

Abstract
Background
Type 2 diabetes mellitus (T2DM) has become one of the serious public health problems in China, and it affects the quality of survival of patients significantly. The long-term monitoring and early warning of T2DM and its complications should be paid attention to. Artificial diagnosis of T2DM in traditional Chinese medicine (TCM) is subjective and unrepeatable at the present stage. It is important to develop standardized collection and objective analysis methods of TCM inquiry. Therefore, we are interested in establishing syndrome recognition models.
Objective
The establishment of the TCM syndrome recognition model of T2DM is helpful to the syndrome diagnosis of the disease, and the clear diagnosis of the syndrome is the prerequisite for the effective treatment of the disease by TCM. At present, there are few studies on syndrome recognition models of T2DM. Therefore, based on the inquiry information of TCM, we establish a latent structure model (LSM) of T2DM syndrome in Shanghai, hoping to provide services for the health management of TCM for diabetes in the future.
Methods
A total of 587 effective samples of T2DM patients in Shanghai were collected. The gender, course of disease, and chronic complications were analyzed by one-way ANOVA and frequency analysis. Inquiry symptoms that could be included in the model were screened. In the study, 30 symptoms were used as observable variables to analyze the symptom information of TCM inquiry, and then, the TCM syndrome recognition model was established.
Results
The clinical syndromes of patients with T2DM in Shanghai were mixed with deficiency and excess. The LSM divided the pattern of the disease into qi-yin deficiency pattern, yin deficiency pattern, qi deficiency pattern, and qi stagnation pattern. These patterns were mainly located in the spleen and stomach, liver, and kidney.
Conclusion
The results of the syndrome classification of T2DM by LSM are basically consistent with the TCM clinical characteristics of the disease, which could reflect its main etiology and pathogenesis. The LSM of TCM inquiry syndrome diagnosis of T2DM confirmed the objectivity of TCM syndrome differentiation to some extent, and it will lay a foundation for the development of a mobile APP for TCM health management of T2DM.
1. Introduction
According to the International Diabetes Federation in 2019, there were 463 million diabetes patients between the ages of 20 and 79 worldwide, of which about 4.2 million died from diabetes or its complications only in 2019, accounting for 11.3% of all global deaths. At present, China has become the “largest country” of diabetes, with 116.4 million adult patients (20–79 years old), in which 90% are type 2 diabetes mellitus (T2DM) showed by another study [1]. Thus, T2DM has become one of the serious public health problems in China. T2DM in the middle and later stages of the disease will continue to develop a variety of chronic complications, threatening the health and quality of life of patients. Therefore, carrying out the research on the prevention and treatment of diabetes and realizing the early diagnosis, prevention, and treatment of type 2 diabetes are very important in order to improve the health level of Chinese people and reduce the mortality rate of patients and the national medical burden.
Syndrome differentiation and treatment is the essence of traditional Chinese medicine (TCM). In TCM syndrome differentiation, the inquiry is extremely important, and a lot of clinical information of patients can only be obtained through inquiry, especially those diseases with only conscious symptoms and lack of objective signs. However, to a certain extent, acquiring inquiry data depends on the personal experience, diagnostic skills, cognitive level, and thinking ability of doctors, so that the strong subjectivity, the poor repeatability, and the lack of unified implementation standards make it difficult to unify syndrome differentiation. In recent years, many researchers have established and explored to the standardized collection of TCM inquiry information and the exploration of objective analysis methods, which has made some progress in the objective, standardized, and procedural research of TCM inquiry. Among them, the latent structure model (LSM) proposed by Zhang [2] could analyze the information of TCM inquiry and establish a TCM syndrome recognition model. The model is the result of the multidimensional division of the population from various perspectives based on the characteristics of the data itself, which has strong objectivity and quantification. On this basis, the collection of patient information with TCM inquiry scale, wearable and portable tongue photography equipment, pulse diagnosis bracelet [3], and other objective tools of TCM four diagnosis will help to detect disease progress at low cost and provide a more efficient and fast channel for information feedback and disease follow-up between doctors and patients.
Therefore, taking diabetes as the starting point, we used the diabetes TCM inquiry scale to collect patients' clinical symptom information and established T2DM TCM inquiry database, so that we could analyze the data and construct the latent structure recognition model of TCM syndrome, which would be beneficial to the objective arrangement of the clinical data and rapid diagnosis, lay a research foundation for the objectification of TCM inquiry, and provide a theoretical basis for the realization of T2DM TCM health management mobile service.
2. Materials and Methods
2.1. Samples
All samples were collected from January 2014 to November 2020 in Yueyang Integrated Traditional Chinese and Western Medicine Hospital and Shuguang Hospital.
2.2. Ethical Approval
The study was approved by the Ethics Committee of Shanghai University of TCM in China in January 2014 and performed in accordance with the Declaration of Helsinki. All the subjects had signed informed consent agreements before collecting samples.
2.3. Criteria
2.3.1. Diagnostic Criteria
Glycosylated hemoglobin (HbA1c) ≥ 6.5%, refer to the American Diabetes Association guidelines for Diabetes diagnosis and treatment (2014). The trial was conducted in accordance with the methods certified by the American HbA1c Standardization Program and standardized with the detection of diabetes control and complication studies; or fasting blood glucose ≥7.0 mmol/L, defined as no calorie intake for at least 8 hours. Or oral glucose tolerance test 2 hours blood glucose ≥11.1 mmol/L, according to the standard of World Health Organization, using 75 g anhydrous glucose dissolved in water as glucose load; or in patients with typical symptoms of hyperglycemia or hyperglycemia crisis, random blood glucose ≥11.1 mmol/L. If there is no definite hyperglycemia, the results should be confirmed by repeated tests.
