

Abstract
Objectives:
To test the hypotheses that the Damon system will maintain intercanine, interpremolar, and intermolar widths. To test subsequent hypotheses that the Damon system will not produce a significant difference in maxillary and mandibular incisor position/angulation when compared with control groups treated with conventional fixed orthodontic appliances for similar malocclusion.
Materials and Methods:
Subjects treated with the Damon system (N = 27) were compared with subjects treated with a conventionally ligated edgewise bracket system (N = 16). Subjects' pretreatment and posttreatment lateral cephalometric radiographs and dental models were scanned, measured, and compared to see whether significant differences exist between time points and between the two groups.
Results:
Results did not support the claimed lip bumper effect of the Damon system and showed similar patterns of crowding alleviation, including transverse expansion and incisor advancement, in both groups, regardless of the bracket system used.
Conclusions:
Maxillary and mandibular intercanine, interpremolar, and intermolar widths increased significantly after treatment with the Damon system. The mandibular incisors were significantly advanced and proclined after treatment with the Damon system, contradicting the lip bumper theory of Damon. Posttreatment incisor inclinations did not differ significantly between the Damon group and the control group. Patients treated with the Damon system completed treatment on average 2 months faster than patients treated with a conventionally ligated standard edgewise bracket system.
Keywords: Digital, 3-Dimensional, Damon, Incisor
INTRODUCTION
In the 1990s, Dwight Damon developed a theory asserting that low friction and light forces produced more biologically stable results. His philosophy was the impetus for the creation of his orthodontic appliance system. The Damon system includes broad archwires and self-ligating brackets with a twin configuration and a passive slide on the outward face of the bracket. Studies have shown that self-ligating brackets have less friction during sliding mechanics than conventionally ligated counterparts, and Damon brackets in particular have exhibited less friction than ligated brackets.1–4
Some practitioners claim that the reduced frictional levels of self-ligating brackets lead to faster treatment progress, fewer appointments, and reduced treatment times.5–7 The Damon philosophy also states that biologically friendly light forces do not overpower the musculature. Instead, the arch form aligns by taking the path of least resistance, which is posterior expansion.8,9 The perioral muscles, like the orbicularis oris and the mentalis muscle, act as a “lip bumper,” which minimizes the anterior movement of the incisors.9 Damon also believes that the mandibular intercanine width does not change significantly with his system, and his lateral cephalometric tracings show minimal labial movement of incisors in his published articles. In cases of Class I malocclusion with anterior crowding and treated nonextraction using conventionally ligated brackets, mandibular incisors are typically advanced and proclined.10,11 When the Damon 2 bracket system was compared with a conventional edgewise counterpart, both groups experienced an increase in mandibular incisor proclination and mandibular transverse dimension. In fact, the only significant difference noted between groups was an increase in mandibular intermolar width in the sample treated with self-ligating brackets.11 Crowding was resolved by a combination of transverse expansion and incisor proclination, regardless of the bracket type used.
The purpose of this study was to evaluate radiographically the anteroposterior change in the position and inclination of the maxillary and mandibular incisors (whether the posttreatment incisor inclinations differed between the two samples) and to examine transverse (intercanine, interpremolar, and intermolar) dimension changes in dental arches treated with the Damon system.
MATERIALS AND METHODS
Approval to conduct this study was obtained from a university institutional review board. Patients were retrospectively selected as subjects from one private practice orthodontic office because their malocclusions met the following criteria: a Class I dental and skeletal malocclusion, permanent dentition, no prior orthodontic treatment, constricted arches or crowding in both arches, and no skeletal crossbites present. A total of 27 patients underwent orthodontic treatment with a 0.022-inch-slot Damon appliance, and 16 patients underwent orthodontic treatment with a 0.018-inch-slot conventionally ligated standard edgewise bracket system. All mechanics were consistent with a nonextraction treatment plan. No other appliances (ie, headgear, Herbst, lip bumper, or distalizing appliances) were used in conjunction with the Damon system.
In the group treated with the conventionally ligated edgewise system, the brackets used were standard edgewise (Dentsply GAC, Bohemia, NY). The treating orthodontist used the following archwire sequence: 0.013-inch nickel titanium (NiTi) or 0.014-inch copper (Cu) NiTi (Ormco, Glendora, Calif); 0.016-inch Cu NiTi (Highland Metals, San Jose, Calif); 0.016-inch stainless steel (SS) (Oscar, Fisher, Ind); and 0.016 × 0.022-inch SS (Rocky Mountain Orthodontics, Denver, Colo). The orthodontist did not use a template for any of the SS archwires before placing them in the mouth. Instead, he used patients' pretreatment arch forms as a guide in this sample. Torque was placed in the steel archwires as needed. In the group treated with the Damon appliance, D3 MX self-ligating brackets (Ormco) were bonded. The following Ormco archwires were sequentially used: 0.012- to 0.014-inch Cu NiTi; 0.016-inch Cu NiTi; 0.014 × 0.025-inch Cu NiTi; 0.018 × 0.025-inch Cu NiTi; and 0.019 × 0.025-inch titanium molybdenum alloy (TMA) or SS.
The subjects' casts were deidentified by the staff of a private practice orthodontist from whom the sample was collected. Pretreatment and posttreatment plaster models for all 43 patients were scanned using a nondestructive, three-axis laser surface scanner (3Shape R-700 Desktop Orthodontic Scanner, Copenhagen, Denmark). The model was placed on a platform capable of rotating and tilting, enabling a dual-image capture from two cameras and one laser (Figure 1A). A high-resolution scan of each model took approximately 2 minutes. Images produced were stereolithography (STL) files with an accuracy of 0.20 micron (Figure 1B). Measurements such as the curve of Spee (Figure 1C) and arch perimeter (Figure 1D) were then performed on these digital images using analytical software (ESM Digital Solutions, Dublin, Ireland).
Figure 1.

