

Abstract
Cardiovascular disease (CVD) poses a serious threat to urban health with the development of urbanization. There are multifaceted and comprehensive influencing factors for CVD, so clarifying the spatial distribution characteristics of CVD and multiple environmental influencing factors is conducive to improving the active health intervention of urban environment and promoting the sustainable development of cities The spatial distribution characteristics of CVD deaths in a certain district, Bengbu City, Huaihe River Basin, China, in 2019 were explored, and the correlation between multiple environmental factors and CVD mortality was investigated in this study, to reveal the action mechanism of multiple environmental factors affecting the risk of mortality. Relevant studies have shown that (1) CVD deaths are characterized as follows: male deaths are more than females; the mortality is higher in those of higher age; most of them are unemployed; cardiocerebral infarction is the main cause of death; and the deaths are mainly distributed in the central city and near the old urban area. (2) The increased CVD mortality can be attributed to the increased density of restaurants and cigarette and wine shops around the residential area, the increased traffic volume, the dense residential and spatial forms, the low green space coverage, and the distance from rivers. Therefore, appropriate urban planning and policies can improve the active health interventions in cities and reduce CVD mortality.
1. Introduction
A great number of studies have demonstrated the high mortality and disability rate of cardiovascular disease (CVD) [1] and the resulting global burden of diseases [2]. The traditional risk factors for CVD include hypertension, diabetes, dyslipidemia, obesity, smoking, alcohol consumption, and lack of physical exercise. However, under the biological-psychosocial medical model, the influencing factors on health are multifaceted and comprehensive, including environmental factors. Previous studies have shown that the urban population is more likely to suffer from cardiovascular diseases than the rural population in some developing countries [3]. Industrialization, urbanization, aging, and constant changes in the ecological environment and lifestyle have brought challenges to people's health in the rapid urban development. A lot of cities are experiencing a major shift in the disease spectrum from infectious diseases to chronic noncommunicable diseases. Therefore, it is conducive to improving active health interventions in urban environment and promoting sustainable urban development in the future to identify the mortality distribution characteristics of CVD and environmental influencing factors.
Previous studies have shown that unreasonable diet, excessive oil, and salt intake will increase the pressure of human circulatory system [4], thereby leading to CVD morbidity and mortality. The increase in the amount of physical activity, such as work, commuting, and leisure, will appropriately reduce the risk of CVD-related death [5], and the accessibility of sports and leisure activity facilities and open space will also have an influence on the level of physical activity of residents [6]. Residents will tend to commute by non-motor vehicles and increase daily activities provided that the urban road slow traffic system is perfect and the bus stops are dense [7]. In addition, residents engaged in manual work will have increased daily activities [8], thus reducing the risk of death. Air pollution [9–11] and noise pollution [12] constitute the important risk factors for CVD, of which long-term air pollution has a greater impact on CVD than short-term one [13]. The closer distance to the pollution source or the greater density of the surrounding pollution sources will increase the possibility of exposure to pollutants [14, 15], including a large number of industrial pollutants [16], the cooking fumes from [17], the exhaust gas emissions of motor vehicles, and urban transportation facilities, such as railways, subway lines, and airports [18]. Roads and restaurants produce noise pollution while causing air pollution, thereby leading to the occurrence of cardiovascular diseases [19]. The nearer distance from rivers and the higher green space coverage can effectively reduce the concentration of particulate matter (Douglas, W., and [20–22]) and lower CVD mortality. Cold weather and sudden temperature drop in winter are prone to causing overreaction of human function, resulting in death from acute CVD [23, 24]. The difference in temperature in different urban regions will lead to the difference in mortality.
In general, current studies focus on the macro-level of county [25], prefecture [26], and state [25], but neglect the small scales, such as communities and streets; meanwhile, the consideration of environmental factors is relatively simple, and the influence of aging population and old urban areas is relatively ignored. A large number of people in the Huaihe River Basin in Central China died of chronic diseases caused by the environment many years ago [27]. The urban environmental pollution is relatively serious now, seriously endangering the physical and mental health of residents. In view of this, the distribution characteristics of CVD deaths were analyzed, and the influences of multiple environmental factors on CVD were systematically investigated in this study with the old urban area in Bengbu City of Huaihe River Basin as the subject, to reduce CVD mortality by proper urban planning and policies, and provide certain research ideas for healthy city construction in other areas of Huaihe River Basin.
2. Materials and Methods
2.1. Study Area
Bengbu City, located in the south of Huaihe River Basin, China, is characterized by high population density and rapid urbanization [28]. Bengbu was an important industrial city and traffic hub in China before, where a large number of chemical, pharmaceutical, and building materials enterprises and the heavy traffic pressure have produced a large amount of pollution in Bengbu, seriously affecting the physical and mental health of residents. A certain district is located in the Western old urban area of Bengbu City, adjacent to the commercial and cultural center of the city in the east and the Huaihe River (one of the seven major rivers in China) in the north, and it is also the administrative area with the largest population in Bengbu City, so it is suitable for the research on urban environment and population health. The study area consisted of 12 blocks numbered YH01-YH12 in a certain district, which were divided into 2,744 spatial units by 100 m grid (Figure 1). The study area is located in the mid-latitude region, where northeasterly wind is the most prevalent throughout the year, the average temperature in January is 1°C, and it is susceptible to cold waves in winter.
Figure 1.
