

Abstract
Background Although information and communication technologies (ICT) are becoming more common among health care providers, there is little evidence on how ICT can support health care aides. Health care aides, also known as personal care workers, are unlicensed service providers who encompass the second largest workforce, next to nurses, that provide care to older adults in Canada.
Objective The purpose of this literature review is to examine the range and extent of barriers and benefits of ICT used by health care workers to manage and coordinate the care-delivery workflow for their clients.
Methods We conducted a literature review to examine the range and extent of ICT used by health care aides to manage and coordinate their care delivery, workflow, and activities. We identified 8,958 studies of which 40 were included for descriptive analyses.
Results We distinguished the following five different purposes for the use and implementation of ICT by health care aides: (1) improve everyday work, (2) access electronic health records for home care, (3) facilitate client assessment and care planning, (4) enhance communication, and (5) provide care remotely. We identified 128 barriers and 130 benefits related to adopting ICT. Most of the barriers referred to incomplete hardware and software features, time-consuming ICT adoption, heavy or increased workloads, perceived lack of usefulness of ICT, cost or budget restrictions, security and privacy concerns, and lack of integration with technologies. The benefits for health care aides' adoption of ICT were improvements in communication, support to workflows and processes, improvements in resource planning and health care aides' services, and improvements in access to information and documentation.
Conclusion Health care aides are an essential part of the health care system. They provide one-on-one care to their clients in everyday tasks. Despite the scarce information related to health care aides, we identified many benefits of ICT adoption.
Keywords: information technology, delivery of health care, health personnel, workflow, aged
Background and Significance
The world's aging population is growing at a significant rate. 1 Globally, a higher increase is noted among individuals aged 65 years and older compared with other age groups. 2 In addition, with advancing age, the risk of developing chronic diseases, such as depression and dementia, becomes higher. 3 All of these combined represent significant challenges for health care systems and providers.
In Canada, health care providers, such as health care aides and personal support workers, provide direct care for the elderly, ill, or persons who require assistance with their activities of daily living and multiple tasks in different settings. 4 5 6 7 These tasks may include self-care, medication management, social interactions, 8 9 emotional support, meal preparation, companionship, socialization, and housekeeping, 10 all while under the supervision of regulated nursing staff or other health professionals. 11 12
Although health care aides are unlicensed support personnel, they comprise the second largest workforce within the health care sector, 13 next to nurses, providing 80% of the direct care to Canadian seniors. 8 9 The situation regarding professional regulation for this group of health care workers is similar between the United States, 14 Canada, 15 and Europe, such that the regulation may vary from one country to another. 16 Depending on the location, this workforce is recognized by different names, 8 including personal support workers, personal care attendants, long-term care aides, resident care workers, nursing aides, nursing assistants, health care assistants, and care aides. 8 9 11 16 17 18 For this study, we will refer to them as health care aides.
The population of health care aides is difficult to estimate. 19 The exact size of the health care aide workforce in Canada is unknown since many are on a contractually, part-time or on-call basis. Most of these workers are women. 18 20 21 The shortage of health care aides in Canada and several high-income countries around the world will continue to grow as the world's senior population is expected to increase in the upcoming years. 8 16 22 23 24 25 26 The necessity for more health care providers is a concern, not unique to Canada. Health care aides are an essential component for the health care sector. 8 16 27 28
These workers are vital for high quality care in continuing care facilities, 12 29 including home care, supportive living, and long-term care. 11 12 29 However, they do not work under a standardized scope of practice. 7 18 Instead, their duties are assigned depending on the employer, work setting, and client needs. 5 9 10 11
Information and communication technologies (ICT) has created numerous avenues for advocating and promoting health care delivery among various age groups. ICT represent an enormous opportunity to improve health care by providing quality, accessibility, and affordability for multiple users. 30 31 32 Current technologies within the scope of practice of nurses 33 and unlicensed health care aides, include telemonitoring and care delivering mobile application. 15 34 35
ICT implementation and adoption are key and beneficial to assist health care aides' workflows and activities. 36 37 Existing supporting health care tools can potentially provide a range of applications and platforms to facilitate health care aides' assignments, 38 transmit observations, and enhance communication between families, clients, and health care providers within the ecosystem of care. 39 ICT can help to deliver real-time support and keep clients' information confidential and available, 40 41 and ultimately improve caring activities and health care delivery. 37
Despite the various technology-based interventions that exist, none have been designed with health care aides in mind or intended to support their workflows. 37 For example, Steele Gray et al 42 found that ICT for health care aides are inefficient and often do not fit their workflows. Also, Sterling et al 37 described how health care aides consistently identified existing ICT as outdated and ineffective; and not convenient for their needs, they suggested that current technologies exacerbate health care aides' existing communication challenges by not allowing real-time communication with different health care provides.
The existing evidence suggests that health care aides face multiple challenges to access and share patient information 15 37 and communicate with other health care providers. 43 This has a negative impact on their ability to care for their clients. 15 Saari et al 15 identified technology as having the ability to facilitate effective communication and address information gaps for health care aides. Consequently, opportunities for ICT intended for health care aides include features of portability, 44 ubiquity, 45 interoperability, 46 communication tools to assist care plans, 43 and integration with remote care, telemonitoring, and assistive technologies. 36
To our knowledge, no comprehensive review has studied the range and extent of ICT used by health care aides to support their workflows and practice. Likewise, it is important to understand the barriers and benefits of implementation and adoption of ICT by health care aides. This understanding can inform the design, implementation, and adoption of future technologies and tools, since the role of health care aides is becoming more important, as they provide direct care to clients.
Objectives
To date, there is little evidence on how ICT can support health care aides' workflow and practice as the barriers and benefits of ICT use and adoption remain unknown. The purpose of this literature review is to examine the range and extent of barriers and benefits of ICT used by health care aides to manage and coordinate the care-delivery workflow for their clients.
Methods
We conducted a literature review based on Daudt et al, 47 modifications of the methodology by Arksey and O'Malley. 47 48 This methodology followed six steps: (1) determine the research questions following the PICOS (population, intervention, comparison, outcome, and study design) framework, (2) identify the relevant studies, (3) study selection, (4) chart data, (5) collect and summarize, and (6) report the results. Modification made by Daudt et al 47 of this methodology includes an interprofessional team in step (2) and use a three-tiered approach to cross-check and select the articles in step (3). 47 49
Data Sources and Search Strategy
We examined peer-reviewed literature published between January 2010 and March 2020, considering the past 10 years of technology development. We searched three academic databases: Medline, EMBASE, and CINAHL. We defined the search strategy in collaboration with an expert subject expert librarian. Then, we formulated and followed two main concepts to extract relevant studies from the electronic databases (N.N. and S.M.):
Health care professionals providing care to people who require health-related personal care.
Use of technologies within care.
We combined keywords for the above concepts, thesaurus terms including subject headings and the Medical Subject Headings (MeSH) terms, and free-text words using the Boolean operators of “AND” and “OR” (N.N., S.M., and A.M.C.). In addition, we customized search terms, strategies, and limits for each database (N.N., S.M., and A.M.C). For more details about the search strategy, see Supplementary Table S1 (available in the online version).
Study Selection Process
We exported all studies to EndNote, a reference management software, and removed duplicates (N.N., S.M., and H.P.). Then, we transferred the remaining studies to Covidence, a primary screening and data extraction tool (N.N., S.M., and H.P.). Following, we removed additional duplicates using Covidence or manually as we progressed in the review process (N.N., S.M., H.P., and S.P.). Then, two researchers engaged in the title and abstract screening independently (N.N. and S.M.) where we compared studies with the inclusion and exclusion criteria. We resolved conflicts between the researchers through a discussion where consensus was reached (N.N., S.M., A.M.C., S.P., and H.P.). If a disagreement persisted after the discussion, one senior researcher or domain expert researcher resolved the conflict (N.N., A.M.C., and L.L.).
Next, two researchers assessed the full texts (N.N. and S.M.). A third rater decided if those studies should be included in the data extraction phase if disagreement occurred (A.M.C.). All researchers were thoroughly calibrated and trained on applying the inclusion and exclusion criteria before evaluating studies.
Inclusion Criteria
We included papers that:
Examined the use of ICT primarily by healthcare workers, including health care aides and home care nurses.
Reported ICT intended to assist in providing caregiving services at home.
Were published and available in full text in peer-reviewed journals, doctoral or master's theses, and conference proceedings.
Were published in English.
Exclusion Criteria
We excluded papers that:
Did not report the use of ICT.
Were related to care providers with a professional designation or regulated scope of practice.
Reported ICT that were not intended for caregiving services at home.
Described primary ICT use by someone other than health care aides or home care nurses.
Did not provide enough information to categorize or extract information from.
Were beyond the scope of this literature review.
Were not available in full text or published in peer-reviewed journals, doctoral or master's theses, or conference proceedings.
Data Extraction Process
Three researchers (N.N., S.M., and A.M.C.) extracted data from the selected studies in an Excel spreadsheet file where we operationalized the variables. We reviewed each study in full and extracted data for the areas of interest for this review (N.N., S.M., S.P., H.P., and A.M.C.). Finally, two researchers met regularly during the study extraction phase to discuss differences and reach a consensus (S.M. and N.N.).
