

Testosterone products have been approved by the Food and Drug Administration (FDA) for replacement therapy in men with “classic hypogonadism” — primary or secondary hypogonadism caused by specific, well-recognized medical conditions, such as Klinefelter syndrome, pituitary injury, or toxic damage to the testicles.1 Treatment with testosterone to restore serum concentrations in men with classic hypogonadism has long been considered the standard of care. On the basis of this intended use, we at the FDA have required only that testosterone products reliably bring low serum testosterone concentrations into the normal range, defined as the concentrations seen in healthy young men. The FDA has not mandated that clinical trials show improvements in signs or symptoms of hypogonadism in order for a testosterone product to be approved.
In recent years, however, testosterone use has increased markedly among middle-aged and elderly men for a controversial condition that the FDA calls “age-related hypogonadism.” This condition, also referred to as “late-onset hypogonadism,” is typically diagnosed in men who, for no discernable reason other than advanced age, have serum testosterone concentrations below the normal range for healthy young men, as well as signs and symptoms that may or may not be caused by low testosterone concentrations.2 Serum testosterone appears to decline as men age,3 and although this decline is usually modest, concentrations can fall below the normal range for healthy young men. In these cases, it is unclear whether coexisting nonspecific signs and symptoms, such as decreases in energy and muscle mass, are a consequence of the age-related decline in endogenous testosterone or whether they are a result of other factors, such as coexisting conditions, concomitant medications, or perhaps aging itself.
In 2002, prompted by the growing numbers of older men using testosterone to delay or treat a variety of signs and symptoms, the Institute of Medicine formed a committee to assess the state of knowledge regarding testosterone therapy. After reviewing the medical literature, the committee concluded that the available evidence on the effects of testosterone therapy in older men was limited and inconclusive.4 To date, there is no definitive evidence that increasing serum testosterone concentrations in these men is beneficial and safe, and the need to replace testosterone in older men who lack a distinct, well-recognized cause of hypogonadism remains debatable.
Despite these uncertainties, older men have been the target of direct-to-consumer advertisements for testosterone products and nonbranded disease-awareness campaigns for “low T” that imply treatment benefits that are not supported by substantial evidence from controlled trials. An analysis by the FDA showed that more than 80% of prescription testosterone users are men between 40 and 74 years of age (see graph).1 The most common International Classification of Diseases, 9th revision (ICD-9) diagnosis code associated with testosterone use is testicular hypofunction, not elsewhere classified (ICD-9 code 257.2), which does not specify a distinct, well-recognized cause of hypogonadism.1 The average duration of use in these patients is relatively brief (approximately 6 months over the 5-year period examined), which is inconsistent with the need for lifelong hormone replacement in men with classic hypogonadism. The FDA also sampled a health claims data set and found that 28% of men who received a new testosterone prescription had no evidence of a prior serum testosterone measurement.1 Others have estimated even higher rates of omission of testing.5 Given these patterns of use, it appears that a majority of men prescribed testosterone may have age-related hypogonadism rather than classic hypogonadism.
Estimated Number of Men with a Prescription Claim for a Testosterone Product in U.S. Outpatient Retail Pharmacies, Stratified by Age, 2010–2013.
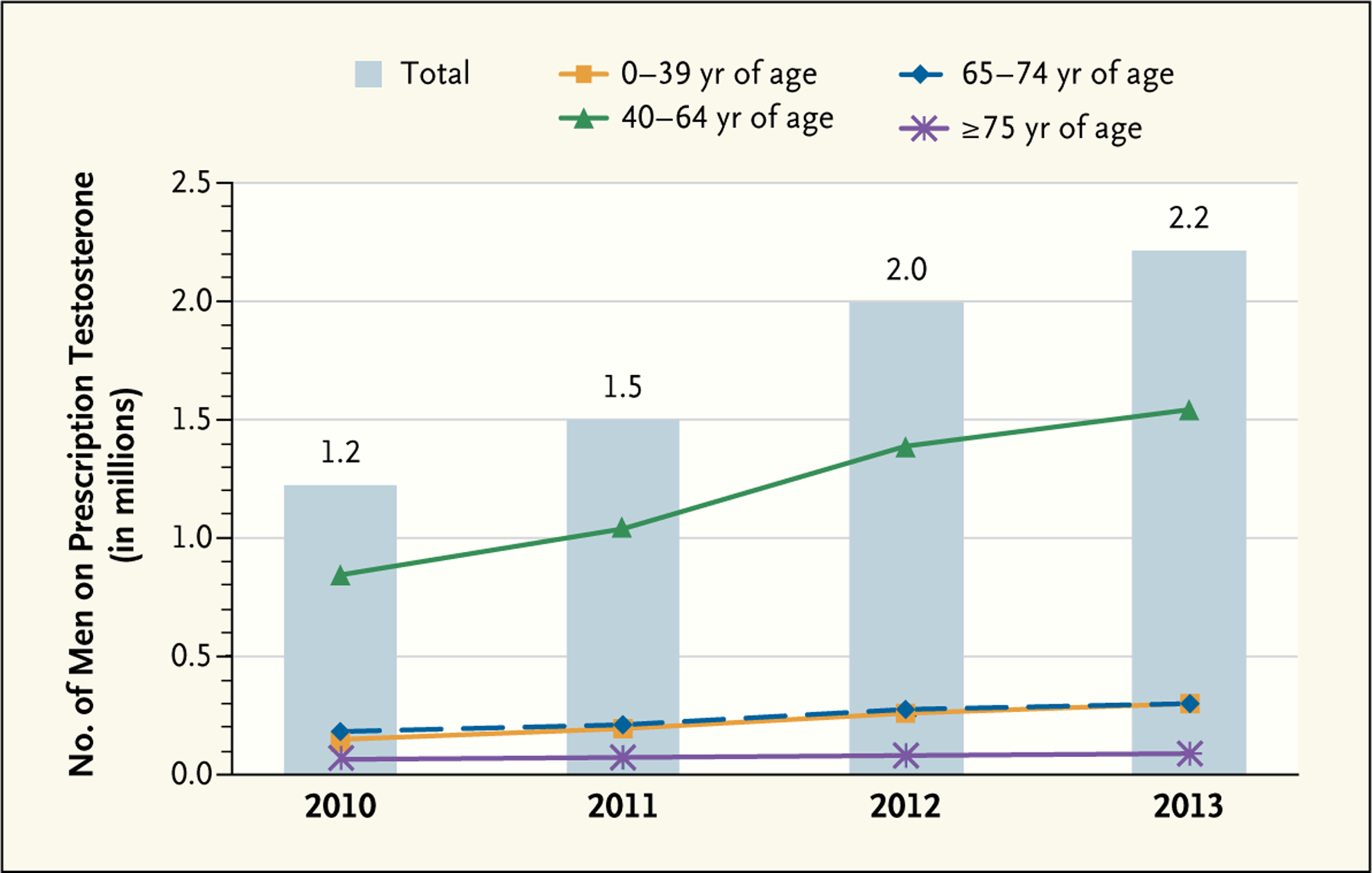
Data are from Symphony Healthcare Solutions Anonymous Patient Longitudinal Database, extracted May 2014.
