

Abstract
Objective
To compare the amount of alleviation of lower anterior crowding and changes in intercanine width (ICW), intermolar width (IMW), and arch depth (AD) dimensions using 2 different types of nickel-titanium (NiTi) archwires.
Methods
Thirty participants were randomly allocated to 2 treatment groups, using heat-activated NiTi (HANT) or super-elastic (SE-NiTi) round (0.014”) archwires. The inclusion criteria were a Little’s Irregularity Index (LII) greater than 4, malocclusion requiring non-extraction therapy, all teeth erupted to the second molars in the lower arch, and Angle’s Class I malocclusion. The primary aim was to measure alleviation in mandibular crowding over 12 weeks; the secondary aim was to measure changes in ICW, IMW, and AD during those 12 weeks. Simple randomization was performed. The measurements were made on dental stone casts using a coordinate measuring machine at 4-week intervals.
Results
LII at 0, 4, 8, and 12 weeks was 8.59 ± 1.44, 6.17 ± 1.65, 4.65 ± 1.63, and 3.28 ± 1.57 mm in the HANT; 8.87 ± 1.29, 6.92 ± 1.49, 5.25 ± 1.32, and 3.63 ± 1.32 mm in the SE-NiTi group, respectively. ICW increased from 25.43 ± 1.39 to 27.41 ± 1.29 mm in the HANT and from 25.81 ± 1.78 to 27.27 ± 1.83 mm in the SE-NiTi groups over a period of 12 weeks, at P < .05. There was a statistically significant increase in IMW, CAD (canine arch depth), and MAD (molar arch depth), favoring the HANT group (P < .05). No significant differences in LII between the 2 groups were noted (P > .05).
Conclusions
The amount of alleviation of lower anterior crowding was similar with both archwires. ICW, IMW, and AD increased with HANT archwires.
Keywords: Orthodontic wire, nitinol, crowding, arch dimensions, coordinate measuring machine, tooth movement
Introduction
Fixed appliance therapy is a pillar of contemporary orthodontic treatment, in which archwires are used for force application. The aim of using aligning archwires at treatment initiation is primarily to alleviate crowding. Aligning archwires use light forces to move teeth, thereby reducing root resorption.1 The dimensional and physical–chemical properties of an archwire determine the amount of force delivered clinically. Ideal properties of aligning archwires include a large range of activation, flexibility, low modulus of elasticity with reduced friction, low cost, and ease of manufacture.2
Stainless steel (SS) archwires were the clinicians’ first choice before the introduction of nickel-titanium (NiTi) archwires.3 Subsequent developments led to the production of stabilized NiTi alloys by “Unitek Corporation” under the trade name Nitinol (Nickel Titanium Naval Ordinance Laboratory), for clinical use. This archwire soon replaced SS wires. Further searches for a better archwire for orthodontic use led to the development of super-elastic NiTi (SE-NiTi) alloys in 1978. Many modifications in archwire properties were made to obtain an ideal archwire with definite clinical advantages. One was the addition of copper (Cu) to NiTi wires, called Copper-NiTi (CuNiTi) wire or heat-activated archwires. These archwires demonstrated true shape-memory effects above the transition temperature range.
Adding Cu to the NiTi alloy improves shape-memory properties, thermal stability, and fatigue endurance; mitigates hysteresis and loading stress; and helps regulate transition temperature range.4,5 These effects help in accelerating tooth movement.6 Different compositions of NiTi alloy archwires with varied mechanical properties have shown various advantages in the literature.6,7 However, most studies have been in vitro and require validation by in vivo studies. The findings obtained from in vitro6,7 conditions are ambiguous compared to in vivo studies.8-10 Two studies11,12 showed contrasting results of alignment efficiency, where no significant difference was noted between Cu-NiTi and NiTi archwires. Conversely, another study13 found that heat-activated NiTi (HANT) was more efficient in aligning teeth. Weiland et al.14 demonstrated greater efficiency with SE-NiTi wires but with higher root resorption. These conflicting findings from multiple investigators make it difficult to gauge which archwire is better in terms of performance or alignment.15
The purpose of the present study was to investigate differences in the degree of alleviation of lower anterior crowding using SE-NiTi and HANT round archwires for alignment. It also aimed to assess intermandibular arch dimensional changes over 12 weeks using a coordinate measuring machine (CMM). The authors hypothesized that no difference would be observed between SE-NiTi and HANT archwires in the alleviation of lower anterior crowding over 12 weeks. The second hypothesis was that no difference would exist between SE-NiTi and HANT archwires in intermandibular arch dimensional changes in the same period.
Methods
This study was a single-center prospective trial conducted in the Department of Orthodontics and Dentofacial Orthopaedics. Before recruitment, the research protocol was accepted by the ethical committee of the Institute (ACDS/IEC/32/Oct 2018). All participants were given a research participant information sheet, which detailed why the research was being conducted, what it would involve, and what was expected of them as participants. The participants completed a questionnaire about past dental and medical history and were subsequently evaluated intraorally to assess Angle’s classification of molar relation and Little’s Irregularity Index (LII).
