

Abstract
Objectives:
To evaluate the dental and skeletal effects of chin cup using two different force magnitudes in the management of Class III malocclusion cases.
Materials and Methods:
Fifty growing patients (26 males and 24 females) with skeletal Class III and mandibular prognathism were selected. The patients were divided into three groups. Patients in group 1 (n = 20) were treated with a chin cup and occlusal bite plane using 600 g of force per side. Patients in group 2 (n = 20) were subjected to the same treatment as in group 1 but using 300 g of force per side. In group 3 (n = 10) no treatment was performed. For all patients, lateral cephalograms were taken before treatment and after 1 year. Cephalograms were traced and analyzed. The collected data were analyzed statistically using one-way analysis of variance and the Tukey test.
Results:
In the treatment groups, the SNB angle and ramus height decreased significantly. The ANB angle, Wits appraisal, anterior facial height, mandibular plane angle, and retroclination of the mandibular incisors were significantly increased in comparison to the control group. Utilization of either force showed no significant differences, except that the reduction in the ramus height was significantly greater with the use of higher force.
Conclusions:
The use of a chin cup improved the maxillomandibular base relationship in growing patients with Class III malocclusion but with little skeletal effect. The utilization of either force had the same effects, except that the higher force had a more pronounced effect in reduction of ramus height.
Keywords: Class III, Chin cup, Force magnitude
INTRODUCTION
In clinical orthodontics, skeletal Class III malocclusions are considered among the most difficult cases to treat.1,2 Subjects with Class III may display maxillary retrusion, mandibular protrusion, or a combination of the two. Several orthopedic appliances have been developed for correction of such cases, including maxillary protraction appliances,1–4 functional appliances,5–9 and the chin cup.1,10–14
The chin cup has been utilized for almost a century for management of mandibular protrusion in growing patients.15 The rationale for a chin cup is to apply pressure on the temporomandibular joint to inhibit or redirect condylar growth.14 The effects of the chin cup have been studied by many authors.10–14 Significant mandibular growth retardation and a decrease in the prechondroblastic layer of the condylar cartilage were reported in animal experimental studies using a chin cup.16,17 In addition, clinical studies in human patients have reported that the chin cup had skeletal and dental effects. Changes in mandibular growth, clockwise rotation of the mandible, and lingual tipping of the mandibular incisors were among the most common findings of these studies.10–14
Orthodontic or orthopedic force magnitudes are a critical issue in clinical orthodontics. Optimal force is the lowest force magnitude that could produce the desired dental or skeletal effects. There has been much debate regarding the force magnitude needed to achieve adequate force levels at the condyle to affect the mandibular growth. A relatively low force magnitude of 150–200 g was utilized by Thilander.18 Higher forces of 400 g were used by Tanne et al.19 Ritucci and Nanda12 investigated the effect of a chin cup with 500 g orthopedic force. Gokalp and Kurt14 and Tuncer et al.15 reported the use of 600 g. Stronger forces of 1000–1200 g were evaluated by Deguchi and Kitsugi.20
In spite of a large number of studies regarding the chin cup, inadequate information is available comparing the effects of different force magnitude. Katashiba et al.21 found that the use of a chin cup with the lighter force, but with a longer wearing time, provided more skeletal correction than the use of heavier force for a shorter time. On the other hand, it was reported that a high force was needed to achieve skeletal effects with a chin cup.22
The present study was conducted to evaluate the dental and skeletal effects of a chin cup utilizing two retraction orthopedic forces, 300 g and 600 g per side, for the same wearing time, in the treatment of Class III patients who were still growing.
MATERIALS AND METHODS
Fifty growing patients were selected for this study (26 boys and 24 girls). They were selected according to the following criteria: skeletal Class III pattern (ANB angle < 1 degree) and protrusive mandible (SNB angle > 80 degrees). All patients had anterior crossbite. Hand-wrist radiographs were obtained for each patient to assess skeletal maturation. All patients had not passed the peak of pubertal growth spurt, as shown by the epiphysis of the middle phalanx of the third finger having capped its diaphysis. The patients were randomly divided into three groups. Group 1 consisted of 20 patients (10 boys and 10 girls), group 2 consisted of 20 patients (11 girls and 9 boys), and group 3 consisted of 10 patients (5 boys and 5 girls). The mean ages at the start of treatment were 9.6, 10.1, and 9.2 years for groups 1, 2, and 3, respectively.