2.3.2. Inclusion Criteria
Patients who (1) met the diagnostic criteria of T2DM, (2) were between 30 and 80 years old, and (3) were volunteered to cooperate with the study and signed the informed consent form were included.
2.3.3. Exclusion Criteria
Patients who (1) had gestational diabetes or diabetes with pregnancy, (2) psychopath, (3) with other serious primary diseases were excluded; and (4) had acute metabolic disorders such as diabetic ketoacidosis and complicated infection in recent 1 month.
2.4. TCM Inquiry Information Collection
The clinical cases were collected by using the TCM inquiry of the T2DM scale developed by our research group, and the scale (Copyright Bureau of Shanghai Registration Number: 09-2011-A-118) had passed the test of reliability and validity. As the objectivity of TCM clinical consultation data is largely affected by the subjective factors of both doctors and patients, in order to ensure the unity of collection standards in the process of investigation, members of the collection team were trained regularly and discussed on typical cases to ensure the standardization and consistency of the information collected as far as possible.
The symptom information of all inquiries was assigned to “1” and “0”, respectively, according to their “yes” and “no”. Data input was used by EpiData3.1 software.
2.5. Statistical Analysis
IBM SPSS Statistics19.0 statistical software was used for statistical analysis. The data were analyzed by one-way ANOVA and frequency analysis.
LSM was used to construct the TCM syndrome recognition model of T2DM. Hierarchical latent class model, referred to as HLC model, is a special latent variable model [4]: (1) The network structure is a nontrivial rooted tree, in which the root node has at least two child nodes. (2) All leaf nodes represent observable variables, so they are also called observable nodes. All inner nodes represent latent variables, so they are also called latent nodes. Figure 1 shows an HLC model.
Figure 1.
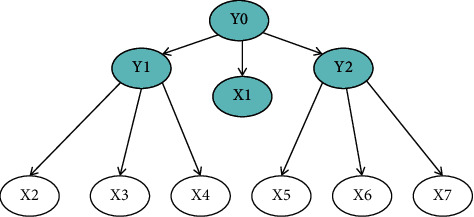
In the HLC mode, Y0, Y1, and Y2 are latent variables, and X1 and X2…X7 are observable variables.
There are many latent variables in the HLC model, and each latent variable corresponds to a clustering method. We used the double hill climbing (DHC) algorithm. That is, the model optimization problem was decomposed into potential learning problem and premodel learning problem. DHC did not search in the space of all regular HLC models directly but divided the space into two levels by using potential learning and premodel learning and searches in each level, respectively.
The analysis tool used in this paper was Lantern5.0 software. HLCM is a learning toolbox for latent structure analysis of JAVA language written by Professor Lianwen Zhang of Hong Kong University of Science and Technology. This toolbox consists of the following three parts:
Hlcm.zip//Learning the encapsulated classes in the package
LearnHLCM.Java//Running main program
SampleData.Txt//Providing reference data format
The operation of the software needs to download and install the Java running environment jdk tool and set the environment variables after the download and installation. The running platform can make use of the DOS command window of the system. Before using the HLCM toolbox, we need to rewrite our format according to the format required by the tool, and during the calculation, the resulting model data are saved in a separate file.
2.6. Model Evaluation
Bayesian information criterion [5] (BIC) is the score matched with the optimal model in the process of running the DHC. The quality of HLC can be measured by the BIC score. On the one hand, the model is required to fit the data and reveal the laws implied in the data. On the other hand, the model is required to be as simple as possible. In the process of operation, the fitting degree between the model and data was improved continuously, so that the BIC score increased gradually. When the model becomes too complex to meet the requirements, the BIC falls instead of rises. Then, the process stops. The BIC score was measured by a negative number. In general, the higher the BIC score, the better the model.
3. Results
3.1. Summary of Demographics and Clinic Characteristics of Samples
A total of 587 T2DM patients were included in this study, in which the oldest patient was 89 years old, and the youngest patient was 24 years old. The average age was 63.35 ± 11.14 years old, including 520 patients aged 50 or above, accounting for 88.59% of all patients. The sex, course of disease, abnormality of routine physical and chemical indexes, and chronic complications are detailed in Table 1.
Table 1.
Summary of gender, course of disease, and chronic complications of patients (n = 587).
