

Abstract
Background
The Covid-19 pandemic and its accompanying public-health orders (PHOs) have led to (potentially countervailing) changes in various risk factors for overdose. To assess whether the net effects of these factors varied geographically, we examined regional variation in the impact of the PHOs on counts of nonfatal overdoses, which have received less attention than fatal overdoses, despite their public health significance.
Methods
Data were collected from the Overdose Detection Mapping Application Program (ODMAP), which recorded suspected overdoses between July 1, 2018 and October 25, 2020. We used segmented regression models to assess the impact of PHOs on nonfatal-overdose trends in Washington DC and the five geographical regions of Maryland, using a historical control time series to adjust for normative changes in overdoses that occurred around mid-March (when the PHOs were issued).
Results
The mean level change in nonfatal opioid overdoses immediately after mid-March was not reliably different in the Covid-19 year versus the preceding control time series for any region. However, the rate of increase in nonfatal overdose was steeper after mid-March in the Covid-19 year versus the preceding year for Maryland as a whole (B = 2.36; 95% CI, 0.65 to 4.06; p = .007) and for certain subregions. No differences were observed for Washington DC.
Conclusions
The pandemic and its accompanying PHOs were associated with steeper increases in nonfatal opioid overdoses in most but not all of the regions we assessed, with a net effect that was deleterious for the Maryland region as a whole.
Introduction
In January 2020, the United States experienced initial rises in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; hereafter referred to as “Covid-19”) infections [1–3]. By March, state and local government began issuing public-health orders (PHOs) such as school closures, limitations on commerce and gatherings, and stay-at-home orders [4–6]. The potential impact these changes have had on problematic use of psychoactive drugs and accompanying rates of overdose has been of particular concern [7–10]. Before the Covid-19 pandemic, the US was already experiencing multiple drug epidemics (e.g., opioids, alcohol, amphetamines, novel synthetic drugs), with opioids being the primary drivers of overdose [11, 12]. Understanding the ways that Covid-19 and its accompanying PHOs have impacted opioid overdoses could inform the design and implementation of preventive measures during future public-health emergencies.
Since the start of the Covid-19 pandemic, reports of changes in opioid or other drug-related overdoses during Covid-19 have focused mainly on fatal overdose. Non-peer reviewed reports from state and national public-health agencies have almost all documented outbreaks or prolonged increases in opioid and other drug-related fatalities since the start of Covid-19 [13]. Peer-reviewed reports have also detailed an increase in fatal opioid overdoses, either in aggregate during 2020, or after the implementation of Covid-19 PHOs [e.g., 14–16].
Patterns of nonfatal overdoses are generally less documented through official channels, but recently there has been a concerted effort by ODMAP (http://www.odmap.org)—a overdoses and to use this information for public health and safety. Identifying trend changes in nonfatal overdose might be important as a bellwether not only of fatality but of the many deleterious effects associated with increased opioid use in a region. Furthermore, nonfatal overdoses are not simply a dodged bullet. The hypoxia that accompanies an opioid overdose can be prolonged and severe, with chronic and possibly lifelong sequelae that may accumulate across multiple nonfatal overdoses during a lifetime [17]. Perhaps most importantly, the risk for fatal overdose often increases after a nonfatal overdose [18–20].
To our knowledge, only a few peer-reviewed reports have examined changes in nonfatal overdoses separate from fatal overdoses during Covid-19. These studies, which examined changes in Emergency Department (ED) visits for nonfatal overdoses in a small sample of healthcare systems, found increased rates of such visits (as a proportion of all ED visits) during 2020 compared with previous years [16, 21, 22]. However, counts of such visits increased in only some of the health systems evaluated, and even declined in others [22]. Recent data released by the CDC also documented variation across US states in suspected nonfatal overdoses from ED visits [23]. These findings suggest that changes in nonfatal overdoses during Covid-19 are not entirely straightforward: at least for ED visits for nonfatal overdoses, there appears to be between-state variation in these changes. State health authorities may also be interested in such variability within states and from additional data sources given the overall paucity of data.
To address this gap, we used near real-time data from ODMAP to examine regional differences in the impact of Covid-19 PHOs on suspected nonfatal overdoses in Washington DC, Maryland, and Maryland state’s five geographical regions. To prevent erroneously concluding that changes in nonfatal overdoses after the PHOs in 2020 were the specific result of those PHOs rather than normative seasonal patterns, we used interrupted time series analysis with a historical time series of comparable overdose counts from the same regions. Finally, we focused on estimating both the immediate potential changes in nonfatal overdoses after PHO implementation, and any enduring changes in the longer-term trend of overdoses in the different geographical regions.
Methods
Data sources
These analyses were the result of a collaboration agreement between investigators at the National Institute on Drug Abuse’s (NIDA) Intramural Research Program (IRP) in Baltimore, Maryland and the deputy director of the Washington/Baltimore High Intensity Drug Trafficking Area program’s (HIDTA) Overdose Detection Mapping Application Program (ODMAP) data-aggregation project. ODMAP is an online platform for data collection, visualization, and reporting of suspected overdoses. It was launched as a pilot program in parts of Maryland and West Virginia in early 2017; it now receives data from states throughout the US, although we have thus far only received permission to analyze data from Maryland (MD) and Washington DC. Suspected overdose events are uploaded to ODMAP from participating public-health or law-enforcement agencies manually or through an API. Users can visualize suspected overdoses that have been entered into the database via an online dashboard and run simple analyses. The overall goal of ODMAP is to provide near-real-time surveillance of suspected overdose events across different regions in the US. More information on ODMAP can be found in the S1 Appendix.
