

Abstract
Repeated head impact exposure and concussions are common in American football. Identifying the factors associated with high magnitude impacts aids in informing sport policy changes, improvements to protective equipment, and better understanding of the brain’s response to mechanical loading. Recently, the Stanford Instrumented Mouthguard (MiG2.0) has seen several improvements in its accuracy in measuring head kinematics and its ability to correctly differentiate between true head impact events and false positives. Using this device, the present study sought to identify factors (e.g., player position, helmet model, direction of head acceleration, etc.) that are associated with head impact kinematics and brain strain in high school American football athletes. 116 athletes were monitored over a total of 888 athlete exposures. 602 total impacts were captured and verified by the MiG2.0’s validated impact detection algorithm. Peak values of linear acceleration, angular velocity, and angular acceleration were obtained from the mouthguard kinematics. The kinematics were also entered into a previously developed finite element model of the human brain to compute the 95th percentile maximum principal strain. Overall, impacts were (mean ± SD) 34.0 ± 24.3 g for peak linear acceleration, 22.2 ± 15.4 rad/s for peak angular velocity, 2979.4 ± 3030.4 rad/s2 for peak angular acceleration, and 0.262 ± 0.241 for 95th percentile maximum principal strain. Statistical analyses revealed that impacts resulting in Forward head accelerations had higher magnitudes of peak kinematics and brain strain than Lateral or Rearward impacts and that athletes in skill positions sustained impacts of greater magnitude than athletes in line positions. 95th percentile maximum principal strain was significantly lower in the observed cohort of high school football athletes than previous reports of collegiate football athletes. No differences in impact magnitude were observed in athletes with or without previous concussion history, in athletes wearing different helmet models, or in junior varsity or varsity athletes. This study presents novel information on head acceleration events and their resulting brain strain in high school American football from our advanced, validated method of measuring head kinematics via instrumented mouthguard technology.
Keywords: head impact sensor, concussion, brain injury, head acceleration, finite element model, helmet
Introduction
Over one million male high school athletes participate in American football in the United States, contributing to its success as the country’s most popular contact sport. However, high school football has experienced a decline in participation numbers in recent years, likely due to growing concerns over athlete brain health.41 Concussion42 and repeated head impact exposure8 are both frequent in American football; these forms of trauma may increase the risk of neurodegeneration over time2 and are often associated with long-lasting neurological consequences.45 Identifying risk factors for dangerous head impacts in American football is important to inform potential rule changes,10 training regimens,15,55 or innovations in protective equipment3 that could reduce the likelihood of brain injury and the cumulative burden of repeated impact exposure.
Linear and angular head kinematics resulting from sport-related impacts have been associated with the risk of ensuing brain injury51 and are regularly used to describe the relative severity of impacts. The magnitudes of head accelerations, even in the absence of diagnosed concussion, have been associated with elevated levels of blood biomarkers of brain injury,35,63 changes in oculomotor function,34,64 structural and functional brain changes observed via a variety of imaging techniques,5,19,20,49 and obvious performance decrement6 in high school football players. Further, head kinematics are often used to directly derive kinematic-based injury criteria59 or serve as input to finite element (FE) models24 and machine learning models28,60 to estimate the strain-based response endured by the brain tissue.
Researchers frequently employ head impact sensors to measure head kinematics resulting from the impacts that contact sport athletes sustain on the field. Several kinds of head impact sensors have been used in American football, including helmet-mounted sensors,18 headband-mounted sensors,56 skin patch sensors,55 and instrumented mouthguards.6,22 These devices can suffer from recording a high number of false positive events (i.e., those not associated with any contact involving significant head movement).47 Therefore, various filtering algorithms that aim to determine which recorded events are true or false positives have been developed for many head impact sensors.22,27,57 Further, several studies have found a significant amount of error in the kinematic measurements reported by many of these devices.33,36 Instrumented mouthguards, however, have recently been shown to be accurate and reliable devices for measuring head kinematics,36,40 as they are worn firmly against the upper dentition of athletes. The upper dentition is rigidly affixed to the skull and closer to the head’s center of gravity than locations on the outside of the skull, where other types of devices are worn.
Many factors, such as skill level,53 helmet model,52 impact location,18 and player position,18 have been found to influence the magnitude of head impact kinematics in previous studies of American football, but more research is necessary to resolve the sport’s persisting issues with athlete brain safety. Accurate measurement of head kinematics can aid in more precisely describing the relative severity of impacts among various athlete populations and in estimating the tissue-level response of the brain to an impact. Recently, the Stanford Instrumented Mouthguard (MiG2.0) and its impact detection algorithm (MiGNet) have improved in accurately recording head kinematics and identifying true positive impacts.22,40 Therefore, this study aimed to use the MiG2.0 with MiGNet to characterize head kinematics and brain strain experienced in high school American football athletes, as well as identify sport-specific factors that influence the magnitude of football impacts.
Methods
Participants
All activities were approved by the Institutional Review Board at Stanford University prior to any participant enrollment in the study. High school football players (age = 16.0 ± 1.2 years) from four high schools were recruited for study participation during the 2018 and 2019 Fall competitive seasons (n = 116). At the beginning of each season, age, weight, height, concussion history, skill level (i.e., varsity or junior varsity (JV)), helmet model, and player positions were recorded for each athlete. Body mass index (BMI) was also calculated for each athlete according to the CDC definition and weight and height values at baseline assessment.
In high school football, athletes often change player positions throughout the season and can play multiple positions during a single game (e.g., both offensive and defensive positions). Therefore, similar to previous work,53 player positions were grouped into two categories: line positions and skill positions. Athletes were put into the line position group if they reported playing offensive or defensive line positions (e.g., center, defensive end, defensive tackle, tight end, offensive tackle, offensive guard); skill positions were classified as all other positions.
Head Impact Data Collection
Study participants wore MiG2.0 mouthguards during their respective team’s practices and games (Figure 1). Dental impressions were taken for each athlete prior to the beginning of data collection so the MiG2.0 devices could be customized to each individual player’s upper dentition. Each MiG2.0 mouthguard contained a triaxial accelerometer that acquired linear acceleration data at 1000 Hz and a triaxial gyroscope that acquired angular velocity data at 8000 Hz. The mouthguards were programmed such that they would be triggered to record a 200 ms time window (50 ms pre-trigger, 150 ms post-trigger) of linear and angular kinematics whenever any of the X, Y, or Z directions of linear acceleration exceeded a threshold of 10 g. The custom MiG2.0 mouthguard with these same settings was previously validated to provide accurate kinematic measurements that could reliably be used to calculate brain injury criteria.39 Data was collected by the MiG2.0 mouthguards from a total of 888 athlete-exposures during the monitored time period. An athlete-exposure (AE) was defined as an athlete entering a game or practice session wearing their instrumented mouthguard.
