

Abstract
Introduction
The COVID-19 pandemic has strongly affected global healthcare systems. Prior epidemiological studies on different infectious diseases have shown a strong correlation between serum vitamin D levels and the incidence of certain infectious diseases. Vitamin D has an important immunomodulatory effect on innate immunity and exhibits several other mechanisms in the pathogenesis of the cytokine storm, which is one of the main contributing factors to fatality in COVID-19 patients.
Methods
A keyword search was conducted in the PubMed and Google Scholar research databases. The abstracts and/or full texts of selected papers were further evaluated. Articles that fulfilled the inclusion criteria were included in the systematic review.
Results
The 28 studies summarized in this review provide observational findings that vitamin D levels are related to the incidence, severity, and mortality rate of COVID-19 infection. The literature does not suggest that COVID-19 could be eliminated with supplementation of vitamin D, but there are implications that vitamin D deficiency might increase the risk for COVID-19 infection and severity of the disease progression.
Discussion
Current literature and several guidelines support the supplementation of vitamin D as a reasonable strategy for correcting and preventing vitamin D deficiency. The recommended dose for maintaining normal 25(OH)D levels by consensus is 1000 to 2000 IU vitamin D daily for at-risk teens and adults.
Conclusion
Vitamin D supplementation might play an important role in protecting from acute respiratory infections like the SARS CoV2, and in high-risk individuals with COVID 19 from progressing to critical clinical condition and reducing mortality.
Keywords: COVID-19, vitamin D, systematic reviews
Izvleček
Uvod
Pandemija COVID-19 je močno zamajala zdravstvene sisteme po svetu. Predhodne epidemiološke študije o različnih nalezljivih boleznih so pokazale močno povezavo med ravnjo vitamina D v serumu in incidenco nekaterih nalezljivih bolezni. Znano je, da ima vitamin D pomemben imunomodulatorni učinek, ki okrepi prirojeno imunost. Poleg tega ima vitamin D tudi številne druge mehanizme, vključno z ublažitvijo citokinskega viharja, ki je eden glavnih dejavnikov obolevnosti in smrtnosti pri bolnikih s COVID-19.
Metode
Iskanje po ključnih besedah je bilo izvedeno v raziskovalnih podatkovnih bazah PubMed in Google Scholar. Povzetki in/ali celotna besedila izbranih, potencialno pomembnih prispevkov so bili nadalje ocenjeni. Članki, ki so ustrezali merilom, so bili vključeni v sistematični pregled.
Rezultati
V preglednem članku je povzetih 28 študij, ki obsegajo ugotovitve, da so ravni vitamina D tako ali drugače povezane z incidenco, resnostjo bolezni in stopnjo umrljivosti zaradi okužbe s COVID-19. Literatura ne kaže, da bi lahko COVID-19 odpravili z dodatkom vitamina D, vendar obstajajo podatki, da pomanjkanje vitamina D lahko poveča tveganje za okužbo s COVID-19 in je povezano s hujšo stopnjo obolevnosti in smrtnosti.
Diskusija
Trenutna literatura in več smernic podpirajo dodajanje vitamina D kot razumno strategijo za odpravo in preprečevanje pomanjkanja vitamina D. Priporočeni odmerek za vzdrževanje normalne ravni 25(OH)D s konsenzom je 1000 do 2000 IE vitamina D na dan za ogrožene najstnike in odrasle.
Zaključek
Dodatek vitamina D pri posameznikih s pomanjkanjem vitamina D ima lahko pomembno vlogo pri zaščiti posameznikov pred akutnimi okužbami dihal ter pri tistih z visokim tveganjem za hud potek COVID-19 in smrt zaradi te bolezni.
Ključne besede: COVID-19, vitamin D, sistematični pregledi
1. Introduction
The COVID-19 pandemic has strongly affected global healthcare systems. In the early spring of 2020, a severe acute respiratory syndrome coronavirus 2 (SARS CoV2) crisis began in European countries, with many critical cases and deaths, particularly in high-risk groups.
Several retrospective analyses were performed, observing the effects on different disease courses, and other reasons for the clinical outcome differences were questioned. According to the reported data, there are seasonal fluctuations of COVID-19 disease severity (1).
It has been known for decades that seasonal changes cause significant immunity variation, including fluctuations in lymphocyte response and circulating levels of lymphocytes and neutrophils (2, 3). Epidemiological studies have shown also a strong reverse correlation between serum vitamin D (25-hydroxyvitamin D, 25(OH)D) levels, which are normally higher during the summer season, and the incidence of certain infectious diseases (2, 3). Vitamin D induces cathelicidin and beta defensin transcription and synthesis in macrophages and a favourable anti-inflammatory Th1 to Th2 phenotype ratio. Additionally, vitamin D exhibits a mitigating effect on the pathogenesis of the cytokine storm, which is one of the main contributing factors to fatality in COVID-19 patients (4). Vitamin D showed also potent activity against SARS CoV 2 in vitro (5).
