

Abstract
Working from a life course perspective, we examined how acquiescence (i.e., “lack of resistance”) to an unwanted (i.e., “without experiencing a concomitant desire”) first sexual experience was related to health and well-being in late life. Data were drawn from the second wave of the National Social Life, Health, and Aging Project (2010/11). The sample included 2558 older adults ages 62–99 (1182 men and 1376 women). Results from regression models suggested those respondents whose first sex was acquiesced reported higher levels of psychological distress and poorer physical health during late life than respondents whose first sex was wanted. Results from generalized structural equation modeling analysis further suggested that the association between acquiesced first sex and late-life health operated through adulthood socioeconomic status but not through marital relationships. We did not find gender differences in these processes.
Keywords: First sex, Sexual acquiescence, Psychological distress, Self-rated health, Older adults
Introduction
Most Americans’ first experience of sex occurs during adolescence and young adulthood, constituting a major life milestone (Heywood et al., 2015). In the United States, the median age of first sexual intercourse is about 17, with boys engaging in sex slightly earlier than girls (Finer & Philbin, 2014). The common assumption is that, except in cases of rape, individuals who engage in sex did so because they desired it (Houts, 2005). However, empirical evidence indicates that even when young adults first engage in sex with a chosen partner, many of these sexual experiences are marked by the ambiguity of their wantedness or one partner acquiesces to sex (Abma et al., 2010; Houts, 2005; Katz & Schneider, 2015), with sexual acquiescence more common among women than men (Laumann et al., 1994; Martinez et al., 2011). Following Conroy et al. (2015), we define sexual acquiescence as “lack of resistance to unwanted sexual activity” (p. 1842). O’Sullivan and Allgeier (1998) define unwanted sexual activities as “situations in which a person freely consents to sexual activity with a partner without experiencing a concomitant desire for the initiated sexual activity” (p. 234). Previous studies of first sexual experience have focused primarily on predicting the timing of sexual initiation, and thus researchers do not yet have a thorough understanding of the long-term health consequences of acquiesced first sexual experience or the life-course pathways that lead to such consequences.
Using data from the second wave of the National Social Life, Health, and Aging Project (NSHAP), we present one of the first population-based studies on the long-term effects of acquiesced first sexual experience on late-life health and well-being. We address three major research questions. First, is acquiesced first sexual experience related to individuals’ psychological distress and self-rated physical health in late life? Second, what are the specific pathways through which acquiesced first sexual experience is linked to individual health and well-being over the life course? We focus on two potential pathways—adult-hood socioeconomic status and marital relationships—based on prior evidence of their linkages to early life sexuality as well as their significance for health and well-being. Third, do these processes differ by gender? The results can inform policy and public programs that seek to assist individuals with the long-term recovery process after an early acquiesced sexual experience.
Previous Studies on Sexual Acquiescence
Recent literature has expanded on how social and cultural expectations exist to pressure a person into having an unwanted sexual activity (Conroy et al., 2015) and that sexual wantedness exists on a continuum (Peterson & Muehlenhard, 2007). Scholars argue that in situations where a person feels they are unable to decline sex—perhaps for fear of social or interpersonal consequences from their refusal (Conroy et al., 2015)—it is challenging to determine if sex is actually consensual (Fahs et al., 2020). Sexual acquiescence is a commonly used term to depict unwanted, nonviolent sexual activity, where a person just “went along with it.” Conroy et al. (2015) note that sexual acquiescence occurs when one has unwanted sexual activity without giving clear consent—this may be passively participating or not protesting the sexual activity occurring.
Research suggests that a significant share of Americans, particularly women, acquiesced to their first sexual intercourse (Abma et al., 1998; Houts, 2005; Laumann et al., 1994; Weitzman & Mallory, 2019). Analysis of representative data from the National Health and Social Life Survey suggested that about a quarter (24.5%) of women reported not wanting their first intercourse to happen, although they were not forced into it; instead, many reported acquiescing because of feelings for their sexual partner or pressure from their peers (Laumann et al., 1994). Another national study based on data from the 1995 National Study of Family Growth (NSFG) also suggested that about one-quarter of women ages 15–24 reported their first intercourse was voluntary but not wanted (Abma et al., 1998). Furthermore, women in racial-ethnic minority groups or in low socioeconomic status were found to be less willing to refuse unwanted sex than others (Abma et al., 1998; Houts, 2005; Weitzman & Mallory, 2019). A descriptive study (without controlling for any covariates) of first coital experience using 2006–2010 NSFG data found that 48% of women and 32.5% of men were ambivalent about their wantedness of first inter-course with mixed feelings about the experience occurring, while 10.8% of women and 5% of men indicating they did not want their first sexual experience to occur at the time (Martinez et al., 2011)—suggesting that sexual acquiescence occurred for both men and women.
Previous research indicates that there are various reasons why a person may acquiesce to sex. They may do so in order to promote or maintain commitment or intimacy with their partner, or they may “go along with” unwanted sex in order to avoid negative pressures to have sex, such as physical or mental coercion (Conroy et al., 2015; Katz & Tirone, 2010). A person may also acquiesce to sex because they put their partner’s desires above their own (Moor et al., 2020), or they see it as their duty or feel socially coerced (Basile, 1999; Finkelhor & Yllo, 1987). One qualitative study that interviewed 11 women and 10 men 19–30 years old about acquiescence in their casual sex experiences found that women tended to report that they just “went along with” what was happening because they were uncertain about their sexual desire and interest, while men also reported ambiguity about how their female partner felt in the sexual moment (Beres, 2010).
So far, little research has been conducted to examine the health effects, especially long-term, of sexual acquiescence, although a growing body of research has considered how unwanted, unforced sex is linked to health outcomes. A study of 566 female college students found that having a sexual experience against their will was related to higher levels of psychological distress (Crown & Roberts, 2007). Another study of 178 undergraduate men and women found that those women who had unwanted sexual intercourse during a hook-up experienced elevated stress in response to that incident (Flack et al., 2007). A study of 64 college students found that men and women who complied with more frequent sex than they desired had higher levels of stress, as measured by cortisol, compared to those who had the sexual frequency that they desired (Hartmann & Crockett, 2016). Note, none of the aforementioned studies have controlled for socioeconomic status and in fact, most prior studies in this area are based on samples of young or middle-aged individuals—often college students—with very few control covariates. Few studies have examined how acquiescence during the first sexual experience may shape health in later life through specific life-course pathways.
A Life Course Perspective on Cumulative Disadvantage: Understanding the Link Between Acquiescence During First Sexual Experience and Late-Life Health
Increasingly, health scholars use a life-course perspective to explore the influence of early life experiences on health development over the life course (Mayer, 2009). Both theoretical and empirical work suggests that early life adversity may have cumulative effects on individuals’ health and well-being throughout their life span (Haas, 2008; Hatch, 2005; Hayward & Gorman, 2004; Miller et al., 2011; Shonkoff et al., 2009; Umberson et al., 2014; Warner & Hayward, 2006). The cumulative-advantage/disadvantage theory suggests that advantages or disadvantages experienced in early life launch individuals onto distinct developmental pathways that persist into later stages of the life course. Early life adversity initiates a life-course chain of “insults” (Hayward & Gorman, 2004) wherein earlier disadvantages are compounded or amplified across the life course, thus leading to later disadvantages due to an increasingly compromised capacity to cope with new insults (O’Rand & Hamil-Luker, 2005). This proliferation of disadvantages takes a toll on health over the life course via “successively contingent structural constraints, life course transitions, and health behaviors that increase disease risk” (O’Rand & Hamil-Luker, 2005, p. 117).
Early life disadvantages such as experiencing poverty, parental divorce, or domestic violence during childhood are well documented to be associated with poorer physical and mental health and well-being in later life (Fors et al., 2009; Kalil et al., 2016; Miller et al., 2011; Pakpahan et al., 2017). Analogous to these early life disadvantages, a first sexual experience where one sexually acquiesced may modify the subsequent context of an individual’s life course, for example by interfering in an individual’s education (Erickson & Rapkin, 1991; Zimmer-Gembeck & Helfand, 2008) or marital relationships (Basile, 1999)—as discussed next, and may, in turn, have negative health impacts over the life course (Weitzman & Mallory, 2019). Our general hypothesis is that:
Hypothesis 1 Acquiescence during the first sexual experience is related to poorer health and well-being in late life.
