

Abstract
Objective:
To evaluate transverse changes from Schwarz appliances on both jaws in young, growing patients using cone-beam computed tomography (CBCT).
Materials and Methods:
All subjects had Angle Class I molar relationships and crowding. They were randomly divided into two groups; 30 expanded and 30 control subjects. Three-dimensional CBCT software was used to evaluate and compare treatment effects between the groups. To test for any significant differences between groups at T0 and T1, an independent t-test and paired t-tests were used.
Results:
The interbuccal dentoalveolar width (BDAW), interpalatal dentoalveolar width (PDAW), and interlingual dentoalveolar width (LDAW) values showed significant changes when measured from a point 3 mm coronal to the cementoenamel junction (CEJ) to 8 mm apical to the CEJ. When compared with mandibular interdentoalveolar width differences (BDAW-LDAW), significant differences (P < .05) were observed. The soft tissue width of the maxillary and mandibular teeth and alveolar bone showed no significant changes (P > .05), even with dentoalveolar arch expansion in both jaws.
Conclusions:
This study indicates that Schwarz appliances primarily affect the dentoalveolar complex and have varying effects on mandibular and maxillary alveolar bone width. Also, soft tissue is not affected in the area of expansion in this research.
Keywords: Three-dimensional (3D) CBCT, Multiplanar reconstruction (MPR) image analysis, Superimposition, Iterative closest point (ICP) method, Schwarz appliances
INTRODUCTION
When a maxillary arch is constricted, orthopedic skeletal expansion of the midpalatal suture is the corrective treatment of choice. To normalize the constricted maxillary dental arch, rapid maxillary expansion (RME) is a routine clinical resource in current mechanotherapy. It increases the dental arch perimeter by midpalatal suture splitting and by applying additional buccal rotational force on the maxillary alveolar shelves.1
The maxilla differs from the mandible in that the former is composed of two distinct bones, joined at the midpalatal and intermaxillary sutures. The effects of mandibular expansion are localized to alveolar bones and mainly induce tooth inclination. The reported amount of expansion in the maxilla and mandible differs because of the difference in the expansion mechanism.
Clinicians are interested in evaluating arch width changes that accompany growth and treatment. However, there are still controversies regarding the optimal magnitude and timing of these changes and their impact on treatment planning and ultimate stability. Changes in the arch width that occur because of growth or treatment should be carefully considered during treatment planning. A better understanding of normal growth vs treatment changes in arch width should help to elucidate this clinical problem.
Cone-beam computed tomography (CBCT) analysis allows measurement of transverse dimensions and changes in axial inclination of the posterior teeth in three planes.1 The aim of this study was to quantify and compare the dentoskeletal effects and soft tissue changes produced by Schwarz appliances using a new 3-dimensional (3D) CBCT superimposition method.
MATERIALS AND METHODS
Subjects consisted of 60 patients who were diagnosed with Angle Class I malocclusions with crowding and normal vertical dimensions with no posterior crossbites. The study was approved through protocols set by the Kansai Hospital Ethics Committee. Informed consent was obtained from the participants. After an initial documentation of the data, patients were randomized into two groups: patients treated with Schwarz appliances (exp group) and a nonexpanded control group (nonexp group) (Figure 1). Data were gathered from the groups at two separate times. Initial records were gathered from the exp group before treatment (T0) and then during a retention period of approximately 9 months following 6–12 months of expansion (T1). In the control group, two sets of records were obtained approximately 13–21 months apart. The expanded group consisted of 30 patients (15 male/15 female) with an average age of 8 years 3 months at T0 and 9 years 10 months at T1. The nonexpanded group received no treatment and consisted of 30 subjects (15 male/15 female) with an average age of 7 years 11 months at T0 and 9 years 7 months at T1. Both groups were compared with respect to the transverse dimensions of their mandible and maxilla.
Figure 1.

Lower Schwarz appliance used in this study.