Factors that have been shown to contribute to vitamin D deficiency include older age, smoking, higher body mass index (BMI) and obesity, lack of proper sun (UVB) exposure, dark skin and the presence of chronic illnesses, such as diabetes, malignant disease, high blood pressure, various gastrointestinal disorders and many others. Most people with these risk factors have been shown to be at increased risk regarding both severity of the disease and mortality from COVID-19 (6). Ethnic differences in the prevalence of common genetic polymorphisms of vitamin D receptor (VDR) and a series of cytochrome P450-containing sterol hydroxylases provide an additional explanation for low vitamin D levels. The exact role of genetic background in the responsiveness to vitamin D supplementation is yet to be determined (7).
In Slovenia, epidemiological data about vitamin D status in the population were investigated by a nationwide Nutrihealth study in 2017/18. A particularly concerning situation was observed during extended wintertime (November–April); severe vitamin D deficiency (defined as 25(OH)D levels below 30 nmol/L) was found in 40.8% of adults (age 18 – 64 years) and 34.6% of elderly people (age 65 to 74 years), while levels below 50 nmol/L (vitamin D deficiency) were observed in 81.6% and 78.8%, respectively. The results of the study showed high seasonal variations in serum 25(OH)D levels in both the adult and elderly population. The prevalence of vitamin D deficiency in Slovenia is among the highest in Europe and poses a serious public health risk that needs to be addressed with appropriate recommendations and policy interventions (8).
In 2021 a Slovenian systematic review of vitamin D status and dietary intake in various Slovenian populations was published. A meta-analysis of 43 studies that addressed serum 25(OH)D status and 16 that addressed vitamin D intake was conducted. The results showed that various population groups across Slovenia are at high risk of vitamin D insufficiency and deficiency, particularly during wintertime. All included studies reported daily intakes below the recommended level (9).
In Slovenia, because of the COVID-19 pandemic, medical doctors and the general population were urgently advised by leading experts to supplement vitamin D in fragile, vitamin D deficient high-risk individuals and COVID-19 patients (10, 11). At the beginning of the COVID-19 pandemic there were no data on the effects of vitamin D in SARS-CoV-2 infection; then again, there were reliable data on the beneficial effects of cholecalciferol in attenuating viral respiratory infections in people with low levels of vitamin D (12). The European Centre for Disease Prevention and Control encouraged health care professionals to take actions that are logical, based on previously known findings in related fields (13). However, in more than a year of the COVID-19 pandemic new data has become available to support the important role of vitamin D in SARS-CoV-2 infection, and some recommendations of vitamin D supplementation are already available (8, 9, 10).
Several studies have investigated the correlation between serum 25(OH)D levels and the incidence, severity and mortality of COVID-19 patients. The objective of this systematic review was to review the studies that explored the relationship between vitamin D and the course of COVID-19. The aim of our study was to explore whether optimal vitamin D status mitigates COVID-19 and if vitamin D supplementation is beneficial in the phase of COVID-19 pneumonia.
2. Materials and methods
2.1. Literature search strategy
The systematic review was prepared following the PRISMA recommendations (17).
2.2. Search strategy
We used the PubMed and Google Scholar research databases to search for published research (18, 19).
The search command consisted of the following MeSH Terms: (Vitamin D AND COVID-19) and was narrowed to search in titles and abstracts. Abstracts were then examined by two independent observers. Studies available in full text that included key terms in the title or abstract were considered. The abstracts and/or full texts of selected, potentially relevant papers were further evaluated.
Two independent reviewers (D.S., T.J.) completed a study identification and selection search in MEDLINE and Google Scholar, and disagreements were discussed with another reviewer (N.R.K.).
2.3. Methods of inclusion and exclusion criteria
The selection was limited to surveys published in English in 2020. The last inquiry was made on 30th November 2020. By reviewing the titles and abstracts, articles that were assessing the impact of vitamin D on COVID-19 infection in participating subjects or in populations were chosen. We searched for outcomes of COVID-19 (severity or/and mortality or/and incidence). For the purpose of our research the association of vitamin D and COVID-19 was divided into two groups: positive or negative (YES or NO), positive association meaning there was a statistically significant association between higher vitamin D levels and better outcome of COVID-19. Only studies with accessible full text and quantitatively reported outcomes were included.
The exclusion criteria for articles were: no accessible full text, publications with only abstracts, posters, editorials and comments available. Articles for paediatric populations and case studies were also excluded. Studies that did not report specific outcomes quantitatively were also excluded.
3. Results
3.1. Search results and study selection
The search of PubMed returned 321 articles and Google Scholar returned 574 articles. By following the inclusion and exclusion criteria explained in the method section, and after removing duplicates, the number of articles fell to 361. After reading the abstracts, we found 58 full text articles eligible for full reading. After reading the full texts, we excluded 30 articles not assessing either the severity, mortality or the incidence of COVID-19. We also excluded editorials, systematic reviews, case studies, studies of paediatric population and in vitro studies. A study assessing the impact of vitamin D together with other micronutrients on COVID-19 severity was also excluded.
A total of 28 articles were relevant for the purpose of content analysis (Figure 1).
Figure 1.
