

Abstract
An increasing number of countries have set tobacco endgame goals that target dramatic reduction in smoking prevalence. To achieve those targets and promote health equity, policies are needed to reduce the retail supply and visibility of tobacco products. Focusing on retailer reduction strategies and tobacco display bans, this special communication reviews solution-oriented research about the retail environment. It highlights examples of policy implementation and identifies data needs and research gaps for designing and evaluating retail policies to promote population health equitably.
Keywords: Endgame, Environment, Disparities, Priority/special populations, Advertising and Promotion
Background
To continue progress in decreasing cigarette smoking and tobacco use, the tobacco control community has made a global call for a tobacco endgame strategies, described as “initiatives designed to change/eliminate permanently the structural, political and social dynamics that sustain the tobacco epidemic, in order to end it within a specific time.”1 Several countries have established endgame goals to reduce smoking prevalence to 5% or lower, including, Hong Kong (by 2022), Ireland (2025), New Zealand (2025), Scotland (2034), and Wales (2040).2 The United States Department of Health and Human Services specified the same target by 2030,3 absent any mention of a tobacco endgame or ending the tobacco epidemic altogether.
Tobacco Retailer Availability & Product Displays
The past decade of tobacco control research has been marked by greater attention to aspects of place, including the tobacco retail environment, as a critical focus of policy interventions to help countries reach endgame targets.2, 4–6 Tobacco retailer availability captures the retail supply of tobacco products by measuring the concentration of tobacco retailers within a geographic area (density) as well as the distance (proximity) between a tobacco retailer and points of interest (e.g., households, schools, other tobacco retailers).7 A meta-analysis of 11 studies from 6 countries (Australia, Canada, India, New Zealand, Scotland, USA) about youth tobacco use found that greater retailer density near homes was associated with higher odds of past-month cigarette smoking (OR=1.08, 95% CI 1.04 to 1.13).8 In addition, a meta-analysis of 27 studies from 6 Organization for Economic Cooperation and Development countries (Australia, Canada, Finland, New Zealand, UK, USA) about adult tobacco use indicated that reductions in tobacco retailer density and proximity were associated with an estimated 2.5% reduction (95% CI 1.95 to 3.02) in the relative risk of tobacco use.9 Importantly, many of the associations were evident even after controlling for various individual-level and area-level covariates.8, 9
In many countries, the omnipresence of tobacco retailers implies widespread exposure to point-of-sale marketing (e.g., advertisements, price promotions, product displays). Two systematic reviews of studies from 8 countries (Australia, Canada, England, Ireland, New Zealand, Norway, United Kingdom [UK], USA) concluded that greater exposure to such marketing was associated with greater susceptibility to smoking, initiation, cravings for cigarettes, and impulse purchases.10, 11 Additionally, a meta-analysis of 13 studies (10 from USA and 3 from Japan, New Zealand, UK) found that youth with greater exposure to retail tobacco marketing had 1.61 times the odds (95% CI 1.33 to 1.96) of smoking and 1.32 times (95% CI 1.09 to 1.61) the odds of smoking susceptibility.12 As the authors note, a preponderance of cross-sectional studies (11 of 13) raises concern about reverse causation.12 However, this is unlikely to explain evidence of positive associations between incidental exposure to retail tobacco marketing and greater susceptibility to smoke among never users.12 Notably, pooled associations for smoking and susceptibility outcomes were larger for studies from countries where tobacco displays were the only form retail marketing than from countries where stores also contain tobacco advertising, indicating that comprehensive bans on tobacco displays as well as advertising are likely most effective to prevent tobacco use.12
Prioritizing Health Equity
Racism and discriminatory systems (e.g., residential segregation) have resulted in the stratification of people by sociodemographic characteristics as well as the inequitable distribution of health-promoting and health-harming resources across space.13–18 In the USA, tobacco retailers concentrate disproportionately in neighborhoods with a higher proportion of Black and Latino or Hispanic residents as well as neighborhoods with lower socioeconomic status and those with a greater concentration of same-sex couples.19–24 The past decade of research confirmed that a pattern of greater tobacco availability in areas of socioeconomic disadvantage is not unique to the USA but also evident in Australia, Canada, Germany, Scotland and elsewhere.25–28 Not surprisingly, differential exposures to point-of-sale tobacco marketing follow similar patterns. A systematic review of 43 studies (33 from the USA and 10 from Australia, Canada, Guatemala, Argentina, India, New Zealand, UK) documented widespread racial and socioeconomic inequities in exposure.29 That availability of tobacco retailers and visibility of tobacco marketing are inequitably distributed across neighborhoods may contribute to persistent inequities in tobacco use. Therefore, policies are needed to reduce tobacco retail availability and marketing everywhere, and particularly in communities that are disproportionately affected. In addition, research is needed to identify retail policies with the greatest potential for pro-equity impacts that would narrow or eliminate existing inequities in tobacco use and tobacco-related disease.
This Special Communication focuses on policies that aim to reduce tobacco supply (retailer availability) and visibility (product displays) because brick-and-mortar stores remain the primary source for tobacco product purchasing among adults30, 31 and a primary source for youth.32 In addition, the retail environment remains the dominant channel for tobacco industry marketing.33–35 We present a brief overview of retailer reduction and tobacco display policies, discuss considerations for design and implementation, and provide recommendations for future research and practice. Other important retail strategies (e.g., non-tax mechanisms to increase price, increasing the minimum legal sales age, restricting flavored tobacco) are discussed in the “Tobacco and social justice” issue of Tobacco Control.4, 36
Reducing supply: Tobacco retailer availability
An oversupply of tobacco exists wherever there are more tobacco retailers than necessary to meet consumer demand. For example, Figure 1 compares the number of retailers per 10,000 US adults who reported past-month use of prescription drugs, alcohol and tobacco. Retail supply was 10 times greater for tobacco than prescription drugs and more than two times greater for tobacco than alcohol. Presumably an oversupply of tobacco retailers is not unique to the USA, and comparative data for other countries would be informative.
Figure 1. Retail supply for prescription drugs, alcohol, and tobacco (number of retailers per 10,000 past-month product users), United States.