Figure 1.

MiG2.0 instrumented mouthguard device (top) and mouthguard electronics (bottom). Arrows show placement of electronics embedded in the mouthguard.
Kinematics Data Processing
All recorded events were processed by the MiGNet program, a validated, deep learning algorithm that distinguishes true head impacts from false positive events caused by mouthguard handling, application, or other movements that are unrelated to impacts.22 Recorded mouthguard events in the present study were not verified on video. The kinematics of true impact events (as classified by MiGNet) were further examined for additional scrutiny. The purpose of the following exclusion criteria was not to further distinguish true impacts from potential false positives, but rather to ensure that quality mouthguard measurements were used in our analyses. Events were considered erroneous if they met one of the following criteria: 1) Obvious high-frequency components (i.e., above 400 Hz); 2) Linear acceleration at the accelerometer above 200 g; 3) Magnitude of angular velocity in each direction higher than 70 rad/s, which is the measuring range of the gyroscope. Events with angular acceleration peaks smaller than 500 rad/s2 were also eliminated considering the likelihood that their signals were largely influenced by noise and not reliable for estimating brain strain.
The linear acceleration and angular velocity of remaining impact events were filtered by a fourth-order Butterworth filter at 160 Hz. A five-point stencil derivative was performed on the angular velocity to calculate angular acceleration, which was also filtered by a fourth-order Butterworth filter at 160 Hz. The linear acceleration was transformed from the accelerometer location to the estimated center of gravity (CoG) of the head. The initial 200 ms time window was then truncated to 190 ms (45 ms pre-trigger, 145 ms post-trigger) to avoid noise at the beginning and end of the kinematics recordings, a change that was previously confirmed to not significantly influence brain strain calculations.39 Peak linear acceleration (PLA), peak angular velocity (PAV) and peak angular acceleration (PAA) were recorded for each of the events that remained after these data processing steps.
The direction of head movement resulting from impacts was then estimated using the direction of head CoG linear acceleration at the time of its peak. The linear acceleration data 1 ms and 2 ms before the peak time, at the peak time, and 1 ms and 2ms after the peak time (i.e., a total of 5 ms centered around the time of peak linear acceleration) were averaged at each of the X, Y, and Z directions. The resulting direction was classified according to the orientation system defined in Society of Automotive Engineers document J211. Briefly, the geometry of the head was divided into four equal sections of 90° azimuth about its circumference. These sections were centered at the front, left, right, and back of the head. Impacts with resulting head accelerations pointing from the back to the front of the head were classified as Forward impacts, and from the front to back of the head as Rearward impacts. Impact accelerations pointing from left to right and right to left were grouped together as Lateral impacts. Any impact with a peak acceleration direction vector pointing down through the head at an elevation of 65° or greater was classified as a Downward impact. This categorization of head acceleration direction was similar to the estimated impact location in previous work utilizing the Head Impact Telemetry (HIT) System.17 However, the present method to identify head acceleration directions, rather than head impact locations, was used in part because body impacts, which do not have a head impact location, can induce head accelerations. Additionally, head impact sensors have shown considerable difficulty in accurately predicting head impact location.13
Brain Strain Simulation
The Kungliga Tekniska högskolan (KTH) finite element (FE) head model,37 which has been validated by cadaver experiments,31,61 was used to evaluate maximum principal strain of the brain for each impact. In these simulations, the skull was assumed to be rigid and move according to the measured angular velocity and linear acceleration. The simulations were performed using LS-DYNA with a double precision solver. The peak value of the 95th percentile maximum principal strain (MPS95) was extracted from the simulation results to represent the severity of brain tissue deformation.
Statistical Analysis
In total, four primary endpoints were evaluated in this study: PLA, PAV, PAA, and MPS95. The Generalized Estimating Equations (GEE) with Huber-White sandwich estimates were used to assess the association between primary endpoints and a set of covariates, including the acceleration direction (Rearward, Lateral, Forward), helmet model (Riddell Speedflex, VICIS Zero1), player position (line, skill), skill level (JV, varsity), BMI, school, and concussion history. For the primary analysis, all observed data was used to fit GEE models, using the unstructured correlation within participants. For sensitivity analysis, subgroup analyses were performed within each helmet model category, player position category, and acceleration direction category. Downward impacts were not included as there were too few (n = 8), and only the Riddell Speedflex and VICIS Zero1 helmets were worn by enough athletes for these analyses. Finally, both GEE (with each study participant treated as a cluster) and Welch’s t-test were used to compare MPS95 values to a previously published dataset of 118 collegiate football impacts39 that were also recorded by the MiG2.0 and simulated with the KTH FE head model, to test whether the distribution of MPS95 in high school football impacts significantly differed from that of the collegiate football impacts. All GEE models were fitted using the gee() function in R version 3.6.3. All p-values were calculated using the two-sided test unless otherwise noted.
Results
In total, the instrumented mouthguards recorded 66,969 accelerative events. Of these, 713 were verified as head impacts by the MiGNet program. After data processing, 602 impacts remained and were included in statistical analyses. Of the 116 athletes participating in the study, 84 sustained an impact during the monitored time period. The distribution of these 602 impact events by skill level, acceleration direction, helmet model, and position is displayed in Table 1. Overall, impacts sustained by the present cohort were (mean ± SD) 34.0 ± 24.3 g for PLA, 22.2 ± 15.4 rad/s for PAV, 2979.4 ± 3030.4 rad/s2 for PAA, and 0.262 ± 0.241 for MPS95. These results are displayed in Figure 2.
Table 1.
Distribution of impact events verified by MiGNet.
| JV (181) |
Varsity (421) |
Overall (602) |
|
|---|---|---|---|
| Acceleration Direction | |||
| Forward | 42 | 54 | 96 |
| Rearward | 74 | 182 | 256 |
| Lateral | 61 | 181 | 242 |
| Downward | 4 | 4 | 8 |
| Helmet Model | |||
| VICIS Zero1 | 63 | 100 | 163 |
| Riddell Speedflex | 68 | 305 | 373 |
| Other | 50 | 16 | 66 |
| Position | |||
| Skill | 69 | 168 | 237 |
| Line | 97 | 252 | 349 |
| Missing | 15 | 1 | 16 |
A variety of helmet models were worn, but the VICIS Zero1 and Riddell Speedflex were most predominantly worn; all other helmet models were grouped into the “Other” category. Impacts sustained by athletes that did not report their player position are reflected in the “Missing” category.
Figure 2.
