

Abstract
Background and Objectives
Little is known about the effect of education or other indicators of cognitive reserve on the rate of reversion from mild cognitive impairment (MCI) to normal cognition (NC) or the relative rate (RR) of reversion from MCI to NC vs progression from MCI to dementia. Our objectives were to (1) estimate transition rates from MCI to NC and dementia and (2) determine the effect of age, APOE, and indicators of cognitive reserve on the RR of reversion vs progression using multistate Markov modeling.
Methods
We estimated instantaneous transition rates between NC, MCI, and dementia after accounting for transition to death across up to 12 assessments in the Nun Study, a cohort study of religious sisters aged 75+ years. We estimated RRs of reversion vs progression for age, APOE, and potential cognitive reserve indicators: education, academic performance (high school grades), and written language skills (idea density, grammatical complexity).
Results
Of the 619 participants, 472 were assessed with MCI during the study period. Of these 472, 143 (30.3%) experienced at least one reverse transition to NC, and 120 of the 143 (83.9%) never developed dementia (mean follow-up = 8.6 years). In models adjusted for age group and APOE, higher levels of education more than doubled the RR ratio of reversion vs progression. Novel cognitive reserve indicators were significantly associated with a higher adjusted RR of reversion vs progression (higher vs lower levels for English grades: RR ratio = 1.83; idea density: RR ratio = 3.93; and grammatical complexity: RR ratio = 5.78).
Discussion
Knowledge of frequent reversion from MCI to NC may alleviate concerns of inevitable cognitive decline in those with MCI. Identification of characteristics predicting the rate of reversion from MCI to NC vs progression from MCI to dementia may guide population-level interventions targeting these characteristics to prevent or postpone MCI and dementia. Research on cognitive trajectories would benefit from incorporating predictors of reverse transitions and competing events, such as death, into statistical modeling. These results may inform the design and interpretation of MCI clinical trials, given that a substantial proportion of participants may experience improvement without intervention.
Cognition is fluid and cognitive states can improve or decline over time. Individuals with mild cognitive impairment (MCI) typically progress to dementia, but some instead revert to normal cognition (NC).1-4 Determining the rate of transition from MCI to NC, comparing rates of reversion (MCI to NC) to progression (MCI to dementia), and identifying predictors associated with these transitions is important to inform the clinical prognosis of individuals with MCI and the design and interpretation of MCI clinical trials, and to develop public health strategies to prevent or delay dementia.
Little is known about the effect of education or other indicators of cognitive reserve on the rate of reversion from MCI to NC or the relative rate of reversion from MCI to NC vs progression from MCI to dementia. Younger age5,6 and absence of an APOE ε4 allele6-9 have been reported to be significantly associated with reversion from MCI to NC, whereas results for education are inconsistent.5,6,10 However, none of these risk factor studies accounted for transitions to dementia and to death despite the fact that these competing transitions are common in older adults.
Our aims were to jointly model the instantaneous rates of reversion from MCI to NC and progression from MCI to dementia while considering transitions from MCI to death and determine the effect of age, APOE, and indicators of cognitive reserve (educational attainment, academic performance, and written language skills) on the relative transition rate of reversion vs progression.
Methods
Study Sample
The methodology of the Nun Study has been described previously.11 In brief, it is a longitudinal study of aging and cognition among members of a religious congregation (the School Sisters of Notre Dame) living in the United States. Participants were all women with similar adult lifestyles, including socioeconomic status, social support, marital and reproductive histories, alcohol and tobacco use, and access to health services. Of 1,031 eligible religious sisters aged 75 years or older at baseline (1991–1993), 678 agreed to participate, and their mean age, race, death rate, and country of birth did not differ significantly from nonparticipants.11 Cognitive function was assessed at baseline and approximately annually thereafter, until death or the end of the 12th round of assessments. The analytic sample was restricted to participants with postbaseline data (i.e., at least one follow-up cognitive assessment or date of death) and data on APOE status and education (n = 619). For a subset of participants, data from convent archives were available on academic performance (course grades for English, n = 454; Latin, n = 416; algebra, n = 451; geometry, n = 435) and written language skills (idea density, n = 164; grammatical complexity, n = 164).
Measures
Cognitive States
The diagnostic criteria for NC, MCI, and dementia applied at each assessment have been described previously12 and are summarized briefly below. Cognitive performance in the Nun Study was assessed using 5 measures from the Consortium to Establish a Registry for Alzheimer's Disease (CERAD) neuropsychological battery13: Delayed Word Recall, Verbal Fluency, Boston Naming, Constructional Praxis, and the Mini-Mental State Examination (MMSE). Cut points on these tests for NC, MCI, and dementia were based on CERAD normative data,12,14 which included women with comparable age and education to those of the Nun Study.12
Normal Cognition
Criteria for NC were based on intact cognition in the Delayed Word Recall (≥5), Boston Naming (≥14), Verbal Fluency (≥12), and Constructional Praxis (≥9) tests; intact global cognition based on the MMSE (≥24)15; and intact function in activities of daily living (ADL)16 (feeding, dressing, walking, standing [transferring], and toileting), defined as the ability to independently complete at least 4 of the 5 activities.
Mild Cognitive Impairment
Individuals with MCI did not meet criteria for NC or dementia. They had at least one specific area of impaired cognitive function, with cut points for impairment at 1.5 SD below age-appropriate means (Delayed Word Recall <5, Boston Naming <14, Verbal Fluency <12, and Constructional Praxis <9). They could also be impaired in global cognitive ability (MMSE < 24) or ADL; however, they did not meet criteria for dementia because if more than one area of cognition was impaired, they were intact in ADL. This cognitive state reflects all cognitive impairment states less severe than dementia (previously described12).
