

Abstract
Prerecorded video content in medical education has become more common. Increasingly accessible technology coupled with the COVID-19 pandemic and subsequent need for distanced learning has greatly increased the interest in and need for high-quality video content. The use of short educational videos to augment other teaching methods has been shown to improve learners’ experiences, knowledge retention, and understanding of content. Multiple studies have demonstrated that video education can be a highly effective tool for learning, particularly for hard-to-visualize processes and for procedural education. Videos allow learners to view content at their own pace and revisit materials on demand. In addition, well-designed videos can be repurposed by educators, ultimately reducing time needed to create high-quality educational content. Currently available technology allows educators to create high-quality videos at minimal cost and with a modest investment of time. This article details practical tips for creating high-yield educational videos.
Key Words: education, fellow training, pearls, resident training
Relevant Literature Review
Videos and digital media have played an increasingly important role in medical education, and there is growing evidence that thoughtfully produced videos are effective teaching tools. Short educational videos, which can be created by a stepwise approach (Fig 1), have been shown to improve clinical skill acquisition1,2 and to augment observational learning, whereby the trainee observes appropriate visuomotor behavior in a specific context by observing the actions of others and their outcomes.3 Extensive literature in surgical education supports the use of videos to augment the traditional apprenticeship model of procedural training.4 Training in pulmonary and critical care medicine shares, with surgical training, the fact that trainees must become competent at multiple procedures. Although at times learners intentionally observe experts to learn new information, observational learning can also occur unintentionally, with the risk of acquiring bad habits. Videos create a controlled learning environment in which the skills demonstrated can be standardized. Such videos can serve as both introductory training, for novice learners before initial simulation training, and just-in-time training, for learners to quickly review before completing a procedure on a clinical rotation. Studies indicate that the use of videos in addition to traditional teaching materials improves performance and decreases procedure time.5,6 Procedural learning theories emphasize the importance of watching procedures as part of training.7 Videos allow learners to watch procedures repeatedly, at their own pace, whenever they find it helpful.
Figure 1.
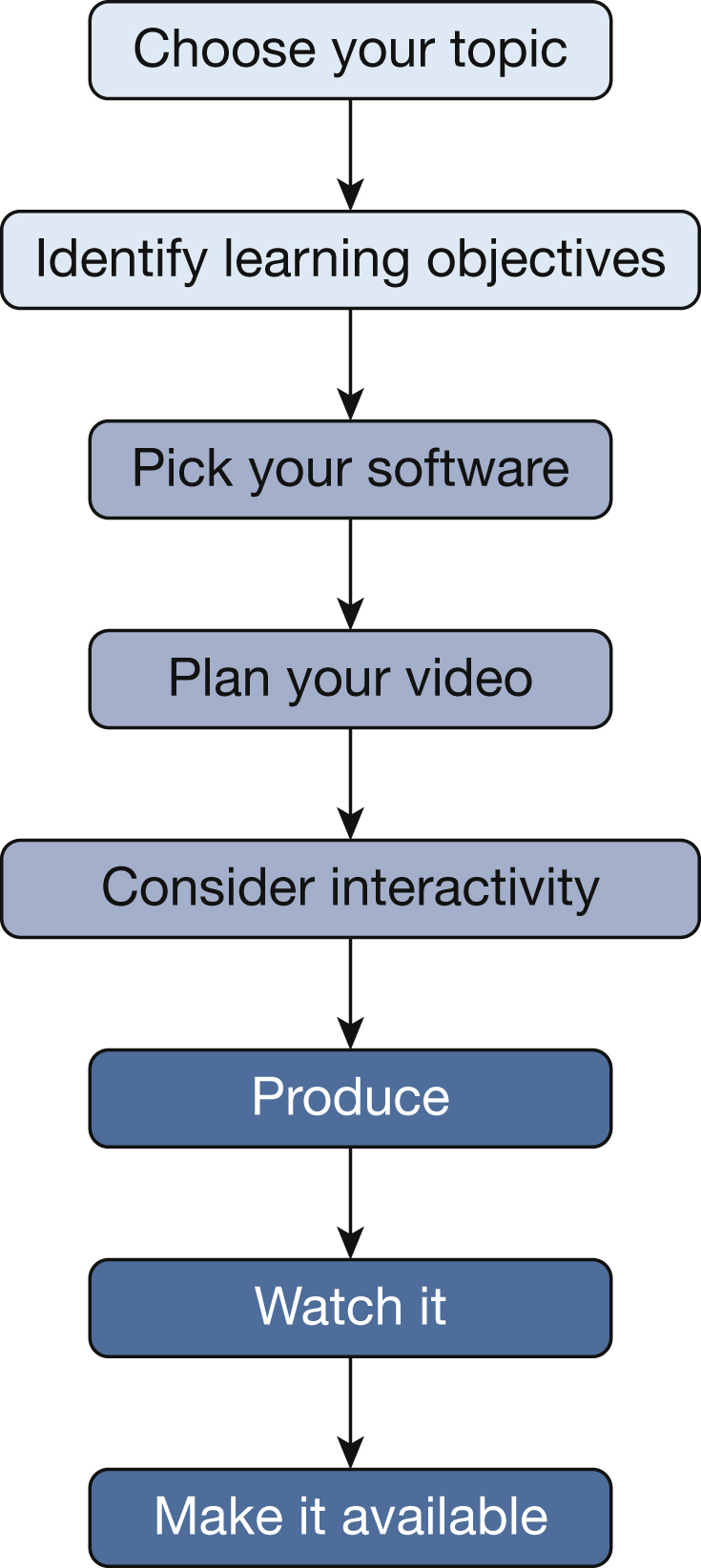
Summary of our approach to creating educational videos.
