

Evidence for health disparities in uterine cancer from the Uterine Cancer Evidence Review Conference is summarized.
Abstract
The Centers for Disease Control and Prevention recognized the need for educational materials for clinicians on the prevention and early diagnosis of gynecologic cancers. The American College of Obstetricians and Gynecologists convened a panel of experts in evidence review from the Society for Academic Specialists in General Obstetrics and Gynecology and content experts from the Society of Gynecologic Oncology to review relevant literature, best practices, and existing practice guidelines for the development of evidence-based educational materials for women's health care clinicians about uterine cancer. This article is the evidence summary of the literature review of health disparities and inequities related to uterine cancer. Substantive knowledge gaps are noted and summarized to provide guidance for future research.
The Centers for Disease Control and Prevention (CDC) has defined health disparities as, “preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations.”1 Significant and enduring disparities in uterine cancer, the most common gynecologic malignancy, have been reported in the literature for decades. The CDC funded a project to develop clinician educational materials for the prevention and early diagnosis of uterine cancer, which included a review of the literature on disparities in uterine cancer diagnosis, treatment, and outcomes. In conducting this review, we found abundant evidence on stark inequities in uterine cancer care and outcomes experienced by historically and contemporaneously marginalized groups, and no recent review comprehensively summarizing them. This article is the evidence summary of the literature on health disparities in uterine cancer, including differences in incidence and mortality between racial and ethnic groups as well as contributing factors, including differences in stage of disease at diagnosis, histology, socioeconomic status, and treatment. The health care professional educational material is available online at acog.org.
METHODS
Overall methods for the evidence review process are outlined in detail in the companion summary, “Executive Summary of the Uterine Cancer Evidence Review Conference”.2 Key questions and PICO criteria (P=patient, problem, or population; I=intervention; C=comparison, control, or comparator; O=outcome[s]) for framing the health disparities review are listed in Box 1. Evidence Review Conference participants included representatives from stakeholder professional and patient advocacy organizations, including those representing historically and contemporaneously excluded populations, such as the Black Women's Health Imperative, the National LGBT Cancer Network, and the National Alliance for Hispanic Health. Stakeholders had the opportunity to review the detailed literature summary and provide input at the Evidence Review Conference or by separate email communication. At the conference, evidence review panelists and invited representatives from stakeholder organizations mutually recommended that the summary of evidence of health disparities be brought forward as a separate published document, because inclusion in the main executive summary would not allow presentation in adequate detail and publication solely as an online appendix to the main executive summary would limit dissemination of this important information.
Box 1. Key Questions and PICO Criteria for Health Disparities in Uterine Cancer Literature Search.
What groups experience disparities in the uterine cancer care continuum and what are those observed disparities? What groups experience inequities and disparities in the uterine cancer care continuum and what are those observed disparities?
P: Adults with diagnosis of uterine cancer; members of historically marginalized or underserved group(s) including:
• Racial identities: non-Hispanic Black or African American, Asian, American Indian/Alaska Native, native Hawaiian and other Pacific Islander, multiracial
• Ethnic identities: Hispanic or Latinx, Mexican, Puerto Rican
• Sexual- and gender-diverse populations (eg, women who have sex with women [lesbian and bisexual], transgender men, gender nonbinary or nonconforming people, queer people)
• Lower SES (eg, income below the federal poverty level, publicly insured [eg, Medicaid], uninsured)
• Other marginalized identities (currently incarcerated, undocumented immigration status, veteran, experiencing marginal housing or homeless, individuals with substance use disorder)
O: RR or OR of uterine cancer, subtype of uterine cancer, incidence, stage at diagnosis, survival rate, quality-adjusted life-years, receipt of standard-of-care treatment, mortality rates
What factors contribute to health disparities in uterine cancer?
P: Adults with diagnosis of uterine cancer
I: Living conditions and exposures (physical environment, access to care, systemic racism, transphobia, homophobia, or bias), mistrust of health care system
C: Individuals who experience living conditions and exposures listed above vs individuals who do not
O: RR or OR of uterine cancer, subtype of uterine cancer, incidence, stage at diagnosis, survival rate, quality-adjusted life-years, receipt of standard-of-care treatment, mortality rates
How can health disparities in uterine cancer be mitigated so that optimal care and desirable outcomes are experienced by historically and contemporarily underserved populations?
P: Adults with diagnosis of uterine cancer
I: Interventions or recommendations to mitigate or reduce health disparities in uterine or gynecologic cancer
C: One guideline vs another
O: RR or OR of uterine cancer, subtype of uterine cancer, incidence, stage at diagnosis, survival rate, quality-adjusted life-years, receipt of standard-of-care treatment, mortality rates
PICO, P=patient, problem, or population; I=intervention; C=comparison, control, or comparator; O=outcome(s); SES, socioeconomic status; RR, relative risk; OR, odds ratio.
Studies almost uniformly used the term “women” or “females” to refer to the gender of those affected by uterine cancer. Although we acknowledge that uterine cancer can affect individuals of different genders who possess a uterus, we used the term “women” or “females” in this review to reflect the cited literature. In keeping with the most common categories of race and ethnicity used in national data collection, we used “Black” to refer to non-Hispanic Black or African American individuals and “White” to refer to non-Hispanic White or Caucasian individuals. We used the term “Hispanic” and not “Latinx,” because “Latinx” was rarely used in any of the articles reviewed. Although some studies restricted their analysis to Hispanic White individuals, others included Hispanic individuals of any race. Given the lack of consistency in the literature, we used the term “Hispanic,” without reference to race. In line with the literature, we used “American Indian/Alaska Native” to refer to Indigenous people of the United States. The majority of the literature reviewed aggregated individuals of the Asian diaspora with those identifying as Native Hawaiian; thus, we used the term “Asian/Pacific Islander.”
EVIDENCE REVIEW
Incidence and Mortality Disparities by Race and Ethnicity
The review found many studies examining disparities in incidence and mortality by race and ethnicity. By far the largest number of studies focused on disparities experienced by Black women, and most used White women as the comparison group. Some studies combined all uterine cancers, and others examined specific types.
Black Women
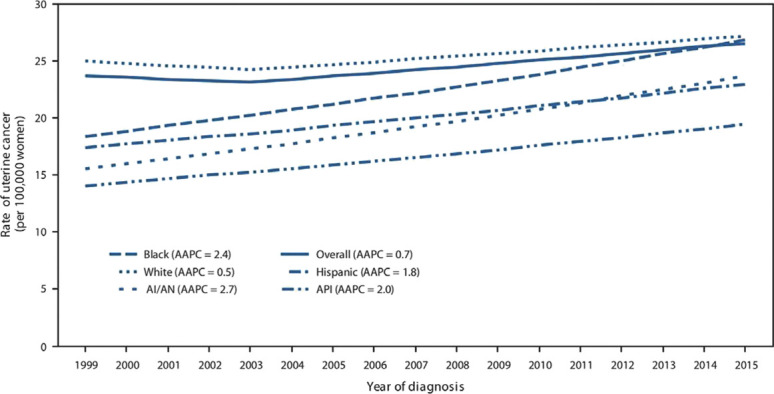
Black women have a higher incidence of uterine cancer than White women. Older studies reported the opposite.3 These studies did not account for the higher hysterectomy rate among premenopausal Black women compared with White women, underestimating the true incidence among Black women at risk for uterine cancer.3,4 In an analysis of SEER (Surveillance, Epidemiology, and End Results) data that adjusted for hysterectomy, the incidence of endometrial cancer among Black women has exceeded that of White women since 2000.4 Most recently, the CDC reported that the incidence of invasive uterine cancer in 2015, unadjusted for hysterectomy, was higher among Black and White women (27 cases/100,000) than other racial and ethnic groups (19–23/100,000).5 The incidence of uterine cancer increased from 1999 to 2015, with larger increases observed among Black women than among White women (Fig. 1).5
Fig. 1. Trends* in age-adjusted uterine cancer incidence rates† by racial and ethnic group§—United States,¶ 1999–2015. Reprinted from Henley SJ, Miller JW, Dowling NF, et al. Uterine cancer and mortality—United States, 1999–2016. MMWR, 2018;67 (48):1333–1338. The sources of the figure cited in Henley SJ et al are CDC's National Program of Cancer Registries and the National Cancer Institute's Surveillance, Epidemiology, and End Results program. *Trends were measured with average annual percent change (AAPC) in rates and were considered to increase or decrease if P<.05; otherwise, rates were considered stable. AAPC is the weighted average of the annual percent change over the period 1999–2015 using a Joinpoint regression model (up to 2 joinpoints). †Per 100,000 women, age-adjusted to the 2000 U.S. standard population. Uterine cancers were defined as microscopically confirmed cancers of the corpus uteri (International Classification of Diseases for Oncology, Third Edition [ICD-O-3] site codes C54.0–C54.3, C54.8, C54.9) and uterus, not otherwise specified (C55.9), excluding cases that were identified by autopsy or death certificate only. §Mutually exclusive racial/ethnic groups are based on information about race and ethnicity that was collected separately and combined for this report. White, Black, American Indian/Alaska Native (AI/AN), and Asian/Pacific Islander (API) race categories are all non-Hispanic. Hispanic persons can be any race. ¶Cancer incidence compiled from cancer registries that meet the data quality criteria for each year during the period 1999–2015, covering 98% of the U.S. population.
