

Abstract
OBJECTIVE
Subgroups of adolescent single and dual e-cigarette and cigarette users have been identified, but usage patterns have changed in recent years, and there has been an increase in marijuana use. Research is needed with current data to identify subgroups of use including marijuana and determine their behavioral correlates.
METHODS
We cross classified ever and recent use of e-cigarettes, combustible cigarettes, and marijuana among US high school students in the 2019 Youth Risk Behavior Survey (YRBS), providing 8 different groups. Levels of 14 risk and protective factors were compared across groups in general linear models with demographic covariates by using omnibus tests, pairwise comparisons, and planned contrasts. Replicability was tested through identical analyses for 2017 YRBS data.
RESULTS
The nonuser group was 43.9% of the sample. The most frequent user groups were triple users (ever-use proportion: 16.9%), dual (e-cigarette and marijuana) users (15.8%), and exclusive e-cigarette users (13.2%). For risk profiles on levels of psychosocial variables, the triple-user group was typically elevated above all other groups. Exclusive e-cigarette users were above nonusers in risk profile but below dual users (both cigarettes and marijuana). Results were similar for ever use and recent use. The patterning of results in 2019 YRBS data were closely replicated in 2017 YRBS data.
CONCLUSIONS
Co-occurrence of e-cigarette, cigarette, and marijuana use is currently substantial among adolescents and is associated with an elevated psychosocial risk profile. This has implications for both epidemiology and prevention studies. Further research is needed to study prevalence and identify pathways to triple use.
Use of electronic nicotine delivery systems (hereafter, e-cigarettes) among US adolescents has increased considerably in recent years.1 The current prevalence of recent (30 day) use is 27.5% among high school students,2 and many youth e-cigarette users report use of devices containing nicotine.3 The substantial prevalence and use of nicotine has raised concerns about development of nicotine dependence4,5 and transitions to cigarette smoking6–9 or marijuana use10–13 as well as health consequences for adolescents.14
E-cigarette users are not a homogeneous population. Some adolescents use e-cigarettes exclusively, and some combine e-cigarette use with cigarette smoking (ie, dual users15,16). Profiles on psychosocial factors that increase odds of adverse health and social outcomes (eg, psychiatric symptomatology, aggressive behavior) typically show exclusive e-cigarette users elevated above nonusers but lower than dual users.16–20 However, these studies were based mostly on data from before 2015, but since that time there has been a decline in cigarette smoking and an increase in marijuana use.21,22A linkage between e-cigarette use and marijuana initiation has been demonstrated in several studies,10–13 and some data suggest marijuana having adverse effects not in common with e-cigarettes or cigarettes.23,24 This suggests more attention to the triple concurrence of e-cigarettes, cigarettes, and marijuana.
The aim of this research was to determine the relative prevalence of various patterns of usage for the 3 substances in current data and test how different combined patterns of usage are related to established predictors of risk from the epidemiology literature. We determined groupings of single and combined use of e-cigarettes, cigarettes, and marijuana in a 2019 nationally representative sample of high school students and compared levels of risk and protective factors across groups. For testing group differences, we selected variables from several theoretical domains that have a history of empirical validation for predicting smoking and other substance use in adolescence; these include antisocial behavior and low academic competence,25,26 psychiatric symptomatology and illicit drug use,27 and cognitive protective factors, such as conscientiousness and health-protective behavior.28–30
Extending from previous findings that exclusive users of e-cigarettes have a lower risk profile than dual users do,15,16 we hypothesized that exclusive users of any substance (including cigarettes and marijuana) would have a lower risk profile compared with dual users. Deriving from the fact that marijuana has historically been illegal in the United States31,32 and has been linked in longitudinal studies to more adverse outcomes in the domains of antisocial behavior, interpersonal relationships, and educational attainment,33 we hypothesized that groups including marijuana use would have a higher risk profile than groups that did not.
We selected variables from 6 theoretical domains to test whether group differences are specific or general ones and combined the variables in a composite risk index. The use of composite risk indexes has a considerable history in adolescent research, deriving from original studies by Bry et al34 and Newcomb et al35 and continuing in areas such as community psychology, program evaluation, and developmental psychology.36–38 For the present research, we focused on the most recently available data, the 2019 Youth Risk Behavior Survey (YRBS) survey. For testing replicability of effects, we compared the results with comparable analyses for 2017 YRBS data. We conducted analyses for both ever use and recent (30 day) use of the 3 substances. This controls for level of consumption because persons who report recent use are more likely to be frequent users, compared with persons who simply report ever having used a substance.
Methods
The 2019 YRBS is conducted biyearly by the Centers for Disease Control and Prevention (CDC) using a multistage design to produce a representative sample of ninth through 12th grade students in public and private schools in the United States.39 From 181 schools selected, there was a 75% school response rate and 80% student response rate. A 99-item questionnaire was administered to students in classrooms by trained research staff using a standardized protocol that emphasizes voluntary and anonymous participation. Local procedures were used for parental permission, including signed parental consent and alternative (opt in) procedures.39 A total of 13 677 usable questionnaires were obtained. The present research uses anonymized data obtained from CDC and was approved by the Institutional Review Board of the University of Hawaii at Manoa. (The 2017 YRBS had the same methodology, a 75% school response rate, 81% student response rate, and 14 765 usable questionnaires.) Methodologic studies have repeatedly supported the reliability and validity of the YRBS measures for assessing health risk behavior and adolescent substance use.39–43
Substance Use Grouping Questions
E-cigarette Use
Items covered ever use (“Have you ever used an electronic vapor product?” (no or yes) and recent use (“During the past 30 days, on how many days did you use an electronic vapor product?”: 7 responses, 0 days to all 30 days).
Cigarette Smoking
Items covered ever smoking (“Have you ever tried cigarette smoking, even one or 2 puffs?”: no or yes) and recent smoking (“During the past 30 days, on how many days did you smoke cigarettes?”: 7 responses, 0 days to all 30 days).
Marijuana
Items for marijuana tapped ever use (“During your life, how many times have you used marijuana?”: 7 responses, 0 times to 100 or more times) and recent use (“During the past 30 days, how many times did you use marijuana?”: 6 responses, 0 times to 40 or more times).
Covariates: Demographics
Items asked about age in years (7 responses, 12 through 18 years) and sex (dichotomous). Items about ethnicity (“Are you Hispanic or Latino?”: yes or no) and race (“What is your race?”: 5 options, multiple responding allowed) were combined by CDC in an 8-category measure termed race and ethnicity.
