

Abstract
Objective:
To evaluate the pain during the use of intermaxillary elastics and to compare it with that of initial archwire placement.
Materials and Methods:
Sixteen orthodontic patients who underwent initial bonding (7 girls, 13 boys; mean age 16.75 ± 2.61 years) and 19 patients who would be using intermaxillary elastics for the first time (13 girls, 7 boys; mean age 16.21 ± 3.01 years) were enrolled in this prospective study. A visual analog scale form was given to each patient to measure the pain levels, and these were measured by the same investigator using a digital caliper. Data were evaluated using Mann Whitney U-test.
Results:
The pain started to increase 2 hours after the application of elastics. The highest levels were achieved at the sixth hour and the same night. The pain levels started to decrease at day 2. Although the pain levels of the elastic group started to decrease after the second day, the pain levels of the initial bonding group were still significantly high.
Conclusions:
Intermaxillary elastics cause similar amounts of pain compared with initial archwire placement, but the pain of the elastics did not last as long as the pain felt after initial bonding.
Keywords: Pain, Intermaxillary elastics, Visual analog scale
INTRODUCTION
Orthodontic treatment is not pain-free. Between 90%–95% of the orthodontic patients reported pain during their treatment.1,2 Patients have described pressure, tension, tooth sensitivity, and pain complaints after the application of orthodontic forces.3 Many studies in the literature have implied that the pain affects patients' cooperation and even daily life activities negatively.4,5
The pain levels during orthodontic treatment differ with the use of different types of appliances. A study suggested that fixed or functional appliances cause significantly more pressure, tension, tooth sensitivity, and pain than removable appliances.4 The pain levels at band placement were found to be comparable to band separation and full arch bonding.5 In a study that aimed to compare the differences of 0.014-inch and 0.016-inch nickel-titanium archwires during initial leveling, the pain levels were found to be similar.6
Many studies evaluated the course of pain at the beginning of fixed orthodontic treatment. The results of these were similar, and all found that the highest pain levels were achieved after 24 hours and decreased the following week.2,7–10 However, Scheurer et al.1 pointed out that 25% of 170 patients still had some degree of pain 7 days after bonding.1 Generally, the pain started on the day the appliances were placed, reached the highest level the following morning, and then tended to decrease.1,2,11,12
The cause of the pain during fixed orthodontic treatment is the alterations in the periodontal ligament which occur with the forces delivered to teeth via archwires. Periodontal pain occurs with the effect of pressure, ischemia, inflammation, and edema.13 At the initial stages of the orthodontic treatment, an acute inflammatory reaction is seen with periodontal vasodilation, and hypersensitivity occurs because of this inflammatory response.14 When the orthodontic forces are applied to the teeth, the acute inflammatory response begins with the alterations in the blood flow, and this response causes release of inflammatory mediators such as substance P, histamine, enkephalin, dopamine, serotonin, prostaglandins, and leukotrienes.15,16 Substance P, released by the peripheral sensory nerve endings, modulates the release of interleukin-1β (IL-1β), IL-6, and tumor necrosis factor-α (TNF-α) by the monocytes which are proinflammatory cytokines.17 These cytokines appear in acute or chronic inflammation and stimulate the resorption of bone.
During the use of intermaxillary elastics, which are frequently used in fixed orthodontic treatment, there is a need for patient cooperation. The compliance of the patient is one of the most important factors required to achieve perfect treatment results. There are many factors affecting patient compliance,18 including the personality of the patient, need and request for the treatment, socioeconomic and cultural situation, former dental experiences, and the pain that occurs during and after the treatment.1,15,19
The presence of pain is an important factor in patient motivation. In a study that investigated the relationship between the complaints of orthodontic patients and compliance, a significant negative correlation was shown between the pain level and compliance during 3 months of follow up.6 Another study suggested that 1 of 10 patients terminated the treatment due to pain.13 In the literature, many studies investigated the amount of pain during the placement of bands, braces, and archwires, and the ways to reduce this pain. However, the pain associated with the use of intermaxillary elastics has not been investigated. The aim of this prospective study is to evaluate the initial pain levels of patients who will be using intermaxillary elastics for the first time and to compare these with the pain levels of the patients receiving full arch braces.