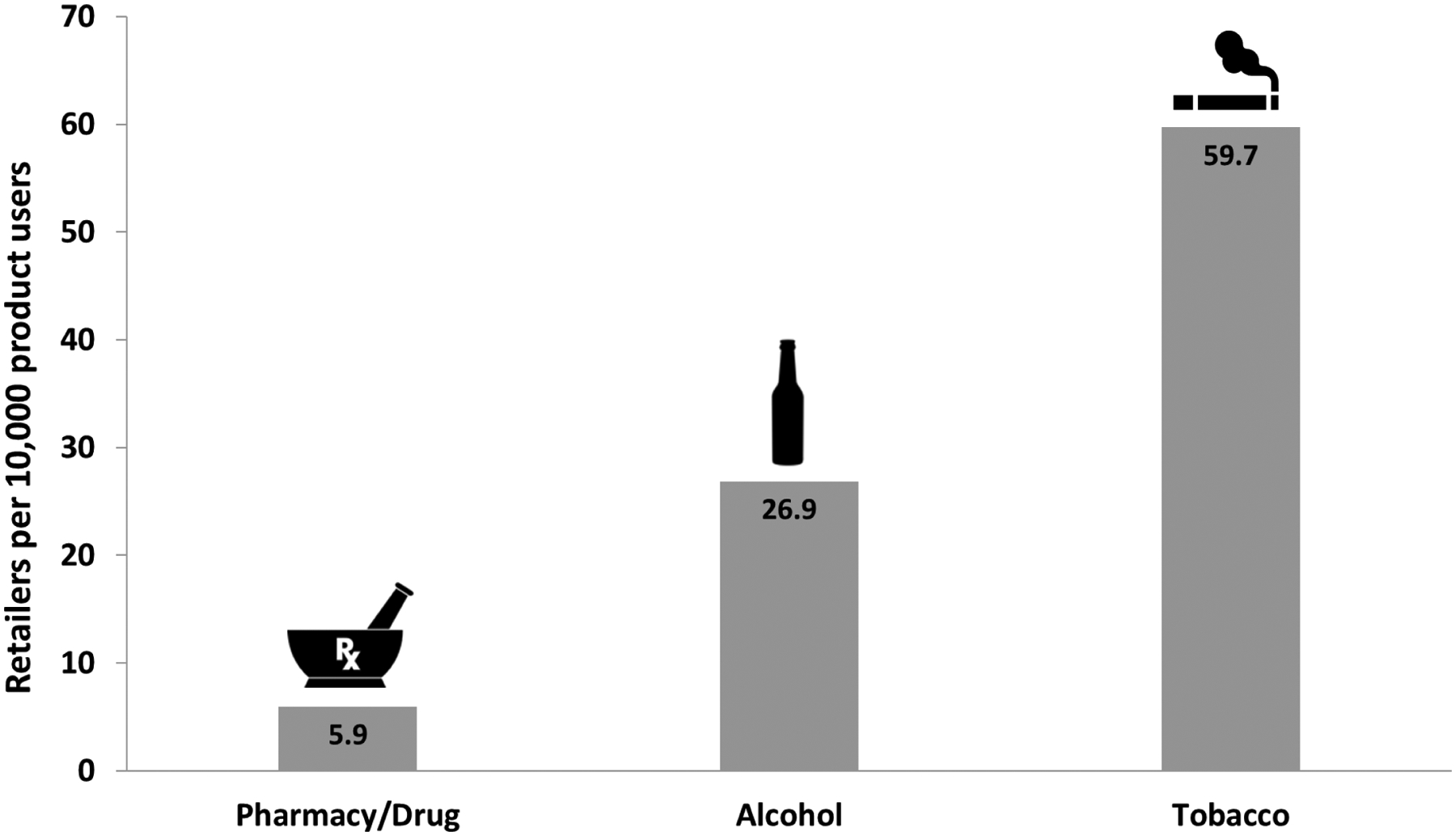
Data Sources: 1) Pharmacy/Drug: U.S. National Pharmacy Market Summary, 2019; OneKey by IQVIA; National Health and Nutrition Examination Survey, 2015–2018; National Center for Health Statistics; 2) Alcohol: Beverage Information Group Factbook, 2019; National Survey on Drug Use and Health, 2019; Center for Behavioral Health Statistics and Quality; 3) Tobacco: Reference USA, 2018; see Kong et al.23; National Survey on Drug Use and Health, 2019; Center for Behavioral Health Statistics and Quality
Limiting sales of commercial tobacco products
One retail strategy to reduce tobacco retailer availability is to end the sale of commercial tobacco products altogether.37–39 The state of California (USA) set an endgame goal to accomplish this by 2035,40 and local policies are leading the way, as in Beverly Hills41 and Manhattan Beach.42 These early adopters are high-income and predominately non-Hispanic white communities, which raises concerns about equity impacts. Therefore, tracking policy diffusion is important to determine what proportion of populations defined by high rates of tobacco use and tobacco-related disease are covered by retail policies.43
Bhutan was the first country to end tobacco sales but suspended its policy during the COVID-19 pandemic.44 In response to the pandemic, several countries introduced temporary bans on sales of tobacco products, including South Africa, Botswana, and India.45 According to a survey in South Africa, 93% of individuals who currently smoked reported being able to purchase cigarettes during the ban, indicating the need for stronger enforcement and perhaps certain preconditions (e.g., less than 10% smoking prevalence)39 before implementing such a ban.45
Other strategies to reduce tobacco retail availability
Retail reduction policies limit the quantity, location, and/or type of stores that can sell tobacco. Strategies include capping the number of retailers, prohibiting tobacco sales near schools or parks/playgrounds, maximizing the distance between tobacco retailers, and restricting which types of stores are eligible to sell tobacco.46, 47 For example, the Netherlands plans to reduce tobacco retailers from 16,000 to 6000 by first phasing out tobacco vending machines by 2022 and ending tobacco sales in supermarkets by 2024.48 In Hungary, sales were restricted to government licensed National Tobacco Shops in 2013, which was projected to reduce the number of tobacco retailers from 42,000 to just 7000.49 Many countries require tobacco-free pharmacies44 and Iceland considered limiting tobacco sales to pharmacies by prescription after failed cessation attempts.50, 51
Simulation studies model the hypothetical impact of retailer reduction policies on availability overall and on inequities in retailer availability by race, ethnicity, socioeconomic status, and rurality.52 For example, restricting tobacco sales to 50% of all liquor stores in New Zealand would result in the highest estimated reduction in smoking and net health costs savings, with greater gains for Māori people compared to non-Māori people.53 Additionally, a simulation study in Queensland (Australia) indicated that adult daily smoking prevalence would decrease by 0.65 percentage points from 2018 to 2037 if alcohol retailers are required to have a license to sell tobacco products.54 In Scotland, simulations that removed tobacco product sales in some store types (liquor, pharmacy) reduced retail density by 75–86%; however, these policies exacerbated socioeconomic inequities in density.55 Notably, only an explicitly equity-oriented policy (i.e. strategically prohibiting specific types of retailers that are more common in neighborhoods with higher socioeconomic deprivation from selling tobacco) eliminated socioeconomic inequities in retailer density.55 Of course, some policies can exacerbate inequities in some settings. For example, the existence of ―pharmacy deserts‖ in the USA56 suggests that implementing tobacco-free pharmacies (alone) would reduce tobacco retailer density more in neighborhoods with greater economic advantage and lower proportions of racially/ethnically minoritized groups.23, 57,58 However, simulations for the state of Ohio (USA) illustrated that implementing tobacco-free pharmacies in tandem with other policies (e.g., prohibiting tobacco retailers near schools) can result in a more equitable reduction in tobacco retailers across neighborhoods.58
Evaluations of policy implementation are much needed to complement simulations of hypothetical solutions. For example, San Francisco (California, USA) capped the number of tobacco licenses with an equity-oriented goal to achieve parity in the number tobacco retailers across supervisorial districts (min=37, max=180, goal=45).59 Between 2014 and 2019, there was a 24% reduction in tobacco licenses, and the greatest reduction was in the lowest-income neighborhood (32% reduction).60 After implementing similar strategies and increasing the tobacco retail licensing fee (from $50 to $300 in 2017), Philadelphia (Pennsylvania, USA) observed a 20.3% reduction in tobacco retailers within three years, and a significantly greater decline in density in lower-income districts.61 In South Australia, a 2007 license fee increase from $A12.90 to $A200 led to a 23.7% decrease in tobacco licenses over two years.62 Similarly, Finland’s 2017 license fee increase (maximum EUR 500 per cash register) was associated with a decrease from over 10,000 to 7250 tobacco licenses.63
Future Directions
Continued surveillance and further evaluations are needed to assess the impact of real-world tobacco retailer reduction policies on youth and adult tobacco use. For example, while a meta-analysis found that higher odds of past-month smoking among youth was associated with greater tobacco retailer density near home (not school),8 future research should evaluate other tobacco use outcomes, such as smoking susceptibility.12 Additionally, restricting tobacco retail proximity to schools is predicted to ameliorate or eliminate neighborhood inequities in retailer availability,55, 58, 64 which could benefit adults living near schools, as well.