Educational Achievement and Socioeconomic Status
Research on the relationship between adolescent sexual behavior and academic attainment has found that unwanted early sexual activity is negatively related to academic success (Erickson & Rapkin, 1991) potentially via an association with teen parenthood (Hofferth et al., 2001; Hoffman et al., 1993). Additionally, data from a majority-white sample of middle and high school students indicate that those who delay their sexual debut have better school performance (Lammers et al., 2000). Adolescent girls who experience unwanted sex are less likely to use contraception and thus more likely to experience teen childbearing, which can disrupt school performance and increase the risk of school dropout (Erickson & Rapkin, 1991). In contrast, those whose first sex is wanted and planned to are more likely to use contraception at first intercourse (Fairfortune et al., 2020; Ott et al., 2012), which may facilitate adherence to a planned academic path and achievement of academic goals. Moreover, an analysis of racially diverse middle and high school students found that grade point average was lower and instances of skipping school were higher for those who had unwanted sexual experiences, including intercourse—either due to force or acquiescence—compared to those who did not (Erickson & Rapkin, 1991). Poor academic achievement may, in turn, perpetuate disadvantaged socioeconomic status (SES) in later life, which is one of the most robust social predictors of poor well-being in old age (Braveman & Gottlieb, 2014; Cornman et al., 2014; Lantz et al., 2005; Link & Phelan, 1995; Mirowsky & Ross, 2003; Pampel et al., 2010). Therefore, we hypothesize that:
Hypothesis 2 The association between acquiesced first sex and late-life health and well-being is partially explained by socioeconomic status in adulthood.
Marital Roles and Transitions
Acquiesced first sexual experience may affect health and well-being via an interaction with marital transitions over the life course. There are several possible pathways through which acquiescence to unwanted first sex may be linked to individuals’ later relationship development and maintenance. For example, previous studies have found that those who experienced sexual debut at younger ages, often unwanted or acquiesced (Martinez et al., 2011), tended to get married at younger ages, on average, than those who first had sex at older ages—even after controlling for social class (Miller & Heaton, 1991), and early marriage is a predictor of later relationship instability after controlling for basic sociodemographic covariates such as education and race (Booth & Edwards, 1985; Martin & Bumpass, 1989). Moreover, prior research suggests that experiencing sexual coercion or acquiescence in adolescence is related to continued behavior of having unwanted sex in college (Baier et al., 1991) and to a higher chance of being in sexually aggressive relationships in the future (Walker, 1997), thus increasing the risk of experiencing relationship dissolutions. In addition, unwanted early sex is associated with lower rates of contraception use, continued unprotected sexual activity, and increased risks of pregnancy (Erickson & Rapkin, 1991), all of which increase the risk of relationship instability. Marital dissolution is one of the most traumatic life events adults can experience; the experience creates stress and strains (e.g., economic stress, loss of a confidant) that have a long-term negative impact on both physical and mental health in late life (Kiecolt-Glaser & Newton, 2001; Liu, 2012). Taken together, we hypothesize that:
Hypothesis 3 The association between acquiesced first sex and late-life health and well-being is partially explained by marital relationships and transitions.
Gender Differences
Research finds that in heterosexual experiences, it is often men who assume sexual acquiescence will occur (Moor et al., 2020), and women more often acquiesce to sex with men than men acquiesce to women (Fenner, 2017; Impett & Peplau, 2003; Vannier & O’Sullivan, 2010). A review of research indicates that girls have a higher risk of experiencing unwanted sexual activity and abuse in early life than boys (Putnam, 2003). Note, men may also feel pressured not to refuse sex, so they may acquiesce to sex due to cultural pressures to be sexually successful and demonstrate their masculinity to their partner and peers (Muehlenhard, 1988).
Few studies have examined gender differences in the health impacts of sexual acquiescence. The long-observed cultural norm of a sexual double standard that encourages men’s sexual activities but suppresses women’s (Milhausen & Herold, 1999) suggests that women may be more psychologically susceptible to exploitation in their first sexual experience than men (Laumann et al., 1994). Reviews of empirical research indicate that women suffer greater psychological consequences from negative sexual experiences (e.g., sexual abuse, which is most often studied) than do men (Rind & Tromovitch, 1997); and women also have higher physical risks associated with sex than men due to their risk of getting pregnant (Meier, 2007). On the other hand, while men are expected to initiate sex and women to be passive receivers (Fahs et al., 2020; Muehlenhard, 1988), Basson’s theory of women’s sexual response posits that a woman may lack the desire to have sex at the initiation of the sexual activity, but she can respond positively to the activity and continue in it because it became something she desired or enjoyed (Basson, 2000, 2003). Thus, while the sex may have started out as acquiesced with low wantedness, it may be something that she goes along with and ends up giving her pleasure. In this case, there may not be negative or harmful health consequences. Given the mixed evidence, we conduct an exploratory analysis rather than a hypothesis-driven analysis of gender differences in the relationship between acquiesced first sex and late-life health and well-being.
Method
Participants
We used data from the 2010/11 wave of the National Social Life, Health, and Aging Project (NSHAP). NSHAP is a nationally representative study of the intimate relationships, sexuality, and health of community-dwelling older Americans. While NSHAP is a longitudinal study of older adults who were first interviewed in 2005/06 (Wave 1), the survey only included questions about the acquiesced first sexual experience in the second wave of data collection, 2010/11. The second wave surveyed 3377 community-dwelling men and women ages 62–99 in the United States as well as their spouses (Waite et al., 2014). We excluded respondents who had missing data on acquiesced first sex (n = 148) and who reported their first sex was forced into (n = 89) because of our interest in sexual acquiescence. We further excluded missing data on other key variables (mostly income) (n = 582). Analysis using imputation of missing income data (e.g., at the median value, results reported in Appendix) revealed findings similar to those reported in the paper. The final analytic sample included 2558 respondents (1182 men and 1376 women).
Measures
Acquiescence During First Sexual Experience
NSHAP respondents were asked to retrospectively recall: “At this first occasion [of sex], is this something you wanted at the time, went along with, or were forced into?” Because only 89 respondents answered “were forced into,” we excluded them from the analysis because of our focus on sexual acquiescence, as well as concerns of low statistical power. Based on responses to this question, we coded acquiesced first sex into two categories: 1 = yes (i.e., “went along with”) and 0 = no (i.e., “wanted at the time”).
Late-Life Health Outcomes
We considered both physical and mental health in late life and included two health outcome measures: self-rated physical health and psychological distress. Self-rated physical health was based on the question “Would you say your health is excellent, very good, good, fair, or poor?” The responses were recoded into five numeric categories, with higher values indicating better health. Psychological distress was created using 11 questions from the Center for Epidemiological Studies Depression Scale (CES-D; Cronbach’s alpha = 0.79; Radloff, 1977). This measure combined a respondent’s reports of how often they had experienced the following in the previous week: (a) “I did not feel like eating,” (b) “I felt depressed,” (c) “I felt that everything I did was an effort,” (d) “My sleep was restless,” (e) “I was happy,” (f) “I felt lonely,” (g) “People were unfriendly,” (h) “I enjoyed life,” (i) “I felt sad,” (j) “I felt that people disliked me,” and (k) “I could not get ‘going.’” Responses ranged from 0 (rarely or none of the time) to 3 (most of the time). Each question was coded so that a higher value represented greater depression. The final CES-D scale was the sum of the scores for the 11 items.
Adulthood Socioeconomic Status (SES)
We measured adulthood SES using two variables: educational attainment and family income. Educational attainment was assessed by whether the respondent had ever attended college (1 = yes, 0 = no). Family income was derived from a question that asked respondents to assess their family income relative to the incomes of other American families. Responses were grouped into two categories: above average (coded as 1) and all others including average or below average (coded as 0).
Marital Factors
We included three key indicators of marital status and transitions across the life course history: (1) current marital status (0 = married, 1 = unmarried) at the time of the survey; (2) age at first marriage (in years); and (3) a total number of marriages (range: 0–7).
Covariates
We controlled for two types of covariates: sociodemographic factors and childhood adversity. First, we controlled for basic sociodemographic characteristics. Age was measured as a continuous variable in years. Gender was measured as 1 for females and 0 for males. Race-ethnicity included four categories: non-Hispanic White (reference), non-Hispanic Black, Hispanic, and other. Second, because previous studies suggest that childhood adversity is related to both first sexual experiences (Brown et al., 2015; Davis & Friel, 2001; Hillis et al., 2001; Mott et al., 1996) and later life health (Bowen & Gonzalez, 2010; Cohen et al., 2010; Guralnik et al., 2006; Haas, 2008; Montez & Hayward, 2014), we also controlled for several measures of childhood adversity including whether the respondent had the following experiences between ages 6 and 16: (1) lived with both parents (1 = no, 0 = yes); (2) family was well off (1 = no, including not very well off at all and not so well off, 0 = yes, including above average, fairly well off, and very well off); (3) experienced violence (1 =yes, 0 = no); (4) witnessed violence (1 = yes, 0 = no); and (5) poor health (1 = yes, including poor or fair health, 0 = no, including good, very good, or excellent health). The childhood adversity measures also included two variables assessing childhood SES: (6) mother graduated from high school (1 =yes, 0 = no); and (7) father graduated from high school (1 =yes, 0 = no).