Videos lend themselves to pulmonary and critical care medicine training, not only for their benefits in procedural training, but also because critical care medicine is a field in which health-care providers are expected to manage high-risk, but low-frequency medical conditions, where rapid just-in-time training is likely to be helpful. One such condition is massive variceal hemorrhage, necessitating the placement of an esophageal tamponade catheter. One EM:RAP (Emergency Medicine Reviews and Perspectives) video on this topic, available on YouTube, has received more than 47,000 views.8 In addition, the COVID-19 pandemic has highlighted the importance of asynchronous and distance learning tools,9 especially in the field of critical care medicine. Staffing overfilled critical care units has sometimes required the provision of just-in-time training to non-critical care-trained providers.10 In addition to augmenting procedural learning, videos have been shown to improve understanding of complex cognitive concepts.11 High-quality videos can also improve student satisfaction,1 which in turn improves content engagement, an important factor for knowledge retention and understanding. Learners have noted that videos are a preferred educational format for the flexibility and opportunity to self-manage learning.12 This medium allows learners to control the speed and sequence of information, which has been shown to improve content comprehension.13 In summary, high-quality videos can be used to augment educational experiences, facilitating ease of interleaving (when a learner switches between subjects or topics), as well as spaced repetition, both of which are widely acknowledged as effective tools to increase knowledge retention.14
Two overlapping educational theories are particularly important to consider when developing educational videos: dual-channel processing and cognitive load theory. Multimedia content such as video is processed by working memory using two different channels: audio and visual. The dual-channel principle states that humans can process visual and auditory/written information simultaneously15 (Fig 2). However, cognitive load theory states that each channel has a limited capacity to process information,16 and when incoming information exceeds that capacity, cognitive overload occurs and inhibits learning.17 A number of strategies can be used in video creation to avoid cognitive overload, while simultaneously taking advantage of both the audio and visual working memory to facilitate understanding and retention. Evidence supports using static images when helpful, using concise narration, using short annotations and captions, and segmenting longer videos into smaller, discrete steps to promote maximal effective use of the audio and visual working memory pathways.18 It is important to avoid distractions, for example, background noise, poor-quality audio, and unnecessary images, as these all contribute to extraneous cognitive load. Extraneous cognitive load is created by material that requires processing but is not the focus of the video. It therefore reduces the processing capacity available for the relevant information.16
Figure 2.