Dementia
Participants were diagnosed with dementia based on the presence of an impairment in memory and in at least one other cognitive domain. For dementia, impairment was identified based on performance below the fifth percentile of CERAD normative data14 (Delayed Word Recall <4, Boston Naming <13, Verbal Fluency <11, and Constructional Praxis <8), functional impairment in ADL, and decline from a previous level of cognitive function.12
Predictors
Genotyping of APOE was performed according to standard methods17 and blinded to cognitive status. Convent archival records provided data on age, educational attainment, and academic performance in first-year high school courses (English, Latin, algebra, and geometry), which was extracted from high school transcripts listing courses and grades achieved. Measures of written language skills (idea density and grammatical complexity) were based on handwritten autobiographies from the convent archives and have been described previously.11 In brief, these autobiographies were written at a mean age of 22 years (SD 2.9) before entering the religious order and provided a summary of life events. The last 10 sentences of each autobiography were coded to yield mean scores for idea density and grammatical complexity, which were ranked within each convent. Scores for idea density were based on the mean number of ideas expressed per 10 words; scores for grammatical complexity on an 8-level scale were based on the Developmental Level metric.11,18-20
Statistical Analysis
Multistate Markov models were used to estimate the instantaneous rates of transition among 3 transient cognitive states—NC (state 0), MCI (state 1), and dementia (state 2)—and one absorbing state (death) (state 3) (Figure). Transitions were treated as reversible between NC and MCI and unidirectional between other states (i.e., nonreversible from dementia and MCI, as well as from death to any cognitive state).
Figure. Multistate Diagram of a 4-State Transition Model.
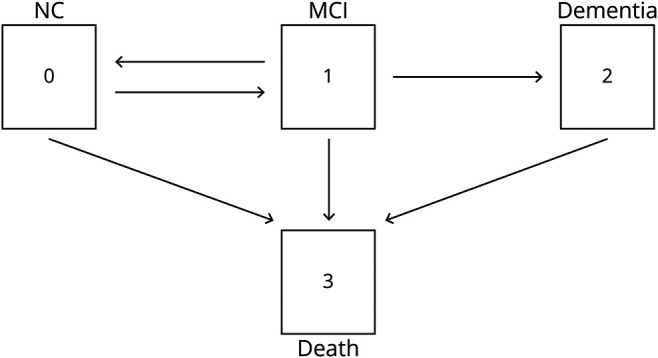
The nodes represent the 3 cognitive states and death. A multistate Markov model was used for joint modeling of transitions between cognitive states and death, focusing on reversion from mild cognitive impairment (MCI) to normal cognition (NC) and progression from MCI to dementia, and considering that death could occur at any time.
The Markov assumption is most commonly adopted in multistate models for which the transition rates only depend on the current state and time and not the full history of past transitions. Multistate Markov models in continuous time are formulated by specifying transition intensity functions: the instantaneous rate of making one of these transitions given the individual is at risk of such a transition at a given time point. Let  denote the intensity for the state
denote the intensity for the state  to state
to state  transition at age
transition at age  ; then,
; then,  indicates the intensity for the transition from state 0 to state 1 (NC → MCI), while
indicates the intensity for the transition from state 0 to state 1 (NC → MCI), while  indicates the intensity for the reverse transition from state 1 to state 0 (MCI → NC),
indicates the intensity for the reverse transition from state 1 to state 0 (MCI → NC),  represents the transition rate from MCI to dementia, and
represents the transition rate from MCI to dementia, and  and
and  are mortality intensities for individuals with NC, MCI, and dementia, respectively. Covariates are associated with the transition intensities based on the proportional intensity model (similar to the Cox proportional hazard model in survival analysis for a single event) such that
are mortality intensities for individuals with NC, MCI, and dementia, respectively. Covariates are associated with the transition intensities based on the proportional intensity model (similar to the Cox proportional hazard model in survival analysis for a single event) such that  , where X is the vector of covariates (age, APOE ε4, education, academic performance, and written language skills),
, where X is the vector of covariates (age, APOE ε4, education, academic performance, and written language skills),  represents the covariate effects that differ from one transition to another, and
represents the covariate effects that differ from one transition to another, and  represents the baseline transition rate with a piecewise-constant structure, that is,
represents the baseline transition rate with a piecewise-constant structure, that is,  for age category l. Conditional on the initial state, the likelihood function was constructed based on the multistate Markov model with mixed types of panel observation for cognitive status (observed at prespecified times) and death (upon occurrence). The msm package for R21 was used for fitting continuous-time Markov multistate models with piecewise-constant transition intensities to longitudinal data.
for age category l. Conditional on the initial state, the likelihood function was constructed based on the multistate Markov model with mixed types of panel observation for cognitive status (observed at prespecified times) and death (upon occurrence). The msm package for R21 was used for fitting continuous-time Markov multistate models with piecewise-constant transition intensities to longitudinal data.
Age is the time scale, motivated by knowledge that the risk of MCI, dementia, and death depends on age, after assuming piecewise constant transition rates within each of the age intervals (75–90 and 90+ years). The baseline intensity  depends on time/age. We initially used a piecewise constant model to categorize age
depends on time/age. We initially used a piecewise constant model to categorize age  by 5-year age groups [75, 80), [80, 85), [85, 90), [90, 95) and ≥95, such that
by 5-year age groups [75, 80), [80, 85), [85, 90), [90, 95) and ≥95, such that  when
when  falls in the
falls in the  th age interval,
th age interval, . The final model used 90 years as the sole breakpoint given that assessment of the transition intensities between cognitive states for different 5-year age groups showed that the transition rates were more similar for those 90 years and younger compared to those above 90 years of age.
