

Abstract
High work relative value units (wRVU) per clinical full-time-equivalent (cFTE) productivity by Neonatologists have played a key role in enhancing departmental revenue in Pediatrics. However, such high productivity is not sustainable due to recent changes in trainee schedules and global daily codes and is likely to impact physician morale and wellness. Incentives based on wRVU benchmarks have the capacity to promote desirable behavior such as better documentation and in-person attendance in delivery room resuscitation and consults but comes at a cost of physician time providing care. An alternate method of funding academic Pediatric departments using time- or point-based staffing models, a reduction in productivity benchmarks for academic neonatologists through more accurate reporting of effort and physician leadership that promotes transparency and mutual respect are warranted to improve neonatologist well-being and morale.
Subject terms: Health care economics, Health occupations
Introduction
Neonatal-Perinatal Medicine continues to be the largest pediatric subspecialty in the US with over 7000 neonatologists certified by the American Board of Pediatrics (ABP) and nearly 400 undergoing initial certification in 2020 [1]. Pediatricians enter the field of Neonatal-Perinatal Medicine to provide compassionate and quality care to fragile newborn infants, secondary to an interest in research or quality improvement. Pediatric residents may also be persuaded by the relatively better financial reimbursement in Neonatology compared to other pediatric subspecialties [2–4]. Pediatric cardiologists, intensivists and neonatologists have the highest net present value (NPV) of lifetime earnings among pediatric subspecialists [3, 4] due to work relative value unit (wRVU) generating potential associated with procedures and critical care (Fig. 1) [5].
Fig. 1. Bar graph of benchmark wRVUs (work relative value units) in various Pediatric subspecialties per clinical full-time equivalent (cFTE).
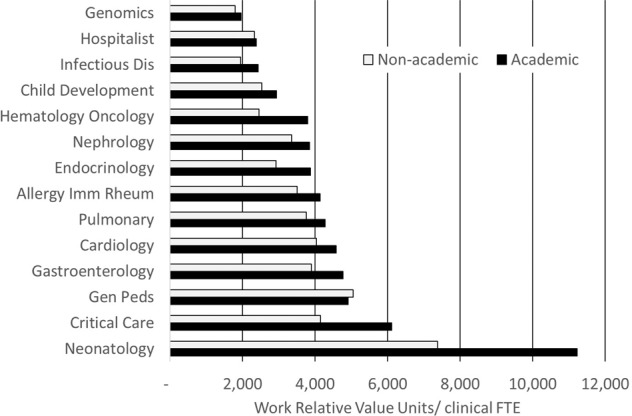
Academic benchmark data are based on 3-year average using clinical practice solutions center (CPSC) and Association of Administrators in Academic Pediatrics with some modifications used by the UC Davis Department of Pediatrics as benchmarks. The non-academic benchmarks are a 3-year average of several sources such as Medical Group Management Association (MGMA) with some modifications specific to UC Davis Health.
In a recent issue of the Journal of Perinatology, Dr. Mark Mercurio elegantly pointed out the perils of utilizing wRVUs to clinical full-time equivalent (cFTE) ratio to provide incentives to neonatologists [6]. Most CPT codes involved in the NICU are based on global daily billing based on the severity of infant’s illness (critical or intensive care). This wRVU/cFTE ratio for the most part is proportional to patient load per physician or average daily census (ADC) of the neonatal intensive care unit (NICU). Generating higher wRVU/cFTE ratio leads an increase in divisional and departmental revenue but is associated with a reduction in physician time per patient (Fig. 2) [6]. This manuscript is a brief review of basic principles of behavioral economics and pediatric departmental finances followed by methods to ensure adequate “neonatologist-time” for every patient. We also bring in a physician-leader’s perspective of balancing physician wellness to departmental financial stability [5].
Fig. 2. The vicious cycle of high wRVU/cFTE generation by academic neonatologists and impact on physician wellbeing and morale.