| Demographics and clinical information | Count | Frequency (%) |
|---|---|---|
| Sample number | 587 | N/A |
| Number of males in the sample | 257 | 43.78 |
| Number of females in the sample | 330 | 56.22 |
| Ratio of males to females | 1 : 1.28 | N/A |
| Average age (year) | 63.35 ± 11.14 | N/A |
| Number (percentage) of samples diagnosed this time | 32 | 9.20 |
| Number (percentage) of samples diagnosed for 1–3 years | 101 | 29.02 |
| Number (percentage) of samples diagnosed for 4–10 years | 132 | 37.93 |
| Number (percentage) of samples diagnosed for 10–20 years | 69 | 19.83 |
| Number (percentage) of samples diagnosed more than 20 years | 14 | 4.02 |
| Number (percentage) of samples with coronary heart disease | 59 | 10.05 |
| Number (percentage) of samples with kidney disease | 34 | 5.79 |
| Number (percentage) of samples with retinopathy | 18 | 3.07 |
| Number (percentage) of samples with neuropathy | 5 | 0.85 |
| Number (percentage) of samples with foot lesions | 2 | 0.34 |
| Number (percentage) of samples with complications more than two | 15 | 2.46 |
3.2. Screening Symptom Information for TCM Inquiry of T2DM
Before the recognition model of TCM syndrome of T2DM is established, it is necessary to screen the inquiry information. The principle of screening the inquiry information of T2DM is that it should reflect not only the clinical characteristics of diabetes in TCM but also the theory of syndrome differentiation of T2DM in TCM and fully embody the guiding role of TCM theory and TCM experts. The method of screening variables is combined with the frequency analysis of T2DM inquiry information and the scoring of TCM experts (3 deputy senior titles and above).
According to the frequency analysis of inquiry symptom information and the ranking of expert scores from high to low, 30 inquiry variables were determined to participate in the modeling. These symptoms included fatigue, thirst with a liking for fluids, soreness and pain of waist and knees, dizziness, difficulty to fall asleep, palpitation, easy to wake up after sleep, chest distress, irritability, dry stool, spontaneous sweating, bitter taste in the mouth, thin and sloppy stool, loss of appetite, fear of chills, tinnitus and deafness due to chronic illness or old age, frequent nocturnal urination, blurred vision, epigastric distention, itchy skin, numbness of hands and feet, anxiety, night sweats, abdominal distention, edema, fear of heat, shortness and less of breath, hiccup and belching, dry, itchy and painful on eyes, and sore mouth and tongue (Table 2).
Table 2.
Inquiring symptoms of T2DM included in latent structure model after the frequency analysis of inquiry symptom information and the ranking of the expert.
| Syndromes | Count (%) |
|---|---|
| Fatigue | 190 (32.37%) |
| Soreness and pain of waist and knees | 160 (27.26%) |
| Difficult to fall asleep | 132 (22.49%) |
| Easy to wake up after sleep | 109 (18.57%) |
| Irritability | 91 (15.50%) |
| Spontaneous sweating | 84 (14.31%) |
| Thin and sloppy stool | 71 (12.10%) |
| Fear of chills | 62 (10.56%) |
| Frequent nocturnal urination | 59 (10.05%) |
| Epigastric distention | 56 (9.54%) |
| Numbness of hands and feet | 45 (7.67%) |
| Night sweats | 42 (7.16%) |
| Edema | 35 (5.96%) |
| Shortness and less of breath | 27 (4.60%) |
| Dry, itchy, and painful on eyes | 21 (3.58%) |
| Thirst with liking for fluids | 172 (29.30%) |
| Dizziness | 136 (23.17%) |
| Palpitation | 130 (22.15%) |
| Chest distress | 101 (17.21%) |
| Dry stool | 89 (15.16%) |
| Bitter taste in mouth | 76 (12.95%) |
| Loss of appetite | 64 (10.90%) |
| Tinnitus and deafness due to chronic illness or old age | 60 (10.22%) |
| Blurred vision | 57 (9.71%) |
| Itchy skin | 50 (8.52%) |
| Anxiety | 43 (7.33%) |
| Abdominal distention | 37 (6.30%) |
| Fear of heat | 28 (4.77%) |
| Hiccup and belching | 24 (4.09%) |
| Sore mouth and tongue | 20 (3.41%) |
3.3. Latent Structure Model of T2DM Syndrome
Thirty symptoms were taken as observable variables, and four recessive variables were obtained after model learning, which were recorded as Y0, Y1, Y2, and Y3, respectively, as shown in Figure 2. The BIC score of our study was −6318.41.
Figure 2.
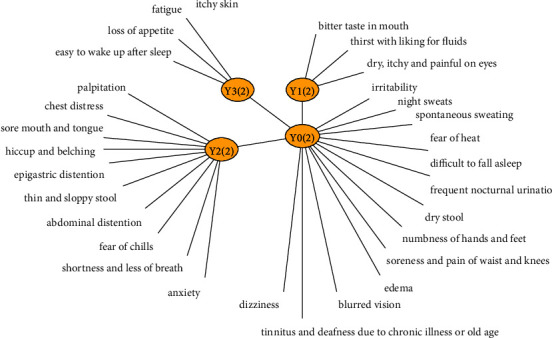
In the latent structure model of T2DM syndrome, Y0(2), Y1(2), Y2(2), and Y3(2) are latent variables, and fatigue, thirst with a liking for fluids, and soreness and pain of waist and knees, sore mouth and tongue are observable variables.
3.4. Comparison between LSM of T2DM Syndrome and TCM Theory in Qualitative and Quantitative Aspect
3.4.1. Interpretation of TCM Theory to Model
There were four latent variables in the model. Each latent variable represented the partition of a data sample, and each partition was composed of two or more latent classes. The qualitative evaluation of the model was to explain the meanings of these partitions and latent classes from the perspective of TCM. Each latent variable had two inseparable aspects: on the one hand, it represented a partition; on the other hand, it represented the mechanism of partition. The cases collected and analyzed in our subject were all patients with T2DM, which were consistent with the dysfunction of qi, blood, yin, and yang in TCM.
