

Abstract
Introduction
Recreational scuba diving has existed for over 70 years with organisations emerging that teach individuals with disabilities to dive. It is unclear what the physical and psychosocial effects of scuba interventions might be. This systematic review explores evidence for the effects of scuba diving in individuals with neurological disability, intellectual disability and autism.
Methods
The databases Medline, EMBASE, Ovid Emcare, and SportDiscus were searched. Included papers described a scuba-based intervention for clients with a neurological disability, intellectual disability and autism, with physical or psychosocial outcomes explored in the paper. Quality of the included papers was assessed using the McMaster Appraisal Tools, with descriptive data synthesis completed to explore the physical and psychosocial effects of the interventions.
Results
Four papers met the inclusion criteria: a cross-sectional investigation, a phenomenological study, a case-control study and a multiple case study. The quality of the papers was low to moderate. Papers addressed the psychosocial effects of scuba diving, including motivation to participate, participant experiences, the effect on cognition and physical self-concept. One study reported an increase in self-concept for the majority of participants. An increase in understanding instructions and in visual attention was reported in another. Enjoyment of the activity was reported and motivators to be involved in scuba diving for people with disabilities included fun and excitement. No papers addressed functional outcomes.
Conclusions
Whilst scuba diving interventions appear to enhance physical self-concept and are enjoyable, conclusive evidence regarding effectiveness could not be determined. Research in this area is extremely limited.
Keywords: Adapted physical activity, Disabled diver, Evidence, Physiology, Psychology, Review article
Introduction
The World Health Organisation (WHO) estimates that over 15% of the world's population is living with a disability.[ 1] Therefore, it might be assumed that some scuba divers live with a disability. There are several organisations providing training and scuba experiences for people living with a disability, such as the International Association for Handicapped Divers(https://www.iahd.org/), the Handicapped Scuba Association (https://www.hsascuba.com/) and Disabled Divers International (https://www.ddivers.org/). Additionally, there are services offering pool-based scuba diving experiences in several countries.[ 2 , 3]
A recent scoping review[ 4] revealed that there is little research looking at scuba interventions compared to other water-based interventions for people with neurological disabilities, intellectual disabilities, or autism; however, this is an emerging area. The quality of the sources identified in this review was limited (18 web sites and non-scientific articles met inclusion criteria), and unlike other forms of water-based activity, no review of therapeutic outcomes from scuba diving has been done.
The literature on hydrotherapy suggests that the water environment can be beneficial for people both physically and psychosocially, owing to four properties of water:[ 5 - 7]
Freedom from the effects of gravity on the body (buoyancy), allowing movement that may be impaired on land;[ 6]
the hydrostatic pressure of water can aid in the reduction of oedema;[ 5]
as water is more viscous than air, it adds resistance to a moving limb which can help increase strength;[ 7]
a typical therapy pool is usually between 32-33°C, and this warm environment allows for greater muscle relaxation and a decrease in tone.[ 8]
It is unknown to what extent these qualities may apply to scuba diving, particularly considering potential differences such as decreased water temperature and increased hydrostatic pressure. However, even at the lower temperatures typical of diving environments, there is evidence of physical benefits such as a decrease in plasma renin activity, plasma cortisol concentrations, heart rate and blood pressure.[ 9] In addition to the physical effects of water environments, there is a potential for psychosocial benefits, with one theory, 'blue mind',[ 10] positing that being in or around water improves brain chemistry and decreases stress levels, ultimately improving mental health. Such factors as cold, increased pressure, hyperoxia and the formation of intravascular bubbles all potentially contribute to increase oxidative stress.[ 11 , 12]
The aim of this review was to explore all available research on the physical and psychosocial effects of scuba diving for individuals with neurological disability, autism and intellectual disabilities.
Method
The review protocol was registered with PROSPERO (ID number CRD42019131724) and followed the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement 27-item checklist.[ 13]
INCLUSION AND EXCLUSION CRITERIA
The modified PICO (population, intervention, comparator and outcome), PIO (population, intervention and outcome) format was used in the formation of the question and the inclusion/exclusion criterion, as there was no comparator in this review.