Evidence of positive associations between tobacco retailer availability and tobacco-related disease is emerging, but the topic is understudied. In Australia, the odds of heart disease diagnosis and hospital admission for adults who smoke was greater for those who had more tobacco retailers within a mile of their home.65 Two California studies found that a higher number of tobacco retailers was associated with more hospitalizations for chronic obstructive pulmonary disease (COPD).66, 67 Similarly, greater tobacco retailer density in US counties was associated with a higher rate of COPD-related discharges, days spent in the hospital, and financial costs.68 In Baltimore City (Maryland, USA), census tracts with higher tobacco retailer density had significantly lower life expectancy, greater age-adjusted mortality, and greater rates of death from chronic respiratory disease.69 Across these studies, observed relationships persisted even after adjusting for individual-level (e.g., age, sex) and/or area-level (e.g., socioeconomic status, air pollution) factors.
Longitudinal studies are needed to disentangle the mechanisms of observed relationships between the retail environment, tobacco use, and tobacco-related disease. Further research is needed to provide evidence about how much and how quickly tobacco retailer reduction strategies can change the environment, affect tobacco use/cessation, and reduce tobacco-related disease, particularly among priority populations defined by higher tobacco use and a disproportionate burden of disease. In addition, studies that link potential policy impacts to health care costs/savings could promote public/political support and encourage policy adoption.70
While home and school neighborhoods have been primary environments for studying retailer availability, they likely underestimate individuals’ exposure to tobacco retailers and marketing across time and space. A growing body of research using Global Position Systems (GPS) methodologies can better capture real-time environmental exposure to tobacco retailers in individuals’ activity spaces. For example, in Montreal (Canada), measuring the number of tobacco retailers and their proximity in young adults’ activity space were both associated with current smoking (vs. not).71 Only the count (not proximity) of tobacco retailers near home was associated with smoking status, perhaps because young adults rely on multiple retailers, not necessarily the closest one.71 Studies comparing how measures of retailer availability differ are much needed, including which measures best identify neighborhood inequities and explain tobacco acquisition and consumption.23 To inform tobacco control practice, measures of tobacco retailer availability that can be easily calculated, communicated, and tracked over time should also be prioritized.
Reducing visibility: Tobacco point-of-sale display bans
In 2018, 72% of parties to World Health Organization’s (WHO) Framework Convention on Tobacco Control reported having a comprehensive ban on tobacco advertising, promotion, and sponsorship (TAPS), although the WHO noted that countries’ definition of comprehensive may not meet FCTC guidelines.72 Of these 131 countries, 60% reported tobacco point-of-sale display bans.72 According to the Tobacco Control Laws database maintained by the Campaign for Tobacco-Free Kids (see Figure 2), 38 countries have comprehensive display bans and partial bans exist in 42 countries (e.g., Brazil allows pack displays but prohibits branding and advertising on the display itself).44 Notably, support for display bans remains high in countries with such policies, even among individuals who smoke.73, 74
Figure 2. Countries with total, partial, and no tobacco display bans.
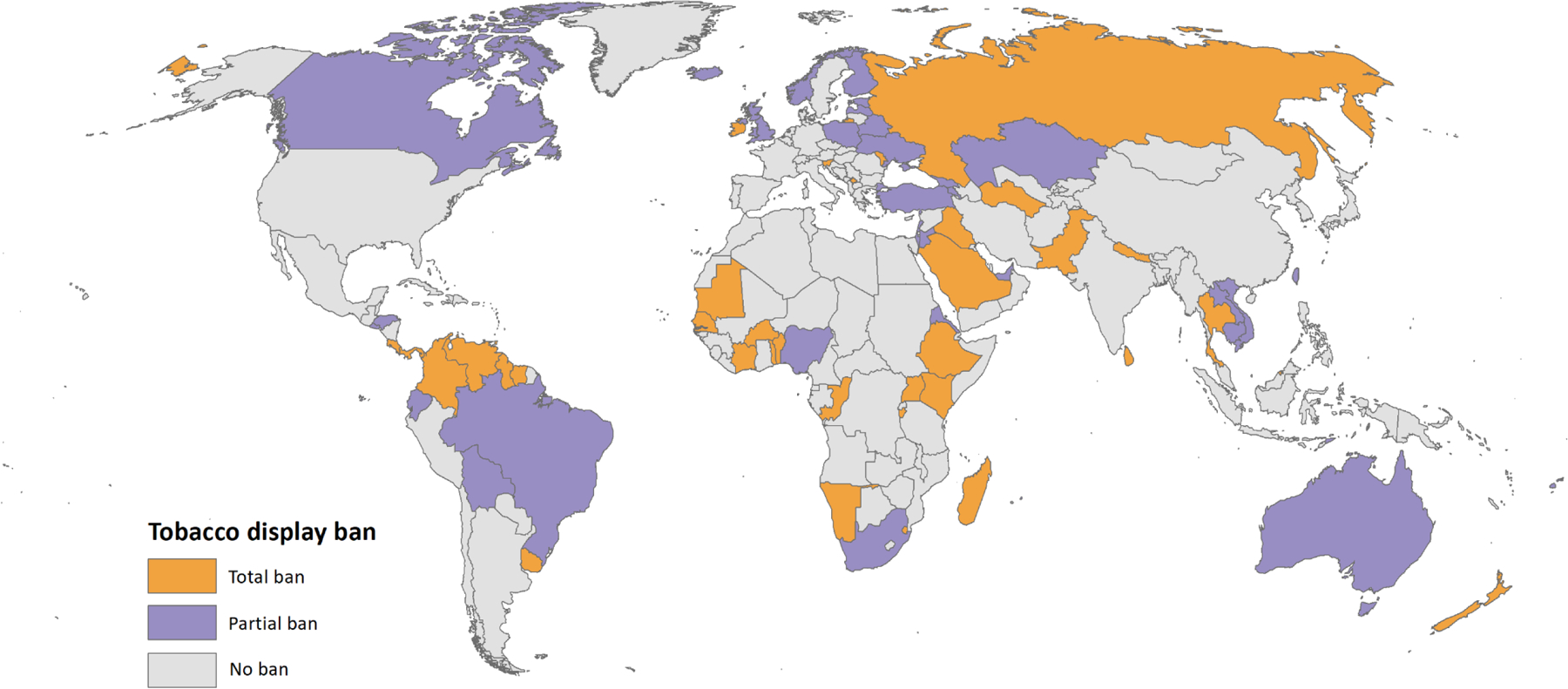
Note: Data were downloaded December 2021 from the Tobacco Control Laws database maintained by the Campaign for Tobacco-Free Kids.44
Evaluations of tobacco display bans
Evaluations demonstrate the efficacy of tobacco display bans for tobacco control. A longitudinal analysis of data from 77 countries estimated that implementing a display ban decreased overall adult daily smoking prevalence by 7%.75 After Ireland’s 2009 tobacco display ban, retail compliance was high, and recall of displays decreased among both adults and teenagers.74 Additionally, following Ireland’s 2009 display ban, there was no direct short-term economic impact on small retailers that resulted in revenue losses and closures.76 Within 6–12 months of implementing display bans in New South Wales and Queensland (Australia), youth and young adults were less likely to recall seeing displays, brand awareness, over-estimate peer smoking, and less likely to report current smoking.77 Following the 2010 display ban in Western Australia, there was a 30% reduction in spontaneous tobacco purchases reported by adults who smoked daily.78 Evidence from studies that manipulate exposure to tobacco displays in brick-and-mortar or online stores provide complementary evidence of the rationale for display bans. For example, youth exposed to tobacco ‘power walls’ were more likely to report smoking susceptibility and higher normative perceptions of smoking.79, 80
Even when tobacco displays are removed, adults who currently smoke or formerly smoked reported that mere exposure to a tobacco retailer, including its shelving units or price boards, can prompt impulse purchases and urges to smoke cigarettes.81 In Australia and Scotland, the tobacco industry used retailer incentives (e.g., price discounts, gifts) in exchange for retailers listing and recommending specific tobacco products on pricing lists as well as maintaining stock levels.82, 83 Such industry tactics promote inequities: for example, Australian stores in areas with lower socioeconomic status listed more discount brands at the top of price boards.84 Additionally, a systematic review of 20 studies from 4 countries (Australia, Scotland, UK, USA) found consistent evidence of lower cigarette prices in neighborhoods characterized by socioeconomic disadvantage, and higher populations of youth and Black residents.85
Future Directions
Continued surveillance and evaluation where display bans are implemented is important. Such research should track compliance, study industry tactics to circumvent bans, and evaluate policy impact on initiation, use, and cessation. Although accurate knowledge of where tobacco retailers are located is essential for these tasks, adequate data do not exist globally. Indeed, many countries do not require tobacco retail licensing. For example, just 38 of 50 US states,86 6 of 8 Australian states87 and five countries in the European Union (Finland, France, Hungary, Italy, Spain)88 have established tobacco retail licensing schemes. Accurate and updated national and sub-national licensing systems are greatly needed.89 Such data would allow governments and researchers to better monitor the impact of retail policies on eliminating, ameliorating, or exacerbating neighborhood inequities in tobacco supply, visibility, and tobacco use.
