

1. Introduction
Approximately 20% of adults report having chronic pain [31; 34; 84; 115]. Unfortunately, response to treatments for chronic pain is often modest and can result in significant side effects including adverse events (AEs) [2; 18; 25; 38; 45; 65; 92; 110]. These realities highlight the need for more effective chronic pain interventions. One challenge in the development of novel treatments is balancing their benefits and risks. An example of this predicament involves the ongoing opioid crisis in the United States, which requires balancing the analgesic benefits of opioid medications with their significant risks, including persisting side effects, dependence potential, and risk of overdose [61; 70; 95; 97; 107; 116; 153]. Prescription opioid analgesics provide a timely example of the need to relieve pain while also protecting patients from the risks of pain interventions.
Benefit and risk data are not reported consistently in many randomized clinical trials (RCTs), including chronic pain trials, making it difficult to combine and compare results across studies [13; 37; 60; 63; 73; 75; 78; 79; 87; 111; 138; 139; 159]. Moreover, the primary outcomes in clinical trials often focus on treatment benefits (efficacy) rather than on risks such as AEs [27; 88]. This is often because studies are designed prospectively to have sufficient power to detect efficacy rather than identify risk [35]. In addition, benefits and risks of treatment are most commonly examined as separate outcomes in clinical trials, which cannot address whether there might be a relationship between the two [42]. For example, patients who benefit from an intervention could also be the same patients who are more (or less) likely to experience harms (i.e., correlated benefit and risk outcomes within the same patients).
Multiple frameworks and methods have been developed to account for benefit and risk outcomes in relation to each other in a combined metric rather than as separate outcomes [13; 21; 29; 30; 40; 54; 63; 87; 111; 112; 120; 122–124; 132; 146; 154]. These methods are diverse and can include qualitative and/or quantitative steps for combining benefits and risks for each treatment condition (group level assessment) [40; 48; 111]. Benefit-risk assessments can also be evaluated at the level of an individual patient and then compared across treatment conditions (individual level assessment) [12; 42; 53; 88; 93]. An additional advantage of benefit-risk assessments is that they can be tailored to best address the demands of a specific trial or other considerations such as patient subgroup differences (e.g., age, multimorbidity, type, and intensity of pain). However, the applicability of these benefit-risk composite measures across chronic pain clinical trials has not been adequately evaluated.
The present article provides an overview of the steps associated with benefit-risk assessments applied to pharmacological and non-pharmacological RCTs across a range of chronic pain conditions. Our aims are based on an Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) consensus meeting and are informed by a review of the benefit-risk assessment tools that have been used in published chronic pain trials and/or highlighted by key stakeholders (i.e., U.S. Food and Drug Administration, the European Medicines Agency, Cochrane, and Outcome Measures in Rheumatology [OMERACT]). Using this information combined with the collective expert opinion of the meeting participants, the present article provides considerations for benefit-risk assessment and reporting in RCTs of chronic pain.
2. Methods
Recommendations presented in this article were informed by a 2011 IMMPACT meeting organized by the Analgesic, Anesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks (ACTTION) public-private partnership with the FDA. The meeting addressed approaches for the assessment and interpretation of benefit-risk in chronic pain clinical trials and other related topics [137] (http://www.immpact.org/meetings/Immpact14/participants14.html). In addition, a review of published clinical trials of chronic pain treatments (pharmacological or non-pharmacological) was completed. A summary of the literature review findings are found in the Supplementary Information. Lastly, an internet search of publicly available documents was completed to identify publications and guidance related to benefit-risk assessments specific to chronic pain treatments. Professional organizations that were searched included the FDA, EMA, National Academies of Science, Engineering, and Medicine (NASEM), Cochrane, and Outcome Measures in Rheumatology (OMERACT; an independent initiative of international stakeholders interested in outcome measurement). The documents included for review comprised reports, publications, and white papers. Presentations, website content, or other informal methods of communication were excluded. Iterative revisions to preliminary drafts of this article were made until co-author consensus on its content was achieved.
3.2. Recommendations for Benefit-Risk Assessment from Regulatory Agencies and Professional Organizations
3.2.1. Cochrane.
The Cochrane Handbook addresses the importance of reporting the desirable and undesirable health outcomes of clinical trials (listed in order of importance) in the ‘Summary of findings’ tables included in each Cochrane Review [118]. In addition, the Handbook provides strategies for assessing benefits and AEs in the same review. For example, owing to differences in coding and categorization of AEs between studies, review authors are instructed to be alert to situations in which the coding of AEs splits data unnecessarily (e.g., pain in leg or arm), which may dilute the signal of a more global effect (e.g., all patients affected by pain). Likewise, authors are warned that combining AEs into a general outcome (e.g., total number of AEs) can only give a broad impression of effects and obscure important differences between the interventions. Lastly, Cochrane authors are instructed to include serious AEs (SAEs) in their reporting and note when safety data have not been adequately reported in the literature.
3.2.2. European Medicines Agency (EMA)
The EMA began a benefit-risk methodology project in 2009 [39; 40] (Supplementary Information). The final report was released in 2012 and recommended the use of the Problem formulation, Objectives, Alternatives, Consequences, Trade-offs, Uncertainties, Risk attitude, and Linked decisions (PrOACT-URL) qualitative framework for evaluating benefit-risk, as well as the inclusion of an ‘effects table’ for conveying benefit-risk information. The EMA also recommended that this qualitative framework be supplemented with a multi-criteria decision analysis (MCDA) quantitative approach in more complex situations [39; 40; 87; 163]. In addition, the EMA provided criteria for evaluating benefit-risk assessment tools and determining their contribution to various types of research [111; 120], including (1) logical soundness, (2) comprehensiveness (e.g., ability to handle uncertainty), (3) acceptability of results (e.g., ability to identify inconsistencies in the data and in people’s judgments, understandable and interpretable output from the analysis), (4) practicality (e.g., analysis is time efficient and can be taught to others easily), and (5) “generativeness” (e.g., the benefit-risk approach provides a clear audit trail and the results can be easily understood).
3.2.4. National Academies of Science, Engineering, and Medicine (NASEM)
Eight NASEM reports or workshop summaries that addressed benefit-risk were located (Supplementary Information). In 2014, the FDA and the Institute of Medicine (now NASEM) convened two public workshops on Characterizing and Communicating Uncertainty in the Assessment of Benefits and Risks of Pharmaceutical Products [77]. The workshops were designed to address uncertainty in pharmaceutical regulatory decision-making related to variability in human biology, drug chemistry, and clinical trial research. A focus of the summary included existing tools and approaches for communicating scientific uncertainties to a range of stakeholders invested in the results of pharmaceutical benefit-risk assessments (e.g., FDA; researchers in academia, government, and regulated industry; policymakers; patient groups; the public).
3.2.5. Outcome Measures in Rheumatology (OMERACT)
OMERACT is an international initiative aimed at improving outcome measurement across rheumatologic conditions, including efforts to simplify the simultaneous assessment of benefits and harms at the individual patient level (Table 1) [5; 11; 12; 134]. The OMERACT method, referred to as a 3X3 methodology, analyzes the benefits and harms simultaneously at the individual patient level (rather than at the group treatment level). This approach can account for the possibility that patients benefiting from the intervention could also be the same patients who are more (or less) likely to experience harms (i.e., correlated benefit and risk outcomes within the same patients). The OMERACT method relies on a contingency table that allows for two or three levels of benefit across two or three levels of harm. The specific benefit and harm levels are uniquely defined depending on the chronic pain condition(s) and treatment(s) being evaluated, and therefore can vary. However, the interpretation of the contingency table is consistent across studies, with an “unqualified success” corresponding to a patient with a good response in the benefit category without any AEs in the harm category. An “unmitigated failure” would involve a patient with no response in the benefit category but at least one AE in the harm category. As represented in Figure 1, the OMERACT method was recently applied to data collected from two separate rheumatoid arthritis clinical trials (The Treatment of Early Aggressive Rheumatoid Arthritis, or TEAR trial; the Rheumatoid Arthritis Comparison of Active Therapies, or RACAT trial) [12]. The primary findings from the trials revealed no significant safety concerns of any treatment and significant beneficial effects of treatment relative to comparators in the TEAR trial, but not in the RACAT trial. However, the secondary analysis of benefit-risk in these trials revealed a more complicated pattern of results not identified in the primary analyses. In the secondary analysis, benefit was defined as good, moderate, or no response depending on the patient’s disease activity, and harms were categorized into three types of AE outcomes (no AEs, non-SAEs, and SAEs). Results of the TEAR trial analysis revealed that treatment response and AE rates were weakly associated with no significant difference between the treatment arms). In the RACAT trial, treatment response and AEs were negatively associated such that the frequency of AEs and SAEs increased as beneficial responses decreased. These findings demonstrate that a combined benefit-risk assessment at the individual level can reveal differences in clinical response that are not obvious when benefit and risk are assessed separately. This method is limited because it classifies benefits and AEs categorically, which could oversimplify these outcomes and the final results of the analysis. For example, the AE category that does not include SAEs is very broad and could include a wide range of potential outcomes. Due to these and other limitations, the OMERACT benefit-risk analysis should be considered a complementary method and should not fully replace current analysis and reporting strategies in clinical trials of chronic pain treatments.
Table 1.
Selected Level Benefit-Risk Assessment Frameworks and Methods for Chronic Pain Clinical Trials
| NAME | DESCRIPTION | EXAMPE |
|---|---|---|
| GROUP LEVEL ASSESSMENTS | ||
| EMA PrOACT-URL | The EMA PrOACT-URL is an eight-step qualitative analysis that provides a generic problem structure for identifying favorable and unfavorable effects, as well as the uncertainty of each, that has been adopted by the EMA [39; 40]. The framework is based on the field of decision analysis and was developed through the public-private partnership, IMI PROTECT. | Rheumatoid Arthritis [157] |
| FDA BRF | The FDA BRF five-step qualitative framework provides a simple and user-friendly snapshot of benefit-risk assessment that is intended to be broadly applicable [48–50; 87]. It should be updated as new information is received and can be used throughout the regulatory process. The five steps and questions asked include: (1) Analysis of the condition/”what is the problem?”; (2) Unmet Medical Need/”what other potential interventions exist?”; (3) Benefit; (4) Risk/”what am I worried about?”; (5) Risk Management/”what can I do to mitigate/monitor those concerns?” | Chronic pain (general) [114] |
| PhRMA BRAT | PhRMA BRAT is a six-step qualitative analysis developed to facilitate benefit-risk assessment by pharmaceutical companies and regulators. The method results in a summary table using the following: decision context, outcomes, data sources, framework, outcome importance, and display and interpret key metrics [28; 100]. Benefits and risks are not integrated in this framework, but are assessed separately to reduce complexity. | Migraine [100] |
| MCDA | Multicriteria decision analysis (MCDA) is a quantitative analysis method based on decision theory that combines evaluations of multiple potential benefits and risks (based on pre-specified criteria) into a weighted benefit-risk assessment [33; 111]. The scoring and weighting process allows the effects of different interventions to be placed on a common scale that allows for comparisons across interventions. | Chronic cancer pain [135] |
| INHB | Incremental Net Health Benefit (INHB) is a quantitative analysis method that is based on health-outcomes modeling that incorporates a life-expectancy measure adjusted for quality of life (i.e., quality-adjusted life year; QALY) [30; 57; 58]. The QALY represents an adjustment to length of life for the quality of life experienced and can be easily adapted to benefit-risk analysis by separating outcomes into expected health improvements with positive QALYs (benefits) and adverse health impacts with negative QALYs (risks). Benefit-risk differentials can then be expressed as either ratios or differences although the latter is preferred because the difference can be interpreted as healthy days (or months or years) of life gained (lost) since the units of measurement are the same. While standalone use of the INHB in pain populations is rare, clinical benefit-risk (net QALY impact) is the denominator in a range of cost-utility studies that have evaluated pain interventions. | Arthritis [103] |
| INDIVIDUAL LEVEL ASSESSMENTS | ||
| DOOR | The DOOR method is a quantitative analysis that provides a probability of a participant in the active group having a more desirable outcome than a participant in the control group. These probabilities are determined by ranking trial participants based on the desirability of their total experience of benefits and risks, and then the resulting rankings are compared between intervention arms [42; 43]. A key benefit of DOOR is that its calculation and interpretation are straightforward relative to other benefit-risk assessment methods. | Not yet examined in a chronic pain population |
| ETC Measure | The ETC Measure is a quantitative analysis that Integrates responder criteria for pain reduction (>20%, >30%, or >50% reduction in pain intensity from baseline) and adverse events (no AEs, no or mild AEs, and no or mild drug-related AEs) [88]. The approach assigns a score for both efficacy and tolerability for each day the patient is in the study, thus accounting for incidence, severity, and duration of AEs in one metric. The combination of scores across efficacy and tolerability over time forms a continuous ETC score that generally provides greater statistical power than dichotomous outcomes. The ETC score ranges from 0 to 1 with a clinically intuitive interpretation. For example, a score of 0.45 means the patient’s response was ‘good’ with respect to both efficacy and tolerability 45% of the time. | Chronic low back pain [88] |
| OARSI | OARSI has provided patient-focused, evidence-based, expert consensus guidelines for the management of knee OA that include the recommendation to perform a quantitative analysis using a composite benefit and risk score [105]. The score is voted on across a panel of expert physicians and calculated as the product of the benefit score (on a scale of 1–10) and the transposed risk score (where 1 = highest and 10 = safety) yielding a range of 1 (worst) to 100 (best). The group’s mean risk and benefit scores [along with 95% confidence intervals (CIs)] for each treatment are then plotted separately as bar graphs. | Knee osteoarthritis [105] |
| OMERACT | The OMERACT is a quantitative method that relies on a contingency table that allows for two or three levels of benefit across two or three levels of harm (Figure 1) [12]. The specific benefit and harm levels are uniquely defined depending on the chronic pain condition(s) and treatment(s). The interpretation of contingency table is consistent across studies, with an ‘unqualified success’ being a patient with a good response without any AEs and an ‘unmitigated failure’ being a patient having no benefit, but experiencing at least one AE. | Rheumatoid Arthritis [12] |
Note: Additional benefit-risk approaches that might be considered, and not highlighted in the present table for brevity, include multiple-criteria decision analysis (MCDA), discrete-event simulation, probabilistic simulation, and Bayesian belief networks [109; 110]. AE (Adverse Event); BRF (Benefit-Risk Framework); DOOR (Desirability of Outcome Ranking Evaluation); EMA (European Medicines Agency); ETC (Efficacy-Tolerability Composite); FDA (United States Food and Drug Administration); IMI PROTECT (Innovative Medicines Initiative Pharmacoepidemiological Research on Outcomes of Therapeutics); INHB (Incremental Net Health Benefit); (MCDA (Multi-Criterion Decision Analysis); OMERACT (Outcome Measures in Rheumatology); OARSI (Osteoarthritis Research Society International); PhRMA BRAT (Pharmaceutical Research and Manufacturers of America Benefit-Risk Action Team); PrOACT-URL (Problem formulation, Objectives, Alternatives, Consequences, Trade-offs, Uncertainties, Risk attitude, and Linked decisions).