The inclusion criteria were (a) requiring fixed orthodontic treatment, (b) lower anterior crowding with LII greater than 4, (c) all teeth erupted to the second molars in the lower arch, (d) malocclusion requiring only non-extraction therapy, (e) Angle’s Class I malocclusion, and (f) maximum contact point displacement of 2.5 mm. Patients using medication, or with spacing in the lower anterior segment, or a blocked-out tooth that would not permit bonding in initial alignment, missing lower incisors and/or canines, periodontally compromised dentition, or previous history of orthodontic treatment were excluded. Those eligible to participate in the study signed a consent form.
The 30 included participants were allocated randomly in a 1 : 1 ratio to either of the 2 archwire groups, namely group 1: 0.014” HANT (3M Unitek, Monrovia, USA) or group 2: 0.014” Super-Elastic NiTi (3M Unitek, Monrovia, USA). A CMM was used to measure mandibular anterior irregularity (LII), intercanine width (ICW), intermolar widths (IMW), and arch depth (AD) on the lower cast, at 0, 4, 8, and 12 weeks. A monitoring committee was established to evaluate participant criteria and protocols. No changes were made to established protocols. Simple randomization using a computer-generated table at the beginning of the study allocated the archwires to participants. The allocated archwires were concealed in opaque envelopes, ensuring that both the investigator and participants were blind to the intervention. One author was responsible for the randomization. Both participants and investigators were blinded to the allocation of the archwire group, because the wires were provided in an opaque envelope to the clinician at the time of archwire placement. The investigators were also blinded to outcome measurements because each retrieved dental cast was assigned a number to innominate the data. A single operator treated all enrolled participants using 0.022” × 0.028” slot MBT prescription brackets (Mini-Twin™, Ormco Corp, Orange, CA, USA). The archwires used in the study were (a) 0.014” HANT (3M Unitek, Monrovia, USA) and (b) 0.014” Super-Elastic NiTi (3M Unitek, Monrovia, USA) with ovoid arch form. Teeth were etched with etching gel for 15 seconds. Ortho Solo™ (Ormco Corp, Orange, CA, USA) universal sealant and bond enhancer and Enlight light cure adhesive (Ormco Corp, Orange, CA, USA) were used for bracket bonding. After placement of brackets, an impression of the lower arch was made with alginate for each participant. The assigned archwire was then removed from the sealed envelope and ligated using elastomeric modules. The wire was removed at the next appointment and an impression with alginate was made again. This impression was poured in dental stone Type III. The same archwires were placed again using fresh elastomeric modules. Digital photographs of the lower arch were also obtained at each 4-week interval (Figure 1). At 8 and 12 weeks, the same process was replicated. The dental stone models were adjusted to be precisely positioned in the CMM (Figure 2). Specific points for each tooth were noted in 3 dimensions for all 6 lower anteriors. The central fossa of first molars, cusp tips of canines, and incisal edges of incisors were considered. Measurements of LII, ICW, IMW, and AD were made in the lower arch. ICW was assessed from cusp tips of bilateral lower canines and IMW was measured from central fossae of bilateral first molars. AD was assessed at 2 sites: intermolar depth and intercanine depth as the perpendicular distance from the most prominent lower central incisor to the respective IMW and ICW lines (Figure 3). All measurements were made using a CMM (Explorer Performance, Hexagon Manufacturing Intelligence, Stockholm, Sweden) by one author, who was unaware of the archwire being tested (Figure 4). The measurements were then repeated by another author to assess the reproducibility of measurements. LII, ICW, IMW and AD were noted at all stages. To reflect overall tooth movement, data recorded for intertooth distances (3-2, 2-1, 1-1, 1-2, 2-3) at all 4-week intervals were summed. Thus, the mean alignment value for the lower anterior segment at each phase was attained. The primary outcome was to assess the amount of alleviation of lower anterior crowding with 0.014” SE-NiTi and 0.014” HANT archwires over 12 weeks in non-extraction therapy. A secondary outcome was to assess changes in ICW, IMW, and AD using these archwires for the same duration. No modifications in result assessments were made after the start of the trial.
Figure 1.

(A-D) Alignment at every 4-week interval using heat-activated NiTi; (E-H) Alignment at every 4-week interval using super-elastic NiTi.
Figure 2.

Dental stone models obtained at every 4-week interval.
Figure 3.
