

Abstract
Background
Cardiac arrest after cardiac surgery commonly has a reversible cause, where emergency resternotomy is often required for treatment, as recommended by international guidelines. We have developed a virtual reality (VR) simulation for training of cardiopulmonary resuscitation (CPR) and emergency resternotomy procedures after cardiac surgery, the Cardiopulmonary Resuscitation Virtual Reality Simulator (CPVR-sim). Two fictive clinical scenarios were used: one case of pulseless electrical activity (PEA) and a combined case of PEA and ventricular fibrillation. In this prospective study, we researched the face validity and content validity of the CPVR-sim.
Objective
We designed a prospective study to assess the feasibility and to establish the face and content validity of two clinical scenarios (shockable and nonshockable cardiac arrest) of the CPVR-sim partly divided into a group of novices and experts in performing CPR and emergency resternotomies in patients after cardiac surgery.
Methods
Clinicians (staff cardiothoracic surgeons, physicians, surgical residents, nurse practitioners, and medical students) participated in this study and performed two different scenarios, either PEA or combined PEA and ventricular fibrillation. All participants (N=41) performed a simulation and completed the questionnaire rating the simulator’s usefulness, satisfaction, ease of use, effectiveness, and immersiveness to assess face validity and content validity.
Results
Responses toward face validity and content validity were predominantly positive in both groups. Most participants in the PEA scenario (n=26, 87%) felt actively involved in the simulation, and 23 (77%) participants felt in charge of the situation. The participants thought it was easy to learn how to interact with the software (n=24, 80%) and thought that the software responded adequately (n=21, 70%). All 15 (100%) expert participants preferred VR training as an addition to conventional training. Moreover, 13 (87%) of the expert participants would recommend VR training to other colleagues, and 14 (93%) of the expert participants thought the CPVR-sim was a useful method to train for infrequent post–cardiac surgery emergencies requiring CPR. Additionally, 10 (91%) of the participants thought it was easy to move in the VR environment, and that the CPVR-sim responded adequately in this scenario.
Conclusions
We developed a proof-of-concept VR simulation for CPR training with two scenarios of a patient after cardiac surgery, which participants found was immersive and useful. By proving the face validity and content validity of the CPVR-sim, we present the first step toward a cardiothoracic surgery VR training platform.
Keywords: cardiac surgery, cardiopulmonary resuscitation, emergency resternotomy, virtual reality, simulation training, serious games, virtual reality simulation, digital health, medical training, virtual training
Introduction
Every year, around 2 million patients undergo cardiac surgery worldwide [1]. The incidence of cardiac arrest after cardiac surgery ranges between 0.7% to 8%, with a survival rate of approximately 50% [2-5]. This relatively high survival rate can be explained by a high incidence of reversible causes precipitating the arrest, such as ventricular fibrillation (VF; 25%-50%), cardiac tamponade, hypovolemia, and tension pneumothorax [2,4-6]. Notably, aside from VF, external massage is often ineffective in these cases because of reduced diastolic filling of the heart, resulting in inadequate tissue and brain perfusion [2]. In light of these findings, the Society of Thoracic Surgeons Taskforce on Resuscitation After Cardiac Surgery published an expert consensus in 2017 to provide guidelines for developing local protocols for cardiopulmonary resuscitation (CPR) after cardiac surgery [2]. As reported in the guidelines, early recognition of the clinical signs and symptoms is essential, indicating that emergency resternotomy is required [2,5]. The majority of postoperative cardiac surgery emergencies requiring CPR will involve reopening the sternum [2,5]. Several studies have shown that training and practicing based on a structured protocol improve the time to recognize the need for resternotomy and the time to reopen the thorax [2,7]. Early resternotomy reduces complications and improves outcomes for patients with cardiac tamponade, hypovolemia, or tension pneumothorax [2,7]. However, the paucity of cardiac arrest after cardiac surgery limits the possibilities of clinical training for clinicians [8]. CPR training allows clinical staff to acquire theoretical knowledge on the protocol, together with the ability to physically perform the steps described within the protocol [9]. This is commonly taught in instructor-led training sessions, requiring multiple team members and resources [2]. Moreover, these classroom sessions are currently restricted due to precautionary measures taken during the COVID-19 pandemic [10].
Simulation training enables training of multiple cases with unlimited practice (and possible errors) without compromising patient safety or the need for setting up training sessions [8]. Virtual reality (VR), with 360-degree scenarios, can recreate a fully immersive, interactive, and realistic scenario in which the user can repeatedly train without the need for other supplies or participants. Moreover, VR can be used in a multiuser setting, allowing different users to be present in the same scenario while physically distanced [11]. Multiple studies have shown that simulation training effectively improves knowledge, confidence, motivation, and satisfaction with the training versus standard training methodology [8,9,12,13].
