

Abstract
PURPOSE
Previous work has shown that asthma-related emergency department (ED) use is greatest among Black and Latine populations, but it is unknown whether health care use for exacerbations differs across settings (outpatient, ED, inpatient) and correlates with use of routine outpatient services. We aimed to measure disparities by race, ethnicity, and language in pediatric acute asthma care using data from US primary care community health centers.
METHODS
In an observational study using electronic health records from community health centers in 18 states, we compared non-Hispanic Black, English-preferring Latine, Spanish-preferring Latine, and non-Hispanic White children aged 3 to 17 years on visits for clinic-coded asthma exacerbations (2012-2018). We further evaluated asthma-related ED use and inpatient admissions in a subsample of Oregon-Medicaid recipients. Covariate-adjusted odds ratios (ORs) and rate ratios (RRs) were derived using logistic or negative binomial regression analysis with generalized estimating equations.
RESULTS
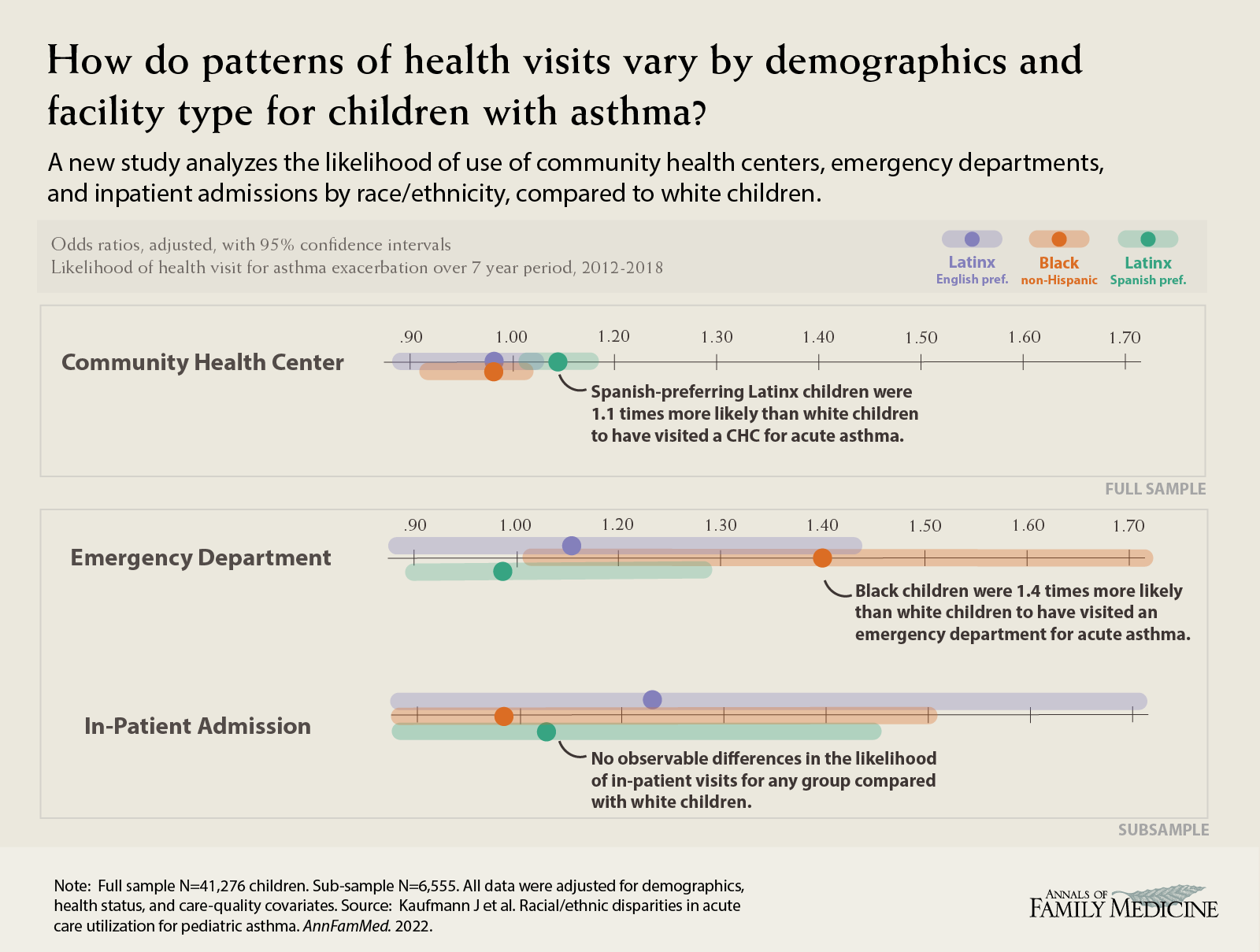
Among 41,276 children with asthma, Spanish-preferring Latine children had higher odds of clinic visits for asthma exacerbation than non-Hispanic White peers (OR = 1.10; 95% CI, 1.02-1.18). Among the subsample of 6,555 children insured under Oregon-Medicaid, non-Hispanic Black children had higher odds and rates of asthma-related ED use than non-Hispanic White peers (OR = 1.40; 95% CI, 1.04-1.89 and RR = 1.49; 95% CI, 1.09-2.04, respectively). We observed no differences between groups in asthma-related inpatient admissions.
CONCLUSIONS
This study is the first to show that patterns of clinic and ED acute-care use differ for non-Hispanic Black and Spanish-preferring Latine children when compared with non-Hispanic White peers. Non-Hispanic Black children had lower use of clinics, whereas Spanish-preferring Latine children had higher use, including for acute exacerbations. These patterns of clinic use were accompanied by higher ED use among Black children. Ensuring adequate care in clinics may be important in mitigating disparities in asthma outcomes.
Key words: asthma; community health center; health care utilization; pediatric asthma; racial/ethnic disparities; health disparity, minority and vulnerable populations; primary care; practice-based research; child health
INTRODUCTION
The prevalence of pediatric asthma in the United States remained relatively stable during 2001-2017, at about 8.5%,1 and national surveys suggest roughly 45% of children with asthma experience exacerbations in a given year.2 Asthma attacks increase a child’s risk of needing to seek emergency treatment and can place time and financial strains on the family, especially when income, insurance, flexible work schedules, and other resources are lacking.3,4 Emergency department (ED) visits and inpatient admissions may pose even greater financial burden5 and often include unnecessary chest imaging and antibiotic prescription.6