Statistical Analyses
We conducted separate analyses for psychological distress and self-rated physical health. The analysis for each outcome was conducted in two steps. First, we assessed the basic association between acquiesced first sex and late-life health; we used negative binomial regression models to predict psychological distress and ordinal logistic regression models to predict self-rated physical health. We estimated both the main effects and gender interaction models. Second, we used a generalized structural equation modeling (GSEM) approach to examine the potential mediating roles of adulthood SES and marital transitions. The GSEM models estimated a series of regression equations simultaneously. The specific regression equations varied according to the level of measurement of the endogenous variables. For example, binary endogenous variables (e.g., attended college, above average income, currently married) were modeled using logistic regressions; count endogenous variables (e.g., total number of marriages) were modeled using Poisson regressions; and continuous variables (e.g., age at first marriage) were modeled using ordinary least squares regressions. A major advantage of GSEM is its ability to integrate the complex relationships between acquiesced first sex, adulthood SES, marital relationships, and late-life health into a single model and to estimate all these relationships simultaneously allowing for different distributional assumptions for endogenous variables. All models controlled for sociodemographic and childhood adversity covariates. All analyses were weighted and adjusted for clustering and stratification based on the complex sampling design using STATA 15 (StataCorp, 2017).
Results
Table 1 presents descriptive statistics for all analytic variables. In the focal sample, 26.15% of respondents reported their first sex was acquiesced; the average CES-D score was 4.65 (range: 0–27); and 21.44% of respondents reported having poor or fair health. With regard to marital history, 67.48% of the respondents were currently married, the average age at first marriage was about 22.31, and the average number of marriages was1.88. A majority of respondents, 61.76%, had attended college and 22.72% reported that their family income was above average. The sample was largely White (83.91%) and just over half of the respondents (54.06%) were women. With regard to the childhood adversity measures, 82.11% of respondents lived with both parents while growing up; 43.40% reported their family was not at all or not so well off during childhood; 9.29% reported witnessing violence during childhood; 8.21% reported experiencing a violent event during childhood, and 5.72% rated their childhood health as poor or fair compared to same-age peers. For the measures of childhood SES, 43.86% of respondents’ mothers graduated from high school and 43.01% of respondents’ fathers graduated from high school.
Table 1.
Weighted descriptive statistics of analytic variables (N = 2558)
| Mean (SD)/% | |
|---|---|
| CES-D | 4.65 (4.70) |
| Self-rated physical health | |
| Poor | 4.78 |
| Fair | 16.66 |
| Good | 33.72 |
| Very good | 32.31 |
| Excellent | 12.53 |
| Marital factors | |
| Current marital status | |
| Married (ref.) | 67.48 |
| Unmarried | 32.52 |
| Age at first marriage | 22.31(5.84) |
| Total number of marriages | 1.88(0.91) |
| SES | |
| Income | |
| Not above average/average (ref.) | 77.28 |
| Above average | 22.72 |
| Education attainment | |
| Did not attend college (ref.) | 38.24 |
| Attended college | 61.76 |
| Demographic Covariates | |
| Age | 71.19(7.87) |
| Gender | |
| Male (ref.) | 45.94 |
| Female | 54.06 |
| Race-ethnicity | |
| Non-Hispanic white (ref.) | 83.91 |
| Non-Hispanic black | 6.70 |
| Hispanic | 6.49 |
| Other | 2.90 |
| Acquiesced first sex | |
| 1 = Yes | 26.15 |
| 0 = No | 73.85 |
| Childhood adversity (ages 6–16) | |
| Lived with both parents | |
| Yes (ref.) | 82.11 |
| No | 13.50 |
| Missing | 4.39 |
| Family well off | |
| Yes (ref.) | 52.48 |
| No | 43.40 |
| Missing | 4.12 |
| Witnessed violent event | |
| Yes | 9.29 |
| No (ref.) | 89.72 |
| Missing | 0.99 |
| Experienced violent | |
| Yes | 8.21 |
| No (ref.) | 90.94 |
| Missing | 0.85 |
| Poor childhood health | |
| Yes | 5.72 |
| No (ref.) | 93.53 |
| Missing | 0.75 |
| Childhood SES | |
| Mother’s education | |
| Did not graduate high school (ref.) | 33.70 |
| Graduated high school | 43.86 |
| Missing | 22.44 |
| Father’s education | |
| Did not graduate high school (ref.) | 33.15 |
| Graduated high school | 43.01 |
| Missing | 23.84 |
Table 2 presents the results for acquiesced first sex in relation to CES-D (from negative binomial regression models) and self-rated physical health (from ordinal logistic models). The results of Model 1 show that when sociodemographic covariates and childhood adversity were controlled, those who experienced acquiesced first sex had significantly higher CES-D scores (IRR = 1.140, p < .01) and lower odds of reporting better health (i.e., a higher category of physical health) (OR = 0.771, p <.05) in late life than those who did not. In Model 2, we added a gender interaction term to further test whether the association between acquiesced first sex and late-life health differed for men and women; the results (Table 2) revealed no significant gender differences in the link between acquiesced first sex and late-life health outcomes.
Table 2.
Estimated effects of acquiesced first sex on CES-D and self-rated physical health (N = 2558)
| CES-D incidence rate ratios |
Self-rated physical health odds ratios |
|||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |
| Acquiesced first sex | 1.140** | 1.156 | 0.771* | 0.967 |
| Acquiesced first sex X female | 0.980 | 0.725 | ||
| Demographic covariates | ||||
| Age | 1.007* | 1.007* | 0.991 | 0.991 |
| Female | 1.088 + | 1.092 + | 1.233 + | 1.319 + |
| Race-ethnicity (0 = Non-Hispanic white) | ||||
| Non-Hispanic black | 0.967 | 0.968 | 0.653* | 0.651* |
| Hispanic | 1.017 | 1.018 | 0.560*** | 0.559*** |
| Other | 1.027 | 1.026 | 1.074 | 1.068 |
| Childhood SES | ||||
| Mother’s education (0 = Did not graduate high school) | ||||
| Graduated high school | 1.015 | 1.015 | 0.878 | 0.877 |
| Missing | 1.052 | 1.052 | 0.647** | 0.643** |
| Father’s education (0 = Did not graduate high school) | ||||
| Graduated high school | 1.115 + | 1.115 + | 0.801* | 0.799* |
| Missing | 1.269** | 1.268** | 0.717* | 0.716* |
| Childhood adversity (ages 6–16) | ||||
| Lived with both parents (0 = Yes) | ||||
| No | 1.003 | 1.004 | 0.922 | 0.925 |
| Missing | 1.048 | 1.047 | 1.226 | 1.208 |
| Family well off (0 = Yes) | ||||
| No | 1.053 | 1.052 | 0.828* | 0.828* |
| Missing | 0.743 | 0.743 | 1.607 | 1.614 |
| Poor/Fair health (0 = No) | ||||
| Yes | 1.312** | 1.312** | 0.661* | 0.661* |
| Missing | 0.867 | 0.869 | 0.392* | 0.396* |
| Witnessed violent event (0 = No) | ||||
| Yes | 1.072 | 1.072 | 0.889 | 0.885 |
| Missing | 1.890* | 1.888* | 0.314*** | 0.311*** |
| Experienced violent event (0 = No) | ||||
| Yes | 1.358** | 1.358** | 0.686* | 0.688* |
| Missing | 0.730 | 0.729 | 3.598** | 3.450** |
p < .001
p < .01
p < .05
p < .10
The results of the GSEM analyses shed light on the potential mediating roles of adulthood SES and marital factors. Figures 1 and 2 illustrate the key path diagrams from the GSEM models for psychological distress and self-rated physical health, respectively. The results in Fig. 1 suggest that acquiesced first sex was negatively associated with family income and education, and family income was in turn negatively related to CES-D in late life. Acquiesced first sex was not significantly associated with any of the marital characteristics, although being currently married was related to lower CES-D (i.e., better psychological well-being) and older age at first marriage was related to higher CES-D (i.e., worse psychological well-being). Notably, even when these indirect effects were controlled, the positive direct effect of acquiesced first sex on late-life CES-D remained significant. Figure 2 shows a very similar pattern for the relationship between acquiesced first sex and self-rated physical health in late life. Acquiesced first sex was negatively associated with family income and education, which were both, in turn, positively related to self-rated physical health in late life. None of the marital characteristics were significantly related to acquiesced first sex or self-rated physical health. The negative direct effect of acquiesced first sex on late-life self-rated physical health remained significant when all indirect effects were included in the model.
Fig. 1.