Data Analysis
Four researchers conducted the data analysis (S.M., N.N., A.M.C., and H.P.). Due to the diversity of the included articles, we decided to use a qualitative approach, and conducted content analysis on the extracted data. We categorized the studies into the following five main groups according to the purpose of each study. In addition, we calculated descriptive statistics for population, study characteristics, ICT features, barriers, and benefits of ICT. Finally, after several rounds of discussions between the research team, we classified the barriers and benefits that were identified in this review. In Table 1 , we present a detail description of the selected studies including characteristics and ICT features.
Table 1. Characteristics of selected studies classified by study purpose.
| Study purpose | Authors | Age of participants (range) | Gender of participants | Study design | Data collection method | Hardware used | Software used |
|---|---|---|---|---|---|---|---|
| Improve everyday work | Stroulia et al 54 | Not reported | Not reported | Multiple methods | Interviews, focus groups, survey Questionnaire |
Tablet | Application |
| Improve everyday work | Sassen et al 55 | Intervention group mean: 38.6, control group mean: 39.7 | Both genders (mostly female) | Quantitative | Survey Questionnaire |
Laptop | Web based |
| Improve everyday work | Nilsson and Fagerström 56 | Not reported | Not reported | Qualitative | Focus groups | Not reported | Not reported |
| Improve everyday work | Lexis et al 61 | Not reported | Female | Quantitative | Survey Questionnaire |
Desk computer | Web based |
| Improve everyday work | Kaunda-Khangamwa et al 52 | Not reported | Not reported | Qualitative | Interviews | Phone | Text messaging |
| Improve everyday work | Gund et al 57 | 38–56; mean = 48 | Not reported | Multiple methods | Interviews | Desk computer | Web based |
| Improve everyday work | Gars and Skov 53 | Not reported | Not reported | Qualitative | Focus groups, observations | Tablet | Application |
| Improve everyday work | Danilovich et al 60 | Not reported | Female | Qualitative | Interviews, Focus groups |
Tablet | Application |
| Improve everyday work | Brown et al 51 | Mean of case managers = 36.4 | Both genders | Multiple methods | Focus groups, survey Questionnaire |
Tablet and computer | Web based and application |
| Improve everyday work | Andersen et al 58 | High strain mean: 47.9, low and moderate strain mean: 37.9 | Both genders (90% female) | Quantitative | Survey Questionnaire |
Phone | Web based |
| Improve everyday work | Alhuwail and Koru 59 | 30– > 51 | Not reported | Qualitative | Interviews, Focus groups |
Tablet | Application |
| Improve everyday work | Alhuwail and Koru 46 | 30– > 52 | Not reported | Qualitative | Interviews, Focus groups, observations |
Not reported | Not reported |
| Access electronic health records for home care | Yang et al 63 | 25–47 | Both genders (mostly female) | Qualitative | Observations | Laptop | Web based |
| Access electronic health records for home care | Westra et al 62 | Not reported | Not reported | Quantitative | Not reported | Not reported | Web based |
| Access electronic health records for home care | Tapper et al 64 | Not reported | Not reported | Quantitative | Survey Questionnaire |
Tablet | Web based |
| Access electronic health records for home care | Sockolow et al 65 | Median age = 49 years | Both genders (88% female) | Mixed methods | Retrospective | Laptop | Application |
| Access electronic health records for home care | Han et al 66 | Not reported | Not reported | Qualitative | Interviews | Not reported | Not reported |
| Access electronic health records for home care | Gjevjon and Hellesø 67 | Not reported | Not reported | Quantitative | Secondary analysis | Desk computer | Web based |
| Access electronic health records for home care | De Vliegher et al 69 | Not reported | Not reported | Qualitative | Interviews, focus groups | Desk computer | Web based |
| Access electronic health records for home care | Bercovitz et al 68 | Not reported | Not reported | Not applicable | Not applicable | Desk computer | Web based |
| Access electronic health records for home care | Alhuwail et al 70 | 30–51 | Not reported | Quantitative | Interviews, Focus groups, observations |
Desk computer | Web based |
| Facilitate client assessment and care planning | Vasalampi 71 | 28–63 | Female | Quantitative | Survey Questionnaire |
Tablet | Web based |
| Facilitate client assessment and care planning | Stutzel et al 75 | Not reported | Not reported | Multiple methods | Focus groups, observations, survey Questionnaire |
Phone and tablet | Application and web based |
| Facilitate client assessment and care planning | Santi et al 72 | Not reported | Not reported | Multiple methods | Survey Questionnaire |
Not reported | Not reported |
| Facilitate client assessment and care planning | Göransson et al 73 | 28–59; mean = 47 | Female | Qualitative | Interviews, focus groups | Phone and tablet | Web based |
| Facilitate client assessment and care planning | Farsjø et al 76 | 23–65; mean = 43 | Both genders (mostly female) | Qualitative | Interviews | Tablet | Application |
| Facilitate client assessment and care planning | Dowding et al 79 | 29–66; mean = 48 | Both genders (mostly female) | Qualitative | Focus groups | Tablet | Web based |
| Facilitate client assessment and care planning | Dean et al., 2016 74 | Not reported | Not reported | Quantitative | Secondary analysis | Phone | Web based |
| Facilitate client assessment and care planning | Bastide et al 77 | Not reported | Not reported | Not applicable | Not applicable | Desk computer | Web based |
| Facilitate client assessment and care planning | Arbaje et al 78 | Not reported | Not reported | Qualitative | Interviews, observations | Desk computer | Web based |
| Enhance communication | Petersen et al 40 | Not reported | Both genders (mostly female) | Qualitative | Focus groups, observations | Desk computer | Web based |
| Enhance communication | Lyngstad et al 81 | Intervention group: 38.6–40.5 (mean = 39.6) Control group: 38.4–40.4 (mean = 39.4) |
Both genders (mostly female) | Quantitative | Survey Questionnaire |
Desk computer | Web based |
| Enhance communication | Lyngstad and Hellesø 80 | Intervention group: 38.6–40.5 (mean = 39.6) Control group: 38.4–40.4 (mean = 39.4) |
Both genders (mostly female) | Quantitative | Survey Questionnaire |
Desk computer | Web based |
| Enhance communication | Lindberg et al 101 | Not reported | Not reported | Systematic review | Not applicable | Tablet and laptop | Web based and application |
| Enhance communication | Gentles et al 82 | Not reported | Not reported | Scoping review | Not applicable | Computer and phone | Web based and phone based |
| Enhance communication | Chiang and Wang 2 | 27–54 | Female | Qualitative | Interviews | Phone | Application |
| Enhance communication | Bossen et al 83 | 30–75 | Both genders | Qualitative | Interviews, observations, focus groups | Tablet and computer | Web based |
| Provide care remotely | Mangwi Ayiasi et al 84 | Not reported | Not reported | Quantitative | Survey Questionnaire |
Phone | Application |
| Provide care remotely | Little et al 85 | Not reported | Not reported | Qualitative | Observations | Phone | Application |
| Provide care remotely | Katalinic et al 35 | Not reported | Not reported | Quantitative | Survey Questionnaire |
Tablet | Application |
Results
Study Selection
Fig. 1 shows the scholarly literature article search results. In the initial search, we identified 8,958 studies from academic databases. After the removal of 1,065 duplicates, 7,893 publications entered in the selection process. The agreement level between raters 50 during the title and abstract phase and the full-text screening phase was high, with a 95.57% level of agreement for the abstracts and 84.71% for the full papers.
Fig. 1.

Scholarly literature article search results. ICT, information and communication technologies.
Most selected studies were conducted in the United States (30%, 12/40), Sweden (12.5%, 5/40), and Norway (12.5%, 5/40). The remaining studies were conducted across nine other countries. Half of the studies were published from 2010 to 2015 and a half after 2015 ( Supplementary Figs. S1 and S2 , available in the online version).
Fig. 2.

Distribution of barriers reported in the selected studies.
Characteristics of the Research Conducted
Population
Of the total included studies, 38 (97.5%) did not use the term “health care aide” or “personal support worker” to refer to the health care workers. However, we considered these studies as they were conducted within samples with a similar scope of practice. Also, most studies did not report the age of their participants. For that reason, it was not possible to extract this information. Also, 24 (60%) studies did not report participant gender or sex. Only 11 (27.5%) studies reported male and female participants, and 5 (12.5%) reported only female participants.
Study Design
Most studies were qualitative ( n = 17, 42.5%) and quantitative ( n = 13, 32.5%), with a smaller proportion of studies that included multiple ( n = 5, 12.5%) or mixed-method designs ( n = 1, 2.5%). One systematic review and one literature review were also included. Two studies did not report their study designs. We extracted 53 data collection methods from the selected studies, as some authors used multiple methods. For that reason, this denominator is not adding up to the total number of selected studies.
We found five different types of data collection techniques: interviews ( n = 14, 26.4%), focus groups ( n = 13, 24.5%), survey/questionnaires ( n = 12, 24.5%), observation ( n = 9, 17%) and one for workshops; and two different types of data analyses: secondary analysis ( n = 3, 5.6%) and retrospective analysis ( n = 1, 1.8%). We present a summary of study designs and data collection methods in Supplementary Table S2 (available in the online version).
