

Abstract
This report describes the two-phase orthodontic treatment of a 7-year-, 6-month-old girl who presented with bilateral gemination of the central incisors. The left side demonstrated a complete gemination, resulting in two separate teeth (#9 and #9a). On the right side the gemination was incomplete, resulting in a large tooth mass (#8) that was 11.5 mm wide with a large pulp chamber and two apices. The tooth mass was extracted and the left central incisor (#9) was successfully moved across the midline (through the midpalatal suture area). The supernumerary incisor (#9a) was then used in the upper left central incisor area.
Keywords: Gemination, Midline
INTRODUCTION
Gemination is a rare dental anomaly, the cause of which is unknown, although there is evidence of familial inheritance. It occurs when a single tooth bud attempts to divide. The result can be complete division, resulting in a normal tooth plus a supernumerary tooth, or incomplete division, resulting in a large tooth mass. The pulp chamber in an incomplete division is usually single and enlarged, and may be partially divided.1 The prevalence in an orthodontic patient population has been reported to be 0.07%.2
There have been reports of movement of teeth across the midline. Cookson3 presented a case report in which #8 was moved across the midline to replace an extracted #9 (which had fused with a supernumerary tooth). The midpalatal suture moved to the left, ahead of #8. A frenectomy was performed to minimize the chance of relapse. The treatment was successful, with no radiographic evidence of root resorption.
Follin4 presented a case report in which #8 was removed due to an odontoma. The space was closed from both sides, placing #9 in the midline. The result was stable, with the long axis of #9 appearing coincident with the midpalatal suture on a periapical film.
Follin et al.5 attempted to determine whether it is possible to move a maxillary central incisor across the midpalatal suture area and to determine what happens histologically to the suture when this movement occurs. Utilizing experimental beagle dogs, they moved maxillary central incisors across the midpalatal suture of both young dogs, whose sutures were still patent, and an old dog, whose suture was already closed. The incisors all moved across the midline. Tooth movement was faster in the old dog but caused significant root resorption. In the young dogs, the sutures changed course apical to the test teeth from a straight vertical to an s-shaped direction, with evidence of the suture on the pressure side of the test teeth.
Follin et al.6 followed up this research with another experiment to determine whether it is possible to move an incisor through the midpalatal suture area after surgical removal of the suture. The anterior portion of the suture was removed in young dogs and allowed to fill in with bone. After 17 months, only 33% of the incisors had moved all the way across the midline and all the teeth demonstrated significant root resorption and bone loss.
Both McCollum7 and Melnik8 presented cases of successful movement of maxillary central incisors across the midline. Both had patients with a similar clinical situation to the patient presented here, with bilateral gemination of the central incisors (one side complete, resulting in a supernumerary incisor, and one side incomplete, resulting in a large tooth mass).
PHASE I
Diagnosis and Etiology
A 7-year-, 6-month-old girl presented to my practice with the chief complaint of a large front tooth (Figure 1). She was physically healthy, with no history of dental trauma. Panoramic and periapical films revealed bilateral gemination of the central incisors (Figure 2a,b). The left side demonstrated a complete gemination, resulting in two separate teeth (#9 and #9a). On the right side the gemination was incomplete, resulting in a large tooth mass (#8) that was 11.5 mm wide with a large pulp chamber and two apices. The patient was referred to an oral surgeon for extraction of the large tooth mass and the upper left primary canine (Figure 3a,b). Phase I records were taken 10 months later, after #9a had erupted (Figures 4 through 7).
Figure 1.

The patient, at 7 years and 6 months of age, soon after eruption of the large #8 tooth mass.
Figure 2.

(a) Screening panoramic radiograph that revealed bilateral gemination. The right side gemination was incomplete, resulting in a large tooth mass (#8). The left side gemination was complete, resulting in a central incisor (#9) and a supernumerary tooth (#9a). (b) Periapical film of #8 that reveals a single enlarged pulp canal.
Figure 3.