The population group included in this review was participants of any age or gender with neurological disabilities, intellectual disabilities or autism. As such, musculoskeletal conditions and other disabilities (not defined as those above) were excluded. Scuba diving-based interventions were considered for inclusion in this review. The intervention must have utilised scuba equipment in any water setting (pool, ocean). Both recreational and therapeutic focused scuba interventions were considered. Other water-based interventions that did not use scuba equipment were excluded. All types of physical and psychosocial outcomes were explored. Papers were excluded if they did not explore intervention outcomes. Only papers written in English (full text) were included. No publication date or publication status restrictions were imposed. Papers could include other disability groups or participants without a disability as long as data for the disabilities of interest (neurological disability, intellectual disability and autism) could be extracted separately.
SEARCH STRATEGY
The initial search was completed on 14 June 2018 and was updated on 05 May 2020. MEDLINE, EMBASE, Ovid Emcare, and SportDiscus online databases were searched, with the following search terms from MEDLINE: 'Disabled Persons/', 'disabil', 'handicapped', '˜Hydrotherapy/', 'hydrotherap* or hydro-therap* or aqua therap* or water therap* or water based or water exercise*', 'immersion* or submersion*', and 'diving or swimming or scuba or snorkel*'. The broader terms were used to ensure no papers were missed owing to alternative descriptions (e.g., swimming or hydrotherapy), and all non-scuba interventions were excluded. The key search terms from above were altered to suit each database, ensuring that as many papers were captured as possible. The above search was completed on the same day for all four databases, ensuring that the information gathered were within the same date restriction.
STUDY SELECTION AND SCREENING
Peer-reviewed literature was imported into EndNote X9.2 (Clarivate, Philadelphia, USA) and then screened through Covidence (Veritas Health Innovation, Melbourne, Australia), with two reviewers completing the abstract, full text and extraction phases (principal investigator and colleague). Any disagreements between the two reviewers were resolved through face-to-face discussion.
QUALITY ASSESSMENT
The McMaster Critical Appraisal tools (quantitative and qualitative) were used for quality assessment.[ 14] The appraisal tools had extended responses and yes/no questions (yes receiving 1 point, N/A or No receiving 0 points) helping to determine the quality of the papers. Quantitative papers received a total score out of 14, while qualitative papers were scored out of 22. The quality assessment tool was completed by both reviewers and compared for discrepancies with any disagreement resolved through face-to-face discussion. Finally, included papers were categorised into an evidence hierarchy as determined by study design, degree of bias and subsequent level of evidence.[ 15]
DATA EXTRACTION
Data were extracted into a purpose-designed Excel® spreadsheet (Microsoft Office 365, Redmond, USA) by both reviewers. From this, a comparison between the information extracted was conducted to ensure consistency. There was a 100% agreement rate between reviews. If there had been any disagreements, these would have been resolved by face-to-face discussion with a third reviewer being involved if needed. The information extracted included author, year, country of origin, participant details (including, age, gender and condition), intervention details (description and length of time participants were involved) and study design.
DATA SYNTHESIS
It was predicted from preliminary literature searches, that there would be a low number of included papers; thus, there was no minimum number required for this review. The included papers were diverse in design and quality. Therefore, a narrative synthesis was conducted to summarise findings. An exploration of the similarities and differences of the interventions, outcome measures and the results was carried out. The narrative synthesis follows the four elements outlined by the Centre for Reviews and Dissemination:[ 16] theory development; preliminary synthesis of included papers; exploring relationships between papers and assessing the robustness of the synthesis.
Results
INCLUDED PAPERS
A total of 1,562 papers were screened in this review of which only four met the inclusion criteria (Figure 1). Therefore, owing to the limited number of papers and the lack of any reported quantitative data or consistency in outcomes, a meta-analysis/meta-synthesis was not completed.
Figure 1.