Quantifying outcomes and the validity of simulations is a difficult task. It is essential that a VR simulator is valid in the sense that it resembles a realistic situation and reinforces the appropriate skills and knowledge [14]. This validity consists of several subtypes, including face validity and content validity. Face validity relates to the realism of a simulator, or in this case how well the simulation resembles real-world clinical practice [14,15]. This can be assessed informally by experts (referents) and nonexperts (novices/trainees) in the field [16-19]. Content validity judges the usefulness of the simulator as a training method that may be assessed by an evaluation of experts in the subject matter of the training [14-16,20]. The implementation of a new protocol and limited incidence of emergency resternotomies after cardiac surgery highlight the need to develop a high-fidelity training method that follows the expert consensus protocol for CPR and resternotomy for patients after cardiac surgery [2]. To facilitate medical staff training at our cardiothoracic surgery (CTS) department, we have developed a dedicated VR-based postcardiac surgery CPR simulation: Cardiopulmonary Resuscitation Virtual Reality Simulator (CPVR-sim). We designed a prospective study to assess the feasibility and to establish the face and content validity of CPVR-sim in a group of novices (eg, surgical residents, junior physicians, and nurse practitioners) and experts (eg, cardiothoracic surgeons and senior residents).
Methods
Simulator
The simulation was designed by a multidisciplinary team consisting of physicians, researchers, software developers, digital transformation experts, VR experts, and cardiothoracic surgeons from the CTS departments at Erasmus Medical Center (Rotterdam, the Netherlands), Zan Mitrev Clinic (Skopje, Republic of North Macedonia), and Distant Point LTD (Skopje, Republic of North Macedonia). Unreal Engine (Epic Games, Cary, North Carolina) software was used for software development. An Oculus Quest 2 (Oculus, Irvine, California) head-mounted display (HMD), in combination with two VR controllers and a high-performance laptop (MSI, New Taipei City, Taiwan), was used to run the CPVR-sim.
To study the feasibility of the CPVR-sim, we developed an immersive VR simulation resembling two CPR scenarios (both shockable and nonshockable cardiac arrest scenarios) after cardiac surgery, based on fictive patient cases (Multimedia Appendix 1). The patient scenarios recreated in the simulation were patients a few days after cardiac surgery through median sternotomy. These patients were found to be unresponsive on the surgical ward and determined to be in cardiac arrest and requiring CPR. In the first scenario, the cardiac arrest was caused by cardiac tamponade leading to pulseless electrical activity (PEA) where a resternotomy had to be performed to obtain the return of spontaneous circulation. The second scenario combined PEA and VF, and participants had to perform multiple actions, including external defibrillation, resternotomy, internal defibrillation, internal heart massage, and intracardiac medication administration.
Before running the simulation, each participant was given a short briefing on the scenario, how to use the VR HMD, and how to interact with the controls and software to perform the CPVR-sim. When the simulation started, the user of the CPVR-sim was placed as a team leader of the CPR team. The team leader was able to assign tasks to the other participants in the simulation or was able to execute several tasks themself to manage the cardiac arrest situation. Figure 1 shows multiple screen captures of the team leader’s view during the simulation. The team leader instructed the virtual colleagues by choosing between different menu options (Figure 1B) with the joystick on the controller. Additionally, a participant wearing the HMD and performing the simulation is shown (Figure 1D). The menu options were shuffled each time the simulation started, so the user did not know the order of the menu options beforehand. When the correct command was given, it was followed by visual and auditory feedback of the instruction. This means, for example, that when “Start Chest Compressions” was chosen at the correct moment, the virtual nurse confirmed the instruction and started chest compressions.
Figure 1.

Screen captures of the Cardiopulmonary Resuscitation Virtual Reality Simulator (CPVR-sim) showing an overview with five virtual nurses in a patient room (A), the main menu (B), opening the incision with a virtual scalpel (C), performing the internal defibrillation (D), and a participant performing the simulation wearing the head-mounted display, with an in-screen screen capture of the CPVR-sim (E).
Study Participants
All participants work at the Erasmus MC in the Cardiothoracic Surgery Department as staff cardiothoracic surgeon, physician (including trainees in CTS), nurse practitioner, or medical student. To assess the content validity of the PEA scenario, participants were assigned to the novice or expert group. Staff cardiothoracic surgeons and certified CPR training instructors were categorized as expert, while the remaining participants were classed as novices (eg, junior physicians, nurse practitioners, surgical residents, and medical students). All participants completed written consent forms for their participation in this study. The research protocol was approved by the Erasmus Medical Center Medical Ethical Review Committee (MEC-2020-0989).
