

Abstract
The goal of this manuscript is to advance HIV risk behavior prevention efforts for South African adolescent girls by identifying distinct trajectory patterns across multiple behavioral domains for adolescent and young adults. We draw from a sample of N=1070 adolescent girls from South Africa who were between the ages of 13–15 at baseline. Participants were followed across 6 waves of data collection between 2011–2019. We focus on predicting trajectories between ages 15 and 21. All participants were HIV negative and had not experienced sexual debut at baseline. We examine group-based multi-variable trajectories across several known HIV risk behaviors: earlier age of sexual debut, engaging in unprotected sex, engaging in transactional sex, earlier age at first pregnancy, and exposure to physical IPV. After characterizing three prototypical joint trajectories (abstainers (54%), early unprotected sex (36%), and high-risk sexually active (11%), we predicted membership based on the following baseline risk and protective factors: household expenditures, bonding to school, parental monitoring, number of close friends, and community engagement. We found that school bonding and parental monitoring were the strongest predictor of sexual risk, and that, among those in both the early unprotected sex and high-risk groups, risky behaviors like unprotected and transactional sex most frequently occurred early in adolescence. These findings suggest that interventions should target girls early in adolescence, and that interventions focused at improving school bonding and promoting parental involvement may be most effective at preventing risky sexual behavior.
Keywords: HIV, adolescent girl, South Africa, trajectories, prevention, sexual risk
Introduction
Adolescent girls and young women (AGYW) in sub-Saharan Africa (SSA) remain at the epicenter of the HIV epidemic, accounting for over 25% of new HIV infections in the region.[1] In South Africa, AGYW contribute more than four times the number of new HIV infections compared to adolescent boys and young men and are infected at earlier ages than their male counterparts.[2, 3, 4] Understanding how patterns of HIV-related sexual behaviors develop from early adolescence, as well as the factors predicting these patterns, is critical for the development of future HIV prevention interventions for this population.
Early adolescence is a critical period in the life course where young people experience puberty, begin to have sex, and first engage in intimate partnerships. Global data indicate that the age of puberty (often occurring between 12 and 16 years) has declined over the last 30 years, widening the period during which young girls are exposed to sexual risks.[5] Early sexual debut in SSA has been associated with increased risk of HIV and STIs due to unprotected sex and increased risk of maternal mortality and school dropout due to unintended childbearing.[6, 5, 7, 8] Early intimate partnerships have been associated with increased risk of experiencing violence among girls due to limited relational power and prevalent gender norms in SSA.[9, 10, 11] In light of these risks, the public health community has indicated that early adolescence is a unique and important window of opportunity for primary prevention and has called for research, programming, and policy for this age group.[12, 13] Despite this call, there have been limited longitudinal studies of HIV-sexual behavior trajectories starting in early adolescence in SSA, particularly those that use a person-centered approach.[14, 15, 16, 17, 18, 19]
Previous studies examining HIV-related sexual behaviors among AGYW in SSA have been largely regression based (variable centered), rather than person-centered. [20] Regression based analyses aim to identify the unique effects of a particular factor over and above other factors. Given that HIV-related sexual behaviors do not exist in isolation, these types of analyses have limited utility for public health practitioners who want to identify vulnerable subgroups who demonstrate distinct patterns or profiles of involvement across multiple types of behavior and appropriately tailor interventions to address these patterns. Person-centered analyses that evaluate how correlated sexual behaviors develop together and interact over time might help in the early identification of AGYW who might be at highest risk of HIV acquisition.[21]
Experiences in early adolescence shape sexual behavioral trajectories and the broader literature on adolescent development has long emphasized the importance of connections to family, peer, school, and community contexts.[22, 23, 24] Social contexts can model and reinforce norms, provide support, connect intimate partners, shape beliefs, and motivate education and economic aspirations. Social control theory further posits that individuals with weak bonds to prosocial contexts are more vulnerable to engaging in or being exposed to risky sexual situations.[25, 23] In support of this hypothesis, research among AGYW in South Africa has documented the association between HIV-related sexual behaviors and weak attachment to parents, interactions with older peers, low school attendance, and limited engagement with church and other conventional community groups.[26, 27, 28, 29] However, the strength of connection to these social contexts varies which in turn might lead to heterogeneity amongst individuals with respect to engagement in HIV-related sexual behaviors.16 Combining a social control theory perspective with a life course perspective also suggests that the impact of connections to social contexts may vary in importance across adolescence.[30, 31, 32] For example, parental influences may be important early on, whereas peers and dating partners are more influential in later adolescence. Identifying groups of AGYW who share similar trajectories of HIV-related sexual behaviors and understanding how they are shaped by potentially modifiable experiences in early adolescence is critical for the development of future HIV prevention interventions.
This manuscript utilizes a person-centered approach and six waves of longitudinal data from a study of AGYW in rural South Africa (ages 13–21) to examine two specific research aims. First, we examine group-based multi-variable trajectories across HIV-related sexual behaviors. Second, we examine how bonding to social contexts predicts group membership
Methods
Sample
Data are from the HIV Prevention Trials Network 068 study (HPTN 068), a phase III randomized controlled trial which aimed to measure the effect of providing cash transfers, conditional on school attendance, on risk of HIV acquisition among AGYW. The study enrolled 2,533 adolescent girls and young women aged 13 to 20 years who were attending high school grades 8 to 11 in the Bushbuckridge sub-district in Mpumalanga province, South Africa. The current analysis focused on trajectories of n=1070 participants who were HIV negative, not yet sexually active, and between 13–15 years old at their baseline study visit. The study area is characterized by high levels of unemployment, poverty, migration for work, and HIV prevalence.[33] Individuals who were pregnant or married at the time of recruitment, unable to read, intending to leave to leave the study area before study completion, or without a parent or guardian in the house were ineligible to participate in the study.
Enrolled AGYW were seen annually from baseline until one-year post study completion or graduation from high school, resulting in up to six assessments for each participant between 2011 and 2019. Each annual study visit included an Audio Computer-Assisted Self-Interview (ACASI) with the young woman. Additional details on recruitment and data collection are available in the parent publication of the trial.[34].
Institutional Review Board approval for this study was obtained from the University of North Carolina at Chapel Hill and the University of the Witwatersrand Human Research Ethics Committee. Each AGYW and her parent or guardian provided written informed consent at the home visit. Written assent was obtained for young women younger than 18 years. Consent and assent forms were available in English and Shangaan.