Risk and Protective Factors
Measures assessing 14 risk and protective factors representing 6 theoretical domains are described in Table 1 For each measure the table includes the literal item and response scale.
TABLE 1.
Measures of Psychosocial Risk and Protective Factors
| Risk Factors | |
|---|---|
| Antisocial Behavior | Item wording / Response scale |
| Fighting | The item asked, “During the past 12 months, how many times were you in a physical fight?” (8 responses, 0 times to 12 or more times). |
| General weapon carrying | “During the past 30 days, how many days did you carry a weapon such as a gun, knife, or club?” (5 responses, 0 days to 6 or more days). |
| Weapon carrying at school | “During the past 30 days, how many days did you carry a weapon such as a gun, knife, or club on school property?” (5 responses, 0 days to 6 or more days). |
| Psychiatric symptomatology | |
| Depression | The item asked, “During the past 12 months, did you ever feel so sad and hopeless almost every day for 2 weeks or more in a row that you stopped doing some usual activities?” (no or yes). |
| Suicide ideation | An item on suicide ideation asked, “During the past 12 months, did you ever seriously consider committing suicide?” (no or yes). |
| Sexual risk behavior | |
| Sexual history | An item on lifetime sexual history asked, “Have you ever had sexual intercourse?” (no or yes). |
| Lifetime No. partners | “During your life, with how many people have you had sexual intercourse?” (7 responses; never had sexual intercourse to had intercourse with 6 or more people). |
| Collateral substance use | |
| Lifetime alcohol history | “How old were you when you had your first drink of alcohol, other than a few sips?” (7 responses, never had alcohol to 17 years or older). |
| Recent alcohol use | “During the past 30 days, on how many days did you have at least 1 drink of alcohol?” (7 responses, 0 d to all 30 days). |
| Recent binge drinking | “During the past 30 days, on how many days did you have 4 or more drinks in a row, that is, within a couple of hours (if female) or 5 or more drinks of alcohol in a row (if you are male)?” (7 responses, 0 days to 20 or more days). |
| Inhalant use | The item asked, “During your life, how many times have you sniffed glue, breathed the contents of aerosol spray cans, or inhaled any paints or sprays to get high?” (6 responses, 0 times to 40 or more times). |
| Nonauthorized prescription drug use | The item asked, “During your life, how many times have you taken prescription pain medicine without a doctor’s prescription or differently from how a doctor told you how to use it?” (6 responses, 0 times to 40 or more times). |
| Protective factors | |
| School grades | Academic performance was indexed by using the following question: “During the past year how would you describe your grades in school?” (5 responses, mostly Fs to mostly As). |
| Seat belt use | An item on self-protective behavior asked, “How often do you wear a seat belt when riding in a car driven by someone else?” (5 responses, never to always). |
Composite Risk Score
We constructed a composite risk score based on dichotomized indices (lower risk versus high risk) for each of the 14 risk and protective factors. Consistent with procedures used in the literature on composite risk scores,34–38 we did not assign differential importance to any factor but rather gave a dichotomous (0,1) score for risk status for each variable, with continuous variables cut at approximately the 20th percentile (upper 20th for risk factors and lower 20th for protective factors). For dichotomous variables (eg, past-year depression), a two-way cut was implemented for the original metric of the variable. The binary indices were summed, providing a composite score with a 0–14 possible range (α = 0.75).
Data Analysis
Weighted prevalence estimates for basic study characteristics were estimated in SAS PROC SURVEYFREQ (SAS Institute, Inc, Cary, NC), with adjustment for stratum and clustering. For this other analyses, we used listwise deletion for missing data. Consistent with procedures of previous research on substance use groupings,14–20 data for ever and 30-day e-cigarette, cigarette, and marijuana use were dichotomized (no use ever or past 30 days versus any use ever or past 30 days). If a response for a given product was missing, then this was treated as missing data. The dichotomous variables were cross classified to form 8 substance use groupings, 1 for ever use and 1 for 30-day use; we then compared the patterning of findings for ever use and 30-day use. This controls for level of consumption because persons who report use in the past 30 days are likely to be more frequent users.
Associations of the substance use groups with the 14 risk and protective factors were analyzed in PROC GLM, treating substance use group as a class variable, with adjustment for age, sex, and race and ethnicity. Because there were significant differences in the prevalence of substance use groups by race and ethnicity as well as differences in levels of psychosocial variables, race and ethnicity was included as a covariate to avoid confounding. The analytic model was: [risk behavior] = [grouping variable] [demographic covariates]. Race and ethnicity was analyzed by using 5 dummy variables that contrasted Asian Americans, Black non-Hispanic individuals, Hispanic individuals, multiracial Hispanic individuals, and multiracial non-Hispanic individuals against white non-Hispanic individuals as the reference group. Adjusted means were computed for the 14 variables using the OM option because the substance use groups differed considerably in size. Pairwise comparisons using SAS default parameters compared levels of risk and protective factors across groups for each variable.
For an overall test of the hypotheses, we performed 3 contrasts to determine how group membership was related to problematic status on each psychosocial risk or protective variable, using the same definitions implemented for constructing the composite risk score (ie,~>80th percentile on the variable). These tested (contrast 1) whether all 3 dual-user groups had a higher rate of problematic status compared with all 3 single-user groups, (contrast 2) whether members of the triple-user group had a higher rate of problematic status compared with all 3 dual-user groups, and (contrast 3) whether all single and dual groups involving marijuana had a higher rate of problematic status compared with all single and dual-user groups not involving marijuana.
Identical procedures were used for analyses of 2019 YRBS data and for analyses based on 2017 YRBS data. Although a large number of statistical tests were performed in the analyses, our basic approach was based on testing predictions about the patterning of results. Tests for hypothesized patterns were conducted across 14 different variables. Results were compared across 2 independent studies to determine if the patterning was replicable.
Results
Demographic data indicated that the sample was 49% female; 12% of the participants were 14 years of age, 25% were 15 years, 26% were 16 years, 24% were 17 years, and 14% were 18 years of age. The sample was 5% Asian American, 12% Black non-Hispanic, 52% white non-Hispanic, 9% Hispanic, 17% multiracial Hispanic, and 5% multiracial race non-Hispanic.
