

Abstract
Background:
Latinx elders are underrepresented in dementia research. In a previous study we assessed research attitudes in urban minority elders and found a significant minority expressed neutral to negative attitudes relating to trust, safety, and personal responsibility to help research.
Objective:
To assess the impact of a composite intervention on attitudes towards research and research participation among elderly Latinx. The intervention was a collaboratively produced research participation video shown during presentations with our elderly community advisory board (CAB) as co-presenters.
Method:
The video was created by the ADRC and CAB. All senior center attendees were eligible to participate. Afterwards, the Research Attitudes Questionnaire (RAQ) and a brief questionnaire on the impact of the video were administered. Using Wilcoxon Rank Sum Tests, Chi Square and OLS regressions, RAQ responses were compared to those from a historical cohort from similar centers.
Results:
74 in the “Historical Cohort 1” and 104 in “Intervention Cohort 2” were included. RAQ total score was higher in Cohort 2 than Cohort 1 (28.5 vs. 26.1, p<0.05) after controlling for age, education and country of origin. In response to the question “Has the video influenced your willingness and interest to participate in research”, 88.7% of the participants in Cohort 2 reported being “more” or “much more” interested in research.
Conclusion:
Tailoring community research recruitment programs to include relatable peers using novel recruitment techniques may have positive implications for improving enrollment of diverse elderly individuals in research.
Keywords: Minorities in research, elder minorities, research participation, attitudes towards research, diversity
INTRODUCTION
The community of older adults in the U.S. population is becoming increasingly ethnically and racially diverse, with those identified as Latino or of Hispanic origin (Latinxs) expected to comprise 21% of the older U.S. population by 2060 [1]. However, Latinxs are underrepresented in clinical research. For example, in the National Alzheimer’s Coordinating Center Uniform Data Set (NACC UDS), which records cumulative enrollment of NIA-funded Alzheimer’s Disease Centers (ADC’s), only 8% of all participants are identified as Latinx [2]. Similarly in the Alzheimer’s Disease Neuroimaging study, over 95% of participants were non-Latinx white[3]. Historically, there are a number of factors contributing to distrust of medical research among Latinx groups including ongoing systemic racism, social and economic disparities[4], lack of information available in Spanish, and misinformation about issues like autonomy and informed consent [5]. Other barriers to research participation include financial concerns such as missing work, lack of information about research, as well as privacy and confidentiality concerns [5–7]. One study reported that Latinxs were equally willing to participate in research as non-Latinx whites if given adequate information[8]. It is important for researchers to accept responsibility and authentically address ongoing systematic issues and power dynamics that perpetuate this mistrust.
The literature suggests that interventions aimed at involving the community (gate keepers, health care providers, community advisory boards, racially/ethnically congruent research assistants, etc.) have been helpful in recruitment of underrepresented minorities [9, 10] [7, 11],[12] [13]. Previous work from our group [14] assessed research attitudes among racially and ethnically diverse elders attending senior center talks in largely low-income communities in New York City. Data demonstrated that a substantial number (42–48%) endorsed concerns about trust and safety. These results prompted our group to explore ways to work collaboratively with the community using community based participatory research methodology to understand and address these concerns. To this end, the ADRC created a Community Advisory Board (CAB), composed primarily of Latina women over 65 from East Harlem. The Mount Sinai Alzheimer’s Disease Research Center (ADRC) is located in East Harlem in New York City, a predominantly low income, Latinx community with whom we have built strong relationships spanning over 20 years.
Our previous community focus group work demonstrated strong preferences from older Latinxs for health information presented in an informal manner through videos featuring same aged peers [15]. This is consistent with literature about engaging diverse communities to participate in health services and research using methodologies such as videos [16, 17] and engaging health promoting peers [18] and community based participatory research strategies [19]. CAB members were recruited from a larger working group of diverse community members who collaborated with the ADRC. The CAB assisted the research team in making educational videos for the community, and became ADRC participants themselves, but did not receive any formal training or payment [15]. One video addressed concerns about safety and trust in research, “Memory Research: Is it right for me?” (https://youtu.be/gg06SY-zuVg).