Figure 1.
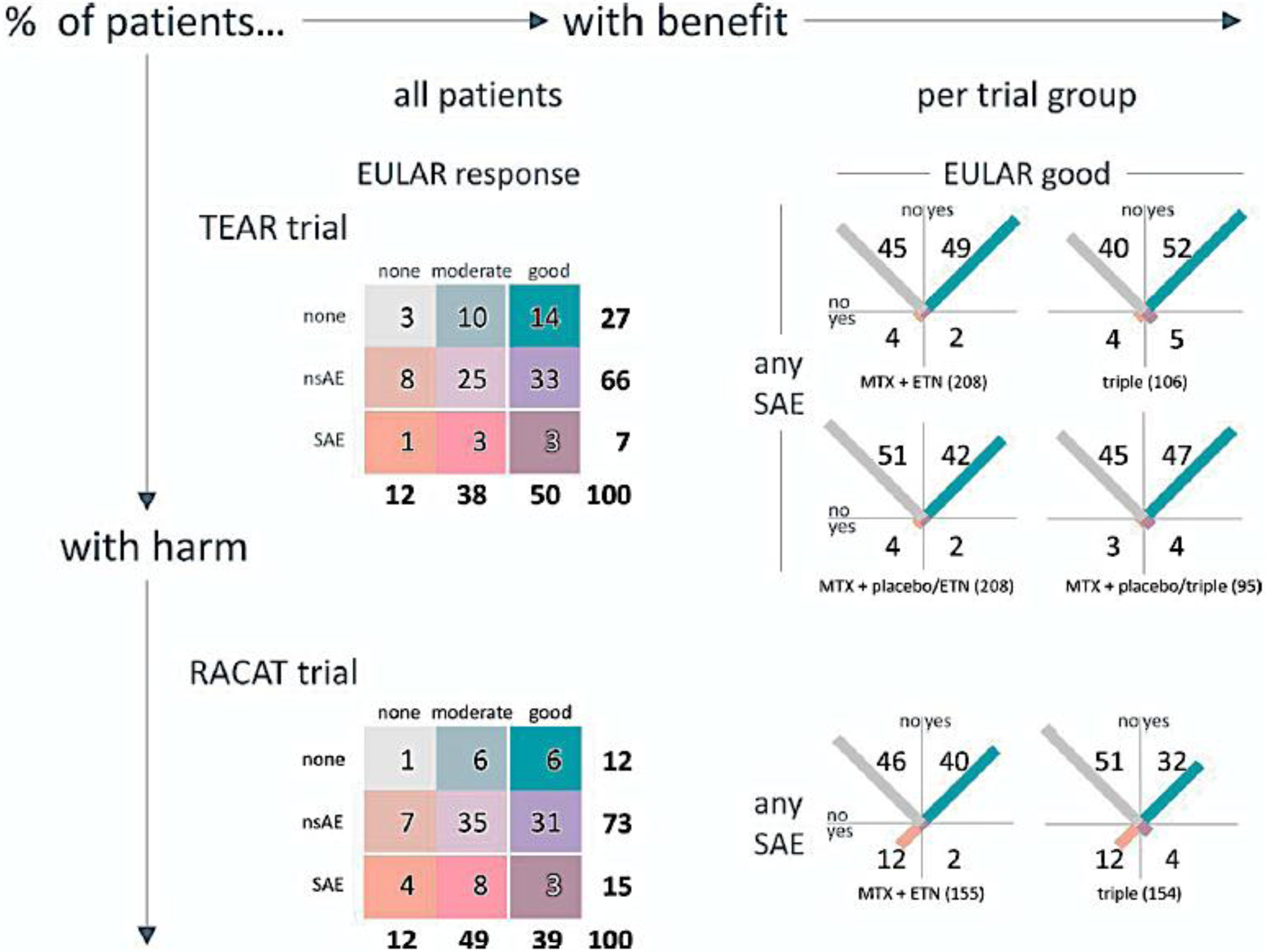
Figure 1 is reproduced from a previous publication [12] and copyright permissions were approved by Figure 1 is reproduced from a previous publication and copyright permissions were approved by Wiley.
The figure illustrates the OMERACT 3×3 Combined Table of Benefits and Risks assessment method [12]. The results represented in the figure are from two randomized controlled trials including the Treatment of Early Aggressive Rheumatoid Arthritis (TEAR) trial (Top Panel) and the Rheumatoid Arthritis Comparison of Active Therapies (RACAT) trial (Bottom Panel). In the panels on the left, results of treatment groups are pooled and categorized according to the combined occurrence of benefit and harm, each in 3 categories. Results are expressed as a percentage of the total group, corrected for rounding. White lines delineate the cutoffs for the 2×2 categorization in the right-hand panels. The panels on the right show the results (percent per treatment group) with the combined occurrence of benefit and harm, each in 2 categories: for benefit, the European League Against Rheumatism (EULAR) good response (yes/no); for harm, the occurrence of any serious adverse event (SAE; yes/no). The length of the diagonal bar in each cell is proportional to the percentage of patients in that cell. The orange/blue (bottom left to top right) diagonal shows the balance between worst and best outcomes. The light grey/purple (top left to bottom right) diagonal shows the balance between 2 types of tradeoff: no benefit + no harm, and benefit + harm. nsAE (non-SAE); MTX (methotrexate); ETN (etanercept); triple (MTX, sulfasalazine, hydroxychloroquine).
3.2.3. U.S. Food and Drug Administration (FDA)
The FDA has released a series of documents focused on benefit-risk assessment, including 10 guidance documents (Supplementary Information). Five of these documents pertain to medical devices, 4 address pharmacological treatments, and one spans multiple FDA centers and addresses benefit-risk reporting on the internet and social media. The FDA currently recommends a structured qualitative benefit-risk framework (BRF) supplemented with quantitative analyses to analyze the benefits and risks associated with medical products [48–50; 87]. The FDA framework addresses four dimensions: (1) the analysis of the condition, (2) current treatment options, (3) benefits, and (4) risk management. The FDA has conducted several public meetings on the topic of benefit-risk assessment in recent years, and draft guidance was scheduled to be published in 2020; however, no updates were located to prepare this article [49; 51; 96]. This guidance is expected to use a case study approach for articulating FDA’s decision-making context for benefit-risk analysis in order to provide stakeholders with a clearer understanding of how considerations of a medication’s benefits versus risks factor into FDA’s regulatory decisions throughout the drug development life-cycle, including pre- and post-market phases. Importantly, this guidance will discuss how relevant patient experience data and related information may be used to inform benefit-risk assessment.
4. Recommendations for Benefit-Risk Assessment and Reporting in Chronic Pain Clinical Trials
4.1. Terminology
Terminology associated with benefit-risk assessment, including operational definitions of key terms, are not standardized and often vary [39; 77]. Opinions vary as to whether the terms “harm” or “tolerability” might be more appropriate than the term “risk” [77; 88]. For this article, we define benefits as the intended favorable effects for the target population associated with an intervention and risks as the unintended clinical and health outcomes or detrimental effects that can be attributed to the intervention [36]. The term risk in the present review includes unwanted side effects, some of which will have an adverse effect on patient functioning, but also includes major safety risks such as myocardial infarction or death. We recommend researchers distinguish between risks attributed to the treatment under study (e.g., chronic nausea or vomiting) relative to those that are most likely not related to the treatment per se (e.g., an injury sustained during a motor vehicle accident). We define benefit-risk assessment as a structured method (qualitative or quantitative) for combining separate benefit and risk outcomes into a composite metric that allows for a clear comparison of benefits and risks in relation to each other at the level of the group or for individual patients. According to our definition, global ratings of patient functioning (e.g., patient global impression of change; PGIC) that do not specifically include harms would not be considered benefit-risk assessment tools. The ratio of the number needed to treat (NNT) and number needed to harm (NNH) could be considered a measure of benefit-risk. We do not consider this approach further because the widely varying definitions used for NNH preclude meaningful treatment comparisons [137].
4.2. Steps Associated with Benefit-Risk Assessment
There are five steps underlying decision-making related to benefits and risks that are common across a range of disciplines(Table 2) [63; 74; 99; 111; 123; 154].
Table 2 –
Steps to consider in benefit and risk assessments in clinical trials of chronic pain treatments
| 1. Specify |
| Specify the chronic pain condition(s) under study and the currently available treatments for the condition(s). Unmet clinical needs associated with the condition and contextual information such as common comorbidities associated with the condition should also be addressed. |
| 2. Identify |
| Identify the key outcomes that will be utilized to assess the benefits (e.g., reductions in pain intensity or severity) and risks (adverse events, reduced quality of life). Patient preference on meaningful benefit and risk outcomes should be incorporated at this level and patient-reported outcomes should be used to gather data. |
| 3. Evaluate |
| Collect and combine data related to the benefits and risks of an intervention(s) in a way that allows for the ranking or weighting of data. In general, two approaches to benefit-risk analyses can be performed: compare and combine at the level of the intervention or combine and compare at the level of the individual patient. |
| 4. Interpret |
| The interpretation of data should incorporate value judgments, or trade-offs between the relative importance of benefits and risks in a particular situation, which can vary depending on the type of stakeholder (patient, clinician, regulatory agency). This step should also address the uncertainty associated with the analysis given that benefit-risk assessments are dynamic and evolve as information changes over time. |
| 5. Communicate |
| Communicate the results of the analysis, including sharing the processes and rationale leading to the final conclusions. Messaging of the findings might need to be tailored depending on the audience and information should be summarized in succinct, transparent, and user-friendly ways (e.g., graphical representations). |
4.1.1. Specify.
The first sequential step involves providing a description of the chronic pain condition(s) examined, current treatments for the condition(s), and any other related contextual information specific to the pain condition that could influence relevant risks, including epidemiological information related to patient demographics or comorbid health conditions (e.g., tobacco use, obesity, concurrent medication use). In addition, the collection of patient preference data at the start of the study to determine patient attitudes regarding benefit-risk has been suggested as an important feature of this step [87].