Prevalence estimates for the 3 substance use indicators and the 8 substance use groups based on weighted analyses are in Table 2. that the analytic N does not always add to 13 677 because the weighting procedure can upweight or downweight cases.) Prevalence was the highest for e-cigarette use, intermediate for marijuana use, and lowest for cigarette smoking; across indicators, rates were higher for ever use than for recent (30 day) use. For substance ever-use groupings, 44% of the sample had never used any of the 3 substances. The most common user groups were triple users (17%), dual e-cigarette and marijuana users (16%), and exclusive e-cigarette users (13%). For 30-day use the proportions were similar but lower for the triple-user group, a consequence of the relatively low rate of recent smoking. The relative proportions of the variables and groupings were similar in 2017 data (Supplemental Tables 6 and 7.
Table 2.
Prevalence Estimates (Weighted n and Percent) for 2019 YRBS Substance Use Variables and Groupings
| Substance Grouping | Ever Use | Past 30-d Use | ||
|---|---|---|---|---|
| n | % | n | % | |
| Independent categories | ||||
| E-cigarettes | ||||
| No | 6624 | 50 | 8637 | 67 |
| Yes | 6655 | 50 | 4205 | 33 |
| Missing | 472 | — | 910 | — |
| Cigarettes | ||||
| No | 8945 | 76 | 12 329 | 94 |
| Yes | 2833 | 24 | 782 | 6 |
| Missing | 3708 | — | 1360 | |
| Marijuana | ||||
| No | 7931 | 63 | 10 448 | 78 |
| Yes | 4617 | 37 | 2904 | 22 |
| Missing | 2018 | — | 372 | — |
| Combined categories | ||||
| Nonuse | 4934 | 44 | 7677 | 63 |
| Exclusive use | ||||
| E-cigarette | 1487 | 13 | 1750 | 14 |
| Cigarette | 196 | 2 | 49 | <1 |
| Marijuana | 381 | 3 | 512 | 4 |
| Dual use | ||||
| E-cigarette and cigarette | 433 | 4 | 165 | 1 |
| E-cigarette and marijuana | 1778 | 16 | 1572 | 13 |
| Cigarette and marijuana | 33 | 1 | 32 | <1 |
| Use of all 3 substances | 1898 | 17 | 454 | 4 |
| Missing | 4180 | 100 | 2244 | 100 |
Analytic n do not always add to 13 677 because the weighting procedure can upweight or downweight cases. —, not applicable.
Cross-tabulation of substance use groups with demographic variables indicated several significant associations (data not shown). Nonuse was more frequent among younger (14–15 years) age groups, whereas exclusive marijuana use and dual use involving marijuana were more frequent among older (15–18 years) age groups. Several substance user groups were less common among Asian Americans; groups involving marijuana use were more common among Black participants; and dual and triple use involving e-cigarettes was more common among white participants.
Associations With Risk and Protective Factors for Ever-Use Groupings
We compared the pattern of findings on psychosocial risk and protective factors for ever use and 30-day use. Adjusted means and SEs for groupings based on ever use are shown in Table 2. table also reports statistical significance of the F tests for overall variation across groups, which are omnibus tests. These were all significant at P < .0001. Pairwise comparisons (subscripts) indicated that the nonuser group always had the lowest risk profile (ie, lower scores on risk-enhancing factors and higher scores on protective factors) compared with any of the user groups. Other pairwise comparisons (reading across rows) indicated a number of significant differences between the various groups, which were generally consistent with prediction.
Results of the 3 contrasts for ever use are reported as odds ratios in Table 5 (3 left columns). indicate the likelihood of one set of groups being in the high-risk range (eg, >80th percentile on a risk factor variable) compared with another set of groups. these results were consistent with the hypotheses. Results for contrast 1 indicated that, with 1 exception, all dual-user groups had a significantly higher likelihood of problematic status compared with all single-user groups. Results for contrast 2 indicated that, with 1 exception, the triple-user group was significantly higher on likelihood of problematic status, compared with all dual-user groups. Contrast 3, hypothesizing a higher likelihood of problem status for marijuana-using groups, was significant at P < .0001 for 8 of 14 tests. This indicates that marijuana is associated with additional elements of psychosocial risk not contributed by e-cigarettes or cigarettes. Although details of individual analyses differed somewhat, a similar patterning was noted for all 14 psychosocial variables. Considering the composite score (bottom row), dual users were 2.8 times more likely to be in the high-risk range, compared with single users, triple users were 3.1 times more likely to be in that range, compared with dual users, and members of marijuana-using groups were 2.1 times more likely to be in the problem range compared with members of nonmarijuana groups. Figure 1A displays graphically how composite psychosocial risk increased almost monotonically across the groups. We note that the patterning of results was similar in 2017 YRBS data (Supplemental Table 8).
Table 5.
Odds ratios for problem status in three contrasts comparing substance use contrast groups on psychosocial variables, for groupings based on ever use and 30-day use, 2019 YRBS data
| Substance use index/ Type of contrast | ||||||
|---|---|---|---|---|---|---|
| Contrast for ever use | Contrast for 30-day use | |||||
| Psychosocial risk/Protection variable | All singles vs. all duals | All duals vs. triple use | All no marj vs. all marj | All singles vs. all duals | All duals vs. triple use | All no marj vs. all marj |
| Fighting† | 1.98D | 1.98D | 1.76d | 1.52D | 2.86D | 1.56D |
| Weapon carrying | 1.35B | 1.68 | 0.90 | 1.32B | 2.54D | 0.95 |
| Weapon at school | 1.48 | 1.68B | 1.40 | 1.43D | 2.82D | 1.05 |
| Depression | 1.54D | 1.44D | 1.47D | 1.42C | 1.72D | 1.27C |
| Suicide ideation | 1.59D | 1.54C | 1.56C | 1.74D | 1.68D | 1.54D |
| Ever had sex | 2.11D | 2.50D | 2.46D | 2.07D | 2.33C | 1.89D |
| Lifetime partners | 2.53D | 2.34D | 2.33D | 2.01D | 2.33D | 1.85D |
| Ever alcohol use | 1.82D | 0.78C | 1.80D | 1.09 | 0.55D | 1.11 |
| 30-day alcohol use | 3.19D | 2.60D | 2.48C | 2.62D | 3.63D | 1.72D |
| 30-day binge | 2.86D | 2.31D | 2.37D | 2.48D | 2.83D | 1.62D |
| Inhalant use | 1.49A | 2.03D | 0.97 | 1.41B | 3.75D | 1.05 |
| Prescription drugs | 1.50D | 2.61D | 1.28A | 1.94D | 3.02D | 1.52D |
| Grades‡ | 0.75D | 0.75D | 0.75D | 0.67D | 0.67D | 0.67D |
| Seat belt use‡ | 0.76D | 0.76D | 0.76D | 0.72D | 0.72D | 0.72D |
| Composite risk score† | 2.82D | 3.11D | 2.06D | 2.63D | 3.93D | 1.90D |
Note: Problem status is binary variable (lower risk vs. high risk) based on definitions described previously for constructing composite risk score. Marj = marijuana. Note that significance level is influenced by distribution of problem status index
First 12 variables and composite score are risk factors. Odds ratio >1 indicates second contrast group (e.g., dual users, Column 1) is at higher risk for problem status than first contrast group (e.g., single users, Column 1).