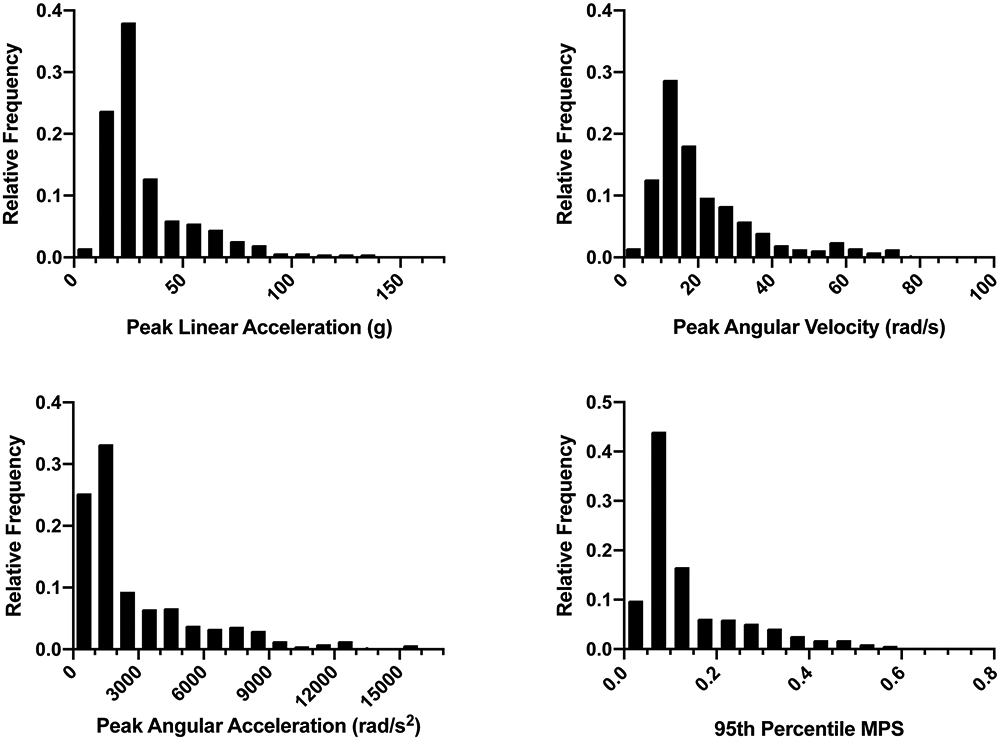
Frequency distributions of high school American football impacts by peak head kinematics and 95th percentile maximum principal strain (MPS).
Relative to Rearward and Lateral impacts, Forward impacts had the highest magnitude by all measures (PLA: p<0.05, PAV: p<0.001, PAA: p<0.001, MPS95: p<0.01). Lateral impacts also had significantly higher magnitudes than Rearward impacts by all measures (PLA: p<0.05, PAV: p<0.001, PAA: p<0.001, MPS95: p<0.001). Athletes in skill positions sustained impacts of significantly higher magnitude than athletes in line positions (PLA: p<0.001, PAV: p=0.06, PAA: p<0.01, MPS95: p=0.015) (Figure 3). Examples of kinematics and FE simulations for median impacts in each category of combined player position and head acceleration direction can be found in Figure 4 and Figure 5, respectively. BMI was significantly higher in athletes playing line positions relative to athletes playing skill positions (p<.001). MPS95 values in the present data were significantly lower than those in a dataset of previously collected collegiate football head impacts that were measured by the MiG2.0 and simulated via the KTH FE head model (p<0.001) (Figure 6).
Figure 3.
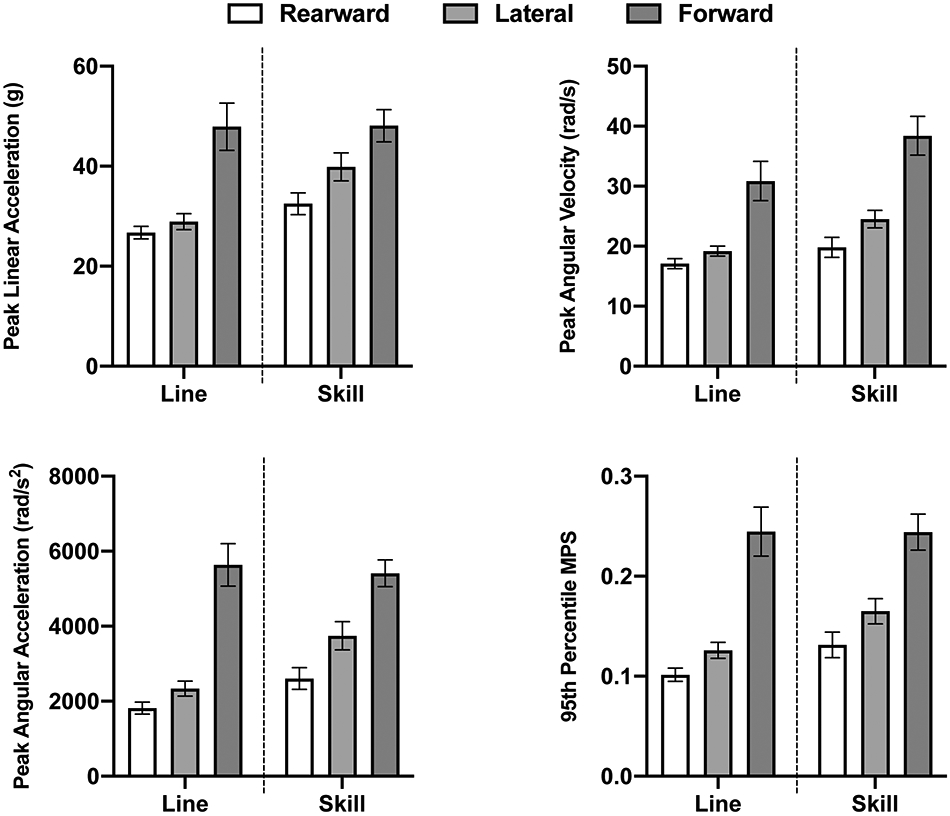
Within-position comparisons of peak head kinematics and 95th percentile maximum principal strain (MPS) between impacts of varying acceleration direction. Error bars represent standard error of the mean.
Figure 4.

Examples of head kinematics and 95% maximum principal strain (MPS) curves for impacts closest to 50th percentile for each category.
Figure 5.

Brain simulations showing 95% maximum principal strain via KTH finite element model. Example images shown are of the median impacts in each combined category of player position (Skill, Line) and head acceleration direction (Rearward, Lateral, Forward).
Figure 6.