4.1.2. Identify (Outcomes and Assessments).
The second step requires identification of the key outcomes and measures that will be used when combining benefits and risks. As presented in Table 3 and in the Supplementary Information, benefits and risks can be assessed using a variety of outcome measures with the most common being reductions in pain intensity (benefits) and AEs (risks). More nuanced outcomes including health-related quality of life, sleep, physical and cognitive functioning, mental health, type/severity/duration of AEs, and abuse liability might also be of interest [147]. Simply analyzing the frequency of AEs or SAEs or combining different types AEs into one heterogenous outcome can fail to detect important group differences in harms that are revealed when severity and duration of AEs are incorporated into analyses [88; 118]. As discussed in detail elsewhere [127], it is essential to consider the use of standardized language when referring to benefits and risks in order to facilitate the comparison and evaluation of study outcomes (e.g., Medical Dictionary for Regulatory Activities (MedDRA), the Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) terminologies).
Table 3 –
Benefit-Risk Terminology
| Benefit | The intended positive or favorable effects of an intervention for the target population (often referred to as “benefits” or “clinical benefits”) that are associated with an intervention [36]. Examples include reduction in pain intensity, increase in number of pain free days, function, and quality of life. |
| Risk | The unintended negative clinical and health outcomes or detrimental effects that can be attributed to the intervention. The use of the term risk in the present article includes side effects, some of which will have an adverse effect on patient functioning, but also includes safety risks, SAEs such as myocardial infarction, or death. The intensity and duration of all treatment-emergent AEs should be collected (total, severe, and serious), as well as the use of active capture, which includes interviews or questionnaires [36; 73]. |
| Benefit-Risk Assessment | A structured method (qualitative or quantitative) for combining separate benefit and risk outcomes into a composite metric that allows for a clear comparison of benefits and risks in relation to each other at the level of the group or for individual patients. |
| Clinical Utility | The ability of a clinical test result(s) to inform a decision that positively changes the outcome of a patient [144] |
| Qualitative Framework | Qualitative or descriptive frameworks provide stepwise instructions for evaluating and balancing benefit and risk, including their frequency and duration, and fully describes how that information weighs into decision making [123]. Examples include: The Problem formulation, Objectives, Alternatives, Consequences, Trade-offs, Uncertainties, Risk attitude, and Linked decisions framework and the United States Food and Drug Administration Benefit-Risk Framework. |
| Quantitative Framework | Quantitative frameworks provide explicit methods for combining and weighing risks and benefits. A quantitative approach may help to improve the transparency of a review, relative to a qualitative approach, by being explicit about how benefits and harms are estimated and compared (Boyd et al., 2012). While quantitative approaches can be used to examine benefit-risk at the level of the group, there are most commonly used for analyses that begin at the level of the individual patient (Table 1). Examples include multiple-criteria decision analysis (MCDA), discrete-event simulation, probabilistic simulation, and Bayesian belief networks [111; 112]. |
| Patient Preferences | Patient preferences represent patient’s attitudes toward a set of alternatives necessary for decision-making [77]. Collecting data related to a patient’s perspective or preference should be taken into account at all stages of research including planning of the clinical trial design and the identification of patient-relevant outcomes [13; 81; 82; 151]. |
| Standardization and Transparency | A systematic and transparent evaluation process that allows for consistency of reporting, replication, and pooling of data across studies [73]. |
Note: AE (adverse event); SAE (serious adverse event).
We recommend this step incorporate the needs and preferences of patients into study planning in two ways. First, as noted, the choice of benefit-risk outcomes should be based, at least in part, on feedback from patients, surrogates, or patient advocacy groups, and not simply chosen based on clinician, investigator, or regulatory considerations [113; 130]. While validated measures of patient preferences are currently lacking in the field, we recommend that at least some measures of benefit and risk include patient-reported outcomes (PRO), or data reported by patients without interpretation by someone else [5; 8; 9; 47]. We recommend that such data be collected through active capture using structured interviews or questionnaires, as well as passive capture/general inquiries, which can identify unanticipated outcomes [36]. A detailed discussion and framework for incorporating patient preference data in benefit-risk assessment can be found elsewhere [71].
Medical conditions and associated symptoms and interventions can also influence patient preferences or perceptions of benefit-risk trade-offs [5; 6; 23; 62; 67]. One example includes older patients with knee osteoarthritis who are sometimes willing to forgo greater treatment effectiveness for a lower risk of AEs [52], whereas there is a large body of work demonstrating that individuals with a range of complex, chronic health conditions, including Crohn’s disease, irritable bowel syndrome, low back pain, and osteoarthritis, are willing to accept high levels of risk in return for disease-modifying benefits of treatment [68; 85; 86; 126; 131; 148]. These observations highlight the potential for subgroup differences among chronic pain populations that can influence the weighting of benefits and risks (e.g., age, drug use and dependence history, multimorbidity) [115; 148]. Lastly, this step should include prospective registration of the trial characteristics, including study objectives and hypotheses [44; 136] and benefit-risk assessments that are planned in a public database(s) such as ClinicalTrials.gov.
4.1.3. Evaluate (Endpoints and Analyses).
The third step involves collecting data related to the benefits and risks of an intervention(s) and combining those data in a way that allows for the ranking or weighting of data in a combined metric. A variety of benefit-risk assessments apply to clinical trials of chronic pain treatments (Table 1) [13; 21; 40; 59; 63; 111; 112; 154]. Two approaches to benefit-risk data include those that combine benefit and risk data at the group level and those that first combine such data at the individual level and then analyze differences on the group level [41–43]. The most common approach involves summarizing benefit-risk data at the level of the group or intervention (placebo versus active treatment) and then combining these data in a way that allows comparisons across treatments. This approach has the advantage that it is easy to analyze outcomes and quickly communicate the findings and examples include the FDA’s BRF and the EMA’s PrOACT-URL (Section 4.2). However, this approach does not account for associations between benefits and risks that might occur at the level of the individual patient. For example, a patient who is experiencing the greatest reduction in pain from an intervention could also be more likely to experience SAEs from the same intervention [11; 12].
An alternative approach involves assessing benefit-risk trade-off within each participant [42; 60; 125]. Examples of benefit-risk assessments that focus on the individual rather than group level analysis are represented in Table 1 and include the Desirability of Outcome Ranking (DOOR), Efficacy-Tolerability Composite (ETC), OMERACT, and OARSI methods. In the DOOR method trial participants are first ranked based on the desirability of their total experience of benefits and risks (across multiple dimensions/outcomes), with a focus on the outcomes that are most important from the patient’s perspective [41–43]. The resulting rankings are then compared between intervention arms (Table 4).
Table 4 –
Analysis of Patients by Treatment from Evans and Follmann (2016)
| Treatment A Efficacy | Treatment B Efficacy | Treatment C Efficacy | ||||
|---|---|---|---|---|---|---|
| Toxicity | 10 | 10 | 50 | 0 | 0 | 50 |
| 40 | 40 | 0 | 50 | 50 | 0 | |
Note: Table is reproduced from a previous publication and copyright permissions were approved by Taylor & Francis [42]. The table represents four patient outcomes as a function of efficacy and toxicity. In all groups, 50% of the patients experience beneficial effects of treatment (efficacy). The interpretation of these outcomes is different when the risks of treatment (toxicity) are combined in the analysis. In treatment A, efficacy and toxicity were uncorrelated resulting in 40 patients that had efficacy without toxicity. In treatment B, efficacy and toxicity were positively correlated resulting in 0 patients that had efficacy without toxicity. In treatment C, efficacy and toxicity were negatively correlated resulting in 50 patients that had efficacy without toxicity..
A last point to consider is that under ideal circumstances, benefit-risk analyses should be compared across different subpopulations that represent different demographic factors and comorbidities [11; 12; 42; 68]. There could be important subgroup differences that can affect the findings from a benefit-risk assessment. For instance, the risks of some pharmacologic treatments can be significantly greater in patients with impaired renal function; thus, the benefit-risk relationship may be quite different in this subgroup of patients relative to the overall study population.
4.1.4. Interpret.
The fourth step incorporates the perspectives of a range of stakeholders (patients, patient advocacy groups, healthcare providers, payers, pharmaceutical and device companies, regulatory agencies) seeking improved treatments for chronic pain, each of whom have a unique perspective on the benefits and risk trade-offs [21; 48; 49; 87; 94; 99; 149]. These various viewpoints add a necessary complexity to benefit-risk assessment [11; 82; 87; 94; 123]. For this reason, we recommend that the interpretation of benefit-risk analyses be as transparent as possible with a clear history of the evaluation process that represents each step taken, including the various stakeholders involved in interpreting the evidence [16; 111; 120]. An additional consideration is the need to account for uncertainty when interpreting benefit-risk findings, including statistical uncertainty, especially for outcomes with low incidence rates such as SAEs. Such uncertainty can also be augmented by accounting for missing data associated with patients who stop their treatment or withdraw early from trials for reasons such as perceived lack of efficacy and adverse side effects [20]. Statistical approaches for addressing intercurrent events and sources of missing data are evolving and are highlighted by the International Council for Harmonisation (ICH) guidance (E9/R1) [22; 76].
4.1.5. Communicate.
The final step includes communicating and reporting the results of the analysis, including sharing the processes and rationale leading to the final conclusions [99]. This step requires that the presentation of the benefit-risk findings can be understood by the target audience (e.g., an individual patient, clinicians, researchers, the public). Basic principles of effective communication apply here, including: 1) providing the information needed for effective decision making which requires an understanding of the patient’s perspective, 2) allowing access to information (e.g., graphical representations), and 3) ensuring that users can comprehend the information (e.g., health literacy) [46]. Composite outcomes such as benefit-risk assessments can be challenging to interpret given that a significant result associated with a composite outcome might not indicate a significantly more beneficial treatment depending how the composite was created [59]. Thus, information should be summarized in succinct, transparent, and user-friendly ways, including graphical representations to the extent possible rather than data heavy text or tables [41; 161].
4.2. Selected Benefit-Risk Assessment Frameworks and Methods
Table 1 describes nine benefit-risk assessment frameworks and methods that are well-suited for clinical trials of chronic pain treatments. The frameworks and methods identified in the table can be complementary and used simultaneously and include tools that combine benefit-risk at the group level (EMA PrOACT-URL, FDA BRF, Incremental Net Health Benefit/INHB and Pharmaceutical Research and Manufacturers of America Benefit-Risk Action Team/PhRMA BRAT), as well as methods that combine benefit-risk at the level of the patient (DOOR, Efficacy-Tolerability Composite/ETC, Measure, Osteoarthritis Research Society International/OARSI Knee Osteoarthritis Model, and the OMERACT method). Few studies have evaluated the various benefit-risk methods described here in clinical trials of chronic pain treatments. For some of these methods, it is possible to use existing clinical trial datasets to evaluate benefits and risks in a combined metric [12; 88].
5. Conclusions
We recommend that benefit-risk assessments be used in chronic pain RCTs to combine benefits and risks at the treatment group level (e.g., FDA BRF or PhRMA BRAT) [28; 48; 49; 100] and at the level of the individual patient (e.g., OMERACT, DOOR) [5; 43] (Table 1). The recommendation to include both types of evaluations is based on the observation that individual differences in clinical response can be obscured when combined at the group level. In many circumstances, it is valuable to include both levels of analysis (group and individual level). It should be emphasized that there is not a “one-size-fits-all” benefit-risk assessment tool for all chronic pain RCTs and that a combination of methods, as represented in Table 1, may be needed depending on the unique circumstances associated with the treatment, chronic pain condition, and clinical trial. Relatedly, given the diversity of benefit-risk assessment tools that can be utilized across clinical trials, researchers should be as transparent as possible when reporting how benefits and risks have been defined, measured, and combined to facilitate the application of study findings to patient care and decision-making.