The aim of the present study was to assess the impact of a composite intervention on attitudes towards research and research participation in community members. This intervention was created in the framework of Entertainment Education [17, 20, 21] and with the understanding of the demonstrated benefit of medically proactive peers [18]. The intervention consisted of showing this video to Latinx seniors in local community centers along with question and answer sessions conducted by the outreach team (ADRC social workers and interns) with our CAB members as co-presenters. The development of the CAB and our collaboration with them to make educational videos that address fears, knowledge gaps and other concerns is detailed in a previous paper [15]. Data was gathered regarding the audience’s feelings about the effectiveness of the video/CAB in addressing research concerns, as well as their responses to the Research Attitudes Questionnaire (RAQ). The RAQ data was then compared to RAQ responses from a historical cohort, a similar group of senior center elders who had no exposure to the video or the presence of the CAB members [14]. The hypothesis was that this intervention would be associated with self-reported willingness to consider research participation and would serve as a non-threatening and engaging tool to open the conversation about research.
METHODS:
Study Design:
This is a case control study which combined a historical, observational cohort who were not exposed to a video/community board intervention with a similar cohort of participants who were exposed to the intervention.
Description of Procedures and Sample Construction
Cohort 1 (“historical cohort”): In 2014–15, 123 under-represented (i.e., Hispanic, Non-Hispanic Black, Asian) older adults (mean age 72.6) across 8 low-income community senior centers in the East Harlem neighborhood of New York City attended 45-minute bilingual informational (non-research) community talks on aging, dementia and caregiver stress. Sessions were conducted by young to middle-aged Latina Mount Sinai staff who were associated with a NY State service grant to increase information and encourage care for AD in the community, with time for questions at the end. All individuals at the center on the day of the talk were invited to attend and complete the RAQ anonymously, afterwards. Demographic variables collected included age, education, country of origin, and whether the RAQ was completed in Spanish or English[14]. While information regarding race/ethnicity was not specifically asked, individuals reported language spoken at home and country of origin. Attendees were characterized as Latinx and included in this cohort (N=74) if they reported speaking Spanish at home or if they were born in a Spanish speaking country (e.g., Puerto Rico, Dominican Republic). Because Latinx groups are heterogeneous, country of origin was used as a proxy to measure possible cultural differences/acculturation issues. More information on this cohort is available in our prior publication[14].
The remainder of the attendees, excluded from the current analysis, included 49 English-speaking respondents born in the US or English-speaking Caribbean countries. This does not preclude the possibility that some Latinx individuals (e.g. U.S. born English speakers) could be in this excluded group.
Cohort 2 (“intervention cohort”): Between July 2018 and February 2019, the 3-minute video “Memory Research: Is it right for me?” was screened at 19 senior centers similar to those from the historical cohort and was followed by question and answer sessions co-led by CAB members and bilingual ADRC faculty. No formal didactic or informational content was presented. CAB members were also ADRC participants and acted in the video. All individuals at the senior center were invited to attend the presentation and Q & A, and complete the video questionnaire and RAQ afterwards. There were 6–20 participants per session, the vast majority of whom filled in the questionnaires at the end. Like methods used in Cohort 1, 104 attendees who reported speaking Spanish at home, were born in Spanish speaking countries and/or self-described as Latinx were characterized as “Latinx”. The remainder of the attendees who were not included in the current analysis (n=129) included 79 African Americans, 29 non-Latinx whites, and 21 who reported other race/ethnic background. Other demographic variables collected included age, gender, years of education, and country of origin.
Assessments and Intervention
Research Attitudes Questionnaire (RAQ)
The Research Attitudes Questionnaire (RAQ) is a 7-item questionnaire used to assess how favorable or unfavorable views are regarding biomedical research (Table 1). The measure was translated and back-translated by native Spanish-speaking ADRC faculty. [22]. Each item is rated on a scale from 1 (strongly disagree) to 5 (strongly agree). A total score was constructed by adding individual item scores, ranging from 7 (most unfavorable) to 35 (most favorable) (Table 3). We also examined differences in responses to each RAQ question individually (Table 3). For other analyses (Figure 1), because so few responses were negative, categories were collapsed into negative (1–2), neutral (3), and positive (4–5).