Data Structure and Coding Time
Data were structured so that age, not visit wave, was the unit of time for analyses. Trajectory analyses focused on repeated measures data spanning ages 15–21. Baseline predictors (collected in wave 1) occurred when participants were between ages 13–15.
Missing Data
Attrition Analysis
We conducted a chi-square test of independence (for categorical variables) and t-tests (for continuous variables) to determine whether participants who stayed in the study until age 21 differed significantly from participants who dropped out prior to age 21 on any of the baseline risk and protection factors or treatment arm. There were no significant differences between participants who provided data for the last time point and those who did not on the following variables: treatment arm, repeating a grade, school bonding, parental warmth and monitoring, number of close friends, or food insecurity. The groups differed with respect to mean household expenditures such that expenditures were slightly higher among the group that attritted prior to age 21.
Handling Missing Data
Missing repeated measures data were handled using full information maximum likelihood estimation (FIML). FIML requires the assumption of conditional ignorability, meaning that, in the context of a trajectory model, inclusion of observed repeated measures is sufficient to induce ignorability on the missing data process.
Variables and Measures
Social bonds measured at baseline.
Parental monitoring was self-reported and measured by the mean of four items: How often does [primary caregiver] try to find out: “about where you go after school?”, “about how you spend your money?”, “who your friends are?”, and “about how you spend your free time?” with the following response categories: 1=”never,” 2=”sometimes,” and 3=”always” (M=2.28; SD=.58; range=1–3). School bonding was self-reported and measured as the mean of four items: During your last full year in school: “did you feel close to people at your school?”, “did you feel like you were part of you school?”, “were you happy to be at your school?”, “did you feel that the teachers at your school treat students fairly?” Responses were dichotomized to represent either a ”yes” answer to all items (79%) or a ”no” to at least one school bonding item (21%) due to strong left skew. [35] Number of close friends was self-reported and measured as a continuous variable. Community group involvement was self-reported and measured as a count (out of seven) of whether participants belonged to any of the following community groups: church, health, HIV/AIDS, dance, sport, and finance/loan (M=2.10, SD=1.26, range=0–7).
Proximal adolescent time-to-event outcomes.
Age of sexual debut and age of first pregnancy were calculated using self-report data.
Proximal adolescent time-varying outcomes.
Physical Intimate partner violence (IPV) was self-reported and measured using a 6-item WHO scale.[36] A binary variable was created to represent any or no experiences of physical IPV in the past 12 months. Unprotected sex in the past three months was self-reported, measured as a binary variable, and defined at each visit as having reported any instance of condomless sex in the past three months with any of up to three reported partners. Transactional sex was self-reported and coded as a binary variable, and defined as reporting exchange of sex with any of up to three reported partners in the past three months because they were given money or gifts.
Covariate.
As a proxy for household income status, we estimated the log of monthly household expenditures, which were measured in Rand currency (M=2.28; SD=.58; range=1–3).
Data Analysis
We used Mplus version 8.6 for trajectory and time-to-event modeling and R for data management and other analyses. For both time-to-event and time-varying outcomes, we first visualized raw data by age (14–21). We then conducted univariate survival models and latent curve models to establish the correct time parameterization for each outcome before combining outcomes in a mixture model.
Finite mixture models.
Time-to-event outcomes were modeled using the parametric multiple event process survival mixture (MEPSUM) model laid out by Dean and colleagues. [37, 38] In this approach, associations among hazard functions for multiple survival processes (p = 1…P) are accounted for by conditioning hazard functions on latent class membership with k = 1…K latent classes:
Here, i = 1…N represents individuals, t = 1…Tip is an indicator of discrete time, and htijk is the hazard function that defines the conditional probability of outcome occurring at a given time period given that it has not yet occurred.
Time-varying outcomes were modeled using semi-parametric growth models, generalized to include multiple processes (called a group-based multi-trajectory model; GBMTM[39]):
where Λkj is an outcome- and class-specific matrix of time-structured factor loadings typical of a latent curve model and αkj represents outcome- and class-specific growth factor means. Survival outcomes (modeled with MEPSUM) and time-varying outcomes (modeled with GBMTM) were modeled simultaneously so the same latent classes underlie the survival and time-varying outcomes.
To aid convergence, we constrained growth factor variances and covariances, including those used for survival models, to be zero. We also constrained intercept means to zero for all processes except physical IPV exposure since, given our restriction of the sample to girls who were not sexually active at baseline, there was no variation in sexual outcomes at baseline. We used robust maximum likelihood estimation with 2000 random start values to avoid local maxima, a common problem for these complex models. ([40])
We relied on standard indices for class enumeration: the sample size-adjusted BIC, the bootstrapped likelihood ratio test (bLRT), and the Lo-Mendel-Rubin likelihood ratio test (LMR). We did not consider solutions with class proportions smaller than 5% because small classes can be unstable.
Predicting latent class membership.
Individuals were classified using modal class assignment. Modal group membership was then used as the outcome variable in a multinomial logistic regression analysis using household expenditures, parental monitoring, number of close friends, school bonding, and community engagement as predictors. This classify-analyze approach has been criticized as resulting in downwardly biased standard errors because uncertainty of class membership is not taken into account. Three-step approaches avoid introducing measurement error into the class membership that would be introduced if we were to use modal class assignment.[41] Unfortunately, this approach is not currently available in combination with our GBMTM. Because of the known increased risk for Type I errors due to unmodeled classification error, we used a more conservative alpha level of .01 for these analyses.
Results
Sample descriptive statistics for baseline risk and protective factors are displayed in Table 1.
Table 1:
Descriptive statistics.
| Median or % | IQR [25th–75th %] | Range | |
|---|---|---|---|
| Risk and Protective Factors at Baseline | |||
| School Bonding | 79% | ||
| Number of Close Friends (up to 3) | 2 | 1–3 | 0–3 |
| Community Involvement | 2 | 1–3 | 0–7 |
| Parental Monitoring | 2.25 | 2–3 | 1–3 |
| Log Household Expenditures | 5.84 | 5.30–6.28 | 2.86–9.72 |
Univariate Trajectories
A linear trend fit best for the univariate time-to-sexual debut and time-to-first pregnancy data. The univariate growth trajectory for engaging in transactional sex was also linear. The univariate growth trajectories for unprotected sexual activity and exposure to physical IPV both followed a quadratic trend. These trends match the observed means, which are presented in Figure 1. When viewing descriptive statistics for sexual activity, it is important to note that the sample was selected to include only participants who were not sexually active at the first wave, when they were between 13–15 years old.