Studies that employ multiple methods may better explain the associations between tobacco retailer availability, exposure to displays and marketing, and tobacco use. For example, geographic ecological momentary assessment (GEMA) tracks where and how often youth and adult tobacco users are exposed to tobacco retailers (with GPS) in combination with real-time, self-reported tobacco use and/or cravings experienced in the retail environment (with Ecological Momentary Assessment [EMA]).90–93 Using GEMA, one study mapped where and when bisexual young adults smoke, and then showed participants the geotagged locations in qualitative interviews about their tobacco use behaviors and experiences at these locations to better understand how surrounding contexts may have contributed to use.94 EMA and GEMA are also used to document real-time exposure to retail tobacco marketing as well as inequities in exposure.95, 96 Eye tracking and functional magnetic resonance imaging MRI (fMRI) would also improve researchers’ understanding of how tobacco displays and other retail marketing stimulate craving and deter cessation.97 For example, research that combined GPS tracking to identify which tobacco retailers participants encountered, and fMRI showing participants tobacco storefronts they visited and did not visit, observed differential neurobiological responses to more frequently visited tobacco storefronts.98 Integrating novel methods may provide better insight on causal and modifiable mechanisms that perpetuate tobacco use, including tobacco displays, price discounts, as well as branded and unbranded tobacco cues in the retail environment.
Conclusion
Given observed inequities in tobacco retailer availability and displays/marketing, strategies that limit tobacco supply and visibility show promise for reducing tobacco use, tobacco-related disease, and importantly, for reducing inequities in these outcomes. Governments should address strategies to regulate the tobacco retail environment as part of a comprehensive approach to tobacco control and prioritize equity-oriented goals. For example, New Zealand’s Smokefree Aotearoa 2025 Action Plan will “only allow smoked tobacco products to be sold by authorized retailers, to: significantly reduce the current number of retailers and ensure retail supply is not concentrated in New Zealand’s most deprived neighbourhoods.”99 Additionally, the government set a goal for daily smoking prevalence of 5% or less among all population groups. To establish and reach equity-oriented goals, ongoing assessment and evaluation of policy solutions to reduce tobacco availability and visibility are much needed in places and among communities that bear the greatest burden of tobacco. This is especially important to ensure that policies do not unintentionally exacerbate inequities in the retail environment.
These recommendations are underscored by increased attention to corporate or commercial determinants of health100 (defined as “strategies and approaches used by the private sector to promote products and choices that are detrimental to health”101). This includes the tobacco industry’s strategies to sustain an oversupply of tobacco products at multiple stages of the supply chain (e.g., agriculture, manufacturing).102 More evidence is needed to refute tobacco industry opposition to retail regulation,103, 104 including studies that debunk industry “footfall” claims about tobacco driving customers to stores and highlight success of retailers who abandon tobacco sales.105–107 Indeed, studies from Australia, New Zealand, and the USA found that sales transactions with tobacco products represented a smaller fraction than industry estimates, and tobacco manufacturers and retailer associations overstate retail profits from tobacco.108–112 Further evidence to refute industry claims may encourage retailers to abandon tobacco and transition to more profitable product lines,113 reducing both the oversupply and visibility of tobacco products. Additionally, policies that prohibit tobacco industry contracts and incentives to promote and sell tobacco products in the retail setting are needed.34, 35
Although this commentary focused on conventional tobacco products and retailers, endgame plans will need to address a proliferation of other nicotine products (e.g., e-cigarettes, heated tobacco, nicotine pouches and products derived from synthetic nicotine) as well as vape shops and online sales.51, 99, 114, 115 Endgame strategies and equity-oriented retail solutions will benefit from collaborations between community members, policymakers and interdisciplinary research teams, including those from tobacco control, public health/policy, health economics, psychology, communications, and geography. These teams are needed to design, implement, and track effective retail policies that prioritize populations experiencing the greatest burden of tobacco use and tobacco-related disease.
What this paper adds.
Tobacco retailer availability and product displays are associated with youth and adult tobacco use behaviors.
An oversupply of tobacco retailers and their disproportionate concentration in some communities may exacerbate tobacco use inequities.
Accumulating evidence suggests that reducing retailer availability and exposure to product display bans may reduce tobacco use behaviors.
Continued progress toward global tobacco endgame targets requires innovative research and continued evaluations of the real-world implementation of retail policies, particularly evaluations of the potential for pro-equity impacts that would narrow or eliminate existing inequities in tobacco use and tobacco-related disease.
Acknowledgements
We are grateful to Trent Johnson and Lindsey Winn (Stanford Prevention Research Center) for assistance with creating the Figures, and to Jaana Kinnunen (Tampere University, Finland) and David Timberlake (University of California, Irvine) for providing information about tobacco licensing in Finland.
Funding
Dr. Kong is supported by the National Cancer Institute of the National Institutes of Health (P30CA225520) and the Oklahoma Tobacco Settlement Endowment Trust (TSET R21-02). Dr. Henriksen is supported by the National Cancer Institute of the National Institutes of Health (P01CA225597). The funders had no role in any aspect of the study design, data analysis and interpretation, writing of the manuscript, or decision to publish.
Footnotes
Competing Interests
Dr. Kong serves as a paid expert consultant in litigation against tobacco companies.
