

Abstract
Background
Familial gigantiform cementoma is an autosomal dominant fibro-cement osseous lesion that causes massive expansion of facial skeleton. Patients with such massive lesions have a compromised quality of life. The main goal of treating such patients is to restore and preserve the jaw as far as possible which would enhance their quality of life.
Purpose
This study was conducted to identify the occurrence of gigantiform cementoma which had affected three generations of a family and also to focus on documentation of the clinical course and management.
Method
Patients (one family—mother, grandmother, aunt and grandson) who had visited the Department of Oral and Maxillofacial Surgery, Tamilnadu Government Dental College and Hospital, Chennai, over a period for their swelling in the maxillofacial region were clinically and radiographically evaluated and histopathologically diagnosed as familial gigantiform cementoma; later, they were surgically managed.
Result
It is very rare to document three generations of this disease which had shown varied clinical presentation (asymptomatic slow growth, arrested growth and one case of aggressive growth). Management of these cases varied from observation to aggressive resection.
Conclusion
Gigantiform cementoma follows an autosomal dominant pattern of inheritance with variable phenotypic expression without gender predilection. These cases require regular observation and intervention if necessary.
Keywords: Familial gigantiform cementoma, Autosomal dominant, Alkaline phosphatase, Familial, Radio opacities
Introduction
Cementomas are benign fibro-osseous periodontal tumors categorized into four types: cementoblastoma, cementifying fibroma, periapical cemental dysplasia and gigantiform cementomas [1]. Gigantiform cementoma was first reported in 1930 by Norberg to describe a condition characterized by diffuse radio-opaque masses scattered throughout the jaw. These masses frequently caused massive expansion. Agazzi and Belloni in 1953 described an Italian family in which several family members were affected and it was designated as “familial gigantiform cementoma” [2].
Familial gigantiform cementoma typically presents in the first 2 decades of life. It follows a autosomal dominant pattern of inheritance with variable phenotypic expression without racial or gender predilection [3]. The term gigantiform cementoma typically presents as a slow growing, multifocal/multiquadrant and expansile lesion involving both jaws. Radiographically gigantiform cementoma presents as multiple circumscribed, expansile, mixed radio-opaque radiolucent lesion usually crossing the midline [4].
Histologically it presents with fibroelastic tissue proliferation with varying cellularity with predominant cemental deposits and limited bone formation. In advanced cases, the lesion presents as remarkable painless swelling with marked facial deformity [4].
The goals of treatment are to preserve the jaw and to restore its function, improve or maintain patient’s quality of life and reduce the complications associated with treatment. Management of familial gigantiform cementoma is difficult because of its rapid expansion, widespread involvement and high rate of recurrence. Incomplete removal of the lesion leads to more rapid growth of the residual lesion. Therefore, an extensive resection can prevent recurrence [5].
Herewith, we are reporting a rare case of gigantiform cementoma where we were able to trace a familial history.
Case report
A 7-year-old male child reported to the Department of Oral and Maxillofacial Surgery, Tamilnadu Government Dental College and Hospital with a chief complaint of massive painless swelling over the left side of the face for the past 7 months.
Patient was apparently normal before 7 months after which he developed a swelling in the left side of mandible which gradually increased to an alarming size (Fig. 1). Patient was not able to close his mouth and also presented with a history of spontaneous bleeding from the mass occasionally. The patient was poorly built, afebrile with normal cardiovascular, respiratory and abdominal findings. On extra oral examination, there was a diffuse firm non-tender swelling apparently arising from the left mandible of size 20 × 20 × 20 cms occupying the entire oral cavity and extending onto the neck. Skin over the swelling was stretched. On intraoral examination, 2/3rd of the oral cavity was obliterated by the swelling. Multiple teeth were displaced and embedded over the mass. Blood reports revealed low hemoglobin levels. Plain radiographs–lateral and anteroposterior view revealed radio opacities in all the four quadrants and the radio-opaque mass over the left side of mandible with multiple teeth embedded in it (Figs. 2, 3). CT scan revealed well-defined expansile lytic lesion on the left maxilla and mandible. (Fig. 4)
Fig. 1.

Patient presenting with massive swelling over the left side of the mandible
Fig. 2.

X-ray AP view showing radio-opaque mass
Fig. 3.

X-ray lateral view
Fig. 4.

CT facial bones showing expansile lytic lesion in left mandible and radioopacities in all the four quadrants
Family history
There was a significant familial history. Patient’s grandmother and grandmother’s sister presented with similar swelling in the upper and lower jaw, respectively (Figs. 5, 6). Patient’s mother also presented with a small swelling in the mandibular left posterior region (Fig. 7).
Fig. 5.

Patient’s grandmother with a swelling in the maxillary anterior region
Fig. 6.

Patient’s grandmother’s sister with a swelling in the mandibular right posterior region
Fig. 7.