. The final model used 90 years as the sole breakpoint given that assessment of the transition intensities between cognitive states for different 5-year age groups showed that the transition rates were more similar for those 90 years and younger compared to those above 90 years of age.
Three sets of analyses were conducted by fitting different multistate Markov models for transition intensities: (1) piecewise-constant baseline transition rates without adjusting for covariates; (2) piecewise-constant baseline intensities and multiplicative effects of APOE; and (3) piecewise-constant baseline rates and multiplicative effects of APOE and each indicator of cognitive reserve (education, academic performance, or written language skills). Note that the effect of each cognitive reserve indicator was evaluated separately to determine its effects independent of other indicators while controlling for the effects of age and APOE ε4 status. We report the corresponding measures from the analyses: (1) unadjusted baseline age-specific transition rates; (2) the relative transition rate (RR), defined as the ratio of the reverse transition rate from MCI to NC to the progression transition rate from MCI to dementia, by age group and APOE ε4 status; (3) RRs by different levels of the cognitive reserve indicators, age group, and APOE ε4 status; and (4) the ratios of RRs, reflecting the effect of the cognitive reserve indicator on the RR of reversion vs progression, adjusted for age group and APOE ε4 status. Here the ratio of RRs reduces to exp (β10–β12), where β1j is the beta coefficient associated with a specific cognitive indicator variable and is defined free of age. Additional statistical details are provided in eAppendix 1 (links.lww.com/WNL/B774). The R code for data analysis is available upon request from Y.S.
Standard Protocol Approvals, Registrations, and Patient Consents
Ethics approval by institutional review boards was obtained from the University of Kentucky for the original Nun Study and from the University of Waterloo for the current study.
Data Availability
The data used in this article will be made available by the corresponding author to qualified investigators upon reasonable request.
Results
Sample Description
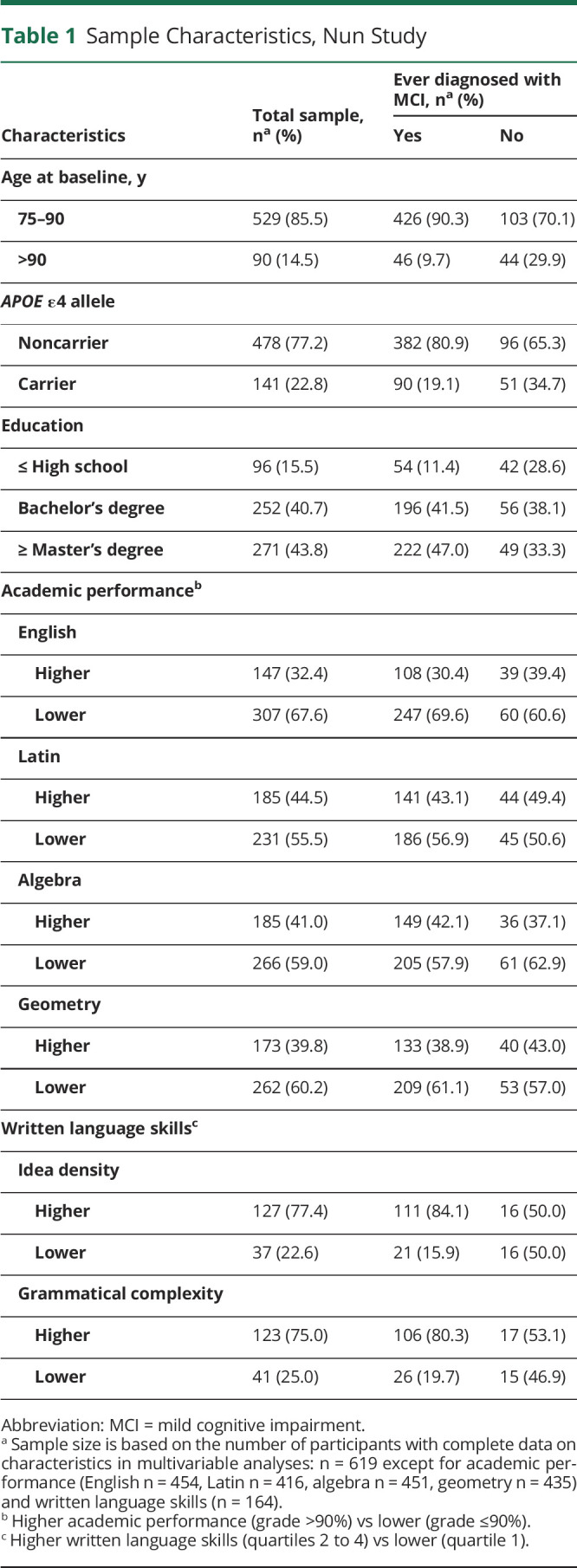
Participants were women 75 years or older at baseline (14.5% >90 years) and generally highly educated (84.5% with an undergraduate or graduate degree) (Table 1). This high level of intellectual achievement was also reflected in strong academic performance across all 4 high school courses. Among the 619 participants, 472 were observed to have MCI at some point during the follow-up period, and 143 (30.3%) of these showed at least one reverse transition from MCI to NC. These 143 participants were followed for an average of 8.6 years (SD 4.1) after their first diagnosis of MCI; 120 (83.9%) never developed dementia over an average of 8.6 years of follow-up, with 34 of these 120 participants remaining cognitively intact after reverting from MCI to NC. Another 142 participants progressed to dementia after a diagnosis of MCI without a reverse transition to NC, 16 remained in the MCI state until the end of the follow-up period, and 171 progressed to death without reversion to NC or progression to dementia. No participant reverted to MCI from dementia.