(a) The relative size of the extracted #8 tooth mass and the upper left central incisor. (b) The extracted tooth mass had 2 apices and one single, enlarged pulp canal.
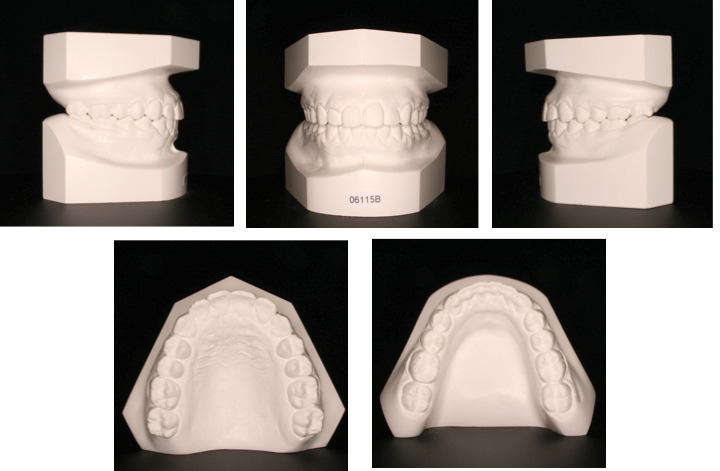
Figures 4–7.

Initial phase I records, taken after #9a erupted.
Figures 4–7.

Initial phase I records. Continued.
Figures 4–7.
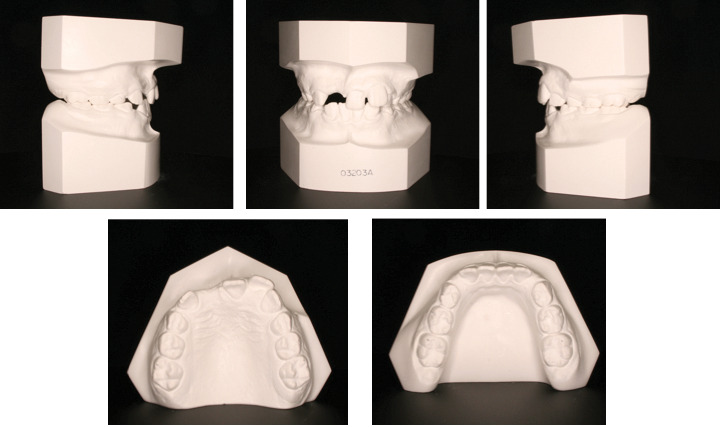
Initial phase I records. Continued.
Figures 4–7.

Initial phase I records. Continued.
The extraoral clinical examination revealed a mildly convex to straight profile with a normal lip profile. There was inadequate incisal display on smile (50%). Dentally, the molars were quarter-cusp Class II with 40% overbite and normal overjet. There was a severe midline discrepancy, with three incisors to the left of the midpalatal suture. There was 3 mm of crowding in each arch. The cephalometric tracing revealed a Class II relationship (ANB 6°) and a mesofacial pattern (Sn-Go-Gn 27°) (Figure 8). Both the maxillary and mandibular incisors were upright (1-Sn 94.5° and 1-MP 89°).
Figure 8.
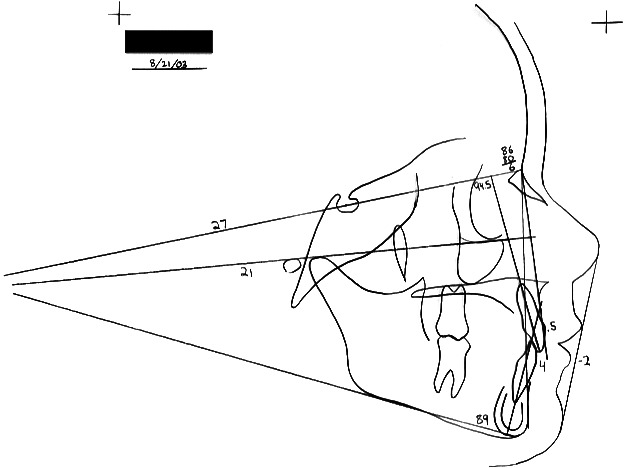
Initial cephalometric tracing.
Treatment
The goal of phase I was to move the midline to the right and effect some distalization/distal rotation of the upper first molars. The upper first molars were banded and 0.018-inch Ormco Diamond twin brackets were placed on the upper primary second molars and incisors. After initial alignment, coil springs with a stopped archwire were used to move the maxillary midline to the right and consolidate the incisors (Figure 9). High-pull headgear was delivered in May 2004 and the patient was instructed to wear it 12 hours/night. The maxillary frenum was “stretched” to the right as the incisors were moved across the midline. Removal of the frenum would potentially allow for a more stable correction. Headgear was stopped and an impression was taken for a Hawley retainer in March of 2005, which was to be delivered 2 weeks after a frenectomy was performed. However, due to loss of insurance the frenectomy was postponed until November 2005 (Figure 10a,b), after which the brackets were removed and a new retainer was delivered.
Figure 9.