Figure 1:
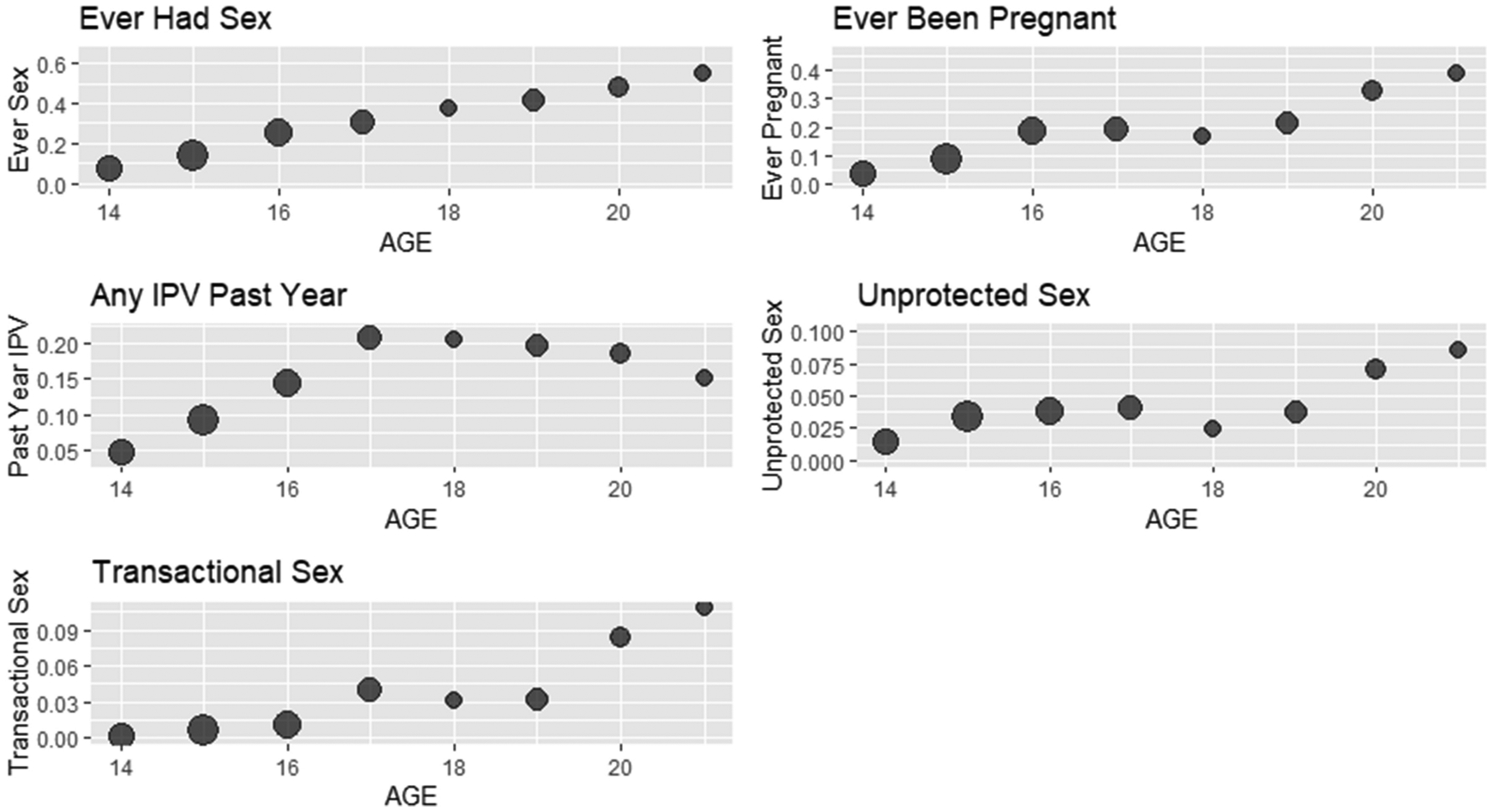
Mean values (observed) of repeated measures by age (14–21). Circle area is proportional to sample size contributing to mean at each age. Y-axis is percent endorsement.
Class Enumeration
We tested 3-, 4-, and 5-class solutions. Fit indices are shown in Table 2. Although the n-adjusted BIC, LMR, and bLRT indices suggested improvement in model fit with additional latent classes, the smallest class size contained fewer than 5% of participants in both the 4- and 5-class models and there were extreme parameter estimates in the 4- and 5-class solutions, suggesting that these results were unstable. We therefore move forward with the 3-class solution.
Table 2:
Latent class enumeration.
| Classes | n-adjusted BIC | LMR | bLRT | Smallest Class p | Entropy |
|---|---|---|---|---|---|
| 3 | 11496 | p < .001. | p < .001 | .11 | .77 |
| 4 | 11423 | p < .001. | p < .001. | .05 | .79 |
| 5 | 11281 | p < .001. | p < .001. | .03 | .78 |
See Figure 2 for model-implied cumulative hazards and time-varying probabilities for sexual risk-taking behaviors. The most prevalent latent class, the ”abstainers,” comprised 53.8% of the sample. The second most prevalent class, ”early unprotected sex,” comprised 35.6% of the sample. The least prevalent class, ”high sexual risk,” comprised 10.6% of the sample.