Questionnaire
To assess participant characteristics, face validity, and content validity, a questionnaire was developed, which included experience with emergency resternotomy, gaming, and VR, among other things. Subsequent questions were scored on a five-point Likert scale, ranging from 1 (fully disagree) to 5 (fully agree). The Likert scale questions were divided into the following categories: usefulness, satisfaction, ease of use [21], effectiveness, and immersiveness [12,22-24], as described in previous studies. Finally, the last part of the questionnaire consisted of open questions to assess the advantages and disadvantages of the simulation. The questionnaire can be found in File S1 in Multimedia Appendix 2. To determine face validity, we used questionnaire results on the ease of use, effectiveness, and immersiveness of all participants. To assess content validity, we looked at the results from the expert group that performed the PEA scenario regarding usefulness and satisfaction.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp). The chi-square test was used to perform statistical analyses of categorical data such as the participant characteristics. Continuous data are presented as medians with IQRs, and categorical data, including Likert scales, are presented as percentages.
Results
Participant Characteristics
All 41 participants performed the simulation and completed the questionnaire. Participants were divided into an expert and novice group to assess content and face validity of the PEA scenario. A total of 15 experts (staff cardiothoracic surgeons and certified CPR instructors) and 15 novices (physicians, residents, nurse practitioners, and medical students) were included in the PEA scenario. The median age of the expert group was 43 (IQR 38-55.5) years and of the novice group 30 (IQR 30-42.5) years (P<.001). Furthermore, the median work experience in CTS was 17 (IQR 9.5-26.5) years in the expert group and 1 (IQR 0.5-4.5) year in the novice group (P<.001). The participant characteristics are shown in Table 1.
Table 1.
Participant characteristics.
| Characteristic | PEAa scenario, n (%) | Combined scenario (PEA + VFb), n (%) | Total (n=41), n (%) | ||
|
|
Experts (n=15) | Novices (n=15) | Experts + novices (n=11) |
|
|
| Sex | |||||
|
|
Male | 12 (80) | 10 (67) | 5 (45) | 27 (66) |
|
|
Female | 3 (20) | 5 (33) | 6 (55) | 14 (34) |
| Profession | |||||
|
|
Cardiothoracic surgeon | 13 (87) | 1 (7) | 0 (0) | 14 (34) |
|
|
CTSc resident | 1 (7) | 4 (27) | 0 (0) | 5 (12) |
|
|
CTS junior physician | 0 (0) | 6 (40) | 6 (55) | 12 (29) |
|
|
CTS nurse practitioner | 1 (7) | 4 (27) | 1 (9) | 6 (15) |
|
|
CTS medical student | 0 (0) | 0 (0) | 4 (36) | 4 (10) |
| Experience with post–cardiac surgery CPRd | |||||
|
|
No experience | 0 (0) | 1 (7) | 5 (45) | 6 (15) |
|
|
1-5 times | 1 (7) | 8 (53) | 4 (36) | 13 (32) |
|
|
6-10 times | 1 (7) | 4 (27) | 1 (9) | 6 (15) |
|
|
>10 times | 13 (87) | 2 (13) | 1 (9) | 16 (39) |
| Experience with emergency resternotomy | |||||
|
|
No experience | 0 (0) | 5 (33) | 6 (55) | 11 (27) |
|
|
1-5 times | 4 (27) | 9 (60) | 4 (36) | 17 (41) |
|
|
6-10 times | 1 (7) | 1 (7) | 1 (9) | 3 (7) |
|
|
>10 times | 10 (67) | 0 (0) | 0 (0) | 10 (24) |
| Experience with gaming console | |||||
|
|
Never used a gaming console | 2 (13) | 2 (13) | 1 (9) | 5 (12) |
|
|
Few times before | 12 (80) | 10 (67) | 7 (64) | 29 (71) |
|
|
Regular basis | 1 (7) | 3 (20) | 3 (27) | 7 (17) |
| Experience with VRe | |||||
|
|
Never had a VR experience | 4 (27) | 5 (33) | 4 (36) | 13 (32) |
|
|
Few times before | 8 (53) | 7 (47) | 7 (64) | 22 (54) |
|
|
Regular basis | 3 (20) | 2 (13) | 0 (0) | 5 (12) |
|
|
VR expert | 0 (0) | 1 (7) | 0 (0) | 1 (2) |
| Experience with simulation training | |||||
|
|
Never had simulation training | 5 (33) | 1 (7) | 1 (9) | 7 (17) |
|
|
Multiple times | 8 (53) | 14 (93) | 9 (82) | 31 (76) |
|
|
Certified trainer | 2 (13) | 0 (0) | 1 (9) | 3 (7) |
| Experience with digital training | |||||
|
|
Never had digital training | 5 (33) | 7 (47) | 2 (18) | 14 (34) |
|
|
Few times before | 8 (53) | 5 (33) | 5 (45) | 18 (44) |
|
|
Multiple times before | 2 (13) | 3 (20) | 4 (36) | 9 (22) |
aPEA: pulseless electrical activity.
bVF: ventricular fibrillation.
cCTS: cardiothoracic surgery.
dCPR: cardiopulmonary resuscitation.
eVR: virtual reality.