Patient-reported surveys suggest asthma-related visits may not be equally distributed across racial and ethnic populations: rates of asthma-related ED visits and inpatient admissions may be greatest for Black and Latine populations, especially among children, low-income households, and Medicaid recipients.4,7–10 Recently, prospective cohort studies have shown that such disparities are reduced when environmental and socioeconomic factors are taken into account.11,12 These studies, however, relied on patient self-reporting of health care use, which may lead to recall bias and/or selection bias due to participant recruitment. Importantly, there are few data on the association of race, ethnicity, and language with acute asthma care use across clinics, EDs, and inpatient settings over time that also consider health status, social determinants of health, and routine primary care.
To address this gap, we conducted an observational multistate study of objectively measured acute asthma care among pediatric patients seen at community health centers (CHCs) with a shared electronic health record platform. We used 2 data sources (electronic health records, which capture ambulatory visits, and Medicaid claims data, which capture hospital-based care) to ascertain episodes of acute asthma care. We investigated racial, ethnic, and language disparities in acute visits for asthma during 2012-2018 across settings. We compared clinic use for acute asthma management and asthma-related ED use and inpatient admissions among non-Hispanic Black, English-preferring Latine, Spanish-preferring Latine, and non-Hispanic White children. We hypothesized that Latine and Black children would have similar rates of asthma exacerbation visits compared with White counterparts in the CHC clinic setting and the hospital setting after accounting for important social determinants of health.11,12
METHODS
Data Sources
We derived patient and encounter data from electronic health records in the Accelerating Data Value Across a National Community Health Center (ADVANCE) Clinical Research Network (managed by OCHIN, Inc) from 345 clinics in 18 states. ADVANCE contains patient- and encounter-level data on acute care use and chronic asthma management, but not hospital data. We therefore linked study patients to Oregon-Medicaid claims data to evaluate hospital-based care in a subset of the ADVANCE full sample (access to Medicaid data was limited to Oregon). Such data linkage has been used extensively in prior studies.13–15 We used electronic health record and Oregon-Medicaid claims data from January 1, 2012 to June 30, 2018. The study was approved by the Oregon Health & Science University Institutional Review Board.