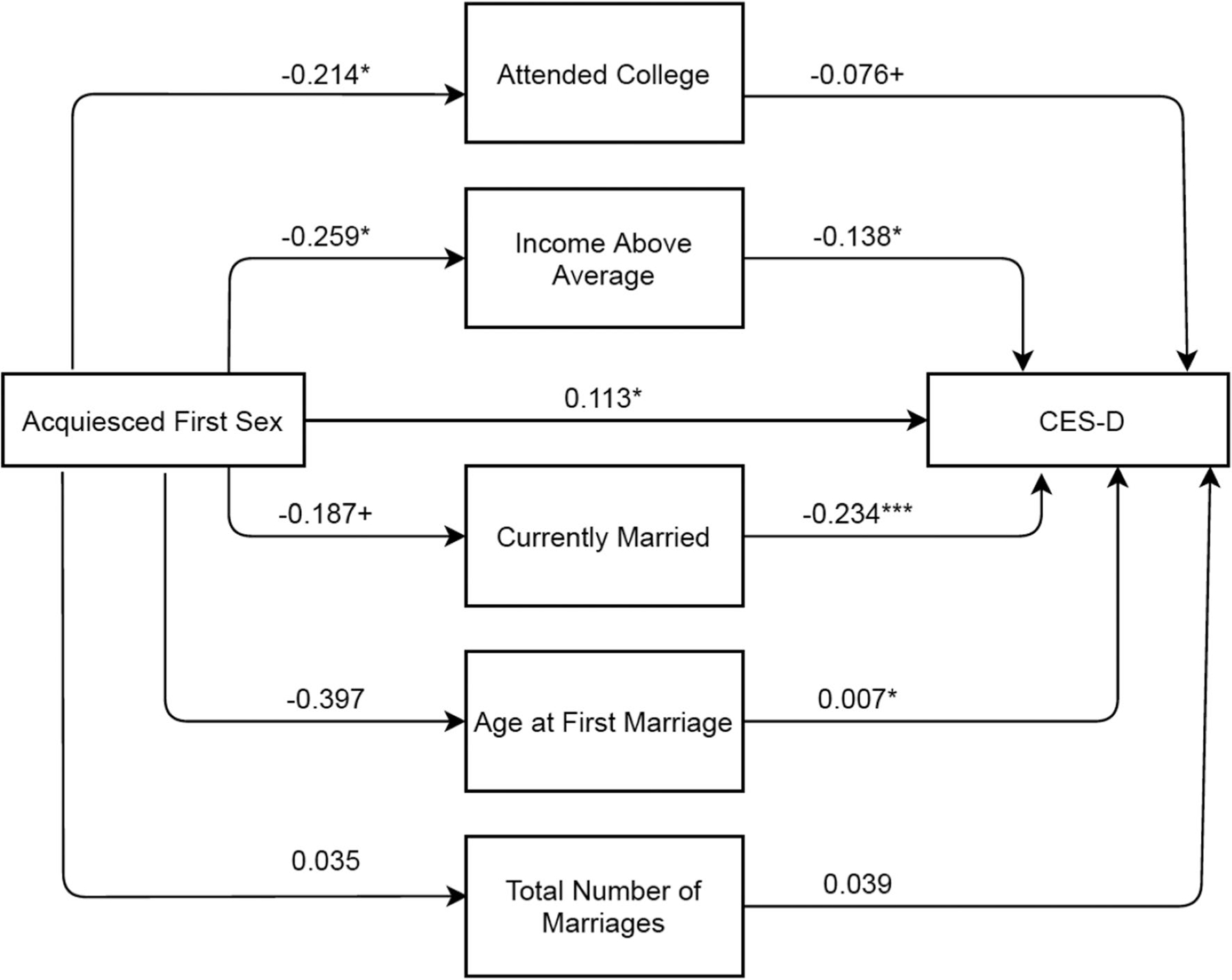
GSEM Path Diagram for Acquiesced First Sex Linked to CES-D in Late Life. N = 2558, ***p < .001, **p < .01, *p < .05, + p < .10. All equations controlled for sociodemographic and childhood adversity covariates. AIC = 44,984.14; BIC = 45,767.63 (for the purpose of comparison, a regular SEM model without allowing for different distributional assumptions of endogenous variables: AIC = 74,806.12; BIC = 75,613.00)
Fig. 2.
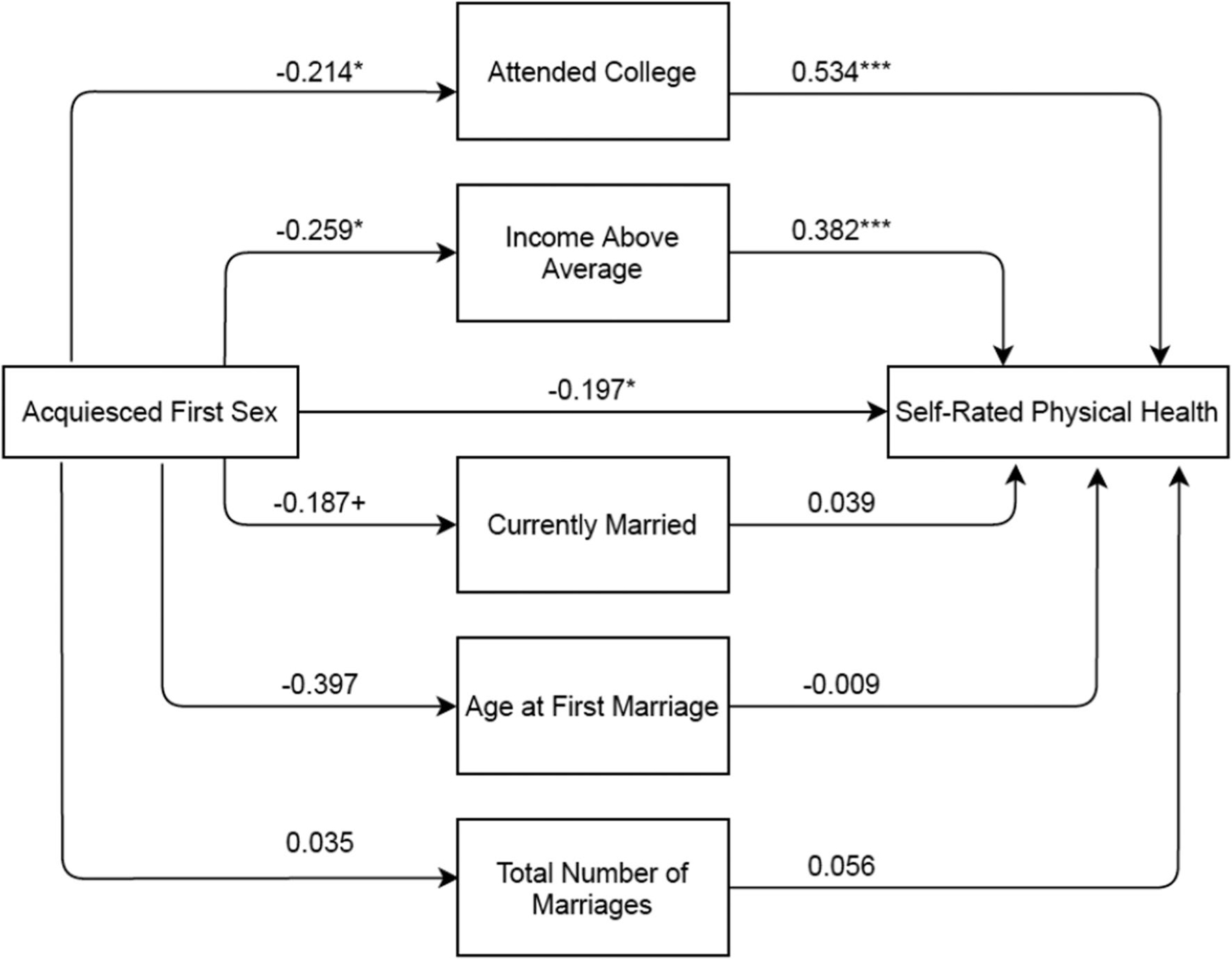
GSEM Path Diagram for Acquiesced First Sex Linked to Self-Rated Physical Health in Late Life. N = 2558, ***p < .001, **p < .01, *p < .05, + p < .10. All equations controlled for sociodemographic and childhood adversity covariates. AIC = 38,607.87; BIC = 39,403.06 (for the purpose of comparison, a regular SEM model without allowing for different distributional assumptions of endogenous variables: AIC = 66,947.91; BIC = 67,754.79)
Discussion
A significant share of Americans’ first sex experiences were not wanted (Martinez et al., 2011). This is important because a negative first sexual experience constitutes a life stressor that may have long-term impacts on physical and emotional well-being. Most prior studies on first sex have focused on understanding the predictors and consequences of the timing of sexual debut. In comparison, little research has examined the long-term health consequences of the context of first sexual experience, such as acquiesced first sex, or the life-course pathways that underlie the long-term health impacts. We analyzed data from the NSHAP 2010/11 to conduct the first population-based, nationally representative study of the long-term consequences of acquiesced first sexual experience for health and well-being in late life. The results reveal three major findings.