MATERIALS AND METHODS
Before the study was initiated, an approval from the Baskent University Institutional Review Board and Ethics Committee and the Baskent University Research Fund (Research: D-KA10/14) was obtained. Patients selected for this study included those who met the following inclusion criteria were selected to enroll in this study:
Lack of any systemic disorder or allergy;
Lack of any regular medication use;
For the elastic group, ordered for intermaxillary elastic use for the first time.
For the bonding group, bonding of both upper and lower arches should be performed at the same session.
A sample size of 16 per group was required to detect differences of at least three units in pain scores (ie, chewing, biting, and biting front and back teeth) at any measurement time with a power of 85% at the 5% significance level. The difference of three units was taken from both pilot study and clinical experience. Sample size estimation was performed by using NCSS and PASS 2000 software.20
Twenty patients who agreed to participate in the study were selected for each group according to these criteria. In the bonding group (7 girls, 13 boys), the mean age of the patients was 16.75 ± 2.61 years (girls: 17.09 ± 2.93 years; boys: 15.50 ± 2.26 years). After the placement of the braces to both maxillary and mandibular arches, 0.014-inch or 0.016-inch Nitinol archwires (Glendora, CA) were inserted for leveling.
In the elastic group (13 girls, 7 boys) the mean age of the patients was 16.21 ± 3.01 years (girls: 16.67 ± 3.48 years; boys: 15.62 ± 2.25 years). All patients had 0.016 × 0.022-inch diameter stainless steel or nickel-titanium archwires or a combination of both. Class II or Class III elastics, which delivered approximately 150 g of force to the teeth, were given to the patients (Figure 1). The patients and the parents in the elastic group were highly motivated to use elastics and were asked to report cases of noncompliance.
Figure 1.
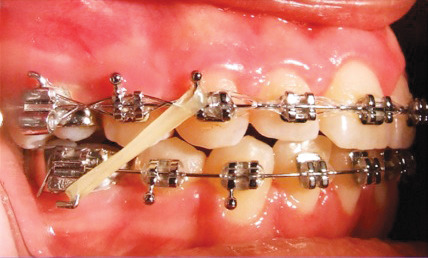
The use of intermaxillary elastics.
The pain assessments were made using a seven-page booklet that contains a 100-mm visual analog scale (VAS) form. The patients were requested to fill it in during the first week after the first archwire placement or intermaxillary elastic application and to mark their pain level on the scale line with one tick. The patients filled in the form during chewing, biting, biting on the front teeth, and biting on the back teeth at six different time intervals: at the second hour, sixth hour, bedtime of the same day, next morning, second morning, third morning, and seventh morning after elastic application. Blinding of the patients was not possible due to the nature of treatments. However, there was no information on the VAS forms about which group the patients belonged to, and therefore blinding of the investigator who measured the VAS forms could be achieved. At the next visit, the pain levels on the returned forms were measured with a digital caliper by the same investigator. Data analysis was performed by using SPSS for Windows, version 11.5 (SPSS Inc, Chicago, Ill). For each different function, mean, standard deviation, median, and interquartile range were calculated as the descriptive statistics for VAS scores. Whether the differences between groups with regard to the VAS scores were statistically significant or not was evaluated by the Mann Whitney U-test. A Bonferroni correction was applied for all possible multiple comparisons. The level of significance was set at .0071 because of the number of tests undertaken.
RESULTS
Sixteen patients in the bonding group and 19 patients in the elastic group returned their booklets. Some of the patients in the bonding group implied that they needed to take analgesics; three patients had one dose, three patients had two doses, one patient had three doses, and another patient had taken seven doses of analgesics. The mean pain values with standard deviations and interquartile ranges are given in Table 1 for chewing, biting, biting front teeth, and biting back teeth.
Table 1.