Questionnaires
The face validity of both scenarios was assessed separately by analyzing the ease of use, effectiveness, and immersiveness questions in the questionnaires. The results of the PEA scenario are displayed in Figure 2. Most participants in the PEA scenario (n=26, 87%) felt actively involved, and 23 (77%) participants felt in charge of the situation, suggesting a predominant positive opinion regarding the face validity in both groups. The simulation software responded adequately and did not lag according to 21 (70%) of the participants, and 24 (80%) of the participants reported that it was easy to learn how to interact with the software. Notably, 12 (80%) of the novices in the PEA scenario said they learned a lot from the simulation, whereas only 7 (47%) experts reported the same. The results of the combined scenario are displayed in Figure 3. Additionally, 10 (91%) of the participants stated that it was easy to move around in the VR environment, and the same amount of people reported that the controller buttons responded adequately.
Figure 2.
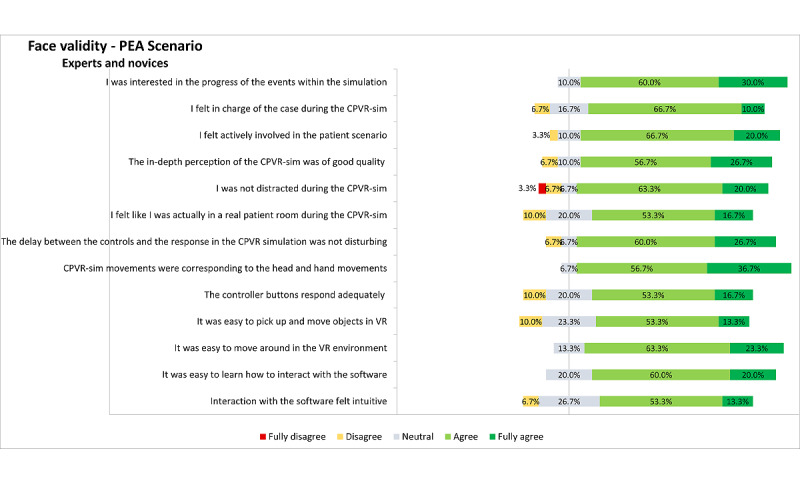
Representation of the results on face validity–related questionnaires assessed from all (expert and novice) participants on the PEA scenario. Inconsistencies in the sum of percentages is due to the rounding of the percentages. CPVR-sim: Cardiopulmonary Resuscitation Virtual Reality Simulator; PEA: pulseless electrical activity; VR: virtual reality.
Figure 3.
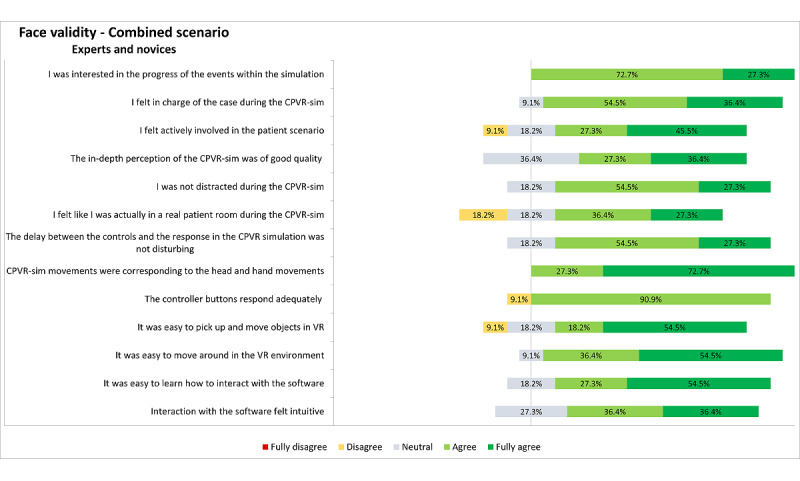
Representation of the results on face validity–related questionnaires assessed from all (expert and novice) participants on the combined scenario. Inconsistencies in the sum of percentages is due to the rounding of the percentages. CPVR-sim: Cardiopulmonary Resuscitation Virtual Reality Simulator; VR: virtual reality.
Subsequently, the content validity was assessed by analyzing the satisfaction and usefulness outcomes of the questionnaire of the expert group (n=15) who performed the PEA scenario (Figure 4).
Figure 4.