Figure 2:
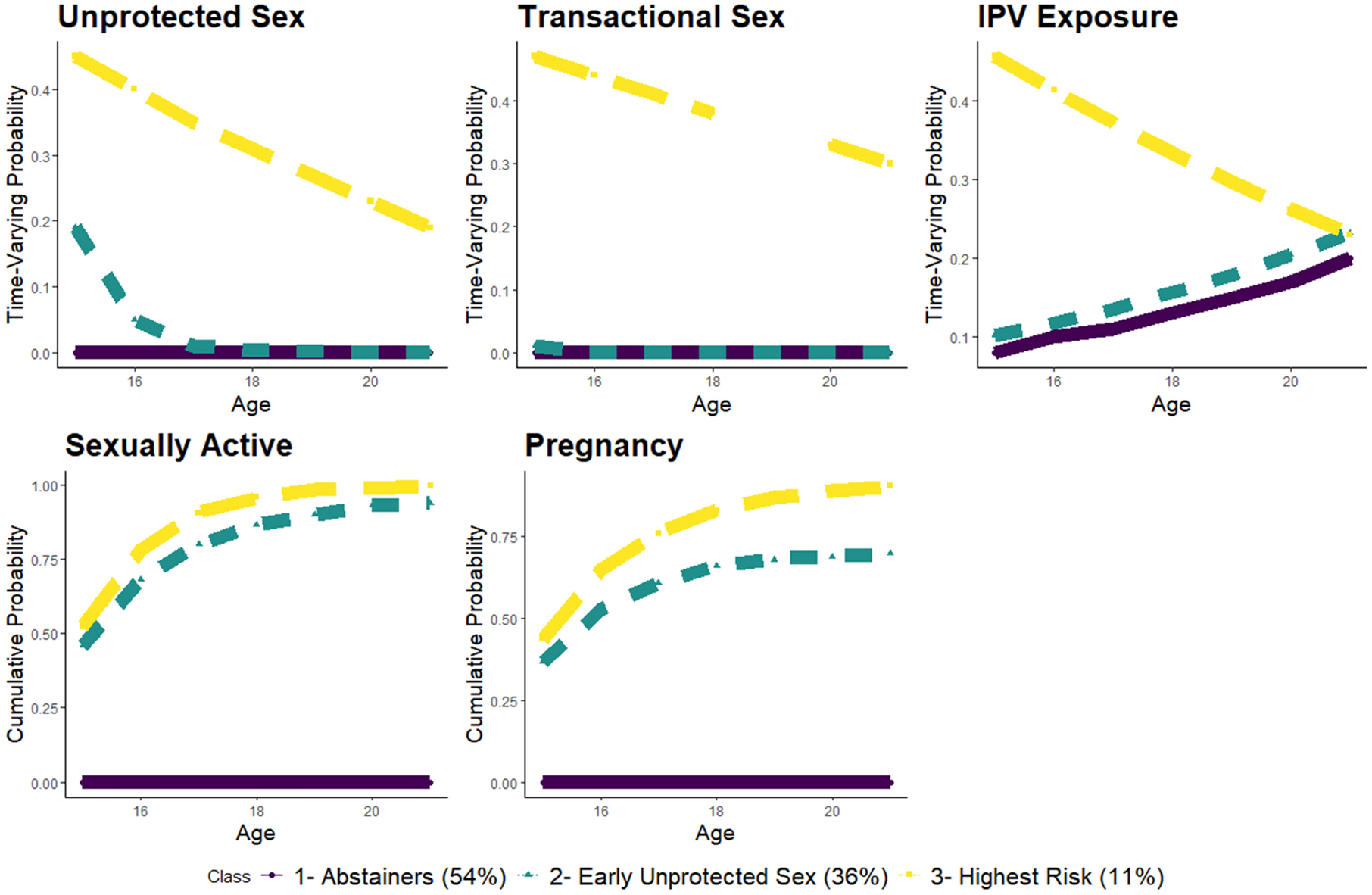
Model-implied cumulative hazards and time-varying probabilities for sexual risk-taking behaviors.
The abstainers reported no sexual activity by age 21. Risk for physical IPV in this group increased to 20% by age 21, but no other risk factors were present.
Approximately 50% of the adolescents in the early unprotected sex group were sexually active at age 15, increasing to approximately 90% by age 21. Half of this group had experienced pregnancy by age 16, increasing to approximately 2/3 of the group by age 21. In this group, the riskiest behaviors occurred early, with 20% of the group engaging in unprotected sex at age 15 but almost none engaging in unprotected sex by age 17. Members of the early unprotected sex group did not engage in transactional sex and physical IPV exposure patterns were similar to those observed in the abstainer class.
Among members of the highest risk group, over half were sexually active by age 15 and nearly all were sexually active by age 18. For this group, nearly all sexual activity that occurred during early adolescence was unprotected and transactional. Physical IPV exposure was highest at age 15 for the highest risk group, with approximately half of the group members reporting experiencing physical IPV at age 15. Although unprotected sex, transactional sex, and IPV exposure decreased over time for the highest risk class, risk remained higher than the abstainer and early unprotected sex classes throughout adolescence. Furthermore, half of the girls in the highest risk class experienced pregnancy by age 15 and nearly all had experienced pregnancy by age 21.
Predicting Class Membership
Results from multinomial logistic regression models are reported in Table 3. Girls in the highest risk class reported lower parental monitoring at baseline than girls in both the abstainer and early unprotected sex categories (aOR=.49 and .58, respectively), but the abstainer and early unprotected sex classes did not differ on parental monitoring. Compared with abstainers, girls in the early unprotected sex and higher-risk classes reported lower levels of school bonding (aOR=.76 and .63, respectively); these groups did not differ from one another on school bonding. Compared to abstainers, girls in the higher risk category had lower household expenditures (aOR=.31 and .72 for early unprotected sex and high-risk class membership, respectively). However, the abstainer and high-risk class comparison did not reach the nominal significance level of α = .01. Number of close friends and community engagement did not distinguish between risk categories.
Table 3:
Baseline predictor effects on the relative odds of membership in a riskier class
| Predictor | Abstainers vs. Early Unprotected | Abstainers vs. High-Risk | Early Unprotected vs. High-Risk |
|---|---|---|---|
| Household Expenditures | .31** (.26,.37) | .72 (.53,.97) | .85 (.62,1.17) |
| Parental Monitoring | .85 (.66,1.11) | .49** (.34,.72) | .58* (.39,.86) |
| School Bonding | .76 (.59,.99)* | .63** (.44,.88) | .82 (.57,1.17) |
| Close Friends | 1.03 (.93,1.14) | .92 (.79,1.08) | .90 (.75,1.07) |
| Community Engagement | .93 (.84,1.03) | .97 (.81,1.16) | 1.05 (.94,1.16) |
Note. Cells contain aORs with 95% confidence intervals. The lower risk category is the reference group.
p < .01;
p < .001
Discussion
To our knowledge, this study is among the first to use a person-centered approach to identify longitudinal patterns of co-occurring HIV-related sexual behaviors starting in early adolescence for girls in SSA. We found three distinct classes: abstainers, early unprotected sex, and high risk. Participants in the latter two classes were at an increased risk of early sexual debut and engaged in sexual behaviors in early adolescence which could result in consequences such as pregnancy and HIV infection. For example, nearly all participants in the high-risk group were pregnant before age 20 and over half were pregnant by age 16. We also found that those in the high-risk group, in comparison to the abstainers, were less likely to be monitored by their parents and to be connected to school settings in early adolescence. Taken together, the shape of the trajectories and our results related to social context predictors reveal the urgency of intervening in early adolescence to prevent the life-altering consequences of early sexual risk-taking behaviors.