Patients in groups 1 and 2 were treated with an occipital pull chin cup (Dentaurum, Ispringen, Germany) and an acrylic occlusal bite plane with a thickness that just freed the occlusion anteriorly. The chin cup used was soft not acrylic. The force magnitude exerted by the chin cup was 600 g per side in group 1 and 300 g per side in group 2. A force gauge (Somfy tec, France) was utilized to determine the applied force. The patients were instructed to wear the appliances for 14 hours each day. In group 3, the patients did not receive any orthodontic or orthopedic treatment during the study period.
Lateral cephalogram films were taken for all patients at two stages: before the start of treatment and after 1 year. All films were traced by one investigator. Landmarks and measurements for cephalometric analysis23 were done and are presented in Figures 1 to 3. Measurements obtained were corrected for standard magnification. The cephalometric films were retraced and the method error was determined with Dalhberg's formula; the error was less than 1 mm and 1 degree.
Figure 1.
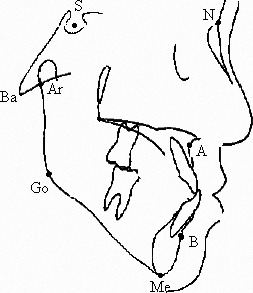
Cephalometric points.
Figure 2.
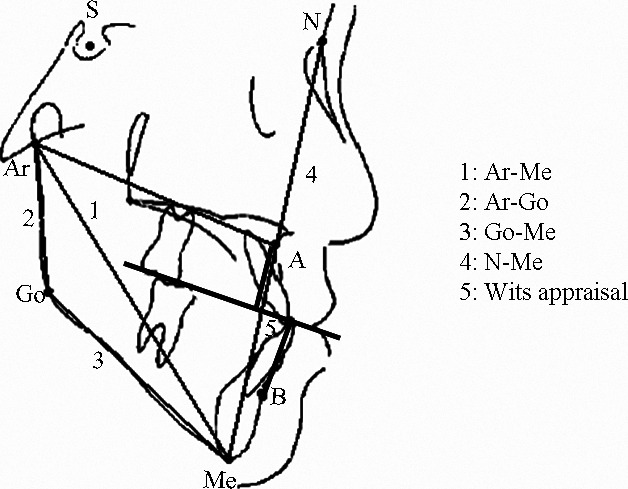
Cephalometric linear measurements.
Figure 3.
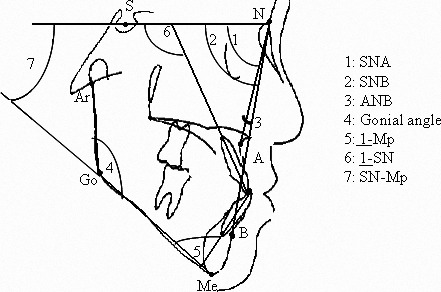
Cephalometric angular measurements.
Statistical Analysis
Means and standard deviations of the calculated measurements and the changes after treatment in each group were determined. The data were analyzed using one-way analysis of variance and Tukey test. Significance for the statistical test was set at P < .05.
RESULTS
Clinically the anterior crossbite was corrected in all patients in the two treatment groups (Figures 4 and 5). Means and standard deviations of the cephalometric measurements of the three groups before treatment are presented in Table 1. One-way analysis of variance indicated that there was a statistically significant difference (P < .05) among the three groups in SNB angle, ANB angle, Wits appraisal, Ar-Go, SN-MP angle, N-Me, and 1-MP angle.
Figure 4.

Pre and posttreatment intraoral photographs of patient utilized chin cup with 600 grams of force per side.
Figure 5.

Pre and posttreatment intraoral photographs of patient utilized chin cup with 300 grams of force per side.
Table 1.
Means and Standard Deviations of the Cephalometric Measurements of the Three Groups Before Treatment

Means and standard deviations of the changes in the cephalometric measurements and the results of the Tukey test are presented in Table 2. In general, there were significant differences (P < .05) in the changes in cephalometric measurements between the two treatment groups and the control group regarding mandibular position (SNB angle), the maxillomandibular relationship (ANB angle and Wits appraisal), ramus height (Ar-Go), vertical measurements (N-Me and SN-MP angle), and inclination of the mandibular incisors (1-MP). In the treatment groups, the SNB angle, ramus height, and mandibular incisor inclinations were significantly decreased in comparison to the control group. The ANB angle, Wits appraisal, SN-MP angle, and anterior facial height were significantly increased in the two treatment groups.