Table 1:
RAQ Questions
| 1 | I have a positive view about medical research in general. |
| 2 | Medical researchers can be trusted to protect the interest of people who take part in their research studies. |
| 3 | We all have some responsibility to help others by volunteering in research. |
| 4 | Society needs to devote more resources to medical research. |
| 5 | Participating in medical research is generally safe. |
| 6 | If I volunteer for medical research, I know my personal information will be kept private and confidential. |
| 7 | Medical research will find cures for many major diseases during my lifetime. |
Table 3:
RAQ scores by Cohort
| Variables | Cohort 1 | Cohort 2 | |||
|---|---|---|---|---|---|
| N=74 | N=104 | ||||
| RAQ, mean | (SD) | RAQ, mean | (SD) | ||
| RAQ Sum Total | 26.1 | 6.7 | 28.5 | 5.2 | *** |
| q1 | 3.9 | 1.0 | 4.2 | 0.9 | ** |
| q2 | 3.4 | 1.1 | 3.9 | 1.0 | *** |
| q3 | 3.5 | 1.2 | 4.0 | 1.0 | *** |
| q4 | 4.1 | 1.2 | 4.3 | 1.0 | |
| q5 | 3.5 | 1.2 | 3.9 | 1.0 | *** |
| q6 | 3.9 | 1.1 | 4.2 | 0.9 | |
| q7 | 3.9 | 1.3 | 4.0 | 0.9 |
p<0.01,
p<0.001
Figure 1.
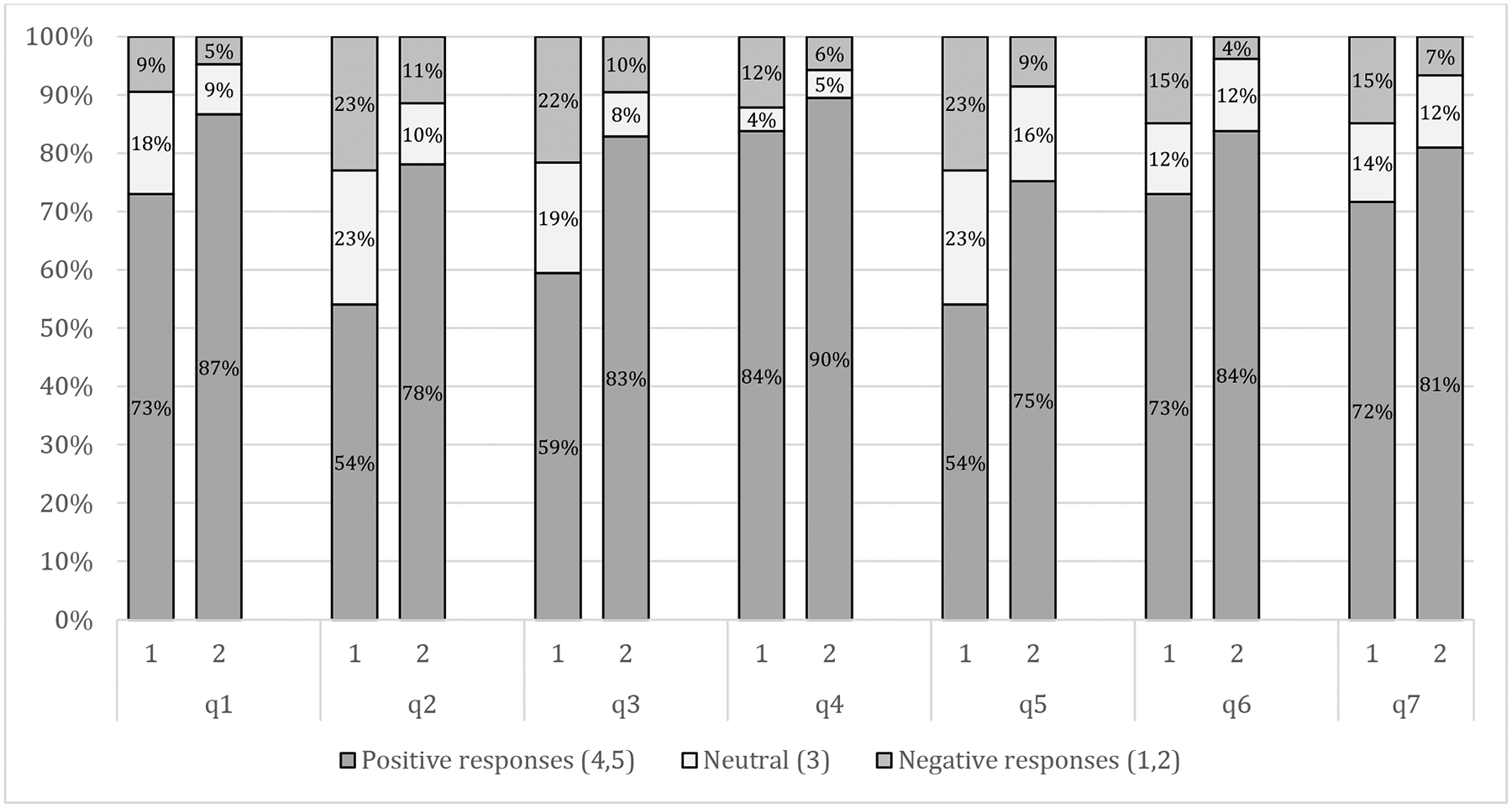
RAQ Responses by Cohort (1, 2)
Video Presentation and Q&A
Three CAB members co-wrote and acted in the 3.17 minute video “Memory research: Is it right for me?” The script was based on ideas from the CAB, depicting several older women at a senior center, discussing the memory research lecture they had just attended. The video showed the women conversing about memory research participation and sharing their concerns. It ended with one woman consulting her college-aged granddaughter who underscored the value of research, encouraged her grandmother to participate and offered to accompany her as a study partner. Because of the growing cultural diversity in the East Harlem community, CAB member actors included two Latina women and one Chinese woman. The video was primarily in English; however, to reflect the common experiences of those in this multicultural community, the video opens with a brief Spanish language section. As part of the dialogue, this is translated by the Spanish speakers to the third character who only spoke English. Video presentations and Q&A sessions were co-led by the CAB members and the outreach team to highlight the cultural congruence of the CAB and audience members. The Q & A was bilingual (English and Spanish) and lasted for about 30 minutes. The preponderance of one or the other language depended on the specific center and the questions and responses were translated immediately after into the other language to make sure all listeners understood. The most common questions related to dementia prevention.