Whetstone. Uterine Cancer Health Disparities. Obstet Gynecol 2022.
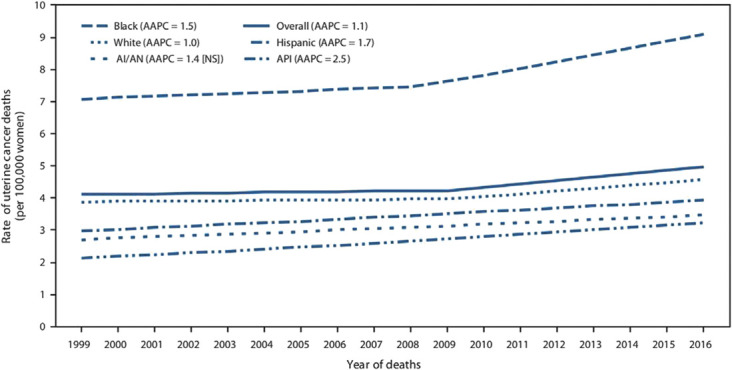
Uterine cancer mortality is higher for Black women, and death rates continue to rise faster than for other groups (Fig. 2).5 In 2016, deaths from uterine cancer among Black women (9.0/100,000) were nearly twice as frequent as any other racial or ethnic group (3.5–5.0 deaths/100,000).5 The most recent statistics from the American Cancer Society reported an absolute difference of 21% in 5-year survival rates, with 63% of Black women surviving compared with 84% of White women.6 This gap in survival represents the second largest of all racial disparities reported. These disparities in mortality are not new; they have been observed for decades. A 2002 meta-analysis of studies of survival of Black patients and White patients after a cancer diagnosis reported higher mortality among Black women than White women with uterine corpus cancer (two studies, hazard ratio [HR] 2.08, 95% CI 1.34–3.21).7 Using 1992–1998 and 2000–2011 SEER data, survival for Black women with uterine cancer was lower than for White women for every stage, grade, and histologic subtype and for every age group.3,8 DeSantis et al used SEER data to estimate disparities between Black and White women in cancer mortality and noted death rates of 7.3 and 3.9 deaths per 100,000 women, respectively, one of the largest disparities identified, exceeded only by stomach, myeloma, and cervical cancers.9 The disparity in mortality has persisted despite controlling for sociodemographic factors, comorbid conditions, and histopathologic variables in studies conducted among a number of databases and populations, including national SEER data,10 the Florida Cancer Registry,11 the National Cancer Database Registry,12 and the Detroit area SEER cancer registry.13 This disparity was also observed in a study using the National Cancer Database looking specifically at uterine carcinosarcoma.14
Fig. 2. Trends* in age-adjusted uterine cancer death rates† by racial and ethnic group§ —United States, 1999–2016. Reprinted from Henley SJ, Miller JW, Dowling NF, et al. Uterine cancer and mortality—United States, 1999–2016. MMWR, 2018;67 (48):1333–1338. The source of the figure cited in Henley SJ et al is CDC's National Center for Health Statistics National Vital Statistics System. *Trends were measured with average annual percent change (AAPC) in rates and were considered to increase or decrease if P<.05; otherwise rates were considered stable. AAPC is the weighted average of the annual percent change over the period 1999–2016 using a Joinpoint regression model (up to 2 joinpoints). †Per 100,000 women, age-adjusted to the 2000 U.S. standard population. Uterine cancer deaths were defined as deaths from cancers of corpus uteri (International Classification of Diseases 10th Edition [ICD-10] codes C54.0–C54.3, C54.8, C54.9) and uterus, not otherwise specified (C55.9). §Mutually exclusive racial/ethnic groups are based on information about race/ethnicity that was collected separately and combined for this report. White, Black, American Indian/Alaska Native (AI/AN), and API, Asian/Pacific Islander (API) race categories are all non-Hispanic. Hispanic persons can be any race. NS, not significant.
Whetstone. Uterine Cancer Health Disparities. Obstet Gynecol 2022.
Hispanic Women
Uterine cancer incidence appears to be lower in Hispanic women than White women. In 2016, the incidence of uterine cancer among Hispanic women was 23.2 cases per 100,000 compared with 27.0 cases per 100,000 in White women. From 1999 to 2015, the incidence increased more significantly for Hispanic women (32% increase) than for White women (9% increase).5 Multiple retrospective cohort studies using national databases have shown that Hispanic women were younger at diagnosis.15–18
Most studies have concluded that Hispanic women have similar15,19 or improved survival17,20 compared with White women after controlling for tumor characteristics, age and other sociodemographic factors, cancer stage, and treatment. Using the National Cancer Database, Malagon-Blackwell et al17 noted improved 5-year survival for endometrial cancer for Hispanic women compared with non-Hispanic White women (83.1 vs 81.4%). Using SEER data, Bregar et al20 noted improved survival (HR 0.87, 95% CI 0.00–0.93) in Hispanic women compared with non-Hispanic White women with high-grade endometrial cancers.
Asian/Pacific Islander Women
In 2016, the CDC reported that the uterine cancer incidence rate was 19.2 cases per 100,000 women for Asian/Pacific Islander women, lower than for Black and White women. There was a larger increase in incidence rates from 1999 to 2016 for Asian/Pacific Islander women (38%) than for White women (9%).5
Recent studies show Asian/Pacific Islander women have a similar mortality to White women for uterine cancer. An older retrospective cohort study from 2003 using the Department of Defense's centralized tumor registry found that Asian/Pacific Islander women had higher-grade endometrial cancer tumors, less favorable histologic subtypes, and significantly worse 5-year survival rates compared with White women (77% vs 91%, P<.01).21 Uterine cancer deaths among Asian/Pacific Islander women increased by 52% from 1999 to 2016, more than the concurrent increase noted in White women (18%). In 2015, Asian/Pacific Islander women had similar uterine cancer death rates to White women (4 vs 5/100,000).5 Rojas et al14 noted similar death rates between Asian/Pacific Islander and White women in patients with uterine carcinosarcoma (HR 1.10, 95% CI 0.93–1.29). Terada et al22 noted no difference in overall mortality rates for endometrial cancer between Native Hawaiian and other Pacific Islander women compared with other women. In separate analyses of SEER data from 1988 to 2009 and from 2000 to 2011, Asian women had better overall and cancer-specific mortality than non-Hispanic White women.8,23
American Indian/Alaska Native Women
American Indian/Alaska Native women appear to have lower uterine cancer incidence rates than other groups. In 2016, the CDC reported that the uterine cancer incidence rate for American Indian/Alaska Native women was 23.1 per 100,000 women. This rate was lower than for Black and White women. Rates increased 53% from 1999 to 2016.5 Between 1974 and 2003, Alaska Native women had significantly lower incidence rates of uterine cancer compared with White women.24
Clear conclusions about disparities in uterine cancer outcomes for American Indian/Alaska Native women are difficult to make given the few studies available, each containing small numbers of patients. Death rates from uterine cancer were similar between American Indian/Alaska Native and White women in Indian Health Service Contract Health Service Delivery Areas.25 There was significant variation by Indian Health Service region, with uterine cancer death rates in American Indian/Alaska Native women exceeding the rates for White women in the Northern Plains, Southern Plains, Southwest, and Pacific Coast regions.25 A small, retrospective cohort study of high-risk endometrial cancer subtypes in women of Lumbee Native American ancestry found no association between such ancestry and worse overall or disease-specific survival.26
Disparities by Immigration Status
Several studies assessed the association of immigration status with uterine cancer outcomes, with conflicting results. Among Asian women diagnosed with endometrial cancer in the United States, outcomes appear to be the same or better in foreign-born women. Mahdi et al23 noted better overall and cancer-specific survival in Asian immigrants than in Asian individuals born in the United States. In an analysis of SEER data from 2001 to 2009, U.S.-born Asian women had a significantly higher proportion of type 1 endometrial cancers than foreign-born Asian women, but 5-year survival for type 1 disease was 92% in both groups.27 Creque et al28 found no difference in overall uterine cancer survival between U.S.-born Black women and foreign-born Black women in Brooklyn, although the authors did observe different predictors of survival in the two groups. Using SEER data, Mahdi et al19 noted better overall and cancer-specific survival in immigrant Hispanic White women compared with U.S.-born Hispanic White women with type 2 endometrial cancer. Rodriguez et al16 used SEER data from 2000 to 2010 and noted risk of cancer death was not statistically significantly different in U.S.-born Hispanic women (HR 1.16, 95% CI 0.99–1.36), but was increased for foreign-born Hispanic women (HR 1.31, 95% CI 1.12–1.52) compared with non-Hispanic White women from 2006 to 2010 among women with any type of endometrial cancer. This study was limited by the birthplace being unknown for 52% of Hispanic women.16 In a study of women in Sweden, foreign-born women had the same rates of stage I and advanced cancers as native-born women.29
Disparities in Care
Stage at Diagnosis
Stage of disease at time of diagnosis varied by racial and ethnic group, with advanced disease more frequent in Black and Hispanic women than in White women. In the most recent CDC report, stage at diagnosis varied across racial and ethnic groups, with a localized disease incidence per 100,000 women of 18.7 in White women, 14.5 in Black women, 15.6 in American Indian/Alaska Native women, 12.8 in Asian/Pacific Islander women, and 14.9 in Hispanic women.5 In a review of five population-based studies and one single-institution study totaling nearly 148,000 women, Black women were more likely to present with more advanced disease than White women. In the review's pooled analysis, 54% of Black women presented with localized disease, compared with 71% of White women (P<.001).30 Non-Hispanic Black individuals were more likely than non-Hispanic White individuals to present with advanced disease in a study of women with uterine carcinosarcoma. The risk of Black women presenting with advanced disease persisted after adjusting for age, tumor grade, and histology.13 Three retrospective cohort studies using national databases reported that Hispanic women were more likely to have later-stage disease than non-Hispanic White women.15–17 (See Box 2 for a summary of disparities in care.)
