

Abstract
Objective
The aim of this study was to evaluate the external apical root resorption (EARR) developed in the maxillary and mandibular teeth of patients undergoing orthodontic treatment with conventional and self-ligating bracket systems.
Methods
Cone-beam computed tomography images of patients treated with self-ligating and conventional bracket systems, which were taken at the beginning and end of treatment, were evaluated. The teeth where EARR developed during the treatment period were identified. EARR was evaluated as yes or no. A P value of < .05 was considered statistically significant.
Results
Of a total of 300 patients (68.7% female, 31.3% male), 20% were treated with the self-ligating bracket system, while 80% were treated with the conventional bracket system. EARR occurred in 8.3% (n = 25) of the patients after treatment. A statistically significant difference was found when the effect of age, gender, and treatment duration on the incidence of EARR was evaluated. The incidence of EARR was higher in the age group of 18-30 years than in the age group of 12-17 years. Similarly, it was found to be higher in men than in women and higher in the group with a treatment duration of 33-49 months than in the group with a treatment duration of 8-32 months.
Conclusion
Treatment duration has been observed to affect the incidence of EARR in patients undergoing fixed orthodontic treatment, and the incidence of EARR increases with increased treatment duration. Furthermore, it has been concluded that EARR during orthodontic treatment is influenced by age and gender. There is no difference between self-ligating and conventional bracket systems in terms of EARR.
Keywords: Orthodontics, bracket systems, external apical root resorption
Introduction
External apical root resorption (EARR) is one of the most common complications seen during the orthodontic treatment.1 It is manifested as the loss of substance in the root apex in permanent teeth and shortening of the root apex.2 A sterile necrotic area is formed when the intensity of the orthodontic force required for the correction of malocclusions during orthodontic treatment is above the capillary blood pressure within the periodontal ligament. Destructive cells, macrophages, and multinucleated cells migrate to this area in response to signals released from necrotic tissues, causing a local inflammatory response. This inflammation is reported to be the main factor in the development of EARR.3,4 In the literature, there are many studies evaluating the relationship between EARR and orthodontic treatment. These studies report that there are many factors associated with EARR, including age, gender, nutrition, treatment with and without tooth extraction, treatment duration, amount of tooth movement, and genetic factors.5,6 Furthermore, the mechanics used during orthodontic treatment and the type of forces applied have been found to be associated with EARR.5 In conclusion, the etiology of EARR is complex and multifactorial. Therefore, it has been reported that patients at risk of developing EARR should be recognized early and patients should be offered radiographic controls 6 months after the initiation of orthodontic treatment.7
The incidence of EARR, the identification of patients who are more likely to develop EARR, its predictability, and preventability are still being studied.8 Although EARR rarely reaches dimensions that may affect the functions of a tooth, EARR developed during orthodontic treatment negatively affects the opinion of orthodontists and patients about treatment success.8 Currently, studies on this subject have regained intensity with the contribution of genetic science and the development of new imaging techniques.8 Although there have been many studies on EARR, its risk factors are still discussed in many studies.7 There are no comprehensive research studies on the effects of genetic structure on root resorption. However, the current studies agree on the important role of genetics, although no information has been provided about which genes are active. Adult patients have been reported to be in the high-risk group for the orthodontic treatment-induced EARR.7 Predictability, prevention, and early diagnosis of EARR are of great importance for the course of orthodontic treatment and the patient's dental health. Therefore, it is important to determine the severity and prevalence of EARR in various populations and its associated risk factors.9
Research studies aimed at improving the effectiveness of orthodontic treatment have focused on new bracket designs. One of them is the self-ligating bracket—the Damon system in particular—which has become popular in recent years.10 The Damon system (Ormco, Glendora, CA) is based on the use of a passive self-ligating brackets and super-elastic nickel-titanium wires.11 This system, which particularly has low friction forces, has been promoted to apply only light forces to move the teeth.12 In the initial leveling and alignment phase, the amount of EARR in this system is similar to that in the conventional bracket systems.4 Studies in the literature have shown that the bracket system or technique used for orthodontic treatment may be related to the EARR severity.9 On the other hand, lighter forces have been shown to often lead to less resorption.10 There are a limited number of studies investigating EARR after orthodontic treatment with the Damon system.11 Although the effectiveness of orthodontic treatment with self-ligating and conventional bracket systems has been extensively studied in the literature, the number of studies on EARR during orthodontic treatment is limited.5,7,9 Therefore, the aim of this retrospective study was to compare EARR developed in maxillary and mandibular teeth in patients treated with self-ligating and conventional brackets.