Suspected nonfatal overdoses in which opioids were recorded as the primary contributor (whether or not alcohol or other drugs were involved) were uploaded to ODMAP from the Maryland Institute for Emergency Medical Services Systems (MIEMSS) and DC Health (Washington DC). Per Maryland state legislative mandate, MIEMSS is required to submit geotagged data on suspected overdoses to ODMAP within 24 hours of responding to an incident. DC Health data are uploaded to ODMAP from an EMS data repository in real time (on average within 15 minutes of the closure of a patient-care record). Because MIEMSS and DC Health started sharing data with ODMAP at different times, the timeframes of overdose data were slightly different for the two regions: July 1, 2018 to September 10, 2020 for Maryland, and August 6, 2018 to October 25, 2020 for Washington DC (DC).
Before providing the data to NIDA, HIDTA completed a data-use agreement with MIEMSS and DC Health. Because no personal identifiers were associated with the data received by the NIDA coauthors, this project was exempted from IRB review by the NIH IRB office.
Outcomes
MIEMSS data
MIEMSS’s initial inclusion criterion for submitting a report to ODMAP was any case where a patient was administered naloxone by Emergency Medical Services (EMS) or prior to EMS arrival. Reports also included the approximate address where the patient was initially encountered or where the overdose occurred, along with the date and time. On July 1, 2019, MIEMSS updated its methods for defining overdose incidents to rule out non-opioid-related overdoses more accurately. The new definition restricted reports to EMS cases where naloxone was administered and there was either: (a) a primary impression of “Suspected opioid overdose (ICD-10-CM F11.9)” or “Poisoning/Overdose/Drug Abuse (ICD-10-CM T50.90)” [24], or (b) a positive response to a service-defined question ("Do you think this patient is suffering from an opioid overdose?"). By MIEMSS estimates, the definition change resulted in a reduction of overdose counts of approximately 14.5%. The additional reports from the naloxone-only definition likely represent cases in which naloxone was administered, but there was uncertainty whether opioids contributed to the patient’s presentation. To adjust for this, we subtracted 14.5% from all Maryland overdoses prior to July 2019. In sensitivity analyses to examine the robustness of the ITS models to MIEMSS estimates, we found that even large misspecifications in these estimates (e.g., > 10%) did not appreciatively change our major conclusions (see S1 Appendix for sensitivity analyses and additional details on the definition change).
DC health data
Standardized case definition of a suspected nonfatal overdoses follows the National Emergency Medical Services Information System (NEMSIS) guidance. A nonfatal opioid overdose is defined as any eligible 911 response where: (a) the Provider’s Primary Impression or Provider’s Secondary Impression are opioid overdose related, or (b) the Primary Symptom or Other Associated Symptoms are opioid overdose related, or (c) medication Administered is naloxone or Narcan and Response to Medication Administered is improved. The patient care report narrative is also queried for opioid- and overdose-related keywords to validate previously identified incidents or identify incidents not previously included. Reports also included the approximate address where the patient was initially encountered or where the overdose occurred, and the date and time.
Study design
We used an interrupted-time-series design (ITS) [25, 26] to compare changes in nonfatal overdoses before and after the implementation of Covid-19 public health orders (our defined intervention). Although ITS analysis of a single time series is considered one of the strongest quasi-experimental approaches [25], it can be further strengthened by the inclusion of a control time series to help rule out cyclical or ongoing influences (e.g., increases or decreases in an outcome that repeat yearly at a specific time) coinciding with the intervention [27]. We took that approach by including a “no-PHO” historical control time series (MD: July 2, 2018 to September 2, 2019; DC: August 6, 2018 to October 20, 2019) in all of our models in addition to the time series of interest, which we called the “Covid year” (MD: July 1, 2019 to September 7, 2020; DC: August 5, 2019 to October 25, 2020). The differences in the timeframes for the two datasets were due to differences in the dates MIEMSS and DC Health started sharing data with ODMAP. The Covid year contained the implementation of PHOs, which, in Maryland, came into effect on March 5, 2020 (state of emergency) and March 30, 2020 (stay-at-home orders). In DC, these orders came into effect on March 11, 2020 (state of emergency) and March 30, 2020 (stay-at-home orders). With the inclusion of the historical control time series, we adjusted for changes in nonfatal overdoses that occurred around mid-March in a year when the Covid-19 pandemic and its accompanying PHOs did not occur. If patterns during the Covid year showed changes similar to those found in the no-PHO historical series, this would weaken the case for a causal connection between Covid PHOs and overdose rates.
To examine regional differences within Maryland, we split the data into five regions: Western, Capital, Central, Southern, and the Eastern Shore. The counties that compose these regions are listed in eTable 1 of the supplemental material S1 Appendix. We used this regional division because it is generally accepted as reflective of the state’s geographic and economic demarcations (Maryland Marketing Partnership, 2021) and because smaller subdivisions (such as counties) would have resulted in sparse data for some regions. These regions are also differentiated by factors associated with regional variation in overdose numbers: population density, income, and EMS request for services (Forati, Ghose, & Mantsch, 2021 [28]; Haffajee et al., 2019 [29]; Monnat, 2019 [30]). Supplemental eTable 2 in S1 Appendix displays median household income and population estimates for the five regions for the 2019 calendar year.
Data analyses
The daily counts of nonfatal overdoses were aggregated to weekly counts to reduce noise. We then used segmented linear regression to fit ITS models. Although Maryland and DC declared a state of emergency (SOE) at different times in early March, both regions implemented stay-at-home orders on the same day (March 30, 2020). We made the assumption that changes (e.g., disruption to addiction treatment services, changes to illicit drug supplies, loneliness/boredom, childcare/economic burden) related to the initial SOE PHO would have delayed effects on overdose rates, and therefore selected March 31, 2020 as the intervention “change point.” We refer to this intervention change point generically as AfterMarch. We were interested in estimating changes in nonfatal overdose before and after this timepoint.