Population
Our full sample included patients aged 3 to 17 years with at least 1 ambulatory visit within the ADVANCE network since January 1, 2012, and an asthma diagnosis before July 1, 2017 (providing at least 1 year of observation). Our subsample included those with any Oregon-Medicaid coverage during the study period. We excluded patients without complete racial/ethnic and preferred language data (<3% of our population). We also excluded 8 patients with cystic fibrosis because of medication-related confounding; 98 who were pregnant and 8 who died because of potential effects on use rates; and those turning 18 years of age prior to having 1 full year of observation.
Dependent Variables
We had 2 sets of outcomes: 1 for the full sample (CHC users) and 1 for the subsample with hospital data (Oregon-Medicaid recipients). In the full sample, we analyzed the prevalence and rate of clinic-coded asthma exacerbations (instances when the clinician used International Classification of Diseases codes specifically for exacerbations) at ambulatory care visits within CHCs. In the Oregon-Medicaid subsample, we repeated the ambulatory care analyses to assess whether associations observed in the full sample were also seen in the subsample, and further examined the prevalence and rate of asthma-related hospital care (ED visits and inpatient admissions).
Independent Variables
The main independent variable was group as defined by race, ethnicity, and language, with sufficient data for 4 groups: non-Hispanic White, non-Hispanic Black, English-preferring Latine, and Spanish-preferring Latine. Preferred language may serve as a proxy for self-identity, acculturation, or both, the effects of which have been shown to impact care use and health outcomes.16,17 Although we use Latine because it is often preferred in our study population, the actual ethnicity information collected by clinics is Hispanic vs non-Hispanic. All children in the non-Hispanic White group reported not identifying as Hispanic, their race as “White,” and their preferred language as English. Overall, children in the Latine groups identified as being Hispanic and/or preferring the Spanish language, while those who identified as Hispanic with a preference for English were grouped accordingly. The Spanish-preferring Latine group included 28 children whose language preference was Spanish and who identified with Black race; all other children who identified as non-Hispanic and of Black race were included in the non-Hispanic Black group. We did not have enough non–English-speaking and non–Spanish speaking Black children to create a separate group for analysis (95% of Black children preferred English).
Covariates
Analyses included important confounders: age, sex, urbanicity of patients’ primary clinic (metropolitan, micropolitan, rural); region (Northeast, South, Midwest, West); documented asthma severity; number of CHC visits per year; aggregate encounter-level data for body mass index (never overweight, sometimes overweight, always overweight—calculated using the “childsds” package in R [R Foundation]; considered overweight if >85th percentile); payer type (some public, some private, both, never insured); income as percent of the US federal poverty level; prescriptions for albuterol and inhaled corticosteroids (first-line medications for asthma18); influenza and pneumococcal vaccinations; and tobacco smoke exposure. Variables for asthma severity, income, and tobacco smoke exposure contain “not documented” categories that we retained as important measures of care and assessment potentially not provided to these children.
Statistical Analysis
First, we described patient characteristics overall and by race, ethnicity, and language group for the full sample of children with asthma and the subsample of Oregon-Medicaid recipients.
Next, for the full sample, we evaluated the binary outcome of ever visiting a CHC for asthma exacerbation through generalized estimating equations (GEE) logistic regression analysis with all aforementioned covariates. We accounted for clustering on the patient’s most frequented clinic through the use of a robust sandwich variance estimator with exchangeable correlation structure. Predicted probabilities and estimated odds ratios (ORs) along with 95% CIs are reported for non-Hispanic Black, English-preferring Latine, and Spanish-preferring Latine children compared with non-Hispanic White children. Additionally, for yearly rates of CHC visits for asthma exacerbation, we used GEE negative binomial regression analysis with the same covariates and clustering methods. For these analyses, we report predicted rates, rate ratios (RRs), and 95% CIs.
