. ; Heart-Brain Connection Collaborative Research Group . Cerebral perfusion and the risk of dementia: a population-based study. Circulation. 2017;136(8):719-728. doi: 10.1161/CIRCULATIONAHA.117.027448 [DOI] [PubMed] [Google Scholar]
- 6.Nortley R, Korte N, Izquierdo P, et al. Amyloid β oligomers constrict human capillaries in Alzheimer's disease via signaling to pericytes. Science. 2019;365(6450):eaav9518. doi: 10.1126/science.aav9518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Graham DI. Ischaemic brain damage of cerebral perfusion failure type after treatment of severe hypertension. Br Med J. 1975;4(5999):739. doi: 10.1136/bmj.4.5999.739 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Birns J, Markus H, Kalra L. Blood pressure reduction for vascular risk: is there a price to be paid? Stroke. 2005;36(6):1308-1313. doi: 10.1161/01.STR.0000165901.38039.5f [DOI] [PubMed] [Google Scholar]
- 9.Wright JT Jr, Williamson JD, Whelton PK, et al. ; SPRINT Research Group . A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-2116. doi: 10.1056/NEJMoa1511939 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nasrallah IM, Pajewski NM, Auchus AP, et al. ; SPRINT MIND Investigators for the SPRINT Research Group . Association of intensive vs standard blood pressure control with cerebral white matter lesions. JAMA. 2019;322(6):524-534. doi: 10.1001/jama.2019.10551 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ruland S, Aiyagari V. Cerebral autoregulation and blood pressure lowering. Hypertension. 2007;49(5):977-978. doi: 10.1161/HYPERTENSIONAHA.107.087502 [DOI] [PubMed] [Google Scholar]
- 12.Strandgaard S. Autoregulation of cerebral blood flow in hypertensive patients: the modifying influence of prolonged antihypertensive treatment on the tolerance to acute, drug-induced hypotension. Circulation. 1976;53(4):720-727. doi: 10.1161/01.CIR.53.4.720 [DOI] [PubMed] [Google Scholar]
- 13.Nobili F, Rodriguez G, Marenco S, et al. Regional cerebral blood flow in chronic hypertension: a correlative study. Stroke. 1993;24(8):1148-1153. doi: 10.1161/01.STR.24.8.1148 [DOI] [PubMed] [Google Scholar]
- 14.Fujishima M, Ibayashi S, Fujii K, Mori S. Cerebral blood flow and brain function in hypertension. Hypertens Res. 1995;18(2):111-117. doi: 10.1291/hypres.18.111 [DOI] [PubMed] [Google Scholar]
- 15.Dai W, Lopez OL, Carmichael OT, Becker JT, Kuller LH, Gach HM. Abnormal regional cerebral blood flow in cognitively normal elderly subjects with hypertension. Stroke. 2008;39(2):349-354. doi: 10.1161/STROKEAHA.107.495457 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Muller M, van der Graaf Y, Visseren FL, Mali WPTM, Geerlings MI; SMART Study Group . Hypertension and longitudinal changes in cerebral blood flow: the SMART-MR study. Ann Neurol. 2012;71(6):825-833. doi: 10.1002/ana.23554 [DOI] [PubMed] [Google Scholar]
- 17.Lipsitz LA, Gagnon M, Vyas M, et al. Antihypertensive therapy increases cerebral blood flow and carotid distensibility in hypertensive elderly subjects. Hypertension. 2005;45(2):216-221. doi: 10.1161/01.HYP.0000153094.09615.11 [DOI] [PubMed] [Google Scholar]
- 18.Claassen JAHR, Thijssen DHJ, Panerai RB, Faraci FM. Regulation of cerebral blood flow in humans: physiology and clinical implications of autoregulation. Physiol Rev. 2021;101(4):1487-1559. doi: 10.1152/physrev.00022.2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.de Jong DLK, de Heus RAA, Rijpma A, et al. Effects of nilvadipine on cerebral blood flow in patients with Alzheimer disease. Hypertension. 2019;74(2):413-420. doi: 10.1161/HYPERTENSIONAHA.119.12892 [DOI] [PubMed] [Google Scholar]
- 20.Stewart IMG. Relation of reduction in pressure to first myocardial infarction in patients receiving treatment for severe hypertension. Lancet. 1979;1(8121):861-865. doi: 10.1016/S0140-6736(79)91274-1 [DOI] [PubMed] [Google Scholar]
- 21.Tryambake D, He J, Firbank MJ, O’Brien JT, Blamire AM, Ford GA. Intensive blood pressure lowering increases cerebral blood flow in older subjects with hypertension. Hypertension. 2013;61(6):1309-1315. doi: 10.1161/HYPERTENSIONAHA.112.200972 [DOI] [PubMed] [Google Scholar]