Questions Concerning the Impact of the Video
To assess whether the video and the presentation were associated with respondents’ attitudes toward research, two Likert type scale questions were asked on a scale of 1 to 5: “Has the video influenced your willingness and interest to participate in research?” (ranging from significantly negative to significantly positive influence), and “Do you think you may want to participate in research?” (ranging from no interest to definite interest in participation). The research described in the sessions by the CAB was participation in a longitudinal study involving yearly cognitive testing through our ADRC[2, 23].
Statistical Analysis
We compared participant characteristics and RAQ responses for Cohort 1 and 2 using Wilcoxon rank sum tests for continuous variables and Chi-square tests for categorical variables as appropriate. An Ordinary Least Squares (OLS) regression model was used to examine cohort differences in the RAQ total score after controlling for participant age, education, and country of origin. Statistical significance was set a priori at p=0.05.
RESULTS
Sample Characteristics (Table 2)
Table 2.
Sample Characteristics by Cohort
| Variables | Cohort 1 | Cohort 2 | |||
|---|---|---|---|---|---|
| N=74 | N=104 | ||||
| Age, mean (SD) | 72.2 | (9.1) | 75.2 | (8.5) | * |
| Female % | - | 81.4% | - | ||
| Education, mean (SD) | 9.4 | (4.4) | 10.7 | (3.9) | * |
| Language, n (%) | |||||
| English/bilingual | 23 | 31.1% | 27 | 25.7% | - |
| Spanish | 51 | 68.9% | 77 | 74.3% | |
| Country of Origin, n (%) | |||||
| Puerto Rico | 53 | 71.6% | 53 | 50.5% | * |
| Dominican Republic | 10 | 13.5% | 17 | 16.2% | |
| USA | 2 | 2.7% | 13 | 12.3% | |
| Other | 9 | 12.2% | 22 | 20.8% |
p<0.05
Other countries of Origin in Cohort 1 included: Ecuador(4), Bolivia(1), El Salvador(1), Honduras(1), Mexico (1), Nicaragua (1)
Other countries of Origin in Cohort 2 included: Ecuador(8), Honduras(3), Cuba (2), Colombia (2), El Salvador(1), Peru(1), Nicaragua (1)
Cohort 1 included 74 participants, with mean ± SD age 72.2±9.1 and 9.35±4.4 years of education. Seventy-two percent of the respondents were born in Puerto Rico. Cohort 2 included 104 participants with mean age 75.2±8.5, 81.4% female, and 10.7±3.9 years of education. Fifty-one percent of the respondents were born in Puerto Rico. Cohort 2 included 10 US-born Latinx participants whose primary language was English. The two cohorts differed in age (p=0.046), education (p=0.045), and country of origin (p=0.019), with Cohort 2 being older, more highly educated, and more likely to be from a diverse group of Spanish-speaking countries, as opposed to being primarily from Puerto Rico.