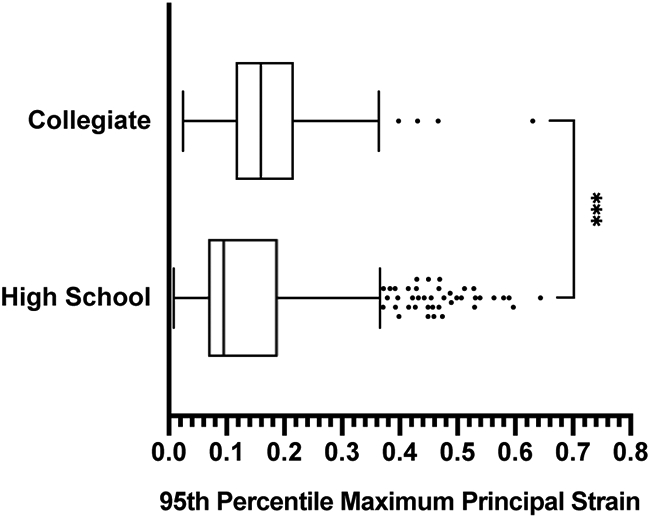
Tukey box plots comparing 95th percentile maximum principal strain between 602 impacts sustained by high school football athletes and 118 impacts sustained by collegiate football athletes. ***p < 0.001.
No significant differences in PLA, PAV, PAA, or MPS95 were found between impacts sustained by athletes wearing the VICIS helmet and the Riddell helmet overall or within any specific direction of head acceleration. Further, no significant differences were found between athletes with and without previous history of concussion, nor between JV and varsity athletes.
Concussion
One athlete sustained a diagnosed concussion while wearing an instrumented mouthguard. Three impacts were detected by the MiG2.0 on the day of the concussion, and the athlete sustained 15 total impacts during the five days leading up to the concussion (including the day of diagnosed injury). Peak head kinematics of these 15 impacts ranged from 6.6 g to 85.9 g PLA, 1.7 rad/s to 44.5 rad/s PAV, and 522.9 rad/s2 to 8160.8 rad/s2 PAA, with median values of 14.2 g PLA, 10.5 rad/s PAV, and 1073.7 rad/s2 PAA. MPS95 and head acceleration direction for all 15 impacts are detailed in Figure 7. This athlete played a line position at the varsity skill level, wore a Riddell Speedflex helmet, and sustained one diagnosed concussion prior to study participation.
Figure 7.
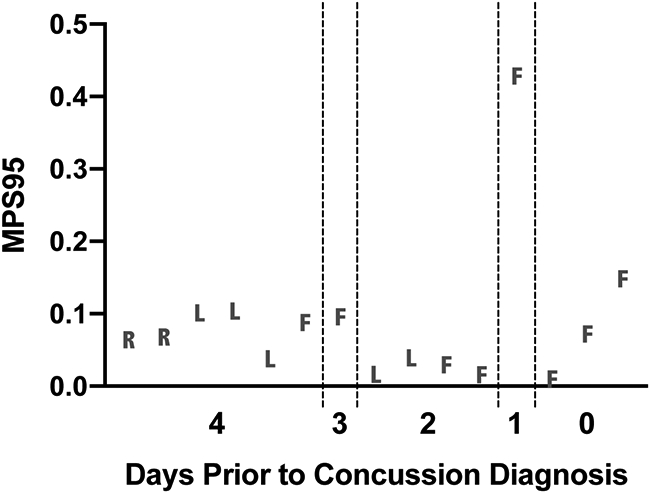
95th percentile maximum principal strain (MPS95) for 15 impacts, in chronological order, leading up to a case of diagnosed concussion. Each point represents an individual impact event. Dotted lines separate consecutive days of American football participation. Impact directions are identified by letter: R = Rearward, L = Lateral, F = Forward. Distance between points on x-axis does not represent time between impacts.
Discussion
Head impact kinematics have been measured extensively in American football by a variety of head impact sensors known to have variable levels of accuracy.33,36 Continued research in this sport, with more accurate measurement technology, is needed to improve our understanding of sport-related brain injury risks and better inform methods of improving athlete brain safety. The present study provides novel information on the range of head kinematics, as measured by the MiG2.0, and brain strain experienced by high school American football players from four different high schools. Further, we detail the relationship of various sport-specific factors to head impact kinematics and brain strain.
Skill position players in the present cohort sustained impacts of higher peak head kinematics and MPS95 than line position players. Higher peak head kinematics have been observed in skill position impacts previously, both at the collegiate and high school levels in studies using the HIT System.11,18,53 Line and skill positions are differentiated by distinct roles and game play scenarios in American football. Line position players tend to be physically larger than skill position players, and such was observed in our cohort via our assessment of athlete BMI. Their playing style relies on power and strength, as line position players play close to the line of scrimmage where their impacts are characterized by close-proximity, square contact with opposing linemen. Skill position players, by contrast, tend to be physically smaller, with a playing style that stresses speed, agility, and ball handling ability. Skill position players do not necessarily directly oppose another specific player at the beginning of plays and typically have ample field space to adjust their trajectory and accelerate, thus leading to impacts of higher velocity.58 Epidemiological studies are in agreement with these findings related to impact magnitude, in that skill position players typically sustain more frequent diagnosed concussions than line position players.21,48 These differences in impact magnitude may be meaningful beyond the risk of concussion, as higher strains in the brain location predominantly associated with pathology of chronic traumatic encephalopathy have been found in skill position impact simulations relative to those of offensive and defensive linemen.62 Due to differences in game play characteristics and injury risks between player positions, the design and implementation of position-specific helmets are of recent interest as a method of improving brain safety in American football.38
Instrumented mouthguards are a useful tool for measuring on-field helmet performance, as some helmet-mounted sensors are limited to specific helmet models or designs. Athletes in our cohort wore a variety of helmets, but the VICIS Zero1 and Riddell Speedflex were by far the most commonly worn and the other helmet models were not worn by a large enough sample to perform any statistical comparisons. We observed no significant differences in on-field helmet performance between the Zero1 and Speedflex helmets. These findings are in contrast to the results of the NFL Helmet Test Protocol in 2018, the first year of our data collection, which ranked the Riddell Speedflex in a lower performance group than the VICIS Zero1.26,65 However, the present results are aligned with both the 2021 NFL helmet test results4,66 and the Virginia Tech STAR helmet ranking system.50,67 Each of these systems rank these two helmets in the same highest performance group (Top-Performing group, 5-STAR). While these findings may seem to suggest that the current NFL and STAR helmet rankings are applicable to high school football, more on-field helmet research with more helmet models at the high school level are needed to assess if this is true. The NFL helmet tests were designed based on NFL concussions4 and have been found to accurately align with concussion incidence in the NFL.3 The Virginia Tech STAR test was based on a large dataset of collegiate football impacts, including concussions, measured via the HIT System.50 Impact velocities at the high school level differ from these two higher levels of play, and it remains unclear if an additional helmet testing protocol specific to high school football may be necessary to accurately predict on-field high school football helmet performance. Regardless, several previous studies have reported on the association of specific helmet models with lower incidence of concussion,3,16,52 which supports future endeavors to design new technologies for impact mitigation1,14 and investigate their performance both on the field and in the laboratory.