For the Oregon-Medicaid subsample, we derived similar GEE models to evaluate CHC asthma exacerbation visits and rates as described above for the full sample. For the outcomes of ever making an asthma-related ED visit and ever having an asthma-related hospital admission, we used a GEE logistic model with all aforementioned covariates and robust sandwich variance estimator with exchangeable correlation structure. We further compared the race, ethnicity, and language groups using yearly rates of asthma-related ED visits and inpatient admissions, estimated using GEE negative binomial regression analysis with the same covariates and clustering methods as before.
For all outcomes, we report unadjusted and adjusted estimates to better understand the effects of our demographic, health status, and care-quality covariates on any disparities or changes therein. Estimates were computed using Stata 15 (StataCorp LLC) and 2-sided testing with a set 5% type I error.
RESULTS
Sample Characteristics
Our full study sample included 41,276 children, and our Oregon-Medicaid recipient subsample included 6,555 children. Characteristics of these 2 populations are shown in Table 1 and Supplemental Table 1, respectively.
Table 1.
Characteristics of Children Aged 3 to 17 Years With Asthma in the ADVANCE Clinical Research Network, 2012-2018
| Racial, Ethnic, and Language Group | |||||
|---|---|---|---|---|---|
| Characteristic | All (N = 41,276) | Non-Hispanic White (n = 10,164) | Non-Hispanic Black (n = 10,041) | Latine, Prefer English (n = 9,239) | Latine, Prefer Spanish (n = 11,832) |
| Female, No. (%) | 17,709 (42.9) | 4,429 (43.6) | 4,257 (42.4) | 4,011 (43.4) | 5,012 (42.4) |
| Age at first visit, mean (SD), y | 7.6 (3.7) | 8.2 (3.8) | 7.6 (3.7) | 7.6 (3.7) | 6.9 (3.4) |
| BMI category, No. (%)a | |||||
| Never overweight | 16,726 (40.5) | 4,663 (45.9) | 4,565 (45.5) | 3,592 (38.9) | 3,906 (33.0) |
| Sometimes overweight | 10,083 (24.4) | 2,222 (21.9) | 2,233 (22.2) | 2,261 (24.5) | 3,367 (28.5) |
| Always overweight | 14,467 (35.0) | 3,279 (32.3) | 3,243 (32.3) | 3,386 (36.6) | 4,559 (38.5) |
| Payor type, No. (%) | |||||
| Never insured | 1,122 (2.7) | 275 (2.7) | 188 (1.9) | 264 (2.9) | 395 (3.3) |
| Some private | 2,423 (5.9) | 1,140 (11.2) | 409 (4.1) | 618 (6.7) | 256 (2.2) |
| Some private and public | 3,324 (8.1) | 984 (9.7) | 659 (6.6) | 1,003 (10.9) | 678 (5.7) |
| Some public | 34,407 (83.4) | 7,765 (76.4) | 8,785 (87.5) | 7,354 (79.6) | 10,503 (88.8) |
| Federal poverty level, No. (%) | |||||
| Always >138% | 2,916 (7.1) | 1,029 (10.1) | 805 (8.0) | 620 (6.7) | 462 (3.9) |
| Above and below 138% | 5,151 (12.5) | 1,350 (13.3) | 946 (9.4) | 930 (10.1) | 1,925 (16.3) |