References
- 1.Malone RE, McDaniel PA, Smith EA. Tobacco control endgames: global initiatives and implications for the UK. 2014, https://www.cancerresearchuk.org/sites/default/files/policy_july2014_fullendgame_report.pdf
- 2.Moon G, Barnett R, Pearce J, Thompson L, Twigg L. The tobacco endgame: The neglected role of place and environment. Health Place. Sep 2018;53:271–278. doi: 10.1016/j.healthplace.2018.06.012 [DOI] [PubMed] [Google Scholar]
- 3.Healthy People 2030: Reduce current cigarette smoking in adults — TU-02. U. S. Department of Health and Human Services; Office of Disease Prevention and Health Promotion. Accessed October 20, 2021. https://health.gov/healthypeople/objectives-and-data/browse-objectives/tobacco-use/reduce-current-cigarette-smoking-adults-tu-02 [Google Scholar]
- 4.Kong AY, King BA. Boosting the Tobacco Control Vaccine: recognizing the role of the retail environment in addressing tobacco use and disparities. Tobacco Control. 2020:tobaccocontrol-2020–055722. doi: 10.1136/tobaccocontrol-2020-055722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Henriksen L Comprehensive tobacco marketing restrictions: promotion, packaging, price and place. Tobacco Control. 2012;21(2):147. doi: 10.1136/tobaccocontrol-2011-050416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Henriksen L The retail environment for tobacco: a barometer of progress towards the endgame. Tobacco Control. 2015;24(e1):e1. doi: 10.1136/tobaccocontrol-2014-051884 [DOI] [PubMed] [Google Scholar]
- 7.Kong AY, Myers AE, Isgett LF, Ribisl KM. Neighborhood racial, ethnic, and income disparities in accessibility to multiple tobacco retailers: Mecklenburg County, North Carolina, 2015. Preventive Medicine Reports. 2020;17 doi: 10.1016/j.pmedr.2019.101031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Finan LJ, Lipperman-Kreda S, Abadi M, et al. Tobacco outlet density and adolescents’ cigarette smoking: a meta-analysis. Tobacco control. 2019;28(1):27–33. doi: 10.1136/tobaccocontrol-2017-054065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lee JG, Kong AY, Sewell KB, et al. Associations of tobacco retailer density and proximity with adult tobacco use behaviours and health outcomes: a meta-analysis. Tobacco Control. 2021, [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Paynter J, Edwards R. The impact of tobacco promotion at the point of sale: a systematic review. Nicotine Tob Res. 2009;11:25–35. doi: 10.1093/ntr/ntn002 [DOI] [PubMed] [Google Scholar]
- 11.Robertson L, McGee R, Marsh L, Hoek J. A systematic review on the impact of point-of-sale tobacco promotion on smoking. Nicotine Tob Res. Jan 2015;17(1):2–17. doi: 10.1093/ntr/ntu168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Robertson L, Cameron C, McGee R, Marsh L, Hoek J. Point-of-sale tobacco promotion and youth smoking: a meta-analysis. Tobacco Control. 2016;25(e2):e83. doi: 10.1136/tobaccocontrol-2015-052586 [DOI] [PubMed] [Google Scholar]
- 13.Diez Roux AV, Mair C. Neighborhoods and health. Ann N Y Acad Sci. Feb 2010;1186:125–45. doi: 10.1111/j.1749-6632.2009.05333.x [DOI] [PubMed] [Google Scholar]
- 14.Lipsitz G The Racialization of Space and the Spatialization of Race: Theorizing the Hidden Architecture of Landscape. Landscape Journal. 2007;26(1):10–23. http://www.jstor.org/stable/43323751 [Google Scholar]
- 15.Williams DR, Collins C. Racial Residential Segregation: A Fundamental Cause of Racial Disparities in Health. Public Health Reports. 2001;116(5):404–416. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1497358/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Williams DR, Lawrence JA, Davis BA. Racism and Health: Evidence and Needed Research. Annual Review of Public Health. 2019/04/01 2019;40(1):105–125. doi: 10.1146/annurev-publhealth-040218-043750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Phelan JC, Link BG. Is Racism a Fundamental Cause of Inequalities in Health? Annual Review of Sociology. 2015/08/14 2015;41(1):311–330. doi: 10.1146/annurev-soc-073014-112305 [DOI] [Google Scholar]
- 18.Phelan JC, Link BG, Tehranifar P. Social Conditions as Fundamental Causes of Health Inequalities: Theory, Evidence, and Policy Implications. Journal of Health and Social Behavior. 2010/03/01 2010;51(1_suppl):S28–S40. doi: 10.1177/0022146510383498 [DOI] [PubMed] [Google Scholar]
- 19.Lee JGL, Sun DL, Schleicher NM, Ribisl KM, Luke DA, Henriksen L. Inequalities in tobacco outlet density by race, ethnicity and socioeconomic status, 2012, USA: results from the ASPiRE Study. J Epidemiol Community Health. May 2017;71(5):487–492. doi: 10.1136/jech-2016-208475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rodriguez D, Carlos HA, Adachi-Mejia AM, Berke EM, Sargent J. Retail tobacco exposure: using geographic analysis to identify areas with excessively high retail density. Nicotine Tob Res. Feb 2014;16(2):155–65. doi: 10.1093/ntr/ntt126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rodriguez D, Carlos HA, Adachi-Mejia AM, Berke EM, Sargent JD. Predictors of tobacco outlet density nationwide: a geographic analysis. Tob Control. Sep 2013;22(5):349–55. doi: 10.1136/tobaccocontrol-2011-050120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kong AY, Delamater PL, Gottfredson NC, Ribisl KM, Baggett CD, Golden SD. Sociodemographic inequities in tobacco retailer density: Do neighboring places matter? Health & Place. 2021;71:102653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kong AY, Delamater PL, Gottfredson NC, Ribisl KM, Baggett CD, Golden SD. Neighborhood Inequities in Tobacco Retailer Density and the Presence of Tobacco-Selling Pharmacies and Tobacco Shops. Health Education & Behavior. 2021:10901981211008390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lee JGL, Pan WK, Henriksen L, Goldstein AO, Ribisl KM. Is There a Relationship Between the Concentration of Same-Sex Couples and Tobacco Retailer Density? Nicotine & Tobacco Research. 2016;18(2):147–155. doi: 10.1093/ntr/ntv046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chaiton MO, Mecredy GC, Cohen JE, Tilson ML. Tobacco retail outlets and vulnerable populations in Ontario, Canada. Int J Environ Res Public Health. Dec 17 2013;10(12):7299–309. doi: 10.3390/ijerph10127299 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shortt NK, Tisch C, Pearce J, et al. A cross-sectional analysis of the relationship between tobacco and alcohol outlet density and neighbourhood deprivation. BMC Public Health. 2015/10/05 2015;15(1):1014. doi: 10.1186/s12889-015-2321-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schneider S, Gruber J. Neighbourhood deprivation and outlet density for tobacco, alcohol and fast food: first hints of obesogenic and addictive environments in Germany. Public health nutrition. Jul 2013;16(7):1168–77. doi: 10.1017/s1368980012003321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wood LJ, Pereira G, Middleton N, Foster S. Socioeconomic area disparities in tobacco retail outlet density: a Western Australian analysis. The Medical journal of Australia. May 20 2013;198(9):489–91. doi: 10.5694/mja12.11539 [DOI] [PubMed] [Google Scholar]