Each model included a constant term (intercept), a binary indicator to assess whether the mean count of overdoses changed after March (AfterMarch: 0,1), a linear slope term (WeekSlope) quantifying overdose counts from July (or August for DC) through March (i.e., when AfterMarch = 0), an interaction term quantifying the slope change in March, a binary indicator for Covid year versus control year, and two more interaction terms, which were the terms of primary interest. The first interaction term (CovidYear X AfterMarch) tested whether the mean level change in overdose counts before and after March differed for the control year versus the Covid year. This allowed us to test whether there was an immediate change in nonfatal overdoses after PHOs and whether this change differed from the control timeframe. The second interaction term (CovidYear X AfterMarch X WeekSlope) tested whether the change in the slope of weekly overdoses before and after March differed for the control year versus the Covid year. This allowed us to test whether there was a sustained change in nonfatal overdoses and whether this changed differed from the control timeframe. We examined evidence for an immediate and sustained change because we hypothesized that changes related to PHOs might have both an immediate impact (e.g., due to closures in addiction treatment clinics) and longer-term impact on counts of overdoses.
We fit separate models to examine changes in nonfatal overdoses for Maryland as a whole and for Washington DC. For finer geographical granularity within Maryland, we fit a separate model for each of the five regions. All models used Newey-West heteroskedasticity-and-autocorrelation-consistent standard errors [31]. We also tested the inclusion of quarter-yearly indicator variables to adjust for seasonal changes in overdoses. These indicator variables only improved the relative fit of the Washington DC models as measured by the AIC and BIC. Thus, we included these indicators in the Washington DC models and excluded them from all Maryland models. Alpha was set at .05, two-tailed. All analyses were conducted using the R (version 3.6.2) programming language (R Core Team, 2019 [32]).
Results
Overall trends in nonfatal-overdose rates for Maryland and Washington, DC, 2018–2020
The unadjusted weekly counts of nonfatal overdoses for the entire analysis period (July 2018 to September 2020) are shown in Fig 1. Even though data have been aggregated from daily to weekly totals, variability across weeks remained prominent. Longer-term trends predating the Covid-19 pandemic are also apparent. Specifically, nonfatal overdoses in Maryland were declining over the entire period prior to Covid-19, with a levelling out around November 2019, followed by a distinct increase starting around April 2020. In contrast, nonfatal overdoses in DC appeared to be generally increasing prior to Covid-19.
Fig 1. Weekly counts of suspected nonfatal overdoses in Maryland state and Washington DC from 2018–2020.

(a) Maryland State. (b) Washington DC. Dashed lines represent the official declaration of a state of emergency (MD: March 5th, 2020; DC: March 11th, 2020) and stay at home orders (MD and DC: March 30th, 2020).
Changes in nonfatal-overdose rates with Covid-19 PHOs
The ITS results are summarized in Table 1 and are shown graphically in Figs 2–4. We also include unadjusted mean weekly counts of overdoses before and after March for each region. Full statistical output from the ITS models is in the Supporting Material S1 Appendix.
Table 1. Mean weekly nonfatal overdose counts and key interrupted time series findings for Maryland state models, Maryland regional models, and Washington DC models.
| Immediate Impact of PHOs? | Sustained Impact of PHOs? | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean weekly count: nonfatal overdoses | Difference in mean level change before vs. after March for control vs. Covid yeara | Difference in weekly slopes before vs. after March for control vs. Covid yearb | Key Findings | ||||||
| Region | Before March | After March | B | 95% CI | p | B | 95% CI | p | |
| MD State | -9.21 | -47.56 to 29.15 | .635 | 2.36 | 0.65 to 4.06 | .007 | Similar pre-March decrease both years; Steeper post-March increase in 2020 | ||
| Covid timeseriesc | 129.05 | 159.18 | |||||||
| Control timeseriesd | 175.41 | 164.15 | |||||||
| MD: Western | 0.73 | -2.80 to 4.27 | .682 | 0.05 | -0.25 to 0.34 | .759 | Very similar post-March increases both years | ||
| Covid timeseries | 7.22 | 7.09 | |||||||
| Control timeseries | 7.39 | 6.63 | |||||||
| MD: Capital | 2.27 | -4.11 to 8.65 | .482 | 0.31 | -0.02 to 0.63 | .066 | Post-March decrease in 2019; Persistent rate in 2020 | ||
| Covid timeseries | 19.10 | 21.77 | |||||||
| Control timeseries | 19.14 | 21.28 | |||||||
| MD: Central | -12.94 | -39.11 to 13.23 | .329 | 1.47 | 0.15 to 2.79 | .029 | Similar pre-March decrease both years; Steeper post-March increase in 2020 | ||
| Covid timeseries | 90.00 | 111.27 | |||||||
| Control timeseries | 131.14 | 121.23 | |||||||
| MD: Southern | -0.21 | -3.30 to 2.88 | .895 | 0.23 | 0.05 to 0.40 | .010 | Similar pre-March decrease both years; New post-March increase in 2020 | ||
| Covid timeseries | 3.55 | 5.05 | |||||||
| Control timeseries | 6.16 | 4.88 | |||||||
| MD: Eastern Shore | 1.01 | -5.08 to 7.10 | .744 | 0.26 | -0.13 to 0.66 | .189 | Graphical suggestion of steeper post-March increase in 2020 | ||
| Covid timeseries | 8.75 | 13.23 | |||||||
| Control timeseries | 11.18 | 9.85 | |||||||
| Washington, DC | -8.20 | -19.50 to 3.10 | .153 | -0.07 | -0.62 to 0.48 | .814 | No steeper post-March increase in 2020 | ||
| Covid timeseriese | 45.94 | 49.07 | |||||||
| Control timeseriesf | 37.80 | 47.21 | |||||||
a CovidYear X AfterMarch interaction term in multivariable regression models.