These two variables are protective factors. Odds ratio < 1 indicates second contrast group (e.g., dual users) is at higher risk for problem status than first contrast group (e.g., single users).
p < .05;
p < .01;
p < .001;
p < .0001.
FIGURE 1.
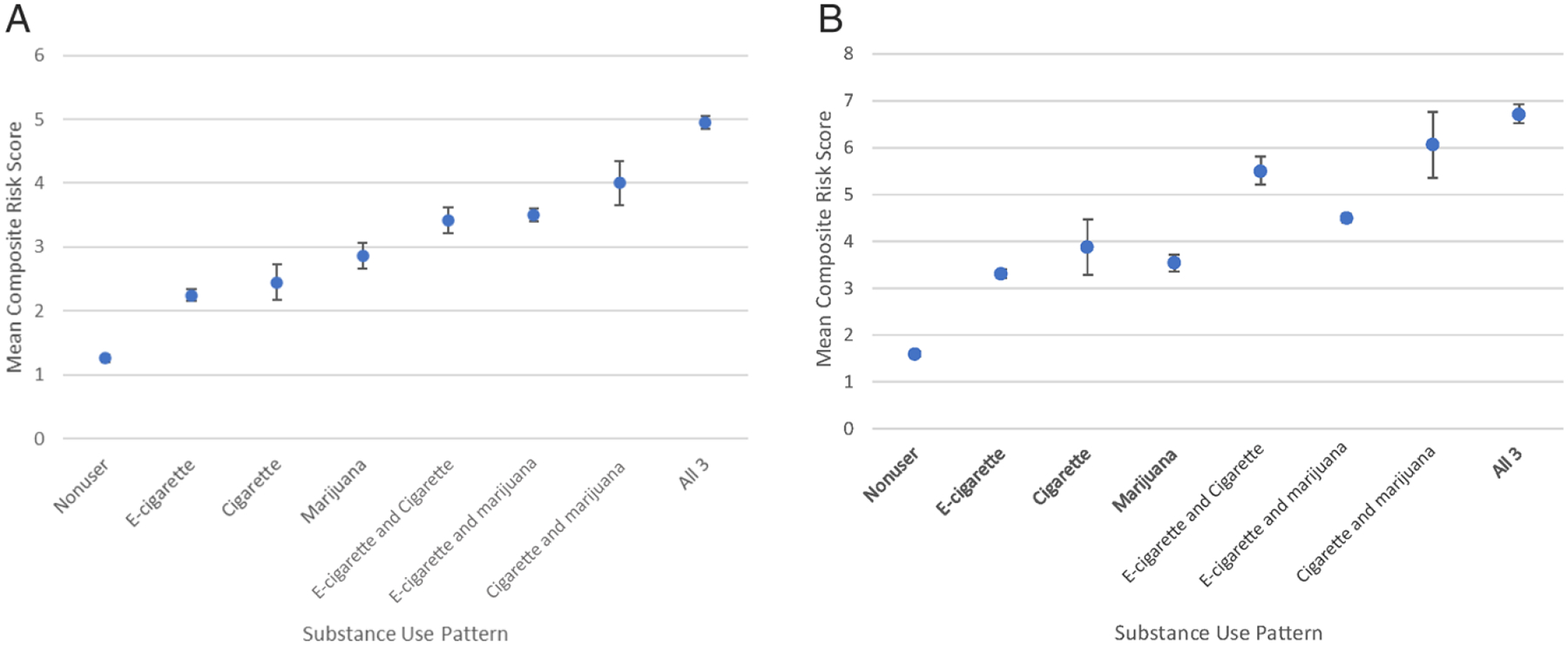
Association of 8 substance use patterns with composite risk score. Barred lines are confidence intervals. A, For ever-use grouping data. B, For 30-day use grouping data.
Some results for individual analyses deserve comment. In most pairwise comparisons, the exclusive e-cigarette user group was significantly lower on the risk profile than the dual e-cigarette and cigarette group. This is consistent with previous research on problem behavior variables15 and psychiatric symptomatology.16 Also, pairwise comparisons of exclusive e-cigarette users and exclusive smokers generally were not significant, although it should be noted that the former group was large relative to the latter group.
Associations With Risk and Protective Factors for Recent-Use Groupings
Results for groupings based on 30-day use (Table 4) were similar to those for ever use despite smaller cell sizes. Contrast 1 indicated dual users had a higher rate of problematic status compared with single users Table 5; 3 right columns), and contrast 2 showed the triple-user group to have a significantly rate of problematic status compared with all dual users. Figure 1B shows a steady increase in risk profile across recent-use groups, although with some variation. Results were similar across variables, and the patterning of results was almost exactly replicated in 2017 YRBS data (Supplemental Table).
TABLE 4.