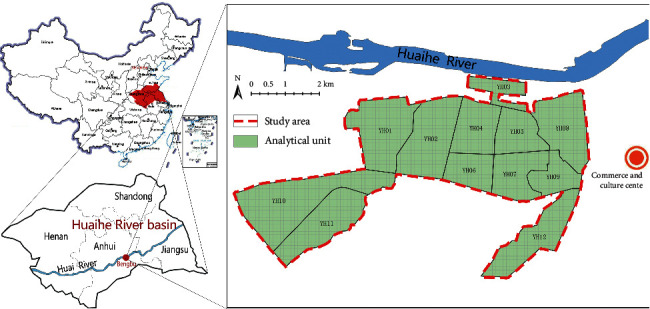
Area bitmap.
2.2. Data Sources
2.2.1. Sources of Data Related to CVD
The data of cardiovascular disease (CVD) mortality were collected from the population whose cause of death was cardiovascular disease (ICD-10 code I00-I99) determined by Bengbu Health Commission in 2019, including detailed address, age, gender, and occupation before death. Inpatients whose home addresses and affiliations were not within the study area were excluded, so the final number was 469 in total. The number of resident population in a certain district in 2019 was derived from the official bulletin of Bengbu National Bureau of Statistics.
2.2.2. Environmental Data Sources
The land use data and built environment data in environmental data were obtained from the Anhui Urban & Rural Planning and Design Institute, and the data contained the main uses of each land in a certain district in 2019, as shown in Figure 2(a), which included roads, green space and river, residential land, industrial land according to urban land classification, and the base area and floor number of each building. Commercial and bus stops are derived from open-source point-of-interest (POI) data, which are characterized by large sample size, wide coverage, and detailed spatial resolution, making spatial analysis more comprehensive, objective, and in-depth, as shown in Figure 2(b). Data of environmental pollution indexes were obtained from the Bengbu Bureau of Ecology and Environment, and the pollution values of each spatial unit were obtained by the interpolation method for the pollution monitoring point data. Data of land surface temperature and vegetation coverage were derived from Landsat 8 remote sensing data in January 2019 provided by USGS and coded LC81210372019023LGN00.
Figure 2.
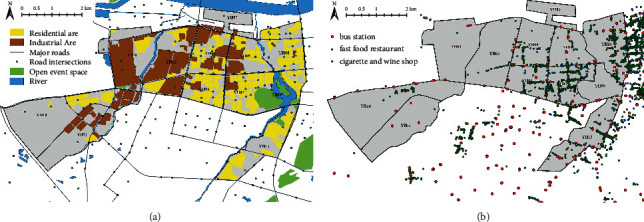
Present distribution.
2.3. Influencing Factor Index System
To explore the distribution characteristics of cardiovascular disease (CVD) and environmental influencing factors in urban residents, the basic characteristics and spatial distribution characteristics of CVD deaths were analyzed, and the correlation between various environmental influencing factors and CVD mortality was explored (Figure 3). Environmental influencing factors included land use, road traffic, spatial form, and natural environment, with their potential impacts on CVD shown in Table 1. The calculation formula for CVD mortality is as follows:
| (1) |
where Nc is the number of deaths due to CVD in a unit and Np is the total population in a unit.
Figure 3.
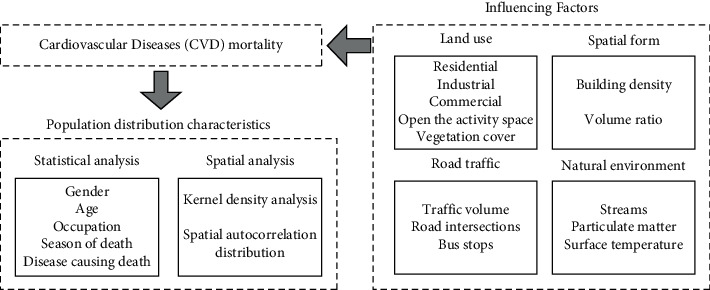
Conceptual framework.
Table 1.
Environmental influencing factors.
| Category | Subcategory | Variable | Unit | Definition | Potential impact of hypothesis |
|---|---|---|---|---|---|
| Land use | Live | Residential density | % | Living area/total land area | Cause pollution and physical and mental stress |
| Industry | Distance from the nearest industry | m | Distance from the nearest industry | The closer you are to industry, the more pollution you get | |
| Business | Fast-food restaurant density | Pcs/ha | Number of fast-food restaurants in 500 m buffer zone/buffer zone area | Intake relatively high salt and oil | |
| Tobacco and liquor shop density | Pcs/ha | Number of tobacco and liquor stores in 500 m buffer zone/buffer zone area | Increase the risk of alcohol and smoking | ||
| Open the activity space | Distance from the nearest open space | m | Distance from the nearest open space | It is more convenient to exercise and relax | |
| Vegetation cover | Normalized difference vegetation index (NDVI) | — | NDVI in 2019 | Vegetation coverage can reduce air pollution, increase green vision rate, and delight body and mind | |
| Road transport | Traffic | Road network density | m/ha | Road length/total land area | Increase air and noise pollution |
| Road intersection | Road intersection density | Pcs/ha | Number of road intersections in 500 m buffer zone/buffer zone area | More air and noise pollution | |
| Bus stop | Bus stop density | Pcs/ha | Number of bus stops in 500 m buffer zone/buffer zone area | It is more convenient to travel and increase the amount of activities | |
| Spatial form | Building density | Building coverage | % | Total area of building basement/total area of land | High density reduces the wind speed, which increases the concentration of air pollutants and makes people depressed |
| Volume fraction | Volume fraction | — | Total construction area/total land area | High density reduces the wind speed, which increases the concentration of air pollutants and makes people depressed | |
| Natural environment | River | Distance from the nearest river | m | Distance from the nearest river | Adsorption of air particles by water body |
| Particulate matter (PM) | Mean PM2.5 | Ug/m3 | Average PM2.5 in 2019 | Increase air pollution | |
| Mean PM10 | Ug/m3 | Average PM10 in 2019 | Increase air pollution | ||
| (Ground) surface temperature | Mean surface temperature | °C | Surface temperature in January 2019 | Cold winter temperatures increase the risk of death |
2.4. Study Methods
2.4.1. Spatial Autocorrelation Assessment
Global spatial autocorrelation [29] is usually measured by Moran's I, and the aggregation of subregional geospatial CVD deaths is judged according to the spatial distribution pattern of the whole region. Moran's I range is [−1, 1], and the larger value indicates the more obvious spatial correlation, and the smaller value indicates the greater spatial difference, with the specific calculation formula as follows:
| (2) |
where n is the number of study units; xi and xj represent the CVD mortality in area i and area j, respectively. ‾x represents the average CVD mortality; Wij represents the spatial weight matrix.