RAQ Responses in Cohort 1 and 2
The RAQ total score was 2.4 points higher in Cohort 2 than Cohort 1 (28.5(+/−5.2) vs. 26.1(+/−6.7), p<0.001) (Table 3). Figure 1 shows the percentage of positive/neutral/negative responses to each item in the RAQ by cohort. When individual RAQ item responses were compared, the distribution of responses (positive, neutral, negative) by cohort was statistically significant for Question 2 (“Medical researchers can be trusted to protect the interest of people who take part in their research studies”, p=0.003), Question 3 (“We all have some responsibility to help others by volunteering in research”, p=0.002), Question 5 (“Participating in medical research is generally safe” p= 0.006), and Question 6 (“If I volunteer for medical research, I know my personal information will be kept private and confidential”, p=0.031). For each of these four RAQ items, the responses were significantly more favorable in Cohort 2 (who saw the video/intervention) than Cohort 1, with 11–23% more people in Cohort 2 rating these four RAQ items more favorably (4 or 5 on Likert type scale). This was particularly notable for the items concerning volunteerism (23%), trust (23%) and safety (20%). The difference in RAQ total score between Cohorts 1 and 2 are largely driven by these 4 questions. The 3 questions for which differences between Cohort 1 and 2 were statistically insignificant were already rated highly in Cohort 1, suggesting a possible ceiling effect.
An OLS regression model estimating the independent cohort differences in the RAQ total score showed that after controlling for participant age, education, and country of origin, the RAQ total score remained significantly higher (almost 2 points on average) in Cohort 2 (coef ± SE)= 1.978±0.958, p<0.05) (Table 4).
Table 4.
OLS regression estimates of participants’ characteristics associated with RAQ
| Coef. | Std. Err. | [95% Conf. Interval] | |||
|---|---|---|---|---|---|
| Cohort 2 (reference=Cohort 1) | 1.978 | (0.958) | * | 0.087 | 3.870 |
| Age | 0.050 | (0.958) | −0.062 | 0.161 | |
| Education | 0.082 | (0.958) | −0.149 | 0.314 | |
| Country of Origin (reference=US) | |||||
| Puerto Rico | 0.889 | (0.958) | −2.428 | 4.206 | |
| Dominican Republic | 2.833 | (0.958) | −0.994 | 6.660 | |
| Other | 2.209 | (0.958) | −1.510 | 5.928 | |
p<0.05
Responses to research video questions in Cohort 2
We examined responses from Cohort 2 concerning interest in research participation and desire to participate in research after viewing the video/CAB presentation. In response to the question “Has the video influenced your willingness and interest to participate in research”, 52.6% of the participants reported being “more”, 36.1% reported “much more” interested in research, 7.2% said the video had “no effect”, and 4.1% reported being “less” or “much less” interested in research.
In response to the question “Do you think you may want to participate in research?”, 40.2% reported that they “might” and 34.0% reported they “definitely” want to participate, 5.2% were “indifferent”, and 20.6% reported either “I don’t think I want to” or “I definitely do not want to” participate in research.
In a post hoc analysis, we examined the RAQ scores in the 25.8% of the participants who stated that they were indifferent/negative regarding interest in research participation. Their RAQ scores were significantly lower on 5 of the 7 RAQ items, with the lowest score on the item regarding trust. There were no demographic differences between those who responded more or less favorably, regarding interest in research participation (Results in Supplementary Table 1).
DISCUSSION
In this report we demonstrate that a video/CAB intervention presented to Latinx senior center attendees was associated with increased interest in the possibility of research participation. Moreover, the intervention cohort reported more positive attitudes about clinical research than a historical cohort of individuals from the same community. Studies suggest that positive research attitudes may be important in research success because higher clinical trial dropout rates are associated with lower RAQ scores[24].
Several studies suggest that underserved minorities have a negative view of research [5, 25], though our findings do not support this. In fact, basic attitudes toward research (“I have a positive view about medical research in general”) were positive in both the intervention (86.7%) and historical cohort (73%). The intervention cohort did endorse stronger positive views on RAQ items regarding trust in researchers, personal safety, and volunteerism. The item concerning volunteerism, “We all have some responsibility to help others by volunteering in research” revealed a particularly robust 83% positive rating compared to only 60% positive in the historical cohort.