b CovidYear X AfterMarch X WeekSlope interaction term in multivariable regression models.
c MD Covid timeseries: July 1, 2019 to September 7, 2020.
d MD Control timeseries: July 2, 2018 to September 2, 2019.
e DC Covid Timeseries: August 5, 2019 to October 25, 2020.
f DC Control Timeseries: August 6, 2018 to October 20, 2019. MD = Maryland. PHOs = Public Health Orders. Washington DC models include quarter-year dummy variables to adjust for seasonality.
Fig 2. ITS adjusted weekly nonfatal overdose counts in Maryland state pre- and post-Covid-19 public health orders.
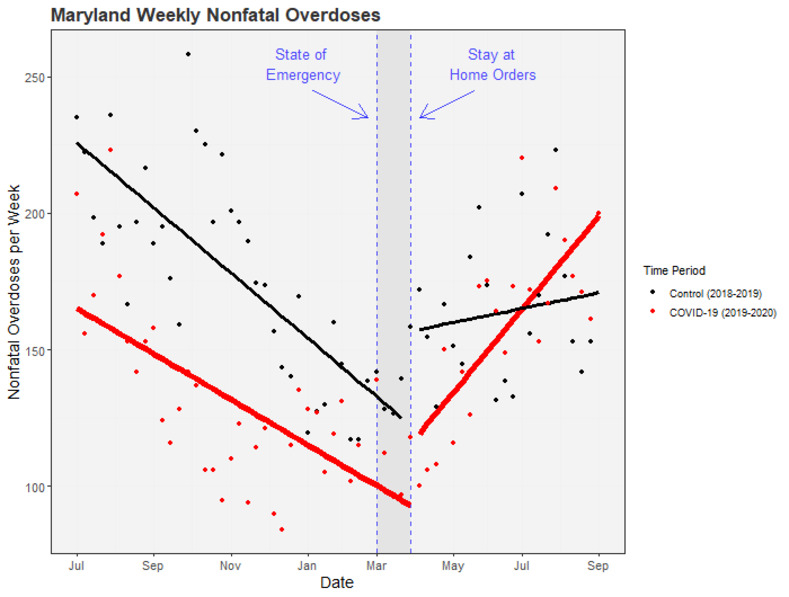
Points represent weekly counts of suspected nonfatal overdoses. Solid lines represent ITS-model-predicted counts: red for the Covid-19 time series (including March 2020), black for the preceding time series (including March 2019). Dashed horizontal lines mark the official declaration of a state of emergency (March 5th, 2020) and stay-at-home orders (March 30th, 2020) in Maryland state.
Fig 4. ITS models of weekly nonfatal overdoses for regions within Maryland.

Regions in Maryland state: Western (a), Capital (b), Central (c), Southern (d), and Eastern Shore (e). Points represent weekly counts of suspected nonfatal overdoses. Solid lines represent ITS-model-predicted counts. Dashed lines represent the official declaration of a state of emergency (March 5th, 2020) and stay at home orders (March 30th, 2020) in Maryland.
Fig 3. ITS adjusted weekly nonfatal overdose counts in Washington DC pre- and post-Covid-19 public health orders.
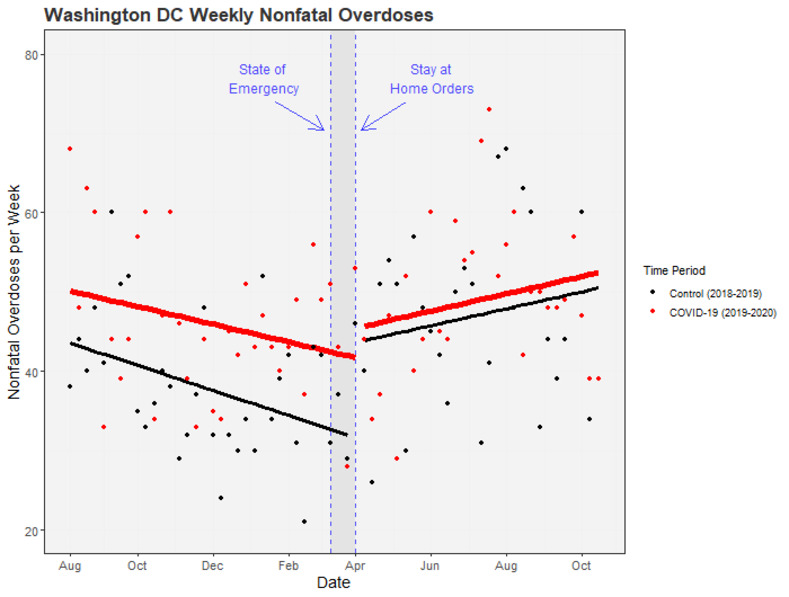
Points represent weekly counts of suspected nonfatal overdoses. Solid lines represent ITS-model-predicted counts: red for the Covid-19 time series (including March 2020), black for the preceding time series (including March 2019). Washington DC models are adjusted for seasonality with quarter-year dummy variables. Quarter-year dummies are set to their means to generate a smooth line. Dashed horizontal lines mark the official declaration of a state of emergency (March 11th, 2020) and stay-at-home orders (March 30th, 2020) in Washington DC.