Several previous reports of on-field head impacts in American football have reported mixed findings when seeking to determine the relationship between head impact location and head kinematics.9,18,25 In this study, we focused on the direction of head accelerations resulting from impact, rather than head impact location, for several reasons. First, our impacts could not be video reviewed and various algorithms used by head impact sensors to predict head impact location have proven to be highly inaccurate, even in controlled laboratory experiments.13 Second, body impacts are capable of causing head accelerations in contact sports12,54 and these impacts would not have a head location to report. We observed that impacts yielding Forward head accelerations were less frequent but greater in magnitude than Rearward or Lateral impacts. Forward impacts likely included impacts that were primarily to the back of the helmet (which would yield a forward motion of the head), which others have also found to be infrequent relative to other head locations but higher in magnitude.17,18,25 Athletes are often unsuspecting and blind to these impacts, leaving them unprepared to fully brace for incoming contact. Contact between the back of the helmet and the ground is also frequent in cases of diagnosed injury among various player positions.38 Therefore, our findings on impact directionality suggest that American football helmets could be improved by design changes that yield better attenuation of impacts causing head accelerations in the forward direction. Overall, we expect that the direction of peak head accelerations likely coincided with head impact locations such that Rearward, Lateral, and Forward impacts included a high amount of impacts to the front, side, and rear of athlete helmets, respectively, but it should be noted that we observed a very small number of Downward impacts. Though some previous reports have also found that impacts to the top of the helmet are less common than other locations,9,18 we believe the limited ability of the neck to compress under loading and the obliqueness of top impacts likely caused impacts to the top of the helmet to have peak head accelerations pointing in a mixture of the Rearward, Lateral, and Forward directions.
Brain strain, which has been found to be associated with neuropathology30,46 and diagnosed concussion,32,43 was calculated by the KTH FE head model in this study. The deformation of brain tissue varies along different directions, and the maximum principal strain describes the largest deformation of brain tissue among all directions. For each impact event, the 95th percentile of maximum principal strain, rather than the peak maximum principal strain, was calculated in order to avoid extremely high strain values caused by numerical errors. Based on laboratory reconstructions of head impacts in the NFL, a previous study using the KTH FE head model found maximum principal strain thresholds for 50% risk of concussive injury to be 0.26 in the gray matter and 0.21 at the corpus callosum.37 Several impact events from the present cohort were found to yield brain deformation above this threshold, but only one athlete in our cohort sustained a diagnosed concussion during the monitored time period. Interestingly, the final six impacts sustained by this athlete, including all three on the day of diagnosed concussion, were Forward impacts. High magnitude impacts to the back of the helmet have been associated with on-field obvious performance decrements (i.e., visual signs of potential concussive injury after impact) in high school and collegiate football.6 The final impact sustained by this athlete had an MPS95 value of 0.147 (69th percentile of all impacts), but the single impact sustained on the day prior to injury had an MPS95 value of 0.427 (95th percentile of all impacts), which is above the proposed thresholds for 50% risk of injury. Previous work has found that athletes typically sustain impacts of greater magnitude on days of diagnosed concussion than on days without.7 While our data only represent one case of concussion, it is possible that concussion diagnosis was delayed from the suprathreshold event on the day prior to diagnosis or that its mechanical loading contributed to injury diagnosis the next day.
Although we found no differences between JV and varsity high school football athletes, MPS95 was significantly lower in our cohort of high school athletes than in collegiate football players. While this may seem to indicate a greater risk for concussive injury in collegiate athletes than high school athletes, trends opposite to that have previously been reported.23,29 It is possible that, despite the use of the same instrumented mouthguard device in both datasets, this comparison may have been influenced by differences in impact verification methods; the collegiate dataset we compared to was solely comprised of video verified impacts, while our high school dataset relied on the use of a previously validated impact detection algorithm that was developed from a dataset of video verified impacts. However, it should be noted that brain injury mechanisms may vary in developing brains. Therefore, the brain strain threshold proposed from NFL injuries may not be appropriate for predicting brain injury in high school athletes, and potential thresholds for injury may vary between youth, high school, collegiate, and professional athletes. Furthermore, the mechanical properties and the geometry of the developing brain were reported to be different from adults,44 so it will be necessary to develop age-specific FE head models for analysis of adolescent sport-related head impacts.
The present study was not without limitations. This study did not aim to identify factors that influence the frequency of impacts sustained by American football athletes, therefore no conclusions should be drawn from our reported distribution of impact events by skill level, position, or helmet model. Our data collection and processing methods sought to only include events that we could confidently assume were true impacts in the absence of video review. This was largely possible due to our use of MiGNet, a validated neural network classifier of head impact events made specifically for use in American football with the MiG2.0.22 MiGNet has been shown to have very high accuracy in differentiating true and false positive events, but its sensitivity performance suggests that it may have incorrectly excluded several true impacts. Therefore, our use of MiGNet and extra data processing methods likely resulted in an underestimate in head impact frequency. Video review of all recorded events has been previously recommended for identifying impact exposure,47 and would also allow for qualitative descriptions of each impact (e.g., mechanism, helmet location, position, play-style, etc). Further, while the KTH FE head model has been used extensively in previous literature and has been validated by cadaver experiments, various FE head models exist and have been found to provide varying results.24 This limits our ability to accurately compare our findings to others that did not use the KTH FE head model for their calculation of MPS95.
Overall, we find that instrumented mouthguards are useful in identifying which sport-specific factors may or may not be associated with increased severity of head impacts in contact sports. In American football, skill position players are at the greatest risk of sustaining high magnitude impacts. Interventions or helmet design improvements that reduce the incidence or severity of impacts yielding forward head accelerations may be beneficial in reducing cumulative mechanical loading of the brain resulting from high school football participation. More research may be necessary to determine the on-field efficacy of helmets at the high school level relative to collegiate and professional game play.
Acknowledgements
This research was supported by the Taube Stanford Children’s Concussion Initiative, Child Health Research Institute at Stanford, Harman Faculty Scholar Award, the NIH National Institute of Neurological Disorders and Stroke (Grant: R24NS098518), the Pac-12 Conference’s Student-Athlete Health and Well-Being Initiative, and the NIH National Center for Advancing Translational Sciences (Grant: UL1TR003142). We sincerely thank all the coaches, trainers, and players at the participating high schools for their willingness to enroll in these studies.
Footnotes
Conflicts of Interest
The MiG2.0 mouthguard and intellectual property associated with it is owned by Stanford University.