The expanded group used a Schwarz expansion appliance on the maxillary and mandibular dentitions to relieve anterior crowding. Maxillary dental arches were also expanded in all expansion group patients using Schwarz appliances to maintain the buccolingual relationships of occlusal contact in posterior teeth during expansion. Patients wore the expansion appliances at night for approximately 6–12 months. The appliance was activated by rotating its screws weekly (0.175 mm at 90°). Expansion plates were adjusted when the appliance disturbed an erupting tooth or did not fit in the dental arch. A new appliance was fabricated when the screw reached its limit. After 6–12 months of expansion, the screw of the Schwarz appliance was fixed with composite (cured) and used as a retainer. In this study, subjects wore only Schwarz appliances in order to avoid any possible influence from other appliances.
For imaging, the subject's head was positioned so that the Frankfort plane was parallel to the floor with the patient in a seated position, and images were taken at the intercuspal position using CB MercuRay (Hitachi Medical Corporation, Tokyo, Japan) equipment.
Five different software programs, Volume-Rugle (Medic Engineering, Kyoto, Japan), MicroAVS (KGT, Tokyo, Japan), VVD2RGL, Point-Rugle, and 3D-Rugle (Medic Engineering) were used to convert the Digital Imaging and Communications in Medicine (DICOM) data from the CBCT images into polygon data (Figure 2). Registration was performed using these data. After registration, target distances were measured. The iterative closest point (ICP) method2 is able to precisely superimpose images with good repeatability where numerous corresponding points are utilized to compare point-based registrations;3 therefore, this method was used to superimpose the two 3D images at T0/T1 (Figure 3).4
Figure 2.

Flow chart outlining the software and conversions used to derive the polygon data from CBCT DICOM data.
Figure 3.

The ICP method at the cranial base. (A) Superimposition was performed in all areas of the cranial base but not on the peripheral zone that experienced growth. (B) Three-dimensional image represents the superimposition of T1 on T0 at the cranial base.
These methods make accurate superimposition of two separate multiplanar reconstruction (MPR) images possible. Specific points on the cranial base served as reference points for registration (superimposition) to enhance the accuracy of the ICP method since the cranial base is not greatly influenced by growth.5
The combined images were cut down an arbitrary plane and separated into two units. The 3D data were converted into MPR images of the cross-sectional surface and compared. The MPR images, which display excellent dimensional accuracy,6 were used to compare the T0/T1 data.
A slice plane, perpendicular to the occlusal plane and passing through both sides of the mesial buccal cusp tips of the maxillary and mandibular first molars, was prepared for the measurements. 3D-Rugle software was used for the measurements, and the distances at T0/T1 were measured as follows.
The width between the lingual aspects of the crowns and cementoenamel junctions (CEJs), buccal and lingual aspect alveolar bones, and soft tissue were measured at the mandibular and maxillary first molars, the second mandibular and maxillary deciduous molars, the first mandibular and maxillary deciduous molars, and the mandibular and maxillary deciduous canines (Figures 4 and 5).
Figure 4.
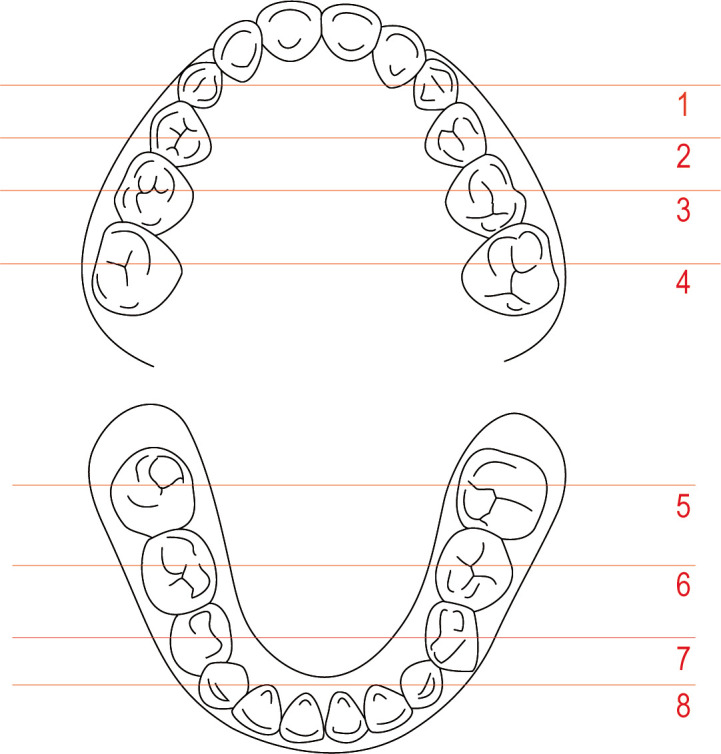
Eight cross-sectional planes for occlusal views of MPR images.