Maryland state and Maryland regions
Between July 2019 and March 2020, Maryland as a whole had a mean weekly nonfatal overdose count of 129.05. During this time, nonfatal overdoses were decreasing (Fig 2). After March 2020, mean weekly counts of nonfatal overdoses increased to 159.18. In contrast, mean weekly counts of nonfatal overdoses after March 2019 during the control time series decreased to 164.15 from a high of 175.41 before March. The five Maryland regions displayed differing patterns of change before and after March: the Capital region of Maryland had increases in nonfatal overdoses after March for both the Covid and control time series; the Western region had decreases after March for both time series; the Central, Southern, and Eastern Shore regions had increases after March during the Covid time series and decreases after March during the control time series.
After accounting for underlying trends, ITS models estimated an increase (not reaching statistical significance) of 22.5 nonfatal overdoses immediately following the PHOs in March during the Covid time series (B = 22.50; 95% CI, -2.97 to 48.00; p = .083). However, when comparing the difference between this change and the change after March during the control time series, we found no reliable differences between these mean-level changes (as reflected by the CovidYear X AfterMarch interaction term, B = -9.21; 95% CI, -47.56 to 29.15; p = .64). There were also no reliable differences between the mean-level changes before and after March for the Covid year versus the control time series for any of the five regions.
However, the pattern of change in the slopes of nonfatal overdoses after March—i.e., in the rate of change across weeks—was different during the Covid year than during the preceding control time series for Maryland as a whole; we estimate that there were an additional 2.4 nonfatal overdoses each week post March in 2020 compared with the post-March slope during the control period (B = 2.36; 95% CI, 0.65 to 4.06; p = .007). This statewide increase was driven by increases in specific subregions: Southern MD had an additional 0.2 overdoses each week post March in 2020 (B = 0.23; 95% CI, 0.05 to 0.40; p = .010) and Central MD had an additional 1.5 overdoses each week (B = 1.47; 95% CI, 0.15 to 2.79; p = .029). There was also some evidence for increases in the Capital region of MD compared to the control time series (B = 0.31; 95% CI, -0.02 to 0.63; p = .066). As shown in Fig 4A–4E, nonfatal overdoses in these regions were decreasing from July to March in both the Covid and control time series, but then diverged after March in region-specific ways: increasing in 2020 only (Southern MD), increasing more steeply in 2020 than in 2019 (Central MD), or not showing a subsequent decrease in 2020 after having decreased in 2019 (MD Capital region).
In the Eastern Shore region of MD, there was a graphical suggestion of a steeper post-March increase during the Covid-19 year, but week-to-week variability precluded its reaching statistical significance (B = 0.26; 95% CI, -0.13 to 0.66; p = .189). In the Western Shore region of MD, rates during the two years largely mirrored each other (B = 0.05; 95% CI, -0.25 to 0.34; p = .759).
Washington DC
In Washington DC, mean weekly counts of nonfatal overdoses increased after March for both the Covid and control timeseries. However, when comparing the difference between these changes for the two timeseries, we found no difference in mean-level changes immediately after March for the Covid versus control time series (B = -8.20; 95% CI, -19.50 to 3.10; p = .153), nor was there sign of a steeper post-March increase in slope during the Covid year (B = -0.07; 95% CI, -0.62 to 0.48; p = .814).
Discussion
We found, after accounting for cyclical patterns and ongoing trends, that the Covid-19 pandemic and its accompanying PHOs were associated with steeper weekly growth in counts of suspected nonfatal opioid overdoses in many but not all regions for which we had data. To give one example in concrete terms, model-estimated weekly counts in one region (Central MD) increased from 116 to 127 in the period of March-September of 2019, and then increased from 81 to 142 in March-September of 2020. In contrast, for Washington, DC, the increases across those time periods were similar in 2019 (44 to 51) and 2020 (50 to 52).
One conclusion we can tentatively draw from our results is that they do not straightforwardly support the narrative that overdoses increased disproportionately in rural versus urban regions [33]. The geographical patterns in our data did not follow a tidy urban/rural dichotomy; however, there was some evidence that there were sustained increases in nonfatal overdoses in regions in MD with higher populations. Recent studies examining regional variation in overdoses before Covid-19 seem to suggest that large metropolitan counties have higher rates of fatal opioid overdoses compared to rural or micropolitan counties (Haffajee et al., 2019; Monnat, 2019). Even so, narrative reviews on geographical heterogeneity in opioid overdoses have found that rural/urban differences in opioid overdose rates appear to vary both between and within single and multi-state regions (e.g., western, northeastern, midwestern, or southern states) in the US (Rigg, Monnat, & Chavez, 2018 [34]), which may explain why changes were observed in Maryland, but not in its neighbor, Washington DC.
Before conducting our analyses, we suspected that differences in overdose rates across regions might be modulated simultaneously upward and downward by countervailing influences. Indeed, recent studies have documented a staggering increase in a variety of risk factors for substance use and overdose, including worsening psychiatric outcomes (e.g., stress, anxiety, depression), loneliness, economic distress, and disruptions to daily living and routine (e.g., childcare burden, poor sleep quality) [35–39], increased likelihood of using drugs alone, changes to illicit drug supplies [23], and reduced physical access to treatment services. On the other hand, mitigating influences could have included the relaxation of restrictions on dispensation of methadone and buprenorphine, disruption to supply chains for illicit drugs, and adherence to stay-at-home mandates and physical-distancing guidelines, which might reduce drug-acquisition behaviors [40–45].
