

ABSTRACT
Across many parts of the globe, the educational system is under a complete shutdown, falling victim to health-safety concerns of the deadly COVID-19; and Bangladesh is no exception. Reportedly, the Bangladesh government prioritized resuming public universities after bringing all the students under vaccination. However, little is known about students’ intention toward the COVID-19 vaccines in Bangladesh. Under the circumstances, this study attempted to assess the COVID-19 vaccine-related knowledge, perceptions, attitude, and acceptability of a COVID-19 vaccine of public university students. Besides, factors affecting the degrees of COVID-19 vaccine-related knowledge, perceptions, attitudes, and vaccine acceptability were also explored. Results from descriptive analyses revealed that most of the respondents showed positive attitudes toward a COVID-19 vaccine, while 78% of them found to have adequate knowledge. Nevertheless, 37% of students exhibiting negative perceptions about the vaccine raised our concern. However, 72.7% of respondents intended to take a COVID-19 vaccine. Outcomes of multinomial logistic model showed that knowledge, perceptions, and attitudes significantly varied across the level of education, residence area, and COVID-19 infection history of the respondents. Further, findings of binary logistic model reported that female students, students of low family income, those free from COVID-19 infection, students having inadequate knowledge, and negative perceptions and attitudes toward the vaccine were susceptible to vaccine hesitancy and resistance. Indeed, our research will assist the authorities in better understanding the students’ attitudes toward the COVID-19 vaccines and in developing appropriate policies for a successful vaccination campaign in Bangladesh and other countries with similar background.
KEYWORDS: Attitude, COVID-19 vaccine, knowledge, perceptions, university students, vaccine acceptance
Introduction
Since the coronavirus has spread rapidly throughout the world from its emergence, health agencies and medical societies consider vaccination to be a pivotal step in reducing or eliminating COVID-19’s burden.1 As a result, inoculation campaigns have emerged as a critical technique in the fight against coronavirus, as they can help achieving herd immunity if a large section of the population is vaccinated. Vaccines generally take years to develop before reaching the clinical application stage, but in 2020, scientists embarked on a race to develop safe and effective coronavirus vaccines in the possible quickest period. Among the vaccines that have been licensed for use in an emergency, Pfizer-vaccine has a 96% efficacy rate, while the vaccines of Moderna and AstraZeneca-Oxford claim efficacy rates of 94.10% and 70%, respectively.2 Meanwhile, Russia’s Sputnik V was revealed to have a 92% efficacy rate.3
COVID-19 has become a serious problem in Bangladesh, as it is in many other South Asian Association for Regional Cooperation (SAARC) countries.4 Expats brought COVID-19 to Bangladesh, and on March 8, 2020, the ‘Institute of Epidemiology, Disease Control and Research (IEDCR)’ reported the first-ever confirmed case of COVID-19.5 As a preventive measure, Bangladesh initially imported supplies of 10 million vaccine doses (including 3 million doses of a gift from the Indian government) of the COVISHIELD vaccine from the Serum Institute of India (SII), the world’s largest vaccine manufacturer and producer of the Oxford-AstraZeneca vaccine.6 Recently, Bangladesh also started to import the vaccine of Pfizer-BioNTech, Moderna, and Sinopharm since the SII was incapable of delivering the contracted quantity within the specified period. Furthermore, the COVAX initiative, led by the World Health Organization (WHO) and the Global Alliance for Vaccines and Immunization (GAVI), is supposed to provide around 12.79 million vaccine doses to Bangladesh.7 It should be noted that Bangladesh initiated its vaccination program on February 7, 2021.8 Although Bangladeshi government states that frontline personnel, including doctors, nurses, and the elderly will be given priority in vaccinations,9 recently the government commenced a nationwide mass vaccination initiative to vaccinate anybody over the age of eighteen who has a National Identity Card.
In the early days of the pandemic, the Bangladesh government imposed a nationwide lockdown on March 26, 202010 with all government, non-government, industry, and educational institutions kept shut except for emergency services. Prior to that, on March 17, 2020, the Bangladesh government decided to close its educational institutions,11 and many of them are still locked today. Some educational institutions have lately launched a limited activity after one and half years break aimed at taking only final year undergraduate students’ examinations, but other students are still in a quandary. Reportedly, more than 0.45 million students are currently enrolled in 49 public universities in Bangladesh.12 Keeping this massive number of students out of vaccination coverage, it is not plausible to fully resume the universities that have been remaining closed for over one and half years. Therefore, Bangladesh’s Education Minister announced that every university student must be vaccinated before the university campuses reopen.13 However, numerous delinquents are circulating misleading and contaminated vaccine-related information, such as its adverse effects, ineffectiveness, and so on, which may deter students from being vaccinated. Facebook’s third-party fact-checking partner in Bangladesh, Boom Bangladesh, claimed that they have disputed different vaccination statements and identified over 1 million Facebook messages that promoted disinformation in January 2021.14 Amid all sorts of rumors, individual willingness, and positive perception and attitude might be the key factors for being COVID-19 vaccinated. Recently, a study in Italy regarding students’ attitudes toward vaccination found that one out of every ten students had a poor intention to vaccinate.15 Besides, a study revealed that 79.6% of surveyed public university students in Canada were willing to get a COVID-19 vaccine.16 Another study in Vietnam claimed that 77.1% of sampled students were eager to be vaccinated against COVID-19.17
However, no substantial research has been done on the awareness, perceptions, attitude, and willingness to take the COVID-19 vaccine of Bangladeshi university students. Therefore, this study aims to assess the knowledge, perceptions, attitude, and acceptance of the COVID-19 vaccine, as well as explore the factors affecting knowledge, perceptions, attitude, and vaccine acceptability. This study contributes to the extant literature of COVID-19 vaccine in several ways. This is one of the pioneer research in Bangladesh focusing on the university students’ intentions to be vaccinated against COVID-19, as vaccination is mandatory for them to attend physical classes. This research paves the way for a deeper understanding of university students’ vaccination intentions. Undeniably, the finding ultimately aids educational policymakers in making the best decisions possible about the way of recommencing the normal education system as quickly as possible. The findings of this study could be beneficial in generating health education messages to promote vaccination acceptability among students who have been hesitant to receive a new vaccine, as well as in larger populations of Bangladesh and other similar countries.