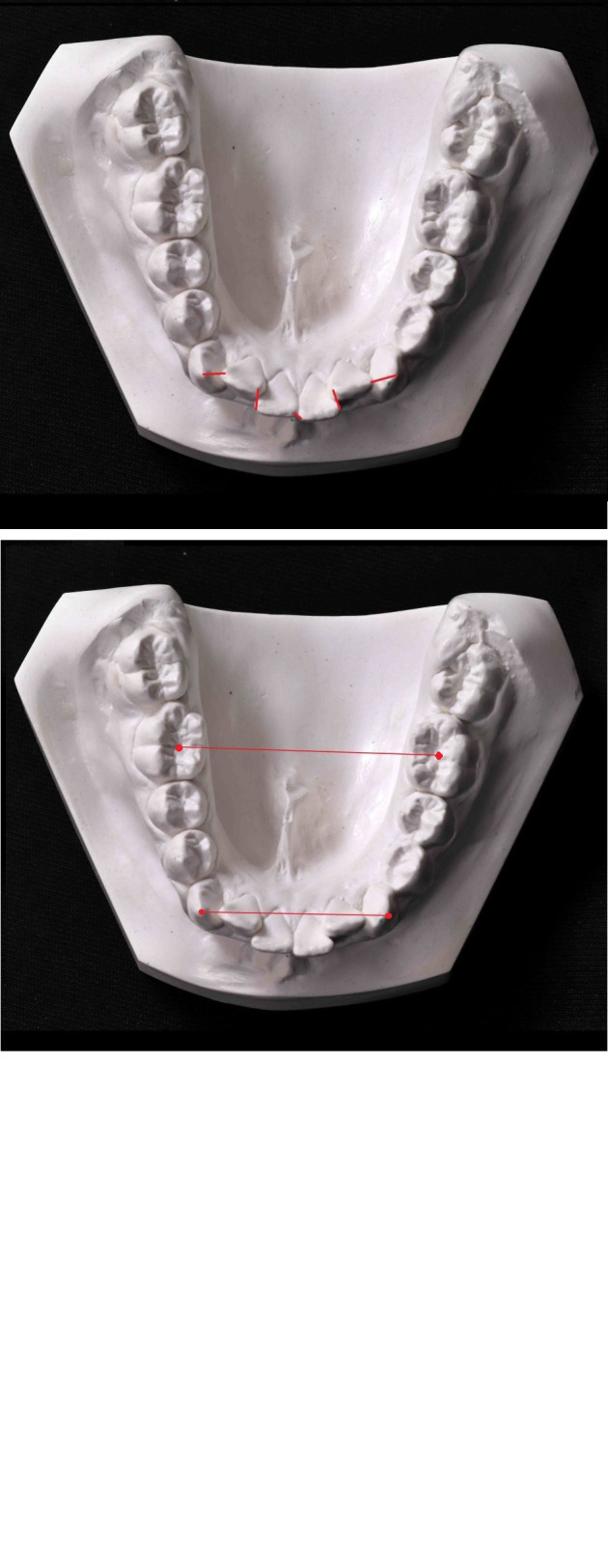
Mandibular measurements: Little’s irregularity index, intercanine width, and intermolar width and arch depth.
Figure 4.

Coordinate measuring machine (Explorer Performance, Hexagon Manufacturing Intelligence, Stockholm, Sweden).
Statistical Analysis
Sample size estimation was performed according to the study by Sebastian.16 The sample size was estimated using G Power software 3.1 using analysis of variance (ANOVA): repeated measures within-between interaction design. Effect size (partial eta squared) (n 2) [effect size measure for interaction between the within and between-subject variables, i.e., between wire and time] was calculated assuming medium (n 2 = 0.06) partial eta squared conversion, and thus effect size determined was 0.2526. Keeping alpha error at 5% or 0.05, statistical power at 90%, assuming correlation among repeated measures 0.5 and non sphericity correction (ε=1), the sample size estimated was 15 per group.
The Statistical Package for Social Sciences version 22.0 software (IBM Corp.; Armonk, NY, USA) was used to perform statistical analyses. Descriptive analysis of all the explanatory and outcome parameters was performed using mean and standard deviation for quantitative variables and frequency and proportions for categorical variables. Independent Student’s t-test was used to compare LII values, ICW, IMW, CAD, and MAD between the 2 groups at different time intervals. Repeated Measures of ANOVA followed by Bonferroni's post hoc analysis was used to compare the mean values of different study parameters between time intervals in each study group. Intra-class correlation (ICC) statistics were used to assess the reproducibility of study measurements between 2 observers at baseline and 12 weeks. The level of significance was set at P < .05.
Results
Participants were recruited over 1 year (July 2018 to July 2019). Sixty-three prospective participants were reviewed for enrolment; 30 were disqualified because they did not meet the inclusion criteria. Three refused to take part. Thirty participants were randomly assigned to either group 1: HANT (n = 15) with a mean age of 17.4 ± 1.12 or group 2: SE-NiTi (n = 15) with a mean age of 17.13 ± 0.92 at the start. A CONSORT diagram (Figure 5) illustrates participant flow throughout the analysis. Table 1 and Table 2 display no significant disparities in statistical or preliminary information between the groups in terms of age, gender or initial amount of crowding.