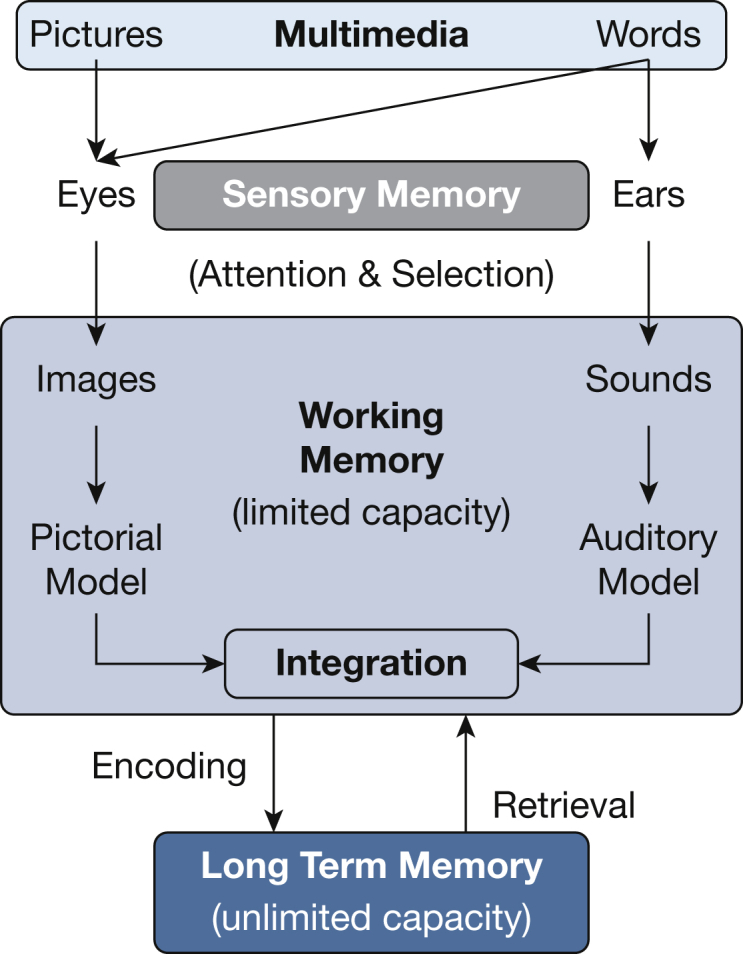
Dual-channel theory posits that multimedia learning is an active process of selecting words and images attended to by the sensory memory. Information from the sensory memory is subsequently processed by two channels (auditory and visual). Each channel has finite capacity, but can be used simultaneously. The working memory organizes these sounds and images and integrates them together and with prior knowledge from long-term memory; this is then encoded into long-term memory. (Adapted from Mayer15 and Thomson et al.18)
Here we provide a theory-based approach to creating educational videos that is practical for the busy educator. Our suggestions are based on research in effective teaching methods and adhere to the principles of cognitive load theory to encourage student engagement and promote active learning.14
Case Example
A trainee is planning to place a central venous catheter in the internal jugular vein of a patient and you ask them to evaluate the presence of lung sliding, using ultrasound. The trainee mentions they don’t feel confident evaluating for lung sliding on their own, as they’re unsure what the absence of lung sliding would look like. How could an educational video be made to help fill this education gap?
Summary of Our Approach
1. Choose Your Topic
Ideal topics for videos are those that will not soon be made obsolete. Consider topics that are taught regularly and unlikely to change, such as human anatomy or fundamental clinical principles. Topics that are likely to change rapidly, including developing guidelines or recent research findings, may not be worth the time investment needed for video creation. Regardless of the topic you choose, be sure to check that there isn’t already a high-quality video available that suits your purposes. In addition, to maximize the quality and lifetime of your video, we recommend assembling a group of colleagues (and potentially learners) to help you in the development stage and during the peer review process.
Lung ultrasound, specifically the appearance of lung slide, is a good topic for a video because the information is unlikely to become obsolete. However, it is worth doing an online search to see if a suitable video already exists on this topic.
2. Identify Specific Learning Objectives and a Target Length
As with any educational curriculum it is best to identify a few learning objectives. Creating successful learning objectives is addressed elsewhere.19,20 We recommend limiting the number of objectives to no more than five per video. Keeping the learning objectives appropriately narrow helps to reduce cognitive load on the learner,17 and focusing only on essential information increases the video’s efficacy.21
Keeping learning objectives tightly focused also helps to limit the video’s duration. This is important for maximizing learner attention. Although there is some disagreement about the ideal length of videos, most studies agree that 5 to 20 min is appropriate, although some have suggested that a 6- to 9-min video is the ideal length to maximize learning gains while minimizing inattention.21,22
For the lung slide video, learning objectives might be that by the end of this video, the learner will be able to:
-
•
recognize the pleural line on lung ultrasound;
-
•
distinguish between the presence and absence of lung slide; and
-
•
list two causes for the absence of lung slide.