- 29.Lee JGL, Henriksen L, Rose SW, Moreland-Russell S, Ribisl KM. A Systematic Review of Neighborhood Disparities in Point-of-Sale Tobacco Marketing. American Journal of Public Health. 2015/09/01 2015;105(9):e8–e18. doi: 10.2105/AJPH.2015.302777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Groom AL, Cruz-Cano R, Mead EL, et al. Tobacco Point-of-Sale Influence on U.S. Adult Smokers. J Health Care Poor Underserved. 2020;31(1):249–264. doi: 10.1353/hpu.2020.0021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kruger J, Jama A, Lee JGL, et al. Point-of-sale cigarette purchase patterns among U.S. adult smokers—National Adult Tobacco Survey, 2012–2014. Preventive Medicine. 2017/08/01/ 2017;101:38–43. doi: 10.1016/j.ypmed.2017.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tanski S, Emond J, Stanton C, et al. Youth Access to Tobacco Products in the United States: Findings From Wave 1 (2013–2014) of the Population Assessment of Tobacco and Health Study. Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco. 2019;21(12):1695–1699. doi: 10.1093/ntr/nty238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Federal Trade Commission Cigarette Report for 2020. Federal Trade Commission; 2021. Accessed December 1, 2021. https://www.ftc.gov/system/files/documents/reports/federal-trade-commission-cigarette-report-2020-smokeless-tobacco-report-2020/p114508fy20cigarettereport.pdf [Google Scholar]
- 34.Lavack AM, Toth G. Tobacco point-of-purchase promotion: examining tobacco industry documents. Tobacco Control. 2006;15(5):377. doi: 10.1136/tc.2005.014639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Watts C, Burton S, Freeman B. ‘The last line of marketing’: Covert tobacco marketing tactics as revealed by former tobacco industry employees. Global Public Health. 2021/07/03 2021;16(7):1000–1013. doi: 10.1080/17441692.2020.1824005 [DOI] [PubMed] [Google Scholar]
- 36.Malone RE. Justice, disparities and the tobacco endgame. Tobacco Control. 2021;30(e2):e76. doi: 10.1136/tobaccocontrol-2021-057188 [DOI] [PubMed] [Google Scholar]
- 37.Thomson G, Wilson N, Blakely T, Edwards R. Ending appreciable tobacco use in a nation: using a sinking lid on supply. Tobacco Control. 2010;19(5):431. doi: 10.1136/tc.2010.036681 [DOI] [PubMed] [Google Scholar]
- 38.Beaglehole R, Bonita R, Yach D, Mackay J, Reddy KS. A tobacco-free world: a call to action to phase out the sale of tobacco products by 2040. The Lancet. 2015;385(9972):1011–1018. doi: 10.1016/S0140-6736(15)60133-7 [DOI] [PubMed] [Google Scholar]
- 39.Smith EA, Malone RE. An argument for phasing out sales of cigarettes. Tobacco Control. 2020;29(6):703. doi: 10.1136/tobaccocontrol-2019-055079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Local Lead Agency Campaign to End Commercial Tobacco. California Tobacco Control Program, California Department of Public Health; 2021. Accessed December 22, 2021. https://www.trdrp.org/about/llaendgamecampaign_1-21-21_final.pdf [Google Scholar]
- 41.Beverly Hills city council approves prohibiting the sale of all tobacco products. City of Beverly Hills. Accessed January 3, 2020. http://www.beverlyhills.org/citymanager/newsroom/beverlyhillscitycouncilapprovesprohibitingthesaleofalltobaccoproducts/ [Google Scholar]
- 42.An Ordinance of the City of Manhattan Beach: ORDINANCE NO. 20–0007. City of Manhattan Beach; 2020. Accessed June 27, 2020. https://www.citymb.info/home/showdocument?id=41659 [Google Scholar]
- 43.Rose SW, Amato MS, Anesetti-Rothermel A, et al. Characteristics and Reach Equity of Policies Restricting Flavored Tobacco Product Sales in the United States. Health Promotion Practice. 2020/01/01 2020;21(1_suppl):44S–53S. doi: 10.1177/1524839919879928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tobacco Control Laws. Campaign for Tobacco-Free Kids; 2021. Accessed October 22, 2021. https://www.tobaccocontrollaws.org/ [Google Scholar]
- 45.Filby S, van der Zee K, van Walbeek C. The temporary ban on tobacco sales in South Africa: lessons for endgame strategies. Tobacco Control. 2021:tobaccocontrol-2020–056209. doi: 10.1136/tobaccocontrol-2020-056209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tobacco Retailer Density: Place-Based Strategies to Advance Health and Equity. ChangeLab Solutions; 2019. Accessed January 28, 2020. https://www.changelabsolutions.org/sites/default/files/CLS-BG214-Tobacco_Retail_Density-Factsheet_FINAL_20190131.pdf [Google Scholar]
- 47.Ackerman A, Etow A, Bartel S, Ribisl KM. Reducing the Density and Number of Tobacco Retailers: Policy Solutions and Legal Issues. Nicotine Tob Res. Feb 2017;19(2):133–140. doi: 10.1093/ntr/ntw124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dutch government outlaws supermarket cigarette sales from 2024. NL Times; 2020. Accessed October 21, 2021. https://nltimes.nl/2020/11/21/dutch-government-outlaws-supermarket-cigarette-sales-2024 [Google Scholar]
- 49.Caceres L, Chaiton M. Hungary: State Licensing for Tobacco Outlets. Tobacco Control. 08/12 2013;22:292–293. doi: 10.1136/tobaccocontrol-2013-051251 [DOI] [Google Scholar]
- 50.Petrovic-van der Deen FS, Blakely T, Kvizhinadze G, Cleghorn CL, Cobiac LJ, Wilson N. Restricting tobacco sales to only pharmacies combined with cessation advice: a modelling study of the future smoking prevalence, health and cost impacts. Tob Control. Nov 2019;28(6):643–650. doi: 10.1136/tobaccocontrol-2018-054600 [DOI] [PubMed] [Google Scholar]
- 51.McDaniel PA, Smith EA, Malone RE. The tobacco endgame: a qualitative review and synthesis. Tobacco Control. 2016;25(5):594. doi: 10.1136/tobaccocontrol-2015-052356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Glasser AM, Roberts ME. Retailer density reduction approaches to tobacco control: A review. Health & Place. 2021/01/01/ 2021;67:102342. doi: 10.1016/j.healthplace.2020.102342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Pearson AL, van der Deen FS, Wilson N, Cobiac L, Blakely T. Theoretical impacts of a range of major tobacco retail outlet reduction interventions: modelling results in a country with a smoke-free nation goal. Tobacco Control. 2015;24(e1):e32. doi: 10.1136/tobaccocontrol-2013-051362 [DOI] [PubMed] [Google Scholar]
- 54.Skinner A, Walker P, Atkinson J-A, et al. Policy options for endgame planning in tobacco control: a simulation modelling study. Tobacco Control. 2021;30(1):77. doi: 10.1136/tobaccocontrol-2019-055126 [DOI] [PubMed] [Google Scholar]
- 55.Caryl F, Shortt NK, Pearce J, Reid G, Mitchell R. Socioeconomic inequalities in children’s exposure to tobacco retailing based on individual-level GPS data in Scotland. Tobacco Control. 2020;29(4):367. doi: 10.1136/tobaccocontrol-2018-054891 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Qato DM, Daviglus ML, Wilder J, Lee T, Qato D, Lambert B. ‘Pharmacy Deserts’ Are Prevalent In Chicago’s Predominantly Minority Communities, Raising Medication Access Concerns. Health Affairs. 2014/11/01 2014;33(11):1958–1965. doi: 10.1377/hlthaff.2013.1397 [DOI] [PubMed] [Google Scholar]
- 57.Giovenco DP, Spillane TE, Mauro CM, Hernandez D. Evaluating the impact and equity of a tobacco-free pharmacy law on retailer density in New York City neighbourhoods. Tob Control. Aug 22 2018;doi: 10.1136/tobaccocontrol-2018-054463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Craigmile PF, Onnen N, Schwartz E, Glasser A, Roberts ME. Evaluating how licensing-law strategies will impact disparities in tobacco retailer density: a simulation in Ohio. Tobacco Control. 2020:tobaccocontrol-2020–055622. doi: 10.1136/tobaccocontrol-2020-055622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.San Francisco Tobacco-Free Project. Reducing Tobacco Retail Density in San Francisco: A Case Study. San Francisco Tobacco-Free Project; 2016. Accessed December 1, 2018. https://sanfranciscotobaccofreeproject.org/wp-content/uploads/Retail-Density-Case-Study-1.27.16-FINAL-to-TFP.pdf [Google Scholar]