First, respondents whose first sex was acquiesced tended to report higher levels of psychological distress and poorer physical health in their late life than others whose first sex was wanted. This finding is consistent with our hypothesis (Hypothesis 1) as well as previous studies suggesting that acquiescence to unwanted sex (either first or later sex) may have detrimental consequences for individuals’ lives and well-being, with most studies focusing on impacts during adolescence and young adulthood (Blythe et al., 2006; Flack et al., 2007). The current study is the first to extend the research to late-life health outcomes, providing evidence of the potential long-arm of acquiescence during the first sexual experience. The findings also add to the broader evidence of the cumulative effects of early life adversity on health development in late life (Haas, 2008; Hatch, 2005; Hayward & Gorman, 2004; Mayer, 2009; Miller et al., 2011; Shonkoff et al., 2009; Umberson et al., 2014; Warner & Hayward, 2006). Like other well-documented early life disadvantages such as childhood poverty and parental divorce, acquiesced first sex may modify the subsequent context of an individual’s life course and launch distinct developmental pathways that persist through later stages of the life course and take a toll on health in late life.
Second, the analyses move beyond the previous literature by testing two specific life-course pathways—adulthood SES and marital relationships—through which acquiesced first sexual experience is linked to an individual’s health and well-being over the life course. Results of GSEM analyses suggest that the association between acquiesced first sexual experience and late-life health occurs partially through adulthood SES (consistent with Hypothesis 2) but not through marital relationships (inconsistent with Hypothesis 3). The results highlight that SES, one of the most robust social predictors of late-life health, is an important pathway through which acquiesced first sexual experience is linked to health in late life. Previous studies have shown that for adolescents, both early sexual activity (Frisco, 2008; Spriggs & Halpern, 2008; Steward et al., 2009) and unwanted sexual experiences (Erickson & Rapkin, 1991) are negatively related to academic success. The stress from experiencing acquiesced first sex may lead to depression, which may impair individuals’ ability to attain higher educational credentials (Melkevik et al., 2016). Moreover, acquiesced sexual debut may interrupt educational attainment through teenage parenthood (Hofferth et al., 2001; Hoffman et al., 1993)—early sexual debut, especially unwanted, may not include the use of contraception and could result in teenage pregnancy, which can have a negative effect on academic attainment (Frisco, 2008; Magnusson & Trost, 2006; Steward et al., 2009).
Finally, we found no evidence of gender differences in these processes. Given the substantial literature on gender differences in sexuality and health, we had expected that the relationship between acquiesced first sex and late-life health would differ for men and women. The results, however, suggested that for both men and women, acquiesced first sexual experience was associated with poorer mental and physical health in late life. In general, women are more likely than men to report that their first experience with sex was acquiesced. In our sample, 37% of women reported their first sex was acquiesced while only 14% of men did so (results not shown in tables). Despite this difference in prevalence, a negative experience of first sex may create similar levels of stress for men and women, which may disrupt their later life well-being to the same extent. Many previous studies on sexual acquiescence focus on women (e.g. Houts, 2005; Walker, 1997), perhaps because they experience a higher prevalence of sexual acquiescence than men (Fenner, 2017; Impett & Peplau, 2003; Vannier & O’Sullivan, 2010). The current results emphasize that it is also important to consider men’s sexual acquiescence because they experience similarly significant consequences. Future studies should continue to investigate potential gender-specific pathways (e.g., unplanned parenthood) through which acquiesced first sex shapes the health of men and women over the life course, even though the overall association is similar for men and women. Nevertheless, we acknowledge that the lack of findings on significant gender differences is also likely due to the relatively small number of men reporting acquiesced first sex in our sample (n = 177).
This study had several limitations. First, although we built our research hypotheses based on a causal theoretical frame-work, we could not rule out the possibility of some reversal relationships in our studied variables (e.g., education affects first sexual experience). Second, we were unable to determine some important contextual factors for the first sex such as the age of the sex partner because the NSHAP did not ask the necessary questions. We also did not have data beyond the first sexual experience, so it is unclear if a first unwanted experience was an isolated event or if there were repeated incidences of unwanted sexual contact. This limited information precludes us from knowing if this single experience is influential over the life course to the point of impacting mental health and distress in later life, or if it is instead related to other markers of disadvantage, such as patterns of sexual acquiescence, interpersonal communication problems, or insecure or anxious attachment styles. These broader patterns may be more indicative of life-course pathways, and these potential results could be targeted by interventions to improve health in later life. Future studies should analyze datasets that include relevant measures to better understand the context of first sex as well as the potentially distinct consequences and pathways for health and well-being in later life. Third, we relied on retrospective data about early sexual experiences and childhood adversity, which are susceptible to reporting errors. Additional work in this area would benefit from a longitudinal design that includes data collected at multiple points following the experience of first sex. Fourth, we examined only two potential pathways, adulthood SES and marital factors, through which acquiesced first sex might produce long-term effects on health in late life. Future studies should investigate other potential pathways (e.g., stress proliferation) to further elucidate these complex processes. Finally, our measures of late-life health were limited to two widely used measures of physical and mental health. Future research should test additional health measures to confirm the robustness of the findings.
Conclusion
Despite the burgeoning research on first sexual experience, neither the long-term health consequences of acquiescence during first sexual experience nor the life-course pathways that lead to these consequences are well understood. We provide the first population-based, nationally representative evidence on the long-term consequences of acquiesced first sexual experience for self-rated physical health and psycho-logical well-being in late life. We found that respondents who acquiesced to their first sex were more likely to report worse physical health and suffer higher levels of psychological distress at older ages than others whose first sex was wanted. These results call attention to the importance of including early sexual history in the discussion of older adults’ health management. Further, our findings on the significant mediating role of adulthood SES highlight the importance of designing and initiating intervention programs that help adolescents and adults in low-SES communities recover from the consequences of acquiesced early sexual experiences. As the older population continues to grow and public health efforts focus on healthy aging, these results indicate the need for healthcare providers and policy makers to consider early life factors such as early life sexuality, in addition to the present context, as they seek to promote the health and well-being of adults in late life.
Acknowledgments
This research was supported by the National Institute on Aging (R01 AG061118).
Appendix: Results with Missing Income Imputed
Fig. 3.
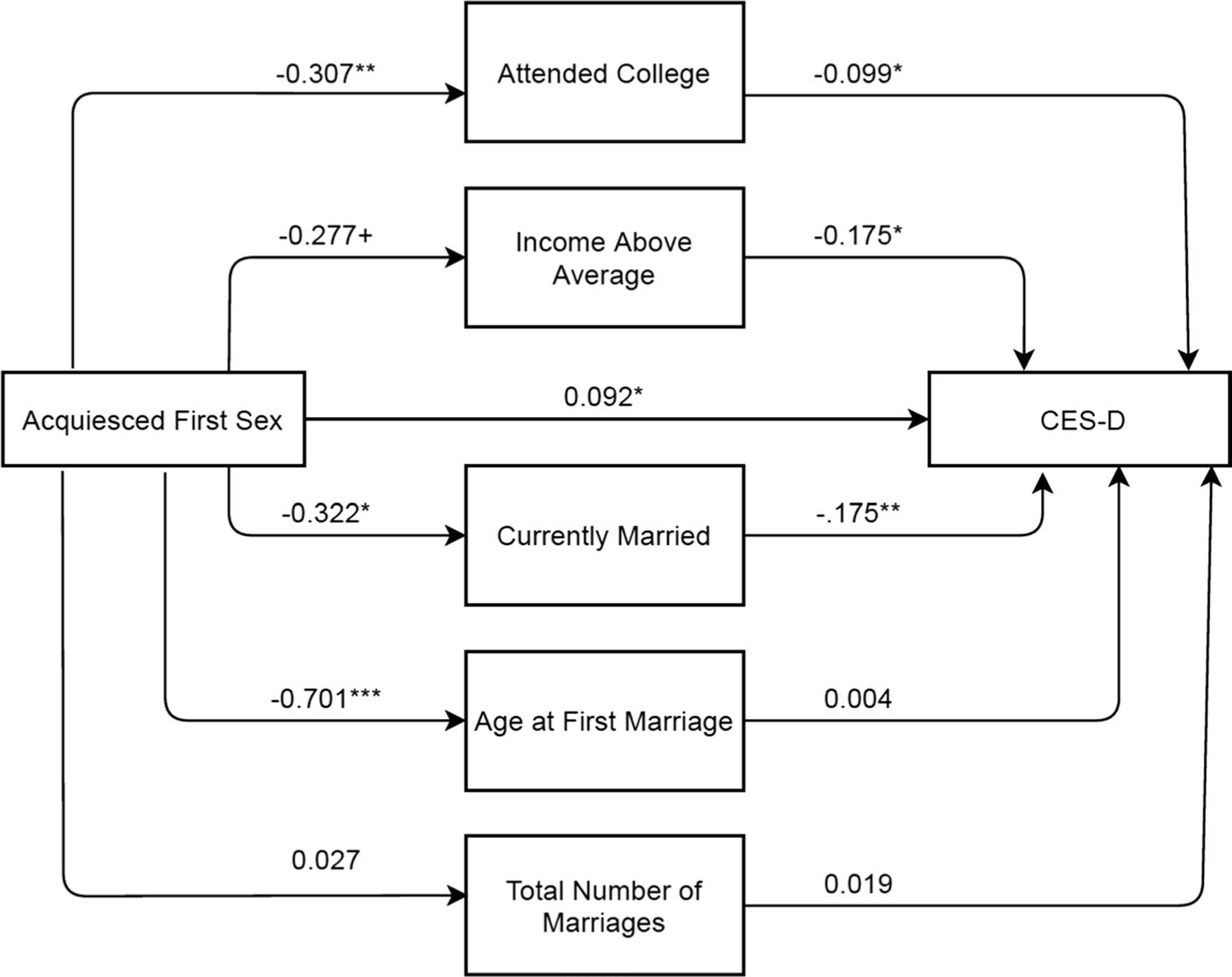
GSEM Path Diagram for Acquiesced First Sex Linked to CES-D in Late Life with Missing Income Imputed. N = 3108, ***p < .001, **p < .01, *p < .05, + p < .10. All equations controlled for sociodemographic and childhood adversity covariates. AIC = 54,701.54; BIC = 55,511.13
Fig. 4.