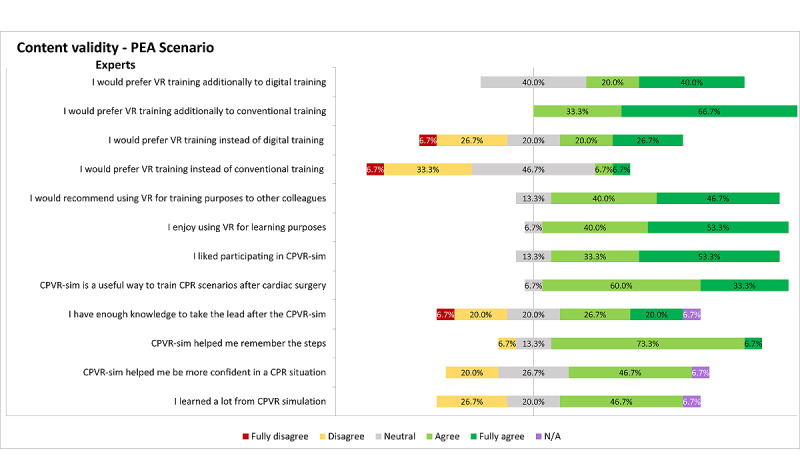
Representation of the results on content validity–based questionnaires of the PEA scenario, assessed from the expert participants. Inconsistencies in the sum of percentages is due to the rounding of the percentages. CPR: cardiopulmonary resuscitation; CPVR-sim: Cardiopulmonary Resuscitation Virtual Reality Simulator; N/A: not applicable; PEA: pulseless electrical activity; VR: virtual reality.
All expert participants in the PEA scenario (n=15, 100%) agreed that this VR training method is useful as a supplement to conventional training methods, and 9 (60%) participants agreed it was useful as a supplement to digital training. Notably, only 2 (14%) expert participants would prefer VR training instead of conventional training; however, 7 (47%) expert participants would prefer VR training instead of digital training. Conversely, 13 of 15 (87%) expert participants would recommend VR training to other colleagues, and most participants (n=14, 93%) reported that the CPVR-sim was a useful method to train infrequently occurring CPR cases after cardiac surgery (File S2 in Multimedia Appendix 2).
Finally, participants were asked for general advantages and disadvantages of the CPVR-sim. The most commonly reported advantages were the broad applicability of VR simulation in various CPR scenarios; the possibility of repetitive, personal, and quick practice sessions without being restricted by logistical challenges; and that the CPVR-sim is a beneficial method for step-by-step sequence training. Additionally, many participants felt it was a fun way of learning. The most important disadvantages of the current CPVR-sim version were the limited freedom of decision-making, lack of team training and interaction with a team, and the absence in the CPVR-sim of the pressure and hectic environment during such an emergency situation, which occasionally made it feel artificial. Results of the face and content validity questionnaire can be found in File S2 in Multimedia Appendix 2, and a complete overview of the advantages and disadvantages filled in by the participants can be found in File S3 in Multimedia Appendix 2.
Discussion
Principal Results
In this prospective study, we have designed and evaluated a VR simulation training platform with two different scenarios for post–cardiac surgery emergencies requiring CPR. To the best of our knowledge, this is the first time that such a VR simulation platform has been developed explicitly for use in a cardiac arrest scenario after cardiac surgery. Although future refinements of this concept are inevitable, we believe that the CPVR-sim will be a successful method that will help to overcome difficult challenges, including the infrequent incidence of resternotomy after cardiac surgery, accessibility, and costs of clinical training [25]. We observed that the expert and novice opinions were generally positive regarding the face validity and content validity. A significant majority of participants from both groups felt that VR simulations are a useful (supplementary) training method, as well as a high likelihood that they would recommend VR simulation training to other colleagues. Furthermore, in the CPVR-sim scenarios, the trainee was more actively involved in experiencing the virtual patient case, as compared with conventional digital training, listening to a presentation, or reading a protocol. This active involvement could be due to the elaborate simulation and multiple actions the user has to perform. This immersive and realistic VR environment facilitates memorizing stepwise procedures more efficiently [25]. Additionally, our results showed that frequent practice and increased exposure in the CPVR-sim is valuable since it refreshes the knowledge and gives the clinician more confidence in taking the lead in future situations, which is in line with previous studies [8,9,12,13]. This is especially important in infrequent CPR cases with emergency resternotomy, which occurs only a few times per year.
Another important feature of this VR training is the improved accessibility since the only requirements are an HMD and a computer, and there is no need to arrange a physical session. VR training has higher initial costs (eg, simulation development and purchase costs of the VR hardware) than conventional training. However, the increased accessibility of VR training results in more trainees being reached, spreading these initial costs over a larger group, compared with the relatively linear cost per trainee for conventional training. Therefore, the average cost per trainee would likely be lower in the long term for VR training than conventional training [26]. Moreover, purchasing and using VR hardware adds a new dimension and armature in training possibilities and other applications (ie, surgical planning) of a department, which can also lead to cost-efficiency. Finally, VR training facilitates the implementation of the new CPR protocol, enabling training for experts and novices alike who are not yet acquainted with the new protocol.