Study Purpose
We classified the selected studies in five groups, according to the main purpose of ICT use by health care aides: (1) improve everyday work ( n = 12, 30%), 46 51 52 53 54 55 56 57 58 59 60 61 (2) access electronic health records for home care ( n = 9, 22.5%), 62 63 64 65 66 67 68 69 70 (3) facilitate client assessment and care planning ( n = 9, 22.5%), 71 72 73 74 75 76 77 78 79 (4) enhance communication ( n = 7, 17.5%), 2 40 80 81 82 83 and (5) provide care remotely ( n = 3, 7.5%). 35 84 85
Features of the Reported Information and Communication Technologies
In Table 1 , we report our findings regarding the hardware and software used in the ICT referred in the selected studies. Desk computers were the most used form of hardware ( n = 11, 27.5%), followed by electronic tablets ( n = 9, 22.5%), mobile phones ( n = 6, 15%), and laptops ( n = 3, 7.5%). Some studies reported a combination of hardware between tablets and desk computers ( n = 2, 5%), tablets and mobile phones ( n = 2, 5%), tablets and laptops ( n = 1, 2.5%), or desk computers and mobile phones ( n = 1, 2.5%). Five studies (12.5%) did not report the type of hardware used.
Regarding software, most studies used a web-based platform ( n = 21, 52.5%), followed by mobile applications ( n = 10, 25%). A few studies used mobile applications and a web-based platform ( n = 4, 10%). One study (2.5%) reported a text messaging technology, and four studies (10%) did not report the type of software.
Barriers and Benefits Identified in Adopting Information and Communication Technologies by Health Care Aides
In this section, we present the information regarding barriers and benefits of ICT used by health care aides.
Barriers
Several studies have explored the barriers of ICT implementation and adoption for various health care professionals. 45 86 87 88 89 90 91 92 93 94 95 Still, the evidence of ICT related barriers for health care aides is limited. The concept of barriers is associated with attitudes, education, training, and limitations for the adoption and use of ICT. 92 Barriers vary, and there is a need to address them to implement ICT. 86 In the literature, the evidence reports that barriers could be related but not limited to inadequate access to useful, relevant, and appropriate hardware and software when implementing ICT. 94 ICT barriers have been observed from the technology, organizational, socioeconomic, and ethical perspectives. 96
In Fig. 2 , we present a list of the barriers we identified for the adoption and implementation of ICT for health care aides. In Supplementary Table S3 (available in the online version), we include an entire list of barriers category, frequency, and the corresponding studies.
In this review, we found 128 barriers related to the adoption and use of ICT by health care aides. The overarching categories were as follows: (1) incomplete hardware and software features, (2) time-consuming ICT adoption, (3) heavy or increased workloads, (4) perceived lack of usefulness of the ICT, (5) cost or budget restrictions, (6) security and privacy concerns, (7) lack of collaboration and integration with current technologies, (8) data quality or validity and communication issues, (9) technical support, and (10) related to the provider–client relationship.
In the group of barriers related to hardware and software, we found that users reported system malfunctions, poor design, and issues regarding software configuration. 35 40 46 63 66 67 70 71 85 In these studies, the software did not reflect users' needs and expectations or did not support their information needs. 70 Some studies described the lack of documentation features. 35 46 65 70 72 In addition to usability issues, 59 we found connectivity issues, as a significant hardware barrier in this group. 56 64 71 84 Some studies reported incomplete hardware features as a significant barrier to adopting and implementing ICT. 56 65 77 86
Time-consuming adoption and implementation was another significant barrier for health care aides, 2 35 40 51 53 55 56 59 63 64 65 85 This further amplifies the need for communication with ICT providers in order for an effective ICT solution. 71 72 76 In some studies, users reported the ICT implementation process as time consuming. 40 52 53 63 64 65 85 A few studies described the lack of time for documentation between clients and providers as a significant barrier. 53 These groups of studies reported that ICT required more time from health care aides. 2 51 56 Likewise, we found that users referred to ICT as a waste of time, particularly during the documentation process.
Studies presenting barriers related to heavy or increased workloads 40 52 55 59 69 71 72 73 83 argued that users perceived a growth in daily workloads due to the use and implementation of ICT. For example, Petersen et al 40 reported problematic ICT use due to report writing taking precedence over the care of their patients. Heavy workload of health care aides was referred as a major barrier of adoption and implementation of new ICT. 71 72
Other studies on the usefulness of ICT, 55 57 58 64 70 71 74 suggesting that ICT did not meet health care aides' needs 64 or represent an immediate advantage. 55 Another significant barrier we found was the associated cost or budget restriction. 35 52 57 64 76 A few studies referred to concerns such as return on investment, 64 licensing and purchasing costs, 35 and financial restrictions to implement or accept the ICT solution. 76
Security and privacy concerns were also highlighted as significant barriers to ICT adoption by health care aides. 2 40 60 72 77 In some studies, users perceived risk regarding their information being leaked, stolen, 2 60 or tracked by malicious users. 77 Other studies highlighted the privacy of information on the devices as an issue. 40
We found barriers associated with the lack of collaboration and integration with current technologies 57 59 68 71 and existing systems. 35 72 76 Such barriers included lack of technical knowledge or skills for implementing and effectively using ICT, 53 83 concerns about interoperability issues, 64 66 69 validity of information (i.e., incompleteness, errors, and inaccurate information), 73 78 lack of continuity in the use of the ICT solution, 40 76 and limitations in software features and system designs. 57 59
Data quality and validity 40 62 72 and communication issues were also reported 40 81 as barriers. A few studies reported technical support as a major barrier. 56 70 Other ICT were reported as not aligned with actual workflows 56 or posed difficulty for scaled or customized implementation. 35 The lack of technical support and learning or training requirements, as well as limited flexibility, were also described as barriers. 40 Finally, some studies indicated that the provider-client relationship was negatively affected by the implementation of ICT. 63 64 71
In summary, the most predominant barriers related to the ICT for health care aides were related to incomplete or limited software features, 35 40 46 52 63 66 67 70 71 85 time-consuming ICT (i.e., in use, adoption, or implementation), 2 35 40 51 53 55 56 59 63 64 65 85 heavy or increased workloads, 40 52 55 59 69 71 72 73 83 and health care aides perceived ICT as not convenient or a useful solution. 55 57 58 64 70 71 74 83
Benefits
Several authors have documented the benefits of ICT for health care providers. 66 78 85 87 95 97 However, there is little evidence on the benefits of technology for health care aides. Benefits of ICT are described as tangible or perceived outcomes derived from the implementation or adaptation of ICT. 98 99 The benefits of using new ICT are usually described with great positivity. A clear description of the benefits of ICT for health care aides can inform the decision-making process regarding the implementation and adoption of new technologies for health care aides. 36 The evidence suggested that benefits related to ICT for health care aides are consistent between different health care professionals. These benefits are related to improvements in documentation, monitoring, and quality of care, and support to existing workflows and information exchange, and enhancement in communications. 100
In Fig. 3 , we report the distribution of benefits identified for ICT used by health care aides. In Supplementary Table S4 (available in the online version), we present an entire list of the benefits we found.
Fig. 3.
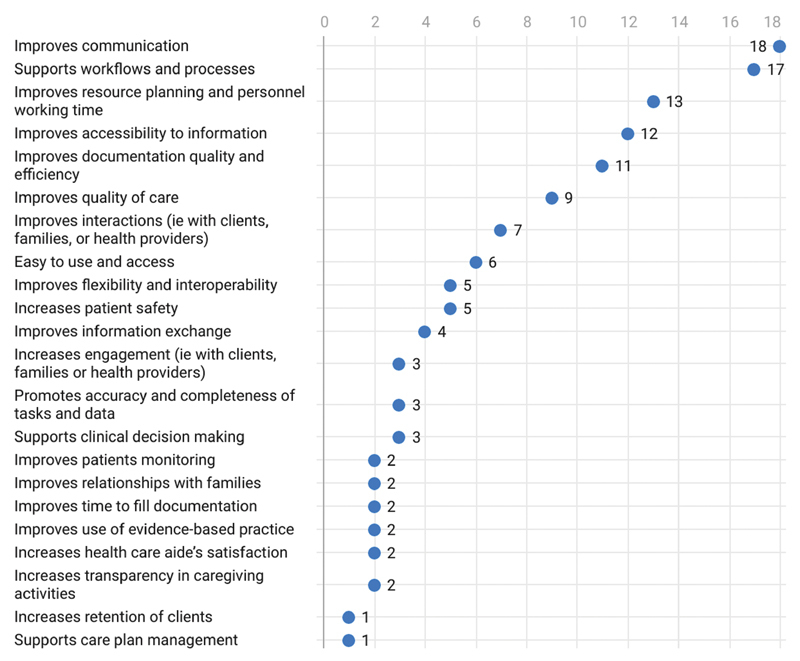
Distribution of benefits reported in the selected studies.
The main benefits we found in this review were related to (1) improvements in communication, (2) support to workflows and processes, (3) improvements in resource planning and health care aides services associated cost and time, (4) improve access to information and documentation, (5) improve documentation quality and efficiency, and (6) improvements in the coordination of care and patient's care follow-up at home, extending care for patients in the community.