Adjusted Mean (SE) on Psychosocial Variables and Composite Risk Score by Past 30-d Substance Use Pattern, with P for Omnibus F Test and Pairwise Comparisons: 2019 YRBS Data
| AQ15 | Pattern for 30 d Use of Substances | P for Omnibus F Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No Use (Analytic Na = 5382), Mean (SE) | Exclusive Use | Dual Use | Triple Use: E-cigarette, Cigarette, and Marijuana (Analytic Na = 309), Mean (SE) | ||||||
| E-cigarette (Analytic Na = 1425), Mean (SE) | Cigarette (Analytic Na = 38), Mean (SE) | Marijuana (Analytic Na = 456), Mean (SE) | E-cigarette and Cigarette (Analytic Na = 142), Mean (SE) | E-cigarette and Marijuana (Analytic Na = 1241), Mean (SE) | Cigarette and Marijuana (Analytic Na = 27), Mean (SE) | ||||
| Aggressive behavior | |||||||||
| 12 mo fighting (1–8) | 1.24a (0.01) | 1.51b (0.03) | 1.30ab (0.17) | 1.70c (0.05) | 1.79c (0.09) | 1.69c (0.03) | 2.65d (0.18) | 2.51d (0.06) | <.0001 |
| 30 d carry weapon (1–5) | 1.22 (0.01) | 1.42a (0.03) | 1.53a (0.16) | 1.43a (0.05) | 2.14b (0.09) | 1.46a (0.03) | 2.17bc (0.19) | 2.05bc (0.06) | <.0001 |
| 30 d weapon school (1–5) | 1.03 (0.01) | 1.05 (0.01) | 1.21a (0.07) | 1.12ab (0.02) | 1.31c (0.03) | 1.08b (0.01) | 1.51c (0.08) | 1.17a (0.02) | <.0001 |
| Psychiatric symptoms | |||||||||
| 12 mo depressed (1,2) | 1.30 (0.01) | 1.42a (0.01) | 1.53b (0.07) | 1.43a (0.02) | 1.54c (0.04) | 1.49c (0.01) | 1.74c (0.09) | 1.62b (0.02) | <.0001 |
| 12 mo suicide ideation (1,2) | 1.14 (0.01) | 1.20 (0.01) | 1.37a (0.06) | 1.24 (0.02) | 1.38ab (0.03) | 1.30a (0.01) | 1.52b (0.07) | 1.42ab (0.02) | <.0001 |
| Sexual risk behavior | |||||||||
| Ever had sex (1,2) | 1.23 (0.01) | 1.49a (0.01) | 1.54ab (0.07) | 1.58b (0.02) | 1.71c (0.04) | 1.67bc (0.01) | 1.74cd (0.08) | 1.81d (0.02) | <.0001 |
| Lifetime partners (1–7) | 1.44 (0.02) | 2.10 (0.04) | 2.53a (0.22) | 2.56a (0.06) | 3.12b (0.14) | 2.73 (0.04) | 3.39b (0.25) | 3.88 (0.07) | <.0001 |
| Alcohol use | |||||||||
| Lifetime alcohol use (1–7) | 2.48 (0.02) | 4.44a (0.05) | 3.80 (0.30) | 4.28b (0.09) | 4.37ab (0.15) | 4.57b (0.05) | 4.45b (0.35) | 4.20ab (0.10) | <.0001 |
| 30 d alcohol use (1–7) | 1.14 (0.01) | 1.80a (0.02) | 1.94a (0.13) | 1.66 (0.04) | 2.83 (0.07) | 2.30b (0.02) | 2.45b (0.15) | 3.52 (0.04) | <.0001 |
| 30 d binge (1–7) | 1.06 (0.01) | 1.45a (0.02) | 1.41ab (0.13) | 1.34b (0.04) | 2.46 (0.07) | 1.90c (0.02) | 2.03c (0.16) | 3.18 (0.05) | <.0001 |
| Illicit drug use | |||||||||
| Inhalant use (1–6) | 1.05 (0.01) | 1.12a (0.01) | 1.20a (0.08) | 1.11a (0.02) | 1.31b (0.04) | 1.16b (0.01) | 1.19ab (0.09) | 1.62 (0.03) | <.0001 |
| Prescriptio drug use (1–6) | 1.16a n(0.01) | 1.27b (0.02) | 1.31ab (0.13) | 1.33b (0.04) | 1.81c (0.07) | 1.46 (0.02) | 1.80c (0.15) | 2.28 (0.05) | <.0001 |
| Protective factors | |||||||||
| Grades (1F–5A) | 4.28 (0.01) | 4.12 (0.02) | 3.82a (0.14) | 4.05 (0.04) | 3.73ab (0.07) | 3.93a (0.02) | 3.62bc (0.15) | 3.43c (0.05) | <.0001 |
| Seat belt in car (1–5) | 4.51 (0.01) | 4.25a (0.02) | 4.04ab (0.15) | 4.21a (0.04) | 3.73bc (0.08) | 4.12c (0.03) | 3.71c (0.17) | 3.61c (0.05) | <.0001 |
| Composite risk score (0–14)b | 1.59 (0.02) | 3.30 (0.05) | 3.87a (0.30) | 3.54a (0.09) | 5.51b (0.15) | 4.49 (0.05) | 6.06b (0.35) | 6.72 (0.10) | <.0001 |
Adjusted for age, sex, and race and ethnicity. In pairwise comparisons (across row), cells with common superscript do not differ significantly (at P < .05).
For given group, tabled n represents approximate midpoint from range of analytic n over all variables.
Composite risk score is based on 14 binary (0,1) indices, reflecting lower-risk versus high-risk status for each row variable in table.
Results for the contrast of no marijuana versus marijuana recent-use groupings (Table 5, right column) were generally similar to those for ever use. In many comparisons, members of groups with marijuana had a higher likelihood of problematic status than groups that did not involve marijuana. This contrast also was typically significant in 2017 YRBS data (Supplemental Table 10).
Discussion
The aim of this research was to determine the prevalence for various groupings of co-occurring e-cigarette, cigarette, and marijuana use in 2019 YRBS data and study their associations with a range of risk and protective factors. The most prevalent groups were triple users, dual (e-cigarette and marijuana) users, and exclusive e-cigarette users. The patterning of correlates for the 8 groups on established risk factors was replicated across a number of variables and across 2 independent studies, supporting construct validity of the groupings, and similar patterns of findings for ever use and recent use indicate that the results are not attributable simply to level of consumption. These findings paint a somewhat different picture than grouping data from previous years.15,16 It is clear that at present, dual use of e-cigarettes and marijuana is one of the 3 most common patterns of (poly) use and that triple use is actually the most prevalent type. To our knowledge, this is the first article to report such data, although Strong et al23 examined different groups of tobacco product users and the additive risk effect of marijuana use.