3. Pick Your Software
There is a wide range of at-home software and equipment available for those interested in making videos. Although there are numerous programs available with varying levels of complexity, software falls into two major groups: those programs that require you to record videos in a single take, and those that allow the user to edit.
A single-take video created using simple technology (even just a smartphone) can be effective,22 although there are advantages to using more complex editing equipment. General features of single-take software vs software with editing capabilities are outlined in Table 1, with features of specific programs listed in Table 2. Program websites typically have helpful instructions, often including videos on how to use their software to make videos.
Table 1.
Two Categories of Video Creation Software
| Feature | Single-Take Software | Software With Editing |
|---|---|---|
| Free versions available | X | X |
| Requires recording in a single take | X | … |
| Records screen and/or webcast | X | X |
| Can record for longer than 15 min | Not typical | X |
| Program watermark must be present on recording | X | … |
| Trim recordings | X | X |
| Record audio + video simultaneously | X | X |
| Automated speech-to-text | … | X |
| Hide cursor or webcast | … | X |
| Add music or sound effects | … | X |
| Edit multiple audio tracks | … | X |
| Import videos/combine videos | … | X |
| Cut, copy, paste recorded sections | … | X |
| Add narration to existing videos | … | X |
| Blur sensitive information | … | X |
| Animate overlays and transitions | … | X |
| Zoom in/out of recorded material | … | X |
| Video overlays for picture-in-picture | … | X |
| Publish directly to websites (eg, YouTube, Google Classroom) | X | X |
| Add quizzes/feedback/other interactivity directly to video | … | X |
Table 2.
Sample of Video Production Software Available to Beginners
| Program | Compatible Operating System | Single-Take Option? | Description |
|---|---|---|---|
| Apple iMovie | iOS, macOS | No | Editing capable. Free with purchase of Mac or iPad, a “drag and drop”-based editing software. Features include video trimming, split-screen, audio editing, premade transitions, and image effects |
| Screencast-O-Matic | Windows, iOS, macOS | Yes | Free version is the “single take” option that records screen and/or webcast. You can trim the video but no other editing is available. Monthly subscription includes expanded features with a wide variety of editing capabilities. Directly add text, shapes, or overlays, splice recordings, video overlays, and picture-in-picture |
| Filmora from Wondershare | Windows, macOS | Yes | Editing capable. Free software, meant for beginners, with a “drag and drop”-based editing software interface. Features include video trimming, audio editing, premade transitions, and video effects |
| FilmoraGo from Wondershare | iOS, Android | Yes | Editing capable. Free phone app, with in-app purchases, that allows you to shoot and edit videos on the go. Excellent for filming on the go, particularly for shorter videos that require minimal effects or splicing |
| OpenShot | Windows, macOS, Linux | No | Editing capable. Free open-source video editing tool with “drag and drop” interface with basic video-editing capabilities (resizing, trimming, scaling, and rotation) with audio editing, watermarks, and customizable title cards |
| Lightworks | Windows, macOS, Linux | No | Editing capable. Free version available with basic editing features. Simple interface aimed at beginners, although some find the interface more complicated than other options listed. Users can easily trim video clips and edit audio, and it has some preset video effects in the free version |
| Shotcut | Windows, macOS, Linux | No | Editing capable. A free open-source video-editing platform. “Drag and drop” editing that accommodates multiple video and audio layers. Has advanced tools available |
| Camtasia | Windows, macOS | Yes | Editing capable. For-purchase video editing that allows incorporation of quizzes, loops of content, editing of audio and video, transitions, and simple animations |
| Aftereffects and Premiere Pro | Windows, macOS | No | Editing capable. Available as part of Adobe Creative Cloud—both are video-editing software used by professionals for creation of videos. Significant capabilities, but may be difficult to learn at first. As part of Adobe Cloud, provides access to many different stock photos |
| Playposit | Windows, macOS, Linux | No | Editing capable. Works with videos as “overlay” to “pause” videos to present participants with questions, multiple choice, multiselect, and short answer. Allows creation of video loops based on answers from participants |
Of the sample videos provided, Video 1 was created with free single-take software, whereas Video 2 was taken with the camera on a smartphone. Although Video 2 has a less professional appearance, with distracting wall decorations that add extraneous cognitive load and an ultrasound image that is difficult to see (Fig 3), the video required almost no investment of time beyond finding an ultrasound clip showing lung slide and writing the summary on a whiteboard. Although not well suited for complex concepts for just-in-time videos, this format offers a quick and easy solution for simple concepts in short video format.
