

ABSTRACT
The effect of the coronavirus disease (COVID-19) pandemic on routine vaccination in low- and middle-income countries are scarce. The current pandemic has disrupted routine immunization globally. We aimed to analyze the effect of COVID-19 pandemic on routine immunizations practice in Pakistan. A retrospective study was conducted. The data were extracted from the immunization registry in order to assess the disruption in routine immunization coverage during 5 months of the lockdown period. We compared 5 months post lockdown against the baseline period of 5 months preceding lockdown. To broaden the horizon of our research we also collected data of vaccination from rural areas within the country. The results of the current study showed that on average, there was a disruption in routine immunization by 36% during lockdown when compared with the prepandemic period. The largest decline was observed for measles vaccination with a decline of 48%. In rural areas there was a lower decline in vaccination coverage with the highest decline noted for rotavirus vaccination of 15%. This monthly decrease in routine vaccination continued to be at a decline for several months during lockdown; however, it slightly increased post lockdown. In conclusion, on average, there was more than 30% declined in routine vaccination during the lockdown period, while somewhat improved post lockdown, i.e. 12%. Thus, this ongoing pandemic is a reminder for the national immunization programs to consider to tackle the disruption in routine immunization, otherwise, this continued disruption may lead to secondary outbreaks of vaccine preventable diseases amongst the public.
KEYWORDS: COVID-19, routine immunization, disruption, child health, vaccine preventable disease
Background
The global mortality and morbidity of coronavirus disease 2019 (COVID-19) is still increasing day by day, but the effect of the COVID-19 pandemic on other health care services is poorly described, especially in developing countries1. Stay at home orders, diversion of resources, interruption of supply chains during COVID-19 lockdown have drastic effects on existing public health care services.1–3 COVID-19 is disrupting routine health services including life-saving childhood immunization globally. This disruption in immunization program may lead to outbreaks of vaccine-preventable diseases (VPDs) especially in low- and middle-income countries.4 It has been observed worldwide that many countries have suspended preventive routine immunization campaigns against disease such as polio, measles, mumps, diphtheria, meningitis and pertussis during COVID-19 lockdown; therefore, millions of children lives are at risk of VPDs.5
Although most of the countries have eradicated all the three types of polioviruses, but only Pakistan and Afghanistan, are still the polio endemic countries in the whole world.6 The impact of COVID-19 pandemic on routine immunization is prominence. It could potentially lead to a secondary outbreak due to vaccine-preventable diseases in low- and middle-income countries. Out of 73 Gavi-eligible countries, 71 have been impacted by the Severe acute respiratory syndrome coronavirus (SARS-CoV-2) with India, Indonesia, Bangladesh, and Pakistan reported the highest number of cases.7 Unfortunately, these countries also have the highest number of children with zero dose of vaccinations. In Pakistan, 66% children have fully immunized as per the immunization schedule. Vaccine campaign have been impacted due to current crises in 42 countries.7,8
Shifts in routine health services occurred due to following lockdown measures, force from parents to suspend routine childhood vaccinations, governments also have reallocate resources from vaccination centers to the COVID-19 response.8,9 In Pakistan, approximately 6260 health care workers involved in Polio Eradication Program have been shifted to help combat COVID-19 for better health communication, contact tracing, and improving testing capacities.10 However the national Polio helpline has also engaged in the provision of COVID-19 related information.10 Pakistan suspended all supplementary immunization activities on March 26, 2020 under the instructions of global polio eradication initiative. Since lockdown, approximately 40 million children missed the polio vaccination nationwide.11
Thus currently, SARS-CoV-2 is not the only infectious agents to be tackled, there are also challenges of immunization against vaccine-preventable diseases (VPDs). In 2019, the emergence of measles outbreak in the shadow of the Ebola epidemic killed twice as much as Ebola by attacking 341,000 individuals in the Democratic Republic of Congo.12,13 Likewise, in Samoa 83 deaths were resulted from measles outbreak after 50% drop off in vaccination.14 Thus, the emergence of such outbreak in the era of COVID-19 pandemic has added an supplementary burden on the healthcare systems.12 Experience from these prior outbreaks are lessons for maintenance of vaccination services.
Herd immunity is lifeblood in vaccine preventable disease to protect the unvaccinated population.15 Nonetheless, the current crisis placed herd immunity at risk for population with dropdown in routine vaccination coverages.5,16 Therefore, giving complexity of this issue the current study will helpful for expanded program on immunization, policy makers and health authorities to identify robust strategies in order to scale-up missed vaccination coverage. Examining the drifts in childhood vaccination will provide a key insight for parents to vaccinate their children with accelerated efforts.