Methods
Study design and participants
The cross-sectional e-survey was conducted among public university students from March 22, 2021, to April 1, 2021, nearly 45 days after enacting the COVID-19 vaccination program in Bangladesh. Hence, it allows us to capture the real scenario about the knowledge, perception, and attitude toward the COVID-19 vaccine. The e-survey was conducted regardless of university location or type (general or technical), assuming that all university students, irrespective of courses or disciplines, have a similar level of knowledge about the COVID-19 vaccination. A convenient sampling procedure was followed to select the studied respondents, i.e., postgraduate and undergraduate students. To collect the primary data, a well-structured questionnaire was developed and integrated into the online survey tool (Kobo toolbox). After that, a shareable link was created, and it was publicly shared through social networking sites (e.g., Facebook, Messenger, WhatsApp, Instagram, LinkedIn, etc.). In addition, the questionnaire link was sent out through e-mail from the authors’ mail list. The respondents were aptly explained about the survey purpose, and their consent was ensured before the online data collection. The respondents were selected based on a set of criteria, including being a Bangladeshi public university student over the age of 18, agreeing to participate in interviews willingly, and having access to the internet.
Sampling and pilot survey
To satisfy the objectives of this study and acceptable statistical power, the sample size was estimated using the RAOSOFT (http://www.raosoft.com/samplesize.html) sample size calculator. Since no analogous research was conducted in Bangladesh focusing on knowledge, perception, and attitude toward the COVID-19 vaccine among public university students, the sample size was calculated by keeping a 96.5% confidence interval, 3.5% error of margin, and a population size of 454530 as the latest statistics found that Bangladesh has approximately 454530 public university students.12 Using the information provided above, the sample size was determined to be 860. However, when the survey portal was closed down, 900 complete responses were recorded. We employed all of the complete responses for this study since the sample size becomes more extensive, and the larger the sample size, the higher the research’s external validity and generalizability. Therefore, our sample size comprehensively satisfied the least sample required for this study. A pilot survey was undertaken on fifteen students before data collection. The questionnaire was reformed and finalized for data collection based on the outcome of the pilot survey.
Study instrument and measure
The questionnaire was formatted following the available literature.15,18,19 The language of the questionnaire was English since it is the medium of instruction at university-level education in Bangladesh. The final questionnaire contained the following five sections:
Section I: Questions regarding respondents’ socio-demographic characteristics were asked, including age, gender, level of education (undergraduate or postgraduate), monthly family income, residence area, COVID-19 infection history, informed about COVID-19 vaccine (yes or no), and sources from where learn about COVID-19 vaccine (Table 1).
Section II: To assess respondents’ knowledge, nine questions related to the COVID-19 vaccine were interrogated for each respondent. The details of specific questions that were requested to respond can be found in Table 2. Respondents acquired one (1) point for each correct response, while a zero (0) score was assigned for an incorrect answer. Then, the total score of nine questions was calculated for each respondent. Thus, the knowledge score ranged from 0 to 9. On the ground of knowledge score, respondents were apportioned into two categories, i.e., having adequate knowledge and inadequate knowledge. The cumulative score was equal to and greater than seven (77% correct answer), which signifies having adequate knowledge, and less than seven indicates inadequate knowledge. The Cronbach alpha of knowledge statements was 0.77.
Section III: This section includes eight specific statements to assess respondents’ perceptions of the COVID-19 vaccine (see details in Table 3). The response of each statement was recorded on a three-point Likert scale (Yes = 1, No = 0, and Not sure = 2). However, if the statements were asked negatively, then the three-point Likert scale score would be revised (No = 1, Yes = 0, and Not sure = 2). The frequency and percentage of responses, i.e., yes, no, and not sure, were estimated for each statement. The total perception score of every participant was calculated by summating the raw scores of the eight statements ranging from 0 to 16. Afterward, the participants were categorized into two sects. The overall score of less than eight indicating positive perception and a score greater than eight symbolizing negative perception towards the COVID-19 vaccine. The Cronbach alpha of perception statements was 0.79.
Section IV: This segment included eight statements to assess the participant’s attitude toward the COVID-19 vaccination (see details in Table 4). A five-point Likert scale (Strongly agree = 5, Agree = 4, Not sure = 3, Disagree = 2, Strongly disagree = 1) was used to record the responses for each statement. Then the total score of each participant was calculated by summing up the raw score against each statement. The overall attitude score varied from 8 to 40; participants with a score of > 24 were considered to have a positive attitude, and < 24 considered having a negative attitude toward the COVID-19 vaccine. The Cronbach alpha of attitudes statements was 0.78.
Section V: The final section of the questionnaire addressed the COVID-19 vaccine acceptability among the participants. The respondents were asked whether they are willing to get vaccinated against COVID-19. If the respondents did not want to receive the vaccine, they were additionally asked why they did not want to.
Table 1.
Characteristics of selected respondents (N = 900)
| Personal and clinical characteristics |
Level |
No. of participants (%) |
|---|---|---|
| Age (years) | Mean ± Standard deviation | 23.95 ± 3.38 |
| Participants category | Postgraduate | 372 (41.3) |
| Undergraduate | 528 (58.7) | |
| Sex | Male | 502 (55.8) |
| Female | 398 (44.2) | |
| Total family income (monthly)* | Low income | 34 (4.0) |
| Lower-middle income | 530 (58.9) | |
| Upper-middle income | 294 (32.7) | |
| High income | 40 (4.4) | |
| Residence area | Urban | 486 (54.0) |
| Rural | 236 (26.2) | |
| Semi-urban | 178 (19.8) | |
| Covid-19 infected (either respondent or any of their family member) | Yes | 84 (9.3) |
| No | 572 (63.6) | |
| Did not test | 244 (27.1) | |
| Have you heard about the COVID-19 vaccine | Yes | 900 (100) |
| No | 0 | |
| Sources from where you first heard about the COVID-19 vaccine | Print newspaper | 160 (17.8) |
| Television/radio | 234 (26.0) | |
| Social media | 290 (41.1) | |
| Medical personnel | 96 (10.7) | |
| Friends and family | 40 (4.4) |
*Total household income categorized into: Low income (≤$85), Lower middle income ($86 to $336), Upper middle income ($337 to $1040), and High income (≥$1040) according to World Bank income group.