Although we cannot be certain which factors were involved–or the relative contribution of each factor–in these changes in nonfatal overdoses, our findings suggest that within-state variability in changes in nonfatal overdoses during Covid-19 did occur and are likely to be found in other states as well [23]. Previous research has also found that the factors likely responsible for regional variation in opioid overdoses can vary geographically as well. For example, before Covid-19, economic distress appeared to have a stronger association with overdose mortality rates than opioid supply factors in rural counties in the US. In contrast, in urban counties, changes to opioid supply factors were more strongly associated with overdose mortality rates than economic distress factors (see Monnat, 2019). It is now known that the increases in fatal overdoses across the US during Covid-19 were primarily driven by synthetic opioids including illicitly manufactured fentanyl (CDC, 2020). It is possible that synthetic opioid supply/distribution changes in different regions in MD and Washington DC contributed to the differences in overdose numbers we observed.
Whatever the specific causes may be, the one clear conclusion we can draw from these findings is that regional variation is a paramount feature of both opioid overdose rates and factors contributing to opioid overdoses. Policymakers and public-health officials responsible for intervention design/deployment or legislation aimed at curtailing factors associated with overdoses in MD, Washington DC, and the US should keep this at the fore; it is likely that both policy and prevention will need to be tailored to specific regions. However, to more fully understand what factors contribute to regional differences, continual surveillance on a wide range of potential factors is needed. Continual follow-up analyses examining the mechanisms driving between and within region variation will need to identify high-risk areas, changes in factors driving overdose rates in these areas, and mechanisms to target via interventions or policy.
Finally, although our main goal was to isolate the impact of Covid-19 PHOs on nonfatal overdoses in Washington DC and Maryland, our use of a historical control timeseries of overdoses from previous years in the same geographical regions revealed potentially interesting findings about longer-term trends predating the Covid-19 pandemic and the impact that the pandemic may have had on these trends. Specifically, the steady long-term decline of nonfatal overdose in Maryland from when our control time series began, appeared to be decisively broken shortly after the implementation of the PHOs in March 2020. Further support for a trend change can only be inferred with more overdose data pre-July 2018 (the beginning of our control timeseries) and post-September 2020. Access to these data was limited by agreements with the original data sources. Future studies should examine longer-term trends in Maryland and elsewhere, because these findings may signal a protracted shift in risk for overdose which may need to be addressed by mitigation efforts.
Limitations
There is an ambiguity inherent in our nonfatal-overdose data: overdoses that resulted in death were, in a sense, censored from the data set. Thus, we could not directly distinguish between an overdose that was avoided and an overdose that became fatal: either of those would be, in effect, one less nonfatal overdose. Ours is not the only published paper with that limitation [46]. However, the ambiguity is lessened by recent findings from the CDC and others: fatal opioid overdoses in Maryland and in Washington, DC, have indeed increased since the implementation of PHOs, over and above ongoing trends [23]. Thus, we assume that any flat or decreasing rates of nonfatal overdoses in our data are at least partly reflective of fatalities, though we cannot currently be precise about the proportions. We conceptualize our nonfatal-overdose data as a tally of an inherently undesirable event that increases the risk of future overdose events and places significant burden on healthcare systems [17]. Our study also only focuses on counts of nonfatal overdoses. While the data available to us precluded examination of rates of nonfatal overdose, future research should examine changes in rates of nonfatal overdoses before and during Covid-19 in MD and Washington DC.
Conclusion
Our findings show that, for counts of suspected nonfatal overdoses, the net effect of the changes that accompanied the Covid-19 pandemic was deleterious in most geographical regions we assessed. However, some regions were clearly more affected than others. Monitoring nonfatal overdoses by region and factors known to contribute to regional variation in overdoses could be a valuable tool for identifying and understanding dangerous trends as the pandemic continues to evolve.
Supporting information
(DOCX)
Data Availability
Data are unable to be shared publicly because they contain potentially sensitive information including the time a place (i.e., geotagged) of nonfatal overdoses in Maryland and Washington DC. Furthermore, ODMAP does not own any data that has been shared with the Washington/Baltimore High Intensity Drug Trafficking Area (W/B HIDTA), any data provided to an external third party would need to be approved by the data owners. Data requests can be sent to tracy.garner@dc.gov (DC Health). Data request forms for Maryland Institute for Emergency Medical Services Systems (MIEMSS) data can be filled out at www.miemss.org/DataRequest.
Funding Statement
ABH, DHE, KES, LVP, DS, and KLP were supported in part by the Intramural Research Program of the National Institutes of Health NIDA. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. This research was supported in part by the Intramural Research Program of the NIH NIDA.