Box 2. Disparities in Uterine Cancer Diagnosis and Treatment.
Diagnosis
• Advanced stage at diagnosis is more common in Black and Hispanic women.5,13,15–17,30
• Black women are more likely to be diagnosed with nonendometrioid (ie, aggressive) histologies.3,8,18
• Black women are less likely to receive guideline-concordant diagnostic procedures.53
Treatment differences
• Black and Hispanic women are less likely to receive surgery, hysterectomy, or definitive surgical treatment.12,15,16,20,30–35
• Minimally invasive surgery is performed less frequently in Black and Hispanic women.20,36–41
• Black and Hispanic women are less likely to have lymph node sampling or dissection.20,30,42,43
• Black women are less likely to receive chemotherapy.31
•Black women are similarly10,13,32,44 or more likely to receive adjuvant radiation therapy.*,45
• Black women are more likely to be cared for by high-volume uterine cancer surgeons, by gynecologic oncologists, and at National Cancer Institute Centers.50,52
Guideline-concordant care
• Black, Hispanic, and American Indian/Alaska Native women are less likely to have guideline-compliant treatment.18,48,51,53
*May reflect higher incidence of advanced disease in Black women, for which studies did not control.
Treatment Differences
Numerous differences have been shown in uterine cancer treatment between racial and ethnic groups. Black and Hispanic women were less likely to receive surgery for treatment of cancer and less likely to have the optimal surgical procedure. Multiple studies extending back more than 20 years show that Black women are significantly less likely to undergo surgery for uterine cancer, to undergo hysterectomy, or to have definitive surgical treatment than White women across all cancer stages and grades.20,30–35 Among those who did undergo surgery, minimally invasive surgery was performed less frequently in Black and Hispanic women.20,36–41 In the most recent American College of Surgeons National Surgical Quality Improvement Project (2010–2015), 49.3% of Black women and 71.3% of White women undergoing hysterectomy for endometrial cancer underwent laparoscopic procedures.38 Although Black and Hispanic women have positive lymph nodes more frequently than White women, Black and Hispanic women had lower rates of lymph node sampling, adequate node sampling, or sentinel lymph node biopsy.20,30,42,43 Hispanic women were less likely to undergo hysterectomy, lymphadenectomy, and definitive surgical treatment than White women.12,15,16,20
We found only one study about chemotherapy. In a multivariate analysis of the SEER Medicare database, Black women with high-grade endometrial cancer were less likely to receive chemotherapy than White women.31
Black women were similarly as likely as White women to receive adjuvant radiation therapy.10,13,32,44 A single study reported higher rates.45 The authors did not conduct a multivariate analysis but postulated that this difference was likely from the higher frequency of advanced disease. Fedewa et al noted that rates of adjuvant therapy (radiation, chemotherapy, and chemoradiation) were “not drastically different across race/ethnic categories.”34 The observed similar rates may be misleading, because Black women more frequently had aggressive cancers that require adjuvant therapy, and many of these studies did not perform multivariate analysis.10
In a modelling study, after controlling for treatment differences and stage, the absolute difference in 5-year survival between Black and White women narrowed from 19.3% to 11.6%. Based on this model, approximately 40% of the Black–White gap in uterine cancer mortality was explained by disparate surgery rates and stage at diagnosis. Chemotherapy was not included in the model, potentially underestimating the effect of inequitable treatment on the disparity in survival.46
Access to High-Volume Surgeons or High-Volume Surgical Centers
Despite these disparities in treatment, the literature suggests that Black patients are more likely to receive care at high-volume facilities and at academic centers.47–51 In an analysis of SEER registries spanning 1991–1999, Black women were more likely to have a gynecologic oncologist perform their surgery and to be treated at hospitals that had high volumes, that were National Cancer Institute Centers, and where a greater proportion of surgeries were performed by gynecologic oncologists.50 Similarly, in analysis of the National Cancer Database from 1998 to 2012, Black women were more likely than White women to receive care at a high-volume center, but Black women with early stage disease still experienced an increased risk of death (HR 1.19, 95% CI 1.03–1.38) at high-volume hospitals compared with White women treated at similar hospitals.47 In this study, increased hospital volume mitigated but did not eliminate racial disparities in endometrial cancer survival. In a retrospective cohort study of discharge data from nonfederal acute care hospitals in Maryland from 2000 to 2009, Black women were more likely to be operated on by surgeons who performed high volumes of uterine cancer surgery (adjusted odds ratio [aOR] 1.27, 95% CI 1.09–1.49) but were less likely to undergo minimally invasive surgery (aOR 0.60, 95% CI 0.45–0.80).52 We found no studies examining multidisciplinary care, access to uterine cancer clinical trials, navigation, or supportive oncology services such as those required for Comprehensive Cancer Center accreditation.
Receipt of Guideline-Concordant Care
Our review found several studies examining disparities in guideline-concordant care between racial and ethnic groups. Overall, Black and Hispanic women were less likely than White or Asian/Pacific Islander women to receive guideline-concordant care. In an analysis using the SEER database, Black women enrolled in Medicare were less likely to have bleeding characterized as postmenopausal, to have bleeding documented, or to undergo appropriate diagnostic procedures. Black women were less likely to undergo guideline-concordant diagnostic evaluation compared with White women (aOR 0.63, 95% CI 0.51–0.77), a finding associated with advanced stage at diagnosis.53 In a study of compliance with National Comprehensive Cancer Network management guidelines using the National Cancer Database, Black women with endometrioid endometrial cancer had lower odds of guideline-concordant treatment than White women (odds ratio [OR] 0.92, 95% CI 0.86–0.98). Lack of guideline-concordant treatment was associated with lower overall survival in the overall study population, but was not significantly associated in non-Hispanic Black women, likely because of a lack of power.51 Although no difference was reported in receipt of guideline-concordant care by race or ethnicity among women diagnosed with nonendometrioid endometrial carcinoma,54 a 2020 analysis using the National Cancer Database from 2004 to 2016 found that White women were more likely to receive endometrial cancer care concordant with five evidence-based quality metrics than Black women and that adherence to evidence-based care was associated with a lower mortality rate.48 Black women who received guideline-concordant care experienced improved but still inferior outcomes compared with White women.48 Kaspers et al51 noted decreased guideline compliance in the care of Hispanic women (OR 0.90, 95% CI 0.83–0.97) and increased guideline compliance in the care of Asian/Pacific Islander women (OR 1.11, 95% CI 1.00–1.23) compared with White women in their analysis of the National Cancer Database. These findings were replicated by Rodriguez et al18 in a recently published retrospective population-based cohort analysis of SEER data from 2006 to 2015.18 Black, Hispanic, and American Indian/Alaska Native women were significantly less likely to receive guideline-adherent treatment for endometrial cancer compared with White women; Asian and Native Hawaiian/Pacific Islander women had greater odds of receiving guideline-adherent treatment.