Table 2.
Responses to knowledge questions related to COVID-19 vaccine (N = 900)
| Question | No. of participants (%) |
|
|---|---|---|
| Correct | Incorrect | |
| What app/website does it require for registration to get a vaccine? | 526 (58.4) | 374 (41.6) |
| Do you know about mandatory vaccination for all public university students prior to open up the institutions? | 522 (58.0) | 378 (42.0) |
| How many vaccines get approval for emergency use? | 620 (68.9) | 280 (31.1) |
| What number of vaccine doses are required for each person? | 766 (85.1) | 134 (14.9) |
| When from Bangladesh Government began mass vaccination? | 562 (62.4) | 338 (37.6) |
| From where Bangladesh received the first vaccine consignment? | 802 (89.1) | 98 (10.9) |
| How many countries/institutes are producing vaccines now? | 500 (55.6) | 400 (44.4) |
| For how many vaccine doses has Bangladesh secured priority contracts with the Serum Institute of India? | 358 (39.8) | 542 (60.2) |
| Which pharmaceutical company has partnered with the government on the vaccination campaign? | 838 (93.1) | 62 (6.9) |
| Overall knowledge score (mean ± SD) | 3.21 ± 4.13 | |
Table 3.
Perceptions about the COVID-19 vaccine among participants (N = 900)
| Statements | No. of participants (%) |
||
|---|---|---|---|
| Yes | Not sure | No | |
| COVID-19 vaccine is effectual | 306 (34.0) | 506 (56.2) | 88 (9.8) |
| I am worried about how vaccine react into my body | 632 (70.2) | 158 (17.6) | 110 (12.2) |
| COVID-19 disease is naturally curable without any vaccine | 68 (7.6) | 276 (30.7) | 556 (61.8) |
| Without any vaccine, antibiotics can cure the disease | 76 (8.4) | 262 (29.1) | 562 (62.4) |
| COVID-19 vaccine can only be applicable for people infected with coronavirus | 96 (10.7) | 320 (35.6) | 484 (53.8) |
| Eating nutritious foods to boost one’s immune function outperforms the vaccine | 68 (7.6) | 304 (33.8) | 528 (58.7) |
| I think vaccine is more applicable for patients with chronic diseases | 286 (31.8) | 362 (40.2) | 252 (28.0) |
| I am confident that vaccine can obliterate COVID-19 from Bangladesh | 450 (50.0) | 374 (41.6) | 76 (8.4) |
| Overall perception score (mean ± SD) | 7.89 ± 2.81 | ||
Table 4.
Attitudes toward COVID-9 vaccine (N = 900)
| Statements | No. of participants (%) |
|||||
|---|---|---|---|---|---|---|
| Strongly agree | Agree | Not sure | Disagree | Strongly disagree | ||
| My family will allow me to get vaccinated | 222 (24.7) | 248 (27.6) | 314 (34.9) | 80 (8.9) | 36 (4) | |
| COVID-19 vaccine will bring us back to normal education system | 258 (28.7) | 264 (29.3) | 288 (32.0) | 66 (7.3) | 24 (2.7) | |
| I might be infected with COVID-19 if I do not get vaccinated | 170 (18.9) | 142 (15.8) | 340 (37.8) | 216 (24.0) | 32 (3.6) | |
| COVID-19 vaccine must be mandatory for all students before the opening up the university | 144 (16.0) | 396 (44.0) | 258 (28.7) | 70 (7.8) | 32 (3.6) | |
| I can easily have the COVID-19 vaccine | 50 (5.6) | 112 (12.4) | 204 (22.7) | 254 (28.2) | 280 (31.1) | |
| If university inaugurate without providing vaccine, I might get infected | 122 (13.6) | 152 (16.9) | 474 (52.7) | 96 (10.7) | 56 (6.2) | |
| I would regret If I become infected with coronavirus even after getting the vaccine | 240 (26.7) | 388 (43.1) | 170 (18.9) | 80 (8.9) | 22 (2.4) | |
| Since a coronavirus vaccine is too new, I might be worried | 348 (38.7) | 246 (27.3) | 168 (18.7) | 98 (10.9) | 40 (4.4) | |
| Overall attitude score (mean ± SD) | 27.39 ± 3.82 | |||||
Data analysis
Data were analyzed using STATA version 15 software; besides, Microsoft Excel 2019 was also employed to clean, edit, and code the data. Descriptive statistics such as frequency and percentages were calculated for categorical variables, and mean ± SD (standard deviation) was considered for continuous variables. A binary logistic regression was run to explore the socio-demographic factors affecting the level of knowledge (adequate and inadequate), perception (positive and negative), and attitude (positive and negative). Besides, a multinomial logistic regression was employed to identify the factors responsible for vaccine acceptability (yes/no/not sure). A p-value < 0.01, and 0.05 were considered to prove statistical significance at 1%, and 5% level, respectively.
Ethical approval
This study did not require any ethical approval since all human involvements were ensured following local legislation and institutional concern. Besides, all proceeds of this study were conducted as per the Helsinki Declaration principles of the human subject survey.
Empirical results
Socio-demographic and clinical characteristics of selected respondents
Table 1 illustrates the socio-demographic and clinical characteristics of the studied participants. The mean age was 23.95 years, while almost six out of ten students were undergraduate. Among the respondents, more than half (55.8%) were males, and the rest (44.2%) were females. As per monthly family income, the maximum number of respondents (58.9%) were from the lower-middle income group, while only 4.4% were from the high-income group. Nearly more than half of the respondents (54%) were from the urban area, whereas 26.2% were from the rural area, and the remainder of the respondents were semi-urban dwellers. All of the respondents stated that they had heard about the COVID-19 vaccine. The most commonly mentioned sources from where they first heard about the COVID-19 vaccine were social media (41.1%), followed by television/radio. While inquiring about the COVID-19 infection, 63.6% of individuals, either themselves or any of their family members, were unaffected by the COVID-19.