Figure 5.

CONSORT flow diagram.
Participants were examined at every follow-up for any bracket breakages, though none were reported. The LII, ICW, IMW, and AD of all 120 casts retrieved during this 12-week study were determined using a CMM, and values were rounded off to the nearest 0.1 mm.
A mean reduction in LII was noted from 8.59 to 3.28 mm for Group 1, and from 8.87 mm to 3.63 mm for Group 2, over a period of 12 weeks. The Student's t-test comparing the means between both the HANT (mean reduction of 5.31 mm) and SE-NiTi groups (mean reduction of 5.24 mm) indicated that LII was not statistically significant at the 5% level (Table 1 ) over a period of 12 weeks.
Table 1.
Comparison of Group 1 and 2 regarding age, initial crowding, reduction in crowding and changes in arch width and depths from week 0 to 12 by Independent Student t test
| Variable | Group 1 | Group 2 | P | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age | 17.4 | 1.12 | 17.13 | 0.92 | .48a |
| Initial crowding | 8.59 | 1.44 | 8.87 | 1.29 | .59a |
| Reduction in LII | 5.31 | 0.28 | 5.24 | 0.24 | .442 a |
| Change in ICW | -1.98 | 0.24 | -1.46 | 0.22 | .001*a |
| Change in IMW | -1.41 | 0.15 | -1.14 | 0.15 | .001*a |
| Change in CAD | -0.67 | 0.18 | -0.49 | 0.13 | .006*a |
| Change in MAD | -0.62 | 0.12 | -0.52 | 0.08 | .012*a |
*Statistically significant at p≤0.05, a: Independent Student t Test, SD: Standard deviation, Group 1: Heat activated NiTi, Group 2: Superelastic NiTi; LII: Irregularity index; ICW: Intercanine width, IMW: Intermolar width, CAD: canine arch depth, MAD: molar arch depth.
However, Table 3 shows that the amount of ICW, IMW, CAD, and MAD increased over a period of 12 weeks, favoring the HANT group. Table 3 portrays the pattern of decline in crowding as assessed with repeated measures ANOVA. LII at 0, 4, 8, and 12 weeks was 8.59 ± 1.44, 6.17 ± 1.65, 4.65 ± 1.63, and 3.28 ± 1.57 in HANT, and 8.87 ± 1.29, 6.92 ± 1.49, 5.25 ± 1.32, and 3.63 ± 1.32 in SE-NiTi group, respectively. ICW increased from 25.43 ± 1.39 to 27.41 ± 1.29 in the HANT and from 25.81 ± 1.78 to 27.27 ± 1.83 in the SE-NiTi groups over a period of 12 weeks. IMW increased from 37.13-38.54 to 40.18-41.32, respectively, in the HANT and the SE-NiTi groups at 12 weeks.
Table 2.
Gender distribution regarding Group 1 and Group 2
| Variable | Category | Group 1 | Group 2 | P | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | Males | 6 | 40.0% | 7 | 46.7% | .71b |
| Females | 9 | 60.0% | 8 | 53.3% | ||
b: Chi Square Test, n: number, Group 1: Heat activated NiTi, Group 2: Superelastic NiTi.
Table 3.
Comparison of LII, ICW, IMW, Canine AD, and Molar AD values between time intervals in Group 1 and Group 2 using Repeated Measures of ANOVA Test
| Group 1 | Group 2 | Difference Between Weeks | |||||
|---|---|---|---|---|---|---|---|
| Parameter | Interval | Mean | SD | Mean | SD | Group 1 | Group 2 |
| LII | 0 weeks | 8.59 | 1.44 | 8.87 | 1.29 | a = 0.001** b = 0.001** c = 0.001** |
a = 0.001** b = 0.001** c = 0.001** |
| 4 weeks | 6.17 | 1.65 | 6.92 | 1.49 | |||
| 8 weeks | 4.65 | 1.63 | 5.25 | 1.32 | |||
| 12 weeks | 3.28 | 1.57 | 3.63 | 1.32 | |||
| P value | .001* | .001* | |||||
| ICW | 0 weeks | 25.43 | 1.39 | 25.81 | 1.78 | a = 0.001** b = 0.001** c = 0.001** |
a = 0.001** b = 0.001** c = 0.001** |
| 4 weeks | 25.99 | 1.4 | 26.23 | 1.73 | |||
| 8 weeks | 26.78 | 1.36 | 26.92 | 1.85 | |||
| 12 weeks | 27.41 | 1.29 | 27.27 | 1.83 | |||
| P value | .001* | .001* | |||||
| IMW | 0 weeks | 37.13 | 3.24 | 40.18 | 1.83 | a = 0.010** b = 0.001** c = 0.001** |
a = 0.001** b = 0.001** c = 0.001** |
| 4 weeks | 37.43 | 3.16 | 40.53 | 1.74 | |||
| 8 weeks | 38.08 | 3.16 | 40.91 | 1.83 | |||
| 12 weeks | 38.54 | 3.19 | 41.32 | 1.82 | |||
| P value | .001* | .001* | |||||
| Canine AD | 0 weeks | 6.35 | 0.63 | 7.11 | 0.80 | a = 0.001** b = 0.001** c = 0.001** |