These recommendations can serve as a starting point for incorporating benefit-risk assessment tools into future chronic pain clinical trials. One important component of a research agenda is evaluating and comparing the properties (e.g., reliability, validity, assay sensitivity) of currently available benefit-risk frameworks and methods to determine if there are approaches that are more informative [12; 88]. There is a need to integrate, to the greatest extent possible, benefit-risk assessment in clinical trials with other types of relevant data such those derived from preclinical and epidemiological studies [15; 121]. This approach could include using health outcomes modeling as a framework, post-approval, epidemiological data regarding the benefits and harms of a particular chronic pain treatment could be combined with individual level data to update earlier benefit-risk assessments, and further guide patient and clinician shared decision making as well as continued drug development and safety monitoring [57]. The systematic assessment of benefit-risk in clinical trials can enhance the clinical meaningfulness of RCT results. We are optimistic that benefit-risk frameworks and methods will be more widely incorporated in future clinical trials of chronic pain treatments.
Supplementary Material
Acknowledgments
We thank Valorie Thompson and Andrea Speckin for their assistance in organizing the meeting on which this article is based, and Linda Hasman, at the University of Rochester School of Medicine and Dentistry, for her assistance in building the search strategy. We acknowledge Laurie Burke for the feedback she provided on an earlier draft of this manuscript and Stephen Morley for his participation in the IMMPACT meeting, and who passed away before publication.
Disclosures
The views expressed in this article are those of the authors, some of whom were, or currently are, employees of pharmaceutical, consulting, or contract research companies and may have financial conflicts of interest related to the issues discussed in this article. At the time of the meeting on which this article is based, several authors were employed by pharmaceutical companies and others had received consulting fees or honoraria from one or more pharmaceutical or device companies. Authors of this article who attended the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) meeting and were not employed by industry or government at the time of the meeting received travel stipends, hotel accommodations, and meals during the meeting provided by the Analgesic, Anesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks (ACTTION) public-private partnership with the US Food and Drug Administration (FDA). ACTTION has received research contracts, grants, or other revenue from the FDA, multiple pharmaceutical and device companies, philanthropy, and other sources. Preparation of background literature reviews and this article was supported by ACTTION. No funding from any other source was received for the meeting, nor for the literature reviews and article preparation. No official endorsement by the FDA, US National Institutes of Health, or the pharmaceutical and device companies that have provided unrestricted grants to support the activities of ACTTION should be inferred.
B. Kleykamp has received in the past 36 months support from the Analgesic, Anesthetic, and Addiction Clinical Trial Translations, Innovations, Opportunities, and Networks public-private partnership with the United States Food and Drug Administration and compensation for medical writing from Palladian Associates, HayesInc/TractManager, STATinMED, and PBS Next Avenue. In addition, between 2014 and 2018 during her previous employment at the consulting firm, PinneyAssociates, she provided consulting advice to pharmaceutical companies, the e-cigarette company NJOY, and the tobacco company, RAI Services Company on non-combustible tobacco products including e-cigarettes.
R. Dworkin has received in the past 5 years research grants and contracts from the US Food and Drug Administration and the US National Institutes of Health, and compensation for serving on advisory boards or consulting on clinical trial methods from Abide, Acadia, Adynxx, Analgesic Solutions, Aptinyx, Aquinox, Asahi Kasei, Astellas, AstraZeneca, Biogen, Biohaven, Boston Scientific, Braeburn, Cardialen, Celgene, Centrexion, Chromocell, Clexio, Collegium, Concert, Confo, Decibel, Dong-A, Editas, Eli Lilly, Ethismos (equity), Eupraxia, Glenmark, Gloriana, Grace, Hope, Immune, Lotus, Mainstay, Merck, Neumentum, Neurana, NeuroBo, Novaremed, Novartis, Olatec, Pfizer, Phosphagenics, Quark, Reckitt Benckiser, Regenacy (also equity), Relmada, Sanifit, Scilex, Semnur, SIMR Bio, SK Life Sciences, Sollis, SPRIM, Teva, Theranexus, Trevena, Vertex, and Vizuri.
D. Turk has received in the past 36 months support from research grants and contracts from US Food and Drug Administration, US National Institutes of Health, and the Patient Centered Outcomes Research Institute, and compensation for consulting on research methods and reporting from AccelRx, Eli Lilly, Flexion, GlaxoSmithKline, Novartis, and Pfizer.
Z. Bhagwagar employee at, and own stock in, Bristol-Myers Squibb and Alexion Pharmaceuticals.
P. Cowan reports no disclosures.
C. Eccleston reports no disclosures.
S. Ellenberg serves on data monitoring committees for Bristol-Myers Squibb, Novartis, Marinus and Rigel Pharmaceuticals.
S. Evans receives grant support from NIAID/NIH and reports personal fees from Takeda, Pfizer, Roche, Novartis, ACTTION, Genentech, Amgen, American Statistical Association, FDA, Osaka University, National Cerebral and Cardiovascular Center of Japan, NIH, Society for Clinical Trials, DeGruyter, AstraZeneca, Teva, Austrian Breast & Colorectal Cancer Study Group (ABCSG)/Breast International Group (BIG) and the Alliance Foundation Trials (AFT), Taylor and Francis, Vir, Shire, Alexion, Gilead, Clinical Trials Transformation Initiative, Tracon, Deming Conference, Antimicrobial Resistance and Stewardship Conference, Advantagene, Cardinal Health, Microbiotix, Stryker, Atricure, BENEFIT, Roivant, Neovasc, Nobel Pharma, Horizon, Roche, Rakuten, Duke University, U. of PENN, Takeda, Nuvelution, Abbvie, Clover, FHI Clinical, Lung Biotech, SAB Biopharm, CIOMS, SVB LEERINK.
L.Garrison received research grants, consulting fees, and/or speaker fees in the last three years from Pfizer, Eli Lilly, Biogen, Merck, Roche, Genentech, Novartis, AveXis, BMS, Medtronic, Mallinckrodt, Amgen, AbbVie, Adamas, Analysis Group, Thrive Detection, Medtronic, Roche Molecular Systems, BioMarin, Global Blood Therapeutics, Sanofi-Pasteur, Medtronic, Aspen Institute, and Premera.
J. Gewandter, in the past 36 months, has received research grants from the NIH and consulting income from Disarm Therapeutics, AlgoTX, Asahi Kasei Pharma, Magnolia Neurosciences, Mitobridge, Orthogonal Neurosciences, Science Branding Communications, and SK Life Science.
V. Goli has been an employee of IQVIA in the last three years and is currently an employee of Syneos Health.
J. Farrar reports grants from NIH-NIDDK - U01 Grant (CoI), grants from NIH-NINDS - U24 Grant (PI), grants from FDA-BAA Contract, during the conduct of the study; personal fees from Pfizer, Daiichi Sankyo, Cara Therapeutic, Biogen, Opioid Post-Marketing Consortium, personal fees NIH-NIA, Analgesic Solutions, Novartis, Aptinyx, DepoMed, Jansen, Evadera, Eli Lilly, Vertex, outside the submitted work
R. Freeman has received personal compensation and/or stock options for serving on scientific advisory boards of AlgoRx, Allergan, Applied Therapeutics, Clexio, Cutaneous NeuroDiagnostics, Glenmark, Glaxo-Smith Kline, Eli-Lilly and Company, Lundbeck, Novartis, NeuroBo, Regenacy, and Vertex.Received personal compensation for his editorial activities (Editor) with Autonomic Neuroscience – Basic and Clinical. Received research support from the National Institutes of Health (U54NS065736, 1R01NS10584401A1, R01HL111465-01A1).
S. Iyengar is an employee of NINDS/NIH, Adjunct Senior Research Professor, IU School of Medicine, Indianapolis, IN 46202.
A. Jadad reports no disclosures.
M. Jensen has received in the past 36 months research grants from the U.S. NationalInstitutes of Health, the U.S. Department of Education, the Administration of Community Living, the Patient-Centered Outcomes Institute, and National Multiple Sclerosis Society, the International Association for the Study of Pain, Zogenix, Inc., and the Washington State Spinal Injury Consortium.
R.Junor reports no disclosures.
N. Katz is an employee of WCG Analgesic Solutions, a consulting company with multiple clients in the pharmaceutical and medical device industries. Dr. Katz does not receive any direct payments from clients.
J.P. Kesslak was a salaried employee of Allergan with stock options at the time of the IMMPACT meeting.
E. Kopecky was a salaried employee with stock options of Endo Pharmaceuticals Inc. at the time of the IMMPACT meeting.
D. Lissin was an employee of DURECT Corporation at the time of the IMMPACT meeting, currently Chief Medical Officer of Scilex Pharmaceuticals, Inc.
J. Markman reports non-financial support from Pfizer Inc and Eli Lilly, during the conduct of the study; grants and other from Clexio, grants from Pfizer, other from Teva, other from Quark, other from Biogen (Convergence), other from Nektar, other from ENDO, other from Immune Pharma, other from Chromocell, other from Collegium, other from Purdue, other from Novartis, grants and other from Depomed, other from Allergan, other from Sanofi, other from Aptinyx, other from Diaachi Sanyko, other from Plasmasurgical, other from Grunenthal, other from Clexio Bioscience, other from Editas Medicine, other from Trevena, other from Inspirion, other from Merck, other from Esteve Pharmaceuticals, other from Tremeau Pharmaceuticals, other from Sophren Pharmaceuticals, other from YellowBlack Corporation, outside the submitted work.
M. McDermott has been supported in the past 36 months by research grants from NIH, FDA, SMA Foundation, Cure SMA, Friedreich’s Ataxia Reseach Alliance, Muscular Dystrophy Association, ALS Association, and PTC Therapeutics, has received compensation for consulting from Fulcrum Therapeutics, Inc. and NeuroDerm, Ltd., and has served on Data and Safety Monitoring Boards for NIH, AstraZeneca, Eli Lilly and Company, Catabasis Pharmaceuticals, Inc., Vaccinex, Inc., Cynapsus Therapeutics, Voyager Therapeutics, Neurocrine Biosciences, Inc., and Prilenia Therapeutics Development, Ltd.
P. Mease has received research grants, consulting fees, and/or speaker fees from Abbvie, Amgen, Bristol Myers, Boehringer Ingelheim, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, SUN Pharma, and UCB.
A. O’Connor has no disclosures to declare.
K.Patel has received in the past 36 months research grants from the US National Institutes of Health and Centers for Disease Control and Prevention.
S. Raja has received in the past 36 months support from research grants, US National Institutes of Health, and is a co-investigator in a research grant from Medtronic, Inc. He is a consultant for Allergan, Averitas Pharma, Bayer, and Lexicon Pharmaceuticals, and has consulted in the past for Aptinyx Inc., and Heron Therapeutics.
M. Rowbotham has provided consulting services to CODA Biotherapeutics, Sustained Therapeutics, SiteOne Therapeutics, Acadia Pharmaceuticals, Editas Medicine, and Amygdala Neurosciences. He serves on a DSMB for Helixmith and is Treasurer of the International Association for the Study of Pain.
C. Sampaio receives salary from CHDI management/CHDI Foundation Inc, and consultancy fees from vTv Therapeutics, Pinteon Pharmaceuticals, Pfizer, Kyowa Kirin, Neuraly,
J. Singh has received consultant fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two labs Inc, Adept Field Solutions, Clinical Care options, Clearview healthcare partners, Putnam associates, Focus forward, Navigant consulting, Spherix, MedIQ, Jupiter Life Science, UBM LLC, Trio Health, Medscape, WebMD, and Practice Point communications; and the National Institutes of Health and the American College of Rheumatology. JAS owns stock options in TPT Global Tech, Vaxart pharmaceuticals and Charlotte’s Web Holdings, Inc. JAS previously owned stock options in Amarin, Viking and Moderna pharmaceuticals. JAS is on the speaker’s bureau of Simply Speaking. JAS is a member of the executive of Outcomes Measures in Rheumatology (OMERACT), an organization that develops outcome measures in rheumatology and receives arms-length funding from 8 companies. JAS serves on the FDA Arthritis Advisory Committee. JAS is the chair of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and the Director of the University of Alabama at Birmingham (UAB) Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis. JAS previously served as a member of the following committees: member, the American College of Rheumatology’s (ACR) Annual Meeting Planning Committee (AMPC) and Quality of Care Committees, the Chair of the ACR Meet-the-Professor, Workshop and Study Group Subcommittee and the co-chair of the ACR Criteria and Response Criteria subcommittee.