References
- 1.Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis. 2020;20(5):533–4. Epub 2020/02/23. doi: 10.1016/S1473-3099(20)30120-1 ; PubMed Central PMCID: PMC7159018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fauver JR, Petrone ME, Hodcroft EB, Shioda K, Ehrlich HY, Watts AG, et al. Coast-to-coast spread of SARS-CoV-2 during the early epidemic in the United States. Cell. 2020;181(5):990–6 e5. Epub 2020/05/11. doi: 10.1016/j.cell.2020.04.021 ; PubMed Central PMCID: PMC7204677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Haynes B, Messonnier NE, Cetron MS. First travel-related case of 2019 novel coronavirus detected in United States: press release 2020. [cited 2020 November 30]. Available from: https://www.cdc.gov/media/releases/2020/p0121-novel-coronavirus-travel-case.html. [Google Scholar]
- 4.Dave D, Friedson AI, Matsuzawa K, Sabia JJ. When do shelter-in-place orders fight COVID-19 Best? policy heterogeneity across states and adoption time. Econ Inq. 2020. Epub 2020/08/25. doi: 10.1111/ecin.12944 ; PubMed Central PMCID: PMC7436765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schuchat A, Team CC-R. Public health response to the initiation and spread of pandemic COVID-19 in the United States, February 24-April 21, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(18):551–6. Epub 2020/05/08. doi: 10.15585/mmwr.mm6918e2 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mervosh S, Lu D, Swales V. See which states and cities have told residents to stay at home. New York Times. 2020. April 7. [Google Scholar]
- 7.Knell G, Robertson MC, Dooley EE, Burford K, Mendez KS. Health behavior changes during COVID-19 pandemic and subsequent “stay-at-home” orders. Int J Environ Res Public Health. 2020;17(17). Epub 2020/09/03. doi: 10.3390/ijerph17176268 ; PubMed Central PMCID: PMC7504386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Linas BP, Savinkina A, Barbosa C, Mueller PP, Cerdá M, Keyes K, et al. A clash of epidemics: Impact of the COVID-19 pandemic response on opioid overdose. Journal of Substance Abuse Treatment. 2020;120:108158. doi: 10.1016/j.jsat.2020.108158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Melamed OC, Hauck TS, Buckley L, Selby P, Mulsant BH. COVID-19 and persons with substance use disorders: Inequities and mitigation strategies. Subst Abus. 2020;41(3):286–91. Epub 2020/07/23. doi: 10.1080/08897077.2020.1784363 . [DOI] [PubMed] [Google Scholar]
- 10.Ornell F, Moura HF, Scherer JN, Pechansky F, Kessler FHP, von Diemen L. The COVID-19 pandemic and its impact on substance use: Implications for prevention and treatment. Psychiatry Res. 2020;289:113096. Epub 2020/05/15. doi: 10.1016/j.psychres.2020.113096 ; PubMed Central PMCID: PMC7219362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hoots B, Vivolo-Kantor A, Seth P. The rise in non-fatal and fatal overdoses involving stimulants with and without opioids in the United States. Addiction. 2020;115(5):946–58. Epub 2020/01/09. doi: 10.1111/add.14878 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thylstrup B, Seid AK, Tjagvad C, Hesse M. Incidence and predictors of drug overdoses among a cohort of >10,000 patients treated for substance use disorder. Drug Alcohol Depend. 2020;206:107714. Epub 2019/11/23. doi: 10.1016/j.drugalcdep.2019.107714 . [DOI] [PubMed] [Google Scholar]
- 13.AMA. Issue brief: Reports of increases in opioid- and other drug-related overdose and other concerns during COVID pandemic 2021 [cited 2021 May 17]. Available from: https://www.ama-assn.org/system/files/2020-12/issue-brief-increases-in-opioid-related-overdose.pdf.
- 14.Glober N, Mohler G, Huynh P, Arkins T, O’Donnell D, Carter J, et al. Impact of COVID-19 pandemic on drug overdoses in Indianapolis. J Urban Health. 2020. Epub 2020/10/03. doi: 10.1007/s11524-020-00484-0 ; PubMed Central PMCID: PMC7529089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Slavova S, Rock P, Bush HM, Quesinberry D, Walsh SL. Signal of increased opioid overdose during COVID-19 from emergency medical services data. Drug Alcohol Depend. 2020;214:108176. Epub 2020/07/28. doi: 10.1016/j.drugalcdep.2020.108176 ; PubMed Central PMCID: PMC7351024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rodda LN, West KL, LeSaint KT. Opioid overdose–related emergency department visits and accidental deaths during the COVID-19 pandemic. Journal of Urban Health. 2020;97(6):808–13. doi: 10.1007/s11524-020-00486-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zibbell J, Howard J, Clarke S, Ferrell A, S. K. Non-fatal opioid overdose and associated health outcomes: final summary report, Office of the Assistant Secretary for Planning and Evaluation. 2019. [cited 2020 December 28]. Available from: https://aspe.hhs.gov/basic-report/non-fatal-opioid-overdose-and-associated-health-outcomes-final-summary-report. [Google Scholar]
- 18.Olfson M, Wall M, Wang S, Crystal S, Blanco C. Risks of fatal opioid overdose during the first year following nonfatal overdose. Drug Alcohol Depend. 2018;190:112–9. doi: 10.1016/j.drugalcdep.2018.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Caudarella A, Dong H, Milloy MJ, Kerr T, Wood E, Hayashi K. Non-fatal overdose as a risk factor for subsequent fatal overdose among people who inject drugs. Drug Alcohol Depend. 2016;162:51–5. doi: 10.1016/j.drugalcdep.2016.02.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stoové MA, Dietze PM, Jolley D. Overdose deaths following previous non-fatal heroin overdose: record linkage of ambulance attendance and death registry data. Drug Alcohol Rev. 2009;28(4):347–52. doi: 10.1111/j.1465-3362.2009.00057.x [DOI] [PubMed] [Google Scholar]
- 21.Ochalek TA, Cumpston KL, Wills BK, Gal TS, Moeller FG. Nonfatal opioid overdoses at an urban emergency department during the COVID-19 pandemic. JAMA. 2020. Epub 2020/09/19. doi: 10.1001/jama.2020.17477 ; PubMed Central PMCID: PMC7501586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Soares WE III, Melnick ER, Nath B, D’Onofrio G, Paek H, Skains RM, et al. Emergency department visits for nonfatal opioid overdose during the COVID-19 pandemic across 6 US healthcare systems. Annals of Emergency Medicine. 2021. doi: 10.1016/j.annemergmed.2021.03.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Centers for Disease Control. Increase in fatal drug overdoses across the United States driven by synthetic opioids before and during the Covid-19 pandemic 2020 [cited 2020 December 28]. Available from: https://emergency.cdc.gov/han/2020/han00438.asp.