a = 0.001** b = 0.001** c = 0.001** |
| 4 weeks | 6.66 | 0.65 | 7.26 | 0.78 | |||
| 8 weeks | 6.80 | 0.65 | 7.40 | 0.77 | |||
| 12 weeks | 7.02 | 0.64 | 7.61 | 0.76 | |||
| P value | .001* | .001* | |||||
| Molar AD | 0 weeks | 24.32 | 0.93 | 25.34 | 0.65 | a = 0.001** b = 0.001** c = 0.001** |
a = 0.001** b = 0.001** c = 0.001** |
| 4 weeks | 24.56 | 0.96 | 25.56 | 0.63 | |||
| 8 weeks | 24.79 | 0.98 | 25.72 | 0.63 | |||
| 12 weeks | 24.94 | 0.97 | 25.86 | 0.62 | |||
| P value | .001* | .001* | |||||
*Statistically significant, group 1: heat-activated NiTi, group 2: super-elastic NiTi, a: 0 week * 4 week; b, 0 week * 8 week; c, 0 week * 12 week; **P < .05 adjusted Bonferroni correction.
SD, standard deviation; LII, irregularity index; ICW, intercanine width; IMW, intermolar width; AD, arch depth.
Canine AD and molar AD also significantly increased in both groups, favoring the HANT group, from 6.35 ± 0.63-7.02 ± 0.64 (mean increase of 0.67 mm) to 24.32 ± 0.93-24.94 ± 0.97 (mean increase of 0.62 mm), respectively, over 12 weeks. The repeated measure factor “time” showed statistical significance (P < .001). Bonferroni’s post hoc analysis of mean differences in LII, ICW, IMW, and AD between different time intervals (0 week * 4 week, 0 week * 8 week, 0 week *12 week) showed statistically significant differences at P < .001 (Table 3).
To check the reproducibility of measurements, all measurements were analyzed twice, by both authors, for all 120 casts retrieved in this study. The reproducibility of repeated measurements was estimated by ICC at 0 and 12 weeks. It demonstrated good reliability, ranging from 0.75 to 0.90 (Table 4).
Table 4.
Intra-class correlation statistics to assess for the reproducibility of measurements between 2 observers at baseline and 12 weeks
| Time | Variables | Group 1 | Group 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| ICC | 95% CI | P | ICC | 95% CI | P | ||||
| Lower | Upper | Lower | Upper | ||||||
| 0 Weeks | LII | 0.77 | 0.43 | 0.91 | .002* | 0.88 | 0.69 | 0.97 | <.001* |
| ICW | 0.8 | 0.47 | 0.92 | <.001* | 0.84 | 0.33 | 0.97 | <.001* | |
| IMW | 0.8 | 0.47 | 0.92 | <.001* | 0.88 | 0.57 | 0.99 | <.001* | |
| Canine AD | 0.82 | 0.46 | 0.85 | <.001* | 0.87 | 0.53 | 0.97 | <.001* | |
| Molar AD | 0.81 | 0.43 | 0.87 | <.001* | 0.86 | 0.54 | 0.87 | <.001* | |
| 12 Weeks | LII | 0.85 | 0.78 | 0.99 | <.001* | 0.89 | 0.7 | 0.97 | <.001* |
| ICW | 0.81 | 0.7 | 0.98 | <.001* | 0.88 | 0.7 | 0.98 | <.001* | |
| IMW | 0.79 | 0.46 | 0.98 | .001* | 0.85 | 0.73 | 0.98 | <.001* | |
| Canine AD | 0.87 | 0.51 | 0.89 | <.001* | 0.82 | 0.75 | 0.96 | <.001* | |
| Molar AD | 0.89 | 0.32 | 0.96 | .001* | 0.83 | 0.76 | 0.88 | <.001* | |
*Statistically significant group 1: heat-activated NiTi, group 2: super-elastic NiTi.
ICC values < 0.50—Poor reliability; 0.50-0.75—moderate reliability; 0.75-0.90—good reliability; > 0.90—excellent reliability.
ICC, intra-class correlation coefficient; CI, class interval; LII, Little’s irregularity index; ICW, intercanine width; IMW, Intermolar width; AD, arch depth.
Discussion
The first phase of fixed orthodontic treatment is leveling and alignment of the arches.17 Besides biological influences that are beyond the orthodontist’s influence, the choice of bracket system and archwires also has a significant impact on overall tooth movement.10
Several clinical trials have been performed to determine the efficiency of aligning archwires. Some have tried and failed to show one archwire’s superior efficacy in alignment over another,8,9,18,19 also others have reported no difference.3,16 Systematic analyses by Riley et al.20 and Jian et al.21 found that clinical studies had provided inadequate evidence for the most efficient alignment archwire. Additionally, the authors reported that more well-designed randomized clinical trials were needed.
