

Abstract
Platelet-rich plasma (PRP) therapy is a new method for the treatment of androgenetic alopecia (AGA), the effectiveness and safety of which continues to be studied. Information on comparative efficacy when combining PRP with other methods of treatment is limited. The aim of the study was a comparative evaluation of the clinical efficacy of minoxidil, PRP therapy, and their combination in the treatment of men with AGA.
Materials and Methods:
The study included 69 men. The patients were divided into three observation groups: the main group (25 people, received applications of a 5% solution of minoxidil in combination with PRP injections), the comparison group (22 people, received intradermal injections of PRP), and the control group (22 people, received applications of a 5% solution of minoxidil). The clinical efficacy of the therapy was evaluated by the dynamics of morphometric indicators of hair growth using a digital camera and the software.
Results:
It was established that after complex therapy in the form of minoxidil applications and injections of PRP, the hair density increased by 32% (P = 0.00004), the diameter of the hair shafts by 26% (P = 0.00004), the share of vellus hair decreased by 30% (P = 0.00082), and the proportion of telogen hair decreased by 39% (P = 0.00008). The results of using complex therapy significantly exceeded the clinical effect of platelet-rich plasma and topical applications of a 5% solution of minoxidil.
Conclusions:
The data obtained allows suggesting that PRP and minoxidil potentiate each other's action when used together and their complex application seems promising for the treatment of androgenetic alopecia.
Key words: Androgenetic alopecia, intradermal injections platelet-rich plasma, minoxidil applications, MPHL, platelet-rich plasma therapy
INTRODUCTION
Androgenetic alopecia (AGA) is one of the most common diseases; it affects up to 50% of men and 40% of women by the age of 50 years.[1,2,3] Platelet-rich plasma (PRP) therapy is a new treatment for hair diseases, which effectiveness and safety continues to be studied. The researchers demonstrated the positive effects of PRP in treatment of patients with AGA, which were manifested in reducing hair loss and increasing hair density.[4,5,6,7,8,9] In 2018, European AGA treatment guidelines focused attention on PRP therapy, though recognizing that clinical data are still insufficient for a good evidence base of this treatment method.[10] At the same time, studies demonstrating the comparative effectiveness of PRP in the complex AGA treatment, for example, in combination with traditional therapies (minoxidil, finasteride), are rare.[11] No work has been published on the comparative evaluation of the efficacy of minoxidil monotherapy, PRP monotherapy, and their combinations in men with AGA.
The aim of our study was a comparative evaluation of clinical efficacy of minoxidil, PRP therapy, and their combination in treatment of men with AGA.
MATERIALS AND METHODS
Sixty-nine patients aged from 18 to 53 years were under our supervision. The criteria for inclusion of patients in the study were as follows: the males; the presence of AGA from the 1st to the 5th stage inclusive according to the Hamilton–Norwood scale; and availability of control measurements before and after treatment. As the requests from patients who meet these criteria were received, they were offered a choice of treatment method (PRP, minoxidil, or their combination) with the doctor's explanation of the advantages and disadvantages of each one, and the expected clinical effect. This is the way the patients were divided into three groups of observation: main group (25 men), comparison group, and control group (22 men each). There were no differences between the observation groups in the history and quality of the hair [Tables 1 and 2].
Table 1.
The structure of the sample before the treatment
| Variable | Monitoring groups |
Total |
||||||
|---|---|---|---|---|---|---|---|---|
| PRP |
Minoxidil |
Complex therapy (PRP + minoxidil) |
||||||
| Number of persons | Percentage | Number of persons | Percentage | Number of persons | Percentage | Number of persons | Percentage | |
| Age (years) | ||||||||
| 20 and younger | 1 | 4.0 | 3 | 13.6 | 0 | 0 | 4 | 5.8 |
| 21-30 | 13 | 52.0 | 12 | 54.6 | 12 | 54.5 | 37 | 53.6 |
| 31-40 | 9 | 36.0 | 5 | 22.7 | 5 | 22.7 | 19 | 27.5 |
| 41 and older | 2 | 8.0 | 2 | 9.1 | 5 | 22.7 | 9 | 13.0 |
| Average age (years), M±m | 30.0±2.5 | 27.3±3.5 | 31.7±3.8 | 29.7±1.9 | ||||
| P | 0.06915 | |||||||
| Severity of AGA according to the Hamilton-Norwood scale | ||||||||
| 1 | 2 | 8.0 | 1 | 4.5 | 1 | 4.5 | 4 | 5.8 |
| 2 | 9 | 36.0 | 8 | 36.4 | 5 | 22.8 | 22 | 31.9 |
| 3 | 7 | 28.0 | 10 | 45.4 | 5 | 22.8 | 22 | 31.9 |
| 4 | 7 | 28.0 | 2 | 9.1 | 10 | 45.4 | 19 | 27.5 |
| 5 | 0 | 0.0 | 1 | 4.5 | 1 | 4.5 | 2 | 2.9 |
| P | 0.1983 | |||||||
PRP – Platelet-rich plasma; AGA – Androgenetic alopecia
Table 2.