Knowledge about the COVID-19 vaccine
Table 2 reveals the level of knowledge related to the COVID-19 vaccine. Approximately 58.4% of participants reported that they were aware of the name of the app/website that required to register for the vaccine. More than half of the participants were cognizant of mandatory vaccination for all public university students. Almost seven out of ten participants were updated about the vaccines that had been approved for emergency use, while the majority (85.1%) of the participants accurately responded to the number of vaccine doses required for each person. About two-thirds of the participants accurately mentioned the schedule when Bangladesh Government started mass vaccination. The majority (89.1%) of participants knew about the country from where the Bangladesh government received the first vaccine consignment. More than half of the participants correctly reported the number of countries or institutes that got approval for vaccine production. However, 60.2% of participants could not accurately answer the number of vaccine doses that Bangladesh has assured for priority contracts with the SII. Almost all the participants could recognize the pharmaceutical company which collaborated with the government on the vaccination campaign. Eventually, the overall knowledge score was found 3.21 ± 4.13 (mean ± SD).
Perceptions about COVID-19 vaccine
Table 3 illuminates that more than half of the participants were uncertain whether the COVID-19 vaccine is effective, while 34% were optimistic about the vaccine efficacy and 9.8% were equivocal. This study found 70.2% of participants were worried about the side effects, whereas 17.6% remained neutral in this regard. However, 12.2% of participants were indifferent to the potential repercussions. Surprisingly, 7.6% of respondents concurred that the pandemic is reversible without vaccines. Notwithstanding, the preponderance (62.4%) of the respondents did not assume that antibiotics can cure the disease as an alternative of any vaccine, while 8.4% perceive that antibiotics can heal the COVID-19 disease. When we asked the participants whether they believe that the COVID-19 vaccine can only be applied to people infected with coronavirus, most of them (53.8%) refuted the statement, whereas the rate of approbation and ambiguity was 10.7% and 35.6%, respectively. The least portion (7.6%) of respondents acceded that eating nutritious food can boost one’s immune system, which eventually can outperform the vaccine. Around three out of ten students contemplate that vaccine is more appropriate for patients with chronic disease. Meanwhile, exactly half of the respondents are confident regarding the demise of the pandemic with the help of vaccines.
Attitude toward COVID-19 vaccine
While posing inquiries about the student’s attitude toward the COVID-19 vaccine, we observed that about 35% of them were unsure about whether their families would allow them to get vaccinated. A somewhat share of members (2.7%) strongly disagreed that the COVID-19 vaccine can bring them back to classrooms, while 32% reported being uncertain about the matter (Table 4). A large portion (37.8%) was found to be doubtful regarding the statement that they might be affected by COVID-19 if they do not receive a COVID-19 vaccine. In contrast, almost the same pie (18.9% and 15.8% individually) of participants strongly agreed and agreed with this statement. Even being university students, a negligible portion (16%) strongly agreed with the statement “COVID-19 vaccine must be mandatory for all students before university reopens,” and only 44% was agreed with this. A critical sum (31.1%) of individuals emphatically differ that they can easily have a COVID-19 vaccine, and 28.2% disagree on the exact statement. More than a moiety of the participants expressed uncertainty about their being affected by COVID-19 if the university reopens without providing a vaccine. A large share of the participants concurred and emphatically accorded (43.1% and 26.7%, respectively) that they would regret if they become infected by coronavirus even after getting the vaccine. The least portion of the participants (approximately 11%) somewhat disagreed with that matter. An observable portion of the respondents (38.7%) firmly admitted their concern since the vaccine is too new, while only 15% of respondents differed, followed by 18.7% who remained skeptical.
Level of knowledge, perceptions, and attitude of COVID-19 vaccine
It is a matter of concern that, despite most of the students hold adequate knowledge and positive attitudes toward the vaccine, a significant portion of them (38%) demonstrated negative perceptions toward the vaccine (Figure 1). However, 78% of participants possess adequate knowledge about the COVID-19 vaccine, and 86% of respondents showed a positive attitude toward the COVID-19 vaccine.
Figure 1.

Percentage of respondents having adequate knowledge, positive perceptions, and attitude.
COVID-19 vaccine acceptability
Despite the fact that almost three-quarters of the respondents stated that they intended to receive the vaccine, still a considerable portion of them had hesitancy about it, while 5.7% of them were directly notified to refuse the vaccine (Figure 2).
Figure 2.

COVID-19 vaccine acceptability among the respondents (N = 900).
As depicted in Figure 3, the most prevalent reason to refuse the COVID-19 vaccine was that the students were dubious about the vaccine’s safety and efficacy (33.6%) and the potential side effects of the vaccine (6.7%). Besides, 11.4% of respondents reported not having sufficient information about the quality of the currently available vaccine was the prime reason for hesitancy. Surprisingly, some of the respondents (3.9%) claimed that they do not require any vaccine to combat the COVID-19.
Figure 3.
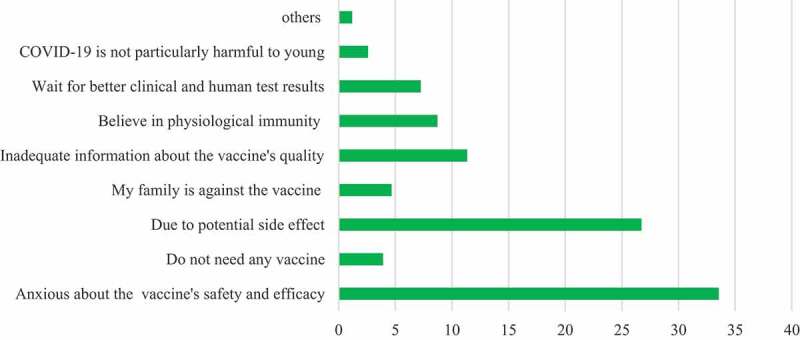
Reasons for refusing to receive COVID-19 vaccine in percentage. The reasons were asked only if the respondents were not interested in receiving the vaccine or not sure (N = 246).