Methods
The study population consisted of a total of 300 patients aged 12-30 who were admitted to the Orthodontic Clinic between 2014 and 2016. The sample size was calculated based on an alpha significance level of 0.05 to achieve 80% of power (0.1 sampling error (d), P = .8, q = 0.2) to detect the frequency of EARR with G*Power software Version 3.0.10. The sample size calculation showed that 60 patients were needed in a group. Patients undergoing fixed orthodontic treatment without tooth extraction, in which the Damon system and Roth 3M bracket system were used, were included in the study. After the study was planned, the Clinical Research Ethics Committee approval was obtained (Decision Number: 2020/02-20). Written informed consent was obtained from the patients who participated in this study. The study was conducted in accordance with the ethical principles of the Helsinki Declaration. Cone-beam computed tomography (CBCT), KaVo 3D eXam (Biberach, Germany) images were obtained with a 4-second exposure time and a 0.3 mm-voxel size using a FOV of 130 at 120 kV and 5 mA. The EARR was evaluated by examining the CBCT images obtained at the beginning and end of treatment in patients treated with passive self-ligating/0.022-inch slot bracket (Damon Q, Ormco, Glendora, CA) and conventional bracket systems/0.022 inch slot (Roth, 3M Unitec, Gemini, Monrovia, Calif). Pre- and post-treatment changes in tooth sizes were evaluated according to Levander and Malmgren index .8 0 = no root resorption; 1= irregular root resorption; 2 = apical root resorption less than 2 mm (minor resorption); 3 = apical root resorption from 2 mm to one-third of the original root length (severe resorption); 4 = apical root resorption exceeding one-third of original root length (excessive resorption) (Figure 1). All evaluations were made by the same researcher (E.Ö). Individuals with skeletal Class I malocclusion, no skeletal asymmetry, no severe deep bite and open bite, no incisor or molar intrusion, permanent dentition, mild or moderate crowding according to Little's irregularity index, and non-extraction treatment were included. Patients who had EARR prior to treatment, those who had previously received orthodontic treatment, individuals with dental anomalies such as agenesis, dental invagination, taurodontism, and dilatation, patients with missing orthodontic records or having low-quality radiographs, were excluded from the study. Non-extraction treatment with the passive self-ligating Damon Q system is characterized by beginning leveling and alignment with round 0.013 in or 0.014 in Nitinol, followed by round 0.016, 0.018 in Nitinol, rectangular 0.014 × 0.025, 0.016 × 0.025, 0.018 × 0.025, and 0.019 × 0.025 in Nitinol archwires. Roth brackets (3M Unitek Gemini) of 0.022-inch slot were used on all arches in the conventional bracket system. In the leveling and alignment stage, orthodontic mechanics involved a wire sequence characterized by an initial round 0.012 in or a 0.014 in Nitinol, followed by round 0.016, 0.018 in Nitinol, and rectangular 017 × 0.025, 0.019 × 0.025 in Nitinol archwires. After the leveling and alignment of the maxillary and mandibular dental arches were completed with Nitinol archwires, rectangular stainless steel archwires were used.
Figure 1.
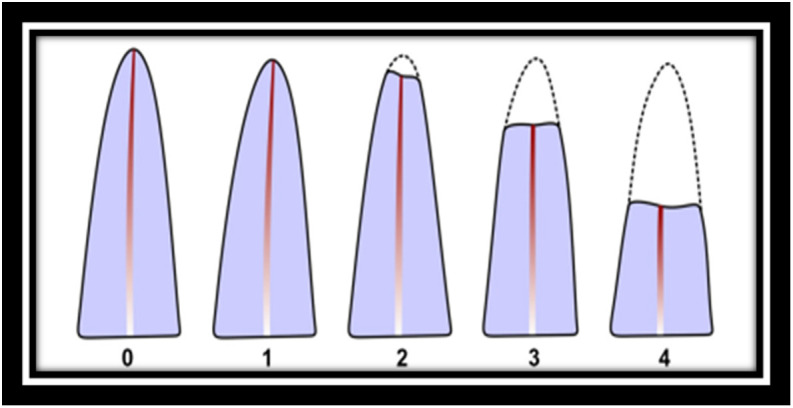
Levels of the external apical root resorption by Levander and Malmgren.8 Grade 0, absence of root resorption; Grade 1, mild resorption; Grade 2, moderate resorption; Grade 3, accentuated resorption; and Grade 4, extreme resorption.28
Statistical Analyses
Fifteen days after the initial evaluation, 50 of the CBCT images were randomly selected, and the EARR scores of the teeth were re-measured by another investigator to determine the inter-investigator error with the Kappa test. (SCC). Scores were calculated for each of the patients with EARR in the self-ligating and conventional bracket system groups. Scores 0 and 1 were considered as insignificant EARR (no) and scores 2, 3, and 4 were considered as EARR (yes) (Figure 2). Statistical analyses were performed using Number Cruncher Statistical System (NCSS) 2007 (Kaysville, Utah, USA). Descriptive statistical methods (mean, standard deviation, median, frequency, percentage, minimum, maximum) were used to evaluate the study data. The suitability of the quantitative data for normal distribution was examined using Shapiro–Wilk test and graphical analyses. Independent-samples t-test was used to compare the quantitative variables with normal distribution between the 2 groups. Qualitative data were compared using Pearson's chi-squared test and Fisher's exact test. A P value of .05 was considered statistically significant.