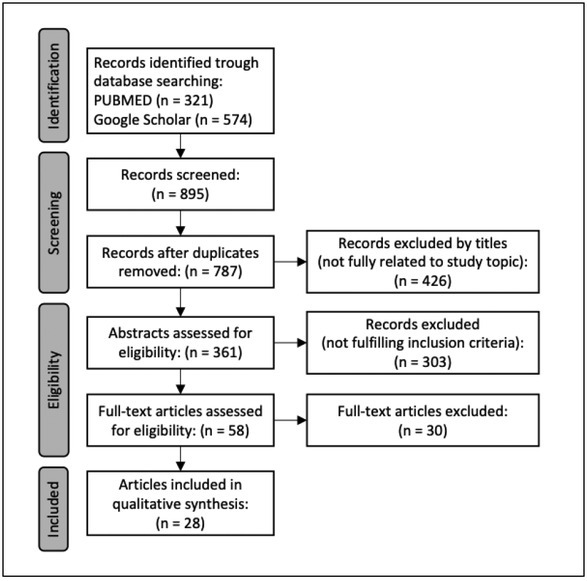
Flowchart of the course of selection of documents in the systematic review of the literature on vitamin D and COVID, following PRISMA.
3.2. General description of selected documents
The final number of studies included in the research was 28. All studies were published in 2020. We collected data on the country where the research was conducted, the number of participants, the number of centres included in the study and the effect of vitamin D on COVID-19. Among the included studies were 22 individual-level studies and 6 population-evel studies. There were 24 observational studies and 4 experimental studies. A positive association between vitamin D and COVID-19 was described in 26 studies and in 2 studies there was no association. The results are shown in Table 1.
Table 1.
Analyses reviewing the effect of Vitamin D on COVID-19 infection, individual-level studies.
| AUTHORS | COUNTRY | DESIGN | SAMPLE SIZE | CENTRE | UTCOME (S-SEVERITY/M- MORTALITY/ I-INCIDENCE) | Association (YES/NO) | EFFECT OF VITAMIN D ON COVID-19 |
|---|---|---|---|---|---|---|---|
| EXPERIMENTAL STUDIES | |||||||
| Entrenas Castillo M et al (20) | Spain | RCT | 76 | 1 | S,M | YES | Positive association. In the treatment group, 2% required admission to the ICU, in the control group 50% |
| Murai IH et al (21) | Brazil | DB RCT | 240 | 2 | S,M | NO | No association. Increased 25(OH) D levels in severe COVID patients, did not reduce hospital length of stay or any other relevant outcomes compared to placebo |
| Rastogi A et al (22) | India | RCT | 40 | 1 | / | YES | Positive association. With vitamin D supplementation more COVID patients turned COVID-19 PCR test negative with significant decrease in fibrinogen |
| Annweiler G et al (23) | France | QES | 77 | 1 | S,M | YES | Positive association. Regular bolus vitamin D supplementation was associated with less severe COVID-19 and better survival in frail elderly nursing home residents |
| OBSERVATIONAL STUDIES | |||||||
| De Smet D et al (24) | Belgium | ROCS | 186 | 1 | S,M | YES | Positive association. Vitamin D deficiency is correlated with the risk for hospitalization for COVID-19 pneumonia and predisposes to more advanced radiological disease stages |
| Jain A et al (25) | India | ROCS | 154 | 1 | / | YES | Positive association. Vitamin D deficiency in COVID-19 asymptomatic group 32.96% and 96.82% in symptomatic group |
| Merzon E et al (26) | Israel | ROCS | 14000 | / | S,I | YES | Positive association. The results demonstrated that low vitamin D levels are an independent risk factor for COVID-19 infection and hospitalization due to COVID-19 |
| Israel A et al (27) | Israel | ROCS | 576455 | / | I | YES | Positive association. Highly significant correlation between prevalence of vitamin D deficiency and COVID-19 incidence |
| Meltzer DO et al (28) | USA | ROCS | 489 | / | I | YES | Positive association. The relative risk of testing positive for COVID-19 was 1.77 times greater for patients with deficient vitamin D status compared with patients with sufficient vitamin D status before disease |
| Kaufman HW et al (29) | USA | ROCS | 190000 | 50 | I | YES | Positive association. The SARS-CoV-2 positivity rate was higher in patients with 25(OH)D deficiency |
| Hastie CE et al (30) | UK | ROCS | 502624 | / | I | NO | No association. Pre-infection blood samples did not support the vitamin D and the SARS-CoV-2 link |
| Daneshkhah A et al (31) | USA | ROCS | 4526 | 6 | I | NO | Positive association. Vitamin D status of a country’s elderly population was associated with the number of severe cases of Covid-19 in that country |
| Hernandez et al (32) | Spain | ROCS | 413 | 1 | S | YES | Positive association. 25(OH)D levels are lower in hospitalized COVID-19 patients than in population |
| Fasano et al (33) | Italy | ROCS | 2693 | 1 | S | YES | Positive association. Vitamin D supplementation was protective for developing COVID-19 in patient with Parkinson disease |
| Maghbooli Z et al (34) | Iran | ROCS | 235 | 1 | S | YES | Positive association between sufficient vitamin D levels and the reduction in clinical severity for COVID-19 |
| D’Avolio A et al (35) | Swizerland | ROCS | 107 | 1 | I | YES | Positive association. Significantly lower 25(OH)D levels were found in PCR-positive for SARS-CoV-2 patients compared with negative patients |
| Carpagnano GE et al (36) | Italy | ROCS | 42 | 1 | S,M | YES | Positive association. Significantly higher mortality rate among patients with vitamin D deficiency in the ICU |
| Baktash V et al (37) | UK | ROCS | 105 | 1 | S,M | YES | Positive association. Patients with vitamin D deficiency and COVID-19 may demonstrate worse morbidity outcomes |