Analyses of baseline social context predictors suggest that a focus on social bonds in school and at home may be key to delaying sexual debut and other concomitant sexual behaviors. Our results align with expectations based on social control theory and life course theory perspectives: young girls who are connected to prosocial contexts in early adolescence are less likely to engage in deviant behaviors that have consequences for their transition to adulthood and later life.[25, 23, 30] While our results related to school context align with previous research among young girls in SSA, our results related to parental monitoring do not.[42, 43, 44, 45, 46, 47, 48] Studies in Burkina Faso, Ghana, Malawi, Uganda, Tanzania, Cameroon, Ethiopia, and Kenya have not found parental monitoring to be protective for sexual debut or condom use among young girls.[44, 45, 46, 47, 48] Given that this association has been found to be consistent and strong in the United States and other high-income countries, researchers have hypothesized that the effect of parental monitoring may depend on sociocultural norms of the geographic context.[44, 49, 50, 51] Studies have also found a strong association between family structure and adolescent sexual behaviors in SSA. Adolescents living in two parent homes, as well as homes with a biological father, had later sexual debut and were less likely to engage in unprotected sex or experience sexual violence.[52, 53, 54] Existing parental monitoring studies in SSA have included participants who are age 12–19 and the adolescent development literature suggests that the influence of parents decreases as individuals move towards adulthood.[44, 45, 46, 47, 48, 55, 56] Thus, our results might also differ because we specifically focused on individuals and parental monitoring in early adolescence, a period where parental influence is the strongest.[55, 56, 57] Furthermore, our monitoring measure tapped in to parental solicitation of information, but not on related domains of disclosure or rule setting. Further research to understand family processes is essential for the development of HIV prevention interventions in SSA that include caregivers.
Number of close friends and community engagement did not predict risk class. Our friendship variable may not have distinguished between quality friendships or the nature of peer influence. Previous studies in this setting have found that having older friends and perceiving that your friends had have sex was associated with increased odds of HIV and HSV-2.[29, 58] Given that the influence of friends increases with age, our results might also be explained by the fact that we measured our friendship variable in early adolescence among participants who had never had sex.[56, 59, 60] Similar to peer influence, community involvement was coarsely measured as a count of groups with which the participant was involved, and this variable did not measure intensity of involvement or the demographics of the community group. Previous studies in South Africa have found that sports groups and groups that include an element of adult supervision are potentially protective, while groups that provide an opportunity for young girls to interact with existing or new intimate partners are potentially risky.[61, 28]
In addition to our social bonding variables, increased household income (measured as household expenditures) provided some protection against membership in higher-risk trajectory classes. Many young girls in our study setting, and other parts of South Africa, experience the transition to adulthood in households impacted by poverty. Existing empirical evidence suggests that there are number of social context pathways through which poverty increases AGYWs vulnerability to HIV. First, poorer young women seek out older male partners to increase their economic and social capital but gender and power imbalances constrain their ability to refuse sex, negotiate safe sex, or leave risky relationships.[62, 63, 64] Second, caregivers in impoverished households might have less time to monitor adolescents or develop strong bonds with them, which in turn might lead to engagement in risky sexual behaviors.[65] Third, young girls in impoverished households might have less opportunity to consistently attend school, a well-established protective context for risky sexual behaviors.[66, 67, 68, 69, 70]
Limitations and Future Directions
This analysis is based on a relatively large, longitudinal study of adolescents and young women from South Africa. High quality data were complemented by the use of a sophisticated data analytic approach that capitalized on the rich measures and longitudinal data structure. Nevertheless, there were some study limitations. First, we had to rely on single-item measures or proxies to measure peer relationships and household income. Some of the measures that we would have liked to include in this analysis were not included in the data set. We did not have any measures of violence or victimization beyond physical IPV and sexual IPV. Endorsement of sexual IPV was very low in our sample and was therefore excluded from our analysis. Based on studies showing that AGYW who experience sexual IPV almost always experience the other types of IPV, we believe that it is unlikely that the inclusion of sexual IPV in our analysis would have changed the results [71, 72]. Because emotional IPV is more common than physical IPV, we are less certain about whether our results might have been affected if were able to include this indicator.
Second, all of the participants in our sample were enrolled in high school at baseline. Although most 13–15-year old girls in South Africa are still enrolled in school, this restriction means that we may have missed the highest-risk segment of the population who had already dropped out of school by this age. We further risked selecting lower-risk participants by choosing to include only the participants who were not sexually active in the first wave. We made this choice to retain temporal precedence of childhood risk factors and sexual outcomes. Additionally, our study was conducted in the context of HPTN 068, a randomized intervention where treatment arm participants, and their households, received financial support in the form of monthly cash transfers, conditional on regular school attendance while the control arm participants received no transfers.[?] Though we measured household income at baseline, before the intervention was implemented, it might be possible trajectory group membership was impacted by intervention arm assignment. Finally, follow-up sample sizes declined as participants aged out of high school. Our attrition analyses suggested only that higher-income adolescents were more likely to be lost to follow up, and our use of FIML estimation allowed us to relax our missing data assumptions. Nevertheless, we may have been able to recover more classes if we had additional data in later years.
Conclusions
Highest risk sexual behaviors occur early. Thus, prevention of sexual risk behaviors for South African adolescent girls should begin around puberty. A multi-level contextual approach to prevention should target parents and schools to promote social control arising from high-quality social bonds.
Acknowledgements:
NLB was supported by the National Institute of Allergy and Infectious Diseases (T32 AI00700140). The HIV Prevention Trials Network is funded by the National Institute of Allergy and Infectious Diseases (UM1AI068619, UM1AI068613, and UM1AI1068617), with co-funding from the National Institute of Mental Health and the National Institute on Drug Abuse, all components of the US National Institutes of Health. This work was also supported by NIMH(R01MH087118) and the Carolina Population Center and its NIH Center Grant (P2C HD050924).