Figure 3.

Video 2, taken with a smartphone camera, has extraneous cognitive load with distracting wall decorations in the background, and the ultrasound image is not clear.
4. Plan Your Video
Storyboarding
Writing out a script may feel overwhelming at first; however, we recommend at least some planning before recording a video. Planning can range from a basic outline of talking points to a fully scripted storyboard. The amount of planning required before filming is related to how “high-stakes” this video will be. How important is it that this video have high production quality? This may reflect audience needs, planned dissemination, or the author’s personal development as a videographer. However, using a script increases the efficiency of the presented material.
Our preferred method (when resources and time allow) is to storyboard the video before recording. This involves writing the script, word for word, in one column with representative images or videos in a second column. Figure 4 shows the storyboard used for the lung slide Video 2. Dictation software can facilitate this process, but this is the most time-intensive method of upfront planning. Ultimately, storyboarding may be the most efficient approach for durable educational material.23 Storyboarding results in a smoother production process, enables development of more effective visual aids, expedites audio recording, and helps with facilitating rerecording in the future. Planning of visual aids also allows easy review for copyrighted material that may require permission for use. In addition, it allows for easy peer review of the material before recording, which affords you an opportunity to solidify key learning points, ensure accurate information, and a logical progression of content before putting in any production work.
Figure 4.

Example of storyboard for a short educational video about lung sliding on ultrasound.
For script language, it has been shown that a conversational tone and informal communication style, using the first-person perspective, results in increased engagement and attention when compared with a more formal presentation style.24 This is different from written teaching resources, and we recommend reading your script aloud before recording. If making a written script sound conversational is a challenge, try dictating scripts rather than typing them.
Creation of a storyboard allows attention to cognitive load. The authors may focus discretely on both the auditory and visual channels, to ensure that material is complementary and not excessively duplicative. Authors can easily weed out extraneous material, and make sure that video content is segmented into chunks that make it more digestible to the learner.25
If detailed storyboarding appears too much for your planned video, at minimum create a basic outline of talking points. This can help you adhere to the learning objectives and present a linear, cohesive story. Scripts can easily be incorporated into the notes of a PowerPoint presentation to allow you to efficiently present your material. A standard approach is to present the learning objectives, review the main content, and then summarize the learning objectives again to conclude the video.
During planning, consider how you will adhere to all relevant privacy and institutional rules, for both the auditory and visual content. You must be careful not to violate patient privacy regulations, for example, by including patient data or identifiable images. Even if patient images are not identifiable, you should adhere to your facility rules about using patient images. For example, you may be required to obtain signed patient consent on a specific form. In addition, your institution may have rules governing allowable online content.
Testing equipment
Although you do not need professional-grade equipment, be sure that your video will be of adequate quality. We recommend focusing on ensuring excellent audio quality and adequate lighting that illuminates the speaker’s face. Guo et al22 have demonstrated that poor-quality videos increase the learner’s cognitive load and decrease learning gains. So, test your equipment, before embarking on video production. A 10-s test recording spoken at your planned volume is invaluable at this step.
When recording audio on its own, recording on a smartphone in a quiet room will generally produce good-quality sound without the need for an additional, expensive microphone. Otherwise, most video-editing software has the option to record audio directly on your computer (including free software versions). If you have difficulty with background noise, you may consider recording inside a closed vehicle with radio and A/C off or inside a walk-in closet, as this typically reduces echo. Just be sure that, when recording audio, the location has minimal distracting, background noises.
5. Consider Adding Activities
Watching videos can be a passive experience and some learners may find it difficult to remain attentive. Providing opportunities for interaction can facilitate cognitive engagement and improve the learning process.26 It has been shown that higher levels of interactivity are associated with more time on-task, which correlates with improved knowledge outcomes.27,28 However, you can have too much of a good thing. Excessive demands for learners to interact will exceed the capacity of working memory and degrade the learning.29 Consider adding one interactive element every 5 to 10 min to maintain attention and promote participation.
There are several ways to achieve this, depending on the software you are using. The simplest approach is to include questions with a pause while the question is showing on the screen, to allow learners time to answer. It is also easy to incorporate a QR code that directs learners to complementary materials, such as an online quiz or a shared editable webpage, where they can submit answers to questions. Alternatively, you could direct learners to complete a “scavenger hunt” for various things from the video, for example, by providing the timestamp at which certain concepts, words, or images are shown.