With setting the cumulative information coverage to 95% in the software, this study derived a lot of symptom information (observable variables) covered by latent variables and exported-related information curves plot.
In the information graph (Figure 3(a)), it could be seen that the latent variable Y0 affected the appearance of variables such as irritability, dizziness, soreness, and pain of waist and knees, spontaneous sweating, blurred vision, difficulty to fall asleep, numbness of hands and feet, tinnitus, and deafness due to chronic illness or old age, fear of heat, and night sweats. Yin deficiency and internal heat caused being afraid of heat. Internal heat disturbed the heart mind, which led patients to be irritable. The deficiency of liver and kidney yin kept eyes out of being moisturized and then blurred vision appeared. Waist tendons and veins lost their nourishment because of loss of kidney essence, so the waist and knees were pained. Abnormal renal function may lead to the lesion of ear function. Chronic illness or old age made kidney yin deficiency, so tinnitus and deafness came out. Liver yin deficiency or qi deficiency, which resulted in blood deficiency or qi deficiency, failed to transport and transform the refined substance, and finally, numbness of hands and feet appeared. Kidney yin deficiency produced internal heat and disturbed heart fire. Heart fire was hyperactive, so it was difficult to fall asleep. Yin deficiency and internal heat forced fluid to leak out, which caused night sweats. Qi deficiency made head and eyes malnutrition, and dizziness appeared. Defensive Qi instability caused spontaneous sweating. Therefore, Y0 could be interpreted as a “qi-yin deficiency pattern” by the theory of TCM.
Figure 3.
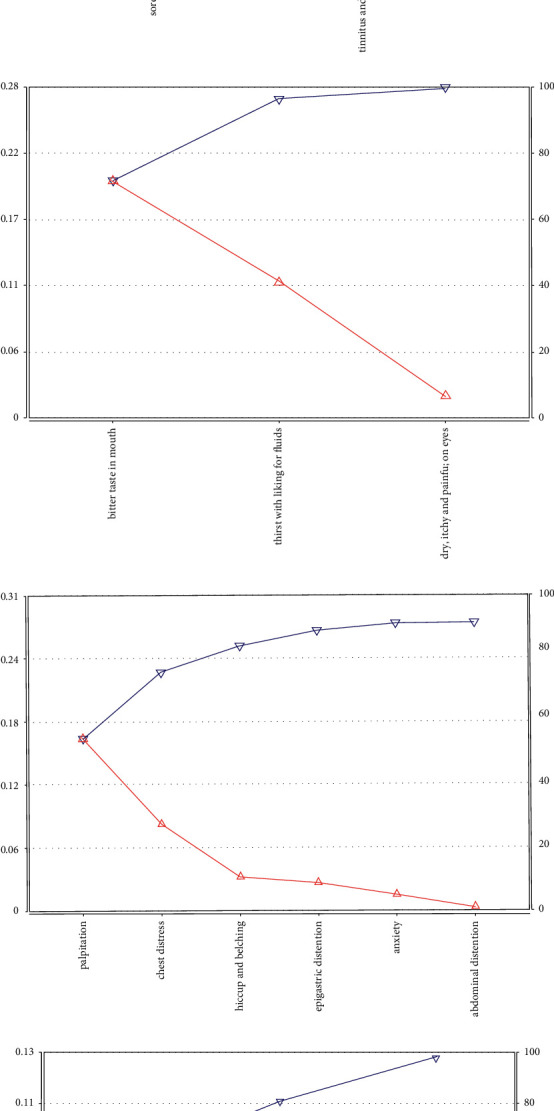
Observable variable mutual information and information coverage curve. (a) Observable variable mutual information and information coverage curve of latent variable Y0. (b) Observable variable mutual information and information coverage curve of latent variable Y1. (c) Observable variable mutual information and information coverage curve of latent variable Y2. (d) Observable variable mutual information and information coverage curve of latent variable Y3.
The latent variable Y1 affected the occurrence of bitter taste in the mouth, thirst with a liking for fluids, and dry, itchy, and painful on eyes. Yin deficiency of liver and kidney caused deficiency of fire. Liver qi was nonflowing, so bile spilling out caused a bitter taste in the mouth. Yin deficiency and internal heat consumed body fluid, which caused thirst with a liking for fluids. Body fluid could not moisten the eyes, so the eyes were dry and painful. Therefore, Y1 could be interpreted as “yin deficiency” by the theory of TCM (Figure 3(b)).
The latent variable Y2 affected palpitation, chest distress, hiccup and belching, epigastric distension, irritability, and abdominal distention. Heart qi stagnated in the heart and chest, or phlegm and blood stasis blocked, which caused heart pulse obstruction, so palpitation and chest distress appeared. Spleen and stomach qi stagnation brought about abnormal transport of cereal nutrients, so epigastric distension and abdominal distension appeared. The stomach was appropriate to fall, so when the stomach qi reversed upward, hiccup and belching came out. When liver qi was depressed, qi was stagnated, which led to irritability. Therefore, Y2 could be interpreted as “qi stagnation” by the theory of TCM (Figure 3(c)).