The Mean Pain Values for Both Bonding Group and Elastic Group for Chewing, Biting, Biting Front Teeth, and Biting Back Teeth

In the bonding group, the pain levels during chewing appeared after the second hour and increased gradually and significantly (P < .0012) until the next morning. While the pain levels decreased on days 2 and 3, they did not show significant differences from the morning values. On day 7 the pain levels were significantly lower than at other time intervals. During biting and biting on the back teeth, the pain levels were typically high at the beginning, and compared with the other time intervals, showed a significant decrease only at day 7. The pain levels during biting on the front teeth were similar to biting, but the pain level on day 7 was significantly lower than the levels on day 2 and 3.
In the elastic group during chewing, the amount of pain started to increase significantly from the second hour and then showed significant decreases on day 7 compared with other time intervals (P < .0012). Pain levels during biting, increased significantly at the sixth hour and began to decrease after the second day. The pain levels during biting on the front and back teeth showed similarities and significantly decreased only on day 7.
When the bonding and elastic groups were compared, the pain levels in the bonding group during chewing on the next morning and the pain levels in the elastic group during biting on the second day were significantly higher than the others (P < .0071). The pain levels in the elastic group during biting on the front teeth decreased significantly from the second day. The patients in the elastic group felt significantly more pain during biting on the back teeth on the second day, but this pain decreased faster than the other group. Overall pain lasted longer after bracket placement than application of intermaxillary elastics.
DISCUSSION
Intermaxillary elastics are an essential part of orthodontic mechanics. At this stage many of the patients show poor cooperation due to the pain and discomfort, and this causes an increase in treatment duration. The patients who showed poor elastic cooperation claimed that they had severe pain. Although elastic cooperation is a very common problem, clinicians typically ignore a patient's discomfort and blame the patient for increased treatment duration. In a recent study, the relationship between what patients felt and how the clinicians evaluated these pain experiences was investigated, and it was reported that the clinicians frequently tend to underestimate the patient's suffering.21 The aim of this study was to determine the pain levels of the patients during the use of intermaxillary elastics.
The study group consisted of adolescents because they comprise the majority of our patients. A previous study that investigated the relationship between age and discontinuation of treatment found that adolescents reported more disturbance than younger or older patients, and they quit treatment more frequently.5 These findings support the fact that physiologic and emotional factors play an important role in treatment compliance. In another study that investigated the pain levels at different treatment stages in different age groups, it was reported that adolescents were more prone to pain than others at every stage of the treatment.3,5 There are conflicting results in the literature for the gender-pain relationship. Whereas some studies suggested that there is no correlation between gender and pain, some claimed there is a connection between them.4,11,21,22 Therefore, though the numbers of boys and girls were close, we did not discriminate the gender of the patients. All of our patients had heavy archwires. While most of the patients had 0.016 × 0.022-inch stainless steel archwires, a small number of patients had flexible rectangular nickel-titanium archwires. In the literature, it has not been investigated how the thick archwires affect the pain yet, but only one study reported that 0.014-inch and 0.016-inch nickel-titanium archwires produced similar pain levels.6 No study has been reported investigating the effect of a variety of heavy archwires on the level of pain, and only one study by Erdinç and Dinçer6 reported that 0.014-inch and 0.016-inch nickel-titanium alignment archwires produced similar pain levels. Since there is no evidence of perception of different pain levels by different archwire materials of the same dimension, we included patients carrying both 0.016 × 0.022-inch nickel titanium and stainless steel archwires in the study groups.
The patients in this study reported that their pain began 2 hours after the placement of the archwires. The pain increased rapidly after bonding on the same night and reached the highest levels on the next day. From the second day after bonding, the pain started to decrease, and on day 7 it almost disappeared. The pain levels in the elastic group were similar to those in the bonding group; the level started to increase rapidly after the second hour. However, unlike the bonding group, pain in the elastic group decreased significantly faster from the second day. On the seventh day, only patients in the bonding group reported that they had significant pain during biting on their front teeth. Similar pain levels were reported from the beginning to the next day at all parameters, but then the highest level was found during biting. The literature is lacking a study that investigates the amount of pain generated by intermaxillary elastics; nevertheless, the pain of the placement of braces and bands has been explored in many studies.5,22 The pain characteristic following the placement of braces was found to be similar to this study. Previously, the highest pain levels with the braces were reported during biting on the front teeth9; according to the present results, peak pain levels were found during chewing. In the elastic group the front teeth did not show differences from the other teeth. It must be emphasized that all patients who participated in this study showed good cooperation of elastics and that the pain decreased in 1 week with good compliance of the patient. However, we also predict that this decrease may prolong treatment with a lack of cooperation. Because the patients remove their elastics due to the presence of pain, the pain cycle may never cease.