Figure 2.
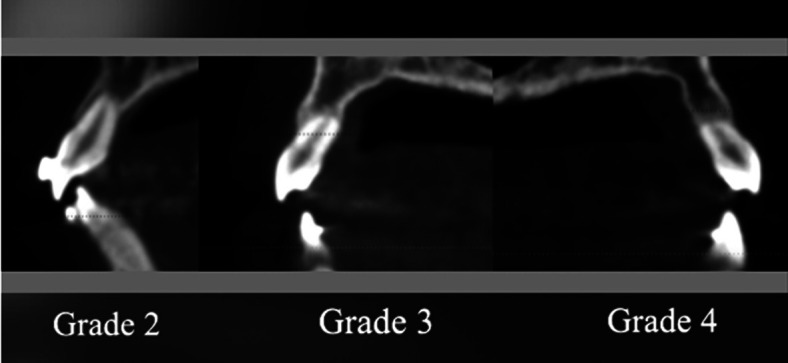
Grades 2, 3, and 4 showing external apical root resorption.
Results
There was a high agreement between the researchers confirming the reliability of the measurements. The Kappa coefficient between researchers was 0.86 for maxillary teeth and 0.82 for mandibular teeth. The study included a total of 300 patients (68.7% (n = 206) female; and 31.3% (n = 94) male). The age of the patients ranged from 12 to 30 years, with a mean age of 16.13 ± 4.08 years. Of the patients, 74% (n = 222) were in the 12-17 age group and 26% (n = 78) were in the 18-30 age group (Table 1, Figure 3).
Table 1.
Descriptive statistics of the study sample
| Variable | Categories | |
|---|---|---|
| Age (years) | Min–max | 12-30 |
| Mean ± SD | 16.13 ± 4.08 | |
| 12-17 years [n (%)] | 222 (74.0) | |
| 18-30 years [n (%)] | 78 (26.0) | |
| Gender | Female [n (%)] | 206 (68.7) |
| Male [n (%)] | 94 (31.3) | |
| EARR after treatment | No [n (%)] | 275 (91.7) |
| Yes [n (%)] | 25 (8.3) | |
| Number of EARR per patient (n = 25) | Min–max | 1-10 |
| Mean ± SD | 4.00 ± 2.06 | |
| Bracket system | Self-ligating system [n (%)] | 60 (20.0) |
| Conventional system [n (%)] | 240 (80.0) | |
| Duration of treatment (months) | Min–max | 8-49 |
| Mean ± SD | 31.99 ± 9.26 |
Min, minimum; Max, maximum; SD, standard deviation; n, number of patients
Figure 3.
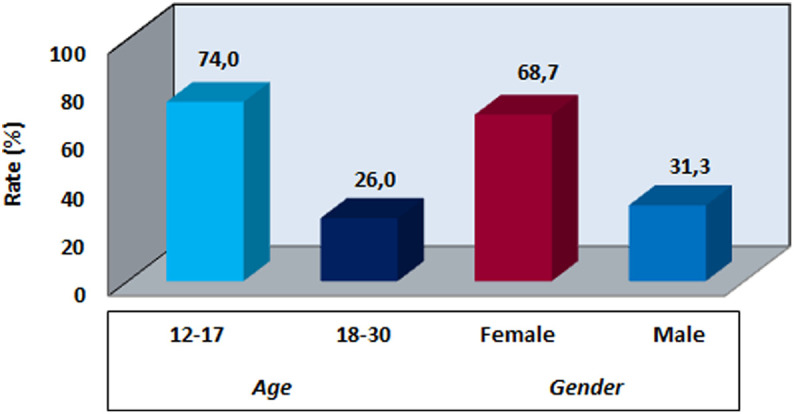
Age and gender distributions.