There are more advanced ways to incorporate activities, ones that require the use of specific software (see Table 1 for some example software programs). Some software allows provision of feedback to questions and can direct learners to different components of the video, based on their correct/incorrect answers. Others allow asynchronous learners to answer polling questions (either multiple choice or short answer) and to see the answers from prior participants. Some programs allow individuals to select “hotspots” on the screen that can be used for multiple choice questions or to advance to a new section of the video.
The lung slide videos, at only 2 min long, are short enough that they do not need to include any activities to keep learners engaged.
6. Produce
Create/assemble/review your images
Given the tenets of dual channel processing, the images shown when teaching are as important as the words being spoken. However, that does not mean that the images need to be complicated; in fact, a simple image or still can illustrate your point as effectively as a complicated video. If you are using a recorded video, for example, of a procedure, consider pausing the recording at suitable time points and adding arrows pointing to the item you are discussing, especially if it might not be obvious to the learner. It is more effective to show a complementary image with voiceover than to show prose and have the narrator read it.17
Many educators have already put a lot of time and effort into teaching presentations, and these slides can be adapted for video use. Simple images with arrows and short annotations are more effective than complicated animations or long sentences, as the latter will create extraneous cognitive load and inhibit learning.17 Video 1 demonstrates how simple slides with minimal annotations can be used to effectively signal the learner where on the screen to concentrate (Fig 5).
Figure 5.

Slides used in Video 1 are simple with short annotations and arrows that signal learners where to focus their concentration. A, The focus is on the soft tissues. B, The focus is on the pleural line.
Annotations should be placed close to the corresponding part of the image to reduce the need to look around the screen, and should be timed to appear simultaneously with the relevant narration.17 It is ideal to use a 24-point font or larger for all text. Alternatives to PowerPoint illustrations include taking photographs, software programs specifically for creating illustrations, and diagrams drawn by hand, for example, using a stylus and touch screen, a drawing tablet, a smart pen, or a smart notebook.
When choosing your images, do not use copyrighted images without following the appropriate guidelines for their reproduction. A summary of fair use laws for copyrighted images is beyond the scope of this review. Instead, create your own figures and images, or use free stock images that are in the public domain. Such images are available at sites such as Creative Commons (https://creativecommons.org) or Pixabay (https://pixabay.com).
You may find at this step that some of your images don’t fit the script, or don’t create the desired effect. If so, change one or the other to best convey the desired learning objective.
Use the webcam appropriately
There is mixed evidence on whether or not the instructor should be visible on the video. Some suggest that having the narrator or instructor be visible at the beginning or end of a video can increase engagement, by creating a connection and familiarity between the audience and the instructor. However, others have found that a “talking head” adds distraction and results in lower retention.18,30 Video 1 demonstrates how having the speaker on camera can contribute to extraneous cognitive load, and reduce the efficacy of an educational video. Single-take recording usually only allows a choice of webcam on or off for the entire video, and in these cases, we prefer not to include the speaker in the video. As in Video 1, watching the speaker does not typically convey additional information, and may distract the learner’s eyes from the material of interest, whereas narration accompanied by images takes advantage of both the auditory and visual channels in a complementary manner without the extraneous cognitive load required to process the image of the speaker’s face.27 However, talking directly to your audience before starting the main content, for example, during the introduction, can help to create a positive learning environment that can lead to increased engagement.22 If you are recording with software that allows editing, the webcam can be selectively turned on during summaries and turned off when there is more detailed visual information viewable.
7. Watch It
Although you may have reviewed your video in bits and pieces as you’ve edited it, be sure to watch the final product as a whole before sharing it. We also recommend having a trusted colleague and/or learner review the video before sharing it widely. They may notice important content that you overlooked and/or may reassure you that details that you find unbearable are not readily apparent to the audience (eg, that the image isn’t exactly what you wanted, or that you stammered).
8. Make the Video Available for Learners
There are several ways to make videos available to learners. Sometimes videos can be emailed to learners, but often they are too large, and so you will need to upload it to a website and then point learners to that website. There are a number of options available for video sharing that are simple and free. Online file-sharing websites, such as Google Drive or DropBox, can serve this purpose, or you can upload your video to a video-streaming website or app. Video-streaming services typically allow you to choose to keep your video private, which gives you some control over who views it, or make it public. Alternatively, you may wish to develop a website for your videos or use a website owned by your institution, if that is a possibility. Some institutional simulation centers host education videos.