Improvements in communication compared with conventional methods, such as fax, traditional mailing, and telephone, 2 80 81 101 was a consistently reported benefit of ICT for health care aides. In these studies, users reported that ICT improved communication between caregivers, patients, 51 54 72 and staff 64 65 by introducing tools such as video calls and telehealth. 35 57 Several studies reported the benefits of telehealth and remote care provided by ICT. 32 102 We observe health care aides' opportunity to provide services in distant places. 102 103 For example, ICT can support health care aides to deliver high-quality health care in remote territories and regions in rural communities and isolated populations. 63 64 102 The need for telehealth services for older adults, especially those living with dementia, has increased over the last few years. 104 A few authors have described how telehealth can improve health care service delivery. 35 54 102 104 105
Also, studies reported that ICT enabled a better cultural understanding by delivering information in different languages. 70 In addition, we found that ICT supported communication across locations, personnel, and families. 76 Moreover, a few studies reported that ICT improve older adults communication capacity about their health concerns. 73 Finally, ICT were found to allow health care aides to respond to issues rapidly. 83
Another group of studies reported that ICT supported workflows and processes 2 35 53 54 66 69 71 72 74 77 81 83 by improving time management, 74 77 81 simplifying and standardizing procedures, 72 reducing repetitive actions, 2 and supporting schedule planning. 2 40 52 61 77 82 84 101 As an example, Stroulia et al 54 reported that ICT for health care aides supported automatization and adaptative scheduling which could potentially reduce travel times and missed appointments. Katalinic et al 35 reported how ICT can support health care aides' remote practice to provide caregiving services to clients in distant locations.
We found a group of studies reporting benefits related to better work and staff organization associated with ICT. 71 Lastly, ICT were observed as a factor for improving staff planning, 66 71 enable caregiving services in a timely manner, 84 and promote time savings in comparison with existing methods of communication. 40 Regarding the benefit of costs and service utilization, 2 101 Chiang et al 2 reported the reduction of medical costs and service consumptions through the use of smartphones applications to provide home care services. Also, Lindberg et al 101 identified several publications describing how ICT for health care aides can reduce cost of caregiving services compared with traditional modes of delivery.
Furthermore, a few studies described accessibility to information and documentation as an enormous benefit 40 53 54 57 59 64 80 101 by providing health care aides quick access or real-time updates to their clients information. 54 59 A significant group of studies reported that ICT improved documentation quality and efficiency, 64 65 68 by improving consistency in documentation, 72 with more precise and updated information. 54 57 59 76
Lastly, we found another group of benefits that reported improvements in the coordination of care and patient follow-up at home. These benefits have proven to extend the care for patients in the community, 2 35 82 84 101 and improve interactions between clients and health care aides. 52 56 57 61 75 The effectiveness of ICT was described as a benefit by providing easy access to health care plans, 35 53 57 72 promoting flexibility and interoperability, 40 63 69 and assisting patient safety. 54 57 71 73
Discussion
This review examined the range and extent of ICT used by health care aides to manage and coordinate care delivery and their workflow with clients. We included 40 studies selected from the academic literature. We organized our findings into five categories of purposes for implementing ICT among health care aides. Additionally, we found a diversity of settings and arrangements for hardware and software to deploy these technologies within health care services and organizations.
In the literature, we identified evidence suggesting that current technologies for health care aides are inefficient and often do not fit their workflows, 42 or outdated and ineffective. 37 From a benefits perspective, ICT is presented as a facilitator of effective communication for health care aides. 15 In this review, we shared additional knowledge about the range and extent of ICT used by health care aides, as well as enhanced our understanding of the barriers and benefits associated with the use, adoption, and implementation of ICT by health care aides.
The literature suggests that across the health care sector, the barriers and benefits of ICT are common for health care professionals. 87 95 Overall, we identified 128 barriers and 130 benefits associated with ICT used by health care aides. Even though ICT can face significant barriers in implementation, we found positive information regarding their benefits. Our findings are consistent with the academic literature that exposed the barriers and benefits of use and implemention of ICT in the health care sector for other providers. 15 35 42 45 66 89 97 106 107
Several authors acknowledge the difficulties related to implementing technologies in health care settings. 45 The common barriers for the adoption and implementation of ICT within this sector are related to resource requirements and costs, 108 109 technological limitations, and lack of global standards and privacy concerns. 110 111 112 These barriers are aside from the previously established structural organizational barriers. 86
In the academic literature, there are several examples describing the barriers related to the adoption and implementation of ICT in health care settings that can be analyzed under the lens of technology acceptance models. 45 113 114 115 Furthermore, the expected benefits of using ICT could inform future implementations. 116 Benefits of good-quality software, compatibility and interoperability with other information systems 117 would promote the adoption of these technologies among health care aides. 118
In this review, our findings suggested that health care aides could experience multiple barriers to use and adopt new ICT in their workflows and practice. The main barriers we found were related to incomplete hardware and software features, time-consuming ICT adoption, and heavy or increased workloads. In past studies, authors have described the financial, organizational, structural, cultural, and technical difficulties to adopting ICT 89 and additional barriers to ICT use and adoption by health care aides, such as professional skills 102 and digital health education and literacy. 119 To overcome these barriers, authors have recommended a more comprehensive 120 and participatory design process involving health care aides' needs and experiences. 60 121 122
Likewise, we observed that health care aides could adopt and use ICT to support new models of care, such as telehealth for client follow-up, and consultation. However, traditional work practices have shaped health care aides' current workflows and procedures. As a result, health care aides face multiple barriers to adopt and use ICT in their practice. One significant barrier is the organizational and provider infrastructure, 42 as providers generally use ICT-specific electronic patient information systems. By increasing their own awareness about the use, capabilities, and benefits of integrating ICT in critical activities of integrated care, health care aides could take advantage of the potential of these technologies to improve activities, such as prevention, 42 collaboration, and delivery of care in innovative ways using ICT.
Barriers to access to data, even at regional levels, present an obstruction to deliver care by health care aides. 42 Accessing and updating information about client's observations and medical conditions are essential for health care aides to provide better caregiving services. Evidence suggests that information exchange also can improve health care aides' communication with other health professionals. 15 Thus, we support the argument that access to information can enhance the ability of health care aides to provide higher quality caregiving services 37 97 102 and make better decisions to improve the quality of care. 36
Since health care aides face structural challenges in their profession, such as lack of regulation and standardized scope of practice, it is crucial to consider these barriers beforehand when implementing new ICT. 8 9 12 29 123 New ICT developments should consider both, the structural and the technological barriers within the health care sector. 124
ICT can support health care aides' work by facilitating caregiving 125 and support the long-term relationship between patients and health care providers. 97 By implementing and adopting ICT in health care aides' professional practice, they could support caregiving services for numerous people. In summary, ICT could serve as a strategy to enable socially isolated people to utilize health care aides' services, 36 102 126 127 and address the lack of direct support from professionals available to provide care services 128 and leverage the shortage of skilled and well-trained health care professionals. 129
Involving health care aides into the process of designing, implementing, and customizing new ICT is crucial to increase the rate of adoption. 36 37 As the older adult population demands more caregiver professional services, we could expect an increasing number of new ICT to support health care aides. 33 36 125 For that reason, we should consider the findings reported in this review related to barriers and benefits of ICT for health care aides.
Future Recommendations
After reviewing an extensive compilation of studies for this review, we recognize the need for more straightforward ICT aligned with health care aides' workflows. In addition, we must consider the involvement of end-users in design, training, and education, and clarity about the use of ICT. The voice of the end-user is essential for developing ICT tools. Future developments should include feedback from users in every step of development and the mindset of improving care. This could be done in participatory design methods 130 to engage users in the ICT.
The novel coronavirus disease 2019 (COVID-19) pandemic has accelerated the adoption of ICT tools, 29 105 such as telehealth applications. 105 These applications include remote consultations for seniors, 131 specifically persons living with dementia, to minimize the risk of contracting COVID-19. 132 The pandemic has impacted the role of health care aides as caregivers by limiting their interactions and communications with their clients and families, 133 as well as it has revealed limitations in their ability to provide remote services. This is considering the gaps between different health care facilities and their preparedness to provide telehealth services with patients who have no internet connection or phone service. 134
At the same time, the pandemic revealed opportunities for the adoption and implementation of ICT tools to monitoring COVID-19 symptoms 109 and coordinating and delivering care. 135 136 In the upcoming years, we can expect a greater demand, adoption, and use of ICT to improve and enable the quality of care. Identifying the health care aides' needs and requirements for design is crucial, 121 as this will pave the road to acceptance and adoption of the ICT. We also believe that critical sociocultural factors need to be understood before developing ICT. 121 In the future, health care aides with technical training may be more receptive to ICT. 38 This could help health care aides to overcome multiple barriers identified in this study.
Finally, although the literature reporting information specific to health care aides is scarce, and there is limited research on evidence-based practices for this population, we cannot understimate the importance of health care aides to sustain the health care system. Indeed, many countries around the world face a shortage of these groups of service providers. In this review, we have seen how ICT can help health care aides in their practice. However, more research is needed to support evidence-based ICT.