EARR occurred in 8.3% (n = 25) of the patients after treatment. Two of these 25 patients were in the self-ligating bracket system group, whereas 23 were in the conventional bracket system group—the total number of teeth with EARR was100 among 25 patients. The number of teeth with EARR ranged from 1 to 10 for each patient, with a mean number of 4.00 ± 2.06 (Table 1).
The treatments were classified according to the bracket systems used. Orthodontic treatment was performed using a self-ligating bracket system in 20% (n = 60) of the patients and a conventional bracket system in 80% (n = 240) (Figure 4). The mean treatment duration was 31.99 ± 9.26 months, ranging from 8 to 49 months (Table 1).
Figure 4. Distributions of.
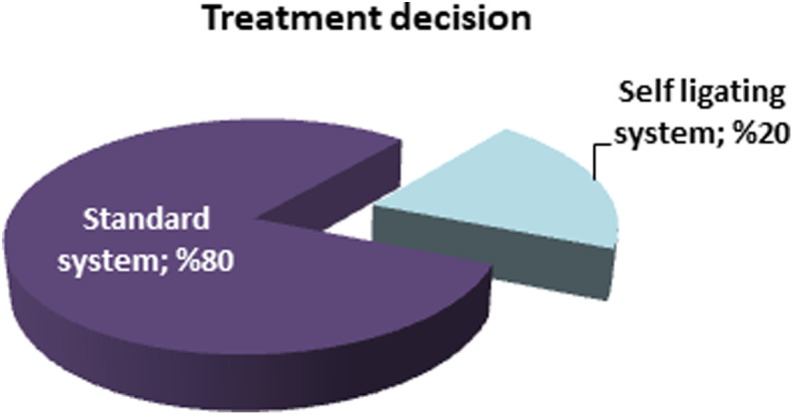
bracket system.
The difference between the age and gender distributions of the patients treated with self-ligating and conventional bracket systems were not statistically significant (P > .05) (Table 2).
Table 2.
Comparison of the bracket systems in terms of age and gender distribution, presence of EARR and treatment duration with Pearson Chi-Square test and Student's t-test
| Variable | Categories | Bracket System | P | |
|---|---|---|---|---|
| Self-ligating System (n=60) | Conventional System (n=240) | |||
| Age (years) | 12-17 [n (%)] | 48 (80.0) | 174 (72.5) | .236a |
| 18-30 [n (%)] | 12 (20.0) | 66 (27.5) | ||
| Gender | Female [n (%)] | 38 (63.3) | 168 (70.0) | .319a |
| Male [n (%)] | 22 (36.7) | 72 (30.0) | ||
| EARR after treatment | No [n (%)] | 58 (96.7) | 217 (90.4) | .117a |
| Yes [n (%)] | 2 (3.3) | 23 (9.6) | ||
| Duration of treatment (months) | Min–max | 14-48 | 8-49 | .775b |
| Mean ± SD | 31.68 ± 8.31 | 32.07 ± 9.50 | ||
aPearson chi-square test; bStudent’s t-test.
Min, minimum; Max, maximum; SD, standard deviation; n, number of patients.
There was not a statistically significant difference between the patients treated with self-ligating and conventional bracket systems in terms of post-treatment EARR (P > .05) (Table 2).
No statistically significant difference was observed between the patients treated with self-ligating and standard bracket systems in terms of orthodontic treatment duration (P > .05) (Table 2).
There was a statistically significant difference between the rates of post-treatment EARR according to age ( P < .01). The incidence of EARR in the 18-30 age group was found to be higher than in the 12-17 age group (Table 3).
Table 3.
Age evaluations
| Root Resorption After Treatment | Age Groups (years) | P a | |
|---|---|---|---|
| 12-17 (n=222), n (%) | 18-30 (n=78), n (%) | ||
| No | 210 (94.6) | 65 (83.3) | .002** |
| Yes | 12 (5.4) | 13 (16.7) | |
aPearson chi-square test; **P < .01.
There was a statistically significant difference between the rates of post-treatment EARR according to gender (P = .020; P < .05). The rate of EARR in male patients was found to be higher than in female patients (Table 4).
Table 4.
Gender evaluations
| Root Resorption After Treatment | Gender | P a | |
|---|---|---|---|
| Female (n=206), n (%) | Male (n=94), n (%) | ||
| No | 194 (94.2) | 81 (86.2) | .020* |
| Yes | 12 (5.8) | 13 (13.8) | |
aPearson chi-square test; *P < .05.
There was a statistically significant difference between the rates of post-treatment EARR according to treatment duration (P = .043; P < .05). The incidence of root resorption in patients receiving treatment for 33-49 months was found to be higher than in patients receiving treatment for 8-32 months (Table 5).