Chemotherapy Response
In attempts to explain the survival difference between Black and White women, an analysis of data from four Gynecologic Oncology Group trials evaluating the role of chemotherapy on stage III–IV or recurrent endometrial cancer is frequently cited.55 This analysis, which sought to “determine whether race influenced the survival” of women with advanced endometrial cancer, found that Black women had lower survival than White women in multivariate analysis; the authors concluded that this difference in survival was due to decreased tumor response to the chemotherapy agents among Black women.55 Further analysis of these data has challenged this interpretation, finding that the reported survival was related to chemotherapy dose received and that dose-dependent response was not modified by race.56
Disparities by Socioeconomic Status
Disadvantaged socioeconomic status was associated with worse outcomes. This association was present whether using single measures, including income, educational level, and insurance type, or composite measures of socioeconomic status. A systematic review found nine studies conducted in four countries including 369,000 women using a variety of measures of socioeconomic deprivation. Eight studies investigated survival and socioeconomic deprivation; the majority showed that socioeconomic deprivation was associated with worse survival from endometrial cancer. One study found no relationship between socioeconomic deprivation and 30-day postoperative mortality. The authors were unable to provide summary estimates of the strength of the association given the many different measures used.57
Neighborhood socioeconomic status was found to be associated with endometrial cancer mortality. One study in a systematic review57 measured neighborhood socioeconomic status and noted a 3% decrease in cancer-specific survival associated with living in a low-income neighborhood.58 In a retrospective review of the California Cancer Registry, neighborhood socioeconomic status was associated with higher risk of endometrial cancer mortality, and Hispanic and Asian/Pacific Islander women in the lowest socioeconomic status neighborhoods had an increased risk of overall and endometrial cancer-specific mortality compared with women of the same race and ethnicity in the highest socioeconomic status neighborhoods.59 Lower neighborhood socioeconomic status was also associated with decreased survival as well as decreased odds of receiving guideline-adherent treatment for endometrial cancer in a recent analysis of retrospective population-based data.18,60 On multivariate analysis, there was a decline in the odds of receiving guideline-concordant treatment by neighborhood socioeconomic status such that women in the high-middle neighborhood socioeconomic status group had an OR of 0.89 (95% CI 0.86–0.93) followed by the middle socioeconomic status group (OR 0.84, 95% CI 0.80–0.88), the low-middle socioeconomic status group (OR 0.80, 95% 0.78–0.86), and the lowest socioeconomic status group (OR 0.73, 95% CI 0.69–0.77).18
Level of education was a significant predictor of worse endometrial cancer incidence and mortality. A systematic review included four studies examining education.57 Three (two in Denmark, one in Japan) showed less education to be associated with worse outcomes; the one study conducted in the United States did not show an association. Having a lower level of education was significantly associated with a higher proportion of higher-stage endometrioid endometrial cancer in patients aged 50–74 year at diagnosis in West Sweden.29
Income was inversely associated with endometrial cancer outcomes in some studies, but not in others. In a systematic review that included five studies examining income,57 one U.S. study and one U.K. study did not show an association with income, and a study from Denmark showed a trend toward better 1-year and 5-year survival with higher income. Two U.S. studies showed worse outcomes with lower income. One, a 2004 analysis of SEER Cancer Registry data from Detroit, found a higher median household income was associated with a decreased risk for death after adjusting for stage, age, treatment, and histology.13 The other showed worse disease-specific survival and a trend toward decreased overall survival for women in the lower household income group with stage I and II endometrioid carcinoma; however, on multivariate analysis, income no longer was a significant predictor of patient outcomes.61 A 2017 analysis of the U.S. National Cancer Database showed an association between highest income (defined as top quartile for median household income for ZIP code of residence) and improved overall survival among individuals with high-grade endometrial cancer.20
Having no or publicly funded insurance has been associated with advanced stage at diagnosis and differences in receipt of treatment and survival. A study using the National Cancer Database from 2000 to 2001 found that uterine cancer patients without private health insurance had worse overall survival, including among patients with early-stage disease.34 The HR for death at 4 years from stages I–III uterine cancer was higher for individuals with Medicare insurance aged 18–64 years (HR 2.49, 95% CI 2.10–2.95) and aged 65–99 years (HR 1.22, 95% CI 1.11–1.34), individuals with Medicaid insurance (HR 1.70, 95% CI 1.46–1.99), and uninsured individuals (HR 1.44, 95% CI 1.20–1.72) in comparison with those with private insurance.34 A separate analysis of patients from the same data set from 1998 to 2012 had similar findings.47 In women diagnosed with endometrial cancer from 1998 to 2010 in the National Cancer Database, public insurance or no insurance was associated with a number of adverse outcomes. Having Medicare (OR 1.14, P<.001) or Medicaid (OR 1.76, P<.001) insurance was associated with advanced-stage disease at time of diagnosis. Uninsured patients were at higher risk for not receiving hysterectomy as primary therapy (OR 1.32, P=.006). Compared with private insurance, all other payer categories were associated with decreased overall survival in all patients and in patients with advanced-stage disease.12 In data from the Nationwide Inpatient Sample from 2007 to 2011, minimally invasive surgery was less likely to be performed in patients with Medicaid than in those with private insurance (aOR 0.67, 95% CI 0.62–0.72).37 These findings were replicated using the same database in 2012,36 although a study using this database from 2012 to 2013 reported that individuals with Medicaid insurance were less likely to undergo open surgery in comparison with patients with private insurance.40 Women with public insurance were more likely to travel more than 50 miles to obtain endometrial cancer surgery. No significant travel difference was noted between uninsured and privately insured patients.62
Even in settings that offer universal health care, marginalization (as defined by validated indices associated with social determinants of health) was persistently associated with worse outcomes. A systematic review that included two studies each from Denmark and the United Kingdom showed worse outcomes with deprivation.57 In a Canadian study, marginalization, as measured by an adaptation of the Canadian Marginalization Index, was associated with increased risk of advanced-stage endometrial cancer, despite adjustment for age, obesity, comorbidities, and disease histology.63
Only a few studies evaluated the correlation of race with socioeconomic status in their analyses of uterine cancer disparities. Madison et al13 showed collinearity of race with median family income and reported that either race (or ethnicity) or income, but not both, was associated with advanced stage at diagnosis. Although Dolly et al64 also found collinearity between Black race and Hispanic ethnicity and Medicaid insurance, the authors did not explain how race, ethnicity, and insurance type interacted to contribute to a longer delay between diagnosis and treatment for individuals identifying as Black or Hispanic or having Medicaid insurance. Fedewa et al34 used a stepwise approach to evaluate the effect of education and insurance on racial survival disparities. With this statistical approach, the HR of death from uterine cancer among Hispanic individuals lost its statistical significance when adjusted for ZIP code level education; the HR for Black individuals declined by 24% when adjusted for education and 4% when adjusted for insurance but still remained significantly elevated.
Other Potential Contributors
Histologic Subtypes
Among women with endometrial cancer, Black women have a higher incidence of nonendometrioid endometrial cancers. In SEER data, non-Hispanic Black women were significantly more likely to be diagnosed with clear cell tumors, carcinosarcoma, and serous tumors than non-Hispanic White, Hispanic, or Asian women.3,8,18 Tumors with aggressive histology accounted for 53% of mortality among Black women, compared with 36% mortality among White women.3 The disproportionate burden of high-risk histology among Black women contributes to their lower 5-year survival rates. However, even among women with aggressive histologic subtypes, Black women have a significantly higher mortality rate than White women, with Black women having mortality rate ratios ranging from 1.52 to 2.90 for the different high-risk histologic subtypes.8,42
Molecular and Genetic Factors
A detailed review of molecular and genetic factors was beyond the scope of this review. Doll et al65 in their Public Health Critical Race Praxis systematic review summarized 11 studies investigating genetic and molecular differences by race. They noted that seven reported negative findings and three reported preliminary evidence for potential differences in molecular markers related to survival. They cited a final Gynecologic Oncology Group-sponsored investigation that did not find any African ancestry-specific single nucleotide polymorphisms associated with worse progression-free survival.66 Although the findings around molecular differences by race are conflicting, Doll et al noted that the studies with positive findings are frequently cited to explain racial disparities in uterine cancer outcomes.