Progress photo demonstrating the mechanics used to move #9 across the midline. Notice the frenum stretched to the right of the midline.
Figure 10.

(a) The frenum was stretched to the right at the time of the frenectomy. (b) Immediately postfrenectomy.
Result
The upper first molars were rotated distally, the upper incisors were consolidated, and the upper midline was moved 4 mm to the right. There was some midline relapse during the period of time the patient waited to have her frenectomy performed.
PHASE II
Diagnosis
Phase II records were taken on April 6, 2006 (Figures 11 through 14). The extraoral examination revealed a straight profile with a retrusive lip profile. There was inadequate incisal display on smile (50%). Dentally, the molars were Class I with 40% overbite and 9 mm of upper crowding and 6 mm of lower crowding. The upper dental midline was 3 mm to the left of the mandibular dental midline and the facial midline. There was normal upper incisor inclination with retroclined lower incisors and lingually tipped lower buccal segments. The upper left central incisor was slightly wider (0.75 mm) than the upper right central incisor. The cephalometric tracing revealed a Class II relationship (ANB 5°) and a mesofacial pattern (Sn-Go-Gn 28.5°) (Figure 15). Comparison of the initial cephalometric tracing to the phase II tracing revealed minimal dental change but significant facial growth (Figure 16).
Figures 11–14.
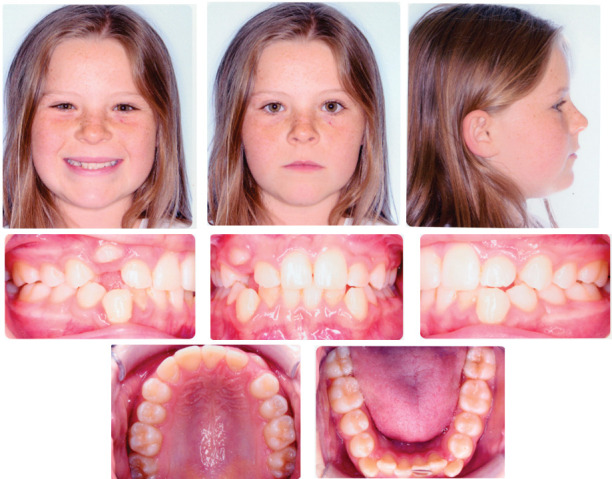
Phase II records.
Figures 11–14.