The goal of the video/CAB intervention was to foster identification and spur conversations through engagement with positive and relatable role models. This was accomplished by involving the CAB in every aspect of this project: identifying a scenario, writing the script, acting, and attending screenings/Q&A’s. They modeled the idea that research is a collaborative venture between scientists and volunteers. Drawing on their own experiences, the CAB members suggested the scenario of friends talking about dementia research, with one taking the role of the skeptic with a college-aged granddaughter serving as trusted family advisor. CAB members felt that this narrative was relatable and addressed misinformation and fears about research. The basis for the identification with the CAB/characters in the video may be multiply determined: race/ethnicity, socioeconomic status, language, familiarity of surroundings (i.e. urban senior center), and/or reliance on friends and family as trusted advisors.
We posit that this identification led to increased openness to research participation and is consistent with the importance of medically proactive peers [18] and the success of lay health educators in improving research recruitment in diverse populations. Lay health educators may serve a similar function to our CAB. For example, in one study, an Alzheimer’s research center increased research participation among African Americans by training highly committed and engaged African American community members to provide presentations [26]. Although our CAB members were not formally trained as lay health educators, they served as a knowledgeable and enthusiastic peer resource because they were all ADRC participants who were passionate about increasing research participation in their community. This approach resonates with the Latino cultural values of personalismo (preferring interactions on a personal basis) and confianza (a careful and significant placement of trust), crucial elements in engaging Latinxs [27].
Audiences responded overwhelmingly positively to the CAB/video intervention. In response to the question “Has the video influenced your willingness and interest to participate in research,” almost 90% reported that the intervention increased their interest. This is consistent with entertainment education literature about impacting health behaviors among Latinxs using videos, foto-novelas and soap operas (“telenovelas”). For example, in Mexico educational health messages were introduced into a publicly aired telenovela, and researchers documented changes in behavior and health practices[28]. In Latinx populations with low literacy in the U.S., videos and foto-novelas have been utilized to promote participation in health services such as screenings for depression and breast cancer, depression treatment, and dementia evaluations [29–32]. Entertainment education strategies may help promote change through affective identification with the characters, their situations and health promoting behaviors [17, 20, 21].
There are limitations to this study, several of which relate to sampling issues. We used a historical comparison cohort rather than a within subjects design and, in both cohorts, we relied on a convenience sample of individuals who responded anonymously to the RAQ. Because data was collected anonymously, it is unknown whether some participants might have attended previous talks by our group, with possible positive carryover effect. However, the ADRC has provided community outreach for 20 years (long before the first intervention) and that exposure effect could have been present in the first cohort. There are over 14,000 East Harlem community members over age 65, and the turnover of attendees at any single senior center is unknown. Additional factors that may have changed in the years between the two cohorts include exposure to dementia through movies or media, other education about Alzheimer’s, or exposure to research concepts more broadly. Because we collected data anonymously, it was not possible to track actual recruitment into ADRC studies; this could be a focus of future efforts using non-anonymized data collection.
We decided to include 10 US born, English-speaking Latinxs in Cohort 2 although their counterparts were not included in Cohort 1. Although there may be unknown cultural factors that affect research attitudes in this group of English-speaking Latinxs in Spanish Harlem, it has been our experience over two decades of working in this community that these individuals are more alike than different. The intervention was aimed at low income, urban Latinxs and these results may not be generalizable to other Latinx groups in the US. RAQ scores were lower among those who were not interested in possibly signing up for research; however other factors (e.g., needing more information, previous negative experiences, family or financial stressors or health concerns) that might have affected their interest in research participation, were not explored. Finally, although the RAQ was translated and back-translated by native Spanish speakers in the ADRC, to our knowledge, the RAQ has not been validated in a Spanish-speaking US sample.
While it is likely that the video and CAB members’ presence at the presentations had a synergistic relationship in promoting research participation, other studies could investigate these components separately to gauge the relative contribution of each. Though video production is costly, it represents a one-time investment. In contrast, recruiting and maintaining an active and diverse CAB with members who have ample time to participate in outreach, requires ongoing investment of time and money. Understanding the relative contribution of each component of the intervention could help identify the most cost-effective ways to maximize recruitment outreach efforts.
In conclusion, the potential value of the video and the CAB is to initiate a process of trust building and conversation about what research is and its core collaborative nature. This intervention may represent just a first step among many. Like Prochaska’s model[33] that proposes multiple steps of contemplation along the way to making changes, individuals who are understandably reluctant to participate in research may benefit from a recruitment process that supports travel along the path from “precontemplation” to consideration of a specific research protocol. In this context, an intervention that increases willingness to consider research participation represents one valuable step along that path.