Figure 5.

(A) MPR image showing reference points. (B) Diagram showing reference points and lines.
To determine the relationship between the amount of expansion in hard tissue and soft tissues, axial CBCT images were taken at the crown, CEJ (soft tissue not included), 3 mm, 6 mm, and 8 mm (soft tissue not included) respectively apical to the CEJ. This was done at the mandibular and maxillary first molars, the second mandibular and maxillary deciduous molars, the first mandibular and maxillary deciduous molars, and the mandibular and maxillary deciduous canines (Figures 4 and 5).
To investigate any changes in the nose and eyes during expansion,7 the distance between the right and left exocanthion, endocanthion, alar base, and lip commissure were measured, respectively (Figure 6).
Figure 6.

Superimposed white (before) and blue (after) images representing the effects of treatment in the volume rendering image, distance between the right and left exocanthion (A), endocanthion (B), alar base (C), and lip commissure (D).
Measurement Error
One examiner took all measurements to eliminate interexaminer errors. To identify systematic errors and to compare measurement accuracy, intraexaminer reliability was evaluated. Potential sources of error included data conversion from the different software and linear CBCT measurements. Also, to prevent bias, the investigator was blinded. Software-based data conversion errors and linear CBCT measurement errors were exposed by repeating measurements at least twice on separate occasions 2 weeks apart. Ten randomly selected subjects from each group were measured by the same investigator at least twice on separate occasions. Intraclass correlation coefficients (ICC) of 0.983 were highly reliable.8
Statistical Analysis
Descriptive statistics were calculated for each measurement. Data were analyzed using statistical software (SPSS version 16.0). Treatments changes between the control and treatment groups and between T0 and T1 were analyzed by an independent t-test and paired t-test. A value of P < .05 was considered to indicate statistical significance.
RESULTS
Table 1 shows the interpalatal dentoalveolar width (PDAW) in the maxillary first molars, interlingual dentoalveolar width (LDAW) in the mandibular first molars, interbuccal dentoalveolar width (BDAW), interdentoalveolar width differences in the maxillary first molars (BDAW-PDAW) and in the mandibular first molars (BDAW-LDAW). In the expanded group, the values of the maxillary first molars in PDAW, BDAW, and BDAW-PDAW expanded significantly (P < .05) compared to the control group. The values of BDAW and LDAW in the mandibular first molars in the expanded group expanded significantly (P < .05) compared with the control group except for BDAW-LDAW.
Table 1.
Comparison of Nonexpansion (Nonexp) Group and Expansion (Exp) Group at the First Molarsa

The measurement comparison between the groups at the deciduous canines and first and second molars showed the same statistical results as the permanent first molars in both mandible and maxilla, so result tables were not included in this study.
The interfacial width (soft tissue) of T0/T1 values was measured at the crown and 3 mm and 6 mm apical to the CEJ level, respectively. The soft tissue width was not measured at the CEJ and 8 mm apical to the CEJ because it was presumed there would not be a significant difference (P > .05) from the other soft tissue measurement points. In the soft tissue measurements at the maxilla and mandible, there were no significant changes either in the expanded or control group (P > .05) (Table 2).
Table 2.
Comparison of Nonexpansion (Nonexp) Group and Expansion (Exp) Group of the Soft Tissuea

The inter-exocanthion length, inter-endocanthion length, interalar base length, and interlip commissure were measured. No significant differences (P > .05) were observed between the groups with regard to the soft tissue (Table 3). There were no significant transverse changes of soft tissues after an average of 9 months of expansion (0.175 mm × 4 weeks = 0.7 mm; 0.7 mm × 9 months = 6.3 mm).