Comorbidities
Two recent studies examined the potential role of differences in prevalence of medical comorbidities such as diabetes, hypertension, and obesity between Black and White women as explanations for the racial disparity in endometrial cancer mortality.67,68 In both studies, a higher comorbidity score was associated with worse overall survival in both Black and White women but not with cancer-specific survival. In a study using the SEER-Medicare database of women diagnosed with endometrial cancer between 2000 and 2005, both Black and White women with diabetes or other conditions had poorer overall survival.67 Diabetes was associated with worse disease-specific survival in White individuals but not in Black individuals. Black women with hypertension had better overall survival (HR 0.74, 95% CI 0.60–0.92). Although Black women still had poorer overall survival (HR 1.16, 95% CI 1.05–1.28) and disease-specific survival (HR 1.27, 95% CI 1.08–1.49) than White women in the multivariate model, the authors reported that both disease-specific and overall survival for Black women changed only minimally after adjustment for comorbidity. In a retrospective cohort study from a large urban integrated health center, diabetes was associated with worse overall survival in White women but not in Black women.68 Again, hypertension was associated with improved overall survival for Black individuals and with better disease-specific survival for both White and Black individuals. In this single institution study, the disparity in overall survival between Black and White women was attenuated after controlling for clinical prognostic factors and comorbid conditions studies. However, Black women still had a significant increased risk of death from endometrial cancer (HR 2.27, 95% CI 1.39–1.68).68 In both studies, the higher prevalence of comorbidities among Black women did not explain the observed differences in endometrial cancer survival by race, and excess uterine cancer mortality experienced by Black women persisted even after controlling for comorbidities.67,68
DISCUSSION
Our review revealed stark racial disparities in uterine cancer (summarized in Box 3). For Black women, these disparities pervade the entire spectrum of care, including risk factors, comorbidities, diagnosis, treatment, and outcomes. Black women with uterine cancer have substantially higher mortality rates and worse survival rates than women of any other race or ethnicity. They are approximately twice as likely to die from uterine cancer than White women. Studies repeatedly and consistently demonstrate that Black women experience a disproportionate risk of death from uterine cancer, particularly endometrial cancer. Our review was not constructed to assess the time course of knowledge about disparities, but these disparities were well established in the earliest articles we reviewed from more than 25 years ago and persisted without change in all studies since. Numerous studies demonstrate that Black and Hispanic women were far less likely than White women to receive optimal care in accordance with national guidelines.
Box 3. Summary of Areas of Racial and Ethnic Uterine Cancer Health Disparities Found in Literature Search.
Areas in which endometrial cancer health disparities were noted:
-
• Outcomes
○ Incidence
○ Mortality
-
• Care
-
○ Diagnostic differences
▪ Higher stage at diagnosis
▪ Histology
▪ Appropriate diagnostic procedure
-
○ Treatment differences
▪ Having surgery
▪ Having optimal surgery
▪ Having minimally invasive surgery
▪ Rate of lymph node sampling
▪ Receipt of chemotherapy
○ Guideline-concordant care
-
Areas in which endometrial cancer health disparities were not noted:
• Chemotherapy response
• Molecular and genetic factors
• Comorbidities (different rates of comorbidities, but not explaining observed differences in mortality)
• Access to gynecologic oncologists and high-volume hospitals
Disparities in uterine cancer mortality were not reported among other racial and ethnic groups, including American Indian/Alaska Native, Asian/Pacific Islander, and Hispanic women. Data from the CDC have shown a progressive rise in mortality rates in all groups, with rates in women of color rising faster than in White women, suggesting that disparities may emerge over time if this trend continues.5 The absence of a disparity in mortality in Hispanic individuals has been observed in other areas of health and has been termed the “Hispanic paradox,” in which Hispanic individuals face significant social and structural barriers to optimal health similar to Black individuals but do not experience similar health disparities.69 For endometrial cancer, the mechanisms behind this paradox are unclear, but there is speculation that lower overall mortality risks among adult Hispanic women, particularly foreign-born Hispanic women, contribute to differences in survival in uterine cancer.17,20 Lower socioeconomic status, as defined by education, income, neighborhood indices of socioeconomic status, and insurance type, was associated with advanced stage of uterine cancer at diagnosis and decreased survival.
Some factors causing significant disparities in uterine cancer survival have been identified. Tumor histology and cancer stage are well-known prognostic factors in cancer outcomes, and significant racial and ethnic disparities in histology and stage of uterine cancer at the time of diagnosis are clear. Given the disparities in diabetes, hypertension, and obesity observed nationally between Black and White women, it has been theorized that the disproportionate prevalence of comorbidities among Black individuals with uterine cancer contributes to their worse survival outcomes. Our literature search did not bear this out; excess uterine cancer mortality among Black women persisted in studies specifically studying the effect of medical comorbidities. Profound inequities were noted in treatment, with Black and Hispanic women receiving less surgery overall, less optimal surgery, including minimally invasive approach and lymphadenectomy, and less chemotherapy. Even the observed similar rates of radiation therapy may be more reflective of advanced disease in Black women than equitable use of radiation. Multiple studies used multivariate analyses to control for observed differences in comorbidities, stage at diagnosis, histologic tumor type, and treatment disparities, and most still reported worse outcomes for Black women even when controlling for these factors, demonstrating that our understanding of the forces driving the inequities is incomplete.
There have been repeated attempts to explain the outcome disparities that persist after controlling for known differences. Many of these explanations have proposed genetic and biological differences between different racial and ethnic groups. No clear differences have been found, which is to be expected given that race is a social, not biological, construct. The course of thought on differing responses to chemotherapy offer a cautionary example. The initial conclusions, which assumed receipt of identical treatment, were interpreted as evidence of molecular or genetic factors contributing to racial disparities70,71; however, with appropriate re-analysis of the data, the initially described differences between Black and White patients disappeared.56,65 Doll cited this progression of thought around chemotherapy response as an example of how racial differences in overall survival are frequently construed in the medical literature as evidence of biological differences between Black and White women.65 We found profound disparities in stage at diagnosis, histology, and treatment between racial and ethnic groups that are not explained by underlying disease and likely reflect a complex interplay of sources, including health system factors and large-scale societal forces such as structural racism and poverty. Despite the persistent racial gap in endometrial cancer survival for decades, we found no studies that explicitly explored the effect of racism, discrimination, and bias in uterine cancer.
Although many researchers strive to disentangle race and socioeconomic status, the ultimate question remains why determining the independent effect of race and ethnicity or socioeconomic status is necessary to disrupting disparities and how it may obfuscate the effect of racism on health outcomes. It is well accepted that race, ethnicity, and socioeconomic status are intimately intertwined in this country—racism and poverty represent overlapping and interlocking forms of systemic oppression that lead to differential access to power, money, and resources, including education, housing, insurance, and health care.72 If we look to the U.S. maternal mortality crisis, we see that high socioeconomic status is not a protective factor for Black birthing individuals. Recent data show that Black women with at least a college degree or higher still experienced a higher pregnancy-related mortality ratio than White women who did not graduate from high school (40.2 pregnancy-related deaths/100,000 births vs 25.0, respectively); even more so, among those with at least a college education, the pregnancy-related mortality ratio for Black birthing individuals was 5.2 times that of White birthing individuals.73 In the uterine cancer disparities literature, racial and ethnic disparities were attenuated but frequently persisted when socioeconomic status covariates were included in multivariate analysis. The endurance of racial and ethnic disparities in uterine cancer and the correlation of race and socioeconomic status reinforce the need to explore how systemic inequities lead to differential outcomes for historically marginalized communities.
We noted key gaps in the literature. The preponderance of studies focused on disparities between Black and White women. Significantly fewer studies involved other races or ethnicities. We found no studies exploring uterine cancer outcomes among populations that are systemically disadvantaged by their sexual orientation, gender identity, rural geography, or other marginalized identities. Most studies were done with national databases, which do not provide enough detail to study systemic, practitioner, and patient factors. Few studies explored the experiences of Black women and individuals from marginalized groups around their diagnosis and treatment of uterine cancer.65,74
Literature in our review was significantly limited by the conceptualization and interpretation of race. Race was rarely defined beyond the self-reported racial categories used in data collection and was frequently interpreted as a biological construct in the discussion sections of articles.65 Using a traditional biomedical framework, article authors implied that biological explanations existed for the stark racial disparities in uterine cancer, obscuring the study of nonbiological factors that underlie the inequities. Contemporary interpretations of race insist that race is a social construct that, “connotes unequal allocation of opportunity and resources” based on social stratification.65 We found no studies explicitly exploring the effect of racism in the diagnosis and treatment of uterine cancer. There was a significant gap in the literature on the role of nonclinical systemic factors in the disparities.
The findings of our review highlight key obligations for us as health care professionals and researchers. Many of the disparities summarized in this document are modifiable. However, we found no published studies of interventions to reduce racial disparities in uterine cancer care, and Doll et al65 noted, “a complete lack of intervention studies to address persistent treatment inequity,” including disparities in surgery, radiation therapy, and chemotherapy. We must prioritize achieving equity in diagnosis and treatment, ensuring that all individuals, especially those from communities that have been socially disadvantaged, have access to early diagnosis and guideline-concordant care. Multiple articles demonstrated that improved access to high-quality, evidence-based care mitigates but does not eliminate disparities in uterine cancer.