| Always ≤138% | 28,103 (68.1) | 5,973 (58.8) | 7,072 (70.4) | 6,437 (69.7) | 8,621 (72.9) |
| Not documented | 5,106 (12.4) | 1,812 (17.8) | 1,218 (12.1) | 1,252 (13.6) | 824 (7.0) |
| Urbanicity, No. (%)b | |||||
| Metropolitan | 35,401 (85.8) | 7,507 (73.9) | 9,619 (95.8) | 7,174 (77.6) | 11,101 (93.8) |
| Micropolitan | 4,493 (10.9) | 1,998 (19.7) | 183 (1.8) | 1,705 (18.5) | 607 (5.1) |
| Rural | 1,382 (3.3) | 659 (6.5) | 239 (2.4) | 360 (3.9) | 124 (1.0) |
| US region, No. (%) | |||||
| Northeast | 4,129 (10.0) | 228 (2.2) | 1,449 (14.4) | 1,163 (12.6) | 1,289 (10.9) |
| South | 17,515 (42.4) | 3,819 (37.6) | 5,293 (52.7) | 3,677 (39.8) | 4,726 (39.9) |
| Midwest | 3,819 (9.3) | 708 (7.0) | 2,457 (24.5) | 356 (3.9) | 298 (2.5) |
| West | 15,813 (38.3) | 5,409 (53.2) | 842 (8.4) | 4,043 (43.8) | 5,519 (46.6) |
| Visits per year, No. (%) | |||||
| ≤1 | 17,900 (43.4) | 5,005 (49.2) | 5,420 (54.0) | 3,914 (42.4) | 3,561 (30.1) |
| 2 or 3 | 8,015 (19.4) | 1,825 (18.0) | 1,933 (19.3) | 1,790 (19.4) | 2,467 (20.9) |
| ≥4 | 15,361 (37.2) | 3,334 (32.8) | 2,688 (26.8) | 3,535 (38.3) | 5,804 (49.1) |
| Maximum asthma severity, No. (%)c | |||||
| Intermittent | 11,348 (27.5) | 2,537 (25.0) | 3,324 (33.1) | 2,169 (23.5) | 3,318 (28.0) |
| Mild persistent | 6,541 (15.8) | 1,193 (11.7) | 1,780 (17.7) | 1,691 (18.3) | 1,877 (15.9) |
| Moderate to severe persistent | 3,583 (8.7) | 787 (7.7) | 1,062 (10.6) | 757 (8.2) | 977 (8.3) |
| Not documented | 19,804 (48.0) | 5,647 (55.6) | 3,875 (38.6) | 4,622 (50.0) | 5,660 (47.8) |
| Influenza vaccination rate, No. (%) | |||||
| <50% annually | 28,851 (69.9) | 8,019 (78.9) | 7,332 (73.0) | 6,743 (73.0) | 6,757 (57.1) |
| 50% to 80% annually | 8,685 (21.0) | 1,542 (15.2) | 1,968 (19.6) | 1,771 (19.2) | 3,404 (28.8) |
| ≥80% annually | 3,740 (9.1) | 603 (5.9) | 741 (7.4) | 725 (7.8) | 1,671 (14.1) |
| Pneumococcal vaccination ever, No. (%) | 26,560 (64.3) | 5,585 (54.9) | 6,705 (66.8) | 5,677 (61.4) | 8,593 (72.6) |
| Smoker, No. (%) | |||||
| Never | 26,905 (65.2) | 6,136 (60.4) | 6,048 (60.2) | 6,010 (65.1) | 8,711 (73.6) |
| Ever | 969 (2.3) | 424 (4.2) | 262 (2.6) | 163 (1.8) | 120 (1.0) |
| Passive only | 3,018 (7.3) | 1,566 (15.4) | 665 (6.6) | 408 (4.4) | 379 (3.2) |
| Not documented | 10,384 (25.2) | 2,038 (20.1) | 3,066 (30.5) | 2,658 (28.8) | 2,622 (22.2) |
| Albuterol prescriptions per year, mean (SD) | 0.6 (0.6) | 0.5 (0.6) | 0.7 (0.7) | 0.6 (0.6) | 0.7 (0.7) |
| Inhaled corticosteroid prescription ever, No. (%) | 12,267 (29.7) | 2,860 (28.1) | 2,944 (29.3) | 2,411 (26.1) | 4,052 (34.2) |
ADVANCE = Accelerating Data Value Across a National Community Health Center; BMI = body mass index; RUCA = rural-urban commuting area; US = United States.