Past studies have investigated the genomic characteristics of the virus,17 patients admission in hospital during COVID-19,18 and hospital mortality.19 Presently, there is very few information related to the routine immunization during the COVID-19. As routine health services remain to be disrupted, so it is necessary to understand the impact on routine immunizations. Therefore, the current study research question is: “Does the COVID-19 pandemic have an impact on routine immunization in Pakistan? The aim of the current study was to evaluate the impact of COVID-19 lockdown on routine immunization coverage during lockdown period and after lockdown period in comparison with a baseline period.
Methods
Study design and population
This retrospective cohort study was conducted in the teaching hospital of Khyber-Pakhtunkhwa, Pakistan. The study population included of children under 5 year of age in both urban and rural areas of Khyber Pakhtunkhwa province, Pakistan.
Data source and procedure
The data was extracted from the Hospital Immunization Registry in order to assess the changes in routine immunization coverage during 5 months COVID-19 lockdown period, 5 months post lockdown period. This was compared against the baseline/reference period 5 months prior to lockdown. Only data from the routine immunization that were provided in hospital was included. Rural area were also included to estimate the dropout in routine childhood vaccination.
To compare the monthly vaccination rates, the period from 01 November 2019 to the end of March, 2020 was defined as pre-lockdown 5. The period from 01 April 2020 to end of August, 2020 was defined as COVID-19 lockdown period . The timeframe from September, 2020 to January, 2021 was identified as post-lockdown. All of the phases lasted for a time frame of 5 months each. Pre COVID-19 lockdown period was used as a reference period for comparison of monthly vaccination in onward period. Same time period was used for both urban and rural areas.
Vaccination schedule
Following 10 routine vaccinations were included in this study in accordance with Pakistan’s Routine Immunization schedule,20,21 as presented in Table 1. All these vaccinations covers 10 Vaccine Preventable Diseases in six visits including, Polio (OPV/IPV; Oral and Inactivated polio vaccine), Tuberculosis (BCG; Bacille Calmette Guerin), Diphtheria, Tetanus, Pertussis, Hepatitis B, Haemophilus influenza (penta; pentavalent vaccine), Pneumococcal diseases (PCV-10), Measles, and Rotavirus Diarrhea.
Table 1.
| Vaccine | Doses | Age for first dose | Time interval between doses |
||
|---|---|---|---|---|---|
| First to second | Second to third | Third to fourth | |||
| BCG | 01 | At birth | – | – | – |
| Hepatitis B | 01 | At birth | – | – | – |
| Polio (OPV) | 04 | At birth | 4–8 weeks | 4–8 weeks | 4–8 weeks |
| Pentavalent | 03 | 06 weeks | 4 weeks | 4 weeks | – |
| Pneumococcal | 03 | 06 weeks | 4 weeks | 4 weeks | – |
| Rotavirus | 02 | 06 weeks | 4 weeks | – | – |
| Polio (IPV) | 02 | 14 weeks | 4–8 weeks | – | – |
Statistical analysis
Data was presented in actual number and the mean was presented for continuous variables. The percentage of reduction in immunization visits was assessed descriptively with that of baseline period as a reference period. We used SPSS version 20 for data analysis and GraphPad Prism 5 for graphs.
Results
Childhood routine immunization during the initial lockdown was efficiently effected with reference to baseline period (prepandemic). However, the immunization process was resumed after lockdown, but it was still not as close enough to baseline period.
Information regarding hospital routine childhood immunizations before COVID-19 lockdown, during lockdown, and after first lockdown is presented in Table 2. During lockdown period we observed fairly decline in routine childhood immunization coverage ranging from 30.7% to 48.6%. In contrast, we observed a little decline (2.8%–20.2%) in the routine immunization after first lockdown. Measles immunization coverage during COVID-19 lockdown period was significantly decreased, i.e. 40.7% for first dose and 48.6% for second dose, thus substantially lower than baseline period. After lockdown the monthly vaccination were decreased from mean of 137 to 112 (17.8% decrease) for first dose of measles while second dose was decreased from 111 to 88 (20.2%). Vaccination of rotavirus infection during lockdown period was drop by more than 30%, while after easing lockdown, the coverage was scaled up to 15% decrease.
Table 2.