I. Steigerwald is an employee of Neumentum, Inc (Chief Medical Officer, SVP) and was an employee of Grünenthal GmbH (Head of Medical Affairs New Brands, SBU Europe, Australia and North America, VP) at the time of the 2011 IMMPACT meeting.
V. Strand is a member of the executive of Outcomes Measures in Rheumatology (OMERACT), an organization that develops outcome measures in rheumatology and receives arms-length funding from 12 companies.
L. Tive is a salaried employee with stock options of Pfizer Pharmaceuticals Inc.
J. Tobias was an employee of NeurogesX, Inc. at the time of the meeting and is currently Partner and Managing Director of Aquila Consulting Group, LLC.
A. Wasan is a consultant for Vertex pharmaceuticals.
H. Wilson was a salaried employee of the University of Washington at the time of the meeting, is currently a salaried employee of the pharmaceutical company Boehringer Ingelheim, and within the past 36 months was previously a salaried employee of a scientific consulting firm Evidera.
References
- [1].Abdel-Meguid TA, Mosli HA, Farsi H, Alsayyad A, Tayib A, Sait M, Abdelsalam A. Treatment of refractory category III nonbacterial chronic prostatitis/chronic pelvic pain syndrome with intraprostatic injection of onabotulinumtoxinA: a prospective controlled study. The Canadian journal of urology 2018;25(2):9273–9280. [PubMed] [Google Scholar]
- [2].Aiyer R, Gulati A, Gungor S, Bhatia A, Mehta N. Treatment of Chronic Pain With Various Buprenorphine Formulations: A Systematic Review of Clinical Studies. Anesthesia and analgesia 2018;127(2):529–538. [DOI] [PubMed] [Google Scholar]
- [3].Al-Ajlouni J, Awidi A, Samara O, Al-Najar M, Tarwanah E, Saleh M, Awidi M, Hassan FA, Samih M, Bener A, Dweik M. Safety and Efficacy of Autologous Intra-articular Platelet Lysates in Early and Intermediate Knee Osteoarthrosis in Humans: A Prospective Open-Label Study. Clin J Sport Med 2015;25(6):524–528. [DOI] [PubMed] [Google Scholar]
- [4].Alev L, Fujikoshi S, Yoshikawa A, Enomoto H, Ishida M, Tsuji T, Ogawa K, Konno S. Duloxetine 60 mg for chronic low back pain: post hoc responder analysis of double-blind, placebo-controlled trials. J Pain Res 2017;10:1723–1731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Andersen KM, Cheah JTL, March L, Bartlett SJ, Beaton D, Bingham CO 3rd, Brooks PM, Christensen R, Conaghan PG, D’Agostino MA, de Wit M, Dueck AC, Goodman SM, Grosskleg S, Hill CL, Howell M, Mackie SL, Richards B, Shea B, Singh JA, Strand V, Tugwell P, Wells GA, Simon LS. Improving Benefit-harm Assessment of Therapies from the Patient Perspective: OMERACT Premeeting Toward Consensus on Core Sets for Randomized Controlled Trials. J Rheumatol 2019;46(8):1053–1058. [DOI] [PubMed] [Google Scholar]
- [6].Andersen KM, Kelly A, Lyddiatt A, Bingham CO III, Bykerk VP, Batterman A, Westreich J, Jones MK, Cross M, Brooks PM, March L, Shea B, Tugwell P, Simon LS, Christensen R, Bartlett SJ. Patient perspectives on DMARD safety concerns in rheumatology trials: Results from inflammatory arthritis patient focus groups and OMERACT attendees discussion. J Rheumatol 2019;46(9):1168–1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Asbury EA, Webb CM, Probert H, Wright C, Barbir M, Fox K, Collins P. Cardiac rehabilitation to improve physical functioning in refractory angina: a pilot study. Cardiology 2012;122(3):170–177. [DOI] [PubMed] [Google Scholar]
- [8].Atkinson TM, Li Y, Coffey CW, Sit L, Shaw M, Lavene D, Bennett AV, Fruscione M, Rogak L, Hay J, Gönen M, Schrag D, Basch E. Reliability of adverse symptom event reporting by clinicians. Quality of Life Research 2012;21(7):1159–1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Basch E. The missing voice of patients in drug-safety reporting. N Engl J Med 2010;362(10):865–869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Blumenfeld AM, Stark RJ, Freeman MC, Orejudos A, Manack Adams A. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J Headache Pain 2018;19(1):13–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Boers M, Brooks P, Fries JF, Simon LS, Strand V, Tugwell P. A first step to assess harm and benefit in clinical trials in one scale. J Clin Epidemiol 2010;63(6):627–632. [DOI] [PubMed] [Google Scholar]
- [12].Boers M, Singh JA, Cofield SS, Bridges SL Jr., Moreland LW, O’Dell JR, Wu H, Leatherman S, Curtis JR. A Novel Method to Combine Assessment of Benefit and Harm: Outcome Measures in Rheumatology 3×3 Methodology Applied to Two Active Comparator Trials. Arthritis Care Res 2019;71(2):319–322. [DOI] [PubMed] [Google Scholar]
- [13].Boyd CM, Singh S, Varadhan R, Weiss CO, Sharma R, Bass EB, Puhan MA. AHRQ Methods for Effective Health Care. Methods for Benefit and Harm Assessment in Systematic Reviews. Rockville (MD): Agency for Healthcare Research and Quality (US), 2012. [PubMed] [Google Scholar]
- [14].Brage K, Ris I, Falla D, Sogaard K, Juul-Kristensen B. Pain education combined with neck- and aerobic training is more effective at relieving chronic neck pain than pain education alone--A preliminary randomized controlled trial. Manual therapy 2015;20(5):686–693. [DOI] [PubMed] [Google Scholar]
- [15].Brønstad A, Newcomer CE, Decelle T, Everitt JI, Guillen J, Laber K. Current concepts of harm–benefit analysis of animal experiments–report from the AALAS–FELASA working group on harm–benefit analysis–part 1. Laboratory animals 2016;50(1_suppl):1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Bujar M, McAuslane N, Salek S, Walker S. Quality of Regulatory Decision-Making Practices: Issues Facing Companies and Agencies. Ther Innov Regul Sci 2016;50(4):487–495. [DOI] [PubMed] [Google Scholar]
- [17].Burmester GR, Blanco R, Charles-Schoeman C, Wollenhaupt J, Zerbini C, Benda B, Gruben D, Wallenstein G, Krishnaswami S, Zwillich SH, Koncz T, Soma K, Bradley J, Mebus C. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: a randomised phase 3 trial. Lancet (London, England) 2013;381(9865):451–460. [DOI] [PubMed] [Google Scholar]
- [18].Busse JW, Wang L, Kamaleldin M, Craigie S, Riva JJ, Montoya L, Mulla SM, Lopes LC, Vogel N, Chen E, Kirmayr K, De Oliveira K, Olivieri L, Kaushal A, Chaparro LE, Oyberman I, Agarwal A, Couban R, Tsoi L, Lam T, Vandvik PO, Hsu S, Bala MM, Schandelmaier S, Scheidecker A, Ebrahim S, Ashoorion V, Rehman Y, Hong PJ, Ross S, Johnston BC, Kunz R, Sun X, Buckley N, Sessler DI, Guyatt GH. Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis. Jama 2018;320(23):2448–2460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Buvanendran A, Kroin JS, Della Valle CJ, Kari M, Moric M, Tuman KJ. Perioperative oral pregabalin reduces chronic pain after total knee arthroplasty: a prospective, randomized, controlled trial. Anesthesia and analgesia 2010;110(1):199–207. [DOI] [PubMed] [Google Scholar]
- [20].Cai X, Gewandter JS, He H, Turk DC, Dworkin RH, McDermott MP. Estimands and missing data in clinical trials of chronic pain treatments: advances in design and analysis. Pain 2020;161(10):2308–2320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Califf RM. Benefit-risk assessments at the US Food and Drug Administration: finding the balance. Jama 2017;317(7):693–694. [DOI] [PubMed] [Google Scholar]
- [22].Callegari F, Akacha M, Quarg P, Pandhi S, von Raison F, Zuber E. Estimands in a chronic pain trial: Challenges and opportunities. Statistics in Biopharmaceutical Research 2020;12(1):39–44. [Google Scholar]
- [23].Chancellor J, Martin M, Liedgens H, Baker MG, Muller-Schwefe GH. Stated preferences of physicians and chronic pain sufferers in the use of classic strong opioids. Value Health 2012;15(1):106–117. [DOI] [PubMed] [Google Scholar]
- [24].Chen LX, Mao JJ, Fernandes S, Galantino ML, Guo W, Lariccia P, Teal VL, Bowman MA, Schumacher HR, Farrar JT. Integrating acupuncture with exercise-based physical therapy for knee osteoarthritis: a randomized controlled trial. J Clin Rheumatol 2013;19(6):308–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Cheng JOS, Cheng ST. Effectiveness of physical and cognitive-behavioural intervention programmes for chronic musculoskeletal pain in adults: A systematic review and meta-analysis of randomised controlled trials. PLoS One 2019;14(10):e0223367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Choi LJ, Huang JS. A pilot study of S-adenosylmethionine in treatment of functional abdominal pain in children. Altern Ther Health Med 2013;19(5):61–64. [PubMed] [Google Scholar]
- [27].Chuang-Stein C, Entsuah R, Pritchett Y. Measures for conducting comparative benefit: risk assessment. Drug information journal: DIJ/Drug Information Association 2008;42(3):223–233. [Google Scholar]
- [28].Coplan PM, Noel RA, Levitan BS, Ferguson J, Mussen F. Development of a framework for enhancing the transparency, reproducibility and communication of the benefit-risk balance of medicines. Clinical pharmacology and therapeutics 2011;89(2):312–315. [DOI] [PubMed] [Google Scholar]
- [29].Council for International Organizations of Medical Sciences Benefit-risk Balance for Marketed Drugs: Evaluating Safety Signals: Report of CIOMS Working Group IV: CIOMS, 1998.
- [30].Cross JT, Veenstra DL, Gardner JS, Garrison LP Jr. Can modeling of health outcomes facilitate regulatory decision making? The benefit-risk tradeoff for rosiglitazone in 1999 vs. 2007. Clinical pharmacology and therapeutics 2011;89(3):429–436. [DOI] [PubMed] [Google Scholar]
- [31].Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L, Kerns R, Von Korff M, Porter L, Helmick C. Prevalence of chronic pain and high-impact chronic pain among adults—United States, 2016. Morbidity and Mortality Weekly Report 2018;67(36):1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Dear BF, Gandy M, Karin E, Ricciardi T, Langman N, Staples LG, Fogliati VJ, Sharpe L, McLellan LF, Titov N. The Pain Course: exploring predictors of clinical response to an Internet-delivered pain management program. Pain 2016;157(10):2257–2268. [DOI] [PubMed] [Google Scholar]
- [33].Dodgson JS, Spackman M, Pearman A, Phillips LD. Multi-criteria analysis: a manual. 2009.
- [34].Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Progress in Neuro-Psychopharmacology and Biological Psychiatry 2019;93:284–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Dworkin RH, Evans SR, Mbowe O, McDermott MP. Essential statistical principles of clinical trials of pain treatments. Pain Rep 2021;6(1):e863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen MP, Katz NP, Kerns RD, Stucki G, Allen RR, Bellamy N, Carr DB, Chandler J, Cowan P, Dionne R, Galer BS, Hertz S, Jadad AR, Kramer LD, Manning DC, Martin S, McCormick CG, McDermott MP, McGrath P, Quessy S, Rappaport BA, Robbins W, Robinson JP, Rothman M, Royal MA, Simon L, Stauffer JW, Stein W, Tollett J, Wernicke J, Witter J. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005;113(1–2):9–19. [DOI] [PubMed] [Google Scholar]
- [37].Edwards JE, McQuay HJ, Moore RA, Collins SL. Reporting of adverse effects in clinical trials should be improved: lessons from acute postoperative pain. Journal of pain and symptom management 1999;18(6):427–437. [DOI] [PubMed] [Google Scholar]
- [38].Ehde DM, Dillworth TM, Turner JA. Cognitive-behavioral therapy for individuals with chronic pain: efficacy, innovations, and directions for research. American Psychologist 2014;69(2):153. [DOI] [PubMed] [Google Scholar]
- [39].European Medicines Agency Benefit-risk methodology project: work package 2 report: applicability of current tools and processes for regulatory benefit-risk assessment. In: HMDa Evaluation editor, 2011.