- 24.WHO. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)2015.
- 25.Shadish WR, Cook TD, Campbell DT. Experimental and Quasi-Experimental Designs for Generalized Causal Inference. Boston: Houghton Mifflin; 2002. doi: 10.1037/1082-989x.7.1.3 [DOI] [Google Scholar]
- 26.Kontopantelis E, Doran T, Springate DA, Buchan I, Reeves D. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 2015;350:h2750. doi: 10.1136/bmj.h2750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hategeka C, Ruton H, Karamouzian M, Lynd LD, Law MR. Use of interrupted time series methods in the evaluation of health system quality improvement interventions: a methodological systematic review. BMJ Global Health. 2020;5(10):e003567. doi: 10.1136/bmjgh-2020-003567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Forati A. M., Ghose R., & Mantsch J. R. (2021). Examining Opioid Overdose Deaths across Communities Defined by Racial Composition: a Multiscale Geographically Weighted Regression Approach. Journal of Urban Health, 98(4), 551–562. doi: 10.1007/s11524-021-00554-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Haffajee R. L., Lin L. A., Bohnert A. S. B., & Goldstick J. E. (2019). Characteristics of US counties with high opioid overdose mortality and low capacity to deliver medications for opioid use disorder. JAMA Network Open, 2(6), e196373–e196373. doi: 10.1001/jamanetworkopen.2019.6373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Monnat S. M. (2019). The contributions of socioeconomic and opioid supply factors to US drug mortality rates: Urban-rural and within-rural differences. Journal of Rural Studies, 68, 319–335. [Google Scholar]
- 31.Newey W.K., K.D. W. Automatic lag selection in covariance matrix estimation. The Review of Economic Studies. 1994;61(4):631–53. doi: 10.2307/2297912 [DOI] [Google Scholar]
- 32.Team, R. C. (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing. http://www.r-project.org [Google Scholar]
- 33.Swift H, Goodnough A. “The drug became his friend”: pandemic drives hike in opioid deaths. New York Times. September 29, 2020. [Google Scholar]
- 34.Rigg K. K., Monnat S. M., & Chavez M. N. (2018). Opioid-related mortality in rural America: Geographic heterogeneity and intervention strategies. International Journal of Drug Policy, 57, 119–129. doi: 10.1016/j.drugpo.2018.04.011 [DOI] [PubMed] [Google Scholar]
- 35.Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain, Behavior, and Immunity. 2020;89:531–42. doi: 10.1016/j.bbi.2020.05.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bareket-Bojmel L, Shahar G, Margalit M. COVID-19-related economic anxiety is as high as health anxiety: findings from the USA, the UK, and Israel. International Journal of Cognitive Therapy. 2020:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.McGinty EE, Presskreischer R, Han H, Barry CL. Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA. 2020;324(1):93–4. doi: 10.1001/jama.2020.9740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Holland KM, Jones C, Vivolo-Kantor AM, Idaikkadar N, Zwald M, Hoots B, et al. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry. 2021;78(4):327–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Del Boca D, Oggero N, Profeta P, Rossi M. Women’s and men’s work, housework and childcare, before and during COVID-19. Review of Economics of the Household. 2020;18(4):1001–17. doi: 10.1007/s11150-020-09502-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bergman BG, Kelly JF, Fava M, Eden Evins A. Online recovery support meetings can help mitigate the public health consequences of COVID-19 for individuals with substance use disorder. Addict Behav. 2020;113:106661. Epub 2020/10/11. doi: 10.1016/j.addbeh.2020.106661 ; PubMed Central PMCID: PMC7493730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Del Pozo B, Rich JD. Revising our attitudes towards agonist medications and their diversion in a time of pandemic. Journal of Substance Abuse Treatment. 2020;119:108139. doi: 10.1016/j.jsat.2020.108139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mellis AM, Potenza MN, Hulsey JN. COVID-19-related treatment service disruptions among people with single-and polysubstance use concerns. Journal of Substance Abuse Treatment. 2020:108180. doi: 10.1016/j.jsat.2020.108180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance use disorders—the perfect storm. Am J Psychiatry. 2020;177(9):805–7. Epub 2020/07/15. doi: 10.1176/appi.ajp.2020.20040417 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Substance Abuse and Mental Health Services Administration. Opioid treatment program guidance 2020 [cited 2020 March 18]. Available from: www.samhsa.gov/sites/default/files/otp-guidance-20200316.pdf.
- 45.Lin LA, Fernandez AC, Bonar EE. Telehealth for substance-using populations in the age of coronavirus disease 2019: recommendations to enhance adoption. JAMA Psychiatry. 2020. Epub 2020/07/02. doi: 10.1001/jamapsychiatry.2020.1698 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Vivolo-Kantor AM, Hoots BE, Scholl L, Pickens C, Roehler DR, Board A, et al. Nonfatal drug overdoses treated in emergency departments—United States, 2016–2017. Morbidity and Mortality Weekly Report. 2020;69(13):371–6. doi: 10.15585/mmwr.mm6913a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
Data Availability Statement
Data are unable to be shared publicly because they contain potentially sensitive information including the time a place (i.e., geotagged) of nonfatal overdoses in Maryland and Washington DC. Furthermore, ODMAP does not own any data that has been shared with the Washington/Baltimore High Intensity Drug Trafficking Area (W/B HIDTA), any data provided to an external third party would need to be approved by the data owners. Data requests can be sent to tracy.garner@dc.gov (DC Health). Data request forms for Maryland Institute for Emergency Medical Services Systems (MIEMSS) data can be filled out at www.miemss.org/DataRequest.