The latent variable Y3 affected the appearance of loss of appetite, being fatigued, and difficulty to fall asleep. Spleen and stomach qi deficiency caused abnormal transportation function, so the loss of appetite appeared. Qi deficiency could not help qi and blood distributing throughout the body, which led to viscera function decline, so the patients were fatigued. Deficiency of heart and spleen qi made qi and blood insufficient transformation. Heart blood deficiency caused heart loss of nourishment, so the patients were easy to wake up after sleep. Therefore, Y3 could be interpreted as “qi deficiency” by the theory of traditional Chinese medicine (Figure 3(d)).
The corresponding relationship between latent variables in the model and TCM syndromes is shown in Table 3.
Table 3.
The corresponding relationship between latent variables in the model and TCM patterns.
| Y 0 | Qi-yin deficiency pattern |
| Y 1 | Yin deficiency pattern |
| Y 2 | Qi stagnation pattern |
| Y 3 | Qi deficiency pattern |
3.4.2. Evaluation of Quantitative Content of Model
The quantitative content of the model has two aspects: (1) The number of latent variables in the model is 4. (2) The class conditional probability distribution is used to quantitatively describe the relationship between variables.
The partition represented by latent variables in the latent structure model is a probabilistic soft partition. A thing may belong to a certain class with a certain probability, and it can also belong to another class with a certain probability. In order to grasp the characteristics of each class in probability soft division, it is necessary to investigate their class conditional probability distribution. We gave the quantitative relationship between the latent variables and the observable variables by the class conditional probability distribution P(X = 1│Y = S1) and P(X = 1│Y = S0). The conditional probability distribution of the two latent classes Y0 = S1 and Y0 = S0 of Y0 is shown in Table 4. There were two values of S1 and S0 in the group of deficiency of both qi and yin in Y0, indicating that model M had divided the population of deficiency of both qi and yin into two categories, namely “appearing” (S1) or “not appearing” (S0). The column P(X = 1│Y0 = S1) gave the probability that the observable variable valued for 1(that is, the occurrence of symptoms) in the latent Y0 = S1, while the column P(X = 1│Y0 = S0) gave the probability that the observable variable valued for 1 in the latent Y0 = S0. According to Table 4, the main difference between the two latent categories was that the probability of occurrence of all 11 symptoms in Y0 = S1 was higher, while in Y0 = S0, the probability was much lower. Especially, fear of heat was close to zero. The relationship between “a deficiency of both qi and yin” and “irritability, dizziness, soreness, and pain of waist and knees” was quantitatively described by conditional probability, which was consistent with the theory of traditional Chinese medicine.
Table 4.
Conditional probability distribution table of two latent class Y0 = S1 and Y0 = S0 of latent variable Y0 class.
| Observable variables | P(X = 1│Y0 = S1) | P(X = 1│Y0 = S0) |
|---|---|---|
| Irritability | 0.36 | 0.05 |
| Dizziness | 0.43 | 0.13 |
| Soreness and pain of waist and knees | 0.47 | 0.17 |
| Spontaneous sweating | 0.29 | 0.07 |
| Blurred vision | 0.22 | 0.04 |
| Difficult to fall asleep | 0.38 | 0.15 |
| Numbness of hands and feet | 0.17 | 0.03 |
| Tinnitus and deafness due to chronic illness or old age | 0.20 | 0.05 |
| Fear of heat | 0.12 | 0.01 |
| Night sweats | 0.13 | 0.04 |
| Dry stool | 0.23 | 0.11 |
As could be seen from Table 5, in the category of Y1 = S1, there was a higher probability of bitter taste in the mouth, thirst with a liking for fluids, and dry, itchy, and painful on eyes, while in the category of Y1 = S0, there was a certain probability of thirst with a liking for fluids. The probability of bitter taste in the mouth and dry, itchy, and painful on eyes was lower. It showed that the symptoms of bitter taste in the mouth and dry, itchy, and painful on eyes also had a certain probability in other patterns. It was quite consistent with the theory of TCM because the relationship between TCM patterns and symptoms was not a one-to-one correspondence. The combination of symptoms played an important role in pattern differentiation.
Table 5.
Conditional probability distribution table of two latent class Y1 = S1 and Y1 = S0 of latent variable Y1 class.
| Observable variables | P(X = 1│Y1 = S1) | P(X = 1│Y1 = S0) |
|---|---|---|
| Bitter taste in mouth | 0.50 | 0.00 |
| Thirst with liking for fluids | 0.67 | 0.16 |
| Dry, itchy, and painful on eyes | 0.10 | 0.01 |
Although TCM theory did not strongly confine the presence of a symptom, it implied that the symptoms depended on the change of the degree of the syndrome. For a symptom, the higher the severity of the pattern, the more likely it was to appear, and the more severe it would appear. Similarly, the class probability distributions of other latent variables in the model are shown in Tables 6 and 7
Table 6.
Conditional probability distribution table of two latent class Y2 = S1 and Y2 = S0 of latent variable Y2 class.
| Observable variables | P(X = 1│Y2 = S1) | P(X = 1│Y2 = S0) |
|---|---|---|
| Palpitation | 0.51 | 0.03 |
| Chest distress | 0.36 | 0.05 |
| Hiccup and belching | 0.10 | 0.00 |
| Epigastric distention | 0.18 | 0.04 |
| Anxiety | 0.13 | 0.04 |
| Abdominal distention | 0.09 | 0.05 |
Table 7.