SE-NiTi and HANT archwires were compared in the present study to evaluate the amount of alleviation of lower anterior crowding as a primary outcome. The secondary outcome was to assess changes in ICW, IMW, and AD over 12 weeks. Other factors which may affect the outcome were standardized, such as bracket slot dimensions, play between archwire and slot (same diameter archwires), and interbracket span (only in the mandibular arch) between both groups. Ages of the participants recruited were similar; the mean was 17.4 years for group 1 and 17.1 years for group 2.
NiTi archwires must be deformed by 50-70 degrees to properly utilize their super-elastic properties. This deformation is clinically possible due to the extent of crowding and shortened interbracket span in lower anterior crowding situations.22 In the analysis, an LII > 4 was considered to optimize the archwires' super-elastic properties.
No relevant differences were noted in gender distribution between the groups, also helping in establishing unbiased results.
The key outcome variable was the amount of mandibular decrowding observed over 12 weeks for both wires. The group treated with HANT wires had a mean LII of 3.28 (± 1.57) at 12 weeks, while it was 3.63 (± 1.32) for the group treated with SE-NiTi archwires. The null hypothesis was not rejected. This agrees with studies published previously.23,24
Experiments conducted in vitro have demonstrated that SE-NiTi wires produce light forces that increase tooth movement and reduce discomfort,1,25 though individual responses could act as confounding factors. Although these laboratory studies have shown the effectiveness of NiTi alloys characterized by superelasticity and shape-memory, the literature provides little clinical evidence supporting the benefits associated with these mechanical properties.26
West et al.3 reported greater alignment using SE-NiTi when compared to multistranded SS in the lower anterior region, which was attributed to reduced interbracket span. In their analysis, the amount of alleviation of lower anterior crowding was 1.20 mm compared to the 1.95 mm noted in this study. This minor variance may be due to differences in initial crowding in participants, differences in ligation methods, or archwires being sourced from different manufacturers.
A significant reduction in crowding was found with HANT in the initial period in the study. A mean reduction in LII of 2.42 mm was noted in the initial 4 weeks using HANT when compared to 1.95 mm using SE-NiTi. HANT provides the benefit of placing a large archwire with low force delivery at the start of treatment. Thus, at the outset of therapy, a better degree of rotational control and alignment was obtained relative to SE-NiTi wires, although the differences were not statistically significant.
Aydin et al.11 compared conventional and CuNiTi archwires in relieving lower crowding and found no substantialdifferences between them in the alleviation of crowding. Contrary to the findings of the present and other studies,9-12,24 Serafim et al.13 found greater alignment with HANT. However, in their study, the archwire diameter was increased substantially. Changes in arch form (transverse) during the alignment process using rectangular archwires are required in non-extraction cases to reduce crowding.27 The ICW changes were 1.46 mm with SE-NiTi and 1.98 mm with HANT. Previous studies have shown increases in ICW ranging from 0.54 to 1.96 mm.28 However, lower arch form should remain in harmony with surrounding structures, to increase long-term stability.29
Both archwires caused an increase in ICW and AD in the study, favoring the HANT group at P < .05, similar to Aydin et al.11 In this analysis, measurements of IMW in the SE-NiTi group were greater than HANT at the end of week 4, and this trend was reversed in the next 8 weeks. This is similar to findings by Aydin et al.,11 who attributed it to an increase in the arch perimeter of the lower canines.
Mandibular crowding can be measured using LII. Previous studies have found this index to be a reliable indicator that could be used to standardize research.30 The major drawback of LII is that it is not sensitive to rotations and axial inclinations. Two types of irregularity measurement methods exist: direct and indirect. Direct methods use Vernier calipers.9 Measurements can also be done indirectly for three-dimensional calculations using advanced instruments such as a reflex metrograph,8 reflection microscope,3 or CMM.16 The use of these specialized instruments provides a complete three-dimensional representation of movements of the contact point. Thus, a coordinate measuring system was used, which provided three-dimensional coordinates for each landmark on the dental casts, increasing the accuracy of measurements.
In clinical research, it is important to address the tendencies observed even when substantive differences are not found,18 because the statistical mean does not always represent the clinical outcome. HANT wires showed a higher rate of reduction in irregularity in the initial 4 weeks from bonding, although the differences were not statistically significant. This may be due to variations in the in vivo transition temperature ranges, limiting the transformation of NiTi archwires, or the general irrelevance of the wires' mechanical behavior derived from the laboratory to clinical loading conditions. Additional variables influencing the clinical output of wires may include the effect of oral cavity conditions.