| Mardani Ret al (38) | Iran | ROCS | 123 | 1 | I | YES | Positive association. Angiotensin-converting enzyme (ACE) concentration showed a higher quantity among individuals with COVID-19 with insufficient vitamin D concentration |
| Radujkovic A et al (39) | Germany | ROCS | 185 | 1 | S,M | YES | Positive association. Vitamin D deficiency was associated with higher risk of invasive mechanical ventilation and death |
| Karahan S et al (40) | Turkey | ROCS | 149 | 1 | S,M | YES | Positive association. Mean serum 25(OH)D was significantly lower in patients with severe-critical COVID-19 compared with moderate COVID-19 |
| Faniyi AA (41) | UK | ROCS | 392 | 1 | I | YES | Positive association. UK health professionals with vitamin D deficiency were more likely to be seropositive for COVID-19 antibodies |
*RCT-Randomized controlled trial, DB RCT-Double blind randomized controlled trial, QES-Quasi-experimental study, ROCS-Retrospective observational cohort study, POCS-Prospective observational cohort study, Mendelian randomization. OUTCOME: severity/mortality of COVID-19 in relation to 25(OH)D levels – S,M; incidence of COVID-19 infection in relation to 25(OH)D levels – INC, interventional studies with vitamin D replacement – INT
Table 2.
Analyses reviewing effect of Vitamin D on COVID-19 infection, population-level studies.
| AUTHORS | COUNTRY | DESIGN | SAMPLE SIZE | CENTRE | UTCOME (S-SEVERITY/M- MORTALITY/ I-INCIDENCE) | Association (YES/NO) | EFFECT OF VITAMIN D ON COVID-19 |
|---|---|---|---|---|---|---|---|
| EKO | |||||||
| Moozhipurath RK et al (42) | Germany | EKO | 6524 | 152 | I | YES | Positive association. UVB radiation (indirect vitamin D) was associated with lower death rates and case fatality rates |
| Jüni P et al (43) | Canada | EKO | 375 609 | 144 | I | NO | No associations of epidemic growth of COVID-19 with latitude and temperature |
| Ilie et al (44) | UK | EKO | / | 20 | S,M | YES | Positive association. Significant correlation between low mean vitamin D levels for both COVID-19 fatalities and cases |
| Singh et al (45) | India | EKO | / | 20 | I | YES | Positive association. Significant inverse correlation between vitamin D levels and case rates |
| Notari A et al (46) | Spain | EKO | / | 50 | I | YES | Positive association. Lower mean annual levels of vitamin D were linearly related to increased COVID-19 infection risk |
| Li M et al (47) | USA | EKO | / | 154 | I | YES | Positive association, vitamin D was associated with reduced COVID-19 infection risk |
*EKO-Ecological study. S-severity, M-mortality, I-incidence
3.3. Detailed qualitative results
3.3.1. Individual-level studies
Out of 22 individual-level studies, only 4 were experimental studies. The majority (3 out of 4) showed a positive correlation between vitamin D supplementation and COVID-19 infection and only one, the Brazil study, showed no correlation. There were 18 observational individual-level studies included, with only one showing no association between vitamin D levels and COVID-19 infection.
3.3.2. Population level studies
There were 6 population-level studies included, all of them being ecological studies. Only the Canadian study had a negative result and did not find any associations between epidemic growth of COVID-19 infection and latitude and temperature. The other 5 included ecological studies showed a positive correlation, where higher vitamin D levels were associated with lower incidence of COVID-19 infection.
4. Discussion
The 28 articles summarized here provide correlational evidence that vitamin D levels impact the incidence, severity and mortality rate of COVID-19 infection. Most of the observational studies show an inverse correlation between vitamin D levels and the severity and mortality of the COVID-19 disease. The same results were found in two other systematic reviews (48, 49). The majority of included observational studies also showed an inverse correlation between vitamin D levels and incidence of COVID-19, whereas results from the meta-analysis by Pereira et al show that vitamin D deficiency was not associated with higher incidence of COVID-19 infection (48). The demonstration of a significant correlation between vitamin D status and COVID-19 incidence, severitiy and even mortality may bring important public health implications regarding a major public health issue represented by vitamin D deficiency in the modern age. Five out of 6 ecological studies showed the correlation between vitamin D, COVID-19 mortality rate and latitude. These population-level studies also show big potential in health promotion regarding vitamin D deficiency prevention in different parts of the world. But correlation does not prove causality. Vitamin D levels are usually higher in healthy individuals in whom vitamin D could be an indicator of a healthy lifestyle.