Although the literature frequently used biological, genetic, or tumor-related factors to explain disparities, the findings in this review reinforce the need to abandon the interpretation of survival disparities in groups experiencing social disadvantage as biological in nature, because this distracts from addressing the structural forces and inequities that affect uterine cancer outcomes. In line with the American College of Obstetricians and Gynecologists' Joint Statement on Collective Action Addressing Racism, there must be a commitment to ensure “that race is not treated as a biologic factor” for uterine cancer and to lead research that “ethically addresses the needs of Black and Indigenous populations and populations of color” and other marginalized groups.75 Some researchers have called for journals to reject articles on racial health disparities that do not examine the role of racism in creating and perpetuating such disparities.76 It is also important to remember that there are individuals and communities whose voices and even inclusion have been missing from uterine cancer studies, such as sexual and gender minority individuals. If we approach health disparities as “avoidable, unfair, and unjust,”77 then we, as health care professionals and researchers, have an obligation to shift the focus of health disparities research in uterine cancer to modifiable, nonbiological factors that affect and perpetuate disparities. But even more so, we must work to understand and disrupt the larger structural forces that affect uterine cancer outcomes, especially for Black women, for women of lower socioeconomic status, and for other populations most at risk of stigma, oppression, exclusion, and lack of services. We recognize that the disparities we are reporting have been available in the literature for years. Despite decades of published studies characterizing and quantifying uterine cancer disparities, we found no evidence that gaps in uterine cancer outcomes have narrowed and no studies on interventions to reduce or eliminate these disparities. We hope that summarizing and highlighting these significant disparities in a single review will help amplify the call for work to address these inequities and build greater momentum and urgency around improving uterine cancer outcomes for the communities and populations most affected.
Footnotes
Supported by the Centers for Disease Control and Prevention (CDC) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement number 6 NU38OT000287-03-03, which was awarded to the American College of Obstetricians and Gynecologists (ACOG).
The authors thank Jean Riedlinger, MSLS, AHIP, Yvonnada McNeil, MSLS, Elizabeth York, MPH, and Jessica Butler, MPH, for their assistance with the database searches; Dana Trevas, Nancy O'Reilly, MHS, PMP, and Apurvi Shah, MPH, for facilitating the management of the review and editing process; and the individuals who attended the January 2021 Uterine Cancer Evidence Review Conference, listed in Appendix 1 online at http://links.lww.com/AOG/C618, for their discussion, input, and comments.
Financial Disclosure Sangini Sheth is a past consultant for Merck & Co., Inc., and a research study grant recipient (drug only: HPV vaccine) from Merck & Co., Inc. She was paid costs of travel and meeting registration (paid directly) and received honoraria payment for an education course from the ASCCP. She also has research grants from the NIH and CDC for studies unrelated to the submitted work. Rebecca Brooks is a member of an AstraZeneca speakers' bureau related to ovarian cancer, a past advisory board member and consultant for GSK and Merck & Co., Inc., and a past non-branded speaker for Clinical Care Options. Brett Worly is an unpaid speaker for AbbVie, Inc. David Chelmow is the president of ASCCP and immediate past president of the Council of University Chairs of Obstetrics and Gynecology, receives a stipend as the editor-in-chief of the Medscape Obstetrics and Gynecology Clinical Reference Book, and was on the American Board of Obstetrics and Gynecology Board of Directors during the evidence review and manuscript writing period. All authors received a one-time payment from ACOG for their participation in the development of uterine cancer educational materials.
Participation in this project as an attendee of the Evidence Review Conference does not constitute organizational or individual endorsement of the conclusions. Information in this article should not be construed as the official position or policy of, or should any endorsements be inferred by CDC, HHS, or the U.S. Government.
David Chelmow is a member of the United States Preventive Services Task Force (USPSTF). This article does not necessarily represent the views and policies of the USPSTF.
Each author has confirmed compliance with the journal's requirements for authorship.
Peer reviews and author correspondence are available at http://links.lww.com/AOG/C619.
Figure.

No available caption
REFERENCES
- 1.Centers for Disease Control and Prevention. Community Health and Program Services (CHAPS): health disparities among racial/ethnic populations. U.S. Department of Health and Human Services; 2008 [Google Scholar]
- 2.Chelmow D, Brooks R, Cavens A, Huber-Keener K, Scott DM, Sheth SS, et al. Executive summary of the Uterine Cancer Evidence Review Conference. Obstet Gynecol 2022:139:626–43. doi: 10.1097/AOG.0000000000004711 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sherman ME, Devesa SS. Analysis of racial differences in incidence, survival, and mortality for malignant tumors of the uterine corpus. Cancer 2003;98:176–86. doi: 10.1002/cncr.11484 [DOI] [PubMed] [Google Scholar]
- 4.Doll KM, Winn AN. Assessing endometrial cancer risk among US women: long-term trends using hysterectomy-adjusted analysis. Am J Obstet Gynecol 2019;221:318.e1–9. doi: 10.1016/j.ajog.2019.05.024 [DOI] [PubMed] [Google Scholar]
- 5.Henley SJ, Miller JW, Dowling NF, Benard VB, Richardson LC. Uterine cancer incidence and mortality – United States, 1999–2016. MMWR Morb Mortal Wkly Rep 2018;67:1333–8. doi: 10.15585/mmwr.mm6748a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.American Cancer Society. Cancer facts & figures 2021. Accessed July 1, 2021. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf [Google Scholar]
- 7.Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, Begg CB. Survival of Blacks and Whites after a cancer diagnosis. JAMA 2002;287:2106–13. doi: 10.1001/jama.287.16.2106 [DOI] [PubMed] [Google Scholar]
- 8.Cote ML, Ruterbusch JJ, Olson SH, Lu K, Ali-Fehmi R. The growing burden of endometrial cancer: a major racial disparity affecting Black women. Cancer Epidemiol Biomarkers Prev 2015;24:1407–15. doi: 10.1158/1055-9965.EPI-15-0316 [DOI] [PubMed] [Google Scholar]
- 9.DeSantis C, Naishadham D, Jemal A. Cancer statistics for African Americans, 2013. CA Cancer J Clin 2013;63:151–66. doi: 10.3322/caac.21173 [DOI] [PubMed] [Google Scholar]
- 10.Wright JD, Fiorelli J, Schiff PB, Burke WM, Kansler AL, Cohen CJ, et al. Racial disparities for uterine corpus tumors: changes in clinical characteristics and treatment over time. Cancer 2009;115:1276–85. doi: 10.1002/cncr.24160 [DOI] [PubMed] [Google Scholar]
- 11.Johnson AL, Medina HN, Schlumbrecht MP, Reis I, Kobetz EN, Pinheiro PS. The role of histology on endometrial cancer survival disparities in diverse Florida. PLoS One 2020;15:e0236402. doi: 10.1371/journal.pone.0236402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fader AN, Habermann EB, Hanson KT, Lin JF, Grendys EC, Dowdy SC. Disparities in treatment and survival for women with endometrial cancer: a contemporary National Cancer Database registry analysis. Gynecol Oncol 2016;143:98–104. doi: 10.1016/j.ygyno.2016.07.107 [DOI] [PubMed] [Google Scholar]
- 13.Madison T, Schottenfeld D, James SA, Schwartz AG, Gruber SB. Endometrial cancer: socioeconomic status and racial/ethnic differences in stage at diagnosis, treatment, and survival. Am J Public Health 2004;94:2104–11. doi: 10.2105/ajph.94.12.2104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rojas C, Tian C, Powell MA, Chan JK, Bateman NW, Conrads TP, et al. Racial disparities in uterine and ovarian carcinosarcoma: a population-based analysis of treatment and survival. Gynecol Oncol 2020;157:67–77. doi: 10.1016/j.ygyno.2020.01.017 [DOI] [PubMed] [Google Scholar]