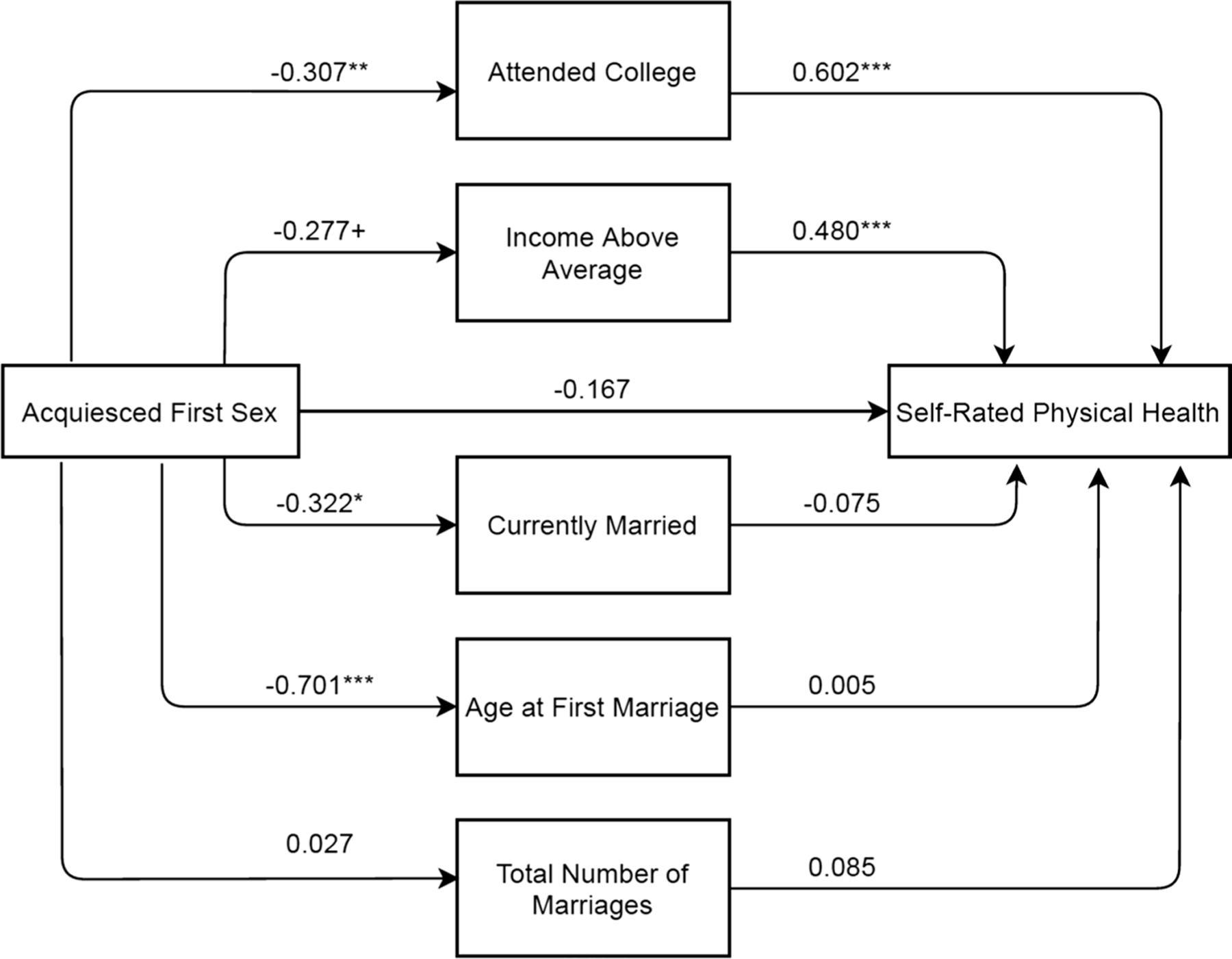
GSEM Path Diagram for Acquiesced First Sex Linked to Self-Rated Physical Health in Late Life with Missing Income Imputed. N = 3,108, ***p < .001, **p < .01, *p < .05, + p < .10. All equations controlled for sociodemographic and childhood adversity covariates. AIC = 46,829.95; BIC = 47,651.62
Table 3.
Estimated effects of acquiesced first sex on CES-D and self-rated physical health with Missing Income Imputed (N = 3108)
| CES-D incidence rate ratios |
Self-rated physical health odds ratios |
|||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |
| Acquiesced first sex | 1.126* | 1.142 | 0.805* | 0.910 |
| Acquiesced first sex X Female | 0.980 | 0.841 | ||
| Demographic covariates | ||||
| Age | 1.007* | 1.007* | 0.985** | 0.986** |
| Female | 1.123* | 1.128* | 1.134 | 1.176 |
| Race-ethnicity (0 = Non-Hispanic white) | ||||
| Non-Hispanic black | 1.014 | 1.014 | 0.650** | 0.650** |
| Hispanic | 0.956 | 0.956 | 0.580*** | 0.579*** |
| Other | 1.000 | 0.999 | 1.113 | 1.108 |
| Childhood SES | ||||
| Mother’s education (0 = Did not graduate high school) | ||||
| Graduated high school | 1.023 | 1.023 | 0.882 | 0.881 |
| Missing | 1.066 | 1.066 | 0.674** | 0.672** |
| Father’s education (0 = Did not graduate high school) | ||||
| Graduated high school | 1.109 + | 1.109 + | 0.823* | 0.822* |
| Missing | 1.260** | 1.260** | 0.731* | 0.732* |
| Childhood adversity (ages 6–16) | ||||
| Lived with both parents (0 = Yes) | ||||
| No | 1.018 | 1.018 | 0.902 | 0.903 |
| Missing | 1.146 | 1.144 | 0.965 | 0.954 |
| Family well off (0 = Yes) | ||||
| No | 1.055 | 1.055 | 0.847 + | 0.846 + |
| Missing | 0.703 | 0.703 | 2.001 | 2.018 |
| Poor/Fair Health (0 = No) | ||||
| Yes | 1.331*** | 1.331*** | 0.671** | 0.670** |
| Missing | 1.069 | 1.073 | 0.364 + | 0.371 + |
| Witnessed violent event (0 = No) | ||||
| Yes | 1.091 | 1.091 | 0.857 | 0.854 |
| Missing | 1.848** | 1.848** | 0.401* | 0.401** |
| Experienced violent event (0 = No) | ||||
| Yes | 1.349** | 1.350** | 0.698* | 0.700* |
| Missing | 0.734 | 0.733 | 3.272 + | 3.223 + |
p < .001
p < .01
p < .05
p < .10
Footnotes
Declarations
Ethical approval This article does not contain any studies with human participants performed by any of the authors.
Conflict of interest No competing financial interests exist.