Table 2.
Means and Standard Deviations of the Changes in Cephalometric Measurements After Treatment in the Three Groups and the Results of Tukey Testa

Regarding the differences in the changes in cephalometric measurements between the two treatment groups utilizing either force magnitude (600 vs 300 g per side), no significant differences were found (P > .05) except in ramus height (Ar-Go). The reduction in ramus height was more pronounced with the utilization of 600 g of force per side than the use of 300 g of force per side (P < .05).
DISCUSSION
The effect of the orthopedic appliances depends on several factors, such as the applied force magnitude, wearing time of the appliance per day, and the duration of treatment.21 The influence of using two orthopedic force magnitudes (300 and 600 g per side) with a chin cup was the scope of this study.
The results of this investigation showed that the SNB angle was significantly decreased in the treatment groups in comparison with the untreated control group. Similar findings were found in previous chin cup studies.1,10–13,24 Such decreases in the SNB angle could be attributed to either restraint in mandibular growth or distal displacement and clockwise rotation of the mandible.1 With regard to changes in the mandibular corpus (Go-Me) among the investigated groups, no significant changes were found in the treatment groups in comparison to the control group. This finding was in agreement with those of Üçüncü et al.1 On the other hand, it differed from the findings of Mitani and Fukazawo.25 Growth of mandibular ramus height (Ar-Go) was significantly decreased in the treatment groups in comparison with the untreated group. These results are compatible with those of other studies.11,12 Reduction of the ramus height could be attributed to the use of the occipital-pull head cap, with the chin cup providing a posterosuperior orthopedic force; hence, pressure was exerted on the superior border of the condyle that could affect vertical mandibular growth.1,22 However, they were in contrast to those of other investigators, who found an increase in ramus height, which was attributed to forward bending of the condylar head.1,14,25 The mandibular length (Ar-Me) showed no noticeable changes among the three groups in the present study. These results are in agreement with those of other investigations aiming to clarify the effects of the chin cup.14 The gonial angle was decreased in the treatment groups; however, this reduction was not significant. These results matched those of other investigations.1,11,26 On the other hand, they contrasted with those presented by other authors.14 However, it was reported that the degree of changes in the gonial angle seemed to be unpredictable.27
In the present study, utilization of a chin cup had no significant effect on maxillary growth, as represented by the SNA angle. This finding is in agreement with those reported in other studies.1,10–13,24 On the other hand, a contrasting result was reported by another investigation,14 which found a significant increase in the SNA angle with the use of a chin cup. The authors suggested that the correction of crossbite could accelerate forward growth of the maxilla. However, the differing results could be a result of the longer treatment time (19 months) of the cited study vs the treatment time in the present study (12 months).
One of the significant effects of chin cup use was the improvement in the relationship of the maxillary and mandibular bases. This was manifested by a significant increase in the ANB angle and Wits appraisal in the treatment groups in comparison with the control group. The decrease in the SNB angle and clockwise rotation of the mandible were responsible for the improvement in the ANB angle and Wits appraisal. These findings are in agreement with those reported in previous studies.1,10–13,18
The anterior facial height (N-Me) and mandibular plane angle (SN-MP) were significantly increased in the treatment groups in comparison with the control group. The backward and downward rotation of the mandible could be responsible for this result. This finding was in agreement with those presented in previous studies on the same topic.1
In general, limited mandibular skeletal effects of the chin cup were found in the present study, irrespective of the use of the two different force magnitudes. This could be explained by the use of a heavier force for a longer duration. This may be essential to obtain the adequate force levels throughout the growing area of the condyle and hence affect growth.22 Such aggressive forces and long duration are applicable only in experimental animal studies, which revealed significant restriction of mandibular growth with the use of a chin cup.16,17
In the present investigation there was significant retroclination of the mandibular incisors in the treatment groups in relation to the control group. This retroclination was observed in previous chin cup studies.12,28 The use of a soft chin cup (not acrylic) in the present study could be responsible for this finding.22
In the present study, no significant differences were found when comparing the effects of the two forces used (300 and 600 g per side) (P > .05). The exception was the ramus height, which was significantly more reduced when the higher force was used (P < .05). Such a decrease could be attributed to the use of 600 g of force per side, which was capable of producing changes at the condyle area and remodeling at the angle of the mandible. The small differences between the use of either force in the present study were in contrast to findings of other investigators,21 who reported that the use of a chin cup with lighter force resulted in more skeletal effects than the use of a chin cup with heavier force. This could be explained by the difference in investigation time between their study (24 months) compared to that of the present one (12 months). In addition, in their study, the wearing time of the chin cup was shorter with the heavier force (10 hours per day), while wearing time was constant in the present study (14 hours per day). Furthermore, it was reported that wearing a chin cup for more than 9 hours and fewer than 15 hours per day could affect the direction of chin growth, as alteration of the direction was limited to the period that the force was applied.27,29
CONCLUSIONS
The use of a chin cup significantly improved the mandibular and maxillary relationship, but with only minor skeletal effects.