Average routine childhood immunization visits during pre-COVID-19 lockdown period (November, 2019–March, 2020), lockdown period (April–-August, 2020), postlockdown period (September, 2020–January, 2021)
| Vaccine type | Before lockdown (5 months) n (mean) | During lockdown (5 months) n (mean) | After lockdown (5 months) n (mean) | Percent change during lockdown % | Percent change after lockdown % |
|---|---|---|---|---|---|
| Measles Ia | 685 (137) | 406 (81) | 563 (112) | −40.7 | −17.8 |
| Measles IIa | 557 (111) | 286 (57) | 444 (88) | −48.6 | −20.2 |
| Rota I | 642 (128) | 441 (88) | 542 (108) | −31.3 | −15.6 |
| Rota II | 598 (119) | 391 (78) | 540 (108) | −34.6 | −9.6 |
| Pentavalent I | 656 (131) | 434 (86) | 565 (113) | −33.8 | −13.8 |
| Pentavalent II | 609 (121) | 390 (78) | 545 (109) | −35.9 | −10.5 |
| Pentavalent IIIa | 568 (113) | 356 (71) | 538 (107) | −37.3 | −5.2 |
| Polio+PCV-10 I | 640 (128) | 443 (88) | 561 (112) | −30.7 | −12.3 |
| Polio+PCV-10 II | 601 (120) | 399 (79) | 543 (108) | −33.6 | −9.6 |
| Polio+PCV-10 III | 562 (112) | 365 (73) | 546 (109) | −35.0 | −2.8 |
PCV-10: Pneumococcal 10-valent conjugate vaccine.
a: I: mean first dose; II: second dose; III: Third dose.
Pentavalent vaccine was markedly decrease during lockdown period, 33% decline in first dose, 35% in second dose, 37% decline in third dose. After lockdown the decline was observed little as 13% for first dose, 10% for second and 5% for third dose. A 31% decrease in average monthly polio and PCV 10 (first dose) immunizations was noted during the lockdown compared to reference period (before lockdown), and the reduction was 33% for second and 35% third dose. After first lockdown the immunization was observed about stable (2% decrease) for third dose of polio and PCV-10 (Table 2).
Monthly neonatal BCG vaccination counts during lockdown period was decrease (mean 90) as compared to reference period before lockdown (mean 124), while after initial lockdown this number was improved (mean 111) as shown in the Figure 1. During COVID-19 lockdown period the monthly hepatitis B vaccination was decrease to 88 (mean) in contrast to baseline period 126 (mean), but improved instantly as the government declined the first lockdown (Figure 2).
Figure 1.
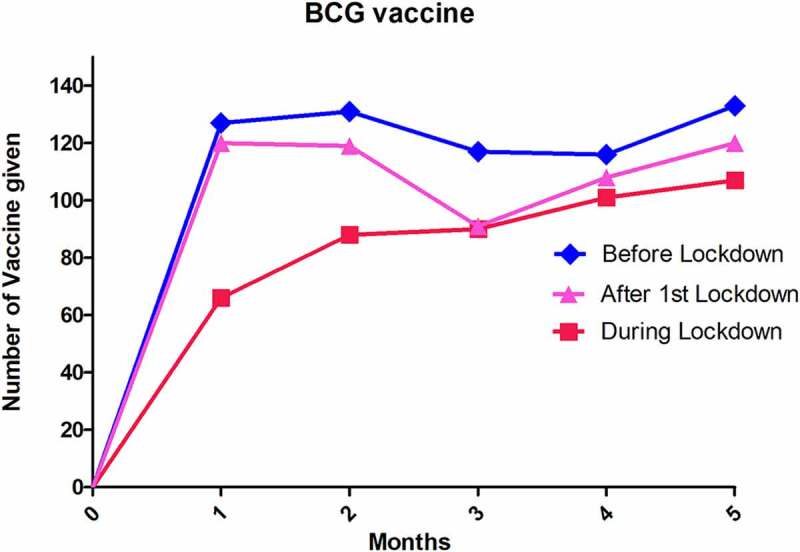
Variation in BCG monthly vaccination in pre-COVID-19, during COVID-19, post-COVID-19 lockdown period.
Figure 2.
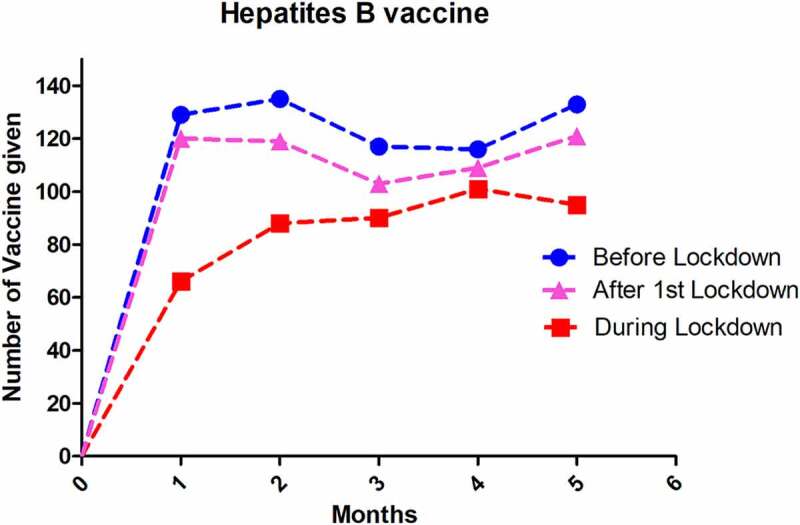
Hepatitis B immunization at birth in three different period.