Footnotes
Publisher's Disclaimer: This AM is a PDF file of the manuscript accepted for publication after peer review, when applicable, but does not reflect postacceptance improvements, or any corrections. Use of this AM is subject to the publisher’s embargo period and AM terms of use. Under no circumstances may this AM be shared or distributed under a Creative Commons or other form of open access license, nor may it be reformatted or enhanced, whether by the Author or third parties. See here for Springer Nature’s terms of use for AM versions of subscription articles: https://www.springernature.com/gp/open-research/policies/accepted-manuscript-terms
Conflicts of Interest: Not applicable.
Ethics approval: From the institutional review board at University of North Carolina, Chapel Hill
References
- [1].“AIDS statistics: 2019 factsheet. UNAIDS,” Global HIV, 2019. [Google Scholar]
- [2].Simbayi L, Zuma K, Zungu N, Moyo S, Marinda E, Jooste S, Mabaso M, Ramlagan S, North A, Van Zyl J, et al. , “South African national HIV prevalence, incidence, behaviour and communication survey, 2017: towards achieving the UNAIDS 90-90-90 targets,” 2019.
- [3].Gómez-Olivé FX, Angotti N, Houle B, Klipstein-Grobusch K, Kabudula C, Menken J, Williams J, Tollman S, and Clark SJ, “Prevalence of HIV among those 15 and older in rural South Africa,” AIDS care, vol. 25, no. 9, pp. 1122–1128, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Pettifor A, O’Brien K, MacPhail C, Miller WC, and Rees H, “Early coital debut and associated HIV risk factors among young women and men in South Africa,” International perspectives on sexual and reproductive health, pp. 82–90, 2009. [DOI] [PubMed] [Google Scholar]
- [5].McCarthy K, Brady M, and Hallman K, “Investing when it counts: Reviewing the evidence and charting a course of research and action for very young adolescents,” Population Council Knowledge Commons, 2016. [Google Scholar]
- [6].Kalamar AM, Bayer AM, and Hindin MJ Journal of Adolescent Health, vol. 59, no. 3, p. S22–S31, 2016. [DOI] [PubMed] [Google Scholar]
- [7].Stockl H, Kalra N, Jacobi J, and Watts C, “Is early sexual debut a risk factor for HIV infection among women in Sub-Saharan Africa? a systematic review,” American Journal of Reproductive Immunology, vol. 69, p. 27–40, 2013. [DOI] [PubMed] [Google Scholar]
- [8].World Health Organization, “Adolescent pregnancy factsheet https://www.who.int/news-room/factsheets/detail/adolescent-pregnancy,” Jan 2020.
- [9].Decker MR, Latimore AD, Yasutake S, Haviland M, Ahmed S, Blum RW, Sonenstein F, and Astone NM, “Gender-based violence against adolescent and young adult women in low-and middle-income countries,” Journal of Adolescent Health, vol. 56, no. 2, p. 188–196, 2015. [DOI] [PubMed] [Google Scholar]
- [10].Dixon-Mueller R, “How young is “too young”? comparative perspectives on adolescent sexual, marital, and reproductive transitions,” Studies in Family Planning, vol. 39, p. 247–262, Dec 2008. [DOI] [PubMed] [Google Scholar]
- [11].Lee RLT, Yuen Loke A, Hung TTM, and Sobel H, “A systematic review on identifying risk factors associated with early sexual debut and coerced sex among adolescents and young people in communities,” Journal of clinical nursing, vol. 27, no. 3–4, p. 478–501, 2018. [DOI] [PubMed] [Google Scholar]
- [12].Blum RW, Astone NM, Decker MR, and Mouli VC, “A conceptual framework for early adolescence: a platform for research,” International Journal of Adolescent Medicine and Health, vol. 26, p. 321–331, Aug 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Sommer M, “An overlooked priority: Puberty in Sub-Saharan Africa,” American Journal of Public Health, vol. 101, p. 979–981, Jun 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Cederbaum JA, Gilreath TD, and Barman-Adhikari A, “Perceived risk and condom use among adolescents in Sub-Saharan Africa: a latent class analysis,” African Journal of Reproductive Health, vol. 18, p. 26–33, Dec 2014. [PubMed] [Google Scholar]
- [15].Small E and Weller BE, “Profiles of malawian adolescents at risk for hiv infections: Implications for targeted prevention, policy, and practices,” AIDS care, vol. 25, no. 3, p. 289–295, 2013. [DOI] [PubMed] [Google Scholar]
- [16].Tibbits MK, Caldwell LL, Smith EA, Vergnani T, and Wegner L, “Longitudinal patterns of active leisure among South African youth: Gender differences and associations with health risk behaviours,” World Leisure Journal, vol. 58, no. 1, p. 60–68, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Weller BE and Small E, “Profiles of risk for HIV/AIDS among young malawian adults: Understanding behavioral intentions,” Sexuality & Culture, vol. 19, p. 685–696, Dec 2015. [Google Scholar]
- [18].Weybright EH, Caldwell LL, Ram N, Smith EA, and Wegner L, “Trajectories of adolescent substance use development and the influence of healthy leisure: A growth mixture modeling approach,” Journal of adolescence, vol. 49, p. 158–169, Jun 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Houle B, Yu S-T, Angotti N, Schatz E, Kabudula CW, Gómez-Olivé FX, Clark SJ, Menken J, and Mojola SA, “Clusters of hiv risk and protective sexual behaviors in agincourt, rural south africa: Findings from the ha nakekela population-based study of ages 15 and older,” Archives of Sexual Behavior, vol. 49, p. 2057–2068, Aug 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Bauer DJ and Shanahan MJ, “Modeling complex interactions: Person-centered and variable-centered approaches,” Modeling contextual effects in longitudinal studies, pp. 255–283, 2007. [Google Scholar]