Table 5.
Evaluation of duration of treatment
| Root Resorption After Treatment | Duration of Treatment (Months) | Pa | |
|---|---|---|---|
| 8-32 months (n=154), n (%) | 33-49 months (n=146), n (%) | ||
| No | 146 (94.8) | 129 (88.4) | .043* |
| Yes | 8 (5.2) | 17 (11.6) | |
aPearson chi-square test; *P < .05.
Discussion
This study aimed to compare the rates of EARR in the maxillary and mandibular teeth of patients treated with Damon and Roth bracket systems. In patients who developed EARR during orthodontic treatment, EARR was observed not only in incisor teeth but also in premolar and molar teeth. Therefore, unlike other studies, the examination was performed on all maxillary and mandibular teeth in the present study.8 Post-treatment EARR occurred in 8.3% (n = 25) of the patients. There was a statistically significant difference between the patients treated with Damon and Roth bracket systems in terms of post-treatment EARR. A statistically significant difference was observed between the post-treatment EARR rates according to age; EARR incidence in the 18-30 age group was found to be higher than in the 12-17 age group. When the EARR incidence was evaluated according to gender, it was found to be higher in males than in females. There was a statistically significant difference between the post-treatment EARR rates according to treatment duration. The EARR rates in patients receiving treatment for 33-49 months were found to be higher than in the patients receiving treatment for 8-32 months.
In almost all studies on tooth movement, EARR, torque, and tipping are defined as the total horizontal movement of the root apex, considered the riskiest movement regarding EARR.12,13 In a study by Baumrind et al.,14 a 1 mm posterior movement of the root apex has been reported to cause EARR of 0.49 ± 0.14 mm. Regardless of the mechanics of treatment, intrusive forces are reported to increase the risk of EARR.15 The methods used in studies investigating the relationship between malocclusion type and EARR are quite different. Therefore, inconsistent and sometimes contradictory results are reported.12,16 Therefore, no malocclusion is considered to be immune to EARR. The common results are as follows: increased overjet and open bite closure are risk factors for maxillary incisors. Angle classification is not effective, and the effect of overbite is controversial.12-16 In this study, EARR was not evaluated according to orthodontic malocclusions. Therefore, we could not compare the present study with other studies.
Prolonged use of the edgewise bracket applying active torque has been reported to increase the risk of resorption.17 Sameshima and Sinclair18 have reported that the type or elastic use of the archwire is not correlated with the EARR. In a histologic study by Maltha et al.,19 the effects of forces of 10, 25, 50, 100, and 200 g on EARR were evaluated, and the amount of force was reported to have no effect on resorption. This conclusion is quite different from other studies. Darendeliler et al.20 studied the resorption craters in human premolar teeth subjected to heavy and light forces through a 3D evaluation and reported an increase in the volume of resorption craters as a result of heavy forces. There are a limited number of studies in which the mechanics used for treatment are evaluated for EARR. In one study, the standard edgewise, Roth straight-wire, and Begg techniques were compared for EARR and reported no difference between the 3 techniques in terms of root resorption.21 In this study, patients treated with Roth and Damon bracket systems were compared, and no difference was found in terms of EARR incidence.
Some studies have reported that the duration of force is a more critical factor than the magnitude of the force in the etiology of EARR, particularly in relation to long treatment duration.5 Therefore, it has been reported that patients at risk for EARR should be recognized early, and patients should be offered radiographic controls 6 months after the initiation of orthodontic treatment.5 In the literature, CBCT imaging has been accepted as the most reliable technique for the measurement of EARR.22 Therefore, CBCT guide orthodontists to continue or change the treatment plan as needed.22 In our study, CBCT images were used to evaluate EARR as it is the most accurate and reliable technique. No additional CBCT was taken for the study since the patients included in the study were selected from patients who had CBCT image recordings, and the patients were not further exposed to radiation for this retrospective study. In this study, EARR was evaluated on CBCT. Patients had the first CBCT for evaluation of impacted teeth before orthodontic treatment. They had a second CBCT after orthodontic treatment to evaluate the risk of complications due to impacted tooth extraction.
It is noteworthy that studies conducted over the last 2 decades evaluating the relationship between orthodontic treatment-induced EARR and gender have reported no correlation. On the other hand, Kjaer,22 who examined the morphological characteristics of the dentitions of patients with excessive EARR during orthodontic treatment, and Horiuchi et al.,16 who evaluated the effect of the relationship between tooth roots and cortical plaque on EARR, have concluded that the risk of EARR was higher in female patients. In contrast, Baumrind et al.,14 who examined the factors affecting EARR in adults and examined the relationship between endodontic treatment and EARR, have concluded that the risk was higher in male patients. Lee and Lee23 have reported that both treatment duration and patient's age have shown a statistically significant correlation with EARR in patients receiving orthodontic treatment and that there is no significant correlation between gender and EARR. In this study, it was concluded that the incidence of EARR varied according to gender and was higher in male patients.