(A) 3Shape R-700 three-dimensional (3D) study model scanner. (B) R-700 digital model scanning software. (C) 3D cast generated by 3Shape R-700 scanner used to measure curve of Spee. (D) 3D cast generated by 3Shape R-700 scanner used to measure dental arch perimeter discrepancy.
The following measurements, illustrated in Figure 2, were collected to determine the transverse and anteroposterior changes that occurred during treatment:
Figure 2.

Transverse and anteroposterior measurements. (A) Arch depth to canines. (B) Intercanine width. (C) Inter–first premolar width. (D) Inter–second premolar width. (E) Intermolar width. (F) Arch depth to mesial of first molars.
Transverse measurements: intercanine width measured at the cusp tip of the canines, inter–first premolar width measured at the central occlusal pit of the first premolar, inter–second premolar width measured at the central occlusal pit of the second premolar, and intermolar width measured at the central occlusal pit on the mesial fossa of the first molar
Anteroposterior measurements: arch depth at the canines, measured from the mid arch point between incisors perpendicular to a line connecting the cusp tips of the canines, arch depth at the first molar, measured from the mid arch point between central incisors perpendicular to a line connecting the mesial contact points of the first molars
Additional intra-arch measurements: curve of Spee, measured from the perpendicular distance between the most gingival cusp tip in the dental arch to a line drawn from the central incisor incisal edge to the mesiobuccal cusp tip of the first molar in the same quadrant, and crowding, measured as the absolute value of the space required subtracted from the space available in the dental arch, as shown in Figure 3
Figure 3.
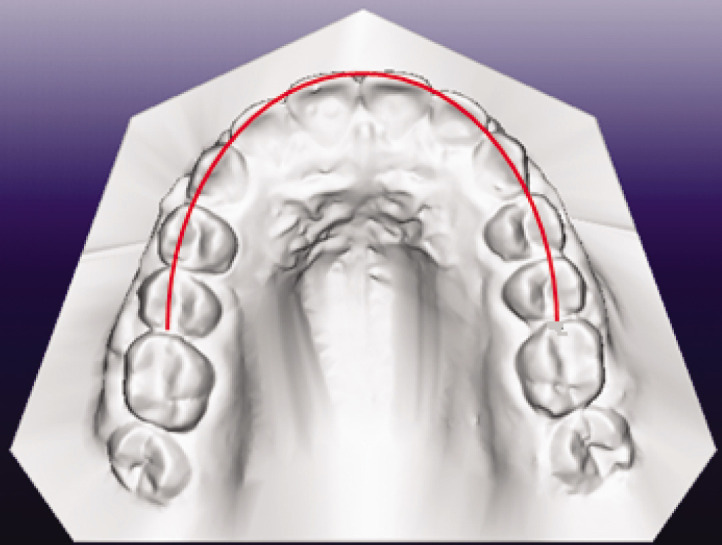
Measurement for arch perimeter in the dental arch.
Each subject's pretreatment and posttreatment lateral cephalometric radiographs were scanned using Adobe Photoshop 7.0 (San Jose, Calif) and were digitally traced using Dolphin, version 10.5 (Chatsworth, Calif). All lateral cephalometric radiographs were traced by the primary investigator, and pretreatment and posttreatment radiographs were superimposed on constant landmarks. The following measurements are illustrated in Figure 4 and were performed on both pretreatment and posttreatment lateral cephalometric radiographs:
Figure 4.