Local spatial autocorrelation [30] can reveal the heterogeneity of local space, make up for the atypical characteristics of local areas in the whole region, and fully reflect the variation trend of local geospatial epidemic risk. The spatial difference in CVD mortality was measured by local indicators of spatial association (LISA) in this study, with the calculation formula shown as follows:
| (3) |
where zi and zj represent the standardized values of CVD mortality in area i and area j, respectively. Wij represents the spatial weight matrix. In the LISA of local spatial autocorrelation, CVD mortality can be divided into four categories: high-high clustering (H-H), high-value clustering; low-low clustering (L-L), low-value clustering; high-low clustering (H-L), outliers with high values mainly surrounded by low values; and low-high clustering (L-H), outliers with low values mainly surrounded by high values.
2.4.2. Spearman's Rank Correlation
To investigate the relationship between CVD and environmental factors, the correlation between the mortality rate of CVD (dependent variable) and the values of various environmental factors (independent variables) was comprehensively measured by Spearman's rank correlation [31], with the specific formula referred to formula (3). Compared with Pearson's correlation, Spearman's rank correlation can make up for the fact that the correlation of environmental factor values may not be linear and are interfered with detection error and other factors, thus making the correlation more significant [32]. CVD mortality and environmental factor values were subject to normalized processing (value range of [0, 1]), which was used to balance the dimensional gap of data and enable different data to be counted under the same conditions.
| (4) |
where ρ is Spearman's correlation coefficient, with the value range of [−1, 1], and the larger absolute value indicates the stronger correlation. n represents the number of areas of CVD mortality, and di represents the rank difference between dependent variable (CVD mortality) and independent variable (environmental influencing factor values).
3. Results
3.1. Basic Characteristics of CVD Deaths
A total of 469 people died of cardiovascular disease (CVD) in the study area in 2019 according to the statistics of collected death data, with the basic characteristics of death population, such as gender, age, occupation, death season, and specific diseases leading to death, shown in Table 2.
Table 2.
Statistics of CVD death population.
| Category | Classify | Death toll | Proportion of deaths (%) |
|---|---|---|---|
| Gender | Man | 254 | 54.16 |
| Woman | 215 | 45.84 | |
| Age | ≥80 years old | 254 | 54.15 |
| 70–79 years old | 109 | 23.24 | |
| 60–69 years | 58 | 12.37 | |
| <60 years old | 48 | 10.23 | |
| Occupation | Unemployed | 122 | 26.01 |
| Worker | 31 | 6.61 | |
| Individual operator | 26 | 5.54 | |
| Farmer | 12 | 2.56 | |
| Other | 278 | 59.27 | |
| Dead season | Spring (March–May) | 110 | 23.45 |
| Summer (June–August) | 98 | 20.90 | |
| Autumn (September–November) | 130 | 27.72 | |
| Winter (December–February of the following year) | 131 | 27.93 | |
| Specific diseases leading to death | Cerebral infarction | 113 | 24.09 |
| Cardiac infarction | 92 | 19.62 | |
| Coronary heart disease | 83 | 17.70 | |
| Encephalorrhagia | 55 | 11.73 | |
| Pulmonary heart disease | 43 | 9.17 | |
| Other | 83 | 17.70 |
The analysis results showed that the mortality among male CVD patients was significantly higher than female patients, with a ratio of about 1.18 : 1. The elderly over 80 years accounted for 54.15% of CVD deaths, and those under 60 years only accounted for about 10%, indicating that the higher the age, the higher the mortality. Winter (December to February of the following year) and autumn (September to November) were the most frequent periods of CVD deaths, accounting for 27.93% and 27.72% of the total number of deaths, respectively, and the mortality in autumn and winter was 1.25 times higher than that in spring and summer. The largest number of CVD deaths was among the unemployed (26.01%), followed by workers (6.61%), freelancers (5.54%), and farmers (2.56%). Among the specific diseases causing death, cerebral infarction and myocardial infarction accounted for 24.09% and 19.62%, followed by coronary heart disease (17.70%).