Our predictions about variation in psychosocial variables across groups were generally supported, the pattern of results being consistent across numerous variables and 2 independent studies. Exclusive e-cigarette users were significantly elevated above nonusers but typically were significantly lower on risk profile relative to the dual-user groups. Consistent with previous studies,15,16,43–46 indicates that e-cigarettes may appeal to adolescents who are relatively low on psychosocial risk and otherwise would be unlikely to use cigarettes or marijuana initially. E-cigarette use gives lower-risk adolescents a chance to practice behaviors key to both cigarette smoking and marijuana use and also exposes them to the addictive properties of nicotine. Hence, initial e-cigarette use may be an important pathway to dual and triple substance use.9–13,47
We found that all types of dual users were elevated on their risk profiles relative to exclusive users of any type. This pattern has been found before for e-cigarettes and smoking, suggesting high public health significance of the additive effects.14–16 The present research extends this through identifying several dual-user groups and demonstrating the effect of marijuana on risk profile. What is most noteworthy is that the triple-user group (e-cigarettes, cigarettes, and marijuana) is prevalent and has the most extreme psychosocial risk profile. This observation of a triple-use group calls for further research to trace the pathway(s) from single use to dual and triple use. Triple-use data may also be useful for screening purposes because 3 simple survey questions can be used to demarcate a particularly high-risk group.
The prediction that groups involving marijuana would be higher on risk profile received considerable support. Results for this contrast were consistently significant in 2019 YRBS data and also in 2017 YRBS data. Pairwise comparisons actually indicated that the dual (e-cigarette and cigarette) group was comparable to or higher on risk factors than the dual (e-cigarette and marijuana) group, but the latter group was large relative to the former one, suggesting that it was a more normative pattern of use. This needs to be explicated in further research.
Some aspects of the present research may present limitations. First, the data were cross-sectional, and temporal relations between variables are not demonstrated. We recognize that some of the variables in Tables 3 and 4 typically occur together, and we do not mean to imply that one domain constitutes a risk for another domain. Rather, the aim was to demonstrate that different subgroups of e-cigarette, cigarette, and marijuana users have different (predicted) patterns of association with recognized measures of adolescent risk behavior. Third, the YRBS has ample data on risk factors but relatively few measures of protective factors; however, the patterning of results for protective-factor measures was consistent with prediction. Finally, the item on marijuana simply asked how many times you have used marijuana but did not ask whether the marijuana was smoked or used in an e-cigarette device.21,44 Further research could use more detailed measures and study the behavioral correlates of different subgroups.
TABLE 3.
Adjusted Mean (SE) on Psychosocial Variables and Composite Risk Score by Ever Substance Use Pattern, With Omnibus F Test and Pairwise Comparisons: 2019 YRBS Data
Composite risk score (0–14)b
| Pattern for Ever Use of Substances | P for Omnibus F Test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No Use (Analytic Na = 3819), Mean (SE) | Exclusive Use | Dual Use | Triple Use: E-cigarette, Cigarette, and Marijuana (Analytic Na = 1383), Mean (SE) | ||||||
| E-cigarette (Analytic Na = 1119), Mean (SE) | Cigarette (Analytic Na = 151), Mean (SE) | Marijuana (Analytic Na = 347), Mean (SE) | E-cigarette and Cigarette (Analytic Na = 326), Mean (SE) | E-cigarette and Marijuana (Analytic Na = 1365), Mean (SE) | Cigarette and Marijuana (Analytic Na = 102), Mean (SE) | ||||
| Aggressive behavior | |||||||||
| 12 mo fighting (1–8) | 1.18 (0.02) | 1.32a (0.03) | 1.39ab (0.08) | 1.46bc (0.05) | 1.61d (0.05) | 1.54cd (0.03) | 2.25 (0.10) | 1.91 (0.03) | <.0001 |
| 30 d carry weapon (1–5) | 1.19 (0.02) | 1.32a (0.03) | 1.36ab (0.08) | 1.36ab (0.06) | 1.74c (0.05) | 1.35ab (0.03) | 1.57cd (0.10) | 1.67d (0.03) | <.0001 |
| 30 d weapon school (1–5) | 1.02a (0.01) | 1.04ab (0.01) | 1.06bc (0.04) | 1.10d (0.02) | 1.09d (0.02) | 1.07cd (0.01) | 1.10bcd (0.04) | 1.12d (0.01) | <.0001 |
| Psychiatric symptoms | |||||||||
| 12 mo depressed (1,2) | 1.27 (0.01) | 1.35a (0.01) | 1.39ab (0.04) | 1.44bc (0.02) | 1.47cd (0.02) | 1.46c (0.01) | 1.58d (0.04) | 1.55d (0.01) | <.0001 |
| 12 mo suicide ideation (1,2) | 1.12 (0.01) | 1.16 (0.01) | 1.23a (0.03) | 1.23ab (0.02) | 1.24a (0.02) | 1.25a (0.01) | 1.34c (0.04) | 1.33c (0.01) | <.0001 |
| Sexual risk behavior | |||||||||
| Ever had sex (1,2) | 1.17 (0.01) | 1.32a (0.01) | 1.29a (0.03) | 1.55b (0.02) | 1.46 (0.02) | 1.56bc (0.01) | 1.56bc (0.04) | 1.73 (0.01) | <.0001 |
| Lifetime partners (1–7) | 1.32 (0.02) | 1.59a (0.04) | 1.57a (0.11) | 2.17b (0.07) | 2.07b (0.08) | 2.29 (0.04) | 2.64 (0.13) | 3.11 (0.04) | <.0001 |
| Alcohol use | |||||||||
| Lifetime alcohol use (1–7) | 2.04 (0.03) | 3.82a (0.05) | 3.39 (0.15) | 3.79a (0.10) | 4.06b (0.10) | 4.60 (0.05) | 4.21bc (0.18) | 4.42c (0.05) | <.0001 |
| 30 d alcohol use (1–7) | 1.09 (0.01) | 1.39a (0.03) | 1.28 (0.07) | 1.41a (0.05) | 1.66b (0.05) | 1.85 (0.02) | 1.53ab (0.09) | 2.43 (0.02) | <.0001 |
| 30 d binge (1–7) | 1.04a (0.01) | 1.16b (0.02) | 1.13ab (0.07) | 1.17b (0.04) | 1.30c (0.05) | 1.50 (0.02) | 1.20bc (0.08) | 2.05 (0.02) | <.0001 |
| Illicit drug use | |||||||||
| Inhalant use (1–6) | 1.03 (0.01) | 1.08a (0.01) | 1.15b (0.04) | 1.08ab (0.03) | 1.23c (0.03) | 1.12b (0.01) | 1.12ab (0.05) | 1.27c (0.01) | <.0001 |
| Prescriptio drug use (1–6) | 1.13 n(0.01) | 1.17 (0.02) | 1.35a (0.06) | 1.26ab (0.04) | 1.30ab (0.04) | 1.25b (0.02) | 1.51 (0.08) | 1.69 (0.02) | <.0001 |
| Protective factors | |||||||||
| Grades (1F–5A) | 4.32 (0.01) | 4.22a (0.02) | 4.04ab (0.07) | 4.14ab (0.05) | 3.99b (0.05) | 4.08b (0.02) | 3.93b (0.08) | 3.73 (0.02) | <.0001 |
| Seat belt in car (1–5) | 4.56 (0.01) | 4.38a (0.03) | 4.28ab (0.07) | 4.35a (0.05) | 4.05c (0.05) | 4.31ab (0.02) | 4.06cd (0.09) | 3.93d (0.02) | <.0001 |
| 1.26 (0.03) | 2.25a (0.05) | 2.45a (0.14) | 2.86 (0.10) | 3.42b (0.10) | 3.50b (0.05) | 4.00 (0.17) | 4.95 (0.05) | <.0001 | |
Adjusted for age, sex, and race and ethnicity. In pairwise comparisons (across row), cells with common superscript do not differ significantly (at P < .05).