The morphometric indicators of hair growth before treatment
| Variable | Monitoring groups |
Total | P | ||
|---|---|---|---|---|---|
| PRP | Minoxidil | Complex therapy (PRP + minoxidil) | |||
| Hair density on 1 cm2 | 381.5±45.4 | 479.3±51.5 | 408.4±43.6 | 421.2±27.5 | 0.35 |
| Share of vellus hair (%) | 49.6±7.3 | 34.4±5.3 | 51.8±6.3 | 45.5±4.0 | 0.79 |
| Average diameter of all hair, μm | 39.8±3.8 | 39.3±1.9 | 38.8±4.2 | 39.3±1.8 | 0.37 |
| Share of telogen hair (%) | 42.0±3.5 | 42.8±6.7 | 50.4±7.3 | 44.9±3.8 | 0.73 |
| Ratio of hair in the telogen/anagen stage | 1/2.28±1/1.51 | 1/1.62±1/0.41 | 1/1.26±1/0.51 | 1/1.74±1/0.57 | 0.69 |
PRP – Platelet-rich plasma
Criteria for patients exclusion from the study were as follows: the presence of AGA of the 6th stage and higher according to the Hamilton–Norwood scale; the presence of laboratory-confirmed hyperandrogenism; the presence of inflammation on the scalp; the use of external preparations stimulating hair growth, including those containing minoxidil; taking antiandrogenic drugs that affect the exchange of steroid hormones (finasteride, dutasteride); the presence of endocrinopathy affecting the exchange of steroid hormones (diabetes, hypo- or hyperthyroidism, hyperprolactinemia); and previous hair transplantation. For patients of the main and the comparison groups, additional exclusion criteria were as follows: taking drugs that reduce the platelets level (aspirin or other nonsteroidal anti-inflammatory drugs); the presence of leukocytosis or thrombocytopenia in blood tests; the presence of side effects of treatment; and a tendency to form keloid or hypertrophic scars in history. Informed consent for examination and treatment was obtained from all patients. The study was approved by the independent ethics committee.
Patients of the main group received PRP injections in combination with applications of 5% minoxidil solution; patients of the comparison group received PRP injections; and patients of the control group received applications of 5% minoxidil solution. The patients of the main and control groups applied minoxidil according to the standard method: on dry skin of the scalp two times a day (every day) in an amount of 1 ml, without subsequent rinsing, during 4 months. The course of PRP injections in patients of the main and the comparison group consisted of four procedures with an interval of 1 month. Monitoring of patients of the control group was performed 4 months after the start of treatment with minoxidil; monitoring of patients of the main and comparison groups was performed 1 month after the fourth PRP therapy procedure.
To obtain PRP from each patient, 18 ml of blood was received in two test tubes with an anticoagulant (3.8% sodium citrate in 1:9 ratio) by venipuncture. Twofold centrifugation of blood was carried out using a GT 416 centrifuge manufactured by Glotech Co., Ltd (Korea), with a horizontal rotor and a soft-start mode. The first centrifugation was carried out for 5 min at a speed of 1800 rpm [Figure 1a], after which the erythrocyte mass was separated. Plasma containing leukocyte and platelet layers was subjected to a second centrifugation at a speed of 2500 rpm for 10 min [Figure 1b]. As PRP, 2 ml of the lower part of the supernatant from each tube was used; plasma separation was performed manually. As an activator, 10% calcium cChloride solution was used in a 1:20 ratio. The scalp surface was treated with chlorhexidine solution, local anesthesia was not applied. The resulting PRP was injected into the scalp by microinjection, intradermally, at approximately 0.15 ml per injection [Figure 2].