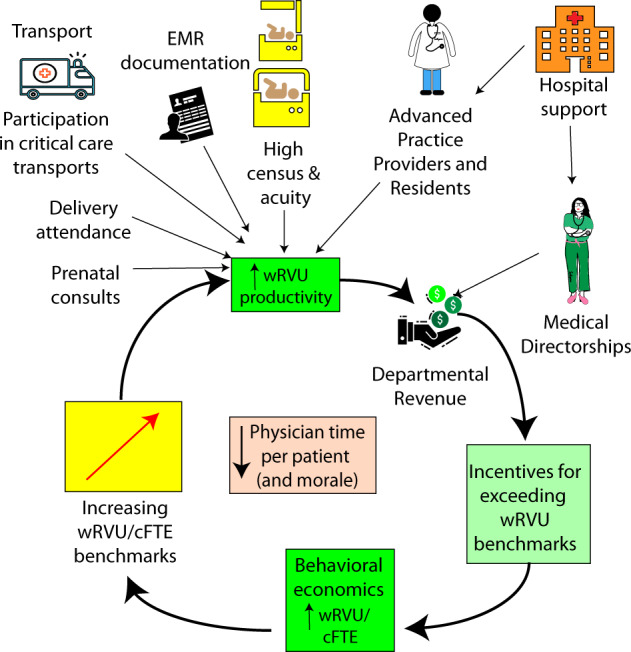
High census and acuity along with support for medical directorships from the hospital generate revenue for the department of Pediatrics.
Neonatology wRVU generation and departmental finances
Two decades ago, traditional NICU coverage included daily rounds by the attending neonatologist followed by evening and night coverage by fellows and residents. The attending neonatologist would provide backup support predominantly by phone with occasional in-person visits to the NICU. In this setting, the neonatologist covered large NICUs with high ADC and acuity resulting in high wRVU generation benchmarks. Neonatology division typically contributes to 20–35% of wRVUs in a Department of Pediatrics [7]. The wRVU benchmarks for Neonatology are almost twice as high as a pediatric intensivist and 3–6 times higher than other pediatric subspecialties in academic settings (Fig. 1). With reduced resident training in the NICU setting, more neonatologists are staying in-house providing 24 × 7 coverage [8]. With the advent of daily global codes in Neonatology, additional wRVU generation during night shift is limited to new admissions before midnight and certain select procedures. In addition to in-person night shifts, delivery room attendance, maternal consults and follow-up clinics are associated with lower wRVU generation compared to day-time critical/intensive care in the NICU. We speculate that these factors in academic NICUs are associated with a general decreasing trend among benchmark median wRVUs over the last 8 years (Fig. 3).
Fig. 3. Trends in median compensation (base and total) for Assistant professors in Neonatology and wRVU benchmarks for a full time cFTE.
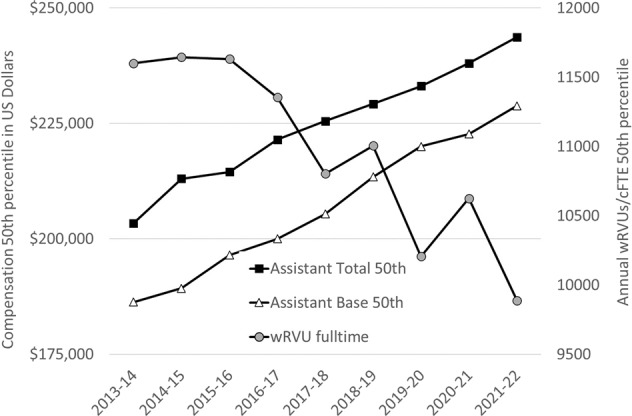
There is a 23% increase in median total salary with an 15% decrease in median wRVU benchmark. Based on Association of Administrators in Academic Pediatrics (AAAP) national data—with permission.
The compensation benchmarks for academic neonatologists, pediatric cardiologists and intensivists are similar, but the productivity benchmarks are over two-fold higher for neonatologists (Fig. 1). Neonatology divisions typically generate high cash collections contributing to departmental funds (Fig. 2). These funds are commonly needed to cross-subsidize subspecialists who provide consultations to the NICU and follow-up programs. High wRVU productivity and cash collections from neonatology are vital for the financial stability of Pediatric departments in traditional collections-based funds flow models. This results in tremendous pressure on Chiefs of Neonatology to generate wRVUs and patient revenue. Productivity incentives provided to neonatologists further increases wRVU/cFTE benchmarks setting up a vicious cycle leading to reduce physician time per patient and provider burnout (Fig. 2). [6]
Alternate models of departmental and divisional funds flow based on time spent and not wRVUs
Most academic Pediatric departments are currently in a collection-based model (based on cash received from insurance companies) or productivity model (based on wRVUs generated through billing and coding). The collection-based model penalizes a department for having a payor mix with high public insurance. Insurance denials also reduce departmental revenue. A productivity model is agnostic to payor mix and denials as it is based on wRVUs generated at the time of coding by the physician group. A third model that is becoming increasing popular is a staffing model where departmental revenue is based on either time spent or assigning points to various clinical activities such as level IV critical-care clinical service, step-down NICU service, follow-up clinic, consult service etc. [5]. In this model, there is no pressure to generate benchmark wRVUs and departmental reimbursement by the health system is based on time spent or points earned by faculty. In addition to using this model for base pay, an incentive based on value (antibiotic stewardship, provider scores on parental feedback surveys etc.,) can reinforce positive behavior. Widespread adaptation of staffing models in academic health centers and Pediatric departments will support adequate time for neonatologists to care for their patients and effectively engage parents in shared decision making without pressure to exceed high wRVU benchmarks. The first step in switching to a staffing model is to determine adequate number of providers to effectively provide compassionate patient care along with non-clinical priorities and missions of the division (Table 1).