Limitations of the Study
This literature review has some limitations. First, despite our efforts to conduct a comprehensive and exhaustive search, the academic literature lacks consistency concerning our search terms. We were looking for healthcare workers, such as health care aides and personal support workers. Due to the limited literature involving this population, we decided to include nurses and personal support providers in studies that referred home care services. We assumed that their experiences are similar, considering different ways of pointing health care aides across Canada and other countries. Second, it was hard to classify barriers and benefits, as some articles reported these indistinctly. For that reason, we defined meanings for each group, and after a process of open discussion, such definitions were organized accordingly. Third, although we identified several barriers and benefits in selected studies, not all studies comprehensively reported all perceived benefits and barriers associated with ICT for health care aides.
Conclusion
Despite challenges, the literature identifies that ICT can improve health care aides' workflow and quality of care for their clients. The main issue we experienced was the scarce literature related specifically to health care aides. We achieved the aim of this literature review to understand the barriers and potential benefits of ICT adoption for health care aides. We classified this information by purpose as reported in the selected studies. Future directions should examine the impact of the ICT on workflows of health care aides.
Clinical Relevance Statement
This literature review showed the information and communication technologies (ICT) used by health care aides to manage and coordinate the care-delivery workflow for their clients. In addition, we have explored the factors that would assist in the development and adoption of electronic platforms, which could improve the overall efficiency of care provided by health care aides.
Multiple Choice Questions
-
What is the most common barrier to implement and adopt information and communication technologies (ICT) faced by health care aides?
Incomplete hardware and software features
Time-consuming ICT adoption
Heavy or increased workloads
Perceived lack of usefulness of ICT
Correct Answer: The correct answer is option a, as health care aides reported system malfunctions, poor design, and issues regarding software configuration. In these studies, the software did not reflect users' needs and expectations or did not support their information needs. Some studies described the lack of documentation features. In addition to usability issues we found connectivity issues, as a hardware significant barrier in this group. Some studies reported incomplete hardware features as a significant barrier to adopting and implementing ICT.
-
What is the most common benefit for health care aides to implement and adopt information and communication technologies (ICT)?
Improvements in communication
Improvements in planning
Improvement in organization staffing
Increase overall productivity
Correct Answer: The correct answer is option a. We found this benefit as the most common in this review. Improvements in communication include communication between caregivers and patients and staff, better cultural understanding. In addition, ICT can support communication across locations, personnel, and families and allow clients to inform their concerns to health care aides.
Acknowledgments
We acknowledge Lauren McLennan, Peyman A. Khaneghah, Wang C. Tang, and Elyse Letts who provided support as research assistants.
Funding Statement
Funding This project is supported by the Centre for Aging and Brain Health Innovation (CABHI) and Alberta Innovates grant number G2019000525 AICE-ABH, received by L.L. as principal investigator.
Conflict of Interest None declared.
Author Contributions
All authors contributed to the study's conception and design. Data extraction, analysis, and synthesis were performed by H.P., N.N., and S.M. The first draft of the manuscript was written by H.P., N.N., S.M., and S.P., and all authors commented on previous versions of the manuscript. L.L., A.M.C., and N.N. read and approved the final manuscript.
Supplementary Material
References
- 1.World Health Organization Ageing and healthAccessed May 3, 2021 at:https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- 2.Chiang K F, Wang H H.Nurses' experiences of using a smart mobile device application to assist home care for patients with chronic disease: a qualitative study J Clin Nurs 201625(13,14):2008–2017. [DOI] [PubMed] [Google Scholar]
- 3.Alzheimer Society of Canada . Report summary prevalence and monetary costs of dementia in Canada (2016): a report by the Alzheimer Society of Canada. Health Promot Chronic Dis Prev Can. 2016;36(10):231–232. [PMC free article] [PubMed] [Google Scholar]
- 4.Personal support workerAccessed March 20, 2021 at:https://settlement.org/alternative-jobs/nurse/personal-support-worker/
- 5.Personal Support Worker H Q.Personal support worker?Accessed January 21, 2022 at:https://www.centennialcollege.ca/programs-courses/full-time/personal-support-worker/
- 6.Online O NIP.Personal support worker (PSW) in CanadaAccessed March 2, 2021 at:http://www.onip.ca/personal-support-worker/
- 7.Saari M, Xiao S, Rowe A. The role of unregulated care providers in home care: a scoping review. J Nurs Manag. 2018;26(07):782–794. doi: 10.1111/jonm.12613. [DOI] [PubMed] [Google Scholar]
- 8.Hewko S J, Cooper S L, Huynh H. Invisible no more: a scoping review of the health care aide workforce literature. BMC Nurs. 2015;14(01):38. doi: 10.1186/s12912-015-0090-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Berta W, Laporte A, Deber R, Baumann A, Gamble B. The evolving role of health care aides in the long-term care and home and community care sectors in Canada. Hum Resour Health. 2013;11(01):25. doi: 10.1186/1478-4491-11-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lilly M. Medical versus social work-places: constructing and compensating the personal support worker across health care settings in Ontario, Canada. Gend Place Cult. 2008;15(03):285–299. [Google Scholar]
- 11.Arain M A, Deutschlander S, Charland P. Are healthcare aides underused in long-term care? A cross-sectional study on continuing care facilities in Canada. BMJ Open. 2017;7(05):e015521. doi: 10.1136/bmjopen-2016-015521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Estabrooks C A, Squires J E, Carleton H L, Cummings G G, Norton P G. Who is looking after mom and dad? Unregulated workers in Canadian long-term care homes. Can J Aging. 2015;34(01):47–59. doi: 10.1017/S0714980814000506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.White D E, Jackson K, Besner J, Norris J M. The examination of nursing work through a role accountability framework. J Nurs Manag. 2015;23(05):604–612. doi: 10.1111/jonm.12186. [DOI] [PubMed] [Google Scholar]
- 14.Franzosa E, Tsui E K, Baron S. Home health aides' perceptions of quality care: goals, challenges, and implications for a rapidly changing industry. New Solut. 2018;27(04):629–647. doi: 10.1177/1048291117740818. [DOI] [PubMed] [Google Scholar]
- 15.Saari M, Patterson E, Killackey T, Raffaghello J, Rowe A, Tourangeau A E.Home-based care: barriers and facilitators to expanded personal support worker roles in Ontario, Canada Home Health Care Serv Q 201736(3,4):127–144. [DOI] [PubMed] [Google Scholar]
- 16.Kroezen M, Schäfer W, Sermeus W, Hansen J, Batenburg R. Healthcare assistants in EU member states: an overview. Health Policy. 2018;122(10):1109–1117. doi: 10.1016/j.healthpol.2018.07.004. [DOI] [PubMed] [Google Scholar]
- 17.Janet L, Jennifer S, Alvin Y.Ontario personal support workers in home and community care: CRNCC/PSNO survey resultsAccessed March 20, 2021 at:https://www.ryerson.ca/content/dam/crncc/knowledge/infocus/factsheets/InFocus-OntarioPSWsinHomeandCommunityCare.pdf
- 18.Booi L, Sixsmith J, Chaudhury H, O'Connor D, Young M, Sixsmith A. 'I wouldn't choose this work again': perspectives and experiences of care aides in long-term residential care. J Adv Nurs. 2021;77(09):3842–3852. doi: 10.1111/jan.14948. [DOI] [PubMed] [Google Scholar]
- 19.Kelly C, Bourgeault I L. The personal support worker program standard in Ontario: an alternative to self-regulation? Healthc Policy. 2015;11(02):20–26. [PMC free article] [PubMed] [Google Scholar]
- 20.National Alliance for Caregiving Caregiving in the U.S. 2020. Accessed January 21, 2022 at:https://www.caregiving.org/caregiving-in-the-us-2020/
- 21.Statistics Canada Care counts: care receivers in Canada, 2018. Accessed February 1, 2021 at:https://www150.statcan.gc.ca/n1/pub/11-627-m/11-627-m2020002-eng.htm
- 22.Government of Canada Government of Canada announces funding to train 4,000 personal support worker interns, support sectorAccessed May 18, 2021 at:https://www.canada.ca/en/employment-social-development/news/2020/12/government-of-canada-announces-funding-to-train-4000-personal-support-worker-interns-support-sector.html
- 23.CBC News Ontario's PSW shortage is impacting people living with disabilities in Waterloo regionAccessed May 18, 2021 at:https://www.cbc.ca/news/canada/kitchener-waterloo/psw-shortage-ontario-waterloo-region-impacts-1.5953472