Limitations
In this simulation, only individual training was possible. It would be desirable to make the simulation available for multiple users at a time, enabling real-time interaction between team members [11]. By making the simulation available for multiple users at the same time, nontechnical skills such as communication and leadership can be trained with the team, which is important in CPR situations [27]. This would also enable learning from other trainees’ mistakes. Multiplayer settings would additionally enable the trainee to view the CPR situation from different viewpoints and the possibility to review their own performance from an alternative perspective [25]. Another shortcoming of the CPVR-sim is that the simulation requires at least five different buttons to be pressed, which can be confusing for the trainee. The simulation would become more realistic and interactive when voice controls and haptic feedback such as hand or even body tracking are implemented to perform the actions within the simulation, instead of using the controllers as input in the simulation [28]. However, implementing voice control can be computationally and algorithmically challenging, as similar information can be said using a variety of different phraseology, and further research should be performed on the best interaction method within the VR environment [25-28].
Finally, a shortcoming in this simulation was the lack of pressure felt by participants and the absence of a hectic environment, characteristic of such an emergency situation. The virtual nurses stood still and walked calmly, and there was a lack of background noise. This could be improved in future development by adding stress components such as sounds or extra persons who are panicking [20]. Making the simulation more resembling the real-life situation might improve the success of VR training [25]. However, further research is needed to ensure such stress components do not compromise the educational value of the CPVR-sim.
Future Perspective
The most crucial next step in improving the simulation and increasing educational value is to extend the CPVR-sim with different roles in the CPR simulation, for example, for nurses. With this functionality, multiplayer scenarios will become possible, and a team can train together at the same time, ultimately creating a more realistic environment that will translate more directly into clinical practice. Furthermore, the simulation can be improved by adding more scenarios, asystole, and external pacing, for example.
In this study, we only assessed the content validity of the PEA scenario, but in future studies, the content must be validated for all different scenarios of the CPVR-sim. These face and content validity results support the use of the simulator as a training tool, but they are subjective measures of validity, and it is imperative to validate the simulation objectively. This can be perceived by determining the construct validity, concurrent validity, and predictive validity of the CPVR-sim [14,15,20]. Construct validity in a simulation is defined as the ability to distinguish objectively between different levels of experience [14,15,20]. In future research, this could be determined by testing a large number of users with various levels of experience in CPR and emergency resternotomy cases after cardiac surgery. Concurrent validity can determine the correlation between the VR simulation and existing evaluation tools [15,20]. Moreover, predictive validity is an even more powerful evidence method, which can be assessed by comparing the outcomes of the simulation with an established assessment method to assess the skills [15,20]. In further research, predictive validity could be determined by comparing the clinical staff’s skills in a real-life simulation setting and CPVR-sim. These skills could be obtained by a structured skills assessment of both the skills in real life and within the VR simulation, determined by blinded experienced CPR trainers.
Conclusion
We have developed a proof-of-concept VR simulation of two CPR scenarios after cardiac surgery, which is immersive and useful, as stated by the expert and novice participants. Additional research is needed to further develop and validate the simulation platform, including multiple possible clinical scenarios; voice control; multiuser possibilities; and assessing the construct, concurrent, and predictive validity. However, we made a first step toward a CTS VR training platform, including multiple realistic and repetitive simulation training for the CTS department by proving the face validity and content validity of the CPVR-sim.
Acknowledgments
We would like to thank Aleksandar Trifunovski, Ivo Matevski, Tomi Jurukovski, and Kristina Kerkez for their collaboration and development of the Cardiopulmonary Resuscitation Virtual Reality Simulator software. Finally, we would like to thank all participants for their time and effort to participate in this study.
Abbreviations
- CPR
cardiopulmonary resuscitation
- CPVR-sim
Cardiopulmonary Resuscitation Virtual Reality Simulator
- CTS
cardiothoracic surgery
- HMD
head-mounted display
- PEA
pulseless electrical activity
- VF
ventricular fibrillation
- VR
virtual reality
Supplementary video of the cardiopulmonary resuscitation virtual reality simulator.