The use of a chin cup significantly reduced the ramus height and increased the anterior facial height, mandibular plane angle, and retroclination of the mandibular incisors.
Utilization of either 300 or 600 g per side as the chin cup retraction force had the same effect, except that the latter had a more pronounced effect in the reduction of ramus height.
REFERENCES
- 1.Üçüncü N, Üçem T, Yüksel S. A comparison of chincap and maxillary protraction appliances in the treatment of skeletal Class III malocclusions. Eur J Orthod. 2000;22:43–51. doi: 10.1093/ejo/22.1.43. [DOI] [PubMed] [Google Scholar]
- 2.Cozza P, Marino A, Mucedero M. An orthopaedic approach to the treatment of Class III malocclusion in the early mixed dentition. Eur J Orthod. 2004;26:191–199. doi: 10.1093/ejo/26.2.191. [DOI] [PubMed] [Google Scholar]
- 3.Kapust A. J, Sinclair P. M, Turley P. K. Cephalometric effects of face-mask/expansion therapy in Class III children: a comparison of three age groups. Am J Orthod Dentofacial Orthop. 1998;113:204–212. doi: 10.1016/s0889-5406(98)70141-6. [DOI] [PubMed] [Google Scholar]
- 4.Baccetti T, Franchi L, McNamara J. Treatment and posttreatment craniofacial changes after rapid maxillary expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2000;118:404–413. doi: 10.1067/mod.2000.109840. [DOI] [PubMed] [Google Scholar]
- 5.Ulgen M, Firatli S. The effects of the Fränkel's function regulator on the Class III malocclusion. Am J Orthod Dentofacial Orthop. 1994;105:561–567. doi: 10.1016/S0889-5406(94)70140-7. [DOI] [PubMed] [Google Scholar]
- 6.Kidner G, DiBiase A, DiBiase D. Class III Twin Blocks: a case series. J Orthod. 2003;30:197–201. doi: 10.1093/ortho/30.3.197. [DOI] [PubMed] [Google Scholar]
- 7.Giancotti A, Maselli A, Mampieri G, Spanò E. Pseudo-Class III malocclusion treatment with Balters' Bionator. J Orthod. 2003;30:203–215. doi: 10.1093/ortho/30.3.203. [DOI] [PubMed] [Google Scholar]
- 8.Tuncer C, Uner O. Effects of a magnetic appliance in functional Class III patients. Angle Orthod. 2005;75:768–777. doi: 10.1043/0003-3219(2005)75[768:EOAMAI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Clark W. J. Twin Block Functional Therapy. London, UK: Mosby-Wolfe; 1995. [Google Scholar]
- 10.Deguchi T, McNamara J. A., Jr Craniofacial adaptations induced by chincup therapy in Class III patients. Am J Orthod Dentofacial Orthop. 1999;115:175–182. doi: 10.1016/s0889-5406(99)70346-x. [DOI] [PubMed] [Google Scholar]
- 11.Graber L. W. Chincup therapy for mandibular prognathism. Am J Orthod. 1977;72:23–41. doi: 10.1016/0002-9416(77)90122-1. [DOI] [PubMed] [Google Scholar]
- 12.Ritucci R, Nanda R. The effect of chincup therapy on the growth and development of the cranial base and midface. Am J Orthod Dentofacial Orthop. 1986;90:475–483. doi: 10.1016/0889-5406(86)90107-1. [DOI] [PubMed] [Google Scholar]
- 13.Deguchi T, Kuroda T, Minoshima Y, Graber T. M. Craniofacial features of patients with Class III abnormalities: growth related changes and effects of short-term and long-term chincup therapy. Am J Orthod Dentofacial Orthop. 2002;121:84–92. doi: 10.1067/mod.2002.120359. [DOI] [PubMed] [Google Scholar]