Many studies have reported that prolonged orthodontic treatment is an important cause of EARR. In a study by Levander and Malmgren,8 resorption has been reported in 34% of the teeth after a 6-9 months, and this rate has been reported to increase to 56% after treatment of 19 months. In a study by Goldin,24 0.9 mm EARR has been reported to develop per year. Unlike these studies, there are also researchers who argue that large amounts of tooth movements occur in the first phase of treatment and that treatment duration is, therefore, not correlated with resorption. In the present study, it has been concluded that EARR increased with the increasing orthodontic treatment duration.
In the majority of studies on the type of force and EARR, intermittent or interrupted forces that provide a resting period for tissues have been reported to cause less EARR.25 Faster correction of orthodontic malocclusion has been reported to have the potential to cause undesirable side effects, such as root resorption, which is a great concern for orthodontists.26 Studies have shown that the bracket system or technique used for orthodontic treatment may be related to the EARR severity.3 There are also studies showing that lighter forces generally lead to less resorption.27 In recent years, there has been a significant increase in the use of self-ligating bracket systems by orthodontists. The Damon system is based on the use of a passive self-ligating bracket and super-elastic nickel-titanium wires.11 This system, which particularly has low friction forces, has been emphasized to apply only light forces to move the teeth.27 In the initial leveling and alignment phase, the amount of EARR in this system has been reported to be similar to that in the conventional bracket systems.27 In this study, patients treated with Roth and Damon bracket systems were compared, and no difference was found in terms of EARR incidence.
In their study, Leite et al.4 have compared the EARR in incisors in patients treated with self-ligating (EasyClip, SP, Brazil) and conventional (3M Unitec, Monrovia, Calif) brackets and found that EARR developed at significant rates in both groups 6 months after orthodontic treatment. In a study by Handem et al.27 involving patients aged between 16 and 19, who were treated with self-ligating (Damon Q) and conventional bracket systems, EARR has been evaluated with Levander and Malmgren scores through periapical radiographs of maxillary and mandibular incisors at the end of orthodontic treatment; the authors have reported no significant difference between the 2 groups in terms of EARR severity. In a study by Aras et al.,28 where Damon Q and conventional brackets (Titanium Orthos [TO]) used, it has been reported that there is no difference between the 2 bracket systems in terms of EARR. In the present study, no statistical difference has been found between the patients treated with Damon Q and conventional bracket systems in terms of EARR, compatible with the literature. Although there are many studies in the literature evaluating the effectiveness of orthodontic treatment with Damon and conventional brackets, the number of studies evaluating the effect of these systems on EARR during orthodontic treatment is limited. We believe that there is a need for further clinical trials.
Technological innovations have made it possible to evaluate the degree of EARR in 3D because of its accuracy in measuring EARR. It is recommended to use nickel-titanium archwires that apply less and optimum force instead of using stainless steel archwires that are thought to cause more resorption.29 Although some amount of EARR (0.25 mm) occurs in all teeth during leveling and alignment phases, this degree of EARR is considered small and clinically irrelevant.29 Self-ligating brackets provide faster tooth movement but are also suggested to pose a high risk for EARR. However, studies have reported that the degree of EARR is similar in orthodontic treatments with conventional or self-ligating bracket systems. In the present study, the effect of self-ligating and conventional bracket systems on the incidence of EARR after orthodontic treatment did not show any statistically significant difference. However, the amount of EARR was higher in the conventional bracket system compared to the self-ligating bracket system. The limitations of this study are that, since the number of patients who had CBCT taken at the beginning and end of treatment was limited, the number of patients could not be increased further and the standardization could not be fully achieved among patients due to the effect of many local and systemic factors on EARR. EARR should be evaluated at least by taking periapical radiographs from incisors, which are considered to be the most affected teeth, in the sixth month of orthodontic treatment; if there are any changes in the root form, treatment at the affected arch should be stopped for a while.
Conclusion
In this study, it was observed that the effect of bracket systems on external root resorption was similar. Age and gender were found to influence root resorption.
Funding Statement
The authors declared that this study has received no financial support
Footnotes
Ethics Committee Approval: This study was approved by Ethics committee of Van Yuzuncu Yil University, (Approval No:2020/02-20).