The initial stage of the orthodontic treatment is a painful process.3 According to the results of this study, the elastic application is also painful for the orthodontic patient. Although bite blocks,23,24 laser therapy,25 and transcutaneous electric nerve stimulation26 were suggested to be effective to reduce the pain, the most common method to overcome patient discomfort is the use of analgesics.27,28 It was shown that taking 2–3 doses of a nonsteroidal anti-inflammatory drug lessened the pain after placement of braces.17 According to the results of this study, it is also necessary to take an analgesic following elastic application. This may be a simple way to promote the use of the elastics and to achieve better treatment results without compromising treatment duration. To avoid a negative impact on cooperation, because of pain, patients should be informed about the pain that they will experience. Furthermore, prescription of an analgesic drug is strongly recommended.
CONCLUSION
The intermaxillary elastics cause pain similar to the initial stage of the treatment, but the pain of the elastics did not last as long as the pain felt after bonding.
REFERENCES
- 1.Scheurer P. A, Firestone A. R, Bürgin W. B. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod. 1996;184:349–357. doi: 10.1093/ejo/18.4.349. [DOI] [PubMed] [Google Scholar]
- 2.Bergius M, Berggren U, Kiliaridis S. Experience of pain during an orthodontic procedure. Eur J Oral Sci. 2002;1102:92–98. doi: 10.1034/j.1600-0722.2002.11193.x. [DOI] [PubMed] [Google Scholar]
- 3.Ngan P, Kess B, Wilson S. Perception of discomfort by patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop. 1989;961:47–53. doi: 10.1016/0889-5406(89)90228-x. [DOI] [PubMed] [Google Scholar]
- 4.Sergl H. G, Klages U, Zentner A. Pain and discomfort during orthodontic treatment: causative factors and effects on compliance. Am J Orthod Dentofacial Orthop. 1998;114:684–691. doi: 10.1016/s0889-5406(98)70201-x. [DOI] [PubMed] [Google Scholar]
- 5.Brown D. F, Moerenhout R. G. The pain experience and physiological adjustments to orthodontic treatment of preadolescents, adolescents and adults. Am J Orthod Dentofacial Orthop. 1991;100:349–356. doi: 10.1016/0889-5406(91)70073-6. [DOI] [PubMed] [Google Scholar]
- 6.Erdinç A. M. E, Dinçer B. Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod. 2004;26:79–85. doi: 10.1093/ejo/26.1.79. [DOI] [PubMed] [Google Scholar]
- 7.Lew K. K. Attitudes and perception of adults towards orthodontic treatment in an Asian community. Community Dent Oral Epidemiol. 1993;21:31–35. doi: 10.1111/j.1600-0528.1993.tb00715.x. [DOI] [PubMed] [Google Scholar]
- 8.Bondemark L, Fredriksson K, Ilros S. Separation effect and perception of pain and discomfort from two types of orthodontic separators. World J Orthod. 2004;52:172–176. [PubMed] [Google Scholar]
- 9.Polat O, Karaman A. I. Pain control during fixed orthodontic appliance therapy. Angle Orthod. 2005;752:214–219. doi: 10.1043/0003-3219(2005)075<0210:PCDFOA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Giannopoulou C, Dudic A, Kiliaridis S. Pain discomfort and crevicular fluid changes induced by orthodontic elastic separators in children. J Pain. 2006;75:367–376. doi: 10.1016/j.jpain.2005.12.008. [DOI] [PubMed] [Google Scholar]
- 11.Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: a randomized controlled clinical trial of two initial aligning arch wires. Am J Orthod Dentofacial Orthop. 1992;102:373–381. doi: 10.1016/0889-5406(92)70054-e. [DOI] [PubMed] [Google Scholar]