- 24.Muir T.Measuring social protection for long-term careAccessed January 21, 2022 at:https://www.oecd-ilibrary.org/social-issues-migration-health/measuring-social-protection-for-long-term-care_a411500a-en
- 25.CIHI Canada's seniors population outlook: uncharted territoryAccessed May 18, 2021 at:https://www.cihi.ca/en/infographic-canadas-seniors-population-outlook-uncharted-territory
- 26.United Nations - Department of Economic and Social Affairs PD World population prospects 2019: highlightsAccessed January 21, 2022 at:https://population.un.org/wpp/Publications/Files/WPP2019_Highlights.pdf
- 27.Brophy J T, Keith M M, Hurley M, McArthur J E. Sacrificed: Ontario healthcare workers in the time of COVID-19. New Solut. 2021;30(04):267–281. doi: 10.1177/1048291120974358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Drennan V M, Ross F. Global nurse shortages-the facts, the impact and action for change. Br Med Bull. 2019;130(01):25–37. doi: 10.1093/bmb/ldz014. [DOI] [PubMed] [Google Scholar]
- 29.Estabrooks C A, Straus S E, Flood C M. Restoring trust: COVID-19 and the future of long-term care in Canada. Facets. 2020;5(01):651–691. [Google Scholar]
- 30.Baker S B, Xiang W, Atkinson I. Internet of things for smart healthcare: technologies, challenges, and opportunities. IEEE Access. 2017;5:26521–26544. [Google Scholar]
- 31.Tyagi R K, Cook L, Olson J, Belohlav J. Healthcare technologies, quality improvement programs and hospital organizational culture in Canadian hospitals. BMC Health Serv Res. 2013;13(01):413. doi: 10.1186/1472-6963-13-413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Boric-Lubecke O, Gao X, Yavari E, Baboli M, Singh A, Lubecke V M.E-healthcare: Remote monitoring, privacy, and securityIn: 2014 IEEE MTT-S International Microwave Symposium (IMS2014). IEEE; 2014:1–3; Tampa, FL
- 33.Report: 2020 national survey of Canadian nurses: use of digital health technology in practiceAccessed January 21, 2022 at:https://www.infoway-inforoute.ca/en/component/edocman/3812-2020-national-survey-of-canadian-nurses-use-of-digital-health-technology-in-practice/view-document?Itemid=0
- 34.Forum on Aging, Disability, and Independence; Board on Health Sciences Policy; Division on Behavioral and Social Sciences and Education; Institute of Medicine; National Research Council . Washington, DC: National Academies Press; 2015. The Future of Home Health Care: Workshop Summary. [Google Scholar]
- 35.Katalinic O, Young A, Doolan D. Case study: the interact home telehealth project. J Telemed Telecare. 2013;19(07):418–424. doi: 10.1177/1357633X13506513. [DOI] [PubMed] [Google Scholar]
- 36.Lindeman D A, Kim K K, Gladstone C, Apesoa-Varano E C. Technology and caregiving: emerging interventions and directions for research. Gerontologist. 2020;60 01:S41–S49. doi: 10.1093/geront/gnz178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sterling M R, Dell N, Tseng E. Home care workers caring for adults with heart failure need better access to training and technology: a role for implementation science. J Clin Transl Sci. 2020;4(03):224–228. doi: 10.1017/cts.2020.36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.King S, Liu L, Stroulia E, Nikolaidis I. Using simulations to integrate technology into health care aides' workflow. Int J Adv Corp Learn. 2013;6(02):28. [Google Scholar]
- 39.Wildevuur S E, Simonse L W. Information and communication technology-enabled person-centered care for the “big five” chronic conditions: scoping review. J Med Internet Res. 2015;17(03):e77. doi: 10.2196/jmir.3687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Petersen H V, Foged S, Madsen A L, Andersen O, Nørholm V. Nurses' perception of how an e-message system influences cross-sectoral communication: a qualitative study. J Nurs Manag. 2018;26(05):509–517. doi: 10.1111/jonm.12575. [DOI] [PubMed] [Google Scholar]
- 41.Aslani N, Ahmadi M, Samadbeik M. A systematic review of the attributes of electronic personal health Records for Patients with multiple sclerosis. Health Technol (Berl) 2020;10(03):587–599. [Google Scholar]
- 42.Steele Gray C, Barnsley J, Gagnon D. Using information communication technology in models of integrated community-based primary health care: learning from the iCOACH case studies. Implement Sci. 2018;13(01):87. doi: 10.1186/s13012-018-0780-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Sterling M R, Silva A F, Leung P BK. “It's like they forget that the word 'health' is in 'home health aide'”: understanding the perspectives of home care workers who care for adults with heart failure. J Am Heart Assoc. 2018;7(23):e010134. doi: 10.1161/JAHA.118.010134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Falconer E, Kho D, Docherty J P. Use of technology for care coordination initiatives for patients with mental health issues: a systematic literature review. Neuropsychiatr Dis Treat. 2018;14:2337–2349. doi: 10.2147/NDT.S172810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rahimi B, Nadri H, Lotfnezhad Afshar H, Timpka T. A systematic review of the technology acceptance model in health informatics. Appl Clin Inform. 2018;9(03):604–634. doi: 10.1055/s-0038-1668091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Alhuwail D, Koru G. Identifying home care clinicians' information needs for managing fall risks. Appl Clin Inform. 2016;7(02):211–226. doi: 10.4338/ACI-2015-11-RA-0160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Daudt H M, van Mossel C, Scott S J. Enhancing the scoping study methodology: a large, inter-professional team's experience with Arksey and O'Malley's framework. BMC Med Res Methodol. 2013;13(01):48. doi: 10.1186/1471-2288-13-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(01):19–32. [Google Scholar]
- 49.Robinson K A, Saldanha I J, McKoy N A. Development of a framework to identify research gaps from systematic reviews. J Clin Epidemiol. 2011;64(12):1325–1330. doi: 10.1016/j.jclinepi.2011.06.009. [DOI] [PubMed] [Google Scholar]
- 50.Belur J, Tompson L, Thornton A, Simon M. Interrater reliability in systematic review methodology: exploring variation in coder decision-making. Sociol Methods Res. 2021;50(02):837–865. [Google Scholar]
- 51.Brown R N, Ruggiano N, Page T F. CareHeroes web and android apps for dementia caregivers. Res Gerontol Nurs. 2016;9(04):193–203. doi: 10.3928/19404921-20160229-02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kaunda-Khangamwa B N, Steinhardt L C, Rowe A K. The effect of mobile phone text message reminders on health workers' adherence to case management guidelines for malaria and other diseases in Malawi: lessons from qualitative data from a cluster-randomized trial. Malar J. 2018;17(01):481. doi: 10.1186/s12936-018-2629-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Gars U, Skov H. The TECS model leads to active use of technology in home care. Nord J Nurs Res. 2017;37(01):51–58. [Google Scholar]
- 54.Stroulia E, Nikolaidisa I, Liua L, King S, Lessard L. Home care and technology: a case study. Stud Health Technol Inform. 2012;182:142–152. [PubMed] [Google Scholar]
- 55.Sassen B, Kok G, Schepers J, Vanhees L. Supporting health care professionals to improve the processes of shared decision making and self-management in a web-based intervention: randomized controlled trial. J Med Internet Res. 2014;16(10):e211. doi: 10.2196/jmir.3170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Nilsson L, Fagerström C.Decision-makers and mediators in a home healthcare digitisation process: nurses' experiences of implementation and use of a decision support system Contemp Nurse 201854(4,5):511–521. [DOI] [PubMed] [Google Scholar]
- 57.Gund A, Sjöqvist B A, Wigert H, Hentz E, Lindecrantz K, Bry K. A randomized controlled study about the use of eHealth in the home health care of premature infants. BMC Med Inform Decis Mak. 2013;13(01):22. doi: 10.1186/1472-6947-13-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Andersen G R, Bendal S, Westgaard R H. Work demands and health consequences of organizational and technological measures introduced to enhance the quality of home care services–a subgroup analysis. Appl Ergon. 2015;51:172–179. doi: 10.1016/j.apergo.2015.04.020. [DOI] [PubMed] [Google Scholar]
- 59.Alhuwail D, Koru G. Leveraging health information technology for fall-risk management in home care: a qualitative exploration of clinicians' perspectives. Home Health Care Manage Pract. 2016;28(04):241–249. [Google Scholar]
- 60.Danilovich M K, Diaz L, Saberbein G, Healey W E, Huber G, Corcos D M.Design and development of a mobile exercise application for home care aides and older adult medicaid home and community-based clients Home Health Care Serv Q 201736(3-4):196–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Lexis M, Everink I, Van Der Heide L, Spreeuwenberg M, Willems C, De Witte L. Activity monitoring technology to support homecare delivery to frail and psychogeriatric elderly persons living at home alone. Technol Disabil. 2013;25(03):189–197. [Google Scholar]