References
- 1.Vahid Alizadeh H, Fanton MG, Domel AG, Grant G, and Camarillo DB. A computational study of liquid shock absorption for prevention of traumatic brain injury. J. Biomech. Eng 143:1–12, 2021. [DOI] [PubMed] [Google Scholar]
- 2.Asken BM, and Rabinovici GD. Identifying degenerative effects of repetitive head trauma with neuroimaging: a clinically-oriented review. Acta Neuropathol. Commun 9:1–17, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bailey AM, McMurry TL, Cormier JM, Funk JR, Crandall JR, Mack CD, Myers BS, and Arbogast KB. Comparison of Laboratory and On-Field Performance of American Football Helmets. Ann. Biomed. Eng 48:2531–2541, 2020. [DOI] [PubMed] [Google Scholar]
- 4.Bailey AM, Sanchez EJ, Park G, Gabler LF, Funk JR, Crandall JR, Wonnacott M, Withnall C, Myers BS, and Arbogast KB. Development and Evaluation of a Test Method for Assessing the Performance of American Football Helmets. Ann. Biomed. Eng 48:2566–2579, 2020. [DOI] [PubMed] [Google Scholar]
- 5.Barber Foss KD, Yuan W, Diekfuss JA, Leach J, Meehan W, DiCesare CA, Solomon G, Schneider DK, MacDonald J, Dudley J, Cortes N, Galloway R, Halstead M, Walker G, and Myer GD. Relative Head Impact Exposure and Brain White Matter Alterations After a Single Season of Competitive Football: A Pilot Comparison of Youth Versus High School Football. Clin. J. Sport Med 29:442–450, 2019. [DOI] [PubMed] [Google Scholar]
- 6.Bartsch AJ, Hedin D, Alberts J, Benzel EC, Cruickshank J, Gray RS, Cameron K, Houston MN, Rooks T, McGinty G, Kozlowski E, Rowson S, Maroon JC, Miele VJ, Ashton JC, Siegmund GP, Shah A, McCrea M, and Stemper B. High Energy Side and Rear American Football Head Impacts Cause Obvious Performance Decrement on Video. Ann. Biomed. Eng 48:2667–2677, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Beckwith JG, Greenwald RM, Chu JJ, Crisco JJ, Rowson S, Duma SM, Broglio SP, McAllister TW, Guskiewicz KM, Mihalik JP, Anderson S, Schnebel B, Brolinson PG, and Collins MW. Head impact exposure sustained by football players on days of diagnosed concussion. Med. Sci. Sports Exerc 45:737–746, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Broglio SP, Eckner JT, and Kutcher JS. Field-based measures of head impacts in high school football athletes. Curr. Opin. Pediatr 24:702–708, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Broglio SP, Sosnoff JJ, Shin SH, He X, Alcaraz C, and Zimmerman J. Head impacts during high school football: A biomechanical assessment. J. Athl. Train 44:342–349, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Broglio SP, Williams RM, O’Connor KL, and Goldstick J. Football players’ head-impact exposure after limiting of full-contact practices. J. Athl. Train 51:511–518, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Campolettano ET, Rowson S, Duma SM, Stemper B, Shah A, Harezlak J, Riggen LD, Mihalik J, Brooks A, Cameron K, Giza CC, McAllister T, Broglio SP, and McCrea M. Factors Affecting Head Impact Exposure in College Football Practices: A Multi-Institutional Study. Ann. Biomed. Eng 47:2086–2093, 2019. [DOI] [PubMed] [Google Scholar]
- 12.Cecchi NJ, Monroe DC, Fote GM, Small SL, and Hicks JW. Head impact exposure and concussion in women’s collegiate club lacrosse. Res. Sport. Med 00:1–6, 2021. [DOI] [PubMed] [Google Scholar]
- 13.Cecchi NJ, Monroe DC, Oros TJ, Small SL, and Hicks JW. Laboratory evaluation of a wearable head impact sensor for use in water polo and land sports. Proc. Inst. Mech. Eng. Part P J. Sport. Eng. Technol 234:162–169, 2020. [Google Scholar]
- 14.Cecchi NJ, Oros TJ, Ringhofer JJ, and Monroe DC. Comparison of head impact attenuation capabilities between a standard American football helmet and novel protective equipment that couples a helmet and shoulder pads. Sport. Eng 22:1–8, 2019. [Google Scholar]
- 15.Champagne AA, Distefano V, Boulanger MM, Magee B, Coverdale NS, Gallucci D, Guskiewicz K, and Cook DJ. Data-informed Intervention Improves Football Technique and Reduces Head Impacts. Med. Sci. Sports Exerc 51:2366–2374, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Collins M, Lovell MR, Iverson GL, Ide T, and Maroon J. Examining concussion rates and return to play in high school football players wearing newer helmet technology: A three-year prospective cohort study. Neurosurgery 58:275–284, 2006. [DOI] [PubMed] [Google Scholar]
- 17.Crisco JJ, Fiore R, Beckwith JG, Chu JJ, Brolinson PG, Duma S, McAllister TW, Duhaime A-C, and Greenwald RM. Frequency and Location of Head Impact Exposures in Individual Collegiate Football Players. J. Athl. Train 45:549–559, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Crisco JJ, Wilcox BJ, Beckwith JG, Chu JJ, Duhaime AC, Rowson S, Duma SM, Maerlender AC, McAllister TW, and Greenwald RM. Head impact exposure in collegiate football players. J. Biomech 44:2673–2678, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Davenport EM, Apkarian K, Whitlow CT, Urban JE, Jensen JH, Szuch E, Espeland MA, Jung Y, Rosenbaum DA, Gioia GA, Powers AK, Stitzel JD, and Maldjian JA. Abnormalities in diffusional kurtosis metrics related to head impact exposure in a season of high school varsity football. J. Neurotrauma 33:2133–2146, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Davenport EM, Whitlow CT, Urban JE, Espeland MA, Jung Y, Rosenbaum DA, Gioia GA, Powers AK, Stitzel JD, and Maldjian JA. Abnormal white matter integrity related to head impact exposure in a season of high school varsity football. J. Neurotrauma 31:1617–1624, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dick R, Ferrara MS, Agel J, Courson R, Marshall SW, Hanley MJ, and Reifsteck F. Descriptive Epidemiology of Collegiate Men’s Football Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 Through 2003–2004. J. Athl. Train 42:221, 2007. [PMC free article] [PubMed] [Google Scholar]