Polio vaccination after birth vaccination followed a similar pattern in lockdown period as other BCG and hepatitis vaccine, varying months by months; particularly low counts (n = 66) in first month of lockdown. These decreased in monthly vaccination remained low for several months during first lockdown but rise slightly after lockdown (Figure 3).
Figure 3.
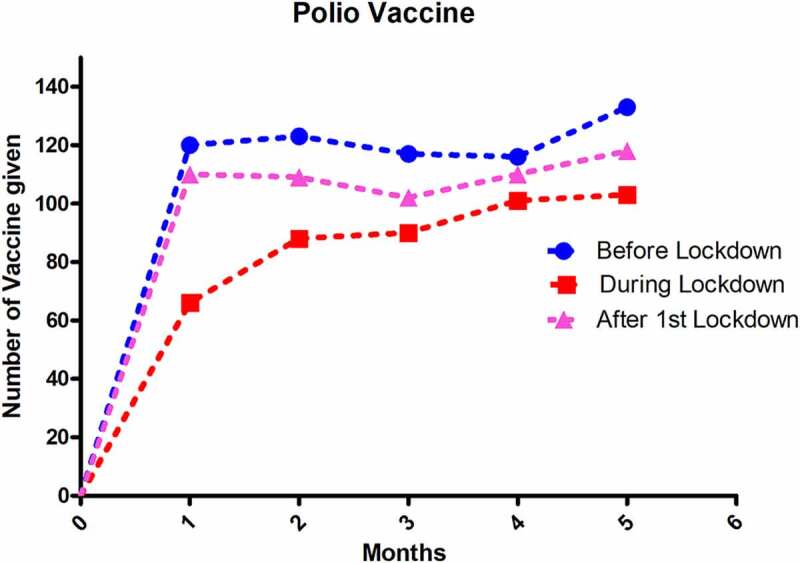
Monthly Polio immunization in three periods.
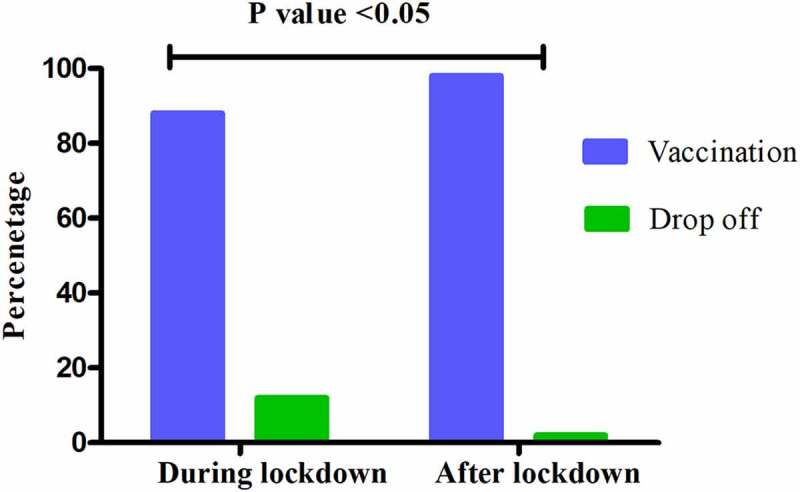
The routine immunization in rural areas were not much disrupted as compared to the urban areas during lockdown period (Table 3). The lockdown mostly affected rotavirus vaccination process, i.e. 15% for first dose, 13% for second dose followed by Polio and PCV-10 with 10.55%, 13.13%, and 12.04% for first, second, and third dose, respectively. There was a low drop off (5%) for measles vaccination during lockdown. After easing lockdown there was a steady recovery in coverage rates with absolute improvement in average immunization visits (<6% decrease during post lockdown period verses ≤15% decrease during lockdown period). In urban area, there was an average of 36% decline and 64% vaccination during the lockdown period, however, the vaccination increase to 88% with decline of 12% post lockdown. Difference between vaccination and drop off is statistically significant (p value <0.05) as shown in Figure 4. In rural area, there was an average of 12% decline and 88% vaccination during the lockdown period, while, the vaccination increased to 98% with only 2% decline post lockdown (p value <0.05) as shown in Figure 5.
Table 3.