A limitation of the study is that it was relatively short-term. Elastomeric modules were used for ligation. A drawback of using these modules is that full engagement of the archwires is not always possible due to rotations and/or crowding. SS ligatures were intentionally not used in the study because using 2 different ligation methods can lead to confounding results. Another drawback is that the effects of periodontal ligament and bone in individual metabolic responses were not discussed.
Conclusion
HANT exhibited no superiority over SE-NiTi archwires in the alleviation of lower anterior crowding. However, the changes in ICW, IMW, and AD favored HANT wires.
Funding Statement
The authors declared that this study has received no financial support.
Footnotes
Ethics Committee Approval: This study was approved by the Institutional Ethical Committee at Army College of Dental Sciences (ACDS/IEC/32/Oct 2018)
Informed Consent: Written informed consent was obtained from the patients who agreed to take part in the study.
Peer Review: Externally peer-reviewed
Author Contributions: Supervision – P.C.; Design – P.K.; Concept – P.K.; Resources – P.C., Materials – P.K.; Data collection/or processing – P.K.; Analysis and /or Interpretation – P.C.; Literature search – P.C.; Writing manuscript – P.K.; Critical review – P.C.
Conflict of Interest: The authors have no conflict of interest to declare.
References
- 1.Phermsang-Ngarm P, Charoemratrote C.Tooth and bone changes after initial anterior dental alignment using preformed vs customized nickel titanium archwires in adults: a randomized clinical trial. Angle Orthod. 2018;88(4):425–434.. 10.2319/090317-589.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lombardo L, Marafioti M, Stefanoni F, Mollica F, Siciliani G.Load deflection characteristics and force level of nickel titanium initial archwires. Angle Orthod. 2012;82(3):507–521.. 10.2319/032511-213.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.West AE, Jones ML, Newcombe RG.Multiflex versus superelastic: a randomized clinical trial of the tooth alignment ability of initial arch wires. Am J Orthod Dentofacial Orthop. 1995;108(5):464–471.. 10.1016/s0889-5406(95)70046-3) [DOI] [PubMed] [Google Scholar]
- 4.Velmurugan C, Senthilkumar V.The effect of Cu addition on the morphological, structural and mechanical characteristics of nanocrystalline NiTi shape memory alloys. J Alloys Compd. 2018;767:944–954.. 10.1016/j.jallcom.2018.07.217) [DOI] [Google Scholar]
- 5.Pompei-Reynolds RC, Kanavakis G.Interlot variations of transition temperature range and force delivery in copper-nickel-titanium orthodontic wires. Am J Orthod Dentofacial Orthop. 2014;146(2):215–226.. 10.1016/j.ajodo.2014.05.017) [DOI] [PubMed] [Google Scholar]
- 6.Gravina MA, Brunharo IH, Canavarro C, Elias CN, Quintão CC.Mechanical properties of NiTi and CuNiTi shape-memory wires used in orthodontic treatment. Part 1: Stress-strain tests. Dent Press J Orthod. 2013;18(4):35–42.. 10.1590/s2176-94512013000400007) [DOI] [PubMed] [Google Scholar]
- 7.Sarul M, Kowala B, Antoszewska J.Comparison of elastic properties of nickel-titanium orthodontic archwires. Adv Clin Exp Med. 2013;22(2):253–260.. [PubMed] [Google Scholar]
- 8.O'Brien K, Lewis D, Shaw W, Combe E.A clinical trial of aligning archwires. Eur J Orthod. 1990;12(4):380–384.. 10.1093/ejo/12.4.380) [DOI] [PubMed] [Google Scholar]
- 9.Pandis N, Polychronopoulou A, Eliades T.Alleviation of mandibular anterior crowding with copper-nickel titanium vs nickel-titanium wires: a double-blind randomized control trial. Am J Orthod Dentofacial Orthop. 2009;136(2):152.e1–7.. 10.1016/j.ajodo.2009.03.030) [DOI] [PubMed] [Google Scholar]
- 10.Abdelrahman RSh, Al-Nimri KS, Al Maaitah EF.A clinical comparison of three aligning archwires in terms of alignment efficiency: a prospective clinical trial. Angle Orthod. 2015;85(3):434–439.. 10.2319/041414-274.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aydın B, Şenışık NE, Koşkan Ö.Evaluation of the alignment efficiency of nickel-titanium and copper-nickel-titanium archwires in patients undergoing orthodontic treatment over a 12-week period: a single-center, randomized controlled clinical trial. Korean J Orthod. 2018;48(3):153–162.. 10.4041/kjod.2018.48.3.153) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gok F, Buyuk SK, Ozkan S, Benkli YA.Comparison of arch width and depth changes and pain/discomfort with conventional and copper Ni-Ti archwires for mandibular arch alignment. J World Fed Orthod. 2018;7(1):24–28.. 10.1016/j.ejwf.2018.01.001) [DOI] [Google Scholar]