- 22.Croall ID, Tozer DJ, Moynihan B, et al. ; PRESERVE Study Team . Effect of standard vs intensive blood pressure control on cerebral blood flow in small vessel disease: the PRESERVE Randomized Clinical Trial. JAMA Neurol. 2018;75(6):720-727. doi: 10.1001/jamaneurol.2017.5153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: a consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-116. doi: 10.1002/mrm.25197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dolui S, Tisdall D, Vidorreta M, et al. Characterizing a perfusion-based periventricular small vessel region of interest. Neuroimage Clin. 2019;23:101897. doi: 10.1016/j.nicl.2019.101897 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dolui S, Wang Z, Shinohara RT, Wolk DA, Detre JA; Alzheimer’s Disease Neuroimaging Initiative . Structural Correlation-based Outlier Rejection (SCORE) algorithm for arterial spin labeling time series. J Magn Reson Imaging. 2017;45(6):1786-1797. doi: 10.1002/jmri.25436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dolui S, Wolk DA, Detre JA. SCRUB: a structural correlation and empirical robust bayesian method for ASL data. Poster presented at: 24th Annual Meeting and Exhibition of the International Society for Magnetic Resonance in Medicine; May 9, 2016; Singapore. [Google Scholar]
- 27.Dolui S, Wolf RL, Nabavizadeh SA, Wolk DA, Detre JA. Automated quality evaluation index for 2D ASL CBF maps. Poster presented at: 25th Annual Meeting and Exhibition of the International Society for Magnetic Resonance in Medicine; April 26, 2017; Honolulu, Hawaii. [Google Scholar]
- 28.Doshi J, Erus G, Ou Y, et al. ; Alzheimer’s Neuroimaging Initiative . MUSE: MUlti-atlas region Segmentation utilizing Ensembles of registration algorithms and parameters, and locally optimal atlas selection. Neuroimage. 2016;127:186-195. doi: 10.1016/j.neuroimage.2015.11.073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dolui S, Wang Z, Wang DJJ, et al. Comparison of non-invasive MRI measurements of cerebral blood flow in a large multisite cohort. J Cereb Blood Flow Metab. 2016;36(7):1244-1256. doi: 10.1177/0271678X16646124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moody DM, Bell MA, Challa VR. Features of the cerebral vascular pattern that predict vulnerability to perfusion or oxygenation deficiency: an anatomic study. AJNR Am J Neuroradiol. 1990;11(3):431-439. [PMC free article] [PubMed] [Google Scholar]
- 31.Doshi J, Erus G, Habes M, Davatzikos C. DeepMRSeg: a convolutional deep neural network for anatomy and abnormality segmentation on MR images. arXiv. Preprint posted online July 3, 2019. https://arxiv.org/abs/1907.02110.
- 32.Ambrosius WT, Sink KM, Foy CG, et al. ; SPRINT Study Research Group . The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT). Clin Trials. 2014;11(5):532-546. doi: 10.1177/1740774514537404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pajewski NM, Williamson JD, Applegate WB, et al. ; SPRINT Study Research Group . Characterizing frailty status in the systolic blood pressure intervention trial. J Gerontol A Biol Sci Med Sci. 2016;71(5):649-655. doi: 10.1093/gerona/glv228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Liu Q, Li C, Wanga V, Shepherd BE. Covariate-adjusted Spearman’s rank correlation with probability-scale residuals. Biometrics. 2018;74(2):595-605. doi: 10.1111/biom.12812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kaschina E, Namsolleck P, Unger T. AT2 receptors in cardiovascular and renal diseases. Pharmacol Res. 2017;125(Pt A):39-47. doi: 10.1016/j.phrs.2017.07.008 [DOI] [PubMed] [Google Scholar]
- 36.Forrester SJ, Booz GW, Sigmund CD, et al. Angiotensin II signal transduction: an update on mechanisms of physiology and pathophysiology. Physiol Rev. 2018;98(3):1627-1738. doi: 10.1152/physrev.00038.2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Saavedra JM, Benicky J, Zhou J. Mechanisms of the anti-ischemic effect of angiotensin II AT(1) receptor antagonists in the brain. Cell Mol Neurobiol. 2006;26(7-8):1099-1111. doi: 10.1007/s10571-006-9009-0 [DOI] [PubMed] [Google Scholar]