Factors affecting knowledge, perceptions, attitude, and vaccine acceptability
Table 5 illuminates the factors affecting students’ knowledge, perception, and attitude regarding the vaccine. The finding signifies that elderly students were more likely to have a positive attitude toward the vaccine. Students from semi-urban and urban settlements were more likely to possess vaster knowledge and are more optimistic about the vaccine. However, education level also seemed to have a significant effect on their knowledge, perception, and attitude toward the vaccine. We observed that those enrolled in the postgraduate level have a greater likelihood to contain adequate knowledge scores and were more confident about the vaccine. The odds of having greater knowledge and a positive attitude regarding the vaccine were higher among the previously infected students than those not affected by the coronavirus.
Table 5.
Logistic regression showing factors significantly affect the respondent’s knowledge, perception, and attitude toward the COVID-19 vaccine (N = 900)
| Knowledge |
Perception |
Attitude |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Categories | Coef. | AOR | P-value | Coef. | AOR | P-value | Coef. | AOR | P-value |
| Age | 0.05 | 1.05 | .14 | 0.12 | 1.51 | .19 | 0.12 | 1.20 | .00*** | |
| Sex | Male (Ref.) | |||||||||
| Female | 0.20 | 1.23 | .41 | 0.05 | 1.05 | .76 | 0.10 | 1.11 | .54 | |
| Residence area | Rural (Ref.) | |||||||||
| Urban | 1.27 | 3.58 | .00*** | 1.04 | 2.85 | .00*** | 0.21 | 1.23 | .18 | |
| Semi-urban | 0.35 | 1.42 | .04** | 0.65 | 1.91 | .00*** | 0.17 | 1.19 | .42 | |
| Economic class | Low income (Ref.) | |||||||||
| Lower-middle income | 0.73 | 2.01 | .12 | 1.89 | 3.25 | .33 | 0.56 | 1.93 | .29 | |
| Upper-middle income | 0.43 | 1.87 | .17 | 1.45 | 2.88 | .46 | 0.51 | 1.76 | .22 | |
| High income | 0. 23 | 1.01 | .28 | 1.34 | 2.09 | .57 | 0.04 | 1.55 | .37 | |
| Participants category | Undergraduate (Ref.) | |||||||||
| Postgraduate | 1.01 | 2.44 | .00*** | 0.59 | 1.84 | .00*** | 0.19 | 1.21 | .00*** | |
| COVID-19 infected | No (Ref.) | |||||||||
| Yes | 0.15 | 1.31 | .04** | 0.14 | 1.14 | .82 | 0.36 | 1.25 | .03** | |
| Did not test | 0.39 | 1.37 | .00*** | 0.16 | 1.18 | .50 | 0.86 | 1.42 | .00*** | |
***, and ** indicates significance at 1%, and 5% level, respectively. In logistic regression, dependent variables are knowledge (1 if having adequate knowledge, 0 for otherwise), perception (1 if having positive perception, 0 for otherwise), and attitude (1 if having positive attitude, 0 for otherwise). AOR = Adjusted Odds Ratio, Ref. = Reference category, Coef. = Coefficient.
Meanwhile, factors involved in determining vaccine acceptance revealed from the multinomial logistic regression model are presented in Table 6. Female students seemed to be prone to vaccine defiance and hesitancy. Alongside, students of lower-income families were more likely to be hesitant toward the vaccine. Interestingly, the likelihood of vaccine resistance and vaccine hesitancy prevailed among students with no COVID-19 infection history. Putting it simply, a pre-infection history raised the vaccine acceptance rate among the studied population. Moreover, students with inadequate vaccine knowledge, negative perceptions, and negative attitudes toward the vaccine were more likely to refuse or equivocate a COVID-19 vaccine.
Table 6.
Multinomial logistic regression showing the factors influencing the vaccine acceptability (N = 900)
| Characteristics of participants | Vaccine acceptance (yes) = Reference |
|||
|---|---|---|---|---|
| Vaccine resistant (no) |
Vaccine hesitant (not sure) |
|||
| AOR (95% CI) | P-value | AOR (95% CI) | P-value | |
| Age (Years) | ||||
| 18 to 24 | 1.08 (0.71 to 2.15) | .28 | 1.13 (1.02 to 2.12) | .14 |
| More than 24 | 0.92 (0.60 to 1.94) | .17 | 1.62 (1.11 to 3.24) | .22 |
| Sex | ||||
| Male | 0.72 (0.23 to 1.78) | .62 | 0.94 (0.64 to 1.38) | .75 |
| Female | 1.87 (1.23 to 3.26) | .02** | 1.94 (1.43 to 2.89) | .00*** |
| Economic class | ||||
| Low income | 1.67 (1.17 to 5.30) | .09 | 1.67 (0.56 to 3.88) | .00*** |
| Lower-middle income | 1.39 (0.17 to 2.92) | .13 | 1.44 (0.79 to 3.65) | .22 |
| Upper-middle income | 3.58 (0.13 to 5.23) | .17 | 1.21 (0.78 to 1.83) | .54 |
| High income | 3.43 (0.11 to 4.34) | .25 | 1.39 (0.79 to 1.89) | .56 |
| Living area | ||||
| Urban | 0.77 (0.52 to 1.49) | .48 | 1.22 (0.81 to 1.89) | .21 |
| Rural | 1.92 (1.03 to 3.82) | .15 | 2.34 (1.28 to 4.56) | .10 |
| Semi-urban | 1.25 (0.81 to 1.95) | .11 | 1.09 (0.65 to 2.23) | .17 |
| Participants category | ||||
| Undergraduate | 0.72 (0.51 to 1.00) | .67 | 0.89 (0.61 to 1.22) | .59 |
| Postgraduate | 0.60 (0.36 to 1.02) | .72 | 0.55 (0.28 to 0.99) | .82 |
| COVID-19 affected | ||||
| No | 2.18 (1.11 to 5.54) | .04** | 2.23 (1.11 to 4.94) | .05** |
| Yes | 0.35 (0.16 to 1.09) | .06 | 0.63 (0.20 to 1.98) | .44 |
| Did not test | 1.44 (0.89 to 2.37) | .12 | 0.83 (0.54 to 1.27) | .29 |
| Knowledge about the COVID-19 vaccine | ||||
| Inadequate | 1.46 (0.82 to 2.59) | .00*** | 2.36 (1.03 to 4.40) | .00*** |
| Adequate | 1.26 (0.59 to 2.17) | .16 | 1.17 (0.67 to 2.04) | .18 |
| Perception of the COVID-19 vaccine | ||||
| Positive | 1.05 (0.53 to 1.65) | 1.23 (0.77 to 1.88) | ||
| Negative | 4.09 (1.19 to 10.48) | .04** | 5.31 (3.09 to 11.92) | .05** |
| Attitude toward COVID-19 vaccine | ||||
| Positive | 1.18 (0.62 to 2.17) | 1.77 (0.49 to 6.39) | ||
| Negative | 2.23 (1.14 to 8.09) | .00*** | 2.82 (1.04 to 7.78) | .02** |
***, and ** indicates significance at 1%, and 5% level, respectively. Multinomial logistic regression was employed to determine the significant factor influencing the vaccine-taking decision (dependent variable). The respondents who were not sure to take vaccine were termed as vaccine-hesitant, while those who refused were denoted as vaccine-resistant. The reference category was vaccine acceptance (respondents who are willing to be vaccinated). All predictors in the model are adjusted for all other covariates. AOR: adjusted odds ratios, 95% CI: 95% confidence intervals for the adjusted odds ratios.