- 62.Westra B L, Oancea C, Savik K, Marek K D. The feasibility of integrating the Omaha system data across home care agencies and vendors. Comput Inform Nurs. 2010;28(03):162–171. doi: 10.1097/NCN.0b013e3181d7812c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Yang Y, Bass E J, Bowles K H, Sockolow P S. Impact of home care admission nurses' goals on electronic health record documentation strategies at the point of care. Comput Inform Nurs. 2019;37(01):39–46. doi: 10.1097/CIN.0000000000000468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tapper L, Quinn H, Kerry J, Brown K G. Introducing handheld computers into home care. Can Nurse. 2012;108(01):28–32. [PubMed] [Google Scholar]
- 65.Sockolow P S, Bowles K H, Adelsberger M C, Chittams J L, Liao C. Impact of homecare electronic health record on timeliness of clinical documentation, reimbursement, and patient outcomes. Appl Clin Inform. 2014;5(02):445–462. doi: 10.4338/ACI-2013-12-RA-0106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Han S, Juell-Skielse G, Smedberg Å, Aasi P, Nilsson A G. Benefits of mobile reporting systems in social home care: the case of seven Swedish municipalities. Int J Technol Assess Health Care. 2014;30(04):409–415. doi: 10.1017/S026646231400052X. [DOI] [PubMed] [Google Scholar]
- 67.Gjevjon E R, Hellesø R.The quality of home care nurses' documentation in new electronic patient records J Clin Nurs 201019(1,2):100–108. [DOI] [PubMed] [Google Scholar]
- 68.Bercovitz A, Sengupta M, Jamison P. Electronic medical record adoption and use in home health and hospice. NCHS Data Brief. 2010;(45):1–8. [PubMed] [Google Scholar]
- 69.De Vliegher K, Paquay L, Vernieuwe S, Van Gansbeke H. The experience of home nurses with an electronic nursing health record. Int Nurs Rev. 2010;57(04):508–513. doi: 10.1111/j.1466-7657.2010.00827.x. [DOI] [PubMed] [Google Scholar]
- 70.Alhuwail D, Koru G, Mills M E.Supporting the information domains of fall-risk management in home care via health information technology Home Health Care Serv Q 201635(3,4):155–171. [DOI] [PubMed] [Google Scholar]
- 71.Vasalampi A. Adoption and use of a mobile system at home care. Stud Health Technol Inform. 2017;242:1042–1046. [PubMed] [Google Scholar]
- 72.Santi S M, Hinton S, Berg K, Stolee P. Bridging the information divide: health information sharing in home care. Can J Nurs Res. 2013;45(01):16–35. doi: 10.1177/084456211304500104. [DOI] [PubMed] [Google Scholar]
- 73.Göransson C, Eriksson I, Ziegert K. Testing an app for reporting health concerns-Experiences from older people and home care nurses. Int J Older People Nurs. 2018;13(02):e12181. doi: 10.1111/opn.12181. [DOI] [PubMed] [Google Scholar]
- 74.Dean K M, Hatfield L A, Jena A B. Preliminary data on a care coordination program for home care recipients. J Am Geriatr Soc. 2016;64(09):1900–1903. doi: 10.1111/jgs.14351. [DOI] [PubMed] [Google Scholar]
- 75.Stutzel M C, Filippo M P, Sztajnberg A. Multi-part quality evaluation of a customized mobile application for monitoring elderly patients with functional loss and helping caregivers. BMC Med Inform Decis Mak. 2019;19(01):1–18. doi: 10.1186/s12911-019-0839-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Farsjø C, Kluge A, Moen A. Using a tablet application about nutrition in home care-Experiences and perspectives of healthcare professionals. Health Soc Care Community. 2019;27(03):683–692. doi: 10.1111/hsc.12685. [DOI] [PubMed] [Google Scholar]
- 77.Bastide R, Bardy P, Borrel B. Plas'O'Soins: a software platform for modeling, planning and monitoring homecare activities. IRBM. 2014;35(02):82–87. [Google Scholar]
- 78.Arbaje A I, Hughes A, Werner N. Information management goals and process failures during home visits for middle-aged and older adults receiving skilled home healthcare services after hospital discharge: a multisite, qualitative study. BMJ Qual Saf. 2019;28(02):111–120. doi: 10.1136/bmjqs-2018-008163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Dowding D W, Russell D, Onorato N, Merrill J A. Technology solutions to support care continuity in home care: a focus group study. J Healthc Qual. 2018;40(04):236–246. doi: 10.1097/JHQ.0000000000000104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Lyngstad M, Hellesø R. Electronic communication experiences of home health care nurses and general practitioners: a cross-sectional study. Stud Health Technol Inform. 2014;201:388–394. [PubMed] [Google Scholar]
- 81.Lyngstad M, Grimsmo A, Hofoss D, Hellesø R.Home care nurses' experiences with using electronic messaging in their communication with general practitioners J Clin Nurs 201423(23,24):3424–3433. [DOI] [PubMed] [Google Scholar]
- 82.Gentles S J, Lokker C, McKibbon K A. Health information technology to facilitate communication involving health care providers, caregivers, and pediatric patients: a scoping review. J Med Internet Res. 2010;12(02):e22. doi: 10.2196/jmir.1390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Bossen C, Christensen L R, Grönvall E, Vestergaard L S. CareCoor: augmenting the coordination of cooperative home care work. Int J Med Inform. 2013;82(05):e189–e199. doi: 10.1016/j.ijmedinf.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 84.Mangwi Ayiasi R, Kolsteren P, Batwala V, Criel B, Orach C G. Effect of village health team home visits and mobile phone consultations on maternal and newborn care practices in Masindi and Kiryandongo, Uganda: a community-intervention trial. PLoS One. 2016;11(04):e0153051. doi: 10.1371/journal.pone.0153051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Little A, Medhanyie A, Yebyo H, Spigt M, Dinant G J, Blanco R. Meeting community health worker needs for maternal health care service delivery using appropriate mobile technologies in Ethiopia. PLoS One. 2013;8(10):e77563. doi: 10.1371/journal.pone.0077563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Lluch M. Healthcare professionals' organisational barriers to health information technologies-a literature review. Int J Med Inform. 2011;80(12):849–862. doi: 10.1016/j.ijmedinf.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 87.de Souza C HA, Morbeck R A, Steinman M. Barriers and benefits in telemedicine arising between a high-technology hospital service provider and remote public healthcare units: a qualitative study in Brazil. Telemed J E Health. 2017;23(06):527–532. doi: 10.1089/tmj.2016.0158. [DOI] [PubMed] [Google Scholar]
- 88.Alaboudi A, Atkins A, Sharp B, Balkhair A, Alzahrani M, Sunbul T. Barriers and challenges in adopting Saudi telemedicine network: the perceptions of decision makers of healthcare facilities in Saudi Arabia. J Infect Public Health. 2016;9(06):725–733. doi: 10.1016/j.jiph.2016.09.001. [DOI] [PubMed] [Google Scholar]
- 89.Kaye R, Kokia E, Shalev V, Idar D, Chinitz D. Barriers and success factors in health information technology: a practitioner's perspective. J Manag Mark Healthc. 2010;3(02):163–175. [Google Scholar]
- 90.Irinoye O O, Ayandiran E O, Fakunle I, Mtshali N. Nurses' perception and barriers to use of information communication technology in a teaching hospital in Nigeria. Comput Inform Nurs. 2013;31(08):394–400. doi: 10.1097/NXN.0b013e3182997a6e. [DOI] [PubMed] [Google Scholar]
- 91.Schoen J, Mallett J W, Grossman-Kahn R, Brentani A, Kaselitz E, Heisler M. Perspectives and experiences of community health workers in Brazilian primary care centers using m-health tools in home visits with community members. Hum Resour Health. 2017;15(01):71. doi: 10.1186/s12960-017-0245-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Eley R, Fallon T, Soar J, Buikstra E, Hegney D. Barriers to use of information and computer technology by Australia's nurses: a national survey. J Clin Nurs. 2009;18(08):1151–1158. doi: 10.1111/j.1365-2702.2008.02336.x. [DOI] [PubMed] [Google Scholar]
- 93.Ramsey A, Lord S, Torrey J, Marsch L, Lardiere M. Paving the way to successful implementation: identifying key barriers to use of technology-based therapeutic tools for behavioral health care. J Behav Health Serv Res. 2016;43(01):54–70. doi: 10.1007/s11414-014-9436-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.O' Connor Y, O' Connor S, Heavin C, Gallagher J, O' Donoghue J. Waltham, MA: Elsevier; 2016. Sociocultural and technological barriers across all phases of implementation for mobile health in developing countries; pp. 212–230. [Google Scholar]
- 95.Shah S GS, Robinson I. Benefits of and barriers to involving users in medical device technology development and evaluation. Int J Technol Assess Health Care. 2007;23(01):131–137. doi: 10.1017/S0266462307051677. [DOI] [PubMed] [Google Scholar]
- 96.Hassan A YI. Challenges and recommendations for the deployment of information and communication technology solutions for informal caregivers: scoping review. JMIR Aging. 2020;3(02):e20310. doi: 10.2196/20310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Omboni S, Caserini M, Coronetti C. Telemedicine and M-health in hypertension management: technologies, applications and clinical evidence. High Blood Press Cardiovasc Prev. 2016;23(03):187–196. doi: 10.1007/s40292-016-0143-6. [DOI] [PubMed] [Google Scholar]