Case Conclusion
After quickly making Video 2 and getting feedback that learners were still unsure about the appearance of the absence of lung slide, you developed Video 1, a 2-min video, and shared it with your resident team, as well as subsequent trainees. All of the program’s residents were able to use this video as a just-in-time review and as part of their critical care curriculum.
Acknowledgments
Financial/nonfinancial disclosures: None declared.
Additional information: The Videos can be found in the Supplemental Materials section of the online article.
Supplementary Data
Example of an effective educational video on lung sliding, using simple PowerPoint figures.
Example of a less effective educational video with extraneous cognitive load.
References
- 1.Cardoso A.F., Moreli L., Braga F.T.M.M., Vasques C.I., Santos C.B., Carvalho E.C. Effect of a video on developing skills in undergraduate nursing students for the management of totally implantable central venous access ports. Nurse Educ Today. 2012;32(6):709–713. doi: 10.1016/j.nedt.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 2.Holland A., Smith F., McCrossan G., Adamson E., Watt S., Penny K. Online video in clinical skills education of oral medication administration for undergraduate student nurses: a mixed methods, prospective cohort study. Nurse Educ Today. 2013;33(6):663–670. doi: 10.1016/j.nedt.2012.01.006. [DOI] [PubMed] [Google Scholar]
- 3.Monfardini E., Gazzola V., Boussaoud D., Brovelli A., Keysers C., Wicker B. Vicarious neural processing of outcomes during observational learning. PLoS One. 2013;8(9) doi: 10.1371/journal.pone.0073879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Green J.L., Suresh V., Bittar P., Ledbetter L., Mithani S.K., Allori A. The utilization of video technology in surgical education: a systematic review. J Surg Res. 2019;235:171–180. doi: 10.1016/j.jss.2018.09.015. [DOI] [PubMed] [Google Scholar]
- 5.Crawshaw B.P., Steele S.R., Lee E.C., et al. Failing to prepare is preparing to fail: a single-blinded, randomized controlled trial to determine the impact of a preoperative instructional video on the ability of residents to perform laparoscopic right colectomy. Dis Colon Rectum. 2016;59(1):28–34. doi: 10.1097/DCR.0000000000000503. [DOI] [PubMed] [Google Scholar]
- 6.Cheng Y.-T., Liu D.R., Wang V.J. Teaching splinting techniques using a just-in-time training instructional video. Pediatr Emerg Care. 2017;33(3):166–170. doi: 10.1097/PEC.0000000000000390. [DOI] [PubMed] [Google Scholar]
- 7.Sawyer T., White M., Zaveri P., et al. Learn, see, practice, prove, do, maintain: an evidence-based pedagogical framework for procedural skill training in medicine. Acad Med. 2015;90(8):1025–1033. doi: 10.1097/ACM.0000000000000734. [DOI] [PubMed] [Google Scholar]
- 8.EM:RAP Medical Linton, Blakemore, & Minnesota tubes overview [YouTube]. April 2, 2016. https://www.youtube.com/watch?v=Yv4muh0hX7Y
- 9.Hilburg R., Patel N., Ambruso S., Biewald M.A., Farouk S.S. Medical education during the coronavirus disease-2019 pandemic: learning from a distance. Adv Chronic Kidney Dis. 2020;27(5):412–417. doi: 10.1053/j.ackd.2020.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Steinbach T.C., Albert T.J., Carmona H.D., et al. Just-in-time tools for training non-critical care providers: troubleshooting problems in the ventilated patient. ATS Sch. 2020;1(2):178–185. doi: 10.34197/ats-scholar.2020-0038IN. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jolley D.F., Wilson S.R., Kelso C., O’Brien G., Mason C.E. Analytical thinking, analytical action: using prelab video demonstrations and e-quizzes to improve undergraduate preparedness for analytical chemistry practical classes. J Chem Educ. 2016;93(11):1855–1862. [Google Scholar]
- 12.Kelly M., Lyng C., McGrath M., Cannon G. A multi-method study to determine the effectiveness of, and student attitudes to, online instructional videos for teaching clinical nursing skills. Nurse Educ Today. 2009;29(3):292–300. doi: 10.1016/j.nedt.2008.09.004. [DOI] [PubMed] [Google Scholar]