- 38.Horiuchi M, Mogi M. Role of angiotensin II receptor subtype activation in cognitive function and ischaemic brain damage. Br J Pharmacol. 2011;163(6):1122-1130. doi: 10.1111/j.1476-5381.2010.01167.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ho JK, Nation DA. Cognitive benefits of angiotensin IV and angiotensin-(1-7): a systematic review of experimental studies. Neurosci Biobehav Rev. 2018;92(May):209-225. doi: 10.1016/j.neubiorev.2018.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hamel E, Royea J, Ongali B, Tong XK. Neurovascular and cognitive failure in Alzheimer’s disease: benefits of cardiovascular therapy. Cell Mol Neurobiol. 2016;36(2):219-232. doi: 10.1007/s10571-015-0285-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Baranello RJ, Bharani KL, Padmaraju V, et al. Amyloid-beta protein clearance and degradation (ABCD) pathways and their role in Alzheimer’s disease. Curr Alzheimer Res. 2015;12(1):32-46. doi: 10.2174/1567205012666141218140953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Rocco MV, Sink KM, Lovato LC, et al. ; SPRINT Research Group . Effects of intensive blood pressure treatment on acute kidney injury events in the Systolic Blood Pressure Intervention Trial (SPRINT). Am J Kidney Dis. 2018;71(3):352-361. doi: 10.1053/j.ajkd.2017.08.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Malhotra R, Craven T, Ambrosius WT, et al. ; SPRINT Research Group . Effects of intensive blood pressure lowering on kidney tubule injury in CKD: a longitudinal subgroup analysis in SPRINT. Am J Kidney Dis. 2019;73(1):21-30. doi: 10.1053/j.ajkd.2018.07.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shaw TG, Mortel KF, Meyer JS, Rogers RL, Hardenberg J, Cutaia MM. Cerebral blood flow changes in benign aging and cerebrovascular disease. Neurology. 1984;34(7):855-862. https://www.ncbi.nlm.nih.gov/pubmed/6539861. doi: 10.1212/WNL.34.7.855 [DOI] [PubMed] [Google Scholar]
- 45.Kobari M, Meyer JS, Ichijo M, Oravez WT. Leukoaraiosis: correlation of MR and CT findings with blood flow, atrophy, and cognition. AJNR Am J Neuroradiol. 1990;11(2):273-281. [PMC free article] [PubMed] [Google Scholar]
- 46.ten Dam VH, van den Heuvel DM, de Craen AJ, et al. Decline in total cerebral blood flow is linked with increase in periventricular but not deep white matter hyperintensities. Radiology. 2007;243(1):198-203. doi: 10.1148/radiol.2431052111 [DOI] [PubMed] [Google Scholar]
- 47.Stewart CR, Stringer MS, Shi Y, Thrippleton MJ, Wardlaw JM. Associations between white matter hyperintensity burden, cerebral blood flow and transit time in small vessel disease: an updated meta-analysis. Front Neurol. 2021;12(May):647848. doi: 10.3389/fneur.2021.647848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chen Y, Wolk DA, Reddin JS, et al. Voxel-level comparison of arterial spin-labeled perfusion MRI and FDG-PET in Alzheimer disease. Neurology. 2011;77(22):1977-1985. doi: 10.1212/WNL.0b013e31823a0ef7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Dolui S, Vidorreta M, Wang Z, et al. Comparison of PASL, PCASL, and background-suppressed 3D PCASL in mild cognitive impairment. Hum Brain Mapp. 2017;38(10):5260-5273. doi: 10.1002/hbm.23732 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Dolui S, Li Z, Nasrallah IM, Detre JA, Wolk DA. Arterial spin labeling versus 18F-FDG-PET to identify mild cognitive impairment. Neuroimage Clin. 2020;25:102146. doi: 10.1016/j.nicl.2019.102146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Moonen JE, Nasrallah IM, Detre JA, et al. Race and sex differences in midlife changes in cerebral volume and perfusion. Alzheimer’s Dement. 2020;16(S4):1-2. doi: 10.1002/alz.040248 [DOI] [Google Scholar]
- 52.Ware JB, Dolui S, Duda J, et al. Relationship of cerebral blood flow to cognitive function and recovery in early chronic traumatic brain injury. J Neurotrauma. 2020;37(20):2180-2187. doi: 10.1089/neu.2020.7031 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eMethods.
eTable 1. Multiple Imputation Conditional Model Specification for Sensitivity Analyses
eTable 2. Changes in Whole Brain Cerebral Blood Flow by Treatment Group and Subgroup
eTable 3. Sensitivity Analyses of the Association of Treatment Group with Cerebral Blood Flow based on Multiple Imputation
eTable 4. The effect of intensive vs. standard BP control on mean Whole Brain CBF within medication use subgroups at the most recent visit prior to the follow-up MRI assessment (N = 315)
eFigure 1. Modified therapeutic intensity score in the two treatment groups over the course of follow-up
eFigure 2. Adjusted Associations between Changes in Cerebral Blood Flow, Total Brain Volume, and White Matter Lesions Volume across the entire cohort with longitudinal CBF
eReferences
Data Sharing Statement