Figure 1.
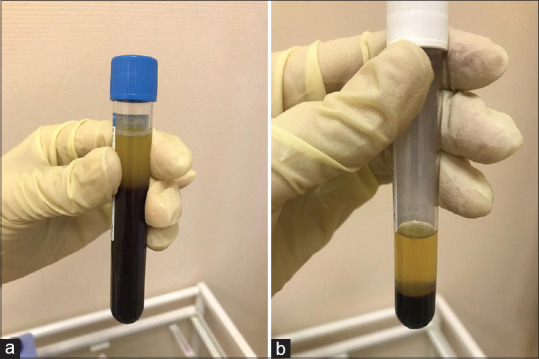
Separation of the erythrocyte layer and plasma after the first (a) and after the second centrifugation (b)
Figure 2.

Performing a platelet-rich plasma injection to a patient
Assessment of AGA severity was carried out during clinical examination according to the Hamilton–Norwood scale (1975). Evaluation of clinical efficacy was performed according to the dynamics of phototrichological parameters. The Aramo S digital video camera (Aram Huvis Co., Ltd., Korea) and the TrichoSciencePro v1.3RUS computer program were used for a phototrichological study with the measurement of hair growth indicators. The control points were marked with a tattoo mark and were located in the parietal zone, approximately 2 cm closer to the center of alopecia from the border of thinning hair. In the field of control measurements, hair was trimmed 48 h before the study and dyed with dark RefectoCil hair color (Austria) which improves contrast and contributes to more accurate counting immediately before trichoscopy and phototrichogram. In the course of phototrichological research, the indicators of hair density (per 1 cm2), average hair diameter (μm), proportion of telogen and vellus hair (%), as well as ratio of the number of anagen hair per telogen one were studied.
Statistical processing and visualization of the results were carried out using the R programming language and the Coin and Ggplot2 libraries. The arithmetic mean was used as an indicator of the distribution center since the distributions correspond to the normal one according to the Shapiro–Wilk test. The estimates stability is reflected using confidence intervals at γ = 0.95. To test the relationship between the nominative (grouped) data, the Fisher's exact test was used (a rigorous analog of the Chi-square test for small samples). The Wilcoxon nonparametric paired t-test was used to check the relationship between the quantitative data. P value, the probability of an error when the null hypothesis is rejected (first kind error probability), was calculated for all statistical tests; P < 0.05 was considered statistically significant.
RESEARCH RESULTS
Patients of the main group who received complex therapy (applications of 5% minoxidil solution and PRP injections) obtained the following result: all indicators of hair growth underwent significant changes. Hair density increased by 32% (P = 0.00004), the average diameter of hair rods increased by 26% (0.00004). The intensity of hair loss decreased by 39% (P = 0.00008), which was combined with a 30% decrease in the share of vellus hair (P = 0.00082). The amount of anagen hair in relation to telogen one increased by 256% (P = 0.00007) [Table 3 and Figure 3].
Table 3.
Dynamics of morphometric indicators of hair growth
| Variable | Unit of measurement | Monitoring groups |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Complex therapy (PRP + minoxidil) |
PRP |
Minoxidil |
||||||||
| Before treatment | After treatment | Dynamics of change | Before treatment | After treatment | Dynamics of change | Before treatment | After treatment | Dynamics of change | ||
| Hair density on 1 cm2 | Abs. | 408.4±43.6 | 539.6±52.1 | 131.2 | 381.5±45.4 | 426.1±50.1 | 44.6 | 479.3±51.5 | 554.8±53.5 | 75.5 |
| ∆ (%) | 32 | 12 | 16 | |||||||
| P | 0.00004 | 0.000067 | 0.00073 | |||||||
| Share of vellus hair (%) | Abs. | 51.8±6.3 | 36.5±7.4 | −15.3 | 49.6±7.3 | 41.0±7.7 | −8.6 | 34.4±5.3 | 35.2±6 | 0.8 |
| ∆ (%) | −30 | −17 | 2 | |||||||
| P | 0.00082 | 0.002225 | 0.7647 | |||||||
| Average diameter of all hair (μm) | Abs. | 38.8±4.2 | 48.8±5.1 | 10.0 | 39.8±3.5 | 44.4±4.5 | 4.6 | 39.3±1.9 | 40±2.9 | 0.7 |
| ∆ (%) | 26 | 12 | 2 | |||||||
| P | 0.00004 | 0.001947 | 0.338 | |||||||
| Share of telogen hair (%) | Abs. | 50.4±7.3 | 30.7±7.4 | −19.7 | 42.0±6.4 | 35.3±7.0 | −6.8 | 42.8±6.7 | 44.9±6.9 | 2.1 |
| ∆ (%) | −39 | −16 | 5 | |||||||
| P | 0.00008 | 0.02836 | 0.338 | |||||||
| Ratio of hair in the telogen/anagen stage | Abs. | 1/1.26±1/0.51 | 1/4.48±1/2.38 | 1/3.22 | 1/2.28±1/1.51 | 1/2.68±1/0.88 | 1/0.4 | 1/1.62±1/0.41 | 1/1.58±1/0.48 | −1/0.04 |
| ∆ (%) | 256 | 18 | −2 | |||||||
| P | 0.00007 | 0.01554 | 0.51 | |||||||
PRP – Platelet-rich plasma
Figure 3.