Table 1.
Sample Characteristics, Nun Study
Unadjusted Age-Specific Transition Rates
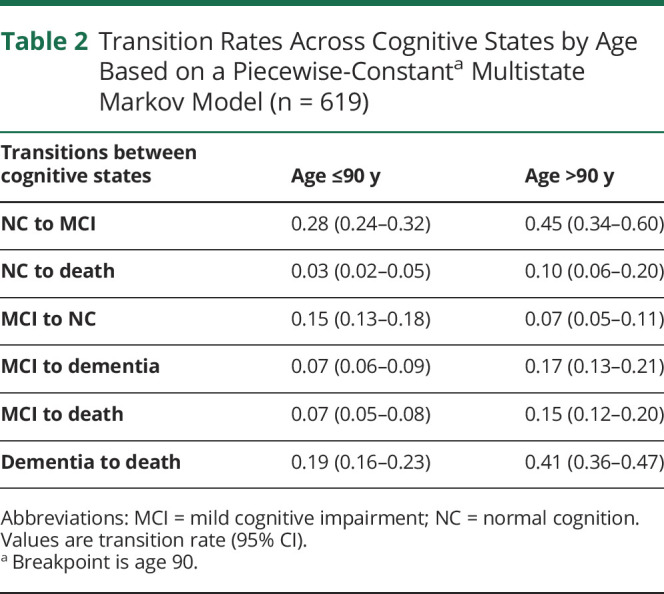
The reverse transition rate from MCI to NC dropped from 0.15 per year (95% CI 0.13–0.18) in participants ≤90 years to 0.07 per year (95% CI 0.05–0.11) in participants >90 years (Table 2). The transition rate from MCI to death more than doubled across age groups, increasing from 0.07 (95% CI 0.05–0.08) in participants ≤90 years to 0.15 (95% CI 0.12–0.20) in those >90 years. The risks of transition from MCI to death, dementia, and NC were 0.07, 0.07, and 0.15, respectively, in participants ≤90 years compared to 0.17, 0.15, and 0.07, respectively, in participants over 90 years of age. That is, for those 90 years or younger, the risks of death and dementia were similar, but reversion to NC was more common. For those over 90 years of age, the risks of death and dementia were similar, but reversion to NC was less common.
Table 2.
Transition Rates Across Cognitive States by Age Based on a Piecewise-Constanta Multistate Markov Model (n = 619)
RRs by Age Group and APOE
The proportion of participants with an APOE ε4 allele (carriers) was similar across age groups at baseline: of the 529 participants ≤90 years, 119 (22%) were APOE ε4 carriers, compared to 22 (24%) of the 90 participants >90 years. Those 529 participants ≤90 years at baseline provided information on transitions in cognitive status prior to 90 years of age. There were 371 participants (75 APOE ε4 carriers and 295 APOE ε4 noncarriers) who survived to have data collected after the age of 90, and they contributed to the estimation of transition rates beyond age 90.
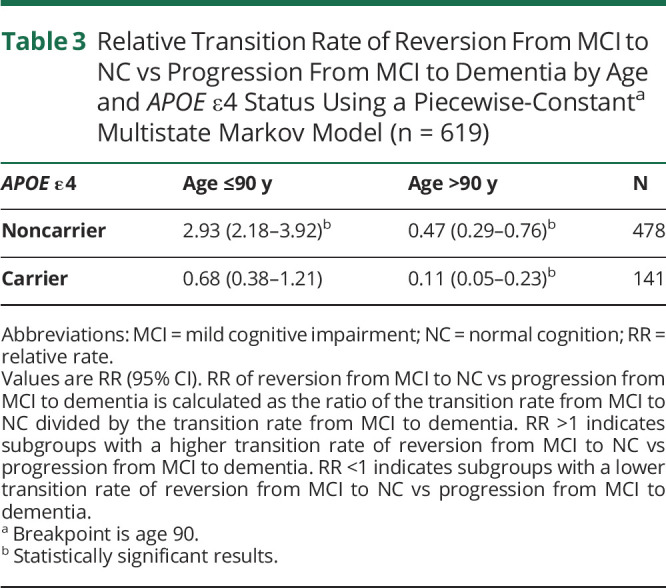
Among participants ≤90 years, APOE ε4 noncarriers showed almost triple the rate of reversion from MCI to NC than progression from MCI to dementia (RR 2.93, 95% CI 2.18–3.92); this was not observed in APOE ε4 carriers (RR 0.68, 95% CI 0.38–1.21) (Table 3). Participants >90 years were more likely to progress to dementia from MCI than to revert to NC regardless of APOE ε4 status. However, APOE ε4 status remained influential, with these older APOE ε4 noncarriers more than 4 times (0.47/0.11) as likely as older APOE ε4 carriers to revert from MCI to NC rather than progress from MCI to dementia (Table 3).
Table 3.