Table 1.
Practical steps to managing transition away from a productivity (wRVU or collections $) based model.
| Level of intervention | Intervention |
|---|---|
| Neonatology Division |
∙ Clear definition of clinical FTE including standard administration/scholarly activity/teaching time given to all academic faculty ∙ Recruitment of adequate faculty to provide support to clinical and non-clinical missions of the division ∙ Accurate reporting of wRVUs excluding “moonlighting” within the division |
| Department of Pediatrics |
∙ Value vs. productivity-based incentives ∙ Budgets for inpatient divisions based on a staffing model (shift or time-based) vs. productivity ($ collections or wRVUs) ∙ Focus on provider wellness and job satisfaction to minimize burnout |
| Academic health center | ∙ Institution of an aligned strategic funds flow system that values the quadripartite mission of clinical, research, teaching, service addressing social determinants of health and promoting diversity, equity and inclusion |
| National organizations |
∙ Organize workshops and discussion sessions on appropriate definitions of clinical FTE that can be adopted by all academic Pediatric departments ∙ Efforts to improve financial literacy among providers ∙ Provide guidelines for reporting accurate benchmarks for productivity and compensation that take into account the academic mission of Pediatric departments |
Are there benefits to wRVU benchmarks?—physician incentives and behavioral economics
Motivation to meet (or exceed) productivity targets can be intrinsic (personal workplace satisfaction, recognition of individual contributions by division chief or chair) or extrinsic (financial incentives or penalties or non-financial awards such as “top-doctor” recognitions) [9, 10] Behavioral economists have studied how individuals can be “nudged” to make desirable choices [11]. There are no controlled studies evaluating financial incentives to achieve a sustainable increase in productivity in Pediatrics. However, providing incentives for productivity above wRVU/cFTE benchmarks is a common practice in Pediatric departments. Value-based incentives for low central line bloodstream infection (CLABSI) and reduced length of stay (LOS) adjusted for case mix index (CMI) at a divisional level are increasingly being practiced by hospital systems. The distinct advantage of using wRVUs is it allows fair comparison between various divisions within the department of Pediatrics (and different departments within a school of medicine) and is linked to financial returns without penalizing for payer mix.
Application of behavioral economics principles in Neonatology [10–12] (Fig. 4 and Table 2)
Fig. 4. Principles of behavioral economics in healthcare.

Motivation to achieve a desired target or behavior can be intrinsic or extrinsic (financial or non-financial). A target or behavior that is meaningful and worthwhile to the physician may bring personal workplace satisfaction leading to intrinsic motivation. A financial incentive that is reasonably large and providing immediately for achieving a target that neither too easy nor too hard to attain with effort is likely to motivate physicians.
Table 2.
Examples of behavioral economic principles in Neonatology: pros and cons.