Informed Consent: Written informed consent was obtained from the patients who participated in this study.
Peer Review: Externally peer-reviewed.
Author Contributions: Supervision – S.Ç.C., E.Ö.; Design – S.Ç.C., E.Ö.; Concept – S.Ç.C., E.Ö.; Resources – S.Ç.C., E.Ö.; Materials – S.Ç.C., E.Ö.; Data Collection and/or Processing – S.Ç.C., E.Ö.; Analysis and/or Interpretation – S.Ç.C., E.Ö.; Literature Search – S.Ç.C., E.Ö.; Writing Manuscript – S.Ç.C., E.Ö.; Critical Review – S.Ç.C., E.Ö.
Conflict of Interest: The authors have no conflict of interest to declare.
References
- 1.McNab S, Battistutta D, Taverne A, Symons AL.External apical root resorption following orthodontic treatment. Angle Orthod. 2000;70(3):227–232.. 10.1043/0003-3219(2000)070<0227:EARRFO>2.0.CO;2) [DOI] [PubMed] [Google Scholar]
- 2.Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE.Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofacial Orthop. 2010;137(4):462–476.; discussion 12A. 10.1016/j.ajodo.2009.06.021) [DOI] [PubMed] [Google Scholar]
- 3.Alzahawi K, Færøvig E, Brudvik P, Bøe OE, Mavragani M.Root resorption after leveling with super-elastic and conventional steel arch wires: a prospective study. Prog Orthod. 2014;15:35. 10.1186/s40510-014-0035-z) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Leite V, Conti AC, Navarro R.Comparison of root resorption between self-ligating and conventional preadjusted brackets using cone beam computed tomography. Angle Orthod. 2012;82(6):1078–1082.. 10.2319/080911-501.1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jiang RP, McDonald JP, Fu MK.Root resorption before and after orthodontic treatment: a clinical study of contributory factors. Eur J Orthod. 2010;32(6):693–697.. 10.1093/ejo/cjp165) [DOI] [PubMed] [Google Scholar]
- 6.Al-Qawasmi RA, Hartsfield JK, Everett ET.Genetic predisposition to external apical root resorption. Am J Orthod Dentofacial Orthop. 2003;123(3):242–252.. 10.1067/mod.2003.42) [DOI] [PubMed] [Google Scholar]
- 7.Guo Y, He S, Gu T, Liu Y, Chen S.Genetic and clinical risk factors of root resorption associated with orthodontic treatment. Am J Orthod Dentofacial Orthop. 2016;150(2):283–289.. 10.1016/j.ajodo.2015.12.028) [DOI] [PubMed] [Google Scholar]
- 8.Levander E, Malmgren O.Long term follow up of maxillary incisors with severe apical resorption. Eur J Orthod. 2000;22(1):85–92.. 10.1093/ejo/22.1.85) [DOI] [PubMed] [Google Scholar]
- 9.Agarwal SS, Chopra SS, Kumar P.A radiographic study of external apical root resorption in patients treated with single-phase fixed orthodontic therapy. Med J Armed Forces India. 2016;72:S8–S16.. 10.1016/j.mjafi.2016.04.005) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen SS, Greenlee GM, Kim JE, Smith CL, Huang GJ.Systematic review of self-ligating brackets. Am J Orthod Dentofacial Orthop. 2010;137(6):726.e1–726.e18; discussion 726.. 10.1016/j.ajodo.2009.11.009) [DOI] [PubMed] [Google Scholar]
- 11.DiBiase AT, Nasr IH, Scott P, Cobourne MT.Duration of treatment and occlusal outcome using Damon3 self-ligated and conventional orthodontic bracket systems in extraction patients: a prospective randomized clinical trial. Am J Orthod Dentofacial Orthop. 2011;139(2):e111–e116.. 10.1016/j.ajodo.2010.07.020) [DOI] [PubMed] [Google Scholar]
- 12.Sameshima GT, Sinclair PM.Characteristics of patients with severe root resorption. Orthod Craniofac Res. 2004;7(2):108–114.. 10.1111/j.1601-6343.2004.00284.x) [DOI] [PubMed] [Google Scholar]
- 13.Brin I, Tulloch JFC, Koroluk L, Philips C.External apical root resorption in Class II malocclusion: a retrospective review of 1 versus 2 phase treatment. Am J Orthod Dentofacial Orthop. 2003;124(2):151–156.. 10.1016/s0889-5406(03)00166-5) [DOI] [PubMed] [Google Scholar]
