

Abstract
The authors argue that postacute SARS-CoV-2 syndrome presents unique challenges in determining risk factors, natural history, and proper management. They call for strategies and actions that are based on rigorous, high-quality evidence.
Early reporting of postacute SARS-CoV-2 syndrome (PASC), or “long COVID” (1), foretells a difficult challenge developing in parallel to the ongoing pandemic. Some patients with prior acute COVID-19 report multiple new or persistent symptoms affecting nearly every organ system (2). In the United States, PASC has already been approved for inclusion and protections within the Americans with Disabilities Act (3) despite limited study data or medical consensus. Yet, we do not know what constitutes long COVID or how to formally diagnose it (4). An improved understanding of this condition is needed to provide appropriate care for our patients. However, developing high-quality scientific evidence on PASC presents a unique challenge due to the evolving circumstances of SARS-CoV-2 and the pandemic itself. Such work will indeed be a long haul.
Inherent sources of potential bias in studying this new phenomenon require that the medical community understand both study design and study limitations when generating, publishing, and using reports (Table). Deriving high-quality, consistent information from diverse study designs and samples is our best hope to inform the understanding of PASC and develop strategies to diagnose, treat, and prevent it. No single study design will be perfectly suited to study PASC, but we must work together to develop and disseminate the highest-quality information.
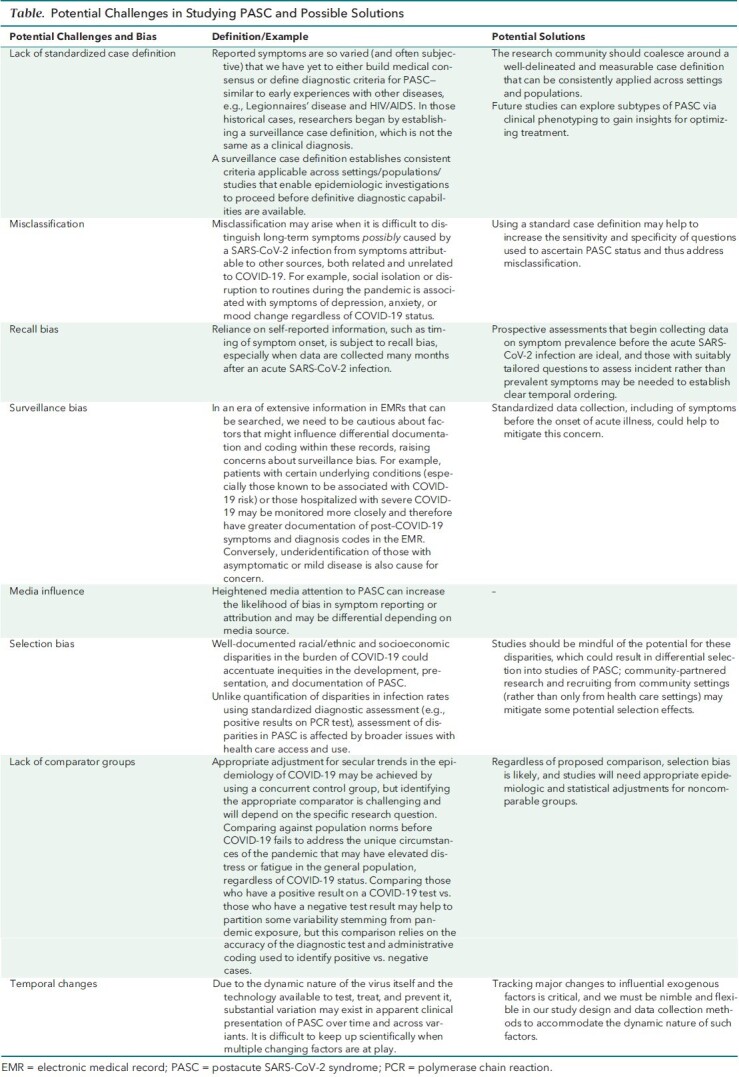
Table.
Potential Challenges in Studying PASC and Possible Solutions
The first challenge when studying a disease is how to diagnose it. Despite the widely reported burden of sequelae stemming from COVID-19, we have yet to derive definitive diagnostic criteria. The World Health Organization proposed a clinical case definition based on the deliberations of a Delphi panel of patients and clinicians (5). However, such definitions do not represent a definitive clinical diagnosis, and the authors acknowledge that their definition may need to evolve as new evidence emerges. As more high-quality data become available, the current list of symptoms may be narrowed and the relationship between the timing and duration of symptoms included in a PASC case definition may be clarified; to date, however, these aspects have proved elusive.
Accurate diagnoses are important so that patients with PASC can receive monitoring, supportive care, and eventually PASC-specific therapy. The Americans with Disabilities Act action makes this particularly important because of medical and legal paperwork requiring detailed diagnosis and treatment plans in the disability filing. Misclassification due to inadequate research data will complicate matters if we remain unable to distinguish between long-term symptoms possibly associated with SARS-CoV-2 infection and symptoms associated with other diagnoses. For example, social isolation and disruption to routines during the pandemic are associated with symptoms of depression, anxiety, or mood change regardless of COVID-19 status (6). Similarly, it is difficult to differentiate between PASC and post–intensive care syndrome, the latter reported among patients who have required care for critical illness (7).
The observation that persistent PASC symptoms may align more closely with self-perceived rather than laboratory-confirmed SARS-CoV-2 infection (8) suggests that thorough evaluation is needed to properly assess whether symptoms are directly related to the virus. Such comprehensive assessments are time-consuming, are expensive, and are not routinely documented in medical records, which precludes study of PASC using large, existing electronic medical records or administrative data. To date, multiple investigations are under way without uniformly applied criterion standards, limiting our ability to conduct useful comparisons across studies.