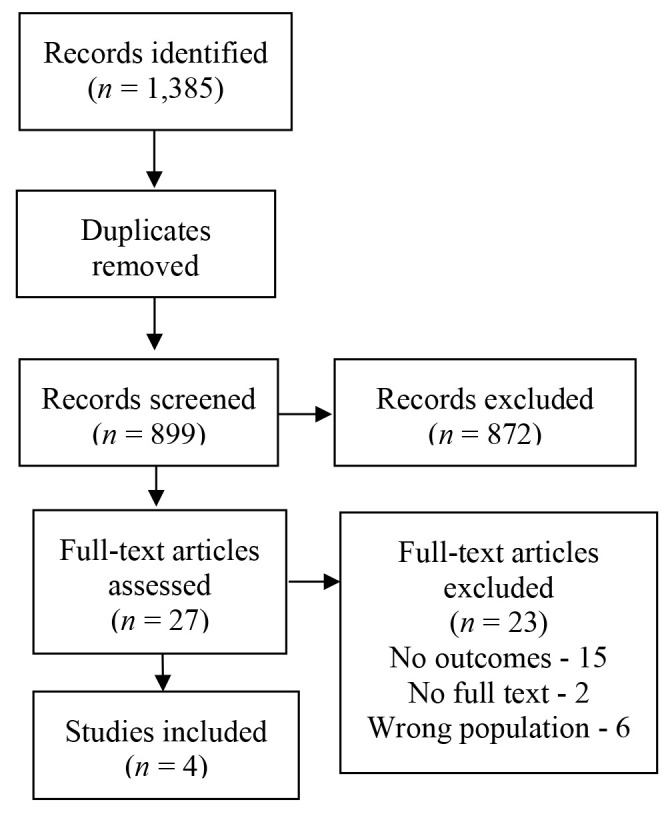
PRISMA flow chart of included papers
OUTCOMES
Sample size for the four papers varied from two to 23 participants, with a range of conditions included. Only one paper mentioned safety or medical guidelines, reporting that all participants underwent a medical screening that was "conducted to a standard described by Edmonds, Lowry and Pennefather and accepted by the Royal Australian Naval School of Underwater Medicine."[ 17] Details provided from the medical screening were minimal, though it was noted that special consideration was needed depending on the disability type and severity. None of the papers reported physical outcomes; however, all four included psychosocial measures, with only descriptive statistics being used in the reporting of results.
Study one,[ 17] from Australia, included case studies of 16 participants. Out of these 16 participants, only eight met the inclusion criteria (and will be the sole focus of this discussion), four with acquired brain injury, two with a spinal cord injury, one with spina bifida and one with post-polio syndrome. All eight participants were male with a mean age of 22.3 years. Participants, new to scuba, were trained to dive. The course was completed over a nine-month period, including 40 hours of theory, 40 hours of training in a pool, and 138 hours of training in the open sea. Psychosocial measures included anxiety levels through the State-Trait Anxiety Inventory, psychophysiological disturbance screened through the Cornell Medical Index and self-concept measured through the Tennessee Self-Concept Scale (TSCS). The paper's focus was on learning how best to safely teach people with disabilities to scuba dive, so minimal effects were reported. However, it was reported that physical self-concept improved for six out of eight completing participants.[ 17]
Study two,[ 18] from the USA, involved two groups of divers in a cross-sectional survey. In a group of seven (one female and six males, mean age 35.1 years, with one to three years of diving experience) divers with disabilities, four had a spinal cord injury, two had cerebral palsy and one an intellectual disability. The second group consisted of eight divers without disabilities from a recreational dive club, selected to match the level of experience of the divers with disabilities. The paper explored the motivation of people with and without a disability to participate in scuba diving through the modified version of the Participation Reasons Scale. Both groups reported similar motivations. The excitement of the activity and participants wishing to play and have fun were reported as the most important reasons for participation for divers with disabilities, with the least important reasons including the activity pleasing others close to the participant and participants feeling needed and wanted by others. For divers without a disability, they rated similar reasons around excitement and having fun, but the third ranking was to relieve tension, whereas divers with disabilities rated this much lower, ranking it twentieth.[ 18]
Study three,[ 19] from Canada, interviewed two men aged 33 and 47 years with spinal cord injuries, with one year and less than one year of diving experience respectively, who were recruited from a recreational dive club. Semi-structured interviews into the experience of scuba diving as a person living with a disability were conducted. The following themes emerged from the interviews: Freedom from impairment (feeling equal to divers without a disability in the water); enhancement of social experiences (meeting new people, interacting with others both with and without a disability); enhancement of self-concept (sense of achievement, increased control and independence) and optimal experience (enjoyment of the activity and environment).[ 19]