- [40].European Medicines Agency Benefit-risk methodology project: work package 4 report: Benefit-risk tools and processes. In: HMDa Evaluation editor, 2012.
- [41].Evans, Bigelow R, Chuang-Stein C, Ellenberg SS, Gallo P, He W, Jiang Q, Rockhold F. Presenting Risks and Benefits: Helping the Data Monitoring Committee Do Its Job. Annals of Internal Medicine 2020;172(2):119–125. [DOI] [PubMed] [Google Scholar]
- [42].Evans, Follmann D. Using Outcomes to Analyze Patients Rather than Patients to Analyze Outcomes: A Step toward Pragmatism in Benefit:risk Evaluation. Stat Biopharm Res 2016;8(4):386–393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Evans, Rubin D, Follmann D, Pennello G, Huskins WC, Powers JH, Schoenfeld D, Chuang-Stein C, Cosgrove SE, Fowler VG Jr, Lautenbach E, Chambers HF. Desirability of Outcome Ranking (DOOR) and Response Adjusted for Duration of Antibiotic Risk (RADAR). Clinical Infectious Diseases 2015;61(5):800–806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Evans SR. Fundamentals of clinical trial design. J Exp Stroke Transl Med 2010;3(1):19–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R, Dworkin RH, Gilron I, Haanpää M, Hansson P, Jensen TS, Kamerman PR, Lund K, Moore A, Raja SN, Rice AS, Rowbotham M, Sena E, Siddall P, Smith BH, Wallace M. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol 2015;14(2):162–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Fischhoff B. Communicating risks and benefits: An evidence based user’s guide: Government Printing Office, 2012.
- [47].Food and Drug Administration Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims. Fed Regist 2009;74(235):65132–65133. [Google Scholar]
- [48].Food and Drug Administration Structured approach to benefit-risk assessment in drug regulatory decision-making. Draft PDUFA V implementation plan–February 2013. Fiscal years 2013;2017. [Google Scholar]
- [49].Food and Drug Administration Benefit-Risk Assessment in Drug Regulatory Decision-Making: Draft PDUFA VI Implementation Plan (FY 2018–2022). 2018.
- [50].Food and Drug Administration. Opioid Analgesic Drugs: Considerations for Benefit-Risk Assessment Framework Guidance for Industry. 2019.
- [51].Food and Drug Administration Public Meeting: Characterizing FDA’s Approach to Benefit-Risk Assessment throughout the Medical Product Life Cycle, 2019.
- [52].Fraenkel L, Bogardus ST Jr., Concato J, Wittink DR. Treatment options in knee osteoarthritis: the patient’s perspective. Arch Intern Med 2004;164(12):1299–1304. [DOI] [PubMed] [Google Scholar]
- [53].Frank E, Kupfer D, Rucci P, Lotz-Wallace M, Levenson J, Fournier J, Kraemer H. Simultaneous evaluation of the harms and benefits of treatments in randomized clinical trials: demonstration of a new approach. Psychological medicine 2012;42(4):865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Furberg CD, Levin AA, Gross PA, Shapiro RS, Strom BL. The FDA and drug safety: a proposal for sweeping changes. Archives of internal medicine 2006;166(18):1938–1942. [DOI] [PubMed] [Google Scholar]
- [55].Garland EL, Hanley AW, Riquino MR, Reese SE, Baker AK, Salas K, Yack BP, Bedford CE, Bryan MA, Atchley R, Nakamura Y, Froeliger B, Howard MO. Mindfulness-oriented recovery enhancement reduces opioid misuse risk via analgesic and positive psychological mechanisms: A randomized controlled trial. Journal of consulting and clinical psychology 2019;87(10):927–940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Garland EL, Manusov EG, Froeliger B, Kelly A, Williams JM, Howard MO. Mindfulness-oriented recovery enhancement for chronic pain and prescription opioid misuse: results from an early-stage randomized controlled trial. Journal of consulting and clinical psychology 2014;82(3):448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Garrison LP. Regulatory benefit-risk assessment and comparative effectiveness research: strangers, bedfellows or strange bedfellows? Pharmacoeconomics 2010;28(10):855–865. [DOI] [PubMed] [Google Scholar]
- [58].Garrison LP Jr., Towse A, Bresnahan BW. Assessing a structured, quantitative health outcomes approach to drug risk-benefit analysis. Health Aff (Millwood) 2007;26(3):684–695. [DOI] [PubMed] [Google Scholar]
- [59].Gewandter JS, McDermott MP, Evans S, Katz NP, Markman JD, Simon LS, Turk DC, Dworkin RH. Composite outcomes for pain trials: considerations for design and interpretation. Pain 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Glasziou PP, Irwig LM. An evidence based approach to individualising treatment. Bmj 1995;311(7016):1356–1359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [61].Gottlieb S, Woodcock J. Marshaling FDA Benefit-Risk Expertise to Address the Current Opioid Abuse Epidemic. Jama 2017;318(5):421–422. [DOI] [PubMed] [Google Scholar]
- [62].Gregorian RS Jr., Gasik A, Kwong WJ, Voeller S, Kavanagh S. Importance of side effects in opioid treatment: a trade-off analysis with patients and physicians. The journal of pain : official journal of the American Pain Society 2010;11(11):1095–1108. [DOI] [PubMed] [Google Scholar]
- [63].Guo JJ, Pandey S, Doyle J, Bian B, Lis Y, Raisch DW. A review of quantitative risk-benefit methodologies for assessing drug safety and efficacy-report of the ISPOR risk-benefit management working group. Value Health 2010;13(5):657–666. [DOI] [PubMed] [Google Scholar]
- [64].Hale ME, Zimmerman TR, Ma Y, Malamut R. Twelve-month, open-label assessment of long-term safety and abuse potential of hydrocodone extended-release formulated with abuse-deterrence technology in patients with chronic pain. J Opioid Manag 2015;11(5):425–434. [DOI] [PubMed] [Google Scholar]
- [65].Haller H, Lauche R, Sundberg T, Dobos G, Cramer H. Craniosacral therapy for chronic pain: a systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet Disord 2019;21(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [66].Hardy J, Quinn S, Fazekas B, Plummer J, Eckermann S, Agar M, Spruyt O, Rowett D, Currow DC. Randomized, double-blind, placebo-controlled study to assess the efficacy and toxicity of subcutaneous ketamine in the management of cancer pain. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2012;30(29):3611–3617. [DOI] [PubMed] [Google Scholar]
- [67].Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ Open 2017;7(5):e014719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [68].Hauber AB, Arden NK, Mohamed AF, Johnson FR, Peloso PM, Watson DJ, Mavros P, Gammaitoni A, Sen SS, Taylor SD. A discrete-choice experiment of United Kingdom patients’ willingness to risk adverse events for improved function and pain control in osteoarthritis. Osteoarthritis Cartilage 2013;21(2):289–297. [DOI] [PubMed] [Google Scholar]
- [69].Hearn JH, Finlay KA. Internet-delivered mindfulness for people with depression and chronic pain following spinal cord injury: a randomized, controlled feasibility trial. Spinal cord 2018;56(8):750–761. [DOI] [PubMed] [Google Scholar]
- [70].Ho A, Nair S. Chapter Nine - Global Chronic Pain: Public and Population Health Responses. In: Buchman DZ, Davis KD, editors. Developments in Neuroethics and Bioethics, Vol. 1: Academic Press, 2018. pp. 171–189. [Google Scholar]
- [71].Ho M, Saha A, McCleary KK, Levitan B, Christopher S, Zandlo K, Braithwaite RS, Hauber AB. A Framework for Incorporating Patient Preferences Regarding Benefits and Risks into Regulatory Assessment of Medical Technologies. Value in Health 2016;19(6):746–750. [DOI] [PubMed] [Google Scholar]
- [72].Hofmann JF, Lal A, Steffens M, Boettger R. Patient-relevant outcomes and health-related quality of life in patients with chronic, severe, noncancer pain treated with tapentadol prolonged release-Using criteria of health technology assessment. J Opioid Manag 2016;12(5):323–331. [DOI] [PubMed] [Google Scholar]
- [73].Honvo G, Bannuru RR, Bruyère O, Rannou F, Herrero-Beaumont G, Uebelhart D, Cooper C, Arden N, Conaghan PG, Reginster J-Y. Recommendations for the reporting of harms in manuscripts on clinical trials assessing osteoarthritis drugs: a consensus statement from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Drugs & aging 2019;36(1):145–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [74].Hughes D, Waddingham E, Mt‐Isa S, Goginsky A, Chan E, Downey GF, Hallgreen CE, Hockley KS, Juhaeri J, Lieftucht A. Recommendations for benefit–risk assessment methodologies and visual representations. Pharmacoepidemiology and Drug Safety 2016;25(3):251–262. [DOI] [PubMed] [Google Scholar]
- [75].Hunsinger M, Smith SM, Rothstein D, McKeown A, Parkhurst M, Hertz S, Katz NP, Lin AH, McDermott MP, Rappaport BA, Turk DC, Dworkin RH. Adverse event reporting in nonpharmacologic, noninterventional pain clinical trials: ACTTION systematic review. Pain 2014;155(11):2253–2262. [DOI] [PubMed] [Google Scholar]
- [76].ICH. ICH E9 (R1) addendum on estimands and sensitivity analysis in clinical trials to the guideline on statistical principles for clinical trials. 2020.