3.2. Spatial Distribution of CVD Deaths
In 2019, there was a significant difference in the number of CVD deaths among different units in the study area. YH07 and YH08 accounted for 73.56% in terms of deaths, of which YH08 had the largest number of CVD deaths, namely 180, followed by 165 deaths in YH07 and no deaths in YH10 and YH11. The kernel density analysis of CVD deaths was conducted with ArcGIS software (Figure 4), and unit density of CVD deaths in the study area could be calculated, which could intuitively reflect the distribution of CVD deaths in a continuous area [33]. The analysis results suggested that CVD deaths were mainly distributed in the vicinity of Unit YH09 in Zhanggongshan Park and the north of Unit YH08 near the Huaihe River. The area near YH09 was an old urban area of Bengbu, characterized by high population density and serious aging. A total of 365 people died within the 1 km buffer zone of Zhanggongshan Park, accounting for 77.82% of the total deaths; moreover, the density of deaths was lower in the area farther away from Zhanggongshan Park. The north of YH08 is also a large population gathering area, close to the central city of Bengbu and Huaihe River in the east.
Figure 4.
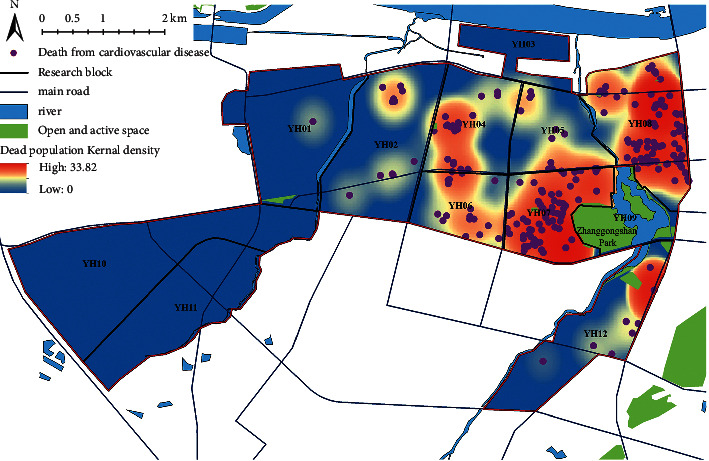
Distribution map of CVD death population.
Among 2,744 study units, 1,053 units containing residential land (i.e., unit population greater than 0) were taken as the research samples after the outlier samples were excluded. The normalized mean value of the calculated CVD mortality values of all study units was normalized to be 0.008, with the standard deviation of 0.055, indicating that there were significant spatial differences in the CVD mortality. Global Moran's I index analysis showed that the spatial distribution of normalized mortality index was of spatial autocorrelation (Moran's I > 0, Z = 2.192, P < 0.05), indicating that there was a significant spatial aggregation phenomenon in the distribution of CVD deaths. In addition, there was a local spatial autocorrelation in the normalized mortality index according to the spatial distribution of LISA clustering (Figure 5), in which H-H clustering (22) was mainly distributed in the middle of YH08, forming a significant H-H clustering of CVD mortality. L-L clusters (121) were mainly distributed in YH05, YH10, and YH12, with a few scattered clusters in other units, showing more L-L clusters in the CVD mortality.
Figure 5.
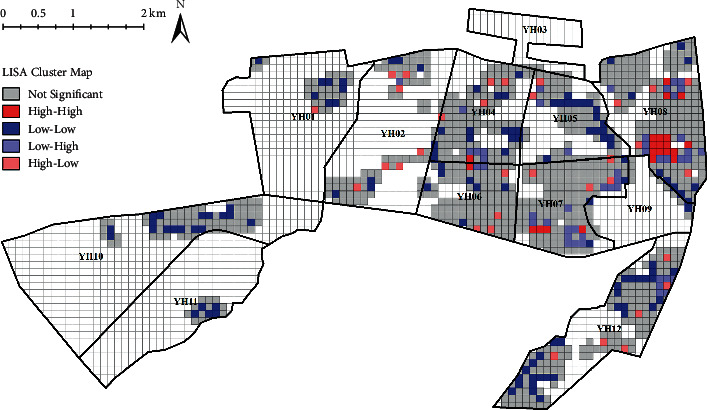
Spatial autocorrelation distribution of CVD normalized mortality index.
3.3. Relationship between Environmental Factors and CVD Mortality
The results of Spearman's rank correlation analysis are shown in Table 3. Among land use, road traffic, spatial form, and natural environment, there are 14 environmental factors showing significant correlation and statistical significance with CVD mortality (P < 0.05). There was no correlation between industry and CVD mortality (P > 0.05). The spatial distribution of environmental influencing factors is shown in Figure 6.
Table 3.
Correlation between environmental factors and CVD mortality.
| Category | Subcategory | Variable | Ρ (correlation coefficient) | P value (double side) |
|---|---|---|---|---|
| Land use | Live | Residential density | 0.127∗ | 0.000 |
| Business | Density of fast-food restaurants in 500 m buffer zone | 0.287∗∗ | 0.000 | |
| Density of tobacco and liquor stores in 500 m buffer zone | 0.286∗∗ | 0.000 | ||
| Industry | Distance from the nearest industry | -0.011 | 0.717 | |
| Open the activity space | Distance from the nearest open space | −0.189∗∗ | 0.000 | |
| Vegetation cover | Normalized difference vegetation index (NDVI) | −0.179∗∗ | 0.000 | |
| Road transport | Traffic | Road network density | 0.138∗∗ | 0.000 |
| Road intersection density in 500 m buffer zone | 0.220∗∗ | 0.000 | ||
| Bus stop | Density of bus stops in 500 m buffer zone | 0.238∗∗ | 0.000 | |
| Spatial form | Building density | Building coverage | 0.104∗∗ | 0.001 |
| Volume fraction | Volume fraction | 0.115∗∗ | 0.000 | |
| Natural environment | River | Distance from the nearest river | 0.121∗∗ | 0.000 |
| Particulate matter (pm) | Average annual pm2.5 | 0.088∗∗ | 0.004 | |
| Average annual pm10 | 0.072∗ | 0.020 | ||
| (Ground) surface temperature | Surface temperature in January 2019 | −0.135∗ | 0.000 |
∗ P < 0.05, ∗∗P < 0.01.