- 22.Domel AG, Raymond SJ, Giordano C, Liu Y, Yousefsani SA, Fanton M, Cecchi NJ, Vovk O, Pirozzi I, Kight A, Avery B, Boumis A, Fetters T, Jandu S, Mehring WM, Monga S, Mouchawar N, Rangel I, Rice E, Roy P, Sami S, Singh H, Wu L, Kuo C, Zeineh M, Grant G, and Camarillo DB. A new open-access platform for measuring and sharing mTBI data. Sci. Rep 11:1–10, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dompier TP, Kerr ZY, Marshall SW, Hainline B, Snook EM, Hayden R, and Simon JE. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 169:659–665, 2015. [DOI] [PubMed] [Google Scholar]
- 24.Fahlstedt M, Abayazid F, Panzer MB, Trotta A, Zhao W, Ghajari M, Gilchrist MD, Ji S, Kleiven S, Li X, Annaidh AN, and Halldin P. Ranking and Rating Bicycle Helmet Safety Performance in Oblique Impacts Using Eight Different Brain Injury Models. Ann. Biomed. Eng. 2021 493 49:1097–1109, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fukuda T, Koike S, Miyakawa S, Fujiya H, and Yamamoto Y. Magnitude and frequency of head impact among university American football players. J. Phys. Fit. Sport. Med 8:1–13, 2019. [Google Scholar]
- 26.Funk J, Crandall J, Wonnacott M, and Withnall C. NFL Linear Impactor Helmet Test Protocol. , 2019. [Google Scholar]
- 27.Gabler LF, Huddleston SH, Dau NZ, Lessley DJ, Arbogast KB, Thompson X, Resch JE, and Crandall JR. On-Field Performance of an Instrumented Mouthguard for Detecting Head Impacts in American Football. Ann. Biomed. Eng 48:2599–2612, 2020. [DOI] [PubMed] [Google Scholar]
- 28.Ghazi K, Wu S, Zhao W, and Ji S. Instantaneous Whole-Brain Strain Estimation in Dynamic Head Impactdoi: 10.1089/neu.2020.7281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Guskiewicz KM, Weaver NL, Padua DA, and Garrett WE. Epidemiology of concussion in collegiate and high school football players. Am. J. Sports Med 28:643–650, 2000. [DOI] [PubMed] [Google Scholar]
- 30.Hajiaghamemar M, and Margulies SS. Multi-Scale White Matter Tract Embedded Brain Finite Element Model Predicts the Location of Traumatic Diffuse Axonal Injury. J. Neurotrauma 38:144–157, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hardy WN, Foster CD, Mason MJ, Yang KH, King AI, and Tashman S. Investigation of Head Injury Mechanisms Using Neutral Density Technology and High-Speed Biplanar X-ray. SAE Tech. Pap , 2001.doi: 10.4271/2001-22-0016 [DOI] [PubMed] [Google Scholar]
- 32.Hernandez F, Wu LC, Yip MC, Laksari K, Hoffman AR, Lopez JR, Grant GA, Kleiven S, and Camarillo DB. Six Degree-of-Freedom Measurements of Human Mild Traumatic Brain Injury. Ann. Biomed. Eng 43:1918–1934, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jadischke R, Viano DC, Dau N, King AI, and McCarthy J. On the accuracy of the head impact telemetry (hit) system used in football helmets. J. Biomech 46:2310–2315, 2013. [DOI] [PubMed] [Google Scholar]
- 34.Joseph JR, Swallow JS, Willsey K, Almeida AA, Lorincz MT, Fraumann RK, Oppenlander ME, Szerlip NJ, and Broglio SP. Pupillary changes after clinically asymptomatic high-acceleration head impacts in high school football athletes. J. Neurosurg 133:1886–1891, 2019. [DOI] [PubMed] [Google Scholar]
- 35.Joseph JR, Swallow JS, Willsey K, Lapointe AP, Khalatbari S, Korley FK, Oppenlander ME, Park P, Szerlip NJ, and Broglio SP. Elevated markers of brain injury as a result of clinically asymptomatic high-acceleration head impacts in high-school football athletes. J. Neurosurg 130:1642–1648, 2019. [DOI] [PubMed] [Google Scholar]
- 36.Kieffer EE, Begonia MT, Tyson AM, and Rowson S. A Two-Phased Approach to Quantifying Head Impact Sensor Accuracy: In-Laboratory and On-Field Assessments. Ann. Biomed. Eng 48:2613–2625, 2020. [DOI] [PubMed] [Google Scholar]
- 37.Kleiven S Predictors for Traumatic Brain Injuries Evaluated through Accident Reconstructions. Stapp Car Crash J. 51:, 2007. [DOI] [PubMed] [Google Scholar]
- 38.Lessley DJ, Kent RW, Cormier JM, Sherwood CP, Funk JR, Crandall JR, Myers BS, and Arbogast KB. Position-Specific Circumstances of Concussions in the NFL: Toward the Development of Position-Specific Helmets. Ann. Biomed. Eng 48:2542–2554, 2020. [DOI] [PubMed] [Google Scholar]
- 39.Liu Y, Domel AG, Cecchi NJ, Rice E, Callan AA, Raymond SJ, Zhou Z, Zhan X, Li Y, Zeineh M, Grant G, and Camarillo DB. Time Window of Head Impact Kinematics Measurement for Calculation of Brain Strain and Strain Rate in American Football. Ann Biomed Eng. 2021. [DOI] [PubMed] [Google Scholar]
- 40.Liu Y, Domel AG, Yousefsani SA, Kondic J, Grant G, Zeineh M, and Camarillo DB. Validation and Comparison of Instrumented Mouthguards for Measuring Head Kinematics and Assessing Brain Deformation in Football Impacts. Ann. Biomed. Eng 48:2580–2598, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Macy JT, Kercher K, Steinfeldt JA, and Kawata K. Fewer US Adolescents Playing Football and Public Health: A Review of Measures to Improve Safety and an Analysis of Gaps in the Literature. Public Health Rep. 00:1–13, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Marar M, McIlvain NM, Fields SK, and Comstock RD. Epidemiology of concussions among united states high school athletes in 20 sports. Am. J. Sports Med 40:747–755, 2012. [DOI] [PubMed] [Google Scholar]
- 43.McAllister TW, Ford JC, Ji S, Beckwith JG, Flashman LA, Paulsen K, and Greenwald RM. Maximum principal strain and strain rate associated with concussion diagnosis correlates with changes in corpus callosum white matter indices. Ann. Biomed. Eng 40:127–140, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.McIlvain G, Schwarb H, Cohen NJ, Telzer EH, and Johnson CL. Mechanical properties of the in vivo adolescent human brain. Dev. Cogn. Neurosci 34:27–33, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Montenigro PH, Alosco ML, Martin BM, Daneshvar DH, Mez J, Chaisson CE, Nowinski CJ, Au R, McKee AC, Cantu RC, McClean MD, Stern RA, and Tripodis Y. Cumulative Head Impact Exposure Predicts Later-Life Depression, Apathy, Executive Dysfunction, and Cognitive Impairment in Former High School and College Football Players. J. Neurotrauma 34:328–340, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.O’Keeffe