Diagram of the cephalometric points and planes used.
The angle formed by the intersection of a line from nasion to A point (NA) with a line drawn along the maxillary central incisor long axis (U1)
The angle formed by the intersection of a line from A point to pogonion (APog) with a line drawn along the maxillary central incisor long axis (U1)
The angle formed by the intersection of a line drawn along the mandibular plane (MP) with a line drawn along the mandibular central incisor long axis (L1)
The angle formed by the intersection of a line from A point to pogonion (APog) with a line drawn along the mandibular central incisor long axis (L1)
Ten sets of lateral cephalometric radiographs were randomly selected, traced, and superimposed according to the previous criteria. Radiographs were retraced, superimposed, and remeasured 1 month later to assess intraoperator reliability. Before the casts were scanned and measurements were taken using ESM Digital Solutions software, the reliability of this scanner was tested. A total of 10 sets of casts were randomly selected and scanned using the desktop scanner. The corresponding 10 pretreatment plaster study models were also measured using digital calipers (Nesco Electronic Digital Calipers, Canton, Mass). High reliability was confirmed for the radiographs and dental model measurements.
Statistical Analysis
The Shapiro-Wilk test was performed on all measurements to ensure that the variables were normally distributed. For those variables for which normality was confirmed, a paired sample t-test was used to assess differences in the means between pretreatment and posttreatment values. The Mann-Whitney test was performed on the variables that were not distributed normally to determine whether the Damon and conventionally ligated groups were significantly different.
An independent t-test was used to assess differences in means between the posttreatment values of both the Damon group and the conventionally ligated group. Last, correlations between incisor inclination, curve of Spee, and crowding were evaluated using the Pearson correlation coefficient.
RESULTS
When the Damon sample was analyzed, results showed that intercanine, inter–first premolar, inter–second premolar, and intermolar widths were significantly larger after treatment (Table 1). The mandibular incisor was proclined, as indicated by the measurement L1-MP. The mandibular incisor was also advanced anteroposteriorly, as indicated by L1-APog and supported by an increase in arch depth. Maxillary incisors were not significantly proclined or advanced at the .05 confidence level.
Table 1.
T-tests of Differences Between Time Points T1 and T2 for The Damon Group