Average routine childhood immunization visits in rural area during pre-COVID-19 lockdown period (November, 2019–March, 2020), lockdown period (April–August, 2020), postlockdown period (September, 2020–January, 2021)
| Vaccine type | Before lockdown (5 months) n (mean) | During lockdown (5 months) n (mean) | After lockdown (5 months) n (mean) | Percent change during lockdown % | Percent change after lockdown % |
|---|---|---|---|---|---|
| BCG | 584 (116) | 520 (104) | 571 (114) | −10.95 | −02.22 |
| Measles I | 497 (99) | 472 (94) | 496 (99) | −05.03 | −0.20 |
| Measles II | 450 (90) | 429 (85) | 446 (89) | −04.70 | −0.88 |
| Rota I | 559 (112) | 475 (95) | 545 (109) | −15.02 | −02.50 |
| Rota II | 538 (107) | 466 (93) | 528 (105) | −13.38 | −01.85 |
| Pentavalent I | 532 (106) | 481 (96) | 528 (113) | −09.58 | −0.75 |
| Pentavalent II | 510 (102) | 450 (90) | 508 (109) | −11.76 | −0.39 |
| Pentavalent III | 489 (105) | 437 (101) | 484 (96) | −10.63 | −01.02 |
| Polio+PCV-10 I | 578 (115) | 517 (103) | 546 (112) | −31.2 | −05.53 |
| Polio+PCV-10 II | 548 (109) | 476 (95) | 535 (108) | −13.13 | −02.37 |
| Polio+PCV-10 III | 523 (109) | 460 (107) | 518 (103) | −12.04 | −0.95 |
Figure 4.
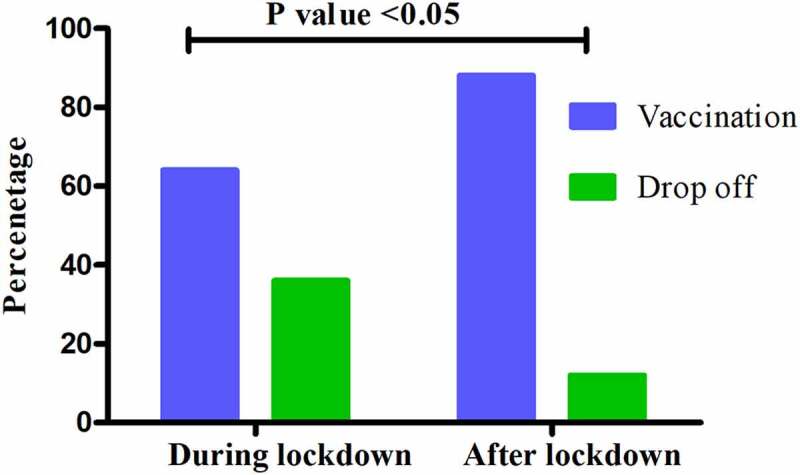
Average vaccination coverage during COVID-19 lockdown and post-COVID-19 lockdown in urban area.
Figure 5.
Average vaccination coverage during COVID-19 lockdown and post-COVID-19 lockdown in rural area.
Discussion
The current study showed that emergence of COVID-19 in Pakistan is coincided with substantial declines in routine immunizations, parallel to what has been noted nationally and globally.8,22 According to World Health Organization, the disruption of routine immunization pose a great risk of developing vaccine-preventable diseases to about 80 million children in 68 countries.4
In Pakistan, soon after birth of new born, BCG vaccination are mostly administered in the hospital. A significant declined in BCG immunization during lockdown was noted which can be either from reduced hospital visits due to fear of COVID-19, or implementation of a national lockdown by the government. Thus COVID-19 lockdown unintentionally affected the emergency obstetric care due to suspension of public transport, because public from low income countries still use public transport for emergency visits.23 The other possible reason for decline in both hepatitis B and BCG immunization is the low number of first postnatal hospital visits, as both these vaccine are often administered after birth. A study in India declared 66.4% decrease in referred obstetric emergencies during lockdown period which is due to social distancing, stay at home and hospital avoidance behavior among pregnant women.24 It is well established that coverage of routine immunization less than 90–95% put the herd immunity at risk in a population and may lead to the outbreak of vaccine preventable diseases. In Pakistan, polio immunization campaign is faced with numerous challenges, including inadequate health facilities, inaccessibility of subjects, administrative and organizational deficiencies, and missed vaccination due to refusals.25 These finding suggest that COVID-19 outbreak may have had unintentional consequences in terms of decline in childhood routine immunization in Pakistan. In present study, COVID-19 pandemic confirms the significant impact on child vaccination coverage during lockdown period based on reference period. The inactivated polio vaccine (IPV) drop off was 26% average decrease, throughout lockdown period, especially in March, 2020 as compared to prelockdown period of COVID-19. This finding was consistent with the recent study in Lebanon which claimed 48% drop in vaccination of inactivated polio vaccine during lockdown period as compared to pre-COVID-19 lockdown period.12 The current study result, in conjunction with previous studies, suggest that routine immunization have been adversely impacted by the current pandemic.22,26,27 According to Pakistan Polio Eradication Program poliovirus was detected in 60% sewage environmental sample in August 2020 while it was 43% in August 2019. There is marked increase over the last year that might be a future concern.28 So increase effort should be made to cover the unimmunized population.