- 13.Brockfeld T., Müller B., de Laffolie J. Video versus live lecture courses: a comparative evaluation of lecture types and results. Med Educ Online. 2018;23(1):1555434. doi: 10.1080/10872981.2018.1555434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sana F., Yan V.X., Kim J.A. Study sequence matters for the inductive learning of cognitive concepts. J Educ Psychol. 2017;109(1):84–98. [Google Scholar]
- 15.Mayer R.E. Applying the science of learning to medical education: applying the science of learning. Med Educ. 2010;44(6):543–549. doi: 10.1111/j.1365-2923.2010.03624.x. [DOI] [PubMed] [Google Scholar]
- 16.Mayer R.E. Applying the science of learning: evidence based principles for the design of multimedia instruction. Am Psychol. 2008;63(8):760–769. doi: 10.1037/0003-066X.63.8.760. [DOI] [PubMed] [Google Scholar]
- 17.Mayer R.E., Moreno R. Nine ways to reduce cognitive load in multimedia learning. Educ Psychol. 2003;38(1):43–52. [Google Scholar]
- 18.Thomson A., Bridgstock R., Willems C. “Teachers flipping out” beyond the online lecture: maximising the educational potential of video. J Learn Design. 2014;7(3):67–78. [Google Scholar]
- 19.Bloom B. Handbook I: Cognitive Domain. David McKay Company; New York: 1956. Taxonomy of educational objectives. [Google Scholar]
- 20.Brodsky D., Newman L.R. Educational perspectives: a systematic approach to curriculum development. Neoreviews. 2011;12(1):e2–e7. [Google Scholar]
- 21.Prober C.G., Khan S. Medical education reimagined: a call to action. Acad Med. 2013;88(10):1407–1410. doi: 10.1097/ACM.0b013e3182a368bd. [DOI] [PubMed] [Google Scholar]
- 22.Guo P., Kim J., Rubin R. Proceedings of the First ACM Conference on Learning @ Scale Conference, March 4-5, 2014. ACM; Atlanta, GA. New York: 2014. How video production affects student engagement: an empirical study of MOOC videos; pp. 41–50. [Google Scholar]
- 23.Norman M.K. Twelve tips for reducing production time and increasing long-term usability of instructional video. Med Teach. 2017;39(8):808–812. doi: 10.1080/0142159X.2017.1322190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Homer B.D., Plass J.L., Blake L. The effects of video on cognitive load and social presence in multimedia-learning. Comput Human Behav. 2008;24(30):786–797. [Google Scholar]
- 25.Brame C.J. Effective educational videos: principles and guidelines for maximizing student learning from video content. CBE Life Sci Educ. 2016;15(4):es6. doi: 10.1187/cbe.16-03-0125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Plass J.L., Schwartz R.N., Heidig (née Domagk) S. In: Seel N.M., editor. Vol. 3. Springer; Boston, MA: 2012. Interactivity in multimedia learning; pp. 1615–1617. (Encyclopedia of the Sciences of Learning). [Google Scholar]
- 27.Cook D.A., Levinson A.J., Garside S. Time and learning efficiency in internet-based learning: a systematic review and meta-analysis. Adv Health Sci Educ Theory Pract. 2010;15(5):755–770. doi: 10.1007/s10459-010-9231-x. [DOI] [PubMed] [Google Scholar]
- 28.McGaghie W.C., Issenberg S.B., Petrusa E.R., Scalese R.J. Effect of practice on standardised learning outcomes in simulation-based medical education. Med Educ. 2006;40(8):792–797. doi: 10.1111/j.1365-2929.2006.02528.x. [DOI] [PubMed] [Google Scholar]
- 29.Kalet A., Song H.S., Sarpel U., et al. Just enough, but not too much interactivity leads to better clinical skills performance after a computer assisted learning module. Med Teach. 2012;34(10):833–839. doi: 10.3109/0142159X.2012.706727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Díaz D., Ramírez R., Hernández-Leo D. ICALT ’15: Proceedings of the 2015 IEEE 15th International Conference on Advanced Learning Technologies, July 6-9, 2015, Hualien, Taiwan. IEEE Computer Society; Washington, DC: 2015. The effect of using a talking head in academic videos: an EEG study; pp. 367–369. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Example of an effective educational video on lung sliding, using simple PowerPoint figures.
Example of a less effective educational video with extraneous cognitive load.