When the sample treated with conventionally ligated edgewise brackets was analyzed, results show that the maxillary and mandibular incisors were significantly proclined after treatment with conventionally ligated edgewise appliances, as indicated by U1-SN and L1-MP, respectively (Table 2). In the transverse dimension, maxillary and mandibular intercanine, inter–first premolar, and inter–second premolar widths were significantly larger after treatment. The mandibular intermolar width showed significant expansion after treatment with no statistically significant expansion on the maxillary intermolar width.
Table 2.
T-tests of Differences Between Time Points T1 and T2 for The Conventionally-Ligated Group

When the two samples were compared, the only significant difference between groups was noted in the maxillary intermolar width. The change in maxillary intermolar width in the Damon group was significantly greater when compared with the conventionally ligated group (P < .05) (Table 3).
Table 3.
T-test of T2-T1 Differences Between Groups Normally Distributed

Pearson correlations revealed that the initial curve of Spee, initial crowding in the mandibular arch, and final incisor inclination were not statistically significant in either sample at the .05 level (Tables 4 and 5).
Table 4.
Correlations Between Initial Crowding, Curve of Spee, and Final Incisor Inclination in The Damon Group (N = 27)

Table 5.
Correlations Between Initial Crowding, Curve of Spee, and Final Incisor Inclination in The Conventionally-Ligated Group (N = 16)