For given group, tabled n represents approximate midpoint from range of analytic n over all variables.
Composite risk score is based on 14 binary (0,1) indices, reflecting lower-risk versus high-risk status for each row variable in table.
Conclusions
The present research provides a novel comprehensive psychosocial profile of current patterns of adolescent substance use and demonstrates the existence of a particularly high-risk group, triple users. We confirmed previous findings that e-cigarettes differentially appeal to lower-risk adolescents who otherwise would be less likely to use cigarettes or marijuana; this suggests that e-cigarettes are an important part of the pathways from never use to dual and triple use. These replicated results provide suggestions for further research on the social and health implications of e-cigarettes and indicate a need for more research on prevention approaches for dual and triple users because additive effects place them at greater risk for adverse health consequences.14,48,49
Supplementary Material
What’s Known on This Subject:
It is known that there are subgroups of adolescents using e-cigarettes or cigarettes and that exclusive e-cigarette users are at lower risk than dual users. However, these groupings have not included marijuana use, which has recently increased in prevalence.
What This Study Adds:
We found sizable subgroups of adolescents who combine e-cigarettes with marijuana. E-cigarette and marijuana users are at greater psychosocial risk than exclusive users of any substance, and triple users have a particularly elevated risk profile compared with all dual-user groups.
FUNDING:
Supported in part by grant P30 CA071789 from the National Cancer Institute, a Tobacco Centers of Regulatory Science award from the National Cancer Institute and the Food and Drug Administration (U54CA180908), and a grant from the National Institute on Drug Abuse (K24DA048160). The funders had no role in design of the research, analysis and interpretation of the data, drafting and revision of the article, and decision to submit the report for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute, National Institute on Drug Abuse, or Food and Drug Administration. Funded by the National Institutes of Health (NIH).
Abbreviations
- CDC
Centers for Disease Control and Prevention
- YRBS
Youth Risk Behavior Survey
Footnotes
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
References
- 1.Miech R, Johnston L, O’Malley PM, Bachman JG, Patrick ME. Trends in adolescent vaping, 2017–2019. N Engl J Med. 2019;381(15):1490–1491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cullen KA, Gentzke AS, Sawdey MD, et al. E-cigarette use among youth in the United States, 2019. JAMA. 2019;322(21):2095–2103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Miech R, Johnston L, O’Malley PM, Bachman JG, Patrick ME. Adolescent vaping and nicotine use in 2017–2018—U.S. national estimates. N Engl J Med. 2019;380(2):192–193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Thorndike AN. E-cigarette use by young adult nonsmokers: next-generation nicotine dependence? Ann Intern Med. 2019;170(1):70–71 [DOI] [PubMed] [Google Scholar]
- 5.Vogel EA, Cho J, McConnell RS, Barrington-Trimis JL, Leventhal AM. Prevalence of electronic cigarette dependence among youth and its association with future use. JAMA Netw Open. 2020;3(2):e1921513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chaffee BW, Watkins SL, Glantz SA. Electronic cigarette use and transition from experimentation to established smoking. Pediatrics. 2018;141(4):e20173594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Osibogun O, Bursac Z, Maziak W. E-cigarette use and regular cigarette smoking among youth: Population Assessment of Tobacco and Health (PATH) Study (2013–2016). Am J Prev Med. 2020;58(5):657–665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pierce JP, Chen R, Leas EC, et al. Use of e-cigarettes and other tobacco products and progression to daily cigarette smoking. Pediatrics. 2021;147(2):e2020025122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Khouja JA, Suddell SF, Peters SE, et al. Is e-cigarette use in nonsmoking young adults associated with later smoking? A systematic review and meta-analysis. Tob Control. 2021;30:8–315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Unger JB, Soto DW, Leventhal A. E-cigarette use and subsequent cigarette and marijuana use among Hispanic young adults. Drug Alcohol Depend. 2016;163:261–264 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wills TA, Gibbons FX, Sargent JD, Schweitzer RJ. How is the effect of adolescent e-cigarette use on smoking onset mediated: A longitudinal analysis. Psychol Addict Behav. 2016;30(8):876–886 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dai H, Catley D, Richter KP, Goggin K, Ellerbeck EF. Electronic cigarettes and future marijuana use: a longitudinal study. Pediatrics. 2018;141(5):e20173787. [DOI] [PubMed] [Google Scholar]
- 13.Audrain-McGovern J, Stone MD, Barrington-Trimis J, Unger JB, Leventhal AM. Adolescent e-cigarette, hookah, and conventional cigarette use and subsequent marijuana use. Pediatrics. 2018;142(3):e20173616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wills TA, Soneji SS, Choi K, Jaspers I, Tam EK. E-cigarette use and respiratory disorders: an integrative review of converging evidence from epidemiological and laboratory studies. Eur Respir J. 2021;57(1):19011815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wills TA, Knight R, Williams RJ, Pagano I, Sargent JD. Risk factors for exclusive e-cigarette use and dual e-cigarette use and tobacco use in adolescents. Pediatrics. 2015;135(1):e43–e51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leventhal AM, Strong DR, Sussman S, et al. Psychiatric comorbidity in adolescent electronic and conventional cigarette use. J Psychiatr Res. 2016;73:71–78 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Demissie Z, Everett Jones S, Clayton HB, King BA. Adolescent risk behaviors and use of electronic vapor products and cigarettes. Pediatrics. 2017;139(2):e20162921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kristjansson AL, Mann MJ, Sigfusdottir ID. Licit and illicit substance use by adolescent e-cigarette users compared with conventional cigarette smokers, dual users, and nonusers. J Adolesc Health. 2015;57(5):562–564 [DOI] [PubMed] [Google Scholar]