Study four,[ 20] from Italy, involved 23 participants with no previous diving experience (seven female and 16 male, aged 16 to 30 years), three with autism spectrum disorder, four with intellectual disability, one with spinal cord injury and 14 with Down syndrome. Participants underwent a specific scuba training course delivered by Disabled Divers International (DDI) with divers obtaining a qualification that allows the diver to "perform recreational dives, within the limits of the certification obtained, in the seas around the world."[ 20] The paper explored the cognitive effects of a specifically designed scuba diving teaching method (by DDI) using the Nepsy II battery.[ 21] A 'general improvement' in visual attention and understanding instruction from being involved in the DDI method was reported.[ 20]
Of the four papers, studies two and four were assessed as low quality,[ 18 , 20] and studies One and Three as of moderate quality.[ 17 , 19] On the McMaster appraisal tools, the three quantitative studies[ 17 , 18 , 20] were rated as level 5 on the hierarchy of evidence,[ 17] with the study designs including a multiple case study and a cross-sectional investigation. study three,[ 19] which included a phenomenological study scored 13/22 on the quality tool. Because of the generally low quality of the data, the detailed scores are not presented here but are available from the author on request.
Discussion
This systematic review is the first that the authors are aware of to collate research on scuba interventions for people with neurological and neurodevelopmental disability. Overall, there is a lack of research in this area, as well as only limited data provided in the few papers identified in the search. Scuba interventions for people living with disabilities were reported as being enjoyable and promoted an increase in self-concept. However, the four studies identified only provide relatively weak evidence with which to determine the psychosocial effects of scuba interventions for the included population.
Self-concept as an outcome was reported in studies one and three.[ 17 , 19] It is suggested that self-concept is lower for people with disabilities than for people without disabilities.[ 22 , 23] As self-concept directly affects mental health and well-being,[ 23] increases in self-concept can highlight the abilities of the person and improve overall health and wellbeing. The overall self-concept of people with disabilities can be raised by instruction in scuba diving, but the long-term effects are unknown.[ 17]
In study three, the two divers with spinal cord injuries expressed that they felt 'in control' of their bodies and had a new-found confidence in themselves.[ 19] Additionally, it was suggested that they experienced feelings of achievement and competency not only from the activity itself but from their ability to adapt to the complex environment of the ocean.[ 19] Several psychosocial benefits were identified, including an enhancement of social experiences, freedom from impairment and equality with other divers. Some of these positive experiences stemmed from meeting and interacting with divers both with and without a disability and working in buddy teams during dives. Additionally, the "psychology of optimal experience" may be used to assist with understanding their responses.[ 19] 'Optimal experience' is defined as an occasion "where we feel a sense of exhilaration, a deep sense of enjoyment, which we cherish".[ 24] It is suggested that scuba interventions provide this deep sense of enjoyment and the experience is cherished.
The findings from study four suggest improved cognition, in particular, visual attention and understanding instruction, for participants with an intellectual disability learning to dive.[ 20] Whether the specific teaching technique (DDI) could be applied to skills other than scuba, is unknown; nonetheless, an increase in visual attention and the ability to understand instructions may translate into learning new skills for daily life.