The literature does not suggest that COVID-19 could be substantially reduced with supplementation of vitamin D, but there are indications that vitamin D deficiency increases the risk for COVID-19 infection and severity of the disease progression, as it does for other acute viral respiratory infections (12). However, there were some studies published that did not confirm this hypothesis. As for the Brazilian randomized controlled trial, it is important to note that the patients received vitamin D supplementation in a single very high dose (200.000 IU or 5000μg) more than a week after the onset of symptoms. Patients who required invasive mechanical ventilation and those admitted to the ICU were excluded. Additionaly, the proportion of patients with 25(OH)D deficiency was considerably lower than in other cohorts. (12, 44). A single dose of vitamin D might cause long-term induction of the inactivating 24-hydroxylase, and induction of fibroblast growth factor 23 (FGF23) that can suppress the 1-alpha-hydroxylase enzyme required for activation of vitamin D. Thus regular daily vitamin D supplementation or daily loading doses at the beginning of the disease (as soon as possible after confirmation of the infection) might have better immunomodulatory effects in COVID-19, rather than large bolus dosing at the time of severe disease (51, 52). In the Indian randomized study, a high-dose cholecalciferol turned a greater proportion of COVID-19 infected patients to become negative, supporting the thesis of the important impact of vitamin D on the innate immunity allowing macrophages to lower the viral burden and mitigate the COVID-19 course (22). A single study included an analysis of VDR and hydroxylase polymorphisms, which could affect results obtained across different populations and ethnic groups, as well as determine the effect of vitamin D levels in certain individuals. One Mendelian randomization study, using summary data from genome-wide association studies and 25(OH)D concentration-related single nucleotide polymorphisms as instrumental variables of genes associated with vitamin D deficiency, showed that there might be no linear causal relationship between 25(OH)D concentrations, susceptibility to COVID-19 infection and severity of disease. This randomization did not consider other factors influencing serum vitamin D levels, such as ambiental UVB (53). Interestingly, a recent Mendelian randomization study analysing the relationship between genetically determined 25(OH)D levels and all-cause mortality found that there was a negative relation only in a vitamin deficient area that was exponential but no relation between 25(OH)D levels above 50 nmol/L and mortality (48). As poor nutritional status compromises the immune response and reduces the treatment response to COVID-19 infection, not just supplementation with vitamin D but proper nutritional therapy in combination with vitamin D supplements would probably improve the effectiveness of COVID-19 treatments (54). Moreover, intake of vitamin D supplements is often limited by relatively poor adherence, especially in individuals with low-socioeconomic status (lower education, marginal groups), who are at the highest risk for vitamin D deficiency. Vitamin D deficiency is a known challenging public health issue, especially during the winter months with high incidence of viral respiratory infections (9). An effective approach to improve vitamin D status in the general population could be systematic vitamin D food fortification, since it is economical, safe and decreases deficiency risk in the entire population, including people that would not use supplements (55). However, current literature supports the supplementation of vitamin D as a reasonable strategy for correcting and preventing vitamin D deficiency. There are already some national ad hoc recommendations addressing vitamin D supplementation in fragile, vitamin D deficient high-risk individuals for COVID-19. Slovenian as well as some other ad hoc recommendations for replacement of vitamin D in periods of respiratory infections and COVID-19 pandemic suggested supplementation with cholecalciferol in a daily dose of 20 to 50μg (800 – 2000 IU) from October to May as a preventive measure in healthy individuals who have the possibility of safe sun exposure in the summer months (15). In individuals with chronic medical conditions and in those with less possibility of safe sun exposure in the summer between 10 a.m. and 4 p.m. such as healthcare providers, a dose of 20 to 50μg was recommended. The same dose was recommended also for individuals who share the same household with a COVID-19 infected person and with a high risk for COVID-19 infection. For hospitalized COVID-19 patients a laboratory analysis of serum 25(OH) D was recommended following vitamin D supplementation according to the serum level (56). For national guidelines of vitamin D supplementation in the COVID-19 pandemic and in periods of viral respiratory infections, data from additional studies is needed especially from larger double blind randomized placebo-controlled studies. Given the lack of highly effective therapies against COVID-19, except perhaps for corticosteroids, it is important to remain open-minded to emerging results from rigorously conducted studies with vitamin D (47).
The strength of this systematic review is its compliance with international standardized guidelines on reporting of systematic reviews and a high heterogeneity of included studies resulting from the baseline study design and the variability of the baseline characteristics. In this review different endpoints such as the incidence of COVID-19, the severity of COVID-19, length of hospitalizations, the need for an intensive care unit and mortality are reported, and our results could have a significant impact on clinical practice and public health. In view of the fact that COVID-19 is a new disease and there is a low number of well-planned intervention studies, this was the main limitation that influenced the conclusion of this research. An additional limitation of our study is that we only searched through two bibliographic databases (we searched the two largest ones) and there was a relatively large number of excluded articles which did not fulfil our carefully chosen criteria for inclusion.