Notes: All children had at least 1 year of observation. Data are representative of 345 clinics spanning 18 US states and 4 regions: Northeast (Massachusetts, Rhode Island), South (Florida, Georgia, Maryland, North Carolina), Midwest (Indiana, Kansas, Missouri, Ohio, Wisconsin), and West (Alaska, California, Hawaii, Nevada, New Mexico, Oregon, Washington).
Overweight if BMI >85th percentile. Category reflects all available measures during study period. Biologically implausible values were flagged as more than 8 SDs above or 4 SDs below mean BMI.
RUCA classification code based on 2010 census tract information and patients’ primary clinic zip code.
Maximum asthma severity diagnosed in an ambulatory visit encounter or documented in the patient problem list.
In the full sample, non-Hispanic White children were more likely to ever have private insurance and less likely to live below 138% of the federal poverty level. Non-Hispanic Black children had the highest proportion (10.6%) of moderate to severe asthma, and the lowest proportion of severity not documented/unknown. Non-Hispanic Black children also had fewer yearly CHC visits; 54% made fewer than 2 visits annually, a minimum standard of care for children with asthma.18 Latine children in general were more often overweight and less often exposed to tobacco smoke, while Spanish-preferring Latine children specifically had higher rates of receipt of influenza and pneumococcal vaccinations, and documented inhaled corticosteroid prescription at some time.
These group differences in the full sample were also seen in the Oregon-Medicaid subsample (Supplemental Table 1). Characteristics of the Oregon-Medicaid and non–Oregon-Medicaid subsamples were also similar (data not shown).
Clinic Visits for Asthma Exacerbation
In unadjusted regression modeling in the full sample, non-Hispanic Black and Latine children overall had a higher probability of ever having had a clinic-coded asthma exacerbation at an ambulatory CHC clinic visit when compared with non-Hispanic White children (Table 2), as did Spanish-preferring Latine children in the Oregon-Medicaid subsample (Supplemental Table 2). After adjusting for confounders, only the Spanish-preferring Latine group in both the full sample (OR = 1.10; 95% CI, 1.02-1.18) and the Oregon-Medicaid subsample (OR = 1.36; 95% CI, 1.17-1.58) still had higher odds of exacerbation. Although rates of CHC visits for asthma exacerbation were higher for Spanish-preferring Latine children in both samples before adjustment, these differences were no longer statistically significant after adjustment.
Table 2.
Clinic Visits for Asthma Exacerbation Among Children With Asthma Aged 3 to 17 Years (N = 41,276)
| Clinic Visit Outcomes for Asthma Exacerbation | ||||
|---|---|---|---|---|
| Outcome and Group | Unadjusted | Adjusteda | ||
| Visits | Predicted probability, %b | OR (95% CI) | Predicted probability, %b | OR (95% CI) |
| Non-Hispanic White | 22.4 | Ref | 34.3 | Ref |
| Non-Hispanic Black | 24.9 | 1.15 (1.02-1.30) | 34.1 | 0.99 (0.89-1.09) |
| Latine, prefer English | 24.1 | 1.10 (1.01-1.20) | 34.1 | 0.99 (0.92-1.06) |
| Latine, prefer Spanish | 27.4 | 1.31 (1.20-1.43) | 36.1 | 1.10 (1.02-1.18) |
| Visit rate | Predicted annual ratec | RR (95% CI) | Predicted annual ratec | RR (95% CI) |
|---|---|---|---|---|
| Non-Hispanic White | 15.1 | Ref | 19.3 | Ref |
| Non-Hispanic Black | 15.3 | 1.01 (0.84-1.23) | 20.0 | 1.03 (0.87-1.23) |
| Latine, prefer English | 24.8 | 1.65 (0.95-2.86) | 22.9 | 1.18 (0.93-1.51) |
| Latine, prefer Spanish | 18.7 | 1.24 (1.03-1.50) | 17.9 | 0.92 (0.80-1.06) |
OR = odds ratio; RR = rate ratio; Ref = reference.
Notes: Visits to community health center ambulatory clinics only. Values in bold denote statistically significant results (P <.05).