- 14.Baumrind S, Korn EL, Boyd RL.Apical root resorption in orthodontically treated adults. Am J Orthod Dentofacial Orthop. 1996;110(3):311–320.. 10.1016/s0889-5406(96)80016-3) [DOI] [PubMed] [Google Scholar]
- 15.Otis LL, Hong JS, Tuncay OC.Bone structure effect on resorption. Orthod Craniofac Res. 2004;7(3):165–177.. 10.1111/j.1601-6343.2004.00282.x) [DOI] [PubMed] [Google Scholar]
- 16.Horiuchi A, Hotokezaka H, Kobayashi K.Correlation between cortical plate proximity and apical root resorption. Am J Orthod Dentofacial Orthop. 1998;114(3):311–318.. 10.1016/s0889-5406(98)70214-8) [DOI] [PubMed] [Google Scholar]
- 17.Linge L, Linge BO.Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofac Orthop. 1991;93:35–43.. 10.1016/S0889-5406(05)81678-6) [DOI] [PubMed] [Google Scholar]
- 18.Sameshima GT, Sinclair PM.Predicting an preventing root resorption: Part II. Am J Orthod Dentofac Orthop. 2001;119:511–515.. 10.1067/mod.2001.113410) [DOI] [PubMed] [Google Scholar]
- 19.Maltha JC, van Leeuwen EJ, Dijkman GE, Kuijpers-Jagtman AM.Incidence and severity of root resorption in orthodontically moved premolars in dogs. Orthod Craniofac Res. 2004;7(2):115–121.. 10.1111/j.1601-6343.2004.00283.x) [DOI] [PubMed] [Google Scholar]
- 20.Darendeliler MA, Kharbanda OP, Chan EK.Root resorption and its association with physical properties of, mineral contents and resorption craters in human premolars following application of light and heavy forces. Orthod Craniofac Res. 2004;7(2):79–97.. 10.1111/j.1601-6343.2004.00281.x) [DOI] [PubMed] [Google Scholar]
- 21.Parker RJ, Harris EF.Directions of orthodontic tooth movements associated with external apical root resorption of the maxillary central incisors. Am J Orthod Dentofacial Orthop. 1998;114(6):677–683.. 10.1016/s0889-5406(98)70200-8) [DOI] [PubMed] [Google Scholar]
- 22.Kjaer I.Morphological characteristics of dentitions developing excessive root resorption during orthodontic treatment. Eur J Orthod. 1995;17(1):25–34.. 10.1093/ejo/17.1.25) [DOI] [PubMed] [Google Scholar]
- 23.Lee YJ, Lee TY.External root resorption during orthodontic treatment in root-filled teeth and contralateral teeth with vital pulp: a clinical study of contributing factors. Am J Orthod Dentofacial Orthop. 2016;149(1):84–91.. 10.1016/j.ajodo.2015.06.027) [DOI] [PubMed] [Google Scholar]
- 24.Goldin B.Labial root torque: effect of the maxilla and incisor root apex. Am J Orthod Dentofacial Orthop. 1989;95(3):208–219.. 10.1016/0889-5406(89)90051-6) [DOI] [PubMed] [Google Scholar]
- 25.Beck BW, Harris EF.Apical root resorption in orthodontically treated subjects: analysis of edgewise and light wire techniques. Am J Orthod Dentofac Orthop. 1994;105:350–361.. 10.1016/S0889-5406(94)70129-6) [DOI] [PubMed] [Google Scholar]
- 26.Sherrard JF, Rossouw PE, Benson BW, Carrillo R, Buschang PH.Accuracy and reliability of tooth and root lengths measured on cone-beam computed tomographs. Am J Orthod Dentofacial Orthop. 2010;137(4)(Suppl):S100–S108.. 10.1016/j.ajodo.2009.03.040) [DOI] [PubMed] [Google Scholar]
- 27.Handem RH, Janson G, Matias M.External root resorption with the selfligating Damon system—a retrospective study. Prog Orthod. 2016;17(1):20. 10.1186/s40510-016-0133-1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Aras I, Unal I, Huniler G, Aras A.Root resorption due to orthodontic treatment using self-ligating and conventional brackets: a cone-beam computed tomography study. J Orofac Orthop. 2018;79(3):181–190.. 10.1007/s00056-018-0133-5) [DOI] [PubMed] [Google Scholar]
- 29.Makedonas D, Lund H, Gröndahl K, Hansen K.Rootresorption diagnosed with cone beam computed tomography after 6 months of orthodontic treatment with fixed appliance and the relation to risk factors. Angle Orthod. 2011;139:e73–e81.. 10.2319/112810-691.1) [DOI] [PMC free article] [PubMed] [Google Scholar]