

Abstract
A 58-year-old man who underwent lower lobectomy of the right lung for primary pulmonary leiomyosarcoma (PPL) 4 years ago presented with epigastric pain and was diagnosed with small bowel intussusception caused by an intestinal mass. Partial resection of the small intestine was performed, and pathological examination revealed metastatic leiomyosarcoma. Masses in the left adrenal gland, subcutaneous tissue of the left upper arm, right pleura, jejunum, right trapezius muscle, and right adrenal gland were subsequently detected in the following 4 years. Resection was performed for each tumor, which was histologically confirmed as metastatic leiomyosarcoma. However, 1 month after the last surgery, multiple systemic metastases were found, thus, he is currently undergoing chemotherapy. The patient has been alive for 8 years and 4 months after the first operation for PPL. PPL is an extremely rare disease with no established treatment strategy for recurrences. Aggressive metastasectomy may be beneficial in selected cases.
Keywords: Primary pulmonary leiomyosarcoma, Metastasectomy, Recurrence
Introduction
Primary pulmonary leiomyosarcoma (PPL) is extremely rare. The most common primary sites are the uterus and gastrointestinal organs, followed by soft tissues such as the retroperitoneal or abdominal tissues [1].
Because of the rarity of the disease, there is no established treatment strategy for it. Furthermore, although there are a few treatment guidelines for soft tissue sarcomas, they are general guidelines for sarcoma as a whole, and apply to many different pathological types of sarcomas, including rhabdomyosarcoma, liposarcoma, and leiomyosarcoma [2, 3]. The clinical practice guideline by the National Comprehensive Cancer Network (NCCN) covers the treatment of extremity, superficial trunk, head and neck, intraabdominal, and retroperitoneal soft tissue sarcomas, but not lung diseases [2]. Based on a retrospective cohort study, surgery is recommended for isolated resectable pulmonary metastases [3]. However, the significance of metastasectomy for extrapulmonary metastases from soft tissue sarcoma has not been fully investigated.
We herein report a case of PPL, where the patient achieved long-term survival after multiple metastasectomies.
Case report
A 58-year-old man who underwent lower lobectomy of the right lung for PPL 4 years ago presented with epigastric pain that persisted for 2 months. Computed tomography (CT) revealed a small bowel mass causing small bowel intussusception (Fig. 1). Laboratory examinations, including tumor markers, were unremarkable. Since a primary malignant tumor of the small intestine was suspected preoperatively, partial resection of the small intestine with regional lymph node dissection was performed. The resected specimen showed an elevated lesion with a rough and irregular macroscopic surface. Microscopically, the tumor consisted of spindle cells with irregularly shaped nuclei. Immunohistochemical (IHC) staining demonstrated that the tumor cells were positive for smooth muscle actin and desmin, and negative for cluster of differentiation 34 (CD34) and KIT (Fig. 2). Thus, a diagnosis of metastatic intestinal tumor from PPL was made.
Fig. 1.

Contrast-enhanced CT showed a mass of the ilium causing small bowel intussusception (a). Coronal image (b)
Fig. 2.

Histological findings of the small intestine tumor. The tumor consisted of spindle cells with irregular-shaped nuclei (hematoxylin and eosin × 200) (a). Immunohistochemistry showed the tumor cells were partly positive for SMA (× 200) (b) and Desmin (× 200) (c)
Eight months after the surgery, follow-up CT revealed a mass in the left adrenal gland. 18F-fluorodeoxyglucose positron emission tomography/CT (18F-FDG PET/CT) showed an increased uptake in the adrenal mass (SUVmax = 5.4), suggesting metachronous metastasis (Fig. 3). No other tumor was detected during the examination. The patient underwent laparoscopy-assisted left adrenalectomy. Pathological examination, including IHC staining of the adrenal mass, also revealed leiomyosarcoma. Ten months later, a subcutaneous mass appeared in the patient’s left upper arm, which was surgically removed under local anesthesia (Fig. 4). Leiomyosarcoma metastasis was confirmed by pathological examination.
Fig. 3.

Computed tomography revealed a mass in the left adrenal gland (a). PET/CT showed an increased uptake of FDG in the mass (b)
Fig. 4.

A subcutaneous mass appeared in the patient’s left upper arm
A month after the third metastasectomy, thickening of the right pleura and a jejunal mass were detected by CT scan. 18F-FDG PET/CT showed an increased uptake of FDG in the pleural (SUVmax = 3.2) and the jejunal mass (SUVmax = 7.7), suggesting recurrence at both the sites (Fig. 5). As metastases were suspected in multiple organs, systemic chemotherapy was selected. Six cycles of doxorubicin monotherapy were performed for about 4 months and the patient was followed up thereafter. Six months after the completion of chemotherapy, the patient developed small bowel obstruction due to the jejunal lesion (Fig. 6). Therefore, partial resection of the small intestine was performed, and pathological examination including IHC staining revealed leiomyosarcoma.
Fig. 5.

PET/CT showed an increased uptake of FDG in the pleural (a) and the jejunal mass (b)
Fig. 6.