Relative Transition Rate of Reversion From MCI to NC vs Progression From MCI to Dementia by Age and APOE ε4 Status Using a Piecewise-Constanta Multistate Markov Model (n = 619)
RRs by Cognitive Reserve Indicator, Age Group, and APOE
The effect of cognitive reserve indicators on reversion from MCI to NC vs progression from MCI to dementia was assessed for education, academic performance, and written language skills separately. In models of education by age and APOE, APOE ε4 noncarriers ≤90 years of age remained more likely to revert than progress from MCI only if they had attained a Bachelor's degree or higher (Table 4). In contrast, progression was significantly more likely than reversion regardless of educational level for those over 90 years of age, as well as for APOE ε4 carriers ≤90 years of age with a high school or lower level of education.
Table 4.
Relative Transition Rate of Reversion From MCI to NC vs Progression From MCI to Dementia for Education by Age and APOE ε4 Status Using a Piecewise-Constanta Multistate Markov Model (n = 619)

In models of academic performance, across all levels and courses, reversion continued to be significantly more likely than progression for APOE ε4 noncarriers ≤90 years, whereas progression was significantly more likely than reversion for APOE ε4 carriers over 90 years of age (Table 5). Examining course-specific effects, for APOE ε4 noncarriers >90 years, progression was significantly more likely than reversion regardless of performance levels in algebra and geometry; however, this held only for the lower performance level for English and Latin. English showed the strongest effects of any of the courses: APOE ε4 noncarriers ≤90 years with higher performance in English had the highest chance of reversion vs progression (RR 4.79, 95% CI 2.86–8.05), while APOE ε4 carriers >90 years with lower performance in English showed the lowest chance (RR 0.07, 95% CI 0.03–0.18) (Table 5).
Table 5.
Relative Transition Rate of Reversion From MCI to NC vs Progression From MCI to Dementia for Academic Performance and Written Language Skills by Age and APOE ε4 Status Using a Piecewise-Constanta Multistate Markov Model

Models of idea density and grammatical complexity showed similar patterns of significance across both of these measures of written language skills. In APOE ε4 noncarriers ≤90 years of age, reversion was significantly greater than progression for those with higher levels of these skills, whereas among APOE ε4 carriers >90 years of age, progression was significantly greater than reversion for those with lower levels (Table 5).
RR Ratios for Cognitive Reserve Indicators Adjusted for Age Group and APOE
For each cognitive reserve indicator, the ratio of RRs by indicator level was used as a measure of its effect on the RR of reversion vs progression in models adjusted for age group and APOE (Table 6). Compared to those with only a grade school or high school education, participants with a Bachelor's degree had more than double (RR ratio 2.60; 95% CI 1.05–6.45) and those with a Master's degree or higher had triple (RR ratio 2.94; 95% CI 1.27–7.22) the RR of reversion vs progression. Higher levels of performance in English and written language skills were associated with a significantly higher RR of reversion vs progression (higher vs lower levels for English grades: RR ratio 1.83, 95% CI 1.07–3.14; idea density: RR ratio 3.93, 95% CI 1.30–11.92; and grammatical complexity: RR ratio 5.78, 95% CI 1.56–21.42) (Table 6).
Table 6.
Ratio of Relative Transition Rates of Reversion From MCI to NC vs Progression to Dementia by Level of Education, Academic Performance, and Written Language Skills Adjusted for Age and APOE ε4 Status Using Piecewise-Constanta Multistate Markov Modelling

Discussion
In this highly educated cohort of older religious sisters, reverse transitions from MCI to NC were relatively common and as frequent as transitions from MCI to dementia. The relatively younger age group (≤90 years) and absence of an APOE ε4 allele (i.e., lack of established risk factors for dementia) contributed to a significantly higher transition rate of reversion from MCI to NC vs progression from MCI to dementia. Higher educational attainment, the traditional indicator of cognitive reserve, was associated with a significantly higher RR of reversion vs progression compared to lower educational attainment. A similar statistically significant association was also found for novel indicators of cognitive reserve: academic performance in high school English and written language skills (idea density and grammatical complexity).
This study demonstrates that those with higher levels of cognitive reserve indicators (educational attainment, academic performance, and written language skills) had a significantly greater chance of reversion from MCI to NC than progression from MCI to dementia. The observed association is consistent with literature on risk factors for dementia.7 Low educational attainment is a well-established risk factor for dementia. Although educational levels are generally higher for participants of the Nun Study than for other women of their era given greater educational opportunities through their religious order, the established association between lower education and higher risk of dementia is also found in the Nun Study.22 In addition, interactions between age, APOE, and education have previously been shown in a subset of the Nun Study, with the highest risk of developing dementia among older APOE ε4 carriers with low levels of education.23 The protective effect of education on reversion from MCI to NC in this study is also consistent with findings from other cohorts of less educated men and women.7 The association between higher educational attainment and lower risk of dementia has traditionally been attributed to cognitive reserve24 and this link has been supported by evidence from imaging studies.25 In addition to a reduced risk of dementia, cognitive reserve may also have effects on other cognitive outcomes, such as reversion from MCI to NC, through mechanisms such as neural compensation, whereby the brain creates compensatory paths to overcome the primary neural changes that lead to MCI.24
Whereas education is the classic proxy for cognitive reserve, other intellectual factors may also predict reversion. Although less studied, higher academic performance has been associated with a lower risk of developing dementia.26-29 Intellectual aptitude in adolescence, including measures of word function in sentences and reading comprehension, has been associated with a reduced risk of Alzheimer disease (AD).30 Early research based on an initial sample of decedents from the Nun Study showed that lower levels of idea density and grammatical complexity were associated with low cognitive test scores in late life and higher risk of AD.11 In our larger sample of Nun Study participants, higher idea density and grammatical complexity, in addition to higher educational level and stronger academic performance in high school English, were associated with a greater chance of reversion from MCI to NC than progression from MCI to dementia. Our results show the importance of academic performance and written language skills as predictors of reversion and also support the importance of education, a more widely available measure. The observed effect of all of these indicators of cognitive reserve has implications for population-level intervention strategies in early life to prevent or postpone MCI and dementia.