This systematic review with a large number of articles included has considerable public health importance because it presents a summation of the latest research of the immunomodulative impact of vitamin D on the COVID-19 course. This review article presents some possibilities and ideas for future research. In future, randomized double blinded studies are needed, with vitamin D supplementation as a preventive measure prior to potential infection.
5. Conclusion
Vitamin D supplementation might play a pivotal role in protecting individuals from COVID-19. Optimal levels of 25(OH)D in the early phase of COVID-19 infection could prevent progression to severe or critical clinical condition and reduce mortality associated with COVID-19. The role of acute supplementation of vitamin D in severely deficient patients in the late phases of COVID-19 pneumonia is still unclear. Therefore, further randomized double blinded clinical trials are needed to provide conclusive evidence.
Funding Statement
This work was unfunded.
Footnotes
Conflict of interest
We declare no competing interests.
Ethical approval
The method used in this systematic literature review involves no ethical issues and ethical approval was not necessary.
Reference
- 1.Coronavirus update (Live): 42,271,844 cases and 1,146,211 deaths from COVID-19 virus pandemic - Worldometer. 2020. https://www.worldometers.info/coronavirus/ Accessed October 23rd.
- 2.The COVID-19 pandemic, seasons and the vitamin D laboratory strategy. 2022. https://www.researchgate.net/publication/350276683_The_COVID-19_Pandemic_Seasons_and_the_Vitamin_D_Laboratory_Strategy Accessed Jan 26th.
- 3.Fares A. Factors influencing the seasonal patterns of infectious diseases. Int J Prev Med. 2013;4(2):128–32. [PMC free article] [PubMed] [Google Scholar]
- 4.Aranow C. Vitamin D and the immune system. J Investig Med. 2011;59(6):881–6. doi: 10.2310/JIM.0b013e31821b8755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mok CK, Ng YL, Ahidjo BA, Hua Lee RC, Choy Loe MW, Liu J. Calcitriol, the active form of vitamin D, is a promising candidate for COVID-19 prophylaxis. BioRxiv. 2020. et al. [DOI]
- 6.Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020;81(2):e16–25. doi: 10.1016/j.jinf.2020.04.021. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tomei S, Singh P, Mathew R, Mattei V, Garand M, Alwakeel M. The role of polymorphisms in vitamin D - related genes in response to vitamin D supplementation. Nutrients. 2020;12(9):1–16. doi: 10.3390/nu12092608. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hribar M, Hristov H, Gregorič M, Blaznik U, Zaletel K, Oblak A. Nutrihealth study: seasonal variation in vitamin D status among the Slovenian adult and elderly population. Nutrients. 2020;12(6):1838. doi: 10.3390/nu12061838. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hribar M, Benedik E, Gregorič M, Blaznik U, Kukec A, Hristov H. A Systematic review of vitamin D status and dietary intake in various Slovenian populations. Zdr Varst. 2021;61(1):55–72. doi: 10.2478/sjph-2022-0009. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Žmitek K, Hribar M, Lavriša Ž, Hristov H, Kušar A, Pravst I. Socio-demographic and knowledge-related determinants of vitamin D supplementation in the context of the COVID-19 pandemic: assessment of an educational intervention. Frontiers Nutrition. 2021;8:290. doi: 10.3389/fnut.2021.648450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Covid-19: vitamin D a risk-assessment tool and to reduce morbidity and mortality in covid-19 pandemic. 2022. https://www.bmj.com/content/369/bmj.m1820/rr BMJ. Accessed Jan 26th.
- 12.Martineau AR, Jolliffe DA, Greenberg L, Aloia JF, Bergman P, Dubnov-Raz G. Vitamin D supplementation to prevent acute respiratory infections: individual participant data meta-analysis. Health Technol Assess. 2019;23(2):1–44. doi: 10.3310/hta23020. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Siuka D, Pfeifer M, Pinter B. Vitamin D supplementation during the COVID-19 pandemic. Mayo Clin Proc. 2020;95(8):1804–5. doi: 10.1016/j.mayocp.2020.05.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Joint Committee on Health Report on addressing Vitamin D deficiency as a public health measure in Ireland. 2021. https://data.oireachtas.ie/ie/oireachtas/committee/dail/33/joint_committee_on_health/reports/2021/2021-04-07_report-on-addressing-vitamin-d-deficiency-as-a-public-health-measure-in-ireland_en.pdf Accessed June 17th, 2021 at.
- 15.Pfeifer M, Siuka D, Pravst I, Ihan A. Priporočila za nadomeščanje holekalciferola (vitamina D3) v obdobjih respiratornih okužb in za nadomeščanje holekalciferola pri posameznikih s COVID-19. 2021. https://endodiab.si/wp-content/uploads/2020/11/30.Okt-2020_PRIPOROCILA-VITAMIN-D-in-COVID-19.pdf Accessed June 17th.