Maintenance of routine immunization is essential to prevent post pandemic outbreak with vaccine preventable disease. In 2015 in Guinea multiple measles outbreaks happened due to disruption in routine immunization during the Ebola epidemic.29 So it is likely that such type of vaccine preventable disease like polio, measles, pertussis can occurred more than expected. It is estimated by WHO and UNICEF that about 80 million children are at risk of polio, measles and diphtheria due to disruptions caused by COVID-19 in routine immunization.4 As the first lockdown terminated the overall routine immunization gradually increased with low decrease as of baseline period. The improvement was actually due to ease of lockdown, opening of schools and resuming health care delivery other than COVID-19. The other plausible explanation is that after lockdown the routine immunization program was operating as usual.25
As the routine health services are also disrupted in urban areas, therefore it is important to understand the health services in rural areas. Interestingly, the data of the current study demonstrated less disruption in RI in rural areas as compared to urban areas. There may be three possible reasons related to this observation. Firstly, the routine health services in most of the teaching hospitals in cities was reallocated to COVID-19 service,30,31 while hospitals in the rural areas was functional as usual. Secondly, rural areas have less COVID-19 cases as compared to urban areas. Thirdly, COVID-19 lockdown measures were not strictly followed in rural areas as compared to urban areas of Pakistan.32,33
Social distancing measures shifts the health seeking behaviors, including immunization services. We observed more than 30% declined in pentavalent, oral polio vaccine, and pneumococcal-10 immunization for all three doses during lockdown period. However after easing lockdown these decline was reflected less than 14% for these vaccine.
While there is some concern that the social distancing measures may have an advantage to temporary prevent the transmissions of infectious diseases, including measles, pneumococcal disease, Hemophiles influenzae, Diphtheria and whooping cough.34 As these infection are transmitted through droplet or airborne,35 but this concern can be only for temporary drop down of this disease while once the restrictions are gradually relaxed it can be resulted an outbreak if a population remained unimmunized. Importantly, such type of assertion do not give an advantage for poliovirus and rotavirus because there transmission mode are fecal oral route instead of droplet. As we encountered an average of more than 30% disruption in both these immunization during lockdown period.
The other possible theme associated with disruption in routine immunization include: lockdown social isolation and social distance measure;27 staff shortage; problems in vaccine supply chain and border restriction;36 User concerns with fear of catching SARS-CoV-2, that is observed in Pakistan;8 unavailability of public transportation.37 These issues played a significant role in utilization of routine immunization.
Study strengths and limitations
The current study included vaccination coverage in hospitals, while there is lack of data regarding immunization in rural area which might be a valuable asset to the current study. An additional limitation was the low population target as the vaccination decline may be varying from overall population vaccination coverage.
To best of our knowledge, this is the first study that highlights the childhood routine immunization during lockdown in comparison with baseline period. The strength of the current study include the use of three different time period (pre-COVID-19, during COVID-19 and post-COVID-19 period) to assess the disruption and improvement in immunization during pandemic. This is an important for policy makers and public health department to implement health-care delivery in low-income country.
Conclusion
We concluded that COVID-19 pandemic have impact on disruption of routine immunization during lockdown, but was gradually improved after lockdown. There is an urgent need to immunize the children who missed the routine vaccination. The declines in routine childhood immunization could increase the risk of vaccine preventable diseases for children. Lesson should be learn from these finding to avoid disruption in routine immunization for countries under COVID-19 crises or in case of future epidemic or pandemic. This study will be a reminder for immunization program to sustain the immunization in area with high number of vaccine disruption.
Acknowledgments
We acknowledge, with thanks all the health care workers who work in Expanded Program on Immunization, Pakistan. We are thankful to Superintendent of teaching Hospital for approval of the study and data collection.
Funding Statement
There was no funding source for current study. The corresponding author of the study had full access to all the data and had final responsibility for the decision to submit for publication.
Author declarations
All authors have gone through and agreed to submission of this manuscript. We confirm that this work has not been published and is not under consideration for publication elsewhere.