| Principle | Example | Pro | Con |
|---|---|---|---|
| Goal gradient (target neither too easy nor too hard) | Incentives for a modest reduction in empiric antibiotic use in the NICU | Gradual promotion of positive behavior with metrics that can be accurately analyzed |
Extreme reduction may harm patients Ability to achieve target may depend on patient risk factors beyond the purview of the provider |
| Weber-Fechner law (incentive should be proportional to base) | The magnitude of performance-based bonus is proportional to base salary | Providers will notice and pay attention to targets/goals | Senior providers and Chiefs benefit more than junior providers for the same task |
| Immediacy (incentives paid close to work completion) | Work RVU based productivity bonus paid monthly instead of yearly | Immediate gratification |
Increased administrative work Variable pay (withholding a portion of base compensation if metrics are not met in subsequent months) may negatively impact morale |
| Nudging | Incentives to improve documentation and attendance at procedures | Increase divisional revenue | May lead to therapies that are not medically indicated |
| Loss aversion | Withholding a portion of bonus for poor chart completion rate | Penalty is more effective in changing behavior | Negative effect on faculty morale |
| Social ranking | Public display of top performer of the year (highest % of discharge orders by 10 am) | Intrinsic motivation at minimal cost | Providers with consistently low performance may perceive this as social shaming |
-
(i)
Goal gradients: Neonatologists are likely to work the hardest when the target is relatively attainable (neither too easy nor too hard) and is worthwhile. For example, empiric antibiotic use is highly variable in the NICUs to prevent early-onset sepsis but can lead to alteration of the baby’s microbiome [13, 14]. Targeting a reduction of early empiric antibiotic use among infants with negative cultures from 15% of all admits to 8% (or the state median) is achievable and worthwhile by improving the infant’s microbiome. Setting the target to 0% is unrealistic and unattainable increasing the risk of early-onset sepsis.
-
(ii)
Weber-Fechner law pertains to psychophysics and perception of a stimulus in relation to the magnitude of the base state. An observer might be able to notice a difference between a 10 g weight and a 15 g weight. However, it is difficult to notice a difference between 1000 g and 1005 g. Similarly, the magnitude of the incentive should be proportional to the base pay to be noticeable (at least 10%) and motivate positive behavior [10].
-
(iii)
Immediacy: In academic NICUs, census and acuity can be variable and not under the control of a neonatologist. There may be weeks of service that are busy with many critical neonates. Knowing that additional work is associated with a financial incentive (wRVU based bonus) can potentially be a source of immediate gratification [10, 11]. Paying these incentives as close to the completed work as possible is more gratifying than paying at the end of the year.
-
(iv)
Nudging: In some NICUs, attending physicians often do not accompany trainees on consults and delivery room resuscitation and just cosign these notes without billing. Providing wRVU based incentives can “nudge” neonatologists to accompany fellows, residents and advanced practice providers (APP) to delivery room resuscitation, maternal high-risk and newborn nursery consults. Incentives based on wRVUs can also enhance documentation of progress and discharge notes. For example, a statement explaining as to how a 5 LPM high flow nasal cannula provides crucial respiratory support without which the infant may experience respiratory distress and failure may justify as critical care (as opposed to intensive care) CPT code. Similarly, specifying time spent on a discharge (≤ 30 min vs. > 30 min) can result in higher-level coding. However, such incentives can also result in negative consequences. Provision of positive pressure ventilation (PPV) during resuscitation to secure a higher-level CPT code (99465 – neonatal resuscitation vs. 99464 – attendance at delivery) when not medically indicated or attending a delivery when not needed could potentially lead to billing for something medically unnecessary. We must be careful to prevent behavior resulting in medically unwarranted therapies due to incentive-based nudges.
-
(v)
Loss aversion and penalties: People feel twice as bad about a loss than they feel good about an equivalent gain [10]. Paying an incentive upfront with a threat to take a portion away if metrics are not met is more powerful motivator than paying a bonus at the end of the year. However, such a “penalty” may have a negative effect on faculty morale.
-
(vi)
Social ranking: If the goal is adherence to a quality control measure such as discharge orders by 10 AM, providing a ranking of all neonatologists and comparison to other inpatient pediatric subspecialists is effective in promoting change.
Some examples of application of these principles to Neonatology along with pros and cons to each intervention are shown in Table 2.