- 16.Tarazona-Santabalbina FJ, Cuadra L, Cancio JM, Carbonell FR, Garrote JMP, Casas-Herrero Á. Vitamin D supplementation for the prevention and treatment of COVID-19: a position statement from the Spanish Society of Geriatrics and Gerontology. Rev Esp Geriatr Gerontol. 2021;56(3):177–82. doi: 10.1016/j.regg.2021.02.001. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9. doi: 10.7326/0003-4819-151-4-200908180-00135. et al. W64. [DOI] [PubMed] [Google Scholar]
- 18.Google Učenjak. 2022. https://scholar.google.com/ Accessed Jan 26th.
- 19.PubMed. 2022. https://pubmed.ncbi.nlm.nih.gov/ Accessed Jan 26th.
- 20.Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, Alcalá Díaz JF, López Miranda J, Bouillon R. “Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: pilot randomized clinical study”. J Steroid Biochem Mol Biol. 2020;203:105751. doi: 10.1016/j.jsbmb.2020.105751. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Murai IH, Fernandes AL, Sales LP, Pinto AJ, Goessler KF, Duran CS C. Effect of vitamin D3 supplementation vs placebo on hospital length of stay in patients with severe COVID-19: a multicenter, double-blind, randomized controlled trial. medRxiv. 2020. et al. [DOI]
- 22.Rastogi A, Bhansali A, Khare N, Suri V, Yaddanapudi N, Sachdeva N. Short term, high-dose vitamin D supplementation for COVID-19 disease: a randomised, placebo-controlled, study (SHADE study) Postgrad Med J. 2020. et al. postgradmedj-2020-139065. [DOI] [PubMed]
- 23.Annweiler G, Corvaisier M, Gautier J, Dubée V, Legrand E, Sacco G. Vitamin D supplementation associated to better survival in hospitalized frail elderly covid-19 patients: the geria-covid quasi-experimental study. Nutrients. 2020;12(11):3377. doi: 10.3390/nu12113377. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.De Smet D, De Smet K, Herroelen P, Gryspeerdt S, Martens GA. Serum 25(OH)D level on hospital admission associated with COVID-19 stage and mortality. Am J Clin Pathol. 2021;155(3):381–8. doi: 10.1093/ajcp/aqaa252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jain A, Chaurasia R, Sengar NS, Singh M, Mahor S, Narain S. Analysis of vitamin D level among asymptomatic and critically ill COVID-19 patients and its correlation with inflammatory markers. Sci Rep. 2020;10(1):20191. doi: 10.1038/s41598-020-77093-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Merzon E, Tworowski D, Gorohovski A, Vinker S, Golan Cohen A, Green I. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study. FEBS J. 2020;287(17):3693–702. doi: 10.1111/febs.15495. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Israel A, Cicurel AA, Feldhamer I, Dror Y, Giveon SM, Gillis D. The link between vitamin D deficiency and Covid-19 in a large population. MedRxiv. 2020. et al. [DOI]
- 28.Meltzer DO, Best TJ, Zhang H, Vokes T, Arora V, Solway J. Association of vitamin D deficiency and treatment with COVID-19 incidence. MedRxiv. 2020. [DOI]
- 29.Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS One. 2020;15(9):e0239252. doi: 10.1371/journal.pone.0239252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hastie CE, Pell JP, Sattar N. Vitamin D and COVID-19 infection and mortality in UK Biobank. Eur J Nutr. 2021;60(1):545–8. doi: 10.1007/s00394-020-02372-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Daneshkhah A, Agrawal V, Eshein A, Subramanian H, Roy HK, Backman V. Evidence for possible association of vitamin D status with cytokine storm and unregulated inflammation in COVID-19 patients. Aging Clin Exp Res. 2020;32(10):2141–58. doi: 10.1007/s40520-020-01677-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hernández JL, Nan D, Fernandez-Ayala M, García-Unzueta M, Hernández-Hernández MA, López-Hoyos M. Vitamin D status in hospitalized patients with SARS-CoV-2 infection. J Clin Endocrinol Metab. 2021;106(3):e1343–53. doi: 10.1210/clinem/dgaa733. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fasano A, Cereda E, Barichella M, Cassani E, Ferri V, Zecchinelli AL. COVID-19 in parkinson’s disease patients living in Lombardy, Italy. Mov Disord. 2020;35(7):1089–93. doi: 10.1002/mds.28176. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Maghbooli Z, Sahraian MA, Ebrahimi M, Pazoki M, Kafan S, Tabriz HM. Vitamin D sufficiency, a serum 25-hydroxyvitamin D at least 30 ng/mL reduced risk for adverse clinical outcomes in patients with COVID-19 infection. PLoS One. 2020;15(9):e0239799. doi: 10.1371/journal.pone.0239799. et al. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 35.D’avolio A, Avataneo V, Manca A, Cusato J, de Nicolò A, Lucchini R. 25-hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2. Nutrients. 2020;12(5):1359. doi: 10.3390/nu12051359. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carpagnano GE, di Lecce V, Quaranta VN, Zito A, Buonamico E, Capozza E. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest. 2021;44(4):765–71. doi: 10.1007/s40618-020-01370-x. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Baktash V, Hosack T, Patel N, Shah S, Kandiah P, van den Abbeele K. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad Med J. 2021;1149;97:442. doi: 10.1136/postgradmedj-2020-138712. et al. –. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Mardani R, Alamdary A, Mousavi Nasab SD, Gholami R, Ahmadi N, Gholami A. Association of vitamin D with the modulation of the disease severity in COVID-19. Virus Res. 2020;289:198148. doi: 10.1016/j.virusres.2020.198148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Radujkovic A, Hippchen T, Tiwari-Heckler S, Dreher S, Boxberger M, Merle U. Vitamin D deficiency and outcome of COVID-19 patients. Nutrients. 2020;12(9):2757. doi: 10.3390/nu12092757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Karahan S, Katkat F. Impact of Serum 25(OH) Vitamin D level on mortality in patients with COVID-19 in Turkey. J Nutr Health Aging. 2021;25(2):189–96. doi: 10.1007/s12603-020-1479-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Faniyi AA, Lugg ST, Faustini SE, Webster C, Duffy JE, Hewison M. Vitamin D status and seroconversion for COVID-19 in UK healthcare workers who isolated for COVID-19 like symptoms during the 2020 pandemic. MedRxiv. 2020. et al. [DOI] [PMC free article] [PubMed]
- 42.Moozhipurath RK, Kraft L, Skiera B. Evidence of protective role of Ultraviolet-B (UVB) radiation in reducing COVID-19 deaths. Sci Rep. 2020;10(1):17705. doi: 10.1038/s41598-020-74825-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Jüni P, Rothenbühler M, Bobos P, Thorpe KE, da Costa BR, Fisman DN. Impact of climate and public health interventions on the COVID-19 pandemic: a prospective cohort study. CMAJ. 2020;192(21):E566–73. doi: 10.1503/cmaj.200920. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ilie PC, Stefanescu S, Smith L. The role of vitamin D in the prevention of coronavirus disease 2019 infection and mortality. Aging Clin Exp Res. 2020;32(7):1195–8. doi: 10.1007/s40520-020-01570-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Singh S, Kaur R, Singh RK. Revisiting the role of vitamin D levels in the prevention of COVID-19 infection and mortality in European countries post infections peak. Aging Clin Exp Res. 2020;32(7):1195–8. doi: 10.1007/s40520-020-01570-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Notari A, Torrieri G. COVID-19 transmission risk factors. MedRxiv. 2020. [DOI] [PMC free article] [PubMed]
- 47.Li M, Zhang Z, Cao W, Liu Y, Du B, Chen C. Identifying novel factors associated with COVID-19 transmission and fatality using the machine learning approach. Sci Total Environ. 2021;764:142810. doi: 10.1016/j.scitotenv.2020.142810. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Pereira M, Dantas Damascena A, Galvão Azevedo LM, de Almeida Oliveira T, da Mota Santana J. Vitamin D deficiency aggravates COVID-19: systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2020. pp. 1–9. –. [DOI] [PubMed]
- 49.Ghasemian R, Shamshirian A, Heydari K, Malekan M, Alizadeh-Navaei R, Ebrahimzadeh MA. The role of vitamin D in the age of COVID-19: a systematic review and meta-analysis along with an ecological approach. MedRxiv. 2020. et al. [DOI]
- 50.Leaf DE, Ginde AA. Vitamin D3 to treat COVID-19: different disease, same answer. JAMA. 2021;325(11):1047–8. doi: 10.1001/jama.2020.26850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hansen KE. High-dose vitamin D: helpful or harmful? Curr Rheumatol Rep. 2011;13(3):257–64. doi: 10.1007/s11926-011-0175-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Griffin G, Hewison M, Hopkin J, Kenny RA, Quinton R, Rhodes J. Perspective: vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19. Clin Med (Lond) 2021;21(2):e144–9. doi: 10.7861/clinmed.2021-0035. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Liu D, Tian Q, Zhang J, Hou H, Wang W, Meng Q. Association of 25 hydroxyvitamin D concentration with risk of COVID-19: a Mendelian randomization study. MedRxiv. 2020. et al. [DOI] [PMC free article] [PubMed]
- 54.Mendes A, Serratrice C, Herrmann FR, Gold G, Graf CE, Zekry D. Nutritional risk at hospital admission is associated with prolonged length of hospital stay in old patients with COVID-19. Clin Nutr. 2021. et al. S0261-5614(21)00156-4. [DOI] [PMC free article] [PubMed]
- 55.Pilz S, März W, Cashman KD, Kiely ME, Whiting SJ, Holick MF. Rationale and plan for vitamin D food fortification: a review and guidance paper. Front Endocrinol (Lausanne) 2018;9:373. doi: 10.3389/fendo.2018.00373. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Pludowski P, Holick MF, Grant WB, Konstantynowicz J, Mascarenhas MR, Haq A. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol. 2018;175:125–35. doi: 10.1016/j.jsbmb.2017.01.021. et al. [DOI] [PubMed] [Google Scholar]