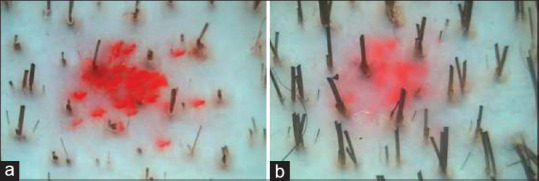
Phototrichogram of a patient receiving complex therapy – applications of a 5% minoxidil solution and platelet-rich plasma injections: (a) before treatment; (b) after treatment. Magnification ×60
Patients of the comparison group who received PRP injections obtained the following result: all the indicators of hair growth were also subject to significant changes. Hair density increased by 12% (P = 0.000,067), average hair diameter increased by 12% (P = 0.001947), the share of vellus hair decreased by 17% (0.002225), and the proportion of telogen hair decreased by 16% (P = 0.02836). At the same time, the number of anagen hair in relation to telogen one increased by 18% (P = 0.015554) [Table 3 and Figure 4]. There were no side effects of PRP therapy in the main and the comparison groups.
Figure 4.
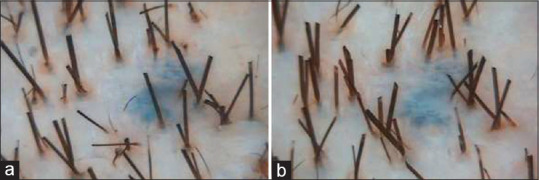
Phototrichogram of a patient who received an injections of platelet-rich plasma: (a) before treatment; (b) after treatment. Magnification ×60
Patients receiving standard therapy with 5% minoxidil solution obtained the following result: hair density significantly increased by 16% (P = 0.00073) [Table 3 and Figure 5].
Figure 5.
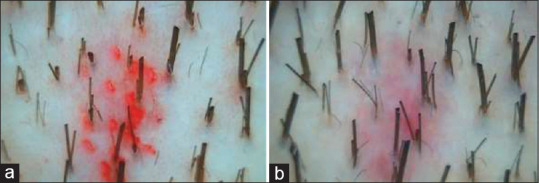
Phototrichogram of a patient who received standard therapy with a 5% minoxidil solution: (a) before treatment; (b) after treatment. Magnification ×60
In the course of a comparative analysis, it was found that the characteristics of complex therapy compared to traditional therapy with minoxidil were as follows: increase in hair density by 1.74 times (△32% and 16%, respectively, P = 0.0347), increase in hair rods thickness by 14.3 times (△26% and 2%, respectively, P = 0.00001); decrease in the share of telogen hair by 9.3 times (△−39% and + 5%, respectively, P = 0.00003), as well as decrease in the share of vellus hair by 19.1 times (△−30% and + 2%, respectively, P = 0.0009). Hair ratio in the anagen and telogen phases in the complex therapy group improved by 80 times as compared with the minoxidil group (△256% and −2%, respectively, P = 0.00001).