- 98.Braun R, Catalani C, Wimbush J, Israelski D. Community health workers and mobile technology: a systematic review of the literature. PLoS One. 2013;8(06):e65772. doi: 10.1371/journal.pone.0065772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Early J, Gonzalez C, Gordon-Dseagu V, Robles-Calderon L. Use of mobile health (mHealth) technologies and interventions among community health workers globally: a scoping review. Health Promot Pract. 2019;20(06):805–817. doi: 10.1177/1524839919855391. [DOI] [PubMed] [Google Scholar]
- 100.Thakkar M, Davis D C. Risks, barriers, and benefits of EHR systems: a comparative study based on size of hospital. Perspect Health Inf Manag. 2006;3:5. [PMC free article] [PubMed] [Google Scholar]
- 101.Lindberg B, Nilsson C, Zotterman D, Söderberg S, Skär L. Using information and communication technology in home care for communication between patients, family members, and healthcare professionals: a systematic review. Int J Telemed Appl. 2013;2013:461829. doi: 10.1155/2013/461829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Choukou M A, Maddahi A, Polyvyana A, Monnin C. Digital health technology for Indigenous older adults: a scoping review. Int J Med Inform. 2021;148:104408. doi: 10.1016/j.ijmedinf.2021.104408. [DOI] [PubMed] [Google Scholar]
- 103.Koo B M, Vizer L M. Examining mobile technologies to support older adults with dementia through the lens of personhood and human needs: scoping review. JMIR Mhealth Uhealth. 2019;7(11):e15122. doi: 10.2196/15122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Brown P, Oliver E, Dening K H. Increasing need for telehealth services for families affected by dementia as a result of Covid-19. J Community Nurs. 2020;34(05):59–64. [Google Scholar]
- 105.Wosik J, Fudim M, Cameron B. Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc. 2020;27(06):957–962. doi: 10.1093/jamia/ocaa067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Alamoodi A H, Garfan S, Zaidan B B. A systematic review into the assessment of medical apps: motivations, challenges, recommendations and methodological aspect. Health Technol (Berl) 2020;10(05):1045–1061. [Google Scholar]
- 107.Abelson J S, Kaufman E, Symer M, Peters A, Charlson M, Yeo H. Barriers and benefits to using mobile health technology after operation: a qualitative study. Surgery. 2017;162(03):605–611. doi: 10.1016/j.surg.2017.05.007. [DOI] [PubMed] [Google Scholar]
- 108.Jha A K, DesRoches C M, Campbell E G. Use of electronic health records in U.S. hospitals. N Engl J Med. 2009;360(16):1628–1638. doi: 10.1056/NEJMsa0900592. [DOI] [PubMed] [Google Scholar]
- 109.Bandini J, Rollison J, Feistel K, Whitaker L, Bialas A, Etchegaray J. Home care aide safety concerns and job challenges during the COVID-19 pandemic. New Solut. 2021;31(01):20–29. doi: 10.1177/1048291120987845. [DOI] [PubMed] [Google Scholar]
- 110.Yao W, Chu C-H, Li Z. The adoption and implementation of RFID technologies in healthcare: a literature review. J Med Syst. 2012;36(06):3507–3525. doi: 10.1007/s10916-011-9789-8. [DOI] [PubMed] [Google Scholar]
- 111.Scott Kruse C, Karem P, Shifflett K, Vegi L, Ravi K, Brooks M. Evaluating barriers to adopting telemedicine worldwide: a systematic review. J Telemed Telecare. 2018;24(01):4–12. doi: 10.1177/1357633X16674087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Tieu L, Sarkar U, Schillinger D. Barriers and facilitators to online portal use among patients and caregivers in a safety net health care system: a qualitative study. J Med Internet Res. 2015;17(12):e275. doi: 10.2196/jmir.4847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Venkatesh M, Davis D. User acceptance of information technology: toward a unified view. Manage Inf Syst Q. 2003;27(03):425. [Google Scholar]
- 114.Davis F D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. Manage Inf Syst Q. 1989;13(03):319. [Google Scholar]
- 115.Venkatesh V, Davis F D. A theoretical extension of the technology acceptance model: four longitudinal field studies. Manage Sci. 2000;46(02):186–204. [Google Scholar]
- 116.Tavares J, Goulão A, Oliveira T. Electronic health record portals adoption: empirical model based on UTAUT2. Inform Health Soc Care. 2018;43(02):109–125. doi: 10.1080/17538157.2017.1363759. [DOI] [PubMed] [Google Scholar]
- 117.Vanneste D, Vermeulen B, Declercq A. Healthcare professionals' acceptance of BelRAI, a web-based system enabling person-centred recording and data sharing across care settings with interRAI instruments: a UTAUT analysis. BMC Med Inform Decis Mak. 2013;13(01):129. doi: 10.1186/1472-6947-13-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.An J-Y, Hayman L L, Panniers T, Carty B. Theory development in nursing and healthcare informatics: a model explaining and predicting information and communication technology acceptance by healthcare consumers. ANS Adv Nurs Sci. 2007;30(03):E37–E49. doi: 10.1097/01.ANS.0000286628.92386.40. [DOI] [PubMed] [Google Scholar]
- 119.Jimenez G, Spinazze P, Matchar D. Digital health competencies for primary healthcare professionals: a scoping review. Int J Med Inform. 2020;143:104260. doi: 10.1016/j.ijmedinf.2020.104260. [DOI] [PubMed] [Google Scholar]
- 120.Tsekleves E, Darby A, Whicher A, Swiatek P. Co-designing design fictions: a new approach for debating and priming future healthcare technologies and services. Arch Des Res. 2017;30(02):5–21. [Google Scholar]
- 121.Aryana B, Brewster L, Nocera J A. Design for mobile mental health: an exploratory review. Health Technol (Berl) 2019;9(04):401–424. [Google Scholar]
- 122.Holden R J, Karanam Y LP, Cavalcanti L H. Health information management practices in informal caregiving: an artifacts analysis and implications for IT design. Int J Med Inform. 2018;120:31–41. doi: 10.1016/j.ijmedinf.2018.09.017. [DOI] [PubMed] [Google Scholar]
- 123.Afzal A, Stolee P, Heckman G A, Boscart V M, Sanyal C. The role of unregulated care providers in Canada-A scoping review. Int J Older People Nurs. 2018;13(03):e12190. doi: 10.1111/opn.12190. [DOI] [PubMed] [Google Scholar]
- 124.Peek S TM, Wouters E JM, van Hoof J, Luijkx K G, Boeije H R, Vrijhoef H JM. Factors influencing acceptance of technology for aging in place: a systematic review. Int J Med Inform. 2014;83(04):235–248. doi: 10.1016/j.ijmedinf.2014.01.004. [DOI] [PubMed] [Google Scholar]
- 125.Moloney J, Abbas R, Beecham S, Ahmad B, Richardson I.Challenges and Opportunities for Caregiving through Information and Communication TechnologyIn: Proceedings of the 13th International Joint Conference on Biomedical Engineering Systems and Technologies. SCITEPRESS - Science and Technology Publications;2020329–336.
- 126.Innes A, Morgan D, Kosteniuk J. Dementia care in rural and remote settings: a systematic review of informal/family caregiving. Maturitas. 2011;68(01):34–46. doi: 10.1016/j.maturitas.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 127.Benefield L E, Beck C. Reducing the distance in distance-caregiving by technology innovation. Clin Interv Aging. 2007;2(02):267–272. [PMC free article] [PubMed] [Google Scholar]
- 128.Tassé M J, Wagner J B, Kim M. Using technology and remote support services to promote independent living of adults with intellectual disability and related developmental disabilities. J Appl Res Intellect Disabil. 2020;33(03):640–647. doi: 10.1111/jar.12709. [DOI] [PubMed] [Google Scholar]
- 129.Ikeda Y, Kobayakawa M, Nakao H, Iseki F, Matsushita H. Switzerland: Springer Nature; 2021. Information Technology/Artificial Intelligence Innovations Needed for Better Quality of Life in Caregiving Homes; pp. 37–58. [Google Scholar]
- 130.Merkel S, Kucharski A. Participatory design in gerontechnology: a systematic literature review. Gerontologist. 2019;59(01):e16–e25. doi: 10.1093/geront/gny034. [DOI] [PubMed] [Google Scholar]
- 131.Neumann-Podczaska A, Seostianin M, Madejczyk K. An experimental education project for consultations of older adults during the pandemic and healthcare lockdown. Healthcare (Basel) 2021;9(04):425. doi: 10.3390/healthcare9040425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Tuijt R, Rait G, Frost R, Wilcock J, Manthorpe J, Walters K. Remote primary care consultations for people living with dementia during the COVID-19 pandemic: experiences of people living with dementia and their carers. Br J Gen Pract. 2021;71(709):e574–e582. doi: 10.3399/BJGP.2020.1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Greenberg N E, Wallick A, Brown L M.Impact of COVID-19 pandemic restrictions on community-dwelling caregivers and persons with dementia Psychol Trauma 202012(S1):S220–S221. [DOI] [PubMed] [Google Scholar]
- 134.Shang J, Chastain A M, Perera U GE. COVID-19 preparedness in US home health care agencies. J Am Med Dir Assoc. 2020;21(07):924–927. doi: 10.1016/j.jamda.2020.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Egan K. Digital technology, health and well-being and the COVID-19 pandemic: it's time to call forward informal carers from the back of the queue. Semin Oncol Nurs. 2020;36(06):151088. doi: 10.1016/j.soncn.2020.151088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Goodman-Casanova J M, Dura-Perez E, Guzman-Parra J, Cuesta-Vargas A, Mayoral-Cleries F. Telehealth home support during COVID-19 confinement for community-dwelling older adults with mild cognitive impairment or mild dementia: survey study. J Med Internet Res. 2020;22(05):e19434. doi: 10.2196/19434. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.