Our findings that almost one-third of participants revert from MCI to NC is consistent with previous reports on the proportion of such reverse transitions in other community settings and populations.1,2,7,31 In their systematic review and meta-analysis, Canevelli and colleagues1 concluded that reversion to NC is common in individuals with MCI but is understudied. The studies that have been conducted on reversion from MCI have typically used standard Cox survival analysis, which does not adjust for competing transitions from MCI to dementia or from MCI to death.32,33 The use of survival analysis makes the assumption that individuals who experience a transition to dementia or death have the same rate of reversion from MCI to NC as those who remain and are included in the calculation of this reversion (i.e., that those censored are representative of those remaining).34,35 However, this assumption is questionable, and ignoring these competing effects of dementia and death may lead to biased estimates of the rate of reversion.34,36,37 Other analytic methods, such as binary logistic regression5 or generalized linear mixed modeling,6 have also been used, but these are discrete time models looking at the probability of reversion and similarly have failed to account for transitions from MCI to dementia and to death.
The use of multistate modeling addresses these analytic limitations and is a strength of our study. Multistate Markov models can account for competing events38 and are increasingly being used to study disease onset, progression, and comorbidities in chronic diseases, including dementia.23,36,39-42 Our multistate models jointly estimated the instantaneous risks of transitions between cognitive states and transition to death, where transitions from MCI to dementia and to death were considered as competing events in the transition from MCI to NC. This joint modeling is particularly useful for studying older adults for whom transitions from MCI to dementia and death can occur at appreciable rates.
Other strengths included the analysis of data from a population-based longitudinal study that included up to 12 cognitive assessments and information on early-life intellectual factors. In addition, our Nun Study participants are uniquely homogeneous on many sociodemographic and lifestyle factors as well as access to health care, providing strong control of potential confounders. In contrast to clinical populations where cognitive changes can precipitate assessments, cognitive assessments in the Nun Study occurred at regularly scheduled intervals unrelated to cognitive status. In addition to the availability of extensive follow-up data with low attrition, these characteristics of the Nun Study data enabled the use of sophisticated modeling approaches. Furthermore, data on novel hypothesized indicators of cognitive reserve (academic performance and written language skills) allowed exploration of factors beyond highest level of education attained, the standard proxy indicator for cognitive reserve. Future research could further investigate the effect of these and other intellectual measures in addition to educational level, such as through linkage studies of educational system and health administrative data.
A limitation of this and other studies of cognitive state transitions is that the exact time of transitions between states is not known. Because assessment is not continuous, unobserved transitions may occur and could, for example, lead to a loss of estimation efficiency for reverse transition from MCI to NC. In addition, cognition is fluid, and although transitions in cognitive states may reflect cognitive reserve, they may also reflect normal variation over time or acute factors influencing cognition. Improvement in cognition across assessments may also reflect regression to the mean or practice effects.
Diagnostic criteria evolve and this cannot be reflected in data already collected, a particular issue for longitudinal studies. Thus, cognitive states were diagnosed according to established criteria at baseline and criteria remained consistent to allow valid comparisons over time. Diagnostic criteria for MCI in particular have evolved, and thus our criteria, based solely on cognitive tests, may be more likely to reflect a transient MCI state than MCI diagnosed using additional information, such as from informant reports. MCI is a heterogeneous cognitive state, and we did not analyze subtypes of MCI (e.g., amnestic vs nonamnestic, single vs multiple-domain). There may be multiple reasons, including intervening medical states, for an individual to be classified with MCI, and these factors may influence transitions between states. We have limited data on some of the potential factors that may cause fluctuations in cognition. We also did not assess the neuropathologic substrate of MCI although it affects the clinical progression of MCI, with those progressing to dementia significantly more likely than those reverting to intact cognition to show severe Alzheimer neuropathology (neurofibrillary tangles, neuritic plaques) as well as other pathologic changes (e.g., hippocampal sclerosis of aging, Lewy body disease).43
The sampling frame of the Nun Study is both a strength and a limitation. Generally speaking, population-based studies appear to show lower conversion rates to dementia and more variable trajectories. In clinical settings, the diagnosis of MCI is usually determined by clinical assessment, often using standardized assessments combined with clinical judgement. As well, the populations studied in clinical settings may be younger, healthier, and more homogeneous than those of population-based studies; clinical samples also include patients who present with symptoms for which they are seeking help. Thus, our findings need to be replicated in clinical settings.
Our modeling approach accounted for diverse age groups and cognitive states at baseline, but it cannot address the effects of potential survival bias on sampling. The Nun Study participants are not representative of the general population of older women in the United States and analyses are based on data collected more than a decade ago; the results of this study thus need to be interpreted accordingly. Data on academic performance and written language skills were not available for all participants. Finally, despite the strengths of Markov modeling, this approach has some limitations. For example, the transition rate of reversion from MCI to NC may depend on the time since diagnosis of MCI, but Markov models do not incorporate the duration in each cognitive state.
Replication of the observed indicators of cognitive reserve in other populations as well as other factors influencing transitions across cognitive states, and in particular reverse transitions from MCI to NC, will help to better understand cognitive reserve and its effect on cognitive trajectories. Further development of analytic methods (e.g., adjusting multistate modeling to reduce the effect of survivor bias in longitudinal studies of aging) is needed to address current limitations. Knowledge of predictors of reversion from MCI to NC is important to inform the design and interpretation of clinical trials, given that a substantial proportion of participants may experience improvement from MCI to NC even without intervention. Evidence of predictors of these reverse transitions may also inform population-level intervention strategies targeting these characteristics to prevent or postpone MCI and dementia.