CT showed the jejunal lesion causing small bowel obstruction
Clinical images showed shrinkage of the pleural mass and no recurrence at other sites of the body. Thus, resection of the right pleural mass—the fifth metastasectomy, was performed 1 month after resection of the jejunal tumor. Pathological examination of the pleural mass revealed fibrous thickening with smooth muscle and microvessel proliferation and infiltration of lymphocytes. No residual tumor cells were observed, suggesting complete response to chemotherapy.
A solitary metastasis in the right trapezius was detected 9 months after the chest surgery; therefore, a sixth resection was performed. Another 4 months later, PET/CT imaging showed an increased uptake of FDG in the right adrenal gland but no other metastases; therefore, a seventh resection was performed. Pathologically, both resected specimens were proven to be leiomyosarcomas.
Nevertheless, 1 month after the last surgery, PET/CT demonstrated increased uptake of FDG in muscles of the entire body including the dorsal neck, both arms, bilateral side of abdominal wall, and both thighs, suggesting systemic metastases in multiple organs. Therefore, the patient was started on pazopanib, a multi-targeted tyrosine kinase inhibitor (TKI). Four years and 4 months after the first metastasectomy, and 8 years and 4 months after the first operation, the patient is alive (Fig. 7).
Fig. 7.
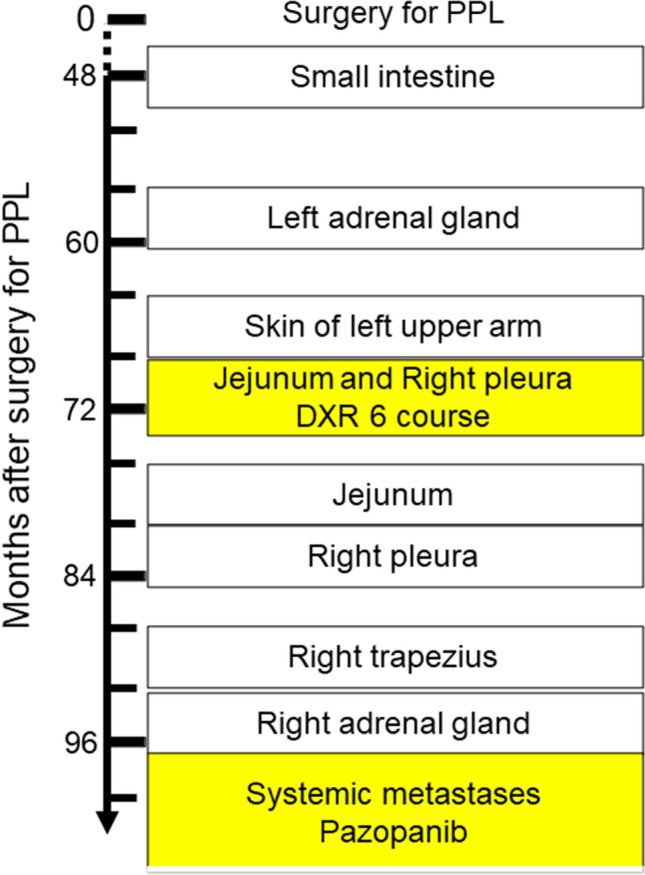
Metastatic sites and treatment. Square represents metastatic site treated by operation, and yellow square represents metastatic sites treated using anti-tumor agents. DXR doxorubicin; PPL primary pulmonary leiomyosarcoma
Discussion
PPL is an extremely rare disease, and thus, there are few reports including large numbers of patients. The report with the largest sample size was a population-based study reported by Qin et al. [4], which included 231 patients with PPL. According to that study, the median overall survival (OS) of the patients was 14.0 months and the overall 1-, 3-, and 5-year survival rates were 52.7%, 29.0%, and 22.2%, respectively.
Patients with distant cancer stages, of whom 71.0% did not undergo surgery, had significantly poorer prognosis with overall 1-, 3-, and 5-year survival rates of 30.3%, 11.6%, and 4.4%, respectively. Patients who had never undergone surgery, 62.9% of whom were in the distant stage, had significantly worse OS than patients who underwent surgery (33.0 months vs. 4.0 months; p < 0.01). Further, in a multivariate analysis, they identified distant stage (p = 0.01) and surgery (p < 0.01) as the only significant factors affecting OS. Considering these results, the survival of patients with distant metastases who do not undergo surgery is very poor [4].
According to the European Society for Medical Oncology guidelines for soft tissue and visceral sarcoma [3], surgical resection is recommended only for single pulmonary metastasis, and chemotherapy is recommended in cases with extrapulmonary metastases. However, surgery can be offered as an option in selected cases. According to the National Comprehensive Cancer Network guidelines [2], the treatment options for patients with metastatic recurrent disease are similar to those for patients with stage IV or synchronous metastatic disease. In such cases, metastasectomy with or without pre- or postoperative chemotherapy and/or radiation therapy can be a treatment option. Kane et al. [5] reported that the OS of patients with soft tissue sarcoma and synchronous metastases who underwent metastasectomy was 16.0 months, while the OS of patients without metastasectomy was 14.0 months. The authors concluded that metastasectomy did not improve survival in patients with synchronous metastasis and, therefore, should be considered as a palliative option. In contrast, Akin et al. [6] reported the significance of metastasectomy for recurrent diseases. In their retrospective study, 21 of the 29 patients with recurrent soft tissue sarcoma underwent surgery, and their OS was significantly longer than that of the remaining eight patients who did not undergo surgery (41.0 vs. 16.6 months, p < 0.001) [5].