Disclosure of potential conflicts of interest
No potential conflict of interest was reported by the author(s).
References
- 1.Dorward J, Khubone T, Gate K, Ngobese H, Sookrajh Y, Mkhize S, Jeewa A, Bottomley C, Lewis L, Baisley K, et al. The impact of the COVID-19 lockdown on HIV care in 65 South African primary care clinics: an interrupted time series analysis. Lancet HIV. 2021;8(3):e158–e165. doi: 10.1016/S2352-3018(20)30359-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fuentes-Alabi S. Effect of the COVID-19 outbreak on paediatric cancer care in low-income and middle-income countries. Lancet Child Adolesc Health. 2021;5:311–13. doi: 10.1016/S2352-4642(21)00058-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Munawar K, Choudhry FR.. Exploring stress coping strategies of frontline emergency health workers dealing Covid-19 in Pakistan: a qualitative inquiry. Am J Infect Control. 2021;49:286–92. doi: 10.1016/j.ajic.2020.06.214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Least A. Million children under one at risk of diseases such as diphtheria, measles and polio as COVID-19 disrupts routine vaccination efforts. Warn Gavi, WHO, UNICEF. [accessed 2020 Jul 2]. https://www.whoint/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef. [Google Scholar]
- 5.Dinleyici EC, Borrow R, Safadi MAP, van Damme P, Munoz FM. Vaccines and routine immunization strategies during the COVID-19 pandemic. Hum Vaccin Immunother. 2021;17:400–07. doi: 10.1080/21645515.2020.1804776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yusufzai A. Efforts to eradicate polio virus in Pakistan and Afghanistan. Lancet Child Adolesc Health. 2020;4:17. doi: 10.1016/S2352-4642(19)30382-7. [DOI] [Google Scholar]
- 7.GAVI . COVID-19 situation report #20; 2020.
- 8.Chandir S, Siddiqi DA, Mehmood M, Setayesh H, Siddique M, Mirza A, Soundardjee R, Dharma VK, Shah MT, Abdullah S, et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: an analysis of provincial electronic immunization registry data. Vaccine. 2020;38:7146–55. doi: 10.1016/j.vaccine.2020.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hirabayashi K. The impact of COVID-19 on the routine vaccinations: reflections during World Immunization Week 2020. Bangkok (THA): UNICEF-East Asia and Pacific; 2020. [Google Scholar]
- 10.GPEI . The first call”: polio eradication staff support COVID-19 response; 2020.
- 11.Din M, Asghar M, Ali M. Delays in polio vaccination programs due to COVID-19 in Pakistan: a major threat to Pakistan’s long war against polio virus. Public Health. 2020;189:1. doi: 10.1016/j.puhe.2020.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mansour Z, Arab J, Said R, Rady A, Hamadeh R, Gerbaka B, Bizri AR. Impact of COVID-19 pandemic on the utilization of routine immunization services in Lebanon. PLoS One. 2021;16(2):e0246951. doi: 10.1371/journal.pone.0246951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nachega JB, Mbala-Kingebeni P, Otshudiema J, Zumla A, Tam-Fum JJM. The colliding epidemics of COVID-19, Ebola, and measles in the Democratic Republic of the Congo. Lancet Global Health. 2020;8(8):e991–e992. doi: 10.1016/S2214-109X(20)30281-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Craig AT, Heywood AE and Worth H. Measles epidemic in Samoa and other Pacific islands. Lancet Infect Dis. 2020;20:273–75. doi: 10.1016/S1473-3099(20)30053-0. [DOI] [PubMed] [Google Scholar]
- 15.Rashid H, Khandaker G and Booy R. Vaccination and herd immunity: what more do we know? Curr Opin Infect Dis. 2012;25:243–49. doi: 10.1097/QCO.0b013e328352f727. [DOI] [PubMed] [Google Scholar]
- 16.Santoli JM. Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration—United States, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:591–93. doi: 10.15585/mmwr.mm6919e2. [DOI] [PubMed] [Google Scholar]
- 17.Lu R, Zhao X, Li J, Niu P, Yang B, Wu H, Wang W, Song H, Huang B, Zhu N, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–74. doi: 10.1016/S0140-6736(20)30251-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mesnier J, Cottin Y, Coste P, Ferrari E, Schiele F, Lemesle G, Thuaire C, Angoulvant D, Cayla G, Bouleti C, et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: a registry study. Lancet Public Health. 2020;5(10):e536–e542. doi: 10.1016/S2468-2667(20)30188-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, Dicker DJ, Chimed-Orchir O, Dandona R, Dandona L, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3:524–48. doi: 10.1001/jamaoncol.2016.5688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.WHO . WHO recommendations for routine immunization-summary tables. [accessed 2021 Jul 29]. https://wwwwhoint/teams/immunization-vaccines-and-biologicals/policies/who-recommendations-for-routine-immunization—summary-tables.