Researchers must also grapple with issues of bias in study design, such as recall bias and surveillance bias, where attention to COVID-19 (including variants and vaccinations) may shape what patients report or clinicians document. Heightened lay attention may affect the likelihood that patients report certain symptoms or the degree to which they recall symptom onset or duration. As well, patients with certain underlying conditions known to be associated with COVID-19 risk or those hospitalized with severe COVID-19 may be monitored more closely than others, with greater documentation of post–COVID-19 symptoms in electronic medical records. Conversely, underidentification of those with asymptomatic or mild disease is a concern. Due to the dynamic nature of the virus itself and the technology available to test, monitor, and treat infection, substantial variation may exist in apparent clinical presentation of PASC. Now more than ever, we must implement robust, standardized, longitudinal assessments of health and well-being across systems and settings, including premorbid evaluation, to facilitate real-time monitoring of trends.
Of note, the burden of the COVID-19 pandemic, including infection, reinfection, hospitalization, and death, has disproportionately fallen on individuals who are already vulnerable to socioeconomic and racial/ethnic disparities in access to health care and in health (9). In the presence of these disparities, inequities in the development, presentation, and documentation of PASC may be accentuated. Unlike quantification of disparities in infection rates using standardized diagnostic assessment (such as positive results on a polymerase chain reaction test), assessment of disparities in PASC is affected by broader issues with health care access and use. For example, the evolving PASC case definition will be influenced by the symptom profiles of those currently seen in clinics or participating in studies. Because marginalized groups receive less timely diagnoses and often have their symptoms unrecognized or undocumented, PASC may be underdescribed in those who are already vulnerable.
Equity in access to accurate diagnostic testing and symptom documentation in the clinical record is a necessary first step for equal ascertainment of PASC across groups with different degrees of vulnerability; we must further consider differences in the availability of appropriate comparator groups that could obfuscate our assessment of PASC risk. Simply following a cohort of patients who had COVID-19 and ascertaining symptoms (such as fatigue) at 3 months after diagnosis fails to account for baseline levels of these symptoms in the general population. Comparing long-term symptoms after SARS-CoV-2 versus influenza infection may help to partition out selection effects caused by disparities in access to diagnostic testing and could simultaneously address elevated symptom rates versus background rates.
Thus, we call for the medical community to take the following actions: 1) coalesce around a well-delineated and measurable PASC case definition that can be consistently applied, 2) implement similarly robust and standardized measures of potential risk factors and outcomes, 3) consider risk of bias in study designs and provide thorough descriptions of ascertainment methodology and assessment tools to facilitate cross-study comparison of published reports, and 4) be judicious in application of this evolving evidence as we all strive to provide effective and efficient care that reduces prior inequities. By recognizing these data challenges and potential study biases early, the research community can ensure that our understanding of PASC, as well as future strategies and actions to address it, is based on high-quality evidence. We are armed with the tools and talent to provide rigorous evidence to aid understanding of this novel illness; however, we must be aware of the unique challenges we face and be prepared to address them.
Footnotes
This article was published at Annals.org on 8 March 2022.
References
- 1. Phillips S , Williams MA . Confronting our next national health disaster — long-haul Covid. N Engl J Med. 2021;385:577-579. [PMID: ] doi: 10.1056/NEJMp2109285 [DOI] [PubMed] [Google Scholar]
- 2. Parker AM , Brigham E , Connolly B , et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: a multidisciplinary model of care. Lancet Respir Med. 2021;9:1328-1341. [PMID: ] doi: 10.1016/S2213-2600(21)00385-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.The Americans with Disabilities Act at 31. HHS Blog. 26 July 2021. Accessed at www.hhs.gov/blog/2021/07/26/the-americans-with-disabilities-act-at-31.html on 20 August 2021.
- 4. National Center for Immunization and Respiratory Diseases. Evaluating and caring for patients with post-COVID conditions: interim guidance. Centers for Disease Control and Prevention. Updated 14 June 2021. Accessed at www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-index.html on 31 January 2022.
- 5. Soriano JB, Allan M, Alsokhn C, et al; World Health Organization clinical case definition working group on post COVID-19 condition. A clinical case definition of post COVID-19 condition by a Delphi consensus. World Health Organization; 2021.
- 6. Varga TV , Bu F , Dissing AS , et al. Loneliness, worries, anxiety, and precautionary behaviours in response to the COVID-19 pandemic: a longitudinal analysis of 200,000 Western and Northern Europeans. Lancet Reg Health Eur. 2021;2:100020. [PMID: ] doi: 10.1016/j.lanepe.2020.100020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bangash MN , Owen A , Alderman JE , et al. COVID-19 recovery: potential treatments for post-intensive care syndrome. Lancet Respir Med. 2020;8:1071-1073. [PMID: ] doi: 10.1016/S2213-2600(20)30457-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Matta J , Wiernik E , Robineau O , et al; Santé, Pratiques, Relations et Inégalités Sociales en Population Générale Pendant la Crise COVID-19-Sérologie (SAPRIS-SERO) Study Group. Association of self-reported COVID-19 infection and SARS-CoV-2 serology test results with persistent physical symptoms among French adults during the COVID-19 pandemic. JAMA Intern Med. 2022;182:19-25. [PMID: ] doi: 10.1001/jamainternmed.2021.6454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Webb Hooper M, Nápoles AM, Pérez-Stable EJ.. COVID-19 and racial/ethnic disparities. JAMA. 2020;323:2466-2467. [PMID: ] doi: 10.1001/jama.2020.8598 [DOI] [PMC free article] [PubMed] [Google Scholar]