Table 3.
Comparison of Nonexpansion Group and Expansion Group on the Surface Dataa

DISCUSSION
One of the goals of early treatment is to correct existing or developing dentoalveolar, skeletal, or muscular imbalances, thus improving the overall oral environment before permanent teeth have completely erupted. By initiating orthodontic and orthopedic therapy at a younger age, it is expected that many future abnormalities in the occlusion will be resolved with a simple second phase of full fixed appliances, thereby reducing the potential need for and severity of complex orthodontic treatment including permanent tooth extraction or orthognathic surgery later.
Several methods are available to expand the maxillary arch, but to achieve the desired skeletal effects, it is necessary to place force directly across the suture. In children, three methods can be used for palatal expansion; a split removable plate with a jackscrew, a quad-helix, or a fixed banded or bonded palatal expander. The rapid palatal expander can be activated for rapid (0.5 mm or more per day), semi-rapid (0.25 mm per day) or slow (1 mm per week) expansion. Removable plates and quad-helix appliances are used for slow expansion.9
It is relatively easy to open the suture in younger children because less force is required. All three types of appliances mentioned above can produce both skeletal and dental expansion in early mixed dentition.10 With a removable appliance, the expansion rate must be slow, and the force employed during the process must be low due to problems with retention. Multiple, well-adjusted clasps are mandatory. Compliance in activation and wear time is always an issue with these appliances.
Widening of both jaws, including the dental arches, should best be completed before any adolescent growth spurt. Usually the intercanine width is more likely to decrease after 12 years of age.11 Changes in arch width exist between boys and girls, and there is more growth in width in the maxillary rather than the mandibular arch.12 In this study, the arch widths in boys grew wider than in girls, and width increased more in the maxillary arch than in the mandibular arch as in the previous studies.12,13 For this reason, girls showed more incisor crowding, particularly mandibular anterior crowding. McNamara and Brudon14 state it is logical to increase the arch size at a young age so that dentoalveolar, skeletal, and muscular adaptations can occur before the eruption of permanent dentition. If an appliance is used in actively growing children, a favorable response can be expected.
Some reports have stated that Schwarz appliances can produce mandibular expansion in only the alveolar bone and may induce tooth inclination.14,15 Although dental arches expand mainly by tooth inclination, the distance between root tips also increases, and the amount of displacement of the alveolar bone is almost the same on the lingual and the buccal side.16 This similarity may be due to remodeling of the alveolar process.
In this study, interdentoalveolar bone widths (BDAW-PDAW, BDAW-LDAW) were significantly different in the maxillary teeth than in the mandibular teeth. As defined originally by Frost,17 bone modeling is an uncoupled process that results in a net change in size or form of osseous tissue. In human adults, typical remodeling rates are about 24% per year for trabecular bone and 3% per year for cortical bone.17 The lower rate in the mandible occurs because only the inner portion of the cortex undergoes the intense turnover of the metabolic fraction, whereas the outer cortex is protected by mechanical function. Therefore, when orthodontic force is applied, maxillary teeth tend to move faster than those in the mandible.
Unlike conventional posteroanterior cephalometric radiographic analysis, this new method permits the precise fusing of two 3D images and then the sectioning of the resulting MPR image through an arbitrary plane so dimensional changes in the cross-sectional surface can easily be evaluated, even in young, growing patients.
This technique is not difficult to learn; however, as with other orthodontic software programs, it takes time to become proficient performing the data conversions, superimpositions, and measurements. Once learned, image measurements can be done with great repeatability. While this sort of measurement might be made with other 2D or 3D procedures or with a cast analysis, this new method is more accurate because it measures the same points on the same surface of an object that was fused with T0/T1 images and can be cut on any arbitrary plane.