Supplementary Material
ACKNOWLEDGMENTS AND FUNDING
Funding for this initiative was provided by the Alzheimer’s Disease Research Center (ADRC) at the Icahn School of Medicine at Mount Sinai (P50AG005138). Drs. Sano, Zhu also are supported by the Department of Veterans Affairs, Veterans Health Administration. Work was done while Sabrina Gonzalez, Alexandra Acabá-Berrocal, Luca Bianchetti, Gabriela Silva, were working with the ADRC at Mount Sinai.
CITATIONS
- [1].Administration for Community Living, Profile of Hispanic Americans Age 65 and Over. 2017, https://acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/2017OAProfileHA508.pdf, Accessed 9/23/20.
- [2].Besser L, Kukull W, Knopman DS, Chui H, Galasko D, Weintraub S, Jicha G, Carlsson C, Burns J, Quinn J, Sweet RA, Rascovsky K, Teylan M, Beekly D, Thomas G, Bollenbeck M, Monsell S, Mock C, Zhou XH, Thomas N, Robichaud E, Dean M, Hubbard J, Jacka M, Schwabe-Fry K, Wu J, Phelps C, Morris JC, Neuropsychology Work Group D, Clinical Core leaders of the National Institute on Aging-funded USAsDC (2018) Version 3 of the National Alzheimer’s Coordinating Center’s Uniform Data Set. Alzheimer Dis Assoc Disord 32, 351–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Alzheimer’s Disease Neuroimaging Initiative, ADNI report, Demographics, http://adni.loni.usc.edu/wp-content/uploads/2012/08/ADNI_Enroll_Demographics.pdf, Accessed 11/12/20.
- [4].Jaiswal J (2019) Whose Responsibility Is It to Dismantle Medical Mistrust? Future Directions for Researchers and Health Care Providers. Behav Med 45, 188–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].George S, Duran N, Norris K (2014) A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am J Public Health 104, e16–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Shavers VL, Lynch CF, Burmeister LF (2002) Racial differences in factors that influence the willingness to participate in medical research studies. Annals of epidemiology 12, 248–256. [DOI] [PubMed] [Google Scholar]
- [7].Gelman CR (2010) Learning from recruitment challenges: barriers to diagnosis, treatment, and research participation for Latinos with symptoms of Alzheimer’s disease. J Gerontol Soc Work 53, 94–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Katz RV, Kegeles SS, Kressin NR, Green BL, Wang MQ, James SA, Russell SL, Claudio C (2006) The Tuskegee Legacy Project: willingness of minorities to participate in biomedical research. Journal of health care for the poor and underserved 17, 698–715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Gilmore-Bykovskyi AL, Jin Y, Gleason C, Flowers-Benton S, Block LM, Dilworth-Anderson P, Barnes LL, Shah MN, Zuelsdorff M (2019) Recruitment and retention of underrepresented populations in Alzheimer’s disease research: A systematic review. Alzheimers Dement (N Y) 5, 751–770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Williams MM, Meisel MM, Williams J, Morris JC (2011) An interdisciplinary outreach model of African American recruitment for Alzheimer’s disease research. Gerontologist 51 Suppl 1, S134–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Samus QM, Amjad H, Johnston D, Black BS, Bartels SJ, Lyketsos CG (2015) A Multipronged, Adaptive Approach for the Recruitment of Diverse Community-Residing Elders with Memory Impairment: The MIND at Home Experience. Am J Geriatr Psychiatry 23, 698–708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].McDougall GJ Jr., Simpson G, Friend ML (2015) Strategies for research recruitment and retention of older adults of racial and ethnic minorities. J Gerontol Nurs 41, 14–23; quiz 24–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Rabinowitz YG, Gallagher-Thompson D (2010) Recruitment and retention of ethnic minority elders into clinical research. Alzheimer Dis Assoc Disord 24 Suppl, S35–41. [PubMed] [Google Scholar]
- [14].Neugroschl J, Sewell M, De La Fuente A, Umpierre M, Luo X, Sano M (2016) Attitudes and Perceptions of Research in Aging and Dementia in an Urban Minority Population. Journal of Alzheimer’s disease : JAD 53, 69–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Neugroschl J, Sewell MC, Umpierre M, Rodriguez R, Meyers L, Kranes S, Aldrete C, Collazo A, Valois L, Sano M (2018) Elderly Latino community members make an educational video: an academic-community collaboration to promote memory evaluations. International psychogeriatrics, 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Baruch N, Allan CL, Cundell M, Clark S, Murray B (2017) Promoting early dementia diagnosis: a video designed by patients, for patients. International psychogeriatrics 29, 863–867. [DOI] [PubMed] [Google Scholar]