Discussion
The resumption of the educational institutions of Bangladesh markedly depends on students’ willingness, perceptions, and attitudes toward the COVID-19 vaccine. However, knowledge regarding the vaccine can also play a vital part in influencing one’s willingness to be vaccinated. Since the inoculation schedule for public university students is in proximity, ambiguity or misconception about the vaccine among the students may impede the government’s efforts; that, in turn, can thwart the vaccine intake, ending in agitated outcomes. Under the circumstances, to the best of our knowledge, this is the first study to explore the COVID-19 vaccine acceptability with the investigation of vaccine-related knowledge, perceptions, and attitude among Bangladeshi public university students.
Our study included a nearly equal proportion of male (55.8%) and female (44.2%) students. Respondents were also sub-grouped as per their family income, area of residence, and previous history of COVID-19 infection. With no surprise, everyone was warried of the COVID-19 vaccine. Nevertheless, our study revealed that about 72% of the students intend to take a COVID-19 vaccine. The vaccine acceptance rate of public university students is higher than the previous study on the general people of Bangladesh,20 the study on French university students,21 the outcome on medical students in Southeast Michigan, USA,22 and the finding of Saied et al.23 regarding the COVID-19 vaccine acceptance. Recently, there is a change in people’s attitude toward vaccination, as most people want to get rid of this pandemic by any means. Therefore, the vaccination rate and intentions toward receiving a COVID-19 vaccine are on the rise. Yet, a significant pie of the students equivocates to receive a vaccine which can be ascribed to the fact that Bangladesh did not participate in the vaccine trials,24 which in turn, might reduce the confidence among students on the vaccine. Also, a negligible portion of Bangladesh’s total population has already received a vaccine, and there is always an impassivity about the vaccine among people. However, while exploring the reasons behind refusing the vaccine, we found that a substantial portion of the respondents (60.3%) reported that they were concerned about the vaccine’s safety, efficacy, and potential side effect. Therefore, it is critical to persuade them of the vaccine’s safety and efficacy. Several academics also agreed that public belief in the vaccine’s safety and efficacy should be attained during mass immunization campaigns.19,25 Otherwise, there is a risk that public interest in vaccination will wane, thereby jeopardizing herd immunity.
This study found that the preponderance of surveyed respondents learned about the COVID-19 vaccination mostly through social networking sites like Facebook, which corroborates a prior study conducted by Mannan and Mannan26 regarding COVID-19. This finding is further supported by the fact that the vast majority of Bangladeshi youth rely on social media and the internet as part of their daily lives, which has increased their exposure of COVID-19 facts, including vaccination information. Approximately four-fifths of the students found having adequate knowledge about the vaccine. Still, the finding appears to be worrisome since a noticeable pie (22%) of respondents lacks proper knowledge. A noteworthy portion of the students (41.6%) did not even know via which app vaccination registration is invited, and a remarkable portion of the respondents (42%) were not aware that the government had announced mandatory vaccination for them. It was expected that almost every respondent possess decent knowledge about the vaccine since all are students at the tertiary level with sufficient scholastic qualifications. This symbolizes a lack of self-awareness, which results in a dearth of knowledge about something.27
Since a substantial number of students have negative attitudes of the vaccine and a significant number of them lack sufficient understanding about the vaccine, the government should enlist the help of health care professionals and clinical interventions to raise vaccine awareness among students. It’s worth noting that healthcare experts’ recommendations and clinical pharmacist interventions can have a significant impact on knowledge, attitude, and perceptions, resulting in increased public confidence and understanding regarding any vaccine.28,29 However, on the other side of the coin, a substantial portion of the students (86%) showed a positive attitude toward the vaccine. Yet, a notable share of them reported that they might find it troublesome to get inoculated. Obviously, vaccine distribution programs might face unsteadiness without skilled public health workers for a heavily populous country like Bangladesh. In addition to this, some culprits are trying to deceive people by spreading rumors via social network platforms regarding vaccine distribution and inoculation.27 Hence, persuasive cyber inspection is required to exterminate such crimes that may obstruct people from taking the vaccine.