References
- Abma J, Driscoll A, & Moore K (1998). Young women’s degree of control over first intercourse: An exploratory analysis. Family Planning Perspectives, 30(1), 12–18. 10.2307/2991518 [DOI] [PubMed] [Google Scholar]
- Abma JC, Martinez GM, & Copen CE (2010). Teenagers in the United States: Sexual activity, contraceptive use, and childbearing, National survey of family growth 2006–2008. Vital and Health Statistics, 23(30), 1–57. [PubMed] [Google Scholar]
- Baier JL, Rosenzweig MG, & Whipple EG (1991). Patterns of sexual behavior, coercion and victimization of university students. Journal of College Student Development, 32(4), 310–322. [Google Scholar]
- Basile KC (1999). Rape by acquiescence: The ways in which women “give in” to unwanted sex with their husbands. Violence Against Women, 5(9), 1036–1085. [Google Scholar]
- Basson R (2000). The female sexual response: A different model. Journal of Sex & Marital Therapy, 26(1), 51–65. 10.1080/009262300278641 [DOI] [PubMed] [Google Scholar]
- Basson R (2003). Biopsychosocial models of women’s sexual response: Applications to management of ‘desire disorders.’ Sexual and Relationship Therapy, 18(1), 107–115. [Google Scholar]
- Beres M (2010). Sexual miscommunication? Untangling assumptions about sexual communication between casual sex partners. Culture, Health & Sexuality, 12(1), 1–14. 10.1080/13691050903075226 [DOI] [PubMed] [Google Scholar]
- Blythe MJ, Fortenberry JD, Temkit MH, Tu W, & Orr DP (2006). Incidence and correlates of unwanted sex in relationships of middle and late adolescent women. Archives of Pediatrics & Adolescent Medicine, 160(6), 591–595. 10.1001/archpedi.160.6.591 [DOI] [PubMed] [Google Scholar]
- Booth A, & Edwards JN (1985). Age at marriage and marital instability. Journal of Marriage and the Family, 47(1), 67–75. 10.2307/352069 [DOI] [Google Scholar]
- Bowen ME, & Gonzalez HM (2010). Childhood socioeconomic position and disability in later life: Results of the Health and Retirement Study. American Journal of Public Health, 100(Suppl. 1), S197–S203. 10.2105/AJPH.2009.160986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braveman P, & Gottlieb L (2014). The social determinants of health: It’s time to consider the causes of the causes. Public Health Reports, 129, 19–31. 10.1177/00333549141291S206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown MJ, Masho SW, Perera RA, Mezuk B, & Cohen SA (2015). Sex and sexual orientation disparities in adverse childhood experiences and early age at sexual debut in the United States: Results from a nationally representative sample. Child Abuse & Neglect, 46, 89–102. 10.1016/j.chiabu.2015.02.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S, Janicki-Deverts D, Chen E, & Matthews KA (2010). Childhood socioeconomic status and adult health. Annals of the New York Academy of Sciences, 1186, 37–55. 10.1111/j.1749-6632.2009.05334.x [DOI] [PubMed] [Google Scholar]
- Conroy NE, Krishnakumer A, & Leone JM (2015). Reexamining issues of conceptualization and willing consent: The hidden role of coercion in experiences of sexual acquiescence. Journal of Interpersonal Violence, 30(11), 1828–1846. 10.1177/0886260514549050 [DOI] [PubMed] [Google Scholar]
- Cornman JC, Glei DA, Goldman N, Chang MC, Lin HS, Chuang YL, Hurng BS, Lin YH, Lin SH, Liu IW, Liu HY, & Weinstein M (2014). Cohort profile: The Social Environment Biomarkers Aging Study (SEBAS) in Taiwan. International Journal of Epidemiology, 45(1), 54–63. 10.1093/ije/dyu179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crown L, & Roberts LJ (2007). Against their will: Young women’s nonagentic sexual experiences. Journal of Social and Personal Relationships, 24(3), 385–405. 10.1177/0265407507077228 [DOI] [Google Scholar]
- Davis EC, & Friel LV (2001). Adolescent sexuality: Disentangling the effects of family structure and family context. Journal of Marriage and Family, 63(3), 669–681. 10.1111/j.1741-3737.2001.00669.x [DOI] [Google Scholar]
- Erickson PI, & Rapkin AJ (1991). Unwanted sexual experiences among middle and high school youth. Journal of Adolescent Health, 12(4), 319–325. 10.1016/0197-0070(91)90007-9 [DOI] [PubMed] [Google Scholar]
- Fahs B, Swank E, & Shambe A (2020). “I just go with it”: Negotiating sexual desire discrepancies for women in partnered relationships. Sex Roles, 83, 226–239. 10.1007/s11199-019-01098-w [DOI] [Google Scholar]
- Fairfortune TS, Stern JE, Richardson BA, Koutsky LA, & Winer RL (2020). Sexual behavior patterns and condom use in newly sexually active female university students. Archives of Sexual Behavior, 49, 1053–1065. 10.1007/s10508-019-1411-z [DOI] [PubMed] [Google Scholar]
- Fenner L (2017). Sexual consent as a scientific subject: A literature review. American Journal of Sexuality Education, 12(4), 451–471. 10.1080/15546128.2017.1393646 [DOI] [Google Scholar]
- Finer LB, & Philbin JM (2014). Trends in ages at key reproductive transitions in the United States, 1951–2010. Women’s Health Issues, 24(3), e271–e279. 10.1016/j.whi.2014.02.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, & Yllö K (1987). License to rape: Sexual abuse of wives The Free Press. [Google Scholar]
- Flack WF Jr., Daubman KA, Caron ML, Asadorian JA, D’Aureli NR, Gigliotti SN, Hall AT, Kiser S, & Stine ER (2007). Risk factors and consequences of unwanted sex among university students: Hooking up, alcohol, and stress response. Journal of Interpersonal Violence, 22(2), 139–157. 10.1177/0886260506295354 [DOI] [PubMed] [Google Scholar]
- Fors S, Lennartsson C, & Lundberg O (2009). Childhood living conditions, socioeconomic position in adulthood, and cognition in later life: Exploring the associations. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 64(6), 750–757. 10.1093/geronb/gbp029 [DOI] [PubMed] [Google Scholar]
- Frisco ML (2008). Adolescents’ sexual behavior and academic attainment. Sociology of Education, 81(3), 284–311. 10.1177/003804070808100304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guralnik JM, Butterworth S, Wadsworth MEJ, & Kuh D (2006). Childhood socioeconomic status predicts physical functioning a half century later. Journals of Gerontology: Medical Sciences, 61, 694–701. 10.1093/gerona/61.7.694 [DOI] [PubMed] [Google Scholar]
- Haas S (2008). Trajectories of functional health: The ‘long arm’ of childhood health and socioeconomic factors. Social Science & Medicine, 66(4), 849–861. 10.1016/j.socscimed.2007.11.004 [DOI] [PubMed] [Google Scholar]
- Hartmann AJ, & Crockett EE (2016). When sex isn’t the answer: Examining sexual compliance, restraint, and physiological stress. Sexual and Relationship Therapy, 31(3), 312–324. 10.1080/14681994.2016.1154142 [DOI] [Google Scholar]
- Hatch SL (2005). Conceptualizing and identifying cumulative adversity and protective resources: Implications for understanding health inequalities. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 50, 130–134. 10.1093/geronb/60.Special_Issue_2.S130 [DOI] [PubMed] [Google Scholar]
- Hayward MD, & Gorman BK (2004). The long arm of childhood: The influence of early-life social conditions on men’s mortality. Demography, 41(1), 87–107. 10.1353/dem.2004.0005 [DOI] [PubMed] [Google Scholar]
- Heywood W, Patrick K, Smith AM, & Pitts MK (2015). Associations between early first sexual intercourse and later sexual and reproductive outcomes: A systematic review of population-based data. Archives of Sexual Behavior, 44(3), 531–569. 10.1007/s10508-014-0374-3 [DOI] [PubMed] [Google Scholar]
- Hillis SD, Anda RF, Felitti VJ, & Marchbanks PA (2001). Adverse childhood experiences and sexual risk behaviors in women: A retrospective cohort study. Family Planning Perspectives, 33(5), 206–211. 10.2307/2673783 [DOI] [PubMed] [Google Scholar]
- Hofferth SL, Reid L, & Mott FL (2001). The effects of early child-bearing on schooling over time. Family Planning Perspectives, 32, 259–267. 10.2307/3030193 [DOI] [PubMed] [Google Scholar]
- Hoffman SD, Foster EM, & Furstenberg FF Jr. (1993). Reevaluating the costs of teenage childbearing. Demography, 30(2), 291–296. 10.2307/2061843 [DOI] [PubMed] [Google Scholar]
- Houts LA (2005). But was it wanted? Young women’s first voluntary sexual intercourse. Journal of Family Issues, 26(8), 1082–1102. 10.1177/0192513X04273582 [DOI] [Google Scholar]
- Impett EA, & Peplau LA (2003). Sexual compliance: Gender, motivational, and relationship perspectives. Journal of Sex Research, 40(1), 87–100. 10.1080/00224490309552169 [DOI] [PubMed] [Google Scholar]
- Kalil A, Duncan GJ, & Ziol-Guest KM (2016). Early childhood poverty: Short and long-run consequences over the lifespan. In Shanahan MJ, Mortimer JT, & Kirkpatrick Johnson M (Eds.), Handbook of the life course (pp. 341–354). Springer. [Google Scholar]
- Katz J, & Schneider ME (2015). (Hetero)sexual compliance with unwanted casual sex: Associations with feelings about first sex and sexual self-perceptions. Sex Roles, 72, 451–461. 10.1007/s11199-015-0467-z [DOI] [Google Scholar]