DISCUSSION
Mandibular incisor proclination and advancement are common findings in studies that analyze alleviation of crowding. Studies have consistently shown that advancement of the mandibular incisors, along with expansion of the buccal segments, occurs when crowding is alleviated during nonextraction treatment when no other appliances (eg, headgear, distalizers, lip bumpers) are used.8,10,11 In fact, Pandis et al.8 observed a 7- to 8-degree proclination of mandibular incisors associated with crowding alleviation when Damon 2 brackets were used; their results were very similar to those obtained in the current study. The notion that incisor advancement and proclination will be significantly less using the Damon system could not be supported by this study. The use of Class II elastics in this study was minimal but could have contributed to mandibular incisor proclination.12,13 Increases in transverse dimension in the Damon group could be explained by the wide Ormco Cu-NiTi archwires that were used during the first part of treatment. However, according to this logic, it would be expected that the mandibular intermolar width would be significantly greater after treatment in the Damon group than in the conventionally ligated group, but this result was not observed, possibly because of the bone biology of the mandible. Mandibular bone is denser than maxillary bone, possibly hindering the extent of mandibular molar expansion. Dental changes produced by the Damon system were not significantly different from those seen with the conventionally ligated bracket system, with the exception of maxillary intermolar expansion. This could also be explained by the difference in transverse dimension between the heaviest SS archwires used in each sample. For example, a Damon maxillary 19 × 25-inch SS archwire has an arch depth of 65 mm on average. The maxillary 16 × 22-inch SS archwire used in the conventionally ligated sample had a transverse dimension of only 65.5 mm at the same arch depth of 65 mm. The greater transverse dimension of the maxillary archwire used in the Damon group could help explain why greater maxillary intermolar expansion was seen in this group as compared with the conventionally ligated sample.
The study could have been improved by eliminating as many differences as possible between the two samples, for example, it would be ideal to have the same manufacturer and slot size utilized in both samples. Studies have been done that examine the mandibular arch only, but more studies with large sample sizes are needed that analyze both arches. Further research comparing the Damon system vs conventionally ligated counterparts would help practitioners identify the strengths and limitations of the Damon system, and the information gained would be a valuable tool in patient selection.
CONCLUSIONS
Intercanine width increased significantly after treatment with the Damon system.
Inter–first premolar and inter–second premolar widths increased significantly after treatment with the Damon system.
Maxillary and mandibular intermolar widths increased significantly after treatment with the Damon system. Maxillary intermolar width was significantly larger by 2.19 mm after treatment with the Damon group compared with the conventionally ligated group.
Mandibular incisors were advanced significantly after treatment with the Damon system, contradicting the lip bumper theory of Damon.
Only the mandibular incisors were proclined significantly after treatment with the Damon system.
Posttreatment incisor inclinations did not differ significantly between the Damon group and the control group.
Acknowledgments
We would like to acknowledge Dr James McNamara (Ann Arbor, Mich), Mr Mark Berry of ESM Digital Solutions (Dublin, Ireland), and Mr Allen Yunqing Pan (Chicago, Ill) for their time, effort, and assistance with the 3D scanning technology used in this research.
REFERENCES
- 1.Damon D. H. The rationale, evolution and clinical application of the self-ligating bracket. Clin Orth Res. 1998a;1:52–61. doi: 10.1111/ocr.1998.1.1.52. [DOI] [PubMed] [Google Scholar]
- 2.Voudouris J. C. Interactive edgewise mechanisms: form and function comparison with conventional edgewise brackets. Am J Orthod Dentofacial Orthop. 1997;111:119–139. doi: 10.1016/s0889-5406(97)70208-7. [DOI] [PubMed] [Google Scholar]
- 3.Pizzoni L, Ravnholt G, Melsen B. Frictional forces related to self-ligating brackets. Eur J Orthod. 1998;20:283–291. doi: 10.1093/ejo/20.3.283. [DOI] [PubMed] [Google Scholar]
- 4.Kim T. K, Kim K. D, Baek S. H. Comparison of frictional forces during the initial leveling stage in various combinations of self-ligating brackets and archwires with a custom-designed typodont system. Am J Orthod Dentofacial Orthop. 2008;133:187.e15–187.e24. doi: 10.1016/j.ajodo.2007.08.013. [DOI] [PubMed] [Google Scholar]
- 5.Birnie D. The Damon passive self-ligating appliance system. Semin Orthod. 2008;14:19–35. [Google Scholar]
- 6.Harradine N. W. Self-ligating brackets and treatment efficiency. Clin Orthod Res. 2001;4:220–227. doi: 10.1034/j.1600-0544.2001.40406.x. [DOI] [PubMed] [Google Scholar]
- 7.Eberting J. J, Straja S. R, Tuncay O. C. Treatment time, outcome, and patient satisfaction comparisons of Damon and conventional brackets. Clin Orthod Res. 2001;4:228–234. doi: 10.1034/j.1600-0544.2001.40407.x. [DOI] [PubMed] [Google Scholar]
- 8.Pandis N, Polychronopoulou A, Eliades T. Self-ligating vs conventional brackets in the treatment of mandibular crowding: a prospective clinical trial of treatment duration and dental effects. Am J Orthod Dentofacial Orthop. 2007;132:208–215. doi: 10.1016/j.ajodo.2006.01.030. [DOI] [PubMed] [Google Scholar]
- 9.Damon D. H. The Damon low-friction bracket: a biologically compatible straight-wire system. J Clin Orthod. 1998b;32:670–680. [PubMed] [Google Scholar]
- 10.Weinberg M, Sadowsky C. Resolution of mandibular arch crowding in growing patients with Class I malocclusions treated nonextraction. Am J Orthod Dentofacial Orthop. 1996;110:359–364. doi: 10.1016/s0889-5406(96)70035-5. [DOI] [PubMed] [Google Scholar]
- 11.Fleming P, DiBiase A. T, Sari G, Lee R. T. Comparison of mandibular arch changes during alignment and leveling with 2 preadjusted edgewise appliances. Am J Orthod Dentofacial Orthop. 2009;136:340–347. doi: 10.1016/j.ajodo.2007.08.030. [DOI] [PubMed] [Google Scholar]
- 12.Combrink F. J, Harris A. M, Steyn C. L, Hudson A. P. Dental skeletal and soft-tissue changes in growing Class II malocclusion patients during nonextraction orthodontic treatment. SADJ. 2006;61:344–350. [PubMed] [Google Scholar]
- 13.Jones G, Buschang P. H, Kim K. B, Oliver D. R. Class II non-extraction patients treated with the Forsus fatigue resistant device versus intermaxillary elastics. Angle Orthod. 2008;78:332–338. doi: 10.2319/030607-115.1. [DOI] [PubMed] [Google Scholar]