- 15.Cook LS, Nelson HE, Cockburn M, Olson SH, Muller CY, Wiggins CL. Comorbidities and endometrial cancer survival in Hispanics and non-Hispanic Whites. Cancer Causes Control 2013;24:61–9. doi: 10.1007/s10552-012-0090-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rodriguez AM, Schmeler KM, Kuo YF. Disparities in endometrial cancer outcomes between non-Hispanic White and Hispanic women. Gynecol Oncol 2014;135:525–33. doi: 10.1016/j.ygyno.2014.10.021 [DOI] [PubMed] [Google Scholar]
- 17.Malagon-Blackwell EM, Seagle BL, Nieves-Neira W, Shahabi S. The Hispanic paradox in endometrial cancer: a National Cancer Database study. Gynecol Oncol 2017;146:351–58. doi: 10.1016/j.ygyno.2017.05.026 [DOI] [PubMed] [Google Scholar]
- 18.Rodriguez VE, LeBrón AMW, Chang J, Bristow RE. Racial–ethnic and socioeconomic disparities in guideline-adherent treatment for endometrial cancer. Obstet Gynecol 2021;138:21–31. doi: 10.1097/AOG.0000000000004424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mahdi H, Hou H, Kowk LL, Moslemi-Kebria M, Michener C. Type II endometrial cancer in Hispanic women: tumor characteristics, treatment and survival compared to non-Hispanic White women. Gynecol Oncol 2014;133:512–7. doi: 10.1016/j.ygyno.2014.03.562 [DOI] [PubMed] [Google Scholar]
- 20.Bregar AJ, Rauh-Hain JA, Spencer R, Clemmer JT, Schorge JO, Rice LW, et al. Disparities in receipt of care for high-grade endometrial cancer: a National Cancer Data Base analysis. Gynecol Oncol 2017;145:114–21. doi: 10.1016/j.ygyno.2017.01.024 [DOI] [PubMed] [Google Scholar]
- 21.Kost ER, Hall KL, Hines JF, Farley JH, Nycum LR, Rose GS, et al. Asian-Pacific Islander race independently predicts poor outcome in patients with endometrial cancer. Gynecol Oncol 2003;89:218–26. doi: 10.1016/s0090-8258(03)00050-7 [DOI] [PubMed] [Google Scholar]
- 22.Terada K, Carney M, Kim R, Ahn HJ, Miyamura J. Health disparities in native Hawaiians and other Pacific Islanders following hysterectomy for endometrial cancer. Hawaii J Med Public Health 2016;75:137–9. doi: 10.1016/s0090-8258(03)00050-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mahdi H, Schlick CJ, Kowk LL, Moslemi-Kebria M, Michener C. Endometrial cancer in Asian and American Indian/Alaskan Native women: tumor characteristics, treatment and outcome compared to non-Hispanic White women. Gynecol Oncol 2014;132:443–9. doi: 10.1016/j.ygyno.2013.11.028 [DOI] [PubMed] [Google Scholar]
- 24.Day GE, Lanier AP, Bulkow L, Kelly JJ, Murphy N. Cancers of the breast, uterus, ovary and cervix among Alaska Native women, 1974–2003. Int J Circumpolar Health 2010;69:72–86. doi: 10.3402/ijch.v69i1.17388 [DOI] [PubMed] [Google Scholar]
- 25.Singh SD, Ryerson AB, Wu M, Kaur JS. Ovarian and uterine cancer incidence and mortality in American Indian and Alaska Native women, United States, 1999–2009. Am J Public Health 2014;104(suppl 3):S423–31. doi: 10.2105/AJPH.2013.301781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhang C, Roque D, Ehrisman JA, DiSanto N, Broadwater G, Doll KM, et al. Lumbee Native American ancestry and the incidence of aggressive histologic subtypes of endometrial cancer. Gynecol Oncol Rep 2015;13:49–52. doi: 10.1016/j.gore.2015.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Simons E, Blansit K, Tsuei T, Brooks R, Ueda S, Kapp DS, et al. Foreign- vs US-born Asians and the association of type I uterine cancer. Am J Obstet Gynecol 2015;212:43.e1–6. doi: 10.1016/j.ajog.2014.07.019 [DOI] [PubMed] [Google Scholar]
- 28.Creque A, Taioli E, Attong-Rogers A, Ragin C. Disparities in uterine cancer survival in a Brooklyn cohort of Black women. Future Oncol 2010;6:319–27. doi: 10.2217/fon.09.169 [DOI] [PubMed] [Google Scholar]
- 29.Svanvik T, Marcickiewicz J, Sundfeldt K, Holmberg E, Stromberg U. Sociodemographic disparities in stage-specific incidences of endometrial cancer: a registry-based study in West Sweden, 1995–2016. Acta Oncol 2019;58:845–51. doi: 10.1080/0284186X.2019.1581947 [DOI] [PubMed] [Google Scholar]
- 30.Long B, Liu FW, Bristow RE. Disparities in uterine cancer epidemiology, treatment, and survival among African Americans in the United States. Gynecol Oncol 2013;130:652–9. doi: 10.1016/j.ygyno.2013.05.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rauh-Hain JA, Buskwofie A, Clemmer J, Boruta DM, Schorge JO, del Carmen MG. Racial disparities in treatment of high-grade endometrial cancer in the Medicare population. Obstet Gynecol 2015;125:843–51. doi: 10.1097/AOG.0000000000000605 [DOI] [PubMed] [Google Scholar]
- 32.Randall TC, Armstrong K. Differences in treatment and outcome between African-American and White women with endometrial cancer. J Clin Oncol 2003;21:4200–6. doi: 10.1200/JCO.2003.01.218 [DOI] [PubMed] [Google Scholar]
- 33.Sud S, Holmes J, Eblan M, Chen R, Jones E. Clinical characteristics associated with racial disparities in endometrial cancer outcomes: a Surveillance, Epidemiology and End Results analysis. Gynecol Oncol 2018;148:349–56. doi: 10.1016/j.ygyno.2017.12.021 [DOI] [PubMed] [Google Scholar]
- 34.Fedewa SA, Lerro C, Chase D, Ward EM. Insurance status and racial differences in uterine cancer survival: a study of patients in the National Cancer Database. Gynecol Oncol 2011;122:63–8. doi: 10.1016/j.ygyno.2011.03.010 [DOI] [PubMed] [Google Scholar]
- 35.Hicks ML, Phillips JL, Parham G, Andrews N, Jones WB, Shingleton HM, et al. The national cancer data base report on endometrial carcinoma in African-American women. Cancer 1998;83:2629–37. doi: 10.1002/(SICI)1097-0142(19981215)83:12<2629::AID-CNCR30>3.0.CO;2-2 [DOI] [PubMed] [Google Scholar]
- 36.Esselen KM, Vitonis A, Einarsson J, Muto MG, Cohen S. Health care disparities in hysterectomy for gynecologic cancers: data from the 2012 National Inpatient Sample. Obstet Gynecol 2015;126:1029–39. doi: 10.1097/AOG.0000000000001088 [DOI] [PubMed] [Google Scholar]
- 37.Fader AN, Weise RM, Sinno AK, Tanner EJ, III, Borah BJ, Moriarty JP, et al. Utilization of minimally invasive surgery in endometrial cancer care: a quality and cost disparity. Obstet Gynecol 2016;127:91–100. doi: 10.1097/AOG.0000000000001180 [DOI] [PubMed] [Google Scholar]
- 38.Lee J, Gerber D, Aphinyanaphongs Y, Curtin JP, Boyd LR. Laparoscopy decreases the disparity in postoperative complications between Black and White women after hysterectomy for endometrial cancer. Gynecol Oncol 2018;149:22–7. doi: 10.1016/j.ygyno.2017.10.033 [DOI] [PubMed] [Google Scholar]
- 39.Mahdi H, Lockhart D, Moslemi-Kebria M, Rose PG. Racial disparity in the 30-day morbidity and mortality after surgery for endometrial cancer. Gynecol Oncol 2014;134:510–5. doi: 10.1016/j.ygyno.2014.05.024 [DOI] [PubMed] [Google Scholar]
- 40.Mannschreck D, Matsuno RK, Moriarty JP, Borah BJ, Dowdy SC, Tanner EJ, 3rd, et al. Disparities in surgical care among women with endometrial cancer. Obstet Gynecol 2016;128:526–34. doi: 10.1097/AOG.0000000000001567 [DOI] [PubMed] [Google Scholar]
- 41.Moss EL, Morgan G, Martin AP, Sarhanis P, Ind T. Surgical trends, outcomes and disparities in minimal invasive surgery for patients with endometrial cancer in England: a retrospective cohort study. BMJ Open 2020;10:e036222. doi: 10.1136/bmjopen-2019-036222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mahdi H, Han X, Abdul-Karim F, Vargas R. Racial disparity in survival of patients with uterine serous carcinoma: changes in clinical characteristics, patterns of care and outcomes over time from 1988 to 2011. Gynecol Oncol 2016;143:334–45. doi: 10.1016/j.ygyno.2016.03.002 [DOI] [PubMed] [Google Scholar]
- 43.Albright BB, Nasioudis D, Byrne ME, Latif NA, Ko EM, Haggerty AF. Perioperative outcomes and disparities in utilization of sentinel lymph node biopsy in minimally invasive staging of endometrial cancer. Gynecol Oncol 2020;159:758–66. doi: 10.1016/j.ygyno.2020.09.032 [DOI] [PubMed] [Google Scholar]
- 44.Elshaikh MA, Munkarah AR, Robbins JR, Laser BS, Bhatt N, Cogan C, et al. The impact of race on outcomes of patients with early stage uterine endometrioid carcinoma. Gynecol Oncol 2013;128:171–4. doi: 10.1016/j.ygyno.2012.10.016 [DOI] [PubMed] [Google Scholar]
- 45.Ozen A, Falchook AD, Varia MA, Gehrig P, Jones EL. Effect of race and histology on patterns of failure in women with early stage endometrial cancer treated with high dose rate brachytherapy. Gynecol Oncol 2015;138:429–33. doi: 10.1016/j.ygyno.2015.05.025 [DOI] [PubMed] [Google Scholar]