Glossary
- AD
Alzheimer disease
- ADL
activities of daily living
- CERAD
Consortium to Establish a Registry for Alzheimer's Disease
- MCI
mild cognitive impairment
- MMSE
Mini-Mental State Examination
- NC
normal cognition
- RR
relative transition rate
Appendix. Authors
Study Funding
This study was funded by Canadian Institutes of Health Research (CIHR) operating grant 137035 to S.L.T. and Natural Sciences and Engineering Research Council of Canada (NSERC) discovery grant RGPIN115928 to L.Z. Funding for the Nun Study at the University of Kentucky was provided by the US National Institute of Aging (R01AG09862, K04AG00553, P50AG05144) and the Kleberg Foundation and, for interpretation of statistical modeling, by R01AG038651 to R.J.K.
Disclosure
M. Iraniparast, Y. Shi, Y. Wu, L. Zeng, C.J. Maxwell, and R.J. Kryscio report no disclosures relevant to the manuscript. P.D. St. John reports financial relationships for contractual clinical and administrative activities (Winnipeg Regional Health Authority and Shared Services Manitoba) and serving as a speaker (University of Ottawa/Regional Geriatric Program of Eastern Ontario) and board member (Meals on Wheels [Manitoba], Age and Opportunity). K. S. SantaCruz and S.L. Tyas report no disclosures relevant to the manuscript. Go to Neurology.org/N for full disclosures.
References
- 1.Canevelli M, Grande G, Lacorte E, et al. Spontaneous reversion of mild cognitive impairment to normal cognition: a systematic review of literature and meta-analysis. J Am Med Dir Assoc. 2016;17(10):943-948. [DOI] [PubMed] [Google Scholar]
- 2.Malek-Ahmadi M. Reversion from mild cognitive impairment to normal cognition: a meta-analysis. Alzheimer Dis Assoc Disord. 2016;30(4):324-330. [DOI] [PubMed] [Google Scholar]
- 3.Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review): report of the quality standards subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1133-1142. [DOI] [PubMed] [Google Scholar]
- 4.Shimada H, Makizako H, Doi T, Lee S, Lee S. Conversion and reversion rates in Japanese older people with mild cognitive impairment. J Am Med Dir Assoc. 2017;18(9):808.e1–808.e6. [DOI] [PubMed] [Google Scholar]
- 5.Gao Q, Gwee X, Feng L, et al. Mild cognitive impairment reversion and progression: rates and predictors in community-living older persons in the Singapore Longitudinal Ageing Studies cohort. Dement Geriatr Cogn Dis Extra. 2018;8(2):226-237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hadjichrysanthou C, McRae-McKee K, Evans S, de Wolf F, Anderson RM; Alzheimer’s Disease Neuroimaging Initiative. Potential factors associated with cognitive improvement of individuals diagnosed with mild cognitive impairment or dementia in longitudinal studies. J Alzheimers Dis. 2018;66(2):587-600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Xue H, Hou P, Li Y, Mao X, Wu L, Liu Y. Factors for predicting reversion from mild cognitive impairment to normal cognition: a meta-analysis. Int J Geriatr Psychiatry. 2019;34(10):1361-1368. [DOI] [PubMed] [Google Scholar]
- 8.Koepsell TD, Monsell SE. Reversion from mild cognitive impairment to normal or near-normal cognition: risk factors and prognosis. Neurology. 2012;79(15):1591-1598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pandya SY, Lacritz LH, Weiner MF, Deschner M, Woon FL. Predictors of reversion from mild cognitive impairment to normal cognition. Dement Geriatr Cogn Disord. 2017;43(3-4):204-214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sachdev PS, Lipnicki DM, Crawford J, et al. Factors predicting reversion from mild cognitive impairment to normal cognitive functioning: a population-based study. PLoS One. 2013;8(3):e59649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Snowdon DA, Kemper SJ, Mortimer JA, Greiner LH, Wekstein DR, Markesbery WR. Linguistic ability in early life and cognitive function and Alzheimer's disease in late life: findings from the Nun Study. JAMA. 1996;275(7):528-532. [PubMed] [Google Scholar]
- 12.Riley KP, Snowdon DA, Markesbery WR. Alzheimer's neurofibrillary pathology and the spectrum of cognitive function: findings from the Nun Study. Ann Neurol. 2002;51(5):567-577. [DOI] [PubMed] [Google Scholar]
- 13.Morris JC, Heyman A, Mohs RC, et al. The Consortium to Establish a Registry for Alzheimer's disease (CERAD): I: Clinical and neuropsychological assessment of Alzheimer's disease. Neurology. 1989;39(9):1159-1165. [DOI] [PubMed] [Google Scholar]
- 14.Welsh KA, Butters N, Mohs RC, et al. The Consortium to Establish a Registry for Alzheimer's Disease (CERAD): Part V: A normative study of the neuropsychological battery. Neurology. 1994;44(4):609-614. [DOI] [PubMed] [Google Scholar]
- 15.Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-198. [DOI] [PubMed] [Google Scholar]
- 16.Kuriansky J, Gurland B. The performance test of activities of daily living. Int J Aging Hum Dev. 1976;7(4):343-352. [DOI] [PubMed] [Google Scholar]
- 17.Saunders AM, Hulette C, Welsh-Bohmer KA, et al. Specificity, sensitivity, and predictive value of apolipoprotein-E genotyping for sporadic Alzheimer's disease. Lancet. 1996;348(9020):90-93. [DOI] [PubMed] [Google Scholar]