Conditional probability distribution table of two latent class Y3 = S1 and Y3 = S0 of latent variable Y3 class.
| Observable variables | P(X = 1│Y3 = S1) | P(X = 1│Y3 = S0) |
|
| ||
| Loss of appetite | 0.78 | 0.07 |
| Fatigue | 0.92 | 0.29 |
| Easy to wake up after sleep | 0.72 | 0.16 |
In order to make the characteristics of latent classes clear, the probability distributions of these classes could be shown in a line chart (Figure 4).
Figure 4.
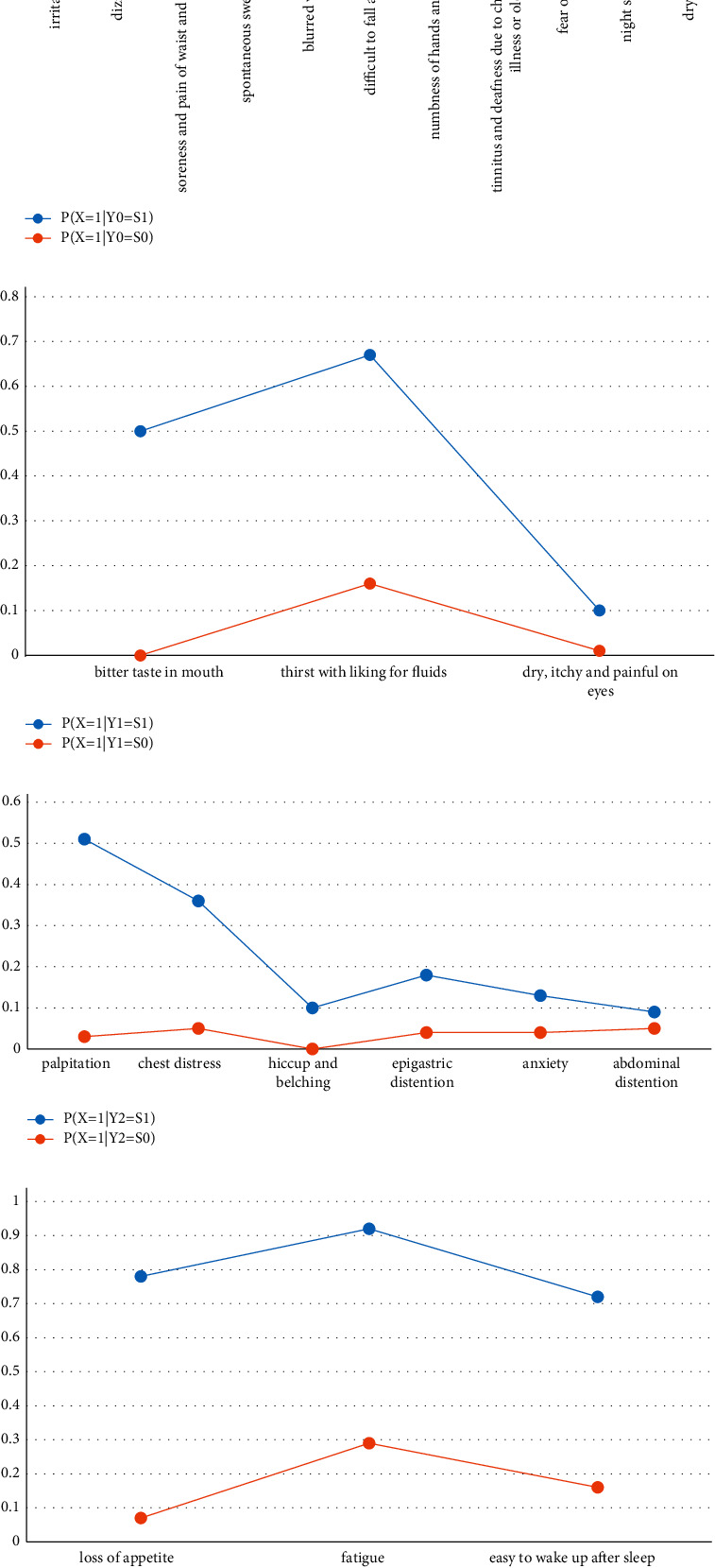
Line charts of conditional probability distributions. (a) Line charts of conditional probability distributions of two latent classes Y0 = S1 and Y0 = S0 of latent variable Y0. (b) Line charts of conditional probability distributions of two latent classes Y1 = S1 and Y1 = S0 of latent variable Y1. (c) Line charts of conditional probability distributions of two latent classes Y2 = S1 and Y2 = S0 of latent variable Y2. (d) Line charts of conditional probability distributions of two latent classes Y3 = S1 and Y3 = S0 of latent variable Y3.
4. Discussion
Based on the Bayesian network and probability graph model, the latent structure model reveals the latent characteristics behind observable variables by analyzing the latent class probability, conditional probability, mutual information, and information coverage and excavates the logical relationship between the observable variables and the latent variables. It is a special method proposed for the research of TCM. The basic idea is to use computers instead of human brains to analyze data and construct latent structures. Whether the symptoms of TCM appear or not is not independent of each other but related to each other. Through the observation of the occurrence of symptoms in many patients, we can find a variety of statistical relationships between them, which provide the basis for finding the latent structure behind the symptoms.
In term of TCM data exploration, we often pay special attention to the relationship and pattern among symptoms and between symptoms and patterns, which means we would pay special attention to the two-variable relationship study between latent variables and latent variables or observable variables. The theory of syndrome differentiation of TCM includes observable variables, latent variables, and latent classes. The relationship between them constitutes a latent structure. The latent structure method [6] is based on the results collected from the clinical epidemiological investigation, by which it replaced the human brain for data analysis on a computer, and constructed a model which could define the pattern well. Finally, the LSM is used to guide syndrome differentiation, which is objective to a certain extent.