- 46.Doll KM, Winn AN, Goff BA. Untangling the Black-White mortality gap in endometrial cancer: a cohort simulation. Am J Obstet Gynecol 2017;216:324–25. doi: 10.1016/j.ajog.2016.12.023 [DOI] [PubMed] [Google Scholar]
- 47.Buskwofie A, Huang Y, Tergas AI, Hou JY, Ananth CV, Neugut AI, et al. Impact of hospital volume on racial disparities and outcomes for endometrial cancer. Gynecol Oncol 2018;149:329–36. doi: 10.1016/j.ygyno.2018.02.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Huang AB, Huang Y, Hur C, Tergas AI, Khoury-Collado F, Melamed A, et al. Impact of quality of care on racial disparities in survival for endometrial cancer. Am J Obstet Gynecol 2020;223:396.e1–13. doi: 10.1016/j.ajog.2020.02.021 [DOI] [PubMed] [Google Scholar]
- 49.Wright JD, Lewin SN, Deutsch I, Burke WM, Sun X, Herzog TJ. Effect of surgical volume on morbidity and mortality of abdominal hysterectomy for endometrial cancer. Obstet Gynecol 2011;117:1051–9. doi: 10.1097/AOG.0b013e31821647a0 [DOI] [PubMed] [Google Scholar]
- 50.Armstrong K, Randall TC, Polsky D, Moye E, Silber JH. Racial differences in surgeons and hospitals for endometrial cancer treatment. Med Care 2011;49:207–14. doi: 10.1097/MLR.0b013e3182019123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kaspers M, Llamocca E, Quick A, Dholakia J, Salani R, Felix AS. Black and Hispanic women are less likely than White women to receive guideline-concordant endometrial cancer treatment. Am J Obstet Gynecol 2020;223:398.e1–18. doi: 10.1016/j.ajog.2020.02.041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Fleury AC, Ibeanu OA, Bristow RE. Racial disparities in surgical care for uterine cancer. Gynecol Oncol 2011;121:571–6. doi: 10.1016/j.ygyno.2011.02.004 [DOI] [PubMed] [Google Scholar]
- 53.Doll KM, Khor S, Odem-Davis K, He H, Wolff EM, Flum DR, et al. Role of bleeding recognition and evaluation in Black-White disparities in endometrial cancer. Am J Obstet Gynecol 2018;219:593.e1–14. doi: 10.1016/j.ajog.2018.09.040 [DOI] [PubMed] [Google Scholar]
- 54.Dholakia J, Llamocca E, Quick A, Salani R, Felix AS. Guideline-concordant treatment is associated with improved survival among women with non-endometrioid endometrial cancer. Gynecol Oncol 2020;157;716–22. doi: 10.1016/j.ygyno.2020.03.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Maxwell GL, Tian C, Risinger J, Brown CL, Rose GS, Thigpen JT, et al. Racial disparity in survival among patients with advanced/recurrent endometrial adenocarcinoma: a Gynecologic Oncology Group study. Cancer 2006;107:2197–205. doi: 10.1002/cncr.22232 [DOI] [PubMed] [Google Scholar]
- 56.Farley JH, Tian C, Rose GS, Brown CL, Birrer M, Risinger JI, et al. Chemotherapy intensity and toxicity among Black and White women with advanced and recurrent endometrial cancer: a Gynecologic Oncology Group Study. Cancer 2010;116:355–61. doi: 10.1002/cncr.24769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Donkers H, Bekkers R, Massuger L, Galaal K. Systematic review on socioeconomic deprivation and survival in endometrial cancer. Cancer Causes Control 2019;30:1013–22. doi: 10.1007/s10552-019-01202-1 [DOI] [PubMed] [Google Scholar]
- 58.Cheung MR. African American race and low income neighborhoods decrease cause specific survival of endometrial cancer: a SEER analysis. Asian Pac J Cancer Prev 2013;14:2567–70. doi: 10.7314/apjcp.2013.14.4.2567 [DOI] [PubMed] [Google Scholar]
- 59.Von Behren J, Abrahão R, Goldberg D, Gomez SL, Setiawan VW, Cheng I. The influence of neighborhood socioeconomic status and ethnic enclave on endometrial cancer mortality among Hispanics and Asian Americans/Pacific Islanders in California. Cancer Causes Control 2018;29:875–81. doi: 10.1007/s10552-018-1063-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Rodriguez VE; LeBrón AMW Chang J Bristow RE. Guideline-adherent treatment, sociodemographic disparities, and cause-specific survival for endometrial carcinomas. Cancer 2021;127:2423–31. doi: 10.1002/cncr.33502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Robbins JR, Mahan MG, Krajenta RJ, Munkarah AR, Elshaikh MA. The impact of income on clinical outcomes in FIGO stages I to II endometrioid adenocarcinoma of the uterus. Am J Clin Oncol 2013;36:625–9. doi: 10.1097/COC.0b013e31825eb386 [DOI] [PubMed] [Google Scholar]
- 62.Benjamin I, Dalton H, Qiu Y, Cayco L, Johnson WG, Balducci J. Endometrial cancer surgery in Arizona: a statewide analysis of access to care. Gynecol Oncol 2011;121:83–6. doi: 10.1016/j.ygyno.2010.11.028 [DOI] [PubMed] [Google Scholar]
- 63.Helpman L, Pond GR, Elit L, Anderson LN, Seow H. Endometrial cancer presentation is associated with social determinants of health in a public healthcare system: a population-based cohort study. Gynecol Oncol 2020;158:130–6. doi: 10.1016/j.ygyno.2020.04.693 [DOI] [PubMed] [Google Scholar]
- 64.Dolly D, Mihai A, Rimel BJ, Fogg L, Rotmensch J, Guirguis A, et al. A delay from diagnosis to treatment is associated with a decreased overall survival for patients with endometrial cancer. Front Oncol 2016;6:31. doi: 10.3389/fonc.2016.00031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Doll KM, Snyder CR, Ford CL. Endometrial cancer disparities: a race-conscious critique of the literature. Am J Obstet Gynecol 2018;218:474–82.e2. doi: 10.1016/j.ajog.2017.09.016 [DOI] [PubMed] [Google Scholar]
- 66.Rocconi RP, Lankes HA, Brady WE, Goodfellow PJ, Ramirez NC, Alvarez RD, et al. The role of racial genetic admixture with endometrial cancer outcomes: an NRG Oncology/Gynecologic Oncology Group study. Gynecol Oncol 2016;140:264–69. doi: 10.1016/j.ygyno.2015.11.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Olson SH, Atoria CL, Cote ML, Cook LS, Rastogi R, Soslow RA, et al. The impact of race and comorbidity on survival in endometrial cancer. Cancer Epidemiol Biomarkers Prev 2012;21:753–60. doi: 10.1158/1055-9965.EPI-11-0735 [DOI] [PubMed] [Google Scholar]
- 68.Ruterbusch JJ, Ali-Fehmi R, Olson SH, Sealy-Jefferson S, Rybicki BA, Hensley-Alfrod S, et al. The influence of comorbid conditions on racial disparities in endometrial cancer survival. Am J Obstet Gynecol 2014;211:627.e1–9. doi: 10.1016/j.ajog.2014.06.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Ruiz JM, Steffen P, Smith TB. Hispanic mortality paradox: a systematic review and meta-analysis of the longitudinal literature. Am J Public Health 2013;103:e52–60. doi: 10.2105/AJPH.2012.301103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Collins Y, Holcomb K, Chapman-Davis E, Khabele D, Farley JH. Gynecologic cancer disparities: a report from the health disparities taskforce of the society of gynecologic oncology. Gynecol Oncol 2014;133:353–61. doi: 10.1016/j.ygyno.2013.12.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Farley J, Risinger JI, Rose GS, Maxwell GL. Racial disparities in Blacks with gynecologic cancers. Cancer 2007;110:234–43. doi: 10.1002/cncr.22797 [DOI] [PubMed] [Google Scholar]
- 72.Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: patterns and prospects. Health Psychol 2016;35:407–11. doi: 10.1037/hea0000242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Petersen EE, Davis NL, Goodman D, Cox S, Syverson C, Seed K, et al. Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. MMWR Morb Mortal Wkly Rep 2019;68:762–5. doi: 10.15585/mmwr.mm6835a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Doll KM, Hempstead B, Alson J, Sage L, Lavallee D. Assessment of prediagnostic experiences of Black women with endometrial cancer in the United States. JAMA Netw Open 2020;3:e204954. doi: 10.1001/jamanetworkopen.2020.4954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.American College of Obstetricians and Gynecologists. Joint statement: collective action addressing racism. Accessed May 28, 2021. https://www.acog.org/news/news-articles/2020/08/joint-statement-obstetrics-and-gynecology-collective-action-addressing-racism [Google Scholar]
- 76.Boyd RW, Lindo EG, Weeks LD, McLemore MR. On racism: a new standard for publishing on racial health inequalities. Accessed August 4, 2021. https://www.healthaffairs.org/do/10.1377/hblog20200630.939347/full/
- 77.Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health 2006;27:167–94. doi: 10.1146/annurev.publhealth.27.021405.102103 [DOI] [PubMed] [Google Scholar]