- [17].Sood S (2002) Audience involvement and entertainment-education. Communication Theory 12, 153–172. [Google Scholar]
- [18].Pescosolido B (1992) Beyond Rational Choice - the Social Dynamics of How People Seek Help. American Journal of Sociology 97, 1096–1138. [Google Scholar]
- [19].De las Nueces D, Hacker K, DiGirolamo A, Hicks LS (2012) A systematic review of community-based participatory research to enhance clinical trials in racial and ethnic minority groups. Health Serv Res 47, 1363–1386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Bhana A, Mellins CA, Petersen I, Alicea S, Myeza N, Holst H, Abrams E, John S, Chhagan M, Nestadt DF, Leu CS, McKay M (2014) The VUKA family program: piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care 26, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Storey D, Sood S (2013) Increasing equity, affirming the power of narrative and expanding dialogue: the evolution of entertainment education over two decades. Critical Arts-South-North Cultural and Media Studies 27, 9–35. [Google Scholar]
- [22].Rubright JD, Cary MS, Karlawish JH, Kim SY (2011) Measuring how people view biomedical research: Reliability and validity analysis of the Research Attitudes Questionnaire. Journal of empirical research on human research ethics : JERHRE 6, 63–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Beekly DL, Ramos EM, Lee WW, Deitrich WD, Jacka ME, Wu J, Hubbard JL, Koepsell TD, Morris JC, Kukull WA, Centers NIAAsD (2007) The National Alzheimer’s Coordinating Center (NACC) database: the Uniform Data Set. Alzheimer Dis Assoc Disord 21, 249–258. [DOI] [PubMed] [Google Scholar]
- [24].Stites SD, Turner RS, Gill J, Gurian A, Karlawish J, Grill JD, Alzheimer’s Disease Cooperative S (2021) Research Attitudes Questionnaire scores predict Alzheimer’s disease clinical trial dropout. Clin Trials 18, 237–244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Corbie-Smith G, Thomas SB, St George DM (2002) Distrust, race, and research. Arch Intern Med 162, 2458–2463. [DOI] [PubMed] [Google Scholar]
- [26].Souder E, Terry TL (2009) Use of lay educators to overcome barriers to research with Black older adults: a case study using Alzheimer’s Disease Center. Research in gerontological nursing 2, 235–242. [DOI] [PubMed] [Google Scholar]
- [27].Gallagher-Thompson D, Singer LS, Depp C, Mausbach BT, Cardenas V, Coon DW (2004) Effective recruitment strategies for Latino and Caucasian dementia family caregivers in intervention research. The American journal of geriatric psychiatry : official journal of the American Association for Geriatric Psychiatry 12, 484–490. [DOI] [PubMed] [Google Scholar]
- [28].Sabido M (2002) El tono: Andanzas teóricas, aventuras practicas, el entretenimiento con beneficio social. The tone: Theoretical vicissitudes, practice adventures, and entertainment with social benefit. National Autonomous University., National Autonomous University., Mexico City, Mexico:. [Google Scholar]
- [29].Valle R, Yamada A-M, Matiella AC (2006) Fotonovelas: A Health Literacy Tool for Educating Latino Older Adults About Dementia. Clinical Gerontologist 30, 71–88. [Google Scholar]
- [30].Gallagher-Thompson D, Tzuang M, Hinton L, Alvarez P, Rengifo J, Valverde I, Chen N, Emrani T, Thompson LW (2015) Effectiveness of a fotonovela for reducing depression and stress in Latino dementia family caregivers. Alzheimer disease and associated disorders 29, 146–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Borrayo EA, Thomas JJ, Lawsin C (2004) Cervical cancer screening among Latinas: the importance of referral and participation in parallel cancer screening behaviors. Women & health 39, 13–29. [DOI] [PubMed] [Google Scholar]
- [32].Cabassa LJ, Molina GB, Baron M (2012) Depression fotonovela: development of a depression literacy tool for Latinos with limited English proficiency. Health promotion practice 13, 747–754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Prochaska JO, Velicer WF (1997) The transtheoretical model of health behavior change. Am J Health Promot 12, 38–48. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.