- Katz J, & Tirone V (2010). Going along with it: Sexually coercive partner behavior predicts dating women’s compliance with unwanted sex. Violence Against Women, 16(7), 730–742. 10.1177/1077801210374867 [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, & Newton TL (2001). Marriage and health: His and hers. Psychological Bulletin, 127(4), 472–503. [DOI] [PubMed] [Google Scholar]
- Lammers C, Ireland M, Resnick M, & Blum R (2000). Influences on adolescents’ decision to postpone onset of sexual intercourse: A survival analysis of virginity among youths aged 13 to 18 years. Journal of Adolescent Health, 26(1), 42–48. 10.1016/s1054-139x(99)00041-5 [DOI] [PubMed] [Google Scholar]
- Lantz PM, House JS, Mero RP, & Williams DR (2005). Stress, life events, and socioeconomic disparities in health: Results from the Americans’ Changing Lives Study. Journal of Health and Social Behavior, 46(3), 274–288. 10.1177/002214650504600305 [DOI] [PubMed] [Google Scholar]
- Laumann EO, Gagnon JH, Michael RT, & Michaels S (1994). The social organization of sexuality: Sexual practices in the United States The University of Chicago Press. [Google Scholar]
- Link BG, & Phelan J (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 80–94. https://www.jstor.org/stable/2626958 [PubMed]
- Liu H (2012). Marital dissolution and self-rated health: Age trajectories and birth cohort variations. Social Science & Medicine, 74(7), 1107–1116. 10.1016/j.socscimed.2011.11.037 [DOI] [PubMed] [Google Scholar]
- Magnusson C, & Trost K (2006). Girls experiencing sexual inter-course early: Could it play a part in reproductive health in middle adulthood? Journal of Psychosomatic Obstetrics & Gynecology, 27(4), 237–244. 10.1080/01674820600869006 [DOI] [PubMed] [Google Scholar]
- Martin TC, & Bumpass LL (1989). Recent trends in marital disruption. Demography, 26(1), 37–51. 10.2307/2061492 [DOI] [PubMed] [Google Scholar]
- Martinez G, Copen CE, & Abma JC (2011). Teenagers in the United States; sexual activity, contraceptive use, and childbearing, 2006–2010 National Survey of Family Growth. Vital and Health Statistics, 23(31), 1–44. [PubMed] [Google Scholar]
- Mayer KU (2009). New directions in life course research. Annual Review of Sociology, 35, 413–433. 10.1146/annurev.soc.34.040507.134619 [DOI] [Google Scholar]
- Meier AM (2007). Adolescent first sex and subsequent mental health. American Journal of Sociology, 112(6), 1811–1847. 10.1086/512708 [DOI] [Google Scholar]
- Melkevik O, Hauge LJ, Bendtsen P, Reneflot A, Mykletun A, & Aarø LE (2016). Associations between delayed completion of high school and educational attainment and symptom levels of anxiety and depression in adulthood. BMC Psychiatry, 16(1), 64. 10.1186/s12888-016-0765-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milhausen RR, & Herold ES (1999). Does the sexual double standard still exist? Perceptions of university women. Journal of Sex Research, 36(4), 361–368. 10.1080/00224499909552008 [DOI] [Google Scholar]
- Miller BC, & Heaton TB (1991). Age at first sexual intercourse and the timing of marriage and childbirth. Journal of Marriage and the Family, 53(3), 719–732. 10.2307/352746 [DOI] [Google Scholar]
- Miller GE, Chen E, & Parker KJ (2011). Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychological Bulletin, 137(6), 959–997. 10.1037/a0024768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirowsky J, & Ross CE (2003). Social causes of psychological distress Hawthorne. [Google Scholar]
- Montez JK, & Hayward MD (2014). Cumulative childhood adversity, educational attainment, and active life expectancy among US adults. Demography, 51(2), 413–435. 10.1007/s13524-013-0261-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moor A, Haimov Y, & Shreiber S (2020). When desire fades: Women talk about their subjective experience of declining sexual desire in loving long-term relationships. Journal of Sex Research, 58(2), 160–169. 10.1080/00224499.2020.1743225 [DOI] [PubMed] [Google Scholar]
- Mott FL, Fondell MM, Hu PN, Kowaleski-Jones L, & Menaghan EG (1996). The determinants of first sex by age 14 in a high-risk adolescent population. Family Planning Perspectives, 28, 13–18. 10.2307/2135957 [DOI] [PubMed] [Google Scholar]
- Muehlenhard CL (1988). “Nice women” don’t say yes and “real men” don’t say no: How Miscommunication and the double standard can cause sexual problems. Women & Therapy, 7(2–3), 95–108. 10.1300/J015v07n02_08 [DOI] [Google Scholar]
- O’Rand AM, & Hamil-Luker J (2005). Processes of cumulative adversity: Childhood disadvantage and increased risk of heart attack across the life course. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 60, 117–134. 10.1093/geronb/60.Special_Issue_2.S117 [DOI] [PubMed] [Google Scholar]
- O’Sullivan LF, & Allgeier ER (1998). Feigning sexual desire: Consenting to unwanted sexual activity in heterosexual dating relationships. Journal of Sex Research, 35(3), 234–243. 10.1080/00224499809551938 [DOI] [Google Scholar]
- Ott MA, Ghani N, McKenzie F, Rosenberger JG, & Bell DL (2012). Adolescent boys’ experiences of first sex. Culture, Health and Sexuality, 14(7), 781–793. 10.1080/13691058.2012.694477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pakpahan E, Hoffmann R, & Kröger H (2017). The long arm of childhood circumstances on health in old age: Evidence from SHARELIFE. Advances in Life Course Research, 31, 1–10. 10.1016/j.alcr.2016.10.003 [DOI] [Google Scholar]
- Pampel FC, Krueger PM, & Denney JT (2010). Socioeconomic disparities in health behaviors. Annual Review of Sociology, 36, 349–370. 10.1146/annurev.soc.012809.102529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson ZD, & Muehlenhard CL (2007). Conceptualizing the “wantedness” of women’s consensual and nonconsensual sexual experiences: Implications for how women label their experiences with rape. Journal of Sex Research, 44(1), 72–88. 10.1080/00224490709336794 [DOI] [PubMed] [Google Scholar]
- Putnam FW (2003). Ten-year research update review: Child sexual abuse. Journal of the American Academy of Child & Adolescent Psychiatry, 42(3), 269–278. 10.1097/00004583-200303000-00006 [DOI] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1(3), 385–401. 10.1177/014662167700100306 [DOI] [Google Scholar]
- Rind B, & Tromovitch P (1997). A meta-analytic review of findings from national samples on psychological correlates of child sexual abuse. Journal of Sex Research, 34(3), 237–255. 10.1080/00224499709551891 [DOI] [Google Scholar]
- Shonkoff JP, Boyce WT, & McEwen BS (2009). Neuroscience, molecular biology, and the childhood roots of health disparities: Building a new framework for health promotion and disease prevention. Journal of the American Medical Association, 301(21), 2252–2259. 10.1001/jama.2009.754 [DOI] [PubMed] [Google Scholar]
- Spriggs AL, & Halpern CT (2008). Timing of sexual debut and initiation of postsecondary education by early adulthood. Perspectives on Sexual and Reproductive Health, 40(3), 152–161. 10.1363/4015208 [DOI] [PubMed] [Google Scholar]
- StataCorp. (2017). Stata statistical software: Release 15 StataCorp LLC. [Google Scholar]
- Steward NR, Farkas G, & Bingenheimer JB (2009). Detailed educational pathways among females after very early sexual inter-course. Perspectives on Sexual and Reproductive Health, 41(4), 244–252. 10.1363/4124409 [DOI] [PubMed] [Google Scholar]
- Umberson D, Williams K, Thomas PA, Liu H, & Thomeer MB (2014). Race, gender, and chains of disadvantage: Childhood adversity, social relationships, and health. Journal of Health and Social Behavior, 55(1), 20–38. 10.1177/0022146514521426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vannier SA, & O’Sullivan LF (2010). Sex without desire: Characteristics of occasions of sexual compliance in young adults’ committed relationships. Journal of Sex Research, 47(5), 429–439. 10.1080/00224490903132051 [DOI] [PubMed] [Google Scholar]
- Waite LJ, Cagney K, Cornwell B, Dale W, Huang E, Laumann EO, … Schumm LP (2014). National Social Life, Health, and Aging Project (NSHAP): Wave 2 and partner data collection Ann Arbor, MI: Inter-university Consortium for Political and Social Research; [distributor]. ICPSR34921-v1. 10.3886/ICPSR34921.v1. [Google Scholar]
- Walker SJ (1997). When “no” becomes “yes”: Why girls and women consent to unwanted sex. Applied and Preventive Psychology, 6(3), 157–166. 10.1016/S0962-1849(97)80003-0 [DOI] [Google Scholar]
- Warner DF, & Hayward MD (2006). Early-life origins of the race gap in men’s mortality. Journal of Health and Social Behavior, 47(3), 209–226. 10.1177/002214650604700302 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weitzman A, & Mallory AB (2019). Racial, socioeconomic, and attitudinal disparities in trajectories of young women’s willingness to refuse unwanted sex. Journal of Adolescent Health, 64(6), 746–752. 10.1016/j.jadohealth.2018.12.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, & Helfand M (2008). Ten years of longitudinal research on U.S. adolescent sexual behavior: Developmental correlates of sexual intercourse, and the importance of age, gender and ethnic background. Developmental Review, 28(2), 153–224. 10.1016/j.dr.2007.06.001 [DOI] [Google Scholar]