- [77].Institute of Medicine Characterizing and communicating uncertainty in the assessment of benefits and risks of pharmaceutical products: Workshop summary: National Academies Press, 2014. [PubMed] [Google Scholar]
- [78].Ioannidis JP, Evans SJ, Gøtzsche PC, O’neill RT, Altman DG, Schulz K, Moher D. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Annals of internal medicine 2004;141(10):781–788. [DOI] [PubMed] [Google Scholar]
- [79].Ioannidis JP, Lau J. Completeness of safety reporting in randomized trials: an evaluation of 7 medical areas. Jama 2001;285(4):437–443. [DOI] [PubMed] [Google Scholar]
- [80].Izquierdo Perez H, Alonso Perez JL, Gil Martinez A, La Touche R, Lerma-Lara S, Commeaux Gonzalez N, Arribas Perez H, Bishop MD, Fernandez-Carnero J. Is one better than another?: A randomized clinical trial of manual therapy for patients with chronic neck pain. Manual therapy 2014;19(3):215–221. [DOI] [PubMed] [Google Scholar]
- [81].Jackson Y, Janssen E, Fischer R, Beaverson K, Loftus J, Betteridge K, Rhoten S, Flood E, Lundie M. The evolving role of patient preference studies in health-care decision-making, from clinical drug development to clinical care management. Expert Rev Pharmacoecon Outcomes Res 2019;19(4):383–396. [DOI] [PubMed] [Google Scholar]
- [82].Janssens R, Huys I, van Overbeeke E, Whichello C, Harding S, Kübler J, Juhaeri J, Ciaglia A, Simoens S, Stevens H, Smith M, Levitan B, Cleemput I, de Bekker-Grob E, Veldwijk J. Opportunities and challenges for the inclusion of patient preferences in the medical product life cycle: a systematic review. BMC Med Inform Decis Mak 2019;19(1):189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [83].Jay K, Brandt M, Schraefel M, Jakobsen MD, Sundstrup E, Sjøgaard G, Vinstrup J, Andersen LL. Neurocognitive performance and physical function do not change with physical-cognitive-mindfulness training in female laboratory technicians with chronic musculoskeletal pain: Randomized controlled trial. Medicine (Baltimore) 2016;95(50):e5554–e5554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [84].Jiang C, Wang H, Wang Q, Luo Y, Sidlow R, Han X. Prevalence of Chronic Pain and High-Impact Chronic Pain in Cancer Survivors in the United States. JAMA Oncology 2019;5(8):1224–1226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [85].Johnson FR, Hauber AB, Özdemir S, Lynd L. Quantifying Women’s Stated Benefit–Risk Trade-Off Preferences for IBS Treatment Outcomes. Value in Health 2010;13(4):418–423. [DOI] [PubMed] [Google Scholar]
- [86].Johnson FR, Ozdemir S, Mansfield C, Hass S, Miller DW, Siegel CA, Sands BE. Crohn’s disease patients’ risk-benefit preferences: serious adverse event risks versus treatment efficacy. Gastroenterology 2007;133(3):769–779. [DOI] [PubMed] [Google Scholar]
- [87].Juhaeri J. Benefit-risk evaluation: the past, present and future. Ther Adv Drug Saf 2019;10:2042098619871180–2042098619871180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [88].Katz NP, Mou J, Trudeau J, Xiang J, Vorsanger G, Orman C, Kim M. Development and preliminary validation of an integrated efficacy-tolerability composite measure for the evaluation of analgesics. Pain 2015;156(7):1357–1365. [DOI] [PubMed] [Google Scholar]
- [89].Kendall JC, French SD, Hartvigsen J, Azari MF. Chiropractic treatment including instrument-assisted manipulation for non-specific dizziness and neck pain in community-dwelling older people: a feasibility randomised sham-controlled trial. Chiropr Man Therap 2018;26:14–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [90].Kimball AB, Kerdel F, Adams D, Mrowietz U, Gelfand JM, Gniadecki R, Prens EP, Schlessinger J, Zouboulis CC, van der Zee HH, Rosenfeld M, Mulani P, Gu Y, Paulson S, Okun M, Jemec GBE. Adalimumab for the treatment of moderate to severe Hidradenitis suppurativa: a parallel randomized trial. Annals of internal medicine 2012;157(12):846–855. [DOI] [PubMed] [Google Scholar]
- [91].Kivitz AJ, Gimbel JS, Bramson C, Nemeth MA, Keller DS, Brown MT, West CR, Verburg KM. Efficacy and safety of tanezumab versus naproxen in the treatment of chronic low back pain. Pain 2013;154(7):1009–1021. [DOI] [PubMed] [Google Scholar]
- [92].Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, Callahan L, Copenhaver C, Dodge C, Felson D, Gellar K, Harvey WF, Hawker G, Herzig E, Kwoh CK, Nelson AE, Samuels J, Scanzello C, White D, Wise B, Altman RD, DiRenzo D, Fontanarosa J, Giradi G, Ishimori M, Misra D, Shah AA, Shmagel AK, Thoma LM, Turgunbaev M, Turner AS, Reston J. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol 2020;72(2):220–233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [93].Kraemer HC, Frank E, Kupfer DJ. How to assess the clinical impact of treatments on patients, rather than the statistical impact of treatments on measures. International journal of methods in psychiatric research 2011;20(2):63–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [94].Kress H-G, Aldington D, Alon E, Coaccioli S, Collett B, Coluzzi F, Huygen F, Jaksch W, Kalso E, Kocot-Kępska M, Mangas AC, Ferri CM, Mavrocordatos P, Morlion B, Müller-Schwefe G, Nicolaou A, Hernández CP, Sichère P. A holistic approach to chronic pain management that involves all stakeholders: change is needed. Current Medical Research and Opinion 2015;31(9):1743–1754. [DOI] [PubMed] [Google Scholar]
- [95].Kroenke K, Alford DP, Argoff C, Canlas B, Covington E, Frank JW, Haake KJ, Hanling S, Hooten WM, Kertesz SG. Challenges with implementing the centers for disease control and prevention opioid guideline: a consensus panel report. Pain Medicine 2019;20(4):724–735. [DOI] [PubMed] [Google Scholar]
- [96].Lackey L, Thompson G, Eggers S. FDA’s Benefit–Risk Framework for Human Drugs and Biologics: Role in Benefit–Risk Assessment and Analysis of Use for Drug Approvals. Therapeutic Innovation & Regulatory Science 2021;55(1):170–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [97].LeBaron VT, Camacho F, Balkrishnan R, Yao N, Gilson AM. Opioid Epidemic or Pain Crisis? Using the Virginia All Payer Claims Database to Describe Opioid Medication Prescribing Patterns and Potential Harms for Patients With Cancer. Journal of oncology practice 2019;15(12):e997–e1009. [DOI] [PubMed] [Google Scholar]
- [98].Lee SW, Liong ML, Yuen KH, Leong WS, Khan NK, Krieger JN. Validation of a sham acupuncture procedure in a randomised, controlled clinical trial of chronic pelvic pain treatment. Acupunct Med 2011;29(1):40–46. [DOI] [PubMed] [Google Scholar]
- [99].Leong J, Salek S, Walker S. Benefit-Risk Assessment of Medicines: The Development and Application of a Universal Framework for Decision-Making and Effective Communication: Springer, 2015. [Google Scholar]
- [100].Levitan BS, Andrews EB, Gilsenan A, Ferguson J, Noel RA, Coplan PM, Mussen F. Application of the BRAT framework to case studies: observations and insights. Clinical pharmacology and therapeutics 2011;89(2):217–224. [DOI] [PubMed] [Google Scholar]
- [101].Licciardone JC, Kearns CM, Crow WT. Changes in biomechanical dysfunction and low back pain reduction with osteopathic manual treatment: results from the OSTEOPATHIC Trial. Manual therapy 2014;19(4):324–330. [DOI] [PubMed] [Google Scholar]
- [102].Lluch E, Schomacher J, Gizzi L, Petzke F, Seegar D, Falla D. Immediate effects of active cranio-cervical flexion exercise versus passive mobilisation of the upper cervical spine on pain and performance on the cranio-cervical flexion test. Manual therapy 2014;19(1):25–31. [DOI] [PubMed] [Google Scholar]
- [103].Lynd LD, Marra CA, Najafzadeh M, Sadatsafavi M. A quantitative evaluation of the regulatory assessment of the benefits and risks of rofecoxib relative to naproxen: an application of the incremental net‐benefit framework. Pharmacoepidemiology and drug safety 2010;19(11):1172–1180. [DOI] [PubMed] [Google Scholar]
- [104].Masala S, Calabria E, Cuzzolino A, Raguso M, Morini M, Simonetti G. CT-guided percutaneous pulse-dose radiofrequency for pudendal neuralgia. Cardiovascular and interventional radiology 2014;37(2):476–481. [DOI] [PubMed] [Google Scholar]
- [105].McAlindon TE, Bannuru RR, Sullivan M, Arden N, Berenbaum F, Bierma-Zeinstra S, Hawker G, Henrotin Y, Hunter D, Kawaguchi H. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and cartilage 2014;22(3):363–388. [DOI] [PubMed] [Google Scholar]
- [106].Mecklenburg G, Smittenaar P, Erhart-Hledik JC, Perez DA, Hunter S. Effects of a 12-Week Digital Care Program for Chronic Knee Pain on Pain, Mobility, and Surgery Risk: Randomized Controlled Trial. Journal of medical Internet research 2018;20(4):e156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [107].Meske DS, Lawal OD, Elder H, Langberg V, Paillard F, Katz N. Efficacy of opioids versus placebo in chronic pain: a systematic review and meta-analysis of enriched enrollment randomized withdrawal trials. J Pain Res 2018;11:923–934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [108].Molegraaf MJ, Torensma B, Lange CP, Lange JF, Jeekel J, Swank DJ. Twelve-year outcomes of laparoscopic adhesiolysis in patients with chronic abdominal pain: A randomized clinical trial. Surgery 2017;161(2):415–421. [DOI] [PubMed] [Google Scholar]
- [109].Monticone M, Ambrosini E, Rocca B, Cazzaniga D, Liquori V, Pedrocchi A, Vernon H. Group-based multimodal exercises integrated with cognitive-behavioural therapy improve disability, pain and quality of life of subjects with chronic neck pain: a randomized controlled trial with one-year follow-up. Clin Rehabil 2017;31(6):742–752. [DOI] [PubMed] [Google Scholar]
- [110].Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesic success. Bmj 2013;346:f2690. [DOI] [PubMed] [Google Scholar]
- [111].Mt-Isa S, Hallgreen CE, Wang N, Callreus T, Genov G, Hirsch I, Hobbiger SF, Hockley KS, Luciani D, Phillips LD, Quartey G, Sarac SB, Stoeckert I, Tzoulaki I, Micaleff A, Ashby D. Balancing benefit and risk of medicines: a systematic review and classification of available methodologies. Pharmacoepidemiol Drug Saf 2014;23(7):667–678. [DOI] [PubMed] [Google Scholar]
- [112].Mt‐Isa S, Ouwens M, Robert V, Gebel M, Schacht A, Hirsch I. Structured benefit–risk assessment: a review of key publications and initiatives on frameworks and methodologies. Pharmaceutical statistics 2016;15(4):324–332. [DOI] [PubMed] [Google Scholar]
- [113].Mühlbacher AC, Juhnke C. Patient preferences versus physicians’ judgement: does it make a difference in healthcare decision making? Applied health economics and health policy 2013;11(3):163–180. [DOI] [PubMed] [Google Scholar]
- [114].National Academies of Sciences E, Medicine. Pain management and the opioid epidemic: balancing societal and individual benefits and risks of prescription opioid use: National Academies Press, 2017. [PubMed] [Google Scholar]
- [115].Patel KV, Guralnik JM, Dansie EJ, Turk DC. Prevalence and impact of pain among older adults in the United States: findings from the 2011 National Health and Aging Trends Study. Pain 2013;154(12):2649–2657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [116].Pergolizzi JV, Varrassi G, Paladini A, LeQuang J. Stopping or Decreasing Opioid Therapy in Patients on Chronic Opioid Therapy. Pain and therapy 2019;8(2):163–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [117].Persson LCG, Lansinger B, Carlsson J, Gard G. Expectations of Qigong and Exercise Therapy in Patients With Long-term Neck Pain: An Analysis of a Prospective Randomized Study. J Manipulative Physiol Ther 2017;40(9):676–684. [DOI] [PubMed] [Google Scholar]
- [118].Peryer G, Golder S, Junqueira DR, Vohra S, Loke YK, Group CAEM. Adverse effects. Cochrane Handbook for Systematic Reviews of Interventions 2019:493–505.