E, Kelly E, Liu Y, Giordano C, Wallace E, Hynes M, Tiernan S, Meagher A, Greene C, Hughes S, Burke T, Kealy J, Doyle N, Hay A, Farrell M, Grant GA, Friedman A, Veksler R, Molloy MG, Meaney JF, Pender N, Camarillo D, Doherty CP, and Campbell M. Dynamic Blood-Brain Barrier Regulation in Mild Traumatic Brain Injury. J. Neurotrauma 37:347–356, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Patton DA, Huber CM, Jain D, Myers RK, McDonald CC, Margulies SS, Master CL, and Arbogast KB. Head Impact Sensor Studies In Sports: A Systematic Review Of Exposure Confirmation Methods. Ann. Biomed. Eng 48:2497–2507, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Pellman EI, Powell JW, Viano DC, Casson IR, Tucker AM, Feuer H, Lovell M, Waeckerle JF, Robertson DW, Kelly DF, Maroon JC, Valadka AB, Ozgur B, Levy ML, and Bailes JE. Concussion in Professional Football: Epidemiological Features of Game Injuries and Review of the Literature - Part 3. Neurosurgery 54:81–96, 2004. [DOI] [PubMed] [Google Scholar]
- 49.Robinson ME, Shenk TE, Breedlove EL, Leverenz LJ, Nauman EA, and Talavage TM. The role of location of subconcussive head impacts in fMRI brain activation change. Dev. Neuropsychol 40:74–79, 2015. [DOI] [PubMed] [Google Scholar]
- 50.Rowson S, and Duma SM. Development of the STAR evaluation system for football helmets: Integrating player head impact exposure and risk of concussion. Ann. Biomed. Eng 39:2130–2140, 2011. [DOI] [PubMed] [Google Scholar]
- 51.Rowson S, and Duma SM. Brain injury prediction: Assessing the combined probability of concussion using linear and rotational head acceleration. Ann. Biomed. Eng 41:873–882, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Rowson S, Duma SM, Greenwald RM, Beckwith JG, Chu JJ, Guskiewicz KM, Mihalik JP, Crisco JJ, Wilcox BJ, Mcallister TW, Maerlender AC, Broglio SP, Schnebel B, Anderson S, and Brolinson PG. Can helmet design reduce the risk of concussion in football? Technical note. J. Neurosurg 120:919–922, 2014. [DOI] [PubMed] [Google Scholar]
- 53.Schnebel B, Gwin JT, Anderson S, and Gatlin R. In vivo study of head impacts in football: A comparison of National Collegiate Athletic Association Division I versus high school impacts. Neurosurgery 60:490–495, 2007. [DOI] [PubMed] [Google Scholar]
- 54.Smith TA, Halstead PD, McCalley E, Kebschull SA, Halstead S, and Killeffer J. Angular head motion with and without head contact: implications for brain injury. Sport. Eng 18:165–175, 2015. [Google Scholar]
- 55.Swartz EE, Broglio SP, Cook SB, Cantu RC, Ferrara MS, Guskiewicz KM, and Myers JL. Early results of a helmetless-tackling intervention to decrease head impacts in football players. J. Athl. Train 50:1219–1222, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Swartz EE, Myers JL, Cook SB, Guskiewicz KM, Ferrara MS, Cantu RC, Chang H, and Broglio SP. A helmetless-tackling intervention in American football for decreasing head impact exposure: A randomized controlled trial. J. Sci. Med. Sport 22:1102–1107, 2019. [DOI] [PubMed] [Google Scholar]
- 57.Wu LC, Kuo C, Loza J, Kurt M, Laksari K, Yanez LZ, Senif D, Anderson SC, Miller LE, Urban JE, Stitzel JD, and Camarillo DB. Detection of American Football Head Impacts Using Biomechanical Features and Support Vector Machine Classification. Sci. Rep 8:1–14, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Zanetti K, Post A, Karton C, Kendall M, Hoshizaki TB, and Gilchrist MD. Identifying injury characteristics for three player positions in American football using physical and finite element modeling reconstructions. 2013 IRCOBI Conf. Proc. - Int. Res. Counc. Biomech. Inj. 525–535, 2013. [Google Scholar]
- 59.Zhan X, Li Y, Liu Y, Domel AG, Alizadeh HV, Raymond SJ, Ruan J, Barbat S, Tiernan S, Gevaert O, Zeineh MM, Grant GA, and Camarillo DB. The relationship between brain injury criteria and brain strain across different types of head impacts can be different. J. R. Soc. Interface 18:20210260, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Zhan X, Liu Y, Raymond SJ, Vahid Alizadeh H, Domel A, Gevaert O, Zeineh M, Grant G, and Camarillo DB. Rapid Estimation of Entire Brain Strain Using Deep Learning Models. IEEE Trans. Biomed. Eng , 2021.doi: 10.1109/TBME.2021.3073380 [DOI] [PubMed] [Google Scholar]
- 61.Zhou Z, Li X, Kleiven S, Shah CS, and Hardy WN. A Reanalysis of Experimental Brain Strain Data: Implication for Finite Element Head Model Validation. Stapp Car Crash J. 62:293–318, 2018. [DOI] [PubMed] [Google Scholar]
- 62.Zimmerman KA, Kim J, Karton C, Lochhead L, Sharp DJ, Hoshizaki T, and Ghajari M. Player position in American football influences the magnitude of mechanical strains produced in the location of chronic traumatic encephalopathy pathology: A computational modelling study. J. Biomech 118:110256, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Zonner SW, Ejima K, Bevilacqua ZW, Huibregtse ME, Charleston C, Fulgar C, and Kawata K. Association of increased serum S100B levels with high school football subconcussive head impacts. Front. Neurol 10:1–10, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Zonner SW, Ejima K, Fulgar CC, Charleston CN, Huibregtse ME, Bevilacqua ZW, and Kawata K. Oculomotor Response to Cumulative Subconcussive Head Impacts in US High School Football Players: A Pilot Longitudinal Study. JAMA Ophthalmol. 137:265–270, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.2018 Helmet Laboratory Testing Performance Results <https://www.nfl.com/playerhealthandsafety/equipment-and-innovation/equipment-testing/2018-helmet-laboratory-testing-performance-results>. Accessed July 5, 2021.
- 66.2021 Helmet Laboratory Testing Performance Results <https://www.nfl.com/playerhealthandsafety/equipment-and-innovation/equipment-testing/helmet-laboratory-testing-performance-results>. Accessed July 5, 2021.
- 67.Varsity Football Helmet Ratings <https://helmet.beam.vt.edu/varsity-football-helmet-ratings.html>. Accessed July 5, 2021.