Figure 6.
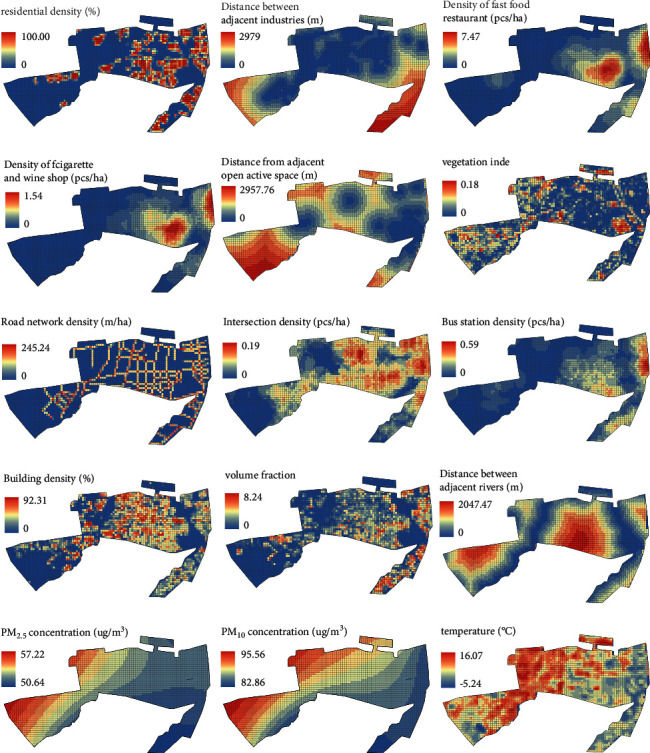
Spatial distribution of environmental influencing factors.
3.3.1. Land Use
The model showed that the residential density was positively correlated with the CVD mortality (ρ = 0.127), indicating that the higher the residential density, the higher the CVD mortality. The density of fast-food restaurants and the density of cigarette and wine shops showed a significant positive correlation with the CVD mortality in the 500 m buffer zone (ρ = 0.287, ρ = 0.286), indicating that the higher the density of fast-food restaurants and cigarette and wine shops, the higher the mortality. There was a significant negative correlation between the nearest distance to the open space and the CVD mortality (ρ = −0.189), indicating that the farther from the park, the lower the CVD mortality. The normalized difference vegetation index (NDVI) in January showed a significant negative correlation with CVD mortality (ρ = −0.179), indicating that the higher the vegetation coverage, the lower the CVD mortality.
3.3.2. Road Traffic
The model showed that the road network density and the intersections within the 500 m buffer zone were significantly positively correlated with the CVD mortality (ρ = 0.138, ρ = 0.220), indicating that the greater the traffic volume, the higher the CVD mortality. Meanwhile, there was a significant positive correlation between the density of bus stops and the CVD mortality within the 500 m buffer zone (ρ = 0.238), indicating that there was a lower risk of death among the people living in the area with sparse bus stops.
3.3.3. Spatial Form
The model showed that building density and floor area ratio were significantly positively correlated with CVD mortality, with the correlation coefficients of 0.104 and 0.115, indicating that high-density space would increase the CVD mortality.
3.3.4. Natural Environment
There was a significant positive correlation between the distance to the nearest river and the CVD mortality (ρ = 0.121), indicating that the closer to the river, the lower the CVD mortality. The average annual PM2.5 and PM10 were significantly positively correlated with the CVD mortality, with the correlation coefficients of 0.088 and 0.072, indicating that the higher the average annual particulate matter (PM) concentration, the higher the CVD mortality. The average temperature was negatively correlated with the CVD mortality, with a correlation coefficient of -0.135, indicating that the lower the temperature in winter would contribute to the increase in the CVD mortality.
4. Discussion
The characteristics of CVD deaths were significant and of spatial clustering.
Consistent with the conclusions of previous international statistical studies, the CVD deaths were characterized as follows: male deaths were more than females; the mortality is higher in those of higher age; most of them are unemployed; and cardiocerebral infarction was the main cause of death. In addition, the deaths were mainly distributed in the old urban area, and there was a significant spatial clustering phenomenon [34]. Previous studies have shown that alcohol abuse [35] and smoking [36] can affect the cardiovascular system, and males are more likely to do alcohol abuse and smoking than females, causing the difference in mortality. The risk of cardiac arteriosclerosis will increase with age; that is, the mortality is higher in those of higher age [37]. Working can reduce the risk of CVD [8], and the risk of CVD is lower in residents engaged in manual work, but higher in those unemployed. Low temperature and sudden drop in air temperature will cause vasoconstriction and elevated blood pressure of human body, increasing the risk of sudden myocardial infarction [23, 24]; therefore, autumn and winter are the seasons of high incidence of CVD, and the mortality is higher in the urban areas with lower urban temperature [38].
The higher density of restaurants and cigarette and wine shops will increase the CVD mortality.