The effects of complex therapy exceeded the effects of PRP monotherapy in terms of hair density by 2.9 times (△32% and 12%, respectively, P = 0.0001), hair stem diameter by 2.2 times (△26% and 12%, P = 0.0071), and also proportion of telogen hair by 2.9 times (△−39% and −16%, P = 0.0025). Hair ratio in the anagen and telogen phases in the complex therapy group improved by 8 times as compared with the PRP group (△256% and 18%, respectively, P = 0.0173). Even though the difference in the share of vellus hair in the main group was 1.8 times higher (−30% in the main group and −17% in the comparison group), it was not statistically significant, P = 0.0715.
When comparing treatment results in the comparison and the control groups, no significant differences were found only in terms of hair density, △12 and 16%, respectively (P = 0.1968). PRP effectiveness in terms of average hair diameter was higher by 6.3 times, △12 and 2%, respectively (P = 0.0248); PRP effectiveness in terms of the share of vellus was higher by 11.8 times, △−17 and 2%, respectively (P = 0.0069). As for the share of telogen, PRP effectiveness was higher by 3.1 times, △−16 and 5%, respectively (P = 0.031), and by the amount of anagen per telogen, it was higher by 10.2 times, △18 and −2%, respectively (P = 0.0243).
DISCUSSION
PRP therapy is a simple, cost-effective, and appropriate option for treating hair loss, and it can be considered as AGA therapeutic alternatives. In the course of our study, it was demonstrated that all indicators of hair growth underwent significant changes in patients receiving PRP injections: hair density and average diameter increased by 12%; the share of vellus hair decreased by 17%, and the share of telogen hair decreased by 16%, which is consistent with data on studies of PRP effectiveness published in world literature.
Hair density significantly increased (by 16%) in patients from the control group receiving standard therapy with 5% minoxidil solution. When comparing the results of treatment in PRP and minoxidil groups, no significant differences were found only in terms of hair density, △12 and 16%, respectively. In all other indicators of hair growth, PRP efficiency was significantly higher: 6.3 times higher in terms of average hair diameter; 11.8 times higher in terms of the share of vellus; 3.1 times higher for the proportion of telogen; and 10.2 times higher by the amount of anagen per telogen. The superior PRP effect over inoxidil may have been due to the fact that average patient follow-up is short, and further studies with longer follow-up are needed to draw key conclusions, including long-term treatment efficacy. Four months is the minimum period for evaluating minoxidil effectiveness; that is why it is better to evaluate it in a more remote period of 6–12 months. However, the data we have sum up that PRP also has a delayed effect and, in some cases, with a longer observation period (8–12 months), shows an improvement in the dynamics of hair growth indicators (these data are planned to be published). Navarro et al. retrospectively compared plasma rich in growth factors (PRGF) with local minoxidil therapy for AGA treatment, where the decrease in the telogen proportion was higher in PRGF group.[12] In a very recently published study, Verma et al. also noted that PRP therapy had an effect that was superior to minoxidil, and could be a valuable alternative to topical therapy with minoxidil during AGA treatment.[13]
In our work, the result of the combined use of PRP and minoxidil was of particular interest. A similar study was published in 2018. Alves R. and Grimalt R. showed that using PRP in combination with the standard treatment method (minoxidil or finasteride) shows a more pronounced clinical effect confirmed by trichoscopy, if compared to monotherapy with the last mentioned.[11] Another study by Shah et al. was aimed at comparing the efficacy of topical administration of minoxidil (5%) and combined use of minoxidil and a dermaroller with PRP injections in men with AGA.[14] A group of patients treated with a combination of minoxidil, PRP, and a dermaroller showed greater satisfaction with the treatment, unlike the minoxidil group. Evaluation of the results was carried out after 6 months on the basis of 7-point questionnaire and survey photographs; morphometric data analysis (trichoscopy, phototrichogram) was not conducted.
In the course of our research, the high clinical efficacy of complex therapy and its advantage over PRP monotherapy and the standard method using minoxidil was demonstrated. In the course of comparative analysis, it was found that the effectiveness of complex therapy exceeds the efficiency of traditional therapy with minoxidil in terms of hair density by 1.74 times; hair shaft thickness by 14.3 times; proportion of telogen hair almost by 9.3 times; and the share of vellus hair by 19.1 times. The effects of complex therapy in our study exceeded the effects of PRP monotherapy in terms of hair density by 2.9 times; hair shafts diameter by 2.2 times; and the share of telogen hair by 2.9 times. Although the difference in the share of vellus exceeded by 1.8 times, it was not statistically significant, P = 0.0715.