Diabetes is a disease related to wasting thirst in TCM. In this study, the latent structure method was used to analyze the TCM inquiry symptom information of 587 patients with T2DM in Shanghai, and the syndrome recognition models of qi-yin deficiency pattern, yin deficiency pattern, qi deficiency pattern, and qi stagnation pattern were established, and these syndromes were mainly located in spleen and stomach, liver, and kidney.
In the modern research of TCM syndrome of diabetes, many researchers believe that the pattern of deficiency of both qi and yin is the most common pattern of T2DM [7, 8]. After a certain period of disease development, phlegm turbidity and blood stasis are still the most common signs during disease evolution [9, 10].
Xu. et al. [11] have investigated the distribution of TCM syndrome types of diabetes, and their results showed that deficiency of both qi and yin accounted for the most significant pattern, in which many of them had blood stasis during the disease. Ai et al. [12] and others found that the distribution of TCM patterns of diabetes mainly included deficiency of both qi and yin, dryness-heat, and phlegm-dampness. The research of Zhao [13] showed that the TCM patterns of diabetic patients were mainly yin deficiency and qi deficiency, accounting for 26.0% and 21.9%, respectively, which were consistent with the syndrome characteristics of qi and yin deficiency of thirst disease. Ren et al. [14] and others studied the patterns of prediabetes by the method of cluster analysis. Their results implied that the characteristics of deficiency in origin and excess in superficiality in prediabetes were obvious, and the symptoms of qi deficiency patterns such as spontaneous sweating and mental fatigue were prominent. It suggested that the qi deficiency pattern played a leading role in patients with prediabetes.
Yang et al. [15] found that patients with diabetes complicated with depression had more obvious pathogenesis characteristics of liver depression and internal obstruction of blood stasis than those without depression. Cao [16], by analyzing single syndrome statistics, found that the patients with qi stagnation patterns accounted for 27.98% of 218 diabetic patients with stable angina pectoris. Zhang [17] found that the frequency of heat in perianal abscess with T2DM was the highest, followed by yin deficiency, phlegm-dampness, and qi stagnation. According to the modern research on the epidemiological investigation of diabetes, qi-yin deficiency pattern, yin deficiency pattern, qi deficiency pattern, and qi stagnation pattern were all common clinical patterns of the disease, which showed that the latent structure model established in this study was basically in line with the clinical actual situation.
In this study, the latent variable qi and yin deficiency pattern led to dizziness. In addition to qi deficiency, the main pathogenesis of dizziness might be related to internal obstruction of phlegm and dampness disturbing clear yang or internal stagnation of blood stasis blocking the flow of qi and blood, and then, the head could not be nourished. The latent variable qi stagnation led to the emergence of palpitation, and its main pathogenesis was not only related to qi stagnation but also related to phlegm-dampness and blood stasis blocking clear yang, resulting in malnutrition of heart spirit. Latent variable qi stagnation also led to epigastric distention and abdominal distension, which might also be related to phlegm-dampness blocking middle-jiao and water accumulating. It could be seen that, in addition to the syndrome obtained by this model, phlegm-dampness syndrome and blood stasis syndrome would also appear in the development of T2DM.
The clinical manifestations related to phlegm-dampness syndrome and blood stasis syndrome are often reflected in the tongue and pulse of patients. The tongue body of patients with phlegm-dampness syndrome is fat, with greasy moss or slippery moss, and the pulse is moist or slippery. The tongue manifestation of blood stasis syndrome is purple and dark, with petechiae, ecchymosis, or sublingual collateral varicose veins. The pulse is usually a rough pulse or irregularly intermittent pulse. However, this study only used the TCM inquiry scale, which did not include the tongue, pulse, and other clinicopathologic data related to inspection and amputation.
In this study, the LSM of TCM inquiry syndrome diagnosis of T2DM confirmed the objectivity of TCM syndrome differentiation to some extent. In the future, based on the ideas and results of this study, we hope to use the “Internet Plus” technology, combined with TCM inquiry scale, tongue photography software, pulse diagnosis bracelet, and other TCM four diagnosis objective mobile devices, to lay the foundation for the research of objective disease recognition model of four diagnosis information fusion. With the development of sensor, chip, mobile Internet, and other technologies, wearable and portable devices have shown great potential. This study will contribute to the development of a mobile APP for TCM health management of T2DM, to achieve mobile monitoring, management, and early warning of the disease development for diabetes. Through the establishment of the web-based information collection system and circulation system for diabetes patients, it can help doctors obtain objective information of diabetes patients in real time, establish a new follow-up system, and provide doctors with a more convenient, fast, and efficient way of follow-up. At the same time, it reduces the difficulty for patients to obtain feedback information, increases the viscosity and compliance of follow-up, reduces the long-term complications of diabetes, and improves physical condition, quality of life, and span of patients. In addition, with the help of the “noncontact” four-diagnosis mode of mobile APP based on TCM health management, it is conducive to the collection of clinical data and rapid diagnosis of isolated patients with infectious diseases such as COVID-19, so as to reduce the medical burden of the country.