Redefining benchmarks for compensation and productivity
Work RVU benchmarks for academic neonatologists are very high and not sustainable. As shown in Fig. 1, academic productivity benchmarks for neonatology are twice that of pediatric critical care and five times that of pediatric hospitalists. An aggregate of non-academic benchmarks for productivity is also shown in Fig. 1 and is approximately two-thirds that of academic benchmarks for NICU and PICU but similar in other pediatric subspecialties. Traditionally, the higher benchmarks for academic NICUs and PICUs was secondary to support provided by fellows and residents, higher acuity and higher patient load per physician. The trend towards a decrease in wRVU benchmarks for academic neonatologists most likely reflects increased need for night coverage by attending physicians (Figs. 2 and 3), a more active role in prenatal consults, follow-up clinics, delivery room attendance and newborn nursery consults that generate low wRVUs compared to critical/intensive care in the NICU. More accurate reporting from academic Pediatric departments on wRVU generation, cFTEs, presence of APPs, moonlighting and incentive structure to benchmarking agencies such as Association of Administrators in Academic Pediatrics (AAAP), Association of American Medical Colleges (AAMC) and Clinical Practice Solutions Center (CPSC) is warranted so that productivity benchmarks for academic neonatologists are more reasonable (Table 1). For example, if a neonatologist is an Assistant Professor doing 22 weeks of clinical service with minimal teaching responsibilities and generates 9,000 wRVUs per year, the Department may report his/her clinical FTE as 0.5 (22 weeks/44 working weeks), 0.8, 0.9 or 1.0 (based on institutional ‘academic/administrative time’ definition). There is also variability in accounting for wRVUs generated from “moonlighting” (working additional shifts in the same institution above that required by that provider’s clinical FTE) in these calculations. Such additional wRVUs should not be included while reporting to benchmarking agencies. These variations result in marked differences in wRVU/1.0 cFTE. Appropriate and uniform definition of cFTE (e.g., at UC Davis, one week of NICU service—daytime = 0.04 cFTE; one week of in-house night shifts = 0.045 cFTE and one 4 h clinic or consults = 0.0025 cFTE) [5] across Pediatric departments may lead to more accurate wRVU/cFTE reporting in Neonatology.
Role of physician leadership—transparency and communication with respect
Neonatologists are perceiving themselves as “wRVU-productivity machines” chasing a target bar that keeps moving higher to meet the financial goals of Pediatric departments (Fig. 2). [6] Neonatal providers are increasingly frustrated due to lack of transparency and poor communication. Effective leadership at the Division Chief, Departmental Chair and Children’s hospital executive level plays an important role in promoting wellness through communication with respect, fairness, recognition of individual neonatologist’s contributions and transparency. [15] Physician leaders are traditionally chosen due to their academic productivity. [16] Non-physician executives often may primarily focus on clinical productivity and finance. Neither may be fully integrating the need for academic productivity, clinical productivity, financial impacts and physician wellness. Physician wellness and engagement undergirds excellence in all the other goals in the long-term. [17] The emergence of the physician executive as a representative of the frontline provider who understands the neonatologist-mindset and can also articulate and implement the vision of the healthcare organization is needed to meet business demands while maintaining physician wellness in Children’s hospitals.
Traditional leadership skills include crisis management, talent acquisition and delegation, and financial acumen with attributes such as courage, focus and intellectual curiosity. These leadership qualities need to be combined with consistent communication with transparency and respect, promotion of diversity and inclusion along with attributes such as adaptability and humility (Fig. 5). [16] This large skill set is rarely innate in any one person, and organizations should have leadership training within and outside the institution to assure capable faculty members turn into excellent leaders.
Fig. 5. Qualities, attributes and skills needed to be a physician leader in Neonatology and Pediatrics.

Traditional attributes (left section) such as being visionary, vigilant (to changes in birth rates, infant demographics and technological advances), financial wisdom, talent acquisition and management need to be combined with humility, adaptability (to challenges such as COVID-19), transparency and communication with respect (right side of the figure) to be an effective leader.
Conclusion
High wRVU per cFTE productivity by Neonatologists has played a key role in financial well-being of departments of Pediatrics. However, such high productivity is not sustainable due to recent changes in trainee schedules and global daily codes and is likely to impact physician morale and wellness. Incentives based on wRVU benchmarks have the capacity to promote desirable behavior such as better documentation and in-person attendance in delivery room resuscitation and consults but comes at a cost of physician time providing care. An alternate method of funding academic Pediatric departments using a time- or point-based staffing model [7] and a reduction in productivity (wRVU) benchmarks for academic neonatologists through more accurate reporting of effort along with physician leadership that promotes transparency and mutual respect are warranted to improve neonatologist well-being and morale. Neonatology divisions should not lose their way succumbing to the siren song of financial margins and wRVUs at the expense of quality, safety and other patient priorities along with physician wellness.
Author contributions
SL conceptualized the outline and drafted the initial manuscript. SO and DAL added additional sections, revised and edited the manuscript. All authors approved the final version of the manuscript.
Funding
There was no funding aside from salary support from UC Davis Health.