- 14.Gokalp H, Kurt G. Magnetic resonance imaging of the condylar growth pattern and disk position after chin cup therapy: a preliminary study. Angle Orthod. 2005;75:568–575. doi: 10.1043/0003-3219(2005)75[568:MRIOTC]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Tuncer B. B, Kaygisiz E, Tuncer C, Yuksel S. Pharyngeal airway dimensions after chin cup treatment in Class III malocclusion subjects. J Oral Rehab. 2009;36:110–117. doi: 10.1111/j.1365-2842.2008.01910.x. [DOI] [PubMed] [Google Scholar]
- 16.Janzen E. K, Bluher J. A. The cephalometric, anatomic and histologic changes in Macaca mulatta after application of a continuous acting retracting force on the mandible. Am J Orthod. 1965;51:823–855. doi: 10.1016/0002-9416(65)90251-4. [DOI] [PubMed] [Google Scholar]
- 17.Noguchi K. Effects of extrinsic forces on the mandibular condyle of young rat: observations using 3H-thymidine autoradiography. J Jap Stomatological Soc. 1970;37:222–241. doi: 10.5357/koubyou.37.222. [DOI] [PubMed] [Google Scholar]
- 18.Thilander B. Treatment of Angle Class III malocclusion with chin cup. Trans Eur Orthod Soc. 1963;39:384–398. [Google Scholar]
- 19.Tanne K, Chieh-Li Lu Y, Tanaka E, Sakuda M. Biomechanical changes of the mandible from orthopaedic chin cup force studied in a three-dimensional finite element model. Eur J Orthod. 1993;15:527–533. doi: 10.1093/ejo/15.6.527. [DOI] [PubMed] [Google Scholar]
- 20.Deguchi T, Kitsugi A. Stability of changes associated with chin cup treatment. Angle Orthod. 1996;66:139–146. doi: 10.1043/0003-3219(1996)066<0139:SOCAWC>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Katashiba S, Deguchi Sr T, Kageyama T, Minoshima Y, Kuroda T, Roberts W. E. The aggressive chin cup protocol (14 h/day for 2 years with excellent compliance) depends on commitment to overcorrection of the skeletal Class III malocclusion. Orthod Waves. 2006;65:57–63. [Google Scholar]
- 22.Proffit W. R, Fields H. W, Jr, Sarver D. M. Contemporary Orthodontics. 4th ed. St Louis, MO: Mosby; 2007. [Google Scholar]
- 23.Iida Y, Deguchi T, Kageyama T. Chin cup treatment outcomes in skeletal Class III dolicho- versus nondolichofacial patients. Angle Orthod. 2005;75:576–583. doi: 10.1043/0003-3219(2005)75[576:CCTOIS]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Irie M, Nakamura S. Orthopedic approach to severe skeletal Class III malocclusion. Am J Orthod. 1975;67:377–392. doi: 10.1016/0002-9416(75)90020-2. [DOI] [PubMed] [Google Scholar]
- 25.Mitani H, Fukazawo H. Effects of chincap force on the timing and amount of mandibular growth associated with anterior reversed occlusion (Class III malocclusion) during puberty. Am J Orthod Dentofacial Orthop. 1986;90:454–463. doi: 10.1016/0889-5406(86)90105-8. [DOI] [PubMed] [Google Scholar]
- 26.Sakamoto T, Iwase I, Uka A, Nakamura S. A roentgenocephalometric study of skeletal changes during and after chin cap treatment. Am J Orthod. 1984;85:341–350. doi: 10.1016/0002-9416(84)90191-x. [DOI] [PubMed] [Google Scholar]
- 27.Mitani H, Sakamoto T. Chin cap force to a growing mandible; long-term clinical reports. Angle Orthod. 1984;54:93–122. doi: 10.1043/0003-3219(1984)054<0093:CCFTAG>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 28.Allen R. A, Conolly I. H, Richardson A. Early treatment of Class III incisor relationship using the chincup appliance. Eur J Orthod. 1993;15:371–376. doi: 10.1093/ejo/15.5.371. [DOI] [PubMed] [Google Scholar]
- 29.Jo K, Mitani H, Kawarada T. Displacement of chin to daily hours of chin cap use. J Michinoku Dent Soc. 1980;11:80–81. [Google Scholar]