- 12.Fernandes L. M, Ogaard B, Skoglund L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. A randomized clinical trial [in English, German] J Orofac Orthop. 1998;59:331–339. doi: 10.1007/BF01299769. [DOI] [PubMed] [Google Scholar]
- 13.Furstman L, Bernick S. Clinical considerations of the periodontium. Am J Orthod. 1972;61:138–155. doi: 10.1016/0002-9416(72)90092-9. [DOI] [PubMed] [Google Scholar]
- 14.Davidovitch Z, Stanfeld J. Biochemical aspects of orthodontic tooth movement. I. Cyclic nucleotide and prostaglandin concentrations in tissues surrounding orthodontically treated teeth in vivo. Am J Orthod Dentofacial Orthop. 1986;90:139–148. doi: 10.1016/0889-5406(86)90046-6. [DOI] [PubMed] [Google Scholar]
- 15.Burstone C. J. The biomechanics of tooth movement. In: Kraus B. S, Riedel R. A, editors. Vistas in Orthodontics. Philadelphia, Pa: Lea & Febiger; 1962. [Google Scholar]
- 16.Krishnan V. Orthodontic pain: from causes to management—a review. Eur J Orthod. 2007;29:170–179. doi: 10.1093/ejo/cjl081. [DOI] [PubMed] [Google Scholar]
- 17.Polat O. Pain and discomfort after orthodontic appointments. Semin Orthod. 2007;13:292–300. [Google Scholar]
- 18.Sinha P. K, Nanda R. S. Improving patient compliance in orthodontic practice. Semin Orthod. 2000;64:237–241. [Google Scholar]
- 19.White L. W. Pain and cooperation in orthodontic treatment. J Clin Orthod. 1984;August:572–575. [PubMed] [Google Scholar]
- 20.Hintze J. NCSS and PASS Number Cruncher Statistical Systems. Kaysville, Utah: 2001. Available at: www.ncss.com. [Google Scholar]
- 21.Krukemeyer A. M, Arruda A. O, Inglehart M. R. Pain and orthodontic treatment. Angle Orthod. 2009;79:1175–1181. doi: 10.2319/121308-632R.1. [DOI] [PubMed] [Google Scholar]
- 22.Bergius M, Broberg A. G, Hakeberg M, Berggren U. Prediction of prolonged pain experiences during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2008;133:339.e1–339.e8. doi: 10.1016/j.ajodo.2007.09.013. [DOI] [PubMed] [Google Scholar]
- 23.Hwang J. Y, Tee C. H, Huang A. T, Taft L. Effectiveness of thera-bite wafers in reducing pain. J Clin Orthod. 1994;28:291–292. [PubMed] [Google Scholar]
- 24.Murdoch S, Phillips C, Khondker Z, Hershey H. G. Treatment of pain after initial archwire placement: a noninferiority randomized clinical trial comparing over-the-counter analgesics and bite wafer use. Am J Orthod Dentofacial Orthop. 2010;137:316–323. doi: 10.1016/j.ajodo.2008.12.021. [DOI] [PubMed] [Google Scholar]
- 25.Fujiyama K, Deguchi T, Murakami T, Fujii A, Kushima K, Takano-Yamamoto T. Clinical effect of CO2 laser in reducing pain in orthodontics. Angle Orthod. 2008;78:299–303. doi: 10.2319/033007-153.1. [DOI] [PubMed] [Google Scholar]
- 26.Roth P. M, Thrash W. J. Effect of transcutaneous electrical nerve stimulation for controlling pain associated with orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 1986;90:132–138. doi: 10.1016/0889-5406(86)90045-4. [DOI] [PubMed] [Google Scholar]
- 27.Nalbantgil D, Cakan D. G, Oztoprak M. O, Arun T. Perception of pain and discomfort during tooth separation. Aust Orthod J. 2009;25:110–115. [PubMed] [Google Scholar]
- 28.Xiaoting L, Yin T, Yangxi C. Interventions for pain during fixed orthodontic appliance therapy. A systematic review. Angle Orthod. 2010;80:925–932. doi: 10.2319/010410-10.1. [DOI] [PMC free article] [PubMed] [Google Scholar]