Patient’s mother with a small swelling in the mandibular left posterior region
Management
Under video laryngoscope guidance, oral intubation was done. General anesthesia was induced and maintained. Incisional biopsy was taken from the superior, middle and inferior portion of the exterior aspect of the swelling. Hemostasis was achieved with bipolar cautery. Histopathological report was suggestive of “fibrous dysplasia” and had to be correlated with clinical findings.
As the radiographic finding revealed the involvement of all the four quadrants and also based on the other clinical findings such as size and extent of the lesion and familial history, the diagnosis was arrived as “Familial gigantiform cementoma”
Considering the airway obstruction that the lesion was causing due to its large size and chances of recurrence, extensive resection was planned under general anesthesia. Elective tracheotomy was done. Patient was intubated, general anesthesia was induced and maintained (Fig. 8). Bilateral submandibular incision and lip split incision were placed. Full thickness flap was raised, and lesion was completely exposed. Osteotomy cuts were placed over right angle of mandible region, and complete disarticulation was done on the left side. The tumor mass was relieved from the surrounding tissues and was removed in toto (Fig. 9) following which reconstruction was done. Patient was maintained under mechanical ventilation after which he recovered uneventfully (Fig. 10). Weaning of tracheostomy was done, and the tracheostomy tube was removed. Histopathological examination of the resected mass revealed irregular calcified material resembling cementum within a fibrous stroma (Fig. 11).
Fig. 8.

Intubation
Fig. 9.
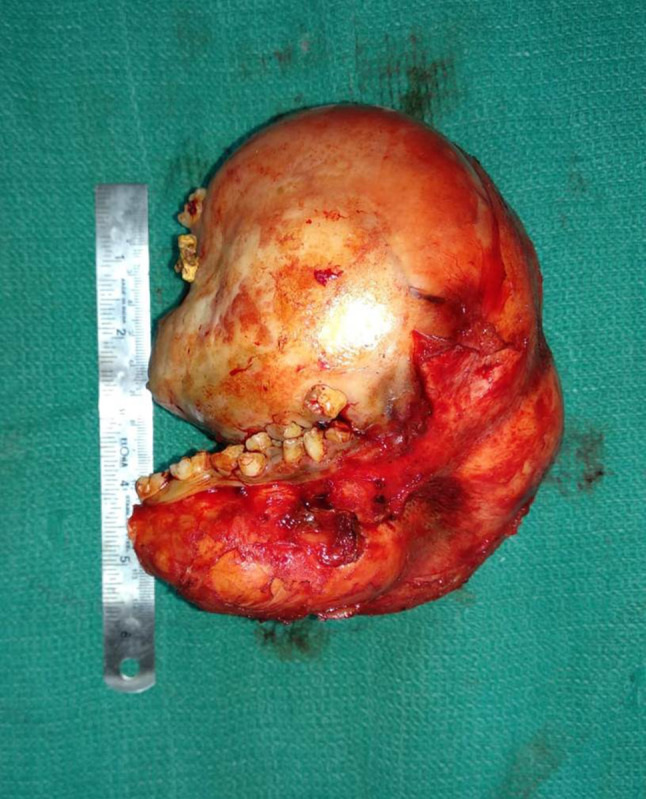
Lesion removed in toto
Fig. 10.