There are both similarities and differences when comparing the motivation to participate in divers with and without disabilities. Divers without disabilities ranked the relief of tension much higher (third) than people with disabilities (ranked twentieth). Divers without disabilities appear to use scuba to escape and relax both mentally and physically. This does not appear to be the same focus for divers with a disability, with statements regarding the challenge and the test of physical skills ranked higher by these individuals. Divers with a disability appear to enjoy the challenge of diving, exploring a different environment and movements that they may not have thought possible.[ 18]
A limitation of this study was the exclusion of non-English papers and the grey literature. Also, as this review focuses only on participants with neurological disability, intellectual disability and autism, this may have limited the number of included papers. More research is needed, including other groups, such as those with musculoskeletal conditions that limit muscle strength, mobility or physical function and those with limited cardiovascular fitness. Exploration into pain, spasticity and mood may also provide valuable insights. Additionally, the scuba interventions described in two of the studies,[ 17 , 20] were completed over prolonged periods of time with extraordinary training measures in comparison to mainstream open water diver training. They are also relatively elaborate in the context of therapeutic or recreational programmes for people with a disability. As such it is important that future research in scuba-based interventions should also consider the burden and difficulty of providing/delivering these interventions.
Finally, since the completion of this review, one additional paper has been discovered that would meet the requirements to be included.[ 25] The paper explored thermal balance of divers with and without a spinal cord injury (SCI) in open water diving. It was found that divers with SCI were unable to maintain gastrointestinal temperature during short, shallow dives in 6°C water and their temperatures fell further post-dive. Overall, the results of this study do not change the overall conclusions of this paper, but do provide valuable information regarding the safety of open water diving in colder temperatures for people with an SCI.
Conclusion
Scuba diving for people with neurological disability, intellectual disability and autism appears to be a fun and enjoyable experience, increasing a person's self-concept. However, there is limited research on scuba interventions for these population groups. Future research direction should explore both the physical and psychosocial effects of scuba interventions, using robust study designs.
Footnotes
Conflict of interest and funding: nil
Contributor Information
Karlee Naumann, Alliance for Research in Exercise, Nutrition and Activity (ARENA), University of South Australia, School of Allied Health and Human Performance, Adelaide, SA, Australia.
Jocelyn Kernot, University of South Australia, School of Allied Health and Human Performance, Adelaide, SA, Australia.
Gaynor Parfitt, Alliance for Research in Exercise, Nutrition and Activity (ARENA), University of South Australia, School of Allied Health and Human Performance, Adelaide, SA, Australia.
Bethayn Gower, Alliance for Research in Exercise, Nutrition and Activity (ARENA), University of South Australia, School of Allied Health and Human Performance, Adelaide, SA, Australia.
Adrian Winsor, Department of Hyperbaric Medicine, Royal Adelaide Hospital, Central Adelaide Local Health Network, SA Health, Adelaide, SA, Australia.
Kade Davison, Alliance for Research in Exercise, Nutrition and Activity (ARENA), University of South Australia, School of Allied Health and Human Performance, Adelaide, SA, Australia.
References
- World Health Organization. Disability and health. [cited 2019 Jan 23]. Available from: https://www.who.int/news-room/fact-sheets/detail/disability-and-health/.
- Dive heart. [cited 2018 Apr 18]. Available from: http://www.diveheart.org/.
- Determined2 . Immersion therapy service. [cited 2018 April 04]. Available from: https://www.determined2.com.au/immersion-therapy.html.