- 18.Cheung H, Kemper S. Competing complexity metrics and adults' production of complex sentences. Appl Psycholinguist. 1992;13(1):53-76. [Google Scholar]
- 19.Kintsch W, Keenan J. Reading rate and retention as a function of the number of propositions in the base structure of sentences. Cognit Psychol. 1973;5(3):257-274. [Google Scholar]
- 20.Turner A, Greene E. The Construction and Use of a Propositional Text Base. Institute for the Study of Intellectual Behavior, University of Colorado; 1977. [Google Scholar]
- 21.Jackson C. Multi-state models for panel data: the msm package for R. J Stat Softw. 2011;38(8):1-28. [Google Scholar]
- 22.Mortimer JA, Snowdon DA, Markesbery WR. Head circumference, education and risk of dementia: findings from the Nun Study. J Clin Exp Neuropsychol. 2003;25(5):671-679. [DOI] [PubMed] [Google Scholar]
- 23.Tyas SL, Salazar JC, Snowdon DA, et al. Transitions to mild cognitive impairments, dementia, and death: findings from the Nun Study. Am J Epidemiol. 2007;165(11):1231-1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stern Y. Cognitive reserve in ageing and Alzheimer's disease. Lancet Neurol. 2012;11(11):1006-1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lavretsky H. Resilience and Aging: Research and Practice. Johns Hopkins University Press; 2014. [Google Scholar]
- 26.Mehta KM, Stewart AL, Langa KM, et al. “Below average” self-assessed school performance and Alzheimer's disease in the Aging, Demographics, and Memory Study. Alzheimers Dement. 2009;5(5):380-387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bezerra ABC, Coutinho ESF, Barca ML, Engedal K, Engelhardt E, Laks J. School attainment in childhood is an independent risk factor of dementia in late life: results from a Brazilian sample. Int Psychogeriatr. 2012;24(1):55-61. [DOI] [PubMed] [Google Scholar]
- 28.Dekhtyar S, Wang H, Fratiglioni L, Herlitz A. Childhood school performance, education and occupational complexity: a life-course study of dementia in the Kungsholmen project. Int J Epidemiol. 2016;45(4):1207-1215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Dekhtyar S, Wang HX, Scott K, Goodman A, Koupil I, Herlitz A. A life-course study of cognitive reserve in dementia: from childhood to old age. Am J Geriatr Psychiatry. 2015;23(9):885-896. [DOI] [PubMed] [Google Scholar]
- 30.Huang AR, Strombotne KL, Horner E, Lapham SJ. Adolescent cognitive aptitudes and later-in-life Alzheimer disease and related disorders. JAMA Netw Open. 2018;1(5):e181726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Abner EL, Kryscio RJ, Cooper GE, et al. Mild cognitive impairment: statistical models of transition using longitudinal clinical data. Int J Alzheimers Dis. 2012;2012:291920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Roberts RO, Knopman DS, Mielke MM, et al. Higher risk of progression to dementia in mild cognitive impairment cases who revert to normal. Neurology. 2014;82(4):317-325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Grande G, Cucumo V, Cova I, et al. Reversible mild cognitive impairment: the role of comorbidities at baseline evaluation. J Alzheimers Dis. 2016;51(1):57-67. [DOI] [PubMed] [Google Scholar]
- 34.Murphy TE, Han L, Allore HG, Peduzzi PN, Gill TM, Lin H. Treatment of death in the analysis of longitudinal studies of gerontological outcomes. J Gerontol A Biol Sci Med Sci. 2011;66(1):109-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Andersen PK, Geskus RB, de Witte T, Putter H. Competing risks in epidemiology: possibilities and pitfalls. Int J Epidemiol. 2012;41(3):861-870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kryscio RJ, Abner EL, Lin Y, et al. Adjusting for mortality when identifying risk factors for transitions to mild cognitive impairment and dementia. J Alzheimers Dis. 2013;35(4):823-832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Crowder MJ. Multivariate Survival Analysis and Competing Risks. CRC Press; 2012. [Google Scholar]
- 38.Cook RJ, Lawless JF. Multistate Models for the Analysis of Life History Data. CRC Press; 2018. [Google Scholar]
- 39.Commenges D, Joly P, Letenneur L, Dartigues JF. Incidence and mortality of Alzheimer's disease or dementia using an illness-death model. Stat Med. 2004;23(2):199-210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Sharples LD. Use of the Gibbs sampler to estimate transition rates between grades of coronary disease following cardiac transplantation. Stat Med. 1993;12(12):1155-1169. [DOI] [PubMed] [Google Scholar]
- 41.Xu J, Kalbfleisch JD, Tai B. Statistical analysis of illness-death processes and semicompeting risks data. Biometrics. 2010;66(3):716-725. [DOI] [PubMed] [Google Scholar]
- 42.Chen HH, Duffy DW, Tabar L, Day NE. Markov chain models for progression of breast cancer: part I: tumour attributes and the preclinical screen-detectable phase. J Epidemiol Biostat. 1997;2:9-23. [Google Scholar]
- 43.Abner EL, Kryscio RJ, Schmitt FA, et al. Outcomes after diagnosis of mild cognitive impairment in a large autopsy series. Ann Neurol. 2017;81(4):549-559. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used in this article will be made available by the corresponding author to qualified investigators upon reasonable request.