Phase II records. Continued.
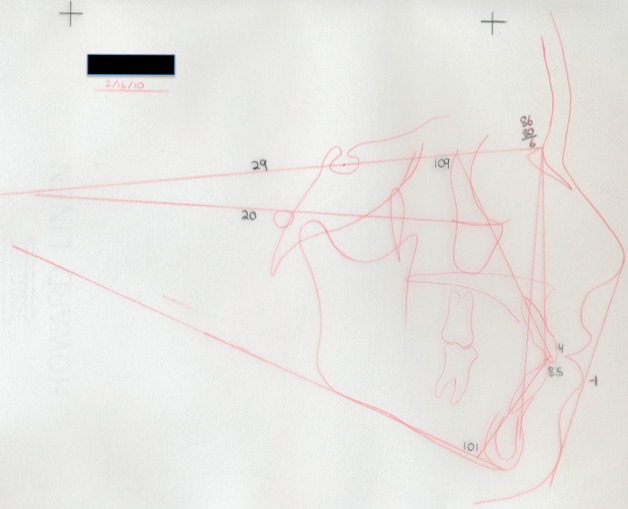
Figure 15.
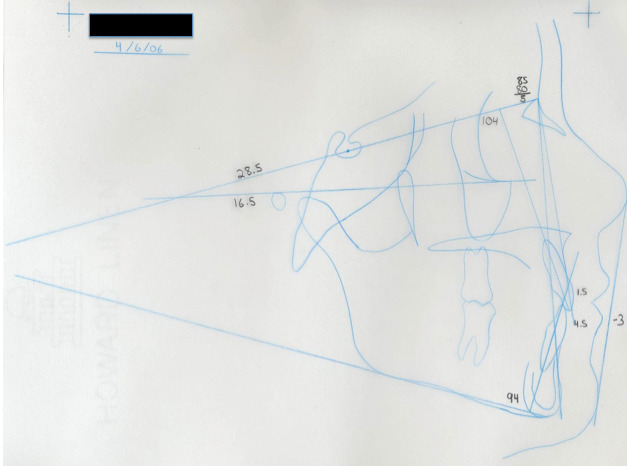
Phase II cephalometric tracing.
Figure 16.
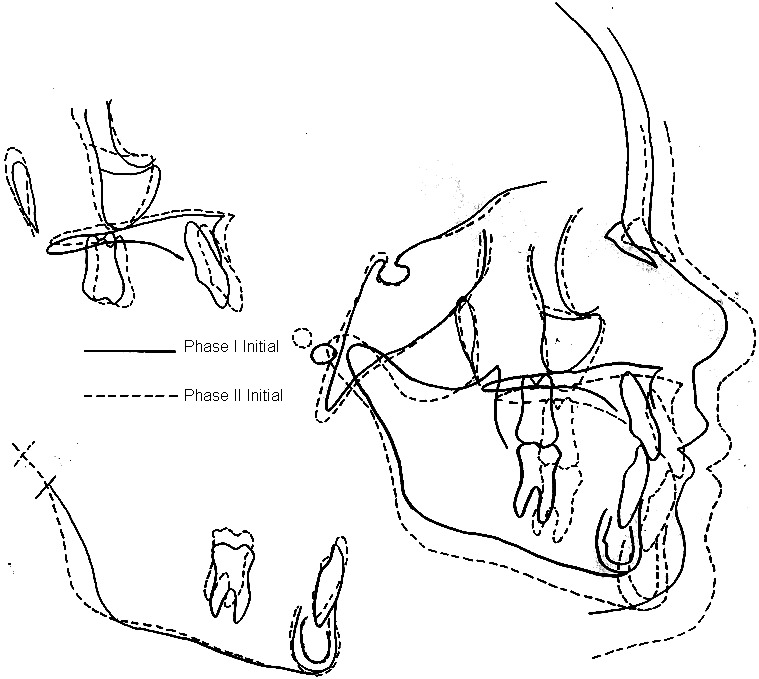
Superimposition of the phase I and phase II tracings.
Figures 11–14.
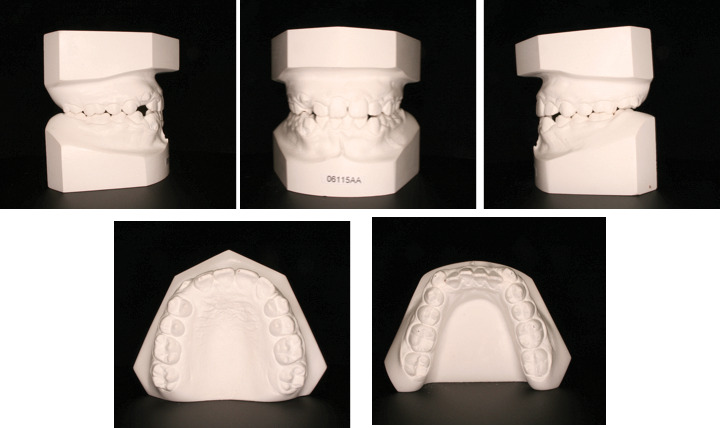
Phase II records. Continued.
Figures 11–14.

Phase II records. Continued.
Treatment
Consideration was given to premolar extractions because of the severity of the crowding and the midline discrepancy. However, after evaluation of the lip profile, a nonextraction treatment plan was offered. We would re-evaluate the midlines and the dental protrusion after alignment; if the profile was too protrusive, or if the midline discrepancy was still a problem, then a premolar extraction plan would be followed.
The upper teeth were bonded with 0.022-inch Damon2 self-ligating brackets in June 2006. An opening nickel-titanium coil spring was placed in the upper left canine area in July 2006, and it was increased in size slowly until May 2007, when a closed coil was used to maintain the space. In July 2007 lower brackets were placed, along with a bracket on the upper left canine. A progress panoramic radiograph was taken in February 2008, and in March 2008 the lower second molars were bonded and some brackets re-positioned. In December 2008, and again in January and April 2009, some interproximal reduction (IPR) was done on the lower incisors to provide space for uprighting them and to manage a slight Bolton maxillary excess. The occlusion was detailed throughout 2009 until the braces were removed in February 2010. A TruTain retainer and a Hawley retainer were delivered within a week and a lower lingual 3-3 retainer was bonded.
Result
Final records were taken on February 16, 2010 (Figures 17 through 22). A Class I occlusion with ideal overjet/overbite and coincident dental midlines was attained after phase II. During phase II, the maxillary incisors experienced labial crown torque and palatal root torque. The mandibular incisors proclined, as planned, during phase II (Figure 23). The maxillary intermolar width increased 3 mm and the distance between the maxillary first premolars increased 3 mm. The mandibular intermolar width increased 2 mm, while the mandibular intercanine width decreased by 4 mm. This decrease in intercanine width was expected due to the initial labial eruption of the lower incisors. Lip profile in repose and smile improved significantly during phase II.
Figures 17–22.