In our case, we also performed surgery for the right pleural metastasis. It was debated whether surgery or systemic anti-tumor agents should have been selected, because a jejunal metastasis and the right pleural metastasis were detected simultaneously, which indicated systemic metastasis. However, when the patient underwent emergency surgery to address bowel obstruction caused by the jejunal lesion after 4 months of chemotherapy and 6 months of no treatment, no other metastases had appeared. Therefore, we aggressively selected surgery to treat the right pleural metastasis. Finally, the patient achieved long-term survival through repeated surgeries for extrapulmonary metastasis, chemotherapy, and multi-targeted TKI.
In the present case, doxorubicin monotherapy was selected when distant metastases in multiple organs, including the right pleura and jejunum, were detected. A randomized controlled phase 3 trial comparing doxorubicin alone and intensified doxorubicin combined with ifosfamide as the first-line chemotherapy regimen for locally advanced or metastatic soft tissue sarcoma has been reported [7]. The OS rates in the doxorubicin alone group and the doxorubicin combined with ifosfamide group were 12.8 and 14.3 months, respectively; the difference was not statistically significant (p = 0.076). Although the results of the study did not support the routine use of combination chemotherapy, it should be noted that the study included various kinds of sarcomas, and only around one-fourth of the subjects had leiomyosarcoma. In a retrospective study, Akin et al. [6] investigated the efficacy of ifosfamide and doxorubicin in 51 patients with initially metastatic or recurrent leiomyosarcoma, including two patients with thoracic leiomyosarcoma. The authors reported an overall response rate of 12% and a median OS of 24.6 months (95% CI 16.2–33.0).
Pazopanib, a multi-targeted TKI, was selected to address systemic metastasis in multiple organs in our case. Pazopanib has been proven to improve progression-free survival in patients with metastatic soft tissue sarcoma when used after standard chemotherapy containing anthracycline in an international phase 3 trial [8] and is listed as a single-agent regimen in the guideline [2]. The efficacy and safety of the agent in Japanese patients were confirmed in a large-scale retrospective study [9].
This study presents a very rare case of PPL, and provides evidence suggesting the benefit of repeated metastasectomy for recurrent tumors. Because of the rarity of PPL, accumulation of case series is still necessary to establish reasonable treatment options, not only for primary tumors, but also for recurrent tumors.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from the patient in this report.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Goldblum JR, Folpe AL, Weiss SW. Leiomyosarcoma. In: Straus M, editor. Enzinger & Weiss’s soft tissue tumors. 7. Missouri: Mosby; 2020. pp. 591–603. [Google Scholar]
- 2.von Mehren M, Randall RL, Benjamin RS, et al. Soft tissue sarcoma, version 2.2018: clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2018;16:536–563. doi: 10.6004/jnccn.2018.0025. [DOI] [PubMed] [Google Scholar]
- 3.Casali PG, Abecassis N, Bauer S, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:51–67. doi: 10.1093/annonc/mdy096. [DOI] [PubMed] [Google Scholar]
- 4.Qin BD, Jiao XD, Zang YS. Primary pulmonary leiomyosarcoma: a population-based study. Lung Cancer. 2018;116:67–72. doi: 10.1016/j.lungcan.2017.12.015. [DOI] [PubMed] [Google Scholar]
- 5.Kane JMIII, Finley JW, Driscoll D, et al. The treatment and outcome of patients with soft tissue sarcomas and synchronous metastases. Sarcoma. 2002;6:69–73. doi: 10.1080/1357714021000022168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Akin S, Dizdar O, Karakas Y, et al. Ifosfamide and doxorubicin in the treatment of advanced leiomyosarcoma. Curr Probl Cancer. 2018;42:344–349. doi: 10.1016/j.currproblcancer.2018.01.011. [DOI] [PubMed] [Google Scholar]
- 7.Judson I, Verweij J, Gelderblom H, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomized controlled phase 3 trial. Lancet Oncol. 2014;15:415–423. doi: 10.1016/S1470-2045(14)70063-4. [DOI] [PubMed] [Google Scholar]
- 8.van der Graaf WT, Blay JY, Chawla SP, et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomized, double-blind, placebo-controlled phase 3 trial. Lancet. 2012;379:1879–1886. doi: 10.1016/S0140-6736(12)60651-5. [DOI] [PubMed] [Google Scholar]
- 9.Nakamura T, Matsumine A, Kawai A, et al. The clinical outcome of pazopanib treatment in Japanese patients with relapsed soft tissue sarcoma: a Japanese Musculoskeletal Oncology Group (JMOG) study. Cancer. 2016;122:1408–1416. doi: 10.1002/cncr.29961. [DOI] [PMC free article] [PubMed] [Google Scholar]