In addition, the cases included in this study were all people in Shanghai, and the distribution of TCM patterns of T2DM also had a certain regional nature. Therefore, in future research, we are going to expand the sample size and collect TCM clinical information of diabetic patients from other representative areas, so that it may constantly improve the syndrome recognition model to make it more universal.
Acknowledgments
This work was supported by the Fund for Fostering Talents in Basic Science of the National Natural Science Foundation of China (No. J1103607), Scientific Research Project of Shanghai Municipal Commission of Health and Family Planning (No.20164Y0279), Shanghai Science and Technology Planning Program (No. 21DZ2271000), and Shanghai Education Commission Program (No. 2021 Science and Technology 02-37).
Data Availability
The Ethics Committee of Shanghai University of TCM limited the measurement data used to support the results of this study in order to protect the privacy of patients. For researchers who meet the criteria for obtaining confidential data, the data of this study can be obtained from Yiming Hao (e-mail: hymjj888@163.com).
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
Yiming Hao was responsible for the study and revised the manuscript. Chunlei Hou, Yanjie Cui, and Ying Xu wrote the manuscript. Chunlei Hou and Ying Xu analyzed the data. Yanjie Cui helped in plotting the results. All authors were involved in samples collection. Chunlei Hou, Yanjie Cui, and Ying Xu contributed equally to this study and share the first authorship.
References
- 1.Chinese Medical Association Diabetes Association. Guideline for prevention and treatment of type 2 diabetes in China (2013 Edition) China Diabetes Journal . 2014;6(7):447–498. [Google Scholar]
- 2.Zhang N. L. Hierarchical latent class models for cluster analysis. Journal of Machine Learning Research . 2004;5(6):697–723. [Google Scholar]
- 3.Hao Y., Cheng F., Pham M., et al. A noninvasive, economical, and instant-Result method to diagnose and monitor type 2 diabetes using pulse wave: case-control study. JMIR mHealth and Health . 2019;7(4) doi: 10.2196/11959.e11959 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zhang L., Guo H. Introduction to Bayesian Networks . 1st. Beijing, China: Science Press; 2006. [Google Scholar]
- 5.Schwarz G. Estimating the dimension of a model. Annals of Statistics . 1978;6(2):461–464. doi: 10.1214/aos/1176344136. [DOI] [Google Scholar]
- 6.Xu Y., Wang Z., Lv Y., Xu Y. The web version of lantern: a online analysis platform for TCM based on latent tree. World science and technology-modernization of traditional Chinese medicine . 2020;22(07):2224–2232. [Google Scholar]
- 7.Fan A., Zeng Y., Peng X., Su Q., Xu R. TCM syndrome types of 901 cases of T2DM in pudong center communities. Liaoning Journal of traditional Chinese medicine . 2016;43(5):905–908. [Google Scholar]
- 8.Gan J., Chen Y. Study on correlation between type 2 diabetes and TCM syndrome differentiation-typing. Journal of Yunnan University of traditional Chinese medicine . 2012;35(5):41–45. [Google Scholar]
- 9.Gao J., Junping W., Zheng Y. Study based on the investigation of TCM syndrome of T2DM in xicheng district. Journal of Basic Chinese Medicine . 2017;23(1):97–99. [Google Scholar]
- 10.Gong G., Qi L., Li J., Xing-Zhi Y., Wen Z. Epidemiology of chronic diabetic complications and Research of symptoms of traditional Chinese medicine of newly-diagnosed type 2 diabetes. Liaoning Journal of traditional Chinese medicine . 2012;39(1):26–30. [Google Scholar]
- 11.Xu B. Clinical Study on the Distribution of TCM Syndromes in Type 2 Diabetes mellitus . Wuhan, China: Hubei University of Traditional Chinese Medicine; 2020. [Google Scholar]
- 12.Ai W., Zhu X., Jiang X. Study on the distribution of TCM syndrome types in type 2 diabetic. Contemporary medicine . 2020;26(30):163–164. [Google Scholar]
- 13.Zhao L. Study on TCM Syndrome Classification and Metabolic Characteristics of Obesity and Non-obesity Type 2 Diabetes Mellitus . Taiyuan, China: Shanxi University of Traditional Chinese Medicine; 2018. [Google Scholar]
- 14.Ren M., Huo D., Sun X., Guo L. Multi-center clinical study on distribution and evolution rules of medicine syndrome in pre-diabetes. Journal of Traditional Chinese Medicine . 2018;59(09):769–772. [Google Scholar]
- 15.Yang X., Sun H., Wu H. Investigation of TCM syndromes in community patients with type 2 diabetes mellitus complicated with depression. Beijing Chinese Medicine . 2013;32(09):687–689. [Google Scholar]
- 16.Cao H. TCM Syndrome Characteristics of Type 2 Diabetes Mellitus with Stable Angina and its Related Influencing Factors . Beijing, China: North China University of Technology; 2018. [Google Scholar]
- 17.Zheng Q. Clinical Research on TCM Syndrome Factors Distribution of the Combination of Anal Abscess and Type 2 Diabetes Mellitus . Fuzhou, China: Fujian University of Traditional Chinese Medicine; 2020. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The Ethics Committee of Shanghai University of TCM limited the measurement data used to support the results of this study in order to protect the privacy of patients. For researchers who meet the criteria for obtaining confidential data, the data of this study can be obtained from Yiming Hao (e-mail: hymjj888@163.com).