From this study, expansion across the nasal floor was 1.17 mm, or 19% of the mean Schwarz appliance expansion of 6.3 mm. This is similar to findings with computed tomography by Garib et al.18 who found nasal floor separation to be one-third of the expansion from a fixed RME appliance. With removable Schwarz appliances it was difficult to predict midpalatal suture opening, but when it was opened, expansion of the lower nasal cavity side wall was observed.
In this study, CBCT measurements showed that the alveolar ridges tip and bend buccally and teeth also tip buccally within the alveoli during expansion. For example, the maxillary and mandibular first molar tipped approximately 8° and 8.7°, respectively, which was similar to our previous study.19
A fixed RME appliance expands the nasal cavity width by an average 1.9 mm, but it widens it as much as 8–10 mm at the inferior turbinates,20 while the more superior areas might move medially.21 Increased nasal cavity width has important clinical implications with respect to nasal breathing because of increased permeability.22
An interesting finding in this study is that increased nasal width was not consistent on a 1 to 1 ratio with the skeletal increases noted in previous studies using fixed rapid expansion appliances.8 The removable, slow expansion appliance did not change facial appearance, and there was no significant difference (P > .05) compared with the control group.
Removable expanders are able to generate considerable forces in young children that may be able to stimulate the midpalatal suture, especially when the appliance is worn for many hours. The findings of this research and clinical experience are encouraging when answering the efficacy of the removable expander, but long-term stability studies are still need.
Future studies will include long-term data including postexpansion measurements from patients who used different types of expansion appliances. The present study was focused primarily on evaluating overall transverse changes over time with MPR image analysis derived from 3D superimposition in patients using a Schwarz appliance in comparison to a control group.
CONCLUSIONS
MPR image measurements demonstrated that Schwarz appliances expand maxillary and mandibular alveolar processes at the first molars, the deciduous second molars, the deciduous first molars, and deciduous canines, respectively. No significant difference was found in the surface point of soft tissue that corresponded, respectively, after 6.3 mm of slow expansion.
Mandibular bone width was not expanded significantly by the Schwarz appliance; however, maxillary bone width changes were observed. This means that other options would be necessary to achieve mandibular bone width expansion.
The distance between the right and left exocanthion, endocanthion, alar base, and lip commissure were not expanded by the Schwarz appliance.
REFERENCES
- 1.Garrett B. J, Caruso J. M, Rungcharassaeng K, Farrage J. R, Kim J. S, Taylor G. D. Skeletal effects to the maxilla after rapid maxillary expansion assessed with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2008;134:8.e1–8.e11. doi: 10.1016/j.ajodo.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Besl P. J, McKay N. D. A method for registration of 3-dimensional shapes. IEEE Trans Pattern Anal Mach Intell. 1992;14:239–256. [Google Scholar]
- 3.Arun K. S, Huang T. S, Blostein S. D. Least-squares fitting of two 3-dimensional point sets. IEEE Trans Pattern Anal Mach Intell. 1987;9:698–700. doi: 10.1109/tpami.1987.4767965. [DOI] [PubMed] [Google Scholar]
- 4.Tai K, Park J. H, Mishima K, Hotokezaka H. Using superimposition of 3-dimensional cone-beam computed tomography images with surface-based registration in growing patients. J Clin Pediatr Dent. 2010;34:361–367. doi: 10.17796/jcpd.34.4.w8n6321878105431. [DOI] [PubMed] [Google Scholar]