- 21.EPI . Expanded programme on immunisation. [accessed 2021 July 29]. http://www.epi.gov.pk/immunisation-schedule/.
- 22.Bramer CA, Kimmins LM, Swanson R, Kuo J, Vranesich P, Jacques‐Carroll LA, Shen AK. Decline in child vaccination coverage during the COVID‐19 pandemic—Michigan care improvement registry, May 2016‐May 2020. Am J Transplant. 2020;20:1930. doi: 10.1111/ajt.16112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wilson A, Hillman S, Rosato M, Skelton J, Costello A, Hussein J, MacArthur C, Coomarasamy A. A systematic review and thematic synthesis of qualitative studies on maternal emergency transport in low-and middle-income countries. Int J Gynecol Obstetrics. 2013;122:192–201. doi: 10.1016/j.ijgo.2013.03.030. [DOI] [PubMed] [Google Scholar]
- 24.Kumari V, Mehta K, Choudhary R. COVID-19 outbreak and decreased hospitalisation of pregnant women in labour. Lancet Global Health. 2020;8:e1116–e1117. doi: 10.1016/S2214-109X(20)30319-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ahmad S, Babar MS, Ahmadi A, Essar MY, Khawaja UA, Lucero-Prisno III DE. Polio amidst COVID-19 in Pakistan: what are the efforts being made and challenges at hand? Am J Trop Med Hyg. 2020;104(2):446. doi: 10.4269/ajtmh.20-1438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nuzhath T, Ajayi KV, Fan Q, Hotez P, Colwell B, Callaghan T, Regan AK. Childhood immunization during the COVID-19 pandemic in Texas. Vaccine. 2021;39(25):3333–37. doi: 10.1016/j.vaccine.2021.04.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Saso A, Skirrow H, Kampmann B. Impact of COVID-19 on immunization services for maternal and infant vaccines: results of a survey conducted by imprint—the immunising pregnant women and infants network. Vaccines. 2020;8:556. doi: 10.3390/vaccines8030556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pakistan Polio Eradication Programme APU . 2020. [accessed 2021 March 12]. https://www.endpolio.com.pk/images/poliobriefer/Pakistan-Polio-Update-August-2020.pdf.
- 29.Sell H, Assi A, Driedger M, Dubé E, Gagneur A, Meyer SB, Robinson J, Sadarangani M, Tunis M, MacDonald SE. Continuity of routine immunization programs in Canada during the COVID-19 pandemic. medRxiv. 2021;39:5532–37. doi: 10.1016/j.vaccine.2021.08.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Habib A, Anjum KM, Shehzad A, Imran M, Ashraf Z, Ramzan M. Outbreak of COVID-19 pandemic in Pakistan and the current scenario. Applied Biol Chem J. 2020;1:67–71. doi: 10.52679/tabcj.2020.0008. [DOI] [Google Scholar]
- 31.Saqlain M, Munir MM, Ahmed A, Tahir AH, Kamran S. Is Pakistan prepared to tackle the coronavirus epidemic? Drugs Ther Perspect. 2020;20:1–2. doi: 10.1007/s40267-020-00721-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ali A, Ahmed M, Hassan N. Socioeconomic impact of COVID‐19 pandemic: evidence from rural mountain community in Pakistan. J Public Aff. 2020;e2355. doi: 10.1002/pa.2355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Umer H, Khan MS. Evaluating the effectiveness of regional lockdown policies in the containment of Covid-19: evidence from Pakistan. arXiv preprint arXiv:200602987; 2020.
- 34.Hungerford D, Cunliffe NA. Coronavirus disease (COVID-19)–impact on vaccine preventable diseases. Eurosurveillance. 2020;25:2000756. doi: 10.2807/1560-7917.ES.2020.25.18.2000756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Simoes EA, Cherian T, Chow J, Shahid-Salles SA, Laxminarayan R, John TJ. Acute respiratory infections in children. In: Disease control priorities in developing countries. 2nd ed. Chapter 25. Co-published by Oxford University Press, New York. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006. https://www.ncbi.nlm.nih.gov/books/NBK11786. [PubMed] [Google Scholar]
- 36.UNICEF . Impact of COVID-19 on vaccine supplies; 2020.
- 37.Mukhtar S. Preparedness and proactive infection control measures of Pakistan during COVID-19 pandemic outbreak. Res Soc Administrative Pharm. 2021;17:2052. doi: 10.1016/j.sapharm.2020.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]