It has been further confirmed in this study that the density of restaurants and smoking restaurants around the residential area showed a significant positive correlation with the CVD mortality. The daily activity distance that can meet the basic material and life needs of residents by 10-min walking is 500 m [39]. Handy et al. [40] found that the frequency of walking to businesses was positively correlated with the number of businesses within the service radius; therefore, people in the areas with highly dense restaurants and cigarette and wine shop will have higher probability of dining out and buying cigarettes and wines. In the study area, located in northern Anhui, the restaurant diet contains high fat and salt, and the dense dining facilities will bring more cooking fumes, sewage, and other environmental pollution, in which a lot of fat and cholesterol oxide [17]will lead to hypertension, hyperlipidemia, and other metabolic disorder CVD, and the increased probability of buying alcohol and tobacco will raise the risk of alcoholism, thereby causing sudden death [17].
The influence of environmental factors related to particulate matter concentration on the CVD mortality.
Consistent with the conclusion of previous studies abroad, long-term exposure to high levels of pollutants will affect the human circulatory system [41], thereby inducing CVD mortality. According to the data of disease burden from Barcelona, Spain, it was estimated that 849 cases of CVD could be prevented each year if the exposure level of air pollution could be reduced to the WHO recommended level [42]. There is a higher risk of death for residents in areas with high concentrations of particulate matter. The finding is further confirmed in this study: the increased traffic volume [43], dense bus stops [44], and dense residential and spatial forms [45, 46], low green space coverage [47], and longer distance from rivers [47] can increase the CVD mortality, of which the possible reason may be associated with the increased concentration of local particulate matter and other noise pollution and psychological harm.
Discussion on the correlation between industrial and open activity space and CVD mortality.
Different from general studies, it is found that there is no significant relationship between CVD mortality and industry in this study, for which reason may lie in that northeasterly wind is the most prevalent in the study area throughout the year, and there are few residential areas located downwind of industry, only accounting for less than 10% of the study units; therefore, the influence of industry on the study unit is not significant. Meanwhile, this study also reveals that CVD mortality is lower in the areas farther from open space area, and the possible reason is that the study area is an old urban area that lacks green space, there are only 3 parks with the area of more than 1 ha within or 500 m from the study area (aggregated distribution), and there is relatively little activity space, which also is the common fault of an old urban area. The elderly are at high risk of dying from CVD, and they will deliberately choose the area around the open activity space when choosing housing, which will have a certain impact on the conclusion.
5. Conclusions and Prospects
To explore the distribution characteristics of cardiovascular disease (CVD) in urban residents and the environmental influencing factors, this study analyzed the basic characteristics and spatial distribution characteristics of CVD death population, explored the correlation between multiple environmental factors and CVD mortality, and revealed the factors affecting the risk of death and its mechanism, with the main conclusions as follows:
The correlation study conducted in this study is of good scientific nature and research significance, and the conclusions are consistent with international studies. Therefore, the study methods can provide some research ideas for the construction of healthy cities in the Huaihe River Basin or other regions.
With obvious characteristics, CVD deaths are mainly distributed in the vicinity of Unit YH09 in Zhanggongshan Park and the north of Unit YH08 near the Huaihe River. Therefore, attention should be paid to the key areas with the maximum number of CVD deaths and the population at high risk, and medical input should be increased to reduce the death risk.
Because long-term exposure to high pollutants in the environment will cause CVD death, the following measures can be taken to reduce the CVD mortality in the construction of healthy cities in the future: increase traffic arterial roads around residential areas to reduce the traffic volume and vehicle exhaust emissions in residential areas; increase open space to reduce living and spatial density; plant more plants and building more rivers to reduce the local air pollution; and make dispersed layout of commercial facilities, such as restaurants and cigarette and wine shops, around residential areas to effectively reduce the risk of CVD death. Meanwhile, attention should also be paid to the influence of the areas with a higher density of the elderly on the analysis results.
Appropriate urban planning and policies can improve the active health interventions in cities and reduce the CVD mortality. To a certain extent, it can also provide more research perspectives for the construction of healthy cities in the future, and promote the development of healthy cities. In addition, this study is based on panel data, and little consideration is given to the changes of built environment and CVD mortality caused by time changes, so time series related research will be carried out in the future. At the same time, different lifestyles will affect CVD mortality, so further research on the correlation between residents' lifestyles and CVD mortality will be conducted in the future.
Acknowledgments
This research was funded by Natural Science Foundation of Anhui Province with grant reference no. 2008085ME160.
Data Availability
The datasets used during this study are available from the corresponding author on reasonable request.
Disclosure
An earlier version of this work was presented as an abstract at 57th ISOCARP World Planning Congress, 2021.
Conflicts of Interest
The authors declared that they have no conflicts of interest in this work.