- 19.Kristjansson AL, Mann MJ, Smith ML, Sigfusdottir ID. Social profile of adolescents who use electronic cigarettes. Prev Sci. 2018;19:805–812 [DOI] [PubMed] [Google Scholar]
- 20.McCabe SE, West BT, Veliz P, Boyd CJ. E-cigarette use, cigarette smoking, dual use, and problem behaviors among US adolescents: results from a national survey. J Adolesc Health. 2017;61(2):155–162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Miech RA, Patrick ME, O’Malley PM, Johnston LD, Bachman JG. Trends in reported marijuana vaping among US adolescents, 2017–2019. JAMA. 2020;323(5):475–476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future National Survey Results on Drug Use, 1975–2019. Secondary School Students. Vol I. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2020 [Google Scholar]
- 23.Strong DR, Myers MG, Pulvers K, et al. Marijuana use among US tobacco users: findings from wave 1 of the PATH study. Drug Alcohol Depend. 2018;186:16–22 [DOI] [PubMed] [Google Scholar]
- 24.Schauer GL, Clayton HB, Njai R, Grant AM. Adolescent marijuana use and related risk behavior, national findings from 2015 to 2017. Am J Prev Med. 2020;59(5):714–724 [DOI] [PubMed] [Google Scholar]
- 25.Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992;112(1):64–105 [DOI] [PubMed] [Google Scholar]
- 26.Petraitis J, Flay BR, Miller TQ. Reviewing theories of adolescent substance use: organizing pieces in the puzzle. Psychol Bull. 1995;117(1):67–86 [DOI] [PubMed] [Google Scholar]
- 27.Stone AL, Becker LG, Huber AM, Catalano RF. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict Behav. 2012;37(7):747–775 [DOI] [PubMed] [Google Scholar]
- 28.Bogg T, Roberts BW. Conscientiousness and health-related behaviors: a meta-analysis of the leading behavioral contributors to mortality. Psychol Bull. 2004;130(6):887–919 [DOI] [PubMed] [Google Scholar]
- 29.Martin LR, Friedman HS, Schwartz JE. Personality and mortality risk across the life span: the importance of conscientiousness as a biopsychosocial attribute. Health Psychol. 2007;26(4):428–436 [DOI] [PubMed] [Google Scholar]
- 30.Winters DE, Brandon-Friedman R, Yepes G, Hinckley JD. Systematic review and meta-analysis of socio-cognitive and socio-affective processes association with adolescent substance use. Drug Alcohol Depend. 2021;219:108479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kandel DB, ed. Stages and Pathways of Drug Involvement: Examining the Gateway Hypothesis. Cambridge, UK: Cambridge University Press; 2002 [Google Scholar]
- 32.Kandel DB. Does marijuana use cause the use of other drugs? JAMA. 2003;289(4):482–483 [DOI] [PubMed] [Google Scholar]
- 33.Scheier LM, Griffin KW. Youth marijuana use: a review of causes and consequences. Curr Opin Psychol. 2021;38:11–18 [DOI] [PubMed] [Google Scholar]
- 34.Bry BH, McKeon P, Pandina RJ. Extent of drug use as a function of number of risk factors. J Abnorm Psychol. 1982;91(4):273–279 [DOI] [PubMed] [Google Scholar]
- 35.Newcomb MD, Maddahian E, Bentler PM. Risk factors for drug use among adolescents: concurrent and longitudinal analyses. Am J Public Health. 1986;76(5):525–531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ostaszewski K, Zimmerman MA. The effects of cumulative risks and promotive factors on urban adolescent alcohol and other drug use: a longitudinal study of resiliency. Am J Community Psychol. 2006;38(3–4):237–249 [DOI] [PubMed] [Google Scholar]
- 37.Arthur MW, Briney JS, Hawkins JD, Abbott RD, Brooke-Weiss BL, Catalano RF. Measuring risk and protection in communities using the communities that care youth survey. Eval Program Plann. 2007;30(2):197–211 [DOI] [PubMed] [Google Scholar]
- 38.Evans GW, Li D, Whipple SS. Cumulative risk and child development. Psychol Bull. 2013;139(6):1342–1396 [DOI] [PubMed] [Google Scholar]
- 39.Underwood JM, Brener N, Thornton J, et al. Overview and methods for the Youth Risk Behavior Surveillance System - United States, 2019. MMWR Suppl. 2020;69(1, SS-01):1–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Brener ND, Kann L, McManus T, Kinchen SA, Sundberg EC, Ross JG. Reliability of the 1999 youth risk behavior survey questionnaire. J Adolesc Health. 2002;31(4):336–342 [DOI] [PubMed] [Google Scholar]
- 41.Brener ND, Billy JOG, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health. 2003;33(6):436–457 [DOI] [PubMed] [Google Scholar]
- 42.Brener ND, Grunbaum JA, Kann L, McManus T, Ross J. Assessing health risk behaviors among adolescents: the effect of question wording and appeals for honesty. J Adolesc Health. 2004;35(2):91–100 [DOI] [PubMed] [Google Scholar]
- 43.Brener ND, Eaton DK, Kann L, et al. The association of survey setting and mode with self reported health risk behaviors among high school students. Public Opin Q. 2006;70:354–374 [Google Scholar]
- 44.Barrington-Trimis JL, Urman R, Berhane K, et al. E-cigarettes and future cigarette use. Pediatrics. 2016;138(1):e20160379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wills TA, Sargent JD, Gibbons FX, Pagano I, Schweitzer R. E-cigarette use is differentially related to smoking onset among lower risk adolescents. Tob Control. 2016;26(5):534–539 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Best C, Haseen F, Currie D, et al. Relation between trying an electronic cigarette and subsequent cigarette experimentation among Scottish adolescents: a cohort study. Tob Control. 2018;27:373–378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chapman S, Bareham D, Maziak W. The gateway effect of e-cigarettes: reflections on main criticisms. Nicotine Tob Res. 2019;21(5):695–698 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Eissenberg T, Maziak W. Are electronic cigarette users at risk for lipid-mediated lung injury? Am J Respir Crit Care Med. 2020;201(8):1012–1013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Braymiller JL, Barrington-Trimis JL, Leventhal AM, et al. Assessment of nicotine and cannabis vaping and respiratory symptoms in young adults. JAMA Netw Open. 2020;3(12):e2030189. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.