- 13.Serafim CM, Gurgel Jde A, Tiago CM, Tavarez RR, Maia Filho EM.Clinical efficiency of two sequences of orthodontic wires to correct crowding of the lower anterior teeth. Sci World J. 2015;2015:1–15.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Weiland F.Constant versus dissipating forces in orthodontics: the effect on initial tooth movement and root resorption. Eur J Orthod. 2003;25(4):335–342.. 10.1093/ejo/25.4.335) [DOI] [PubMed] [Google Scholar]
- 15.Wang Y, Jian F, Lai W.Initial arch wires for alignment of crooked teeth with fixed orthodontic braces. Cochrane Database Syst Rev. 2010;4(4):CD007859. 10.1002/14651858.CD007859.pub2) [DOI] [PubMed] [Google Scholar]
- 16.Sebastian B.Alignment efficiency of superelastic coaxial nickel-titanium vs superelastic single-stranded nickel-titanium in relieving mandibular anterior crowding: a randomized controlled prospective study. Angle Orthod. 2012;82(4):703–708.. 10.2319/072111-460.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Proffit WR, Sarver DM, Fields HW.Contemporary Orthodontics. St. Louis, MO: Mosby Elsevier; 2007. [Google Scholar]
- 18.Evans TJW, Jones ML, Newcombe RG.Clinical comparison and performance perspective of three aligning arch wires. Am J Orthod Dentofacial Orthop. 1998;114(1):32–39.. 10.1016/s0889-5406(98)70234-3) [DOI] [PubMed] [Google Scholar]
- 19.Sandhu SS, Shetty VS, Mogra S.Efficiency, behavior, and clinical properties of superelastic NiTi versus multistranded stainless steel wires: a prospective clinical trial. Angle Orthod. 2012;82(5):915–921.. 10.2319/100311-622.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Riley M, Bearn DR.A systematic review of clinical trials of aligning archwires. J Orthod. 2009;36(1):42–51; discussion 15.. 10.1179/14653120722914) [DOI] [PubMed] [Google Scholar]
- 21.Jian F, Lai W, Furness S.Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances. Cochrane Database Syst Rev. 2013;4(4):CD007859. 10.1002/14651858.CD007859.pub3) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Heo W, Baek SH.Friction properties according to vertical and horizontal tooth displacement and bracket type during initial leveling and alignment. Angle Orthod. 2011;81(4):653–661.. 10.2319/072310-431.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Atik E, Gorucu-Coskuner H, Akarsu-Guven B, Taner T.A comparative assessment of clinical efficiency between premium heat-activated copper nickel-titanium and superelastic nickel-titanium archwires during initial orthodontic alignment in adolescents: a randomized clinical trial. Prog Orthod. 2019;20(1):46. 10.1186/s40510-019-0299-4) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mahmoudzadeh M, Farhadian M, Alijani S, Azizi F.Clinical comparison of two initial arch wires (A-NiTi and Heat activated NiTi) for amount of tooth alignment and perception of pain: A randomized clinical trial. Int Orthod. 2018;16(1):60–72.. 10.1016/j.ortho.2018.01.007) [DOI] [PubMed] [Google Scholar]
- 25.Francisconi MF, Janson G, Henriques JF, Freitas KM, Francisconi PA.Evaluation of the force generated by gradual deflection of 0.016-inch NiTi and stainless-steel orthodontic wires in self-ligating metallic and esthetic brackets. J Clin Exp Dent. 2019;11(5):e464–e469.. 10.4317/jced.55698) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tonner RIM, Waters NE.The characteristics of super-elastic Ni-Ti wires in three-point bending. Part I: the effect of temperature. Eur J Orthod. 1994;16(5):409–419.. 10.1093/ejo/16.5.409) [DOI] [PubMed] [Google Scholar]
- 27.Kim E, Gianelly AA.Extraction vs non-extraction: arch widths and smile Table: esthetics. Angle Orthod. 2003;73(4):354–358.. 10.1043/0003-3219(2003)073<0354:EVNAWA>2.0.CO;2) [DOI] [PubMed] [Google Scholar]
- 28.Burke SP, Silveira AM, Goldsmith LJ.A meta-analysis of mandibular intercanine width in treatment and post retention. Angle Orthod. 1998;68(1):53–60.. 10.1043/0003-3219(1998)068<0053:AMAOMI>2.3.CO;2) [DOI] [PubMed] [Google Scholar]
- 29.Sadowsky C, Sakols EI.Long-term assessment of orthodontic relapse. Am J Orthod. 1982;82(6):456–463.. 10.1016/0002-9416(82)90312-8) [DOI] [PubMed] [Google Scholar]
- 30.Tran AM, Rugh JD, Chacon JA, Hatch JP.Reliability and validity of a computer-based Little irregularity index. Am J Orthod Dentofacial Orthop. 2003;123(3):349–351.. 10.1067/mod.2003.76) [DOI] [PubMed] [Google Scholar]