Adjusted for age, sex, body mass index, insurance type, federal poverty level, urbanicity, US region, documented asthma severity, number of yearly visits, albuterol and inhaled corticosteroid prescriptions, influenza and pneumococcal vaccinations, and tobacco smoke exposure.
Predicted probability of ever having a visit with a clinic-coded asthma exacerbation; adjusted results are averaged over covariates.
Predicted annual rate of visits with clinic-coded asthma exacerbation per 100 person-years; adjusted results are averaged over covariates.
Asthma-Related ED Visits
In our Oregon-Medicaid subsample, non-Hispanic Black children had higher odds of ever having an asthma-related ED visit and had higher yearly rates of those visits compared with non-Hispanic White children in both the unadjusted and adjusted models (adjusted OR = 1.40; 95% CI, 1.04-1.89 and adjusted RR = 1.49; 95% CI, 1.09-2.04, respectively) (Table 3). We found no differences in these outcomes comparing Latine children with non-Hispanic White children.
Table 3.
Asthma-Related ED Visits Among Children With Asthma Aged 3 to 17 Years Receiving Oregon-Medicaid (N = 6,555)
| Asthma-Related ED Visit Outcomes | ||||
|---|---|---|---|---|
| Outcome and Group | Unadjusted | Adjusteda | ||
| Visits | Predicted probability, %b | OR (95% CI) | Predicted probability, %b | OR (95% CI) |
| Non-Hispanic White | 9.5 | Ref | 9.9 | Ref |
| Non-Hispanic Black | 13.3 | 1.47 (1.06-2.04) | 13.3 | 1.40 (1.04-1.89) |
| Latine, prefer English | 10.0 | 1.07 (0.84-1.36) | 10.8 | 1.10 (0.85-1.43) |
| Latine, prefer Spanish | 9.4 | 0.99 (0.78-1.27) | 9.9 | 0.99 (0.77-1.28) |
| Visit rate | Predicted annual ratec | RR (95% CI) | Predicted annual ratec | RR (95% CI) |
|---|---|---|---|---|
| Non-Hispanic White | 5.4 | Ref | 5.9 | Ref |
| Non-Hispanic Black | 9.9 | 1.84 (1.39-2.44) | 8.8 | 1.49 (1.09-2.04) |
| Latine, prefer English | 5.5 | 1.02 (0.75-1.39) | 5.3 | 0.90 (0.67-1.21) |
| Latine, prefer Spanish | 5.4 | 1.00 (0.77-1.31) | 5.4 | 0.92 (0.68-1.24) |
ED = emergency department; OR = odds ratio; RR = rate ratio; Ref = reference.
Note: Values in bold denote statistically significant results (P < .05).
Adjusted for age, sex, body mass index, federal poverty level, urbanicity, documented asthma severity, number of yearly visits, albuterol and inhaled corticosteroid prescriptions, influenza and pneumococcal vaccinations, and tobacco smoke exposure.
Predicted probability of ever having had an asthma-related ED visit; adjusted results are averaged over covariates.
Predicted annual rate of asthma-related ED visits per 100 person-years; adjusted results are averaged over covariates.
Asthma-Related Hospital Inpatient Admissions
In our Oregon-Medicaid subsample, the odds of ever having an asthma-related inpatient hospital admission and the estimated yearly rate of such admissions did not differ significantly for any of the other race, ethnicity, and language groups compared with the non-Hispanic White group (Supplemental Table 3). Overall, the probability of ever having an inpatient admission was less than 5% for all groups, with an estimated rate of 1 to 2 inpatient admissions per 100 person-years.
DISCUSSION
Key Findings
This study provides an analysis of racial/ethnic differences in pediatric acute care use for asthma in a large sample of CHC patients. Previous studies have documented disparities in asthma-related ED use, but none have shown different long-term patterns by race/ethnicity and language across acute care settings (clinics, EDs, inpatient units). We observed several themes that provide further insight into childhood asthma disparities.