Two weeks post operatively
Fig. 11.
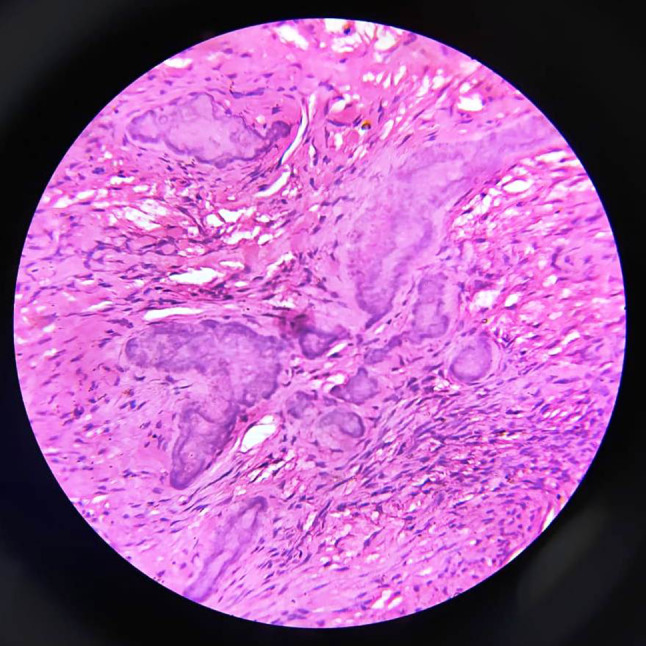
Pictomicrograph showing irregular calcified material in a fibrous stroma
Discussion
Familial gigantiform cementoma is a rare fibro-cemento-osseous lesion that can cause marked expansion of facial skeleton with an autosomal dominant pattern of inheritance and variable phenotypic expression [6]. Sporadic cases of gigantiform cementoma have also been reported [7].
There are 3 distinct growth phases of the tumor: initial onset, rapid expansion and suppression of growth. It develops in the first two decades of life typically followed by rapid expansile growth and stagnates in the fifth decades when untreated [6]. Most cases seen in developed countries present early and are symptomatically treated before the size of the tumor becomes large [1]. In few cases, the alkaline phosphatase levels are reported to be elevated preoperatively and its levels decrease with resection of the tumor [1].
Weinstein et al in 1991 reported the somatic mutation of G protein in McCune-Albright syndrome. Replacement of arginine with cystine or histidine in 201 position of Gs alpha protein decreased the intrinsic GTPase activity by 30-fold, which lead to uncontrolled cellular proliferation. Given the synchronous involvement of jaw and clinicopathological features of familial gigantiform cementoma, it can be viewed as polyostotic fibro-osseous disease similar to fibrous dysplasia as in McCune-Albright syndrome. Therefore, G protein abnormality could be involved in the pathogenesis of familial gigantiform cementoma [4].
Developmentally familial gigantiform cementoma arise from the tooth bearing region of the jaw which cause downward displacement of mandibular canal and superior displacement of floor of maxillary sinus [8].
The radiological differential diagnosis of an expansile well-defined mineralized mass includes benign cementoblastoma, ossifying fibroma, osteoma and familial gigantiform cementoma. The radiographical differential diagnosis between cementoblastoma and familial gigantiform cementoma is difficult as both may occur in periapical region of molars and exhibit radiolucent rim around radio dense mass. Osteomas lack lobular radio dense appearance of familial gigantiform cementoma [7].
Microscopically varying degree of cellularity and variation in size and amount of mineralized deposits is usually observed in familial gigantiform cementoma. Histologically features, developmental stages of the lesion and the clinical behavior and age of patient might correlate. There is a possibility that during skeletal growth the lesion is more cellular and biologically active and has a tendency toward bony expansion and recurrence [4].
Histopathological examination can rule out fibrous dysplasia as familial gigantiform cementoma presents with large basophilic masses, Cherubim can be ruled out because of lack of giant cells. Histopathologically familial gigantiform cementoma is similar to psammomatoid variant of juvenile ossifying fibroma because of the presence of cementicles, however, the gross features of juvenile ossifying fibroma differentiate it from the hard, not easily cleavable familial gigantiform cementoma [8].
Due to the extensive nature, rapid expansion rate and high recurrence, management of familial gigantiform cementoma is difficult [5]. Certain cases have been managed by surgical shaving although there are high chances for recurrence [8], and also the incomplete removal of the lesion can lead to more rapid growth of the residual lesion [5]. Therefore, extensive resection of the lesion is to be preferred to decrease the chances of recurrence.
Conclusion
Familial gigantiform cementoma is a rare condition. Only 40 cases have been reported worldwide. In our study, we encountered 3 generations being affected by this condition. Only one has shown aggressive changes which has led to extensive morbidity affecting the individual’s life. Our study has shown the importance of early diagnosis and prompt treatment in restoring the jaw and improving the patient’s quality of life.
Compliance with ethical standard
Conflict of interest
The authors declare that they have no conflict of interest
Consent for publication
Obtained
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Finical SJ, Kane WJ, Clay RP, Bite U. Familial gigantiform cementoma. Plast Reconstr Surg. 1999;103(3):949–954. doi: 10.1097/00006534-199903000-00027. [DOI] [PubMed] [Google Scholar]
- 2.Young SK, Markowitz NR, Sullivan S, Seale TW, Hirschi R. Familial gigantiform cementoma: classification and presentation of a large pedigree. Oral Surg Oral Med Oral Pathol. 1989;68(6):740–747. doi: 10.1016/0030-4220(89)90165-5. [DOI] [PubMed] [Google Scholar]
- 3.Rossbach H-C, Letson D, Lacson A, Ruas E, Salazar P. Familial gigantiform cementoma with brittle bone disease, pathologic fractures, and osteosarcoma: a possible explanation of an ancient mystery. Pediatr Blood Cancer. 2005;44(4):390–396. doi: 10.1002/pbc.20253. [DOI] [PubMed] [Google Scholar]
- 4.Abdelsayed RA, Eversole LR, Singh BS, Scarbrough FE. Gigantiform cementoma: clinicopathologic presentation of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91(4):438–444. doi: 10.1067/moe.2001.113108. [DOI] [PubMed] [Google Scholar]
- 5.Wang H-W, Ma C-Y, Qin X-J, Zhang C-P. Management strategy in patient with familial gigantiform cementoma. Medicine. 2017 doi: 10.1097/md.0000000000009138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang HW, Yu M, Qin XJ, Zhang CP. Familial gigantiform cementoma: distinctive clinical features of a large Chinese pedigree. Br J Oral Maxillofac Surg. 2015;53(1):83–85. doi: 10.1016/j.bjoms.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 7.Noffke C, Ngwenya S, Nzima N, Raubenheimer E, Rakgwale N. Gigantiform cementoma in a child. Dentomaxillofacial Radiol. 2012;41(3):264–266. doi: 10.1259/dmfr/13435626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kumar VV, Ebenezer S, Narayan TV, Wagner W. Clinicopathologic conference: multiquadrant expansile fibro-osseous lesion in a juvenile. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;113(3):286–292. doi: 10.1016/j.tripleo.2011.08.021. [DOI] [PubMed] [Google Scholar]