- [119].Petersen T, Larsen K, Nordsteen J, Olsen S, Fournier G, Jacobsen S. The McKenzie method compared with manipulation when used adjunctive to information and advice in low back pain patients presenting with centralization or peripheralization: a randomized controlled trial. Spine (Phila Pa 1976) 2011;36(24):1999–2010. [DOI] [PubMed] [Google Scholar]
- [120].Phillips LD. Benefit-risk methodology project: work package 2 report: applicability of current tools and processes for regulatory benefit-risk assessment. European Medicines Agency; 2011. [Google Scholar]
- [121].Pound P, Nicol CJ. Retrospective harm benefit analysis of pre-clinical animal research for six treatment interventions. PloS one 2018;13(3). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [122].Psaty BM, Korn D. Congress responds to the IOM Drug Safety Report—in full. Jama 2007;298(18):2185–2187. [DOI] [PubMed] [Google Scholar]
- [123].Quartey G, Ke C, Chuang-Stein C, He W, Jiang Q, Tsai K-T, Song G, Scott J. Overview of benefit–risk evaluation methods: A spectrum from qualitative to quantitative. Benefit-Risk Assessment Methods in Medical Product Development: Bridging Qualitative and Quantitative Assessments 2016;145. [Google Scholar]
- [124].Ray WA, Stein CM. Reform of drug regulation—beyond an independent drug-safety board: Mass Medical Soc, 2006. [DOI] [PubMed] [Google Scholar]
- [125].Reaney M, Bush E, New M, Paty J, de Climens AR, Skovlund SE, Nelsen L, Flood E, Gater A. The Potential Role of Individual-Level Benefit-Risk Assessment in Treatment Decision Making: A DIA Study Endpoints Community Workstream. Therapeutic Innovation & Regulatory Science 2019;53(5):630–638. [DOI] [PubMed] [Google Scholar]
- [126].Richardson CG, Chalmers A, Llewellyn-Thomas HA, Klinkhoff A, Carswell A, Kopec JA. Pain relief in osteoarthritis: patients’ willingness to risk medication-induced gastrointestinal, cardiovascular, and cerebrovascular complications. J Rheumatol 2007;34(7):1569–1575. [PubMed] [Google Scholar]
- [127].Richesson RL, Fung KW, Krischer JP. Heterogeneous but “standard” coding systems for adverse events: Issues in achieving interoperability between apples and oranges. Contemporary clinical trials 2008;29(5):635–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [128].Saner J, Kool J, Sieben JM, Luomajoki H, Bastiaenen CH, de Bie RA. A tailored exercise program versus general exercise for a subgroup of patients with low back pain and movement control impairment: A randomised controlled trial with one-year follow-up. Manual therapy 2015;20(5):672–679. [DOI] [PubMed] [Google Scholar]
- [129].Sanga P, Katz N, Polverejan E, Wang S, Kelly KM, Haeussler J, Thipphawong J. Long-Term Safety and Efficacy of Fulranumab in Patients With Moderate-to-Severe Osteoarthritis Pain: A Phase II Randomized, Double-Blind, Placebo-Controlled Extension Study. Arthritis & rheumatology (Hoboken, NJ) 2017;69(4):763–773. [DOI] [PubMed] [Google Scholar]
- [130].Sathanapally H, Sidhu M, Fahami R, Gillies C, Kadam U, Davies MJ, Khunti K, Seidu S. Priorities of patients with multimorbidity and of clinicians regarding treatment and health outcomes: a systematic mixed studies review. BMJ Open 2020;10(2):e033445–e033445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [131].Shah SL, Janisch NH, Crowell M, Lacy BE. Patients with irritable bowel syndrome are willing to take substantial medication risks for symptom relief. Clinical Gastroenterology and Hepatology 2021;19(1):80–86. [DOI] [PubMed] [Google Scholar]
- [132].Shaw PA. Use of composite outcomes to assess risk–benefit in clinical trials. Clinical Trials 2018;15(4):352–358. [DOI] [PubMed] [Google Scholar]
- [133].Sieper J, van der Heijde D, Dougados M, Maksymowych WP, Scott BB, Boice JA, Berd Y, Bergman G, Curtis S, Tzontcheva A, Huyck S, Weng HH. A randomized, double-blind, placebo-controlled, sixteen-week study of subcutaneous golimumab in patients with active nonradiographic axial spondyloarthritis. Arthritis Rheumatol 2015;67(10):2702–2712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [134].Simon LS, Strand CV, Boers M, Brooks PM, Tugwell PS, Bombardier C, Fries JF, Henry D, Goldkind L, Guyatt G. How to ascertain drug safety in the context of benefit. Controversies and concerns. The Journal of rheumatology 2009;36(9):2114–2121. [DOI] [PubMed] [Google Scholar]
- [135].Sir E, Batur Sir GD. Evaluating treatment modalities in chronic pain treatment by the multi-criteria decision making procedure. BMC medical informatics and decision making 2019;19(1):191–191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [136].Smith Dworkin. Prospective clinical trial registration: not sufficient, but always necessary. Anaesthesia 2018;73(5):538–541. [DOI] [PubMed] [Google Scholar]
- [137].Smith, Dworkin RH, Turk DC, McDermott MP, Eccleston C, Farrar JT, Rowbotham MC, Bhagwagar Z, Burke LB, Cowan P, Ellenberg SS, Evans SR, Freeman RL, Garrison LP, Iyengar S, Jadad A, Jensen MP, Junor R, Kamp C, Katz NP, Kesslak JP, Kopecky EA, Lissin D, Markman JD, Mease PJ, O’Connor AB, Patel KV, Raja SN, Sampaio C, Schoenfeld D, Singh J, Steigerwald I, Strand V, Tive LA, Tobias J, Wasan AD, Wilson HD. Interpretation of chronic pain clinical trial outcomes: IMMPACT recommended considerations. Pain 2020;Articles in Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [138].Smith SM, Chang RD, Pereira A, Shah N, Gilron I, Katz NP, Lin AH, McDermott MP, Rappaport BA, Rowbotham MC, Sampaio C, Turk DC, Dworkin RH. Adherence to CONSORT harms-reporting recommendations in publications of recent analgesic clinical trials: an ACTTION systematic review. Pain 2012;153(12):2415–2421. [DOI] [PubMed] [Google Scholar]
- [139].Smith SM, Wang AT, Katz NP, McDermott MP, Burke LB, Coplan P, Gilron I, Hertz SH, Lin AH, Rappaport BA, Rowbotham MC, Sampaio C, Sweeney M, Turk DC, Dworkin RH. Adverse event assessment, analysis, and reporting in recent published analgesic clinical trials: ACTTION systematic review and recommendations. Pain 2013;154(7):997–1008. [DOI] [PubMed] [Google Scholar]
- [140].Stahlschmidt L, Zernikow B, Wager J. Satisfaction With an Intensive Interdisciplinary Pain Treatment for Children and Adolescents: An Independent Outcome Measure? Clin J Pain 2018;34(9):795–803. [DOI] [PubMed] [Google Scholar]
- [141].Takahashi H, Okuni I, Ushigome N, Harada T, Tsuruoka H, Ohshiro T, Sekiguchi M, Musya Y. Low level laser therapy for patients with cervical disk hernia. Laser Ther 2012;21(3):193–197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [142].Tan G, Rintala DH, Jensen MP, Fukui T, Smith D, Williams W. A randomized controlled trial of hypnosis compared with biofeedback for adults with chronic low back pain. European journal of pain (London, England) 2015;19(2):271–280. [DOI] [PubMed] [Google Scholar]
- [143].Tchivileva IE, Lim PF, Smith SB, Slade GD, Diatchenko L, McLean SA, Maixner W. Effect of catechol-O-methyltransferase polymorphism on response to propranolol therapy in chronic musculoskeletal pain: a randomized, double-blind, placebo-controlled, crossover pilot study. Pharmacogenet Genomics 2010;20(4):239–248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [144].Teutsch SM, Bradley LA, Palomaki GE, Haddow JE, Piper M, Calonge N, Dotson WD, Douglas MP, Berg AO. The evaluation of genomic applications in practice and prevention (EGAPP) initiative: methods of the EGAPP working group. Genetics in medicine 2009;11(1):3–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [145].Thompson DP, Oldham JA, Woby SR. Does adding cognitive-behavioural physiotherapy to exercise improve outcome in patients with chronic neck pain? A randomised controlled trial. Physiotherapy 2016;102(2):170–177. [DOI] [PubMed] [Google Scholar]
- [146].Tsintis P, La Mache E. CIOMS and ICH initiatives in pharmacovigilance and risk management. Drug safety 2004;27(8):509–517. [DOI] [PubMed] [Google Scholar]
- [147].Turk, Dworkin RH, Allen RR, Bellamy N, Brandenburg N, Carr DB, Cleeland C, Dionne R, Farrar JT, Galer BS, Hewitt DJ, Jadad AR, Katz NP, Kramer LD, Manning DC, McCormick CG, McDermott MP, McGrath P, Quessy S, Rappaport BA, Robinson JP, Royal MA, Simon L, Stauffer JW, Stein W, Tollett J, Witter J. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003;106(3):337–345. [DOI] [PubMed] [Google Scholar]
- [148].Turk D, Boeri M, Abraham L, Atkinson J, Bushmakin AG, Cappelleri JC, Hauber B, Klein K, Russo L, Viktrup L, Walsh D. Patient preferences for osteoarthritis pain and chronic low back pain treatments in the United States: a discrete-choice experiment. Osteoarthritis Cartilage 2020;28(9):1202–1213. [DOI] [PubMed] [Google Scholar]
- [149].US Department of Health Human Services. Pain management best practices Inter-Agency Task force report: updates, gaps, inconsistencies, and recommendations. Retrieved from US Department of Health and Human Services website: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html Accessed Dec 2019.
- [150].Valenza MC, Rodriguez-Torres J, Cabrera-Martos I, Diaz-Pelegrina A, Aguilar-Ferrandiz ME, Castellote-Caballero Y. Results of a Pilates exercise program in patients with chronic non-specific low back pain: a randomized controlled trial. Clin Rehabil 2017;31(6):753–760. [DOI] [PubMed] [Google Scholar]
- [151].van Overbeeke E, Vanbinst I, Jimenez-Moreno AC, Huys I. Patient Centricity in Patient Preference Studies: The Patient Perspective. Front Med (Lausanne) 2020;7:93–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [152].Verra ML, Angst F, Brioschi R, Lehmann S, Benz T, Aeschlimann A, De Bie RA, Staal JB. Effectiveness of subgroup-specific pain rehabilitation: a randomized controlled trial in patients with chronic back pain. Eur J Phys Rehabil Med 2018;54(3):358–370. [DOI] [PubMed] [Google Scholar]
- [153].Vranken MJ, Schutjens MHD, Mantel‐Teeuwisse AK. The double opioid crisis: A call for balance. Pharmacoepidemiology and drug safety 2019;28(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [154].Walker S, McAuslane N, Liberti L, Leong J, Salek S. A Universal Framework for the Benefit-Risk Assessment of Medicines: Is This the Way Forward? Ther Innov Regul Sci 2015;49(1):17–25. [DOI] [PubMed] [Google Scholar]
- [155].Ware MA, Wang T, Shapiro S, Collet JP. Cannabis for the Management of Pain: Assessment of Safety Study (COMPASS). The journal of pain : official journal of the American Pain Society 2015;16(12):1233–1242. [DOI] [PubMed] [Google Scholar]
- [156].Wasan AD, Michna E, Edwards RR, Katz JN, Nedeljkovic SS, Dolman AJ, Janfaza D, Isaac Z, Jamison RN. Psychiatric Comorbidity Is Associated Prospectively with Diminished Opioid Analgesia and Increased Opioid Misuse in Patients with Chronic Low Back Pain. Anesthesiology 2015;123(4):861–872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [157].Wen S, Zhang L, Yang B. Two approaches to incorporate clinical data uncertainty into multiple criteria decision analysis for benefit-risk assessment of medicinal products. Value Health 2014;17(5):619–628. [DOI] [PubMed] [Google Scholar]
- [158].Williams A, Wiggers J, OʼBrien KM, Wolfenden L, Yoong SL, Hodder RK, Lee H, Robson EK, McAuley JH, Haskins R, Kamper SJ, Rissel C, Williams CM. Effectiveness of a healthy lifestyle intervention for chronic low back pain: a randomised controlled trial. Pain 2018;159(6):1137–1146. [DOI] [PubMed] [Google Scholar]
- [159].Williams MR, McKeown A, Pressman Z, Hunsinger M, Lee K, Coplan P, Gilron I, Katz NP, McDermott MP, Raja SN, Rappaport BA, Rowbotham MC, Turk DC, Dworkin RH, Smith SM. Adverse Event Reporting in Clinical Trials of Intravenous and Invasive Pain Treatments: An ACTTION Systematic Review. The journal of pain : official journal of the American Pain Society 2016;17(11):1137–1149. [DOI] [PubMed] [Google Scholar]
- [160].Wilson RD, Gunzler DD, Bennett ME, Chae J. Peripheral nerve stimulation compared with usual care for pain relief of hemiplegic shoulder pain: a randomized controlled trial. Am J Phys Med Rehabil 2014;93(1):17–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [161].Woloshin S, Schwartz LM. Communicating Data About the Benefits and Harms of Treatment: A Randomized Trial. Annals of Internal Medicine 2011;155(2):87–96. [DOI] [PubMed] [Google Scholar]
- [162].Yoon DH, Bin SI, Chan SK, Chung CK, In Y, Kim H, Lichauco JJ, Mok CC, Moon YW, Ng TK, Penserga EG, Shin DA, You D, Moon H. Effectiveness and tolerability of transdermal buprenorphine patches: a multicenter, prospective, open-label study in Asian patients with moderate to severe chronic musculoskeletal pain. BMC Musculoskelet Disord 2017;18(1):337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [163].Zafiropoulos N, Phillips LD, Pignatti F, Luria X. Evaluating benefit-risk: An agency perspective. Regulatory Rapporteur 2012;9(6):5–8. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.