- [21].Comins CA, Rucinski KB, Baral S, Abebe SA, Mulu A, and Schwartz SR, “Vulnerability profiles and prevalence of HIV and other sexually transmitted infections among adolescent girls and young women in ethiopia: A latent class analysis,” PloS one, vol. 15, no. 5, p. e0232598, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Umberson D, Crosnoe R, and Reczek C, “Social Relationships and Health Behavior Across the Life Course,” Annual Review of Sociology, vol. 36, no. 1, pp. 139–157, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Crockett LJ, Bingham CR, Chopak JS, and Vicary JR, “Timing of first sexual intercourse: The role of social control, social learning, and problem behavior,” Journal of youth and adolescence, vol. 25, no. 1, pp. 89–111, 1996. [DOI] [PubMed] [Google Scholar]
- [24].Kotchick BA, Shaffer A, Miller KS, and Forehand R, “Adolescent sexual risk behavior: A multi-system perspective,” Clinical psychology review, vol. 21, no. 4, pp. 493–519, 2001. [DOI] [PubMed] [Google Scholar]
- [25].Hirschi T, “A control theory of delinquency,” Criminology theory: Selected classic readings, vol. 1969, pp. 289–305, 1969. [Google Scholar]
- [26].Price J, Pettifor A, Selin A, Wagner RG, MacPhail C, Agyei Y, Gómez-Olivé FX, and Kahn K, “The association between perceived household educational support and HIV risk in young women in a rural South African community (HPTN 068): A cross sectional study,” PLOS ONE, vol. 14, p. e0210632, Jan. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Stoner MCD, Nguyen N, Kilburn K, Gómez-Olivé FX, Edwards JK, Selin A, Hughes JP, Agyei Y, Macphail C, Kahn K, and Pettifor A, “Age-disparate partnerships and incident HIV infection in adolescent girls and young women in rural South Africa,” AIDS (London, England), vol. 33, pp. 83–91, Jan. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Bhushan NL, Stoner MC, Twine R, Kahn K, Lippman SA, and Pettifor AE, “Community Space, Community Groups, and Incident HIV Infection Among Adolescent Girls and Young Women in Rural South Africa: A Longitudinal Analysis of HIV Prevention Trials Network 068 Data.,” Journal of Acquired Immune Deficiency Syndromes (1999), 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Fearon E, Wiggins RD, Pettifor AE, MacPhail C, Kahn K, Selin A, Gómez-Olivé FX, Delany-Moretlwe S, Piwowar-Manning E, and Laeyendecker O, “Associations between friendship characteristics and HIV and HSV-2 status amongst young South African women in HPTN-068,” Journal of the International AIDS Society, vol. 20, no. 4, p. e25029, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Arnett JJ, “Emerging adulthood: A theory of development from the late teens through the twenties.,” American psychologist, vol. 55, no. 5, p. 469, 2000. [PubMed] [Google Scholar]
- [31].Sawyer SM, Afifi RA, Bearinger LH, Blakemore S-J, Dick B, Ezeh AC, and Patton GC, “Adolescence: a foundation for future health,” The lancet, vol. 379, no. 9826, pp. 1630–1640, 2012. [DOI] [PubMed] [Google Scholar]
- [32].Blum RW, Astone NM, Decker MR, and Mouli VC, “A conceptual framework for early adolescence: a platform for research,” International journal of adolescent medicine and health, vol. 26, no. 3, pp. 321–331, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Collinson MA, “Striving against adversity: the dynamics of migration, health and poverty in rural South Africa,” Global health action, vol. 3, no. 1, p. 5080, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Pettifor A, MacPhail C, Hughes JP, Selin A, Wang J, Gómez-Olivé FX, Eshleman SH, Wagner RG, Mabuza W, Khoza N, et al. , “The effect of a conditional cash transfer on HIV incidence in young women in rural South Africa (HPTN 068): a phase 3, randomised controlled trial,” The Lancet Global Health, vol. 4, no. 12, pp. e978–e988, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Resnick MD, Bearman PS, Blum RW, Bauman KE, Harris KM, Jones J, Tabor J, Beuhring T, Sieving RE, Shew M, et al. , “Protecting adolescents from harm: findings from the National Longitudinal Study on Adolescent Health,” JAMA, vol. 278, no. 10, pp. 823–832, 1997. [DOI] [PubMed] [Google Scholar]
- [36].García-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C, et al. , WHO multi-country study on women’s health and domestic violence against women. World Health Organization, 2005. [Google Scholar]
- [37].Dean DO, Bauer DJ, and Shanahan MJ, “A discrete-time multiple event process survival mixture (mepsum) model.,” Psychological methods, vol. 19, no. 2, p. 251, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Dean DO, Cole V, and Bauer DJ, “Delineating prototypical patterns of substance use initiations over time,” Addiction, vol. 110, no. 4, pp. 585–594, 2015. [DOI] [PubMed] [Google Scholar]
- [39].Nagin DS, Jones BL, Passos VL, and Tremblay RE, “Group-based multi-trajectory modeling,” Statistical Methods in Medical Research, vol. 27, pp. 2015–2023, 2018. [DOI] [PubMed] [Google Scholar]
- [40].Hipp JR and Bauer DJ, “Local solutions in the estimation of growth mixture models.,” Psychological methods, vol. 11, no. 1, p. 36, 2006. [DOI] [PubMed] [Google Scholar]
- [41].Vermunt JK, “Latent class modeling with covariates: Two improved three-step approaches,” Political analysis, pp. 450–469, 2010. [Google Scholar]
- [42].Sommer M and Mmari K, “Addressing structural and environmental factors for adolescent sexual and reproductive health in low-and middle-income countries,” American journal of public health, vol. 105, no. 10, pp. 1973–1981, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Lloyd CB, “The role of schools in promoting sexual and reproductive health among adolescents in developing countries,” 2007.