- 5.Nie X. Cranial base in craniofacial development: developmental features, influence on facial growth, anomaly, and molecular basis. Acta Odontol Scand. 2005;63:127–135. doi: 10.1080/00016350510019847. [DOI] [PubMed] [Google Scholar]
- 6.Kataoka Y, Nakano H, Matsuda Y, Araki K, Okano T, Maki K. Three dimensional diagnostic imaging of the alveolar bone using dento-maxillofacial cone beam X-ray CT. Orthod WavesJpn Ed. 2007;66:81–91. [Google Scholar]
- 7.Berger J. L, Pangrazio-Kulbersh V, Thomas B. W, Kaczynski R. Photographic analysis of facial changes associated with maxillary expansion. Am J Orthod Dentofacial Orthop. 1999;116:563–571. doi: 10.1016/s0889-5406(99)70190-3. [DOI] [PubMed] [Google Scholar]
- 8.Bravo G, Potvin L. Estimating the reliability of continuous measures with Cronbach's alpha or the intraclass correlation coefficient: toward the integration of two traditions. J Clin Epidemiol. 1991;44:381–390. doi: 10.1016/0895-4356(91)90076-l. [DOI] [PubMed] [Google Scholar]
- 9.Proffit W. R, Fields H. W, Jr, Sarver D. M. Contemporary Orthodontics 4th ed. St Louis, Mo: Mosby; 2007. [Google Scholar]
- 10.Sandikçiolu M, Hazar S. Skeletal and dental changes after maxillary expansion in the mixed dentition. Am J Orthod Dentofacial Orthop. 1997;111:321–327. doi: 10.1016/s0889-5406(97)70191-4. [DOI] [PubMed] [Google Scholar]
- 11.Bishara S. E, Jakobsen J. R, Treder J, Nowak A. Arch width changes from 6 weeks to 45 years of age. Am J Orthod Dentofacial Orthop. 1997;111:401–409. doi: 10.1016/s0889-5406(97)80022-4. [DOI] [PubMed] [Google Scholar]
- 12.Lee R. T. Arch width and form: a review. Am J Orthod Dentofacial Orthop. 1999;115:305–313. doi: 10.1016/S0889-5406(99)70334-3. [DOI] [PubMed] [Google Scholar]
- 13.Tsujino K, Machida Y. A longitudinal study on the growth and development of the dental arch width from childhood to adolescence [in Japanese] Jpn J Pedodontics. 1997;35:670–683. [PubMed] [Google Scholar]
- 14.McNamara J. A, Jr, Brudon W. L. Orthodontic and Orthopedic Treatment in the Mixed Dentition. Ann Arbor, Mich: Neeedham Press; 1993. [Google Scholar]
- 15.Schwarz A. M, Gratzinger M. Removable Orthodontic Appliances. Philadelphia, Pa: WB Saunders; 1966. [Google Scholar]
- 16.Motoyoshi M, Shirai S, Yano S, Nakanishi K, Shimizu N. Permissible limit for mandibular expansion. Eur J Orthod. 2005;27:115–120. doi: 10.1093/ejo/cjh092. [DOI] [PubMed] [Google Scholar]
- 17.Frost H. M. Skeletal structural adaptations to mechanical usage (SATMU): 1. Redefining Wolff's law: the bone modeling problem. Anat Rec. 1990;226:403–413. doi: 10.1002/ar.1092260402. [DOI] [PubMed] [Google Scholar]
- 18.Garib D. G, Henriques J. F. C, Janson G, Freitas M. R, Coelho R. A. Rapid maxillary expansion—tooth tissue-borne versus tooth-borne expanders: a computed tomography evaluation of dentoskeletal effects. Angle Orthod. 2005;75:548–557. doi: 10.1043/0003-3219(2005)75[548:RMETVT]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 19.Tai K, Hotokezaka H, Park J. H, Tai H, Miyajima K, Choi M, Kai L, Mishima K. Preliminary cone-beam computed tomography study evaluating dental and skeletal changes after treatment with a mandibular Schwarz appliance. Am J Orthod Dentofacial Orthop. 2010;138:262.e1–262.e11. doi: 10.1016/j.ajodo.2010.02.023. [DOI] [PubMed] [Google Scholar]
- 20.Marcotte M. R. The instantaneous transverse changes in the maxilla due to different points of force application. J Dent Res. 1977;56:465–470. doi: 10.1177/00220345770560050301. [DOI] [PubMed] [Google Scholar]
- 21.Gray L. P. Results of 310 cases of rapid maxillary expansion selected for medical reasons. J Laryngol Otol. 1975;89:601–614. doi: 10.1017/s0022215100080804. [DOI] [PubMed] [Google Scholar]
- 22.Gray L. P. Rapid maxillary expansion and impaired nasal respiration. Ear Nose Throat J. 1987;66:248–251. [PubMed] [Google Scholar]