References
- 1.Beltránsánchez H., Soneji S., Crimmins E. M. Past, present, and future of healthy life expectancy. cold spring harbor perspectives in medicine . 2015;5(11) doi: 10.1101/cshperspect.a025957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kyu H. H. A., Abate D., Abay K. H., et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet . 2018;392:1859–1922. doi: 10.1016/S0140-6736(18)32335-3.10159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jiaying Zhao S. S. A. S. Timing of urbanisation and cardiovascular risks in Thailand: evidence from 51 936 members of the Thai cohort study, 2005–2009. Journal of Epidemiology . 2014;24(6):484–493. doi: 10.2188/jea.je20140063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rani S., Anthony W. Current levels of salt knowledge: a review of the literature. Nutrients . 2014;6(12):5534–5559. doi: 10.3390/nu6125534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Xu Y., Wang F. Built environment and obesity by urbanicity in the US. Health & Place . 2015;34:19–29. doi: 10.1016/j.healthplace.2015.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barnett D. W., Barnett A., Nathan A., Cauwenberg J. V., Barnett A., au fnm Built environmental correlates of older adults’ total physical activity and walking: a systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity . 2017;14 doi: 10.1186/s12966-017-0558-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Stevenson M., Thompson J., De S. á., et al. Land use, transport, and population health: estimating the health benefits of compact cities. Lancet . 2016;388:2925–2935. doi: 10.1016/s0140-6736(16)30067-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ewing R., Meakins G., Hamidi S., Nelson A. C. Relationship between urban sprawl and physical activity, obesity, and morbidity – update and refinement. Health & Place . 2014;26:118–126. doi: 10.1016/j.healthplace.2013.12.008. [DOI] [PubMed] [Google Scholar]
- 9.Ballester F., Tenias J., Perez-Hoyos M. Air pollution and emergency hospital admissions for cardiovascular diseases in Valencia, Spain. Journal of Epidemiology & Community Health . 2001;55:57–65. doi: 10.1136/jech.55.1.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Guo Y., Teixeira J. P., Ryti N. Ambient particulate air pollution and daily mortality in 652 cities. New England Journal of Medicine . 2019;381(8):705–715. doi: 10.1056/NEJMoa1817364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Héroux M. E., Anderson H. R., Atkinson R., Brunekreef B., Walton H. Quantifying the health impacts of ambient air pollutants: recommendations of a WHO/Europe project. International Journal of Public Health . 2015;60(5) doi: 10.1007/s00038-015-0690-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Oh M., Shin K., Kim K., Shin J. Influence of noise exposure on cardiocerebrovascular disease in Korea. The Science of the Total Environment . 2018;651:1867–1876. doi: 10.1016/j.scitotenv.2018.10.081. [DOI] [PubMed] [Google Scholar]
- 13.Brook R. D., Rajagopalan S., Pope C. A., Brook J. R., Kaufman J. D. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation . 2010;121(21):2331–2378. doi: 10.1161/cir.0b013e3181dbece1. [DOI] [PubMed] [Google Scholar]
- 14.Hong-han C., Hong-wei C., Jiang-tao H. F., Zhao-li L., Bing S., Jing S. Health-based risk assessment of contaminated sites:Principles and methods. Earth Science Frontiers . 2006;13(001):216–223. [Google Scholar]
- 15.Lan W., Xiji J., Wenyao S., Xiaojing Z., Jian T. Impact of urban built environment on respiratory health and its planning strategy: a case study of a district in shanghai. China City Planning Review . 2018;42(06):15–22. [Google Scholar]
- 16.Mehraj S. S., Bhat G. A., Balkhi H. M., Gul T. Health Risks for Population Living in the Neighborhood of a Cement Factory. Academic Journals . 2013;7(12):1044–1052. [Google Scholar]
- 17.Fei-hong T. D. K. Y. Analysis on oil fume particles in catering industry cooking emission. Environmental science . 2012;33(006):1958–1963. [PubMed] [Google Scholar]
- 18.Malambo P., Kengne A. P., De Villiers A., Lambert E. V., Puoane T. Built environment, selected risk factors and major cardiovascular disease outcomes: a systematic review. PLoS One . 2017;11(11) doi: 10.1371/journal.pone.0166846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Babisch W. Road traffic noise and cardiovascular risk. Noise and Health . 2008;10(38):27–33. doi: 10.4103/1463-1741.39005. [DOI] [PubMed] [Google Scholar]
- 20.Douglas W. D. Epidemiologic evidence of cardiovascular effects of particulate air pollution. Environmental Health Perspectives . 2001;109:483–486. doi: 10.1289/ehp.01109s4483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Furuuchi M., Murase T., Yamashita M., et al. Temperature distribution and air pollution in phnom penh, Cambodia-influence of land use and the mekong and tonle sap rivers. Aerosol and Air Quality Research . 2006;6(2):134–149. doi: 10.4209/aaqr.2006.06.0003. [DOI] [Google Scholar]
- 22.Valdés S., Araque C. M., Torres F. G., et al. Ambient temperature and prevalence of obesity in the Spanish population: the D i@bet.es study. Obesity . 2014;22(11) doi: 10.1002/oby.20866. [DOI] [PubMed] [Google Scholar]
- 23.Bhaskaran K., Hajat S., Haines A., Herrett E., Wilkinson P., Smeeth L. Short term effects of temperature on risk of myocardial infarction in England and Wales: daily time series regression analysis of the Myocardial Ischaemia National Audit Project (MINAP) registry. BMJ British Medical Journal . 2010;341(7768) doi: 10.1136/bmj.c3823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patz J. A., Campbell-Lendrum D., Holloway T., Foley J. A. Impact of regional climate change on human health. Nature 438: 310-317 (17 november) Nature . 2005;438(7066):310–317. doi: 10.1038/nature04188. [DOI] [PubMed] [Google Scholar]