- 60.Jessica Estrada DRS, Hu-Nguyen Alice, Boone Jacquelyn. Reducing unequal exposure to tobacco in retail environments: The San Francisco story of multiple policy approaches to reduce retail access and retail density. American Public Health Association’s 2019 Annual Meeting and Expo; 2019. Accessed October 21, 2021. https://apha.confex.com/apha/2019/meetingapi.cgi/Session/59147?filename=2019_Session59147.html&template=Word [Google Scholar]
- 61.Lawman HG. The Pro-Equity Potential of Tobacco Retailer Licensing Regulations in Philadelphia. American journal of public health. 2019;109(3):427–428. doi: 10.2105/AJPH.2018.304909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bowden JA, Dono J, John DL, Miller CL. What happens when the price of a tobacco retailer licence increases? Tobacco Control. 2014;23(2):178. doi: 10.1136/tobaccocontrol-2012-050615 [DOI] [PubMed] [Google Scholar]
- 63.Timberlake DS, Laitinen U, Kinnunen JM, Rimpela AH. Strategies and barriers to achieving the goal of Finland’s tobacco endgame. Tobacco Control. 2020;29(4):398. doi: 10.1136/tobaccocontrol-2018-054779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ribisl KM, Luke DA, Bohannon DL, Sorg AA, Moreland-Russell S. Reducing Disparities in Tobacco Retailer Density by Banning Tobacco Product Sales Near Schools. Nicotine Tob Res. Feb 2017;19(2):239–244. doi: 10.1093/ntr/ntw185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Barnes R, Foster SA, Pereira G, Villanueva K, Wood L. Is neighbourhood access to tobacco outlets related to smoking behaviour and tobacco-related health outcomes and hospital admissions? Prev Med. Jul 2016;88:218–23. doi: 10.1016/j.ypmed.2016.05.003 [DOI] [PubMed] [Google Scholar]
- 66.Lipton R, Banerjee A, Dowling KC, Treno AJ. The Geography of COPD Hospitalization in California. COPD: Journal of Chronic Obstructive Pulmonary Disease. 2009;2(4):435–444. doi: 10.1080/15412550500346543 [DOI] [PubMed] [Google Scholar]
- 67.Lipton R, Banerjee A. The Geography of Chronic Obstructive Pulmonary Disease Across Time: California in 1993 and 1999. International Journal of Medical Sciences. 2007;4(4):179–189. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1925151/pdf/ijmsv04p0179.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kong AY, Baggett CD, Gottfredson NC, Ribisl KM, Delamater PL, Golden SD. Associations of tobacco retailer availability with chronic obstructive pulmonary disease related hospital outcomes, United States, 2014. Health & Place. 2021/01/01/ 2021;67:102464. doi: 10.1016/j.healthplace.2020.102464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Galiatsatos P, Kineza C, Hwang S, et al. Neighbourhood characteristics and health outcomes: evaluating the association between socioeconomic status, tobacco store density and health outcomes in Baltimore City. Tob Control. Jul 2018;27(e1):e19–e24. doi: 10.1136/tobaccocontrol-2017-053945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Pearson AL, Cleghorn CL, van der Deen FS, et al. Tobacco retail outlet restrictions: health and cost impacts from multistate life-table modelling in a national population. Tobacco Control. 2017;26(5):579. doi: 10.1136/tobaccocontrol-2015-052846 [DOI] [PubMed] [Google Scholar]
- 71.Shareck M, Kestens Y, Vallée J, Datta G, Frohlich KL. The added value of accounting for activity space when examining the association between tobacco retailer availability and smoking among young adults. Tobacco Control. 2016;25(4):406. doi: 10.1136/tobaccocontrol-2014-052194 [DOI] [PubMed] [Google Scholar]
- 72.2018 Global Progress Report on Implementation of the WHO Framework Convention on Tobacco Control. World Health Organization; 2018. Accessed October 22, 2021. https://www.who.int/fctc/reporting/WHO-FCTC-2018_global_progress_report.pdf [Google Scholar]
- 73.Brown A, Boudreau C, Moodie C, et al. Support for removal of point-of-purchase tobacco advertising and displays: findings from the International Tobacco Control (ITC) Canada survey. Tobacco Control. 2012;21(6):555. doi: 10.1136/tobaccocontrol-2011-050153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.McNeill A, Lewis S, Quinn C, et al. Evaluation of the removal of point-of-sale tobacco displays in Ireland. Tob Control. Mar 2011;20(2):137–43. doi: 10.1136/tc.2010.038141 [DOI] [PubMed] [Google Scholar]
- 75.He Y, Shang C, Huang J, Cheng K-W, Chaloupka FJ. Global evidence on the effect of point-of-sale display bans on smoking prevalence. Tobacco Control. 2018;27(e2):e98. doi: 10.1136/tobaccocontrol-2017-053996 [DOI] [PubMed] [Google Scholar]
- 76.Quinn C, Lewis S, Edwards R, McNeill A. Economic evaluation of the removal of tobacco promotional displays in Ireland. Tobacco Control. 2011;20(2):151. doi: 10.1136/tc.2010.039602 [DOI] [PubMed] [Google Scholar]
- 77.Dunlop S, Kite J, Grunseit AC, et al. Out of Sight and Out of Mind? Evaluating the Impact of Point-of-Sale Tobacco Display Bans on Smoking-Related Beliefs and Behaviors in a Sample of Australian Adolescents and Young Adults. Nicotine Tob Res. Jul 2015;17(7):761–8. doi: 10.1093/ntr/ntu180 [DOI] [PubMed] [Google Scholar]
- 78.Carter OB, Phan T, Mills BW. Impact of a point-of-sale tobacco display ban on smokers’ spontaneous purchases: comparisons from postpurchase interviews before and after the ban in Western Australia. Tob Control. Mar 2015;24(e1):e81–6. doi: 10.1136/tobaccocontrol-2013-050991 [DOI] [PubMed] [Google Scholar]
- 79.Martino SC, Setodji CM, Dunbar MS, Shadel WG. Increased attention to the tobacco power wall predicts increased smoking risk among adolescents. Addict Behav. Jan 2019;88:1–5. doi: 10.1016/j.addbeh.2018.07.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Setodji CM, Martino SC, Gong M, et al. How do tobacco power walls influence adolescents? A study of mediating mechanisms. Health Psychol. 2018;37(2):188–193. doi: 10.1037/hea0000558 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Burton S, Spanjaard D, Hoek J. An investigation of tobacco retail outlets as a cue for smoking. Australasian Marketing Journal (AMJ). 2013;21(4):234–239. doi: 10.1016/j.ausmj.2013.08.003 [DOI] [Google Scholar]
- 82.Stead M, Eadie D, Purves RI, Moodie C, Haw S. Tobacco companies’ use of retailer incentives after a ban on point-of-sale tobacco displays in Scotland. Tobacco Control. 2018;27(4):414. doi: 10.1136/tobaccocontrol-2017-053724 [DOI] [PubMed] [Google Scholar]
- 83.Watts C, Burton S, Freeman B, et al. ‘Friends with benefits’: how tobacco companies influence sales through the provision of incentives and benefits to retailers. Tobacco Control. 2020:tobaccocontrol-2019–055383. doi: 10.1136/tobaccocontrol-2019-055383 [DOI] [PubMed] [Google Scholar]
- 84.Wakefield M, Zacher M, Scollo M, Durkin S. Brand placement on price boards after tobacco display bans: a point-of-sale audit in Melbourne, Australia. Tob Control. Nov 2012;21(6):589–92. doi: 10.1136/tobaccocontrol-2012-050616 [DOI] [PubMed] [Google Scholar]
- 85.Guindon GE, Fatima T, Abbat B, Bhons P, Garasia S. Area-level differences in the prices of tobacco and electronic nicotine delivery systems — A systematic review. Health & Place. 2020/09/01/ 2020;65:102395. doi: 10.1016/j.healthplace.2020.102395 [DOI] [PubMed] [Google Scholar]
- 86.State Tobacco Activities Tracking and Evaluation (STATE) System Licensure Fact Sheet. Centers for Disease Control and Prevention; 2021. Accessed December 30, 2021. https://www.cdc.gov/statesystem/factsheets/licensure/Licensure.html#current-licensing [Google Scholar]