Minoxidil does not change the level of testosterone or adrenal-androgenic secretion, as well as it does not change the genetically programmed sensitivity of hair follicles to androgens. PRP and minoxidil prolong the anagen phase, promote proliferation and lifespan of the dermal papilla cells during the hair growth cycle by inhibiting apoptosis[15,16,17,18] and, apparently, potentiate each other's effects if they are combined. Data on the specific effect on AGA pathogenesis were not obtained; the mechanism of minoxidil and PRP action has not been fully studied. In 2014, PRP was shown to be effective in treating 11 patients with AGA resistant to treatment with inoxidil and finasteride.[7] Minoxidil sulfate (an active metabolite of minoxidil catalyzed by sulfotransferase enzymes) is responsible for stimulating hair growth; resistance to minoxidil is associated, among other things, with low sulfotransferase activity in the scalp skin. At the same time, another study explained that platelets show minoxidil sulfotransferase activity.[19] A possible relationship between sulfotransferase platelet activity and the high efficiency of PRP in combination with minoxidil is one of the vectors for further study.
Different preparation protocols were used in published studies on PRP effectiveness with a positive effect. Due to the lack of a single standard PRP preparation protocol and AGA treatment method at the moment, we prepared PRP using the method of double centrifugation with soft spin in which blood cells layers were separated manually; we also applied platelet activation through coagulation, which causes the secretion of various growth factors and potentiates mitogenic effects in different cell types. The average number of platelet cells in 1 ml PRP was 882.5 ± 143.62 × 109/L. In our protocol, it was the value determined in each ml from 2 ml of the supernatant of cells after the second centrifugation and we found a good therapeutic effect. Four patients noted slight pain at the injection sites; however, no one refused treatment. Redness of the scalp after injections was also observed, which was natural and soon disappeared. In general, the PRP treatment was well tolerated by the patients; we did not observe other side effects.
We did not use questionnaires, a hair pulling test and other subjective tools to assess therapy effectiveness; we used trichoscopy and phototrichogram as noninvasive methods for quantitative analysis of hair growth indicators in patients. A comparative analysis of phototrichological and morphological data as noninvasive and invasive methods for assessing hair growth before and after treatment confirmed that these methods show unidirectional dynamics; the phototrichogram reliably reflects the morphofunctional state of hair follicle.[20]
The main limitation of our study was the period of research and a small number of patients.
CONCLUSION
Comparative evaluation of treatment results with minoxidil and PRP therapy allows us to consider PRP therapy as a promising method for treating AGA. However, the effects of complex therapy significantly exceeded the effects of PRP-therapy and the effects of minoxidil. If we summarize the obtained data on the effect of PRP and minoxidil combined use, this treatment method can be successfully used in patients with AGA up to the 4th stage inclusive according to the Hamilton–Norwood scale.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Blume-Peytavi U, Blumeyer A, Tosti A, Finner A, Marmol V, Trakatelli M, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164:5–15. doi: 10.1111/j.1365-2133.2010.10011.x. [DOI] [PubMed] [Google Scholar]
- 2.Gan DC, Sinclair RD. Prevalence of male and female pattern hair loss in Maryborough. J Investig Dermatol Symp Proc. 2005;10:184–9. doi: 10.1111/j.1087-0024.2005.10102.x. [DOI] [PubMed] [Google Scholar]
- 3.Messenger A. Androgenetic alopecia in men. In: Blume-Peytavi U, Tosti A, Whiting DA, Trüeb R, editors. Hair Growth and Disorders. Berlin Heidelberg: Springer Verlag; 2008. pp. 159–70. [Google Scholar]