- [44].Okigbo CC, Kabiru CW, Mumah JN, Mojola SA, and Beguy D, “Influence of parental factors on adolescents’ transition to first sexual intercourse in Nairobi, Kenya: a longitudinal study,” Reproductive health, vol. 12, no. 1, pp. 1–12, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Biddlecom A, Awusabo-Asare K, and Bankole A, “Role of parents in adolescent sexual activity and contraceptive use in four african countries,” International perspectives on sexual and reproductive health, pp. 72–81, 2009. [DOI] [PubMed] [Google Scholar]
- [46].Mlunde LB, Poudel KC, Sunguya BF, Mbwambo JK, Yasuoka J, Otsuka K, Ubuguyu O, and Jimba M, “A call for parental monitoring to improve condom use among secondary school students in Dar es Salaam, Tanzania,” BMC Public Health, vol. 12, no. 1, pp. 1–11, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Sidze EM and Defo BK, “Effects of parenting practices on sexual risk-taking among young people in cameroon,” BMC public health, vol. 13, no. 1, pp. 1–14, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Negeri EL, “Assessment of risky sexual behaviors and risk perception among youths in Western Ethiopia: the influences of family and peers: a comparative cross-sectional study,” BMC Public Health, vol. 14, no. 1, pp. 1–12, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Dittus PJ, Michael SL, Becasen JS, Gloppen KM, McCarthy K, and Guilamo-Ramos V, “Parental monitoring and its associations with adolescent sexual risk behavior: A meta-analysis,” Pediatrics, vol. 136, no. 6, pp. e1587–e1599, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Kalina O, Geckova AM, Klein D, Jarcuska P, Orosova O, van Dijk JP, and Reijneveld SA, “Mother’s and father’s monitoring is more important than parental social support regarding sexual risk behaviour among 15-year-old adolescents,” The European Journal of Contraception & Reproductive Health Care, vol. 18, no. 2, pp. 95–103, 2013. [DOI] [PubMed] [Google Scholar]
- [51].Parkes A, Henderson M, Wight D, and Nixon C, “Is parenting associated with teenagers’ early sexual risk-taking, autonomy and relationship with sexual partners?,” Perspectives on sexual and reproductive health, vol. 43, no. 1, pp. 30–40, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Pilgrim NA, Ahmed S, Gray RH, Sekasanvu J, Lutalo T, Nalugoda F, Serwadda D, and Wawer MJ, “Family structure effects on early sexual debut among adolescent girls in Rakai, Uganda,” Vulnerable children and youth studies, vol. 9, no. 3, pp. 193–205, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Kidman R and Palermo T, “The relationship between parental presence and child sexual violence: evidence from thirteen countries in Sub-Saharan Africa,” Child abuse & neglect, vol. 51, pp. 172–180, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Somefun OD and Odimegwu C, “The protective role of family structure for adolescent development in Sub-Saharan Africa,” PloS one, vol. 13, no. 10, p. e0206197, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Longmore MA, Manning WD, and Giordano PC, “Parent-child relationships in adolescence,” 2013.
- [56].Steinberg L and Morris AS, “Adolescent development,” Annual review of psychology, vol. 52, no. 1, pp. 83–110, 2001. [DOI] [PubMed] [Google Scholar]
- [57].Kajula LJ, Darling N, Kaaya SF, and De Vries H, “Parenting practices and styles associated with adolescent sexual health in Dar es Salaam, Tanzania,” AIDS care, vol. 28, no. 11, pp. 1467–1472, 2016. [DOI] [PubMed] [Google Scholar]
- [58].Fearon E, Wiggins RD, Pettifor AE, MacPhail C, Kahn K, Selin A, Gómez-Olivé FX, and Hargreaves JR, “Friendships among young south african women, sexual behaviours and connections to sexual partners (HPTN 068),” AIDS and Behavior, vol. 23, no. 6, pp. 1471–1483, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Ali MM and Dwyer DS, “Estimating peer effects in sexual behavior among adolescents,” Journal of adolescence, vol. 34, no. 1, pp. 183–190, 2011. [DOI] [PubMed] [Google Scholar]
- [60].Fearon E, Wiggins RD, Pettifor AE, and Hargreaves JR, “Is the sexual behaviour of young people in Sub-Saharan Africa influenced by their peers? a systematic review,” Social Science & Medicine, vol. 146, pp. 62–74, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [61].Kaufman CE, Clark S, Manzini N, and May J, “Communities, opportunities, and adolescents’ sexual behavior in KwaZulu-Natal, South Africa,” Studies in family planning, vol. 35, no. 4, pp. 261–274, 2004. [DOI] [PubMed] [Google Scholar]
- [62].Kilburn K, Hughes JP, MacPhail C, Wagner RG, Gómez-Olivé FX, Kahn K, and Pettifor A, “Cash transfers, young women’s economic well-being, and HIV risk: Evidence from HPTN 068,” AIDS and Behavior, vol. 23, no. 5, pp. 1178–1194, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Kim J, Pronyk P, Barnett T, and Watts C, “Exploring the role of economic empowerment in HIV prevention,” AIDS, vol. 22, pp. S57–S71, 2008. [DOI] [PubMed] [Google Scholar]
- [64].Krishnan S, Dunbar MS, Minnis AM, Medlin CA, Gerdts CE, and Padian NS, “Poverty, gender inequities, and women’s risk of human immunodeficiency virus/AIDS,” Annals of the New York Academy of Sciences, vol. 1136, p. 101, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Brook DW, Morojele NK, Zhang C, and Brook JS, “South African adolescents: pathways to risky sexual behavior,” AIDS Education & Prevention, vol. 18, no. 3, pp. 259–272, 2006. [DOI] [PubMed] [Google Scholar]
- [66].Stoner MC, Edwards JK, Miller WC, Aiello AE, Halpern CT, Julien A, Selin A, Hughes JP, Wang J, Gomez-Olive FX, et al. , “The effect of schooling on age-disparate relationships and number of sexual partners among young women in rural South Africa enrolled in HPTN 068,” Journal of acquired immune deficiency syndromes (1999), vol. 76, no. 5, p. e107, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Stoner MC, Pettifor A, Edwards JK, Aiello AE, T HALPERN C, Julien A, Selin A, Twine R, Hughes JP, Wang J, et al. , “The effect of school attendance and school dropout on incident HIV and hsv-2 among young women in rural South Africa enrolled in HPTN 068,” AIDS (London, England), vol. 31, no. 15, p. 2127, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [68].Stoner MC, Rucinski KB, Edwards JK, Selin A, Hughes JP, Wang J, Agyei Y, Gomez-Olive FX, MacPhail C, Kahn K, et al. , “The relationship between school dropout and pregnancy among adolescent girls and young women in South Africa: A HPTN 068 analysis,” Health Education & Behavior, vol. 46, no. 4, pp. 559–568, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Pettifor AE, Levandowski BA, MacPhail C, Padian NS, Cohen MS, and Rees HV, “Keep them in school: the importance of education as a protective factor against HIV infection among young South African women,” International journal of epidemiology, vol. 37, no. 6, pp. 1266–1273, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Zuilkowski SS and Jukes MC, “The impact of education on sexual behavior in Sub-Saharan Africa: a review of the evidence,” AIDS care, vol. 24, no. 5, pp. 562–576, 2012. [DOI] [PubMed] [Google Scholar]
- [71].Blasdell R, “The co-occurrence of physical and sexual intimate partner violence among us college females,” International Journal of Criminal Justice Sciences, vol. 16, no. 1, pp. 97–109, 2021. [Google Scholar]
- [72].Sokol RL, Ennett ST, Gottfredson NC, Shanahan ME, Poti JM, Halpern CT, and Fisher EB, “Child maltreatment and body mass index over time: The roles of social support and stress responses,” Children and youth services review, vol. 100, pp. 214–220, 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]