Final records.
Figures 17–22.
Final records. Continued.
Figure 23.
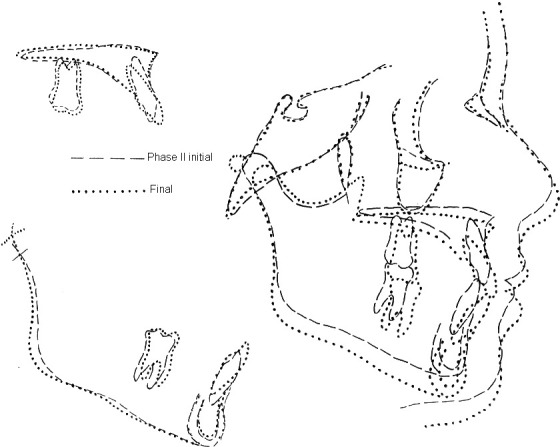
Superimposition of the phase II and final cephalometric tracings.
Figures 17–22.
Final records. Continued.
Figures 17–22.

Final records. Continued.
Figures 17–22.

Final records. Continued.
Figures 17–22.

Final records. Continued.
DISCUSSION
This patient presented with a challenging clinical situation. The case demonstrates that incisors can be moved across the midpalatal suture without dire root resorption problems. The final maxillary occlusal radiograph reveals that the midpalatal suture deviated toward the direction of incisor movement. It is difficult to differentiate between the periodontal ligament of #9 and the midpalatal suture. The final panoramic radiograph revealed some tip resorption to #10, which was likely caused by both the close proximity of the developing #11 and the labial root torque delivered during detailing. The final panoramic radiograph also demonstrates a significant distal root tip to #9a, which should have been addressed during detailing. Despite the crown size difference between #9 and #9a (the “central” incisors in this case), there is no need for postorthodontic restorative work. The final models demonstrate excessive overjet on the distal of the lateral incisors. The smile would be more pleasing with increased incisal display. If more effort had been placed into extrusion of the upper anterior teeth, this could have been improved. The use of a lower lingual holding arch during phase I may have minimized the later need for interproximal reduction (IPR) of the lower incisors.
Movement of a maxillary central incisor across the midline offers a unique challenge for the orthodontist. This case report, along with others, demonstrates that movement across the midline is stable, with minimal to no long-term negative consequences to the treated tooth (root resorption or bone loss).
REFERENCES
- 1.Goaz P, White S. Oral Radiology 2nd ed. Vol. 431 St Louis, MO: Mosby; 1987. [Google Scholar]
- 2.Altug-Atac A, Erdem D. Prevalence and distribution of dental anomalies in orthodontic patients. Am J Orthod Dentofacial Orthop. 2007;131:510–514. doi: 10.1016/j.ajodo.2005.06.027. [DOI] [PubMed] [Google Scholar]
- 3.Cookson A. M. Movement of an upper central incisor across the midline. Br J Orthod. 1981;8:59–60. doi: 10.1179/bjo.8.2.59. [DOI] [PubMed] [Google Scholar]
- 4.Follin M. Orthodontic movement of maxillary incisor into the midline. Swed Dent. 1985;9:9–13. [PubMed] [Google Scholar]
- 5.Follin M, Ericsson I, Thilander B. Orthodontic movement of maxillary incisors through the midpalatal suture area – an experimental study in dogs. Eur J Orthod. 1984;6:237–246. doi: 10.1093/ejo/6.4.237. [DOI] [PubMed] [Google Scholar]
- 6.Follin M, Ericsson I, Thilander B. Orthodontic tooth movement through the midpalatal suture area after surgical removal of the suture. An experimental study in dogs. Eur J Orthod. 1985;7:17–24. doi: 10.1093/ejo/7.1.17. [DOI] [PubMed] [Google Scholar]
- 7.McCollum A. Crossing the midline: a long-term case report. Am J Orthod Dentofacial Orthop. 1999;115:559–562. doi: 10.1016/s0889-5406(99)70280-5. [DOI] [PubMed] [Google Scholar]
- 8.Melnik A. Orthodontic movement of a supplemental maxillary incisor through the midpalatal suture area. Am J Orthod Dentofacial Orthop. 1993;104:85–90. doi: 10.1016/S0889-5406(08)80121-7. [DOI] [PubMed] [Google Scholar]