- 4.Betsi EE, Germain E, Kalbermatten DF, Tremp M, Emmenegger V. Platelet-rich plasma injection is effective and safe for the treatment of alopecia. Eur J Plast Surg. 2013;36:407–12. [Google Scholar]
- 5.Cervelli V, Garcovich S, Bielli A, Cervelli G, Curcio BC, Scioli MG, et al. The effect of autologous activated platelet rich plasma (AA-PRP) injection on pattern hair loss: Clinical and histomorphometric evaluation. Biomed Res Int 2014. 2014:760709. doi: 10.1155/2014/760709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gkini MA, Kouskoukis AE, Tripsianis G, Rigopoulos D, Kouskoukis K. Study of platelet-rich plasma injections in the treatment of androgenetic alopecia through an one-year period. J Cutan Aesthet Surg. 2014;7:213–9. doi: 10.4103/0974-2077.150743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khatu SS, More YE, Gokhale NR, Chavhan DC, Bendsure N. Platelet-rich plasma in androgenic alopecia: Myth or an effective tool. J Cutan Aesthet Surg. 2014;7:107–10. doi: 10.4103/0974-2077.138352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Park KY, Kim HK, Kim BJ, Kim MN. Letter: Platelet-rich plasma for treating male pattern baldness. Dermatol Surg. 2012;38:2042–4. doi: 10.1111/dsu.12037. [DOI] [PubMed] [Google Scholar]
- 9.Sclafani AP. Platelet-rich fibrin matrix (PRFM) for androgenetic alopecia. Facial Plast Surg. 2014;30:219–24. doi: 10.1055/s-0034-1371896. [DOI] [PubMed] [Google Scholar]
- 10.Kanti V, Messenger A, Dobos G, Reygagne P, Finner A, Blumeyer A, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men – Short version. J Eur Acad Dermatol Venereol. 2018;32:11–22. doi: 10.1111/jdv.14624. [DOI] [PubMed] [Google Scholar]
- 11.Alves R, Grimalt R. Platelet-rich plasma in combination with 5% minoxidil topical solution and 1 mg oral finasteride for the treatment of androgenetic alopecia: A randomized placebo-controlled, double-blind, half-head study. Dermatol Surg. 2018;44:126–30. doi: 10.1097/DSS.0000000000001198. [DOI] [PubMed] [Google Scholar]
- 12.Navarro MR, Asín M, Martínez MA, Martínez AM, Molina C, Moscoso L, et al. Management of androgenetic alopecia: A comparative clinical study between plasma rich in growth factors and topical minoxidil. Eur J Plast Surg. 2016;39:173–80. [Google Scholar]
- 13.Verma K, Tegta GR, Verma G, Gupta M, Negi A, Sharma R. A study to compare the efficacy of platelet-rich plasma and minoxidil therapy for the treatment of androgenetic alopecia. Int J Trichology. 2019;11:68–79. doi: 10.4103/ijt.ijt_64_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shah KB, Shah AN, Solanki RB, Raval RC. A comparative study of microneedling with platelet-rich plasma plus topical minoxidil (5%) and topical minoxidil (5%) alone in androgenetic alopecia. Int J Trichology. 2017;9:14–8. doi: 10.4103/ijt.ijt_75_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kwack MH, Kim MK, Kim JC, Sung YK. Dickkopf 1 promotes regression of hair follicles. J Invest Dermatol. 2012;132:1554–60. doi: 10.1038/jid.2012.24. [DOI] [PubMed] [Google Scholar]
- 16.Li W, Enomoto M, Ukegawa M, Hirai T, Sotome S, Wakabayashi Y, et al. Subcutaneous injections of platelet-rich plasma into skin flaps modulate proangiogenic gene expression and improve survival rates. Plast Reconstr Surg. 2012;129:858–66. doi: 10.1097/PRS.0b013e3182450ac9. [DOI] [PubMed] [Google Scholar]
- 17.Li ZJ, Choi HI, Choi DK, Sohn KC, Im M, Seo YJ, et al. Autologous platelet-rich plasma: A potential therapeutic tool for promoting hair growth. Dermatol Surg. 2012;38:1040–6. doi: 10.1111/j.1524-4725.2012.02394.x. [DOI] [PubMed] [Google Scholar]
- 18.Semalty M, Semalty A, Joshi GP, Rawat MS. Hair growth and rejuvenation: An overview. J Dermatolog Treat. 2011;22:123–32. doi: 10.3109/09546630903578574. [DOI] [PubMed] [Google Scholar]
- 19.Johnson GA, Baker CA. Sulfation of minoxidil by human platelet sulfotransferase. Clin Chim Acta. 1987;169:217–27. doi: 10.1016/0009-8981(87)90322-6. [DOI] [PubMed] [Google Scholar]
- 20.Pakhomova EE, Smirnova IO. Morphological substantiation of clinical efficacy of platelet rich plasma in the treatment of androgenetic alopecia. Int J Biomed. 2018;8:317–20. [Google Scholar]