- 25.Xu Y., Wang L. GIS-based analysis of obesity and the built environment in the US. Cartography and Geographic Information Science . 2015;42(1):9–21. doi: 10.1080/15230406.2014.965748. [DOI] [Google Scholar]
- 26.GriffithsC H. M., Jordan G. M. A., Saunders H. Neighbourhood typologies and associations with body mass index and obesity: a cross-sectional study. Preventive Medicine: An International Journal Devoted to Practice and Theory . 2018;111:351–357. doi: 10.1016/j.ypmed.2017.11.024. [DOI] [PubMed] [Google Scholar]
- 27.Zhang P., Lee J., Kang G., et al. Disparity of nitrate and nitrite in vivo in cancer villages as compared to other areas in Huai River Basin, China. The Science of the Total Environment . 2018;612:966–974. doi: 10.1016/j.scitotenv.2017.08.245. [DOI] [PubMed] [Google Scholar]
- 28.Juna Y. Research on the spatial pattern of population destribution in the Huaihe River basin. Journal of Xinyang Normal University . 2014;30(1):525–528. [Google Scholar]
- 29.Hwang T. W., Wang F. B. Dynamics OF a dengue fever transmission model with crowding effect IN human population and spatial variation. Discrete and Continuous Dynamical Systems - Series B . 2013;1(1):147–161. doi: 10.3934/dcdsb.2013.18.147. [DOI] [Google Scholar]
- 30.Varga C., Pearl D. L., Mcewen S. A., Sargeant J. M., Pollari F., Guerin M. T. Area-level global and local clustering of human Salmonella Enteritidis infection rates in the city of Toronto, Canada, 2007–2009. BMC Infectious Diseases . 2015;15(1):p. 359. doi: 10.1186/s12879-015-1106-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Colditz G. A., Willett W. C., Stampfer M. J., et al. The influence of age, relative weight, smoking, and alcohol intake on the reproducibility of a dietary questionnaire. International Journal of Epidemiology . 1987:p. 392. doi: 10.1093/ije/16.3.392. [DOI] [PubMed] [Google Scholar]
- 32.Xiaoyanl W., Meizhou L. The relationship of rank correlation coefficient and spearman rank correlation coefficient. Journal of Guangdong Industry Technical Colleg . 2006;5(004):26–27. [Google Scholar]
- 33.Khosrow D. Density estimation for statistics and data analysis. Technometrics . 2012;29(4):p. 495. [Google Scholar]
- 34.Liu Jie C. T. Y. Y. Exploratory spatial data analysis of patients with acute myocardial infarction from 2007 to 2014 year in Yangpu District, Shanghai. Chin J Evid Based Cardiovasc Med . 2016;8(4):464–467. [Google Scholar]
- 35.Ning X. H., Cuan W. A. C., Hong G. Further research into relationship between alcohol consumption and plasma homocysteine. Adv Cardiovasc Dis . 2010;31(03):445–448. [Google Scholar]
- 36.Qian S., Nanbo Z., Canqing Y., Yu G., Zheng B., Chen Zhengming L. J. Sex-specific associations between tobacco smoking and risk of cardiovascular diseases in Chinese adult. Chinese Journal of Epidemiology . 2018;39(001):8–15. doi: 10.3760/cma.j.issn.0254-6450.2018.01.002. [DOI] [PubMed] [Google Scholar]
- 37.Liu L., Wang J. G., Gong L., Liu G., Staessen J. A. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension: Systolic Hypertension in China (Syst-China) Collaborative Group. Journal of Hypertension . 1998;16(12):p. 1823. doi: 10.1097/00004872-199816120-00016. [DOI] [PubMed] [Google Scholar]
- 38.Liu Xue-en L. Q. Z. Z. Influence of temperature and cold air on mortality of cardio -and cerebral vascular diseases. CHINA PUBLIC HE ALTH . 2002;18(8) [Google Scholar]
- 39.Meng L. The planning strategies of a 15- minute community life circle based on behaviors of residents. Urban Planning Forum01) . 2017;1:111–118. [Google Scholar]
- 40.Handy S., Cao X., Mokhtarian P. L. Self-selection in the relationship between the built environment and walking: empirical evidence from northern California. Journal of the American Planning Association . 2006;72(1):55–74. doi: 10.1080/01944360608976724. [DOI] [Google Scholar]
- 41.Chuan D. F. M. M. Association between ambient PM 10/PM 2.5 levels and population mortality of circulatory diseases:a case-crossover study in Beijing. Journal of Peking University . 2013;45(03):398–404. [PubMed] [Google Scholar]
- 42.Mueller N., Rojas-Rueda D., Basagaa X., et al. Health impacts related to urban and transport planning: a burden of disease assessment. Environment International . 2017;107:243–257. doi: 10.1016/j.envint.2017.07.020. [DOI] [PubMed] [Google Scholar]
- 43.Sinharay R., Gong J., Barratt B., et al. Respiratory and cardiovascular responses to walking down a traffic-polluted road compared with walking in a traffic-free area in participants aged 60 years and older with chronic lung or heart disease and age-matched healthy controls: a randomised, crossov. Lancet (London, England) . 2020;391:339–349. doi: 10.1016/S0140-6736(17)32643-0.10118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Zhao L., Wang X., He Q., et al. Exposure to hazardous volatile organic compounds, PM10 and CO while walking along streets in urban Guangzhou, China. Atmospheric Environment . 2004;38(36):6177–6184. doi: 10.1016/j.atmosenv.2004.07.025. [DOI] [Google Scholar]
- 45.Schweitzer L., Zhou J. Neighborhood air quality, respiratory health, and vulnerable populations in compact and sprawled regions. Journal of the American Planning Association . 2010;76(3):363–371. doi: 10.1080/01944363.2010.486623. [DOI] [Google Scholar]
- 46.Tong B., Lijian H., Liang H., et al. Impact of urban air pollution on surrounding areas in Beijing,Tianjin,and Hebei Provinces. Acta Ecologica Sinica . 2018;038(012):4268–4275. [Google Scholar]
- 47.Wang D., Lau K. L., Yu R., Wong S., Kwok T., Woo J. Neighbouring green space and mortality in community-dwelling elderly Hong Kong Chinese: a cohort study. BMJ Open . 2017;7(7) doi: 10.1136/bmjopen-2016-015794. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used during this study are available from the corresponding author on reasonable request.