- Naumann K, Kernot J, Parfitt G, Gower B, Davison K. Water-based interventions for people with neurological disability, autism and intellectual disability: A scoping review. Adapt Phys Activ Q. 2021;38:474–93. doi: 10.1123/apaq.2020-0036. [DOI] [PubMed] [Google Scholar]
- Becker BE. Aquatic therapy: scientific foundations and clinical rehabilitation applications. PM R. 2009;1:859–72. doi: 10.1016/j.pmrj.2009.05.017. [DOI] [PubMed] [Google Scholar]
- Stan AE. The benefits of participation in aquatic activities for people with disabilities. J Sports Med. 2012;8:1737–42. [Google Scholar]
- Conatser P. Adapted aquatics and rehabilitation: a literature synthesis. Int J Aquat Res Educ. 2007;1:242–54. doi: 10.25035/ijare.01.03.07. [DOI] [Google Scholar]
- Getz M, Hutzler Y, Vermeer A. Effects of aquatic interventions in children with neuromotor impairments: a systematic review of the literature. Clin Rehabil. 2006;20:927–36. doi: 10.1177/0269215506070693. [DOI] [PubMed] [Google Scholar]
- Šrámek P, Šimečková M, Janský L, Šavlíková J, Vybíral S. Human physiological responses to immersion into water of different temperatures. Eur J Appl Physiol. 2000;81:436–42. doi: 10.1007/s004210050065. [DOI] [PubMed] [Google Scholar]
- Nichols WJ. Blue mind, 1st ed. New York (NY): Little, Brown and Company; 2014. [Google Scholar]
- Perović A, Unić A, Dumić J. Recreational scuba diving: negative or positive effects of oxidative and cardiovascular stress? Biochem Med (Zagreb). 2014; 24: 235- 47. 10.11613/BM.2014.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gomes EC, Silva AN, de Oliveira MR. Oxidants, antioxidants, and the beneficial roles of exercise-induced production of reactive species. Oxid Med Cell Longev. 2012;2012:756132. doi: 10.1155/2012/756132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liberati A, Altman AG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Law M, Stewart D, Letts L, Pollock N, Bosch J, Westmorland M. Guidelines for critical review of qualitative studies. McMaster University occupational therapy evidence-based practice research group, 1998. [cited 2019 Jan 23]. Available from: https://healthsci.mcmaster.ca/docs/librariesprovider130/default-document-library/guidelines-for-critical-review-form-qualitative-studies-english.pdf?sfvrsn=64bb7bf5_2
- Straus S, Glasziou P, Richardson S, Haynes B. Evidence-based medicine: how to practice and teach EBM. 5th ed. Edinburgh: Elsevier; 2019.p. 81. [Google Scholar]
- Akers J. Systematic reviews: CRD’s guidance for undertaking reviews in health care. University of York Centre for Reviews Dissemination; 2009. Available from: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf. [Google Scholar]
- Williamson JA, McDonald FW, Galligan EA, Baker PG, Hammond CT. Selection and training of disabled persons for scuba-diving. Medical and psychological aspects. Med J Aust. 1984;141:414–8. [PubMed] [Google Scholar]
- Yarwasky L, Furst DM. Motivation to participate of divers with and without disabilities. Percept Mot Skills. 1996;82:1096–8. doi: 10.2466/pms.1996.82.3c.1096. [DOI] [PubMed] [Google Scholar]
- Carin-Levy G, Jones D. Psychosocial aspects of scuba diving for people with physical disabilities: An occupational science perspective. Can J Occup Ther. 2007;74:6–14. doi: 10.2182/cjot.06.07. [DOI] [PubMed] [Google Scholar]
- Stefania M, Marsico E, Cassese FP. Assessment of the impact of an inclusive diving program, on subjects with cognitive disability: analysis of the enhancement of cognitive processes. J Phys Educ Sport. 2019;19:1937–42. doi: 10.7752/jpes.2019.s5288. [DOI] [Google Scholar]
- Korkman M, Kirk U, Kemp S. NEPSY-II: a developmental neuropsychological assessment. San Antonio (TX): The Psychological Corporation; 2007. p. 80 101. [Google Scholar]
- Wei X, Marder C. Self-concept development of students with disabilities: disability category, gender, and racial differences from early elementary to high school. Remedial Spec Educ. 2012;33:247–57. doi: 10.1177/0741932510394872. [DOI] [Google Scholar]
- Tam SF. Comparing the self-concepts of persons with and without physical disabilities. J Psychol. 1998;132:78–86. doi: 10.1080/00223989809599266. [DOI] [PubMed] [Google Scholar]
- Czikszentmihalyi M. Flow: The psychology of optimal experience. New York: Harper & Row; 1990. [Google Scholar]
- Gajsek U, Sieber A, Finderle Z. Thermal balance of spinal cord injured divers during cold water diving: a case control study. Diving Hyperb Med. 2020;50:256–63. doi: 10.28920/dhm50.3.256-263. [DOI] [PMC free article] [PubMed] [Google Scholar]