Interestingly, students from rural regions proved to carry inferior knowledge compared to those of urban and semi-urban. Parallel to this finding of Banik et al.30 underlined the area of residence remarkably affects Bangladeshi people’s knowledge about COVID-19 related issues. This can be attributed to rural sites’ inadequate internet connections and technological lags of Bangladesh.31 Appending to this, since the surrounding ambiance in the village area is not as dynamic and civilized as that of cities, this can impede the students from the exposure of wide-spaced learning of real life. Results also depicted that respondents being infected by the COVID-19 are more likely to have vaster knowledge and a more positive attitude. It is apparent since having experience of a disease makes a human being more aware and conscious.32 Besides, they were more frequently in touch with the healthcare professionals during their infection period, which boosted their knowledge and attitude toward coronavirus and its vaccines. However, senior students at the postgraduate level scored higher in knowledge, perception, and attitude regarding the COVID-19 vaccine than the juniors (undergraduate level). This is unsurprising given that senior citizens are more worried about health issues and have a greater understanding of the continuing pandemic-related issues. This is synonymous with the COVID 19-related finding of Banik et al.30 and Erfani et al.33
Moreover, this study also explored the factors associated with vaccine hesitancy and resistance. The results unearthed that female students are more likely to refuse and equivocate a COVID-19 vaccine, which are consistent with the findings of a study on Greek adults, found that females are more hesitant to a COVID-19 vaccine.34 The finding regarding having adequate knowledge and positive perceptions enhance vaccine acceptability align with the previous study.35 The study of Sherman et al.18 claimed that having positive attitudes toward COVID-19 vaccines can augment vaccine acceptance, which supports our finding relating negative association of attitudes toward a COVID-19 vaccine with vaccine hesitancy and resistance. Nevertheless, our study revealed a strong link of vaccine acceptability with knowledge, perceptions, and attitudes that should be the prime concerns during the vaccination program.
Our study has certain shortcomings that can be overcome in the future. Firstly, because the survey was conducted online, many students in rural places with poor internet connections were unable to participate. A face-to-face interview may have elicited additional information from a more diverse set of responders. Second, we exclusively included students from public universities in our research. Further research may be undertaken on various target populations, such as general public, health workers, businesspeople, women, and so on. Thirdly, despite the fact that our participants showed a lack of knowledge, our sample was regarded well-educated respondents. As a result, the findings cannot be applied to the entire Bangladeshi population. It can, however, be applied to populations with similar educational and socio-demographic backgrounds. Despite these limitations, our findings reveal important information on students’ knowledge and willingness to receive the COVID-19 vaccine. These findings will be beneficial in developing effective strategies for implementing a successful vaccination program in place.
Concluding remarks and recommendations
From lives to economy, economy to education, COVID-19 has left its blackened footprint. Bangladesh’s education system is one of the worst victims of the pandemic. The Bangladesh government has decided to make vaccinations obligatory before the recommence the normal educational system. Nonetheless, student cooperation is crucial to the successful execution of this vaccination campaign. In light of this, our study attempted to explore vaccination acceptability among students, as well as their knowledge, perceptions, and attitudes concerning the COVID-19 vaccine. We also set out to identify the factors that influence vaccination hesitation and resistance, as well as the factors that influence knowledge, perception, and attitude toward the vaccine. The outcomes revealed that most students have adequate knowledge about the vaccination, yet a substantial number of the respondents have a negative perception of the vaccine. Furthermore, the majority of the students are eager to receive the vaccination and have a positive mentality regarding it. Our findings show that vaccination hesitancy is significantly associated to socio-demographic characteristics as well as knowledge, perceptions, and attitude about the COVID-19 vaccine; hence, it is critical to enhance students’ intentions regarding the COVID-19 vaccine by awareness raising campaigns. To convince the hesitant and resistant respondents about the importance of COVID-19 vaccination, crucial actions taken by the government involving medical practitioners, health workers, teachers, and students’ associations are necessary.
Funding Statement
The author(s) reported there is no funding associated with the work featured in this article.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data may be available from the corresponding author upon request.
References
- 1.Andre FE, Booy R, Bock HL, Clemens J, Datta SK, John TJ, Lee BW, Lolekha S, Peltola H, Ruff TA, et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. 2008;86:140–46. https://www.scielosp.org/article/bwho/2008.v86n2/140-146/en/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Businessinsider . Here’s how the top 3 coronavirus vaccines compare when it comes to efficacy, cost, and more. 2020. [accessed 2021 Apr 11]. https://www.businessinsider.com/how-covid-vaccines-compare-cost-astrazeneca-oxford-pfizer-biontech-moderna-2020-11.
- 3.Logunov DY, Dolzhikova IV, Shcheblyakov DV, Tukhvatulin AI, Zubkova OV, Dzharullaeva AS, Kovyrshina AV, Lubenets NL, Grousova DM, Erokhova AS, et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. The Lancet. 2021;397(10275):671–81. doi: 10.1016/S0140-6736(21)00234-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bhutta ZA, Basnyat B, Saha S, Laxminarayan R.. Covid-19 risks and response in South Asia. BMJ. 2020;368:m1190. doi: 10.1136/bmj.m1190. [DOI] [PubMed] [Google Scholar]
- 5.Banik R, Rahman M, Sikder T, Gozal D.. COVID-19 in Bangladesh: public awareness and insufficient health facilities remain key challenges. Public Health. 2020;183:50. doi: 10.1016/j.puhe.2020.04.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.DW . COVID: Bangladesh faces vaccine shortage as India halts exports. 2021. [accessed 2021 Mar 30]. https://www.dw.com/en/Bangladesh-India-coronavirus-vaccine/a-57200281.
- 7.The Daily Star . Bangladesh to get 1.28 crore vaccines from COVAX programme. 2021. [accessed 2021 Apr 20]. https://www.thedailystar.net/coronavirus-deadly-new-threat/news/Bangladesh-get-128-crore-vaccines-the-covax-programme-2038805.
- 8.The Daily Star . An impressive start to covid vaccination in Bangladesh. 2021. [accessed 2021 Apr 20]. https://www.thedailystar.net/opinion/macro-mirror/news/impressive-start-covid-vaccination-Bangladesh-2044789.
- 9.Dhaka Tribune . Bangladesh likely to get ‘Covidshield’ vaccine in January. 2020. [accessed 2021 Mar 29]. https://www.dhakatribune.com/health/coronavirus/2020/12/08/Bangladesh-likely-to-get-covidshield-vaccine-in-jan.