- 87.Baker J, Masood M, Rahman MA, Begg S. Levels of support for the licensing of tobacco retailers in Australia: findings from the National Drug Strategy Household Survey 2004–2016. BMC Public Health. 2020/05/24 2020;20(1):773. doi: 10.1186/s12889-020-08920-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Kuipers MAG, Nuyts PAW, Willemsen MC, Kunst AE. Tobacco retail licencing systems in Europe. Tobacco Control. 2021:tobaccocontrol-2020–055910. doi: 10.1136/tobaccocontrol-2020-055910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Baker J, Masood M, Rahman MA, Thornton L, Begg S. Identifying tobacco retailers in the absence of a licensing system: lessons from Australia. Tobacco Control. 2021:tobaccocontrol-2020–055977. doi: 10.1136/tobaccocontrol-2020-055977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Kirchner TR, Cantrell J, Anesetti-Rothermel A, Ganz O, Vallone DM, Abrams DB. Geospatial exposure to point-of-sale tobacco: real-time craving and smoking-cessation outcomes. American journal of preventive medicine. 2013;45(4):379–385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Kirchner TR, Shiffman S. Spatio-temporal determinants of mental health and well-being: advances in geographically-explicit ecological momentary assessment (GEMA). Social Psychiatry and Psychiatric Epidemiology. 2016/09/01 2016;51(9):1211–1223. doi: 10.1007/s00127-016-1277-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Shiffman S, Stone AA, Hufford MR. Ecological Momentary Assessment. Annual Review of Clinical Psychology. 2008/04/01 2008;4(1):1–32. doi: 10.1146/annurev.clinpsy.3.022806.091415 [DOI] [PubMed] [Google Scholar]
- 93.Lipperman-Kreda S, Finan LJ, Kowitt SD, et al. Youth daily exposure to tobacco outlets and cigarette smoking behaviors: does exposure within activity space matter? https://doi.org/10.1111/add.15001. Addiction. 2020/09/01 2020;115(9):1728–1735. doi: 10.1111/add.15001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.McQuoid J, Thrul J, Ling P. A geographically explicit ecological momentary assessment (GEMA) mixed method for understanding substance use. Social Science & Medicine. 2018/04/01/ 2018;202:89–98. doi: 10.1016/j.socscimed.2018.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Roberts ME, Lu B, Browning CR, Ferketich AK. Tracking Young Adults’ Attitudes Toward Tobacco Marketing Using Ecological Momentary Assessment (EMA). Substance Use & Misuse. 2017/07/29 2017;52(9):1208–1213. doi: 10.1080/10826084.2017.1302958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Chen-Sankey JC, van de Venne J, Westneat S, et al. Real-Time Context of Tobacco Marketing Exposure and Community Vulnerability-An Ecological Momentary Assessment Among Young Adults. Ann Behav Med. Jul 29 2021;doi: 10.1093/abm/kaab066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Robinson JD, Drobes DJ, Brandon TH, Wetter DW, Cinciripini PM. Evaluating Point of Sale Tobacco Marketing Using Behavioral Laboratory Methods. Tob Regul Sci. 2016;2(4):414–425. doi: 10.18001/TRS.2.4.11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Oliver JA, Sweitzer MM, Engelhard MM, Hallyburton MB, Ribisl KM, McClernon FJ. Identifying neural signatures of tobacco retail outlet exposure: Preliminary validation of a “community neuroscience” paradigm. Addiction Biology. 2021/09/01 2021;26(5):e13029. doi: 10.1111/adb.13029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Smokefree Aotearoa 2025 Action Plan - Auahi Kore Aotearoa Mahere Rautaki 2025. Ministry of Health; 2021. https://www.health.govt.nz/publication/smokefree-aotearoa-2025-action-plan-auahi-kore-aotearoa-mahere-rautaki-2025 [Google Scholar]
- 100.Maani N, Collin J, Friel S, et al. Bringing the commercial determinants of health out of the shadows: a review of how the commercial determinants are represented in conceptual frameworks. European Journal of Public Health. 2020;30(4):660–664. doi: 10.1093/eurpub/ckz197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Kickbusch I, Allen L, Franz C. The commercial determinants of health. The Lancet Global Health. 2016;4(12):e895–e896. [DOI] [PubMed] [Google Scholar]
- 102.Tobacco Supply Chain. Tobacco Tactics, University of Bath; 2021. Accessed December 20, 2021. https://tobaccotactics.org/supply-chain/ [Google Scholar]
- 103.Henriksen L, Mahoney M. Tobacco industry’s T.O.T.A.L. interference. Tobacco Control. 2018;27(2):234. doi: 10.1136/tobaccocontrol-2016-053530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.McDaniel PA, Malone RE. Tobacco industry and public health responses to state and local efforts to end tobacco sales from 1969–2020. PLOS ONE. 2020;15(5):e0233417. doi: 10.1371/journal.pone.0233417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.McDaniel PA, Malone RE. “People over Profits”: Retailers Who Voluntarily Ended Tobacco Sales. PLOS ONE. 2014;9(1):e85751. doi: 10.1371/journal.pone.0085751 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Feletto E, Burton S, Williams K, et al. Who stops selling? A systematic analysis of ex-tobacco retailers. Tobacco Control. 2017;26(2):164. doi: 10.1136/tobaccocontrol-2015-052629 [DOI] [PubMed] [Google Scholar]
- 107.McDaniel PA, Malone RE. Why California retailers stop selling tobacco products, and what their customers and employees think about it when they do: case studies. BMC Public Health. 2011/11/08 2011;11(1):848. doi: 10.1186/1471-2458-11-848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Robertson L, Cameron C, Hoek JA, et al. Prevalence and characteristics of tobacco purchases in convenience stores: results of a postpurchase intercept survey in Dunedin, New Zealand. Tobacco Control. 2019;28(6):696. doi: 10.1136/tobaccocontrol-2018-054643 [DOI] [PubMed] [Google Scholar]
- 109.Marsh L, Cameron C, Quigg R, et al. Is the tobacco ‘footfall’ argument justified for tobacco purchases in New Zealand convenience stores? Tobacco Control. 2020:tobaccocontrol-2020-056032. doi: 10.1136/tobaccocontrol-2020-056032 [DOI] [PubMed] [Google Scholar]
- 110.Ackert K, Brock B, Friedrichsen SC, et al. Countering tobacco industry tactics on the economic costs of restricting menthol tobacco. Tobacco Control. 2020;29(e1):e113. doi: 10.1136/tobaccocontrol-2020-055737 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Lawman HG, Dolatshahi J, Mallya G, et al. Characteristics of tobacco purchases in urban corner stores. Tob Control. Sep 2018;27(5):592–595. doi: 10.1136/tobaccocontrol-2017-053815 [DOI] [PubMed] [Google Scholar]
- 112.Wood L, Gazey A. Tobacco mythbusting—tobacco is not a major driver of foot traffic in low socio-economic small retail stores. Tobacco Control. 2021:tobaccocontrol-2020–056310. doi: 10.1136/tobaccocontrol-2020-056310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Hitchman SC, Calder R, Rooke C, McNeill A. Small Retailers’ Tobacco Sales and Profit Margins in Two Disadvantaged Areas of England. AIMS public health. 2016;3(1):110–115. doi: 10.3934/publichealth.2016.1.110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Hall W, Morphett K, Gartner C. A critical analysis of Australia’s ban on the sale of electronic nicotine delivery systems. Neuroethics. 2021/12/01 2021;14(3):323–331. doi: 10.1007/s12152-019-09402-x [DOI] [Google Scholar]
- 115.Jordt S-E. Synthetic nicotine has arrived. Tobacco Control. 2021:tobaccocontrol-2021-056626. doi: 10.1136/tobaccocontrol-2021-056626 [DOI] [PMC free article] [PubMed] [Google Scholar]