Data availability
The data that support the findings of this study are available from compensation and productivity benchmarking organizations such as Association of Administrators in Academic Pediatrics (AAAP) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of AAAP.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.ABP. The American Board of Pediatrics—2020 Annual Report. 2021 [cited December 4, 2021] Available from: https://www.abp.org/sites/abp/files/pdf/annual-report-2020.pdf.
- 2.Freed GL. The pediatric subspecialty workforce is more complex than meets the eye. JAMA Pediatrics. 2021;175:1006–8. doi: 10.1001/jamapediatrics.2021.1909. [DOI] [PubMed] [Google Scholar]
- 3.Catenaccio E, Rochlin JM, Simon HK. Differences in lifetime earning potential for pediatric subspecialists. Pediatrics. 2021;148:e2021051194. doi: 10.1542/peds.2021-051194. [DOI] [PubMed] [Google Scholar]
- 4.Catenaccio E, Rochlin JM, Simon HK. Association of Lifetime Earning Potential and Workforce Distribution Among Pediatric Subspecialists. JAMA Pediatrics. 2021;175:1053–9. doi: 10.1001/jamapediatrics.2021.1912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Olsen S, Gautham K, Kilbride H, Artman M, Lakshminrusimha S Defining clinical effort for hospital-based pediatricians. J Pediatrics. 2021. 10.1016/j.jpeds.2021.11.063. [DOI] [PubMed]
- 6.Mercurio MR. Neonatology’s race to the bottom: RVUs, cFTEs, and physician time. J Perinatology. 2021;41:2561–3. doi: 10.1038/s41372-021-01192-6. [DOI] [PubMed] [Google Scholar]
- 7.Lakshminrusimha S, Murin S, Kirk JD, Mustafa Z, Maurice TR, Sousa N, et al. “Funds flow” implementation at academic health centers- unique challenges to pediatric departments. J Pediatr. 2022:S0022-3476(22)00089-0. 10.1016/j.jpeds.2022.01.058. Epub ahead of print. [DOI] [PubMed]
- 8.Kourembanas S, Steinhorn R. In-house neonatology: what are we waiting for? Am J Respiratory Crit care Med. 2010;182:728–9. doi: 10.1164/rccm.201006-0949ED. [DOI] [PubMed] [Google Scholar]
- 9.Judson TJ, Volpp KG, Detsky AS. Harnessing the right combination of extrinsic and intrinsic motivation to change physician behavior. JAMA. 2015;314:2233–4. doi: 10.1001/jama.2015.15015. [DOI] [PubMed] [Google Scholar]
- 10.Lubarsky DA, French MT, Gitlow HS, Rosen LF, Ullmann SG. Why money alone can’t (always) “Nudge” physicians: the role of behavioral economics in the design of physician incentives. Anesthesiology. 2019;130:154–70. doi: 10.1097/ALN.0000000000002373. [DOI] [PubMed] [Google Scholar]
- 11.Thaler RH Misbehaving: The Making of Behavioral Economics. W.W. Norton, 2016.
- 12.Thaler RH, Sunstein CR Nudge: Improving Decisions About Health, Wealth, and Happiness. Penguin Publishing Group, 2009.
- 13.Schulman J, Benitz WE, Profit J, Lee HC, Duenas G, Bennett MV, et al. Newborn antibiotic exposures and association with proven bloodstream infection. Pediatrics. 2019;144:e20191105. doi: 10.1542/peds.2019-1105. [DOI] [PubMed] [Google Scholar]
- 14.Underwood MA, Lakshminrusimha S, Steinhorn RH, Wedgwood S. Malnutrition, poor post-natal growth, intestinal dysbiosis and the developing lung. J Perinatology. 2021;41:1797–810. doi: 10.1038/s41372-020-00858-x. [DOI] [PubMed] [Google Scholar]
- 15.Lianov L. A powerful antidote to physician burnout: intensive healthy lifestyle and positive psychology approaches. Am J Lifestyle Med. 2021;15:563–6. doi: 10.1177/15598276211006626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Boothman R, Hickson GB. Time to rethink physician leadership training? Physician Leadersh J. 2021;8:41–6. [Google Scholar]
- 17.Lagasse J Key to top-tier reputation, financial performance lies in workforce engagement, Press Ganey research shows. 2017 [cited 2022 January 9] Available from: https://www.healthcarefinancenews.com/news/key-top-tier-reputation-financial-performance-lies-workforce-engagement-press-ganey-research.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from compensation and productivity benchmarking organizations such as Association of Administrators in Academic Pediatrics (AAAP) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of AAAP.