These findings are troubling in light of evidence from recent large observational studies that suggests potential cardiovascular risk associated with testosterone use. The FDA reviewed five retrospective cohort studies and two meta-analyses of controlled trials on this topic.1 Two of the cohort studies found a significant increase in cardiovascular events associated with testosterone use, whereas two others found a significant reduction in all-cause mortality. The final study found no significant change in the risk of hospitalization for myocardial infarction among testosterone users. The authors of these five studies evaluated a variety of data sources, patient populations, testosterone formulations, and outcomes over a range of follow-up times and performed different statistical adjustments for confounders or time-varying covariates, making it difficult to integrate the findings in a meaningful manner. The meta-analyses also had conflicting findings — one reported an increased risk of broadly defined cardiovascular-related adverse events among testosterone users; the other reported no additional risk of major adverse cardiovascular events. Although the limitations and potential confounders or biases in these studies preclude a clear conclusion regarding the role of testosterone therapy in adverse cardiovascular outcomes, a possible association cannot be over-looked. To date, no randomized, controlled trials have been appropriately designed to evaluate cardiovascular outcomes with testosterone use.
The FDA convened an advisory committee meeting in September 2014 to discuss the use of testosterone for age-related hypogonadism and the recent signal of cardiovascular risk. The committee members concluded that the available evidence supports an indication for testosterone therapy only in men with classic hypogonadism and that drug labels should state that the efficacy and safety of testosterone products have not been established for age-related hypogonadism. In addition, because there is no evidence of laboratory testing before the initial testosterone prescription for some men, committee members recommended adding a statement to drug labels about the need to confirm low serum testosterone concentrations before initiating treatment. The committee acknowledged the limitations of the available data on adverse cardiovascular events but concluded that the totality of the evidence suggests a weak signal of cardiovascular risk and recommended updating drug labels to reflect this information. The FDA agreed with the advisory committee’s recommendations and subsequently required revisions to the labels of all testosterone products. Committee members also commented that only a controlled clinical trial — not observational studies — will be able to definitively determine the effects of testosterone therapy on cardiovascular outcomes.
Given the widespread use of testosterone for age-related hypogonadism, the lack of substantial evidence to support such use, and the unknown effect of the label changes on prescribing patterns, the cardiovascular safety of testosterone products in older men remains an important public health concern. To better determine the effects of testosterone therapy on cardiovascular outcomes among users, the FDA is requiring companies that manufacture these products to conduct a controlled clinical trial. We are encouraging companies to work together on a single trial. We believe the health of American men will be well served by the presence of accurate drug labels and reliable data to inform clinical decision making.
Footnotes
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References
- 1.FDA briefing document for the joint meeting for Bone, Reproductive, and Urologic Drugs Advisory Committee (BRUDAC) and the Drug Safety and Risk Management Advisory Committee (DSARMAC). Silver Spring, MD: FDA Advisory Committee, September 17, 2014 (http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ReproductiveHealthDrugsAdvisoryCommittee/UCM412536.pdf). [DOI] [PubMed] [Google Scholar]
- 2.Wang C, Nieschlag E, Swerdloff R, et al. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Int J Impot Res 2009;21:1–8. [DOI] [PubMed] [Google Scholar]
- 3.Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. J Clin Endocrinol Metab 2001; 86:724–31. [DOI] [PubMed] [Google Scholar]
- 4.Institute of Medicine. Testosterone and aging: clinical research directions. Washington, DC: National Academies Press, 2004. [PubMed] [Google Scholar]
- 5.Layton JB, Li D, Meier CR, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab 2014;99:835–42. [DOI] [PMC free article] [PubMed] [Google Scholar]