Supplementary file.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Parikh CR, Coca SG, Thiessen-Philbrook H, Shlipak MG, Koyner JL, Wang Z, Edelstein CL, Devarajan P, Patel UD, Zappitelli M, Krawczeski CD, Passik CS, Swaminathan M, Garg AX, TRIBE-AKI Consortium Postoperative biomarkers predict acute kidney injury and poor outcomes after adult cardiac surgery. J Am Soc Nephrol. 2011 Sep;22(9):1748–57. doi: 10.1681/ASN.2010121302. https://jasn.asnjournals.org/cgi/pmidlookup?view=long&pmid=21836143 .ASN.2010121302 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Society of Thoracic Surgeons Task Force on Resuscitation After Cardiac Surgery The Society of Thoracic Surgeons expert consensus for the resuscitation of patients who arrest after cardiac surgery. Ann Thorac Surg. 2017 Mar;103(3):1005–1020. doi: 10.1016/j.athoracsur.2016.10.033.S0003-4975(16)31482-5 [DOI] [PubMed] [Google Scholar]
- 3.Wahba A, Götz W, Birnbaum DE. Outcome of cardiopulmonary resuscitation following open heart surgery. Scand Cardiovasc J. 1997;31(3):147–9. doi: 10.3109/14017439709058084. [DOI] [PubMed] [Google Scholar]
- 4.Truhlář A, Deakin CD, Soar J, Khalifa GEA, Alfonzo A, Bierens JJLM, Brattebø G, Brugger H, Dunning J, Hunyadi-Antičević S, Koster RW, Lockey DJ, Lott C, Paal P, Perkins GD, Sandroni C, Thies KC, Zideman DA, Nolan JP, Cardiac arrest in special circumstances section Collaborators European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation. 2015 Oct;95:148–201. doi: 10.1016/j.resuscitation.2015.07.017.S0300-9572(15)00329-9 [DOI] [PubMed] [Google Scholar]
- 5.Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, Kudenchuk PJ, Kurz MC, Lavonas EJ, Morley PT, O'Neil BJ, Peberdy MA, Rittenberger JC, Rodriguez AJ, Sawyer KN, Berg KM, Adult Basic and Advanced Life Support Writing Group Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020 Oct 20;142(16_suppl_2):S366–S468. doi: 10.1161/CIR.0000000000000916. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000000916?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PubMed] [Google Scholar]
- 6.Brand J, McDonald A, Dunning J. Management of cardiac arrest following cardiac surgery. BJA Educ. 2018 Jan;18(1):16–22. doi: 10.1016/j.bjae.2017.11.002. https://linkinghub.elsevier.com/retrieve/pii/S2058-5349(17)30182-8 .S2058-5349(17)30182-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dunning J, Nandi J, Ariffin S, Jerstice J, Danitsch D, Levine A. The Cardiac Surgery Advanced Life Support Course (CALS): delivering significant improvements in emergency cardiothoracic care. Ann Thorac Surg. 2006 May;81(5):1767–72. doi: 10.1016/j.athoracsur.2005.12.012.S0003-4975(05)02172-7 [DOI] [PubMed] [Google Scholar]
- 8.Mundell WC, Kennedy CC, Szostek JH, Cook DA. Simulation technology for resuscitation training: a systematic review and meta-analysis. Resuscitation. 2013 Sep;84(9):1174–83. doi: 10.1016/j.resuscitation.2013.04.016.S0300-9572(13)00246-3 [DOI] [PubMed] [Google Scholar]
- 9.Barsom EZ, Duijm RD, Dusseljee-Peute LWP, Landman-van der Boom EB, Lieshout EJ, Jaspers MW, Schijven MP. Cardiopulmonary resuscitation training for high school students using an immersive 360‐degree virtual reality environment. Br J Educ Technol. 2020 Sep 07;51(6):2050–2062. doi: 10.1111/bjet.13025. [DOI] [Google Scholar]
- 10.Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020 Mar 19;91(1):157–160. doi: 10.23750/abm.v91i1.9397. http://europepmc.org/abstract/MED/32191675 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Triandafilou KM, Tsoupikova D, Barry AJ, Thielbar KN, Stoykov N, Kamper DG. Development of a 3D, networked multi-user virtual reality environment for home therapy after stroke. J Neuroeng Rehabil. 2018 Oct 05;15(1):88. doi: 10.1186/s12984-018-0429-0. https://jneuroengrehab.biomedcentral.com/articles/10.1186/s12984-018-0429-0 .10.1186/s12984-018-0429-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dankbaar MEW, Richters O, Kalkman CJ, Prins G, Ten Cate OTJ, van Merrienboer JJG, Schuit SCE. Comparative effectiveness of a serious game and an e-module to support patient safety knowledge and awareness. BMC Med Educ. 2017 Feb 02;17(1):30. doi: 10.1186/s12909-016-0836-5. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-016-0836-5 .10.1186/s12909-016-0836-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aksoy E. Comparing the effects on learning outcomes of tablet-based and virtual reality-based serious gaming modules for basic life support training: randomized trial. JMIR Serious Games. 2019 May 01;7(2):e13442. doi: 10.2196/13442. https://games.jmir.org/2019/2/e13442/ v7i2e13442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brewin J, Nedas T, Challacombe B, Elhage O, Keisu J, Dasgupta P. Face, content and construct validation of the first virtual reality laparoscopic nephrectomy simulator. BJU Int. 2010 Sep;106(6):850–4. doi: 10.1111/j.1464-410X.2009.09193.x.BJU9193 [DOI] [PubMed] [Google Scholar]