- 10.Islam MS, Tusher TR, Roy S, Rahman M. Impacts of nationwide lockdown due to COVID-19 outbreak on air quality in Bangladesh: a spatiotemporal analysis. Air Qual Atmos Health. 2021;14(3):351–63. doi: 10.1007/s11869-020-00940-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.The Business Standard . Educational institutions to remain closed till March 31 2020. [accessed 2021 Apr 15]. https://www.tbsnews.net/Bangladesh/education/govt-orders-closure-all-educational-institutions-march-17-56947.
- 12.UGC . List of public universities. 2021. [accessed 2021 Mar 27]. http://www.ugc-universities.gov.bd/public-universities.
- 13.The Daily Star . Universities to reopen on May 24, halls on May 17 2021 [accessed 2021 Apr 20]. https://www.thedailystar.net/country/news/universities-reopen-may-24-halls-may-17-2049173.
- 14.DW . COVID: Bangladesh vaccination drive marred by misinformation. 2021. [accessed 2021 Mar 30]. https://www.dw.com/en/covid-Bangladesh-vaccination-drive-marred-by-misinformation/a-56360529.
- 15.Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. 2020;35(8):781–83. doi: 10.1007/s10654-020-00670-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mant M, Aslemand A, Prine A, Jaagumägi Holland A. University students’ perspectives, planned uptake, and hesitancy regarding the COVID-19 vaccine: a multi-methods study. PloS One. 2021;16(8):e0255447. doi: 10.1371/journal.pone.0255447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Le An P, Nguyen HTN, Nguyen DD, Vo LY, Huynh G. The intention to get a COVID-19 vaccine among the students of health science in Vietnam. Hum Vaccin Immunother. 2021;1–6. doi: 10.1080/21645515.2021.1981726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sherman SM, Smith LE, Sim J, Amlôt R, Cutts M, Dasch H, Rubin GJ, Sevdalis N. COVID-19 vaccination intention in the UK: results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum Vaccin Immunother. 2021;17(6):1612–21. doi: 10.1080/21645515.2020.1846397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Neumann-Böhme S, Varghese NE, Sabat I, Barros PP, Brouwer W, van Exel J, Schreyögg J, Stargardt T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Health Econ. 2020;21:977–82. doi: 10.1007/s10198-020-01208-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hossain E, Rana J, Islam S, Khan A, Chakrobortty S, Ema NS, Bekun FV. COVID-19 vaccine-taking hesitancy among Bangladeshi people: knowledge, perceptions and attitude perspective. Hum Vaccin Immunother. 2021:1–10. doi: 10.1080/21645515.2021.1968215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tavolacci MP, Dechelotte P, Ladner J. COVID-19 vaccine acceptance, hesitancy, and resistancy among university students in France. Vaccines. 2021;9(6):654. doi: 10.3390/vaccines9060654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health. 2021;43(3):445–49. doi: 10.1093/pubmed/fdaa230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Saied SM, Saied EM, Kabbash IA, Abdo SAEF. Vaccine hesitancy: beliefs and barriers associated with COVID‐19 vaccination among Egyptian medical students. J Med Virol. 2021;93(7):4280–91. doi: 10.1002/jmv.26910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ali M, Hossain A. What is the extent of COVID-19 vaccine hesitancy in Bangladesh?: a cross-sectional rapid national survey. medRxiv. 2021. doi: 10.1101/2021.02.17.21251917v1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jiang S. Don’t rush to deploy COVID-19 vaccines and drugs without sufficient safety guarantees. Nature. 2020;579:321–321. doi: 10.1038/d41586-020-00751-9. [DOI] [PubMed] [Google Scholar]
- 26.Mannan DK, Mannan KA. Knowledge and perception towards Novel Coronavirus (COVID 19) in Bangladesh. Int Res J Bus Soc Sci. 2020;6(2). doi: 10.2139/ssrn.3578477. [DOI] [Google Scholar]
- 27.Courtney MA. What is self-awareness and why is it important. PositivePsychology; 2021. [accessed 2021 Mar 28]. https://positivepsychology.com/self-awareness-matters-how-you-can-be-more-self-aware/.
- 28.Khalili H, Mohebbi N, Hendoiee N, Keshtkar AA, Dashti-Khavidaki S. Improvement of knowledge, attitude and perception of healthcare workers about ADR, a pre-and post-clinical pharmacists’ interventional study. BMJ Open. 2012;2(1):e000367. doi: 10.1136/bmjopen-2011-000367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lau M, Lin H, Flores G. Factors associated with human papillomavirus vaccine-series initiation and healthcare provider recommendation in US adolescent females: 2007 National Survey of Children’s Health. Vaccine. 2012;30(20):3112–18. doi: 10.1016/j.vaccine.2012.02.034. [DOI] [PubMed] [Google Scholar]
- 30.Banik R, Rahman M, Sikder MT, Rahman QM, Pranta MU. Knowledge, attitudes, and practices related to the COVID-19 pandemic among Bangladeshi youth: a web-based cross-sectional analysis. J Public Health. 2021:1–1. doi: 10.1007/s10389-020-01432-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.The Daily Star . 54% Bangladeshi rural household lacks internet access: survey. 2020. [accessed 2021 Apr 19]. https://www.thedailystar.net/country/news/54-bangladeshi-rural-households-lack-internet-access-survey-1960661.
- 32.Roche . Disease awareness and access to healthcare. 2021. [accessed 2021 Apr 14]. https://www.roche.com/sustainability/access-to-healthcare/our-approach/disease-awareness.htm.
- 33.Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;30(10.2471). doi: 10.2471/BLT.20.251561. [DOI] [Google Scholar]
- 34.Holeva V, Parlapani E, Nikopoulou VA, Nouskas I, Diakogiannis I. COVID-19 vaccine hesitancy in a sample of Greek adults. Psychol Health Med. 2021:1–7. doi: 10.1080/13548506.2021.1948579. [DOI] [PubMed] [Google Scholar]
- 35.Chaudhary FA, Ahmad B, Khalid MD, Fazal A, Javaid MM, Butt DQ. Factors influencing COVID-19 vaccine hesitancy and acceptance among the Pakistani population. Hum Vaccin Immunother. 2021:1–6. doi: 10.1080/21645515.2021.1944743. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data may be available from the corresponding author upon request.