- 15.Carter FJ, Schijven MP, Aggarwal R, Grantcharov T, Francis NK, Hanna GB, Jakimowicz JJ, Work Group for Evaluation and Implementation of Simulators and Skills Training Programmes Consensus guidelines for validation of virtual reality surgical simulators. Surg Endosc. 2005 Dec;19(12):1523–32. doi: 10.1007/s00464-005-0384-2. [DOI] [PubMed] [Google Scholar]
- 16.Graafland M, Dankbaar M, Mert A, Lagro J, De Wit-Zuurendonk L, Schuit S, Schaafstal A, Schijven M. How to systematically assess serious games applied to health care. JMIR Serious Games. 2014 Nov 11;2(2):e11. doi: 10.2196/games.3825. https://games.jmir.org/2014/2/e11/ v2i2e11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McDougall EM. Validation of surgical simulators. J Endourol. 2007 Mar;21(3):244–7. doi: 10.1089/end.2007.9985. [DOI] [PubMed] [Google Scholar]
- 18.Okoro T, Sirianni C, Brigden D. The concept of surgical assessment: part 3 – characteristics of the ideal assessment tool. Bulletin. 2010 Oct 01;92(9):1–2. doi: 10.1308/147363510x527718. [DOI] [Google Scholar]
- 19.Schreuder HW, van Dongen KW, Roeleveld SJ, Schijven MP, Broeders IA. Face and construct validity of virtual reality simulation of laparoscopic gynecologic surgery. Am J Obstet Gynecol. 2009 May;200(5):540.e1–8. doi: 10.1016/j.ajog.2008.12.030.S0002-9378(08)02436-8 [DOI] [PubMed] [Google Scholar]
- 20.Pantelidis P, Chorti A, Papagiouvanni I, Paparoidamis G, Drosos C, Panagiotakopoulos T, Lales G, Sideris M. Virtual and augmented reality in medical education. In: Tsoulfas G, editor. Medical and Surgical Education. London: IntechOpen; 2018. pp. 77–97. [Google Scholar]
- 21.Lund A. Measuring usability with the USE Questionnaire. ResearchGate. 2001. [2020-10-01]. https://www.researchgate.net/publication/230786746_Measuring_Usability_with_the_USE_Questionnaire .
- 22.Jennett C, Cox A, Cairns P, Dhoparee S, Epps A, Tijs T, Walton A. Measuring and defining the experience of immersion in games. Int J Hum Comput Stud. 2008 Sep;66(9):641–661. doi: 10.1016/j.ijhcs.2008.04.004. [DOI] [Google Scholar]
- 23.Dankbaar ME, Roozeboom MB, Oprins EAB, Rutten F, van Merrienboer JJ, van Saase JL, Schuit SC. Preparing residents effectively in emergency skills training with a serious game. Simul Healthc. 2017 Feb;12(1):9–16. doi: 10.1097/SIH.0000000000000194. http://europepmc.org/abstract/MED/27764018 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nichols S, Haldane C, Wilson JR. Measurement of presence and its consequences in virtual environments. Int J Hum Comput Stud. 2000 Mar;52(3):471–491. doi: 10.1006/ijhc.1999.0343. [DOI] [Google Scholar]
- 25.Moore N, Yoo S, Poronnik P, Brown M, Ahmadpour N. Exploring user needs in the development of a virtual reality-based advanced life support training platform: exploratory usability study. JMIR Serious Games. 2020 Aug 07;8(3):e20797. doi: 10.2196/20797. https://games.jmir.org/2020/3/e20797/ v8i3e20797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Farra S, Gneuhs M, Hodgson E, Kawosa B, Miller ET, Simon A, Timm N, Hausfeld J. Comparative cost of virtual reality training and live exercises for training hospital workers for evacuation. Comput Inform Nurs. 2019 Sep;37(9):446–454. doi: 10.1097/CIN.0000000000000540. http://europepmc.org/abstract/MED/31166203 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Andersen PO, Jensen MK, Lippert A, Østergaard D. Identifying non-technical skills and barriers for improvement of teamwork in cardiac arrest teams. Resuscitation. 2010 Jun;81(6):695–702. doi: 10.1016/j.resuscitation.2010.01.024.S0300-9572(10)00073-0 [DOI] [PubMed] [Google Scholar]
- 28.Reznek M, Harter P, Krummel T. Virtual reality and simulation: training the future emergency physician. Acad Emerg Med. 2002 Jan;9(1):78–87. doi: 10.1111/j.1553-2712.2002.tb01172.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=1069-6563&date=2002&volume=9&issue=1&spage=78 . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary video of the cardiopulmonary resuscitation virtual reality simulator.
Supplementary file.