Spanish-preferring Latine children were more likely to have a CHC asthma exacerbation visit compared with non-Hispanic White children; they also had the highest rates of overall CHC use (total visits per year). We observed no disparity in asthma-related ED use for these children, and on average, of all groups, they more consistently received recommended care (influenza and pneumococcal vaccinations, and documented inhaled corticosteroid prescriptions) through their CHC contact. This group thus may have benefitted from better long-term asthma management through reduced risk of respiratory infection, a known trigger, and appropriate prescribing of controller medications.19,20
Non-Hispanic Black children with asthma had overall low CHC use, which may have contributed to their higher rate of asthma-related ED visits. Consistent with other literature, we found that disparities for Black children persisted in asthma-related ED use even after adjusting for important confounders. Prior work has suggested this disparity may be associated with a lack of adequate chronic care.21,22 In our sample, the majority of Black children did not meet the minimum number of recommended yearly visits for asthma management.18 Indeed, adequate prevention and chronic care are associated with reduced ED use for asthma, in particular among racial/ethnic minorities and the young.21–23
Similar to others,24 we observed a lower clinic use rate for Black children, but not Latine children, compared with White peers. Higher use was particularly prominent among the Spanish-preferring Latine group. CHCs provide a large volume of care to low-income individuals and the uninsured.25 As such, the different patterns of use observed suggest that factors beyond affordability influence access to care. Higher ED use by non-Hispanic Black children, then, may stem from other social factors across various domains.
Social Determinants and Care Use
The effects of poverty may have been greater for Black children in our study. In our Oregon-Medicaid subsample, 73% always lived below 138% of the federal poverty level compared with 54% to 58% of the other groups. Inability to take work-leave or fill prescriptions may lead to less regular chronic care. Stressors of financial instability, together with lower primary care use, could lead to escalations of asthma symptoms that require hospital-based care.23,26,27 Studies have shown that when socioeconomic factors are equally distributed across groups, racial/ethnic differences in asthma outcomes are no longer significant.11,12 Thus, eliminating the wealth gap many Black Americans experience may improve asthma outcomes for this population.
The health care experience likely differs by race, ethnicity, and language. In surveys that are not health care setting–specific, Black adults report racial discrimination as a reason for not seeking future care for chronic conditions.28–30 Racial/ethnic representation among clinicians may also influence use as patients often seek clinicians with whom they identify.31–33 It is also possible that CHCs are more tailored to care for Latine than Black populations. Previous findings suggest Latine populations feel safe in these centers.34,35 CHCs are mandated to have appropriate language resources for patients, a service that may have advantaged our Spanish-preferring group through representation and cultural affinity.36 Culturally appropriate interventions that are tailored specifically to Black adults have improved health outcomes.37–39 Understanding the experience of Black families in CHCs is essential to optimizing their care in this setting.
Lastly, the downstream effects of racial/ethnic segregation and social deprivation may differ for Black and Latine communities, in particular when considering preferred language. The Hispanic or immigrant paradox suggests that the health of racial/ethnic minority peoples who recently arrived to the United States with minimal acculturation may be protected in a variety of ways.16,17 Despite the common experience of marked segregation and social deprivation, first-generation immigrants have better health outcomes than future generations who have undergone greater acculturation. These immigrants also have better outcomes (including higher primary care use) than Black people living in equally segregated and socially deprived neighborhoods.16,17 Further work to better understand the advantage of communities with a high proportion of immigrants may inform efforts to repair the ill effects of long-term structural racism against Black families and improve care for asthma and other chronic diseases.
Limitations
Our study has some limitations. First, we were unable to incorporate urgent care centers in our analyses. CHC users are often financially limited in their ability to receive care outside of the CHC network, however, thus minimizing the potential lack of capture of their acute-care receipt.40,41 Second, although our data came from one of the largest networks of CHCs across 18 states, study findings may not generalize to the entire US population. OCHIN’s member CHCs, however, share characteristics of the approximately 1,400 CHCs in the United States; study results therefore have the potential to apply to CHCs nationwide.42 Third, hospital-based outcomes were limited to Oregon-Medicaid claims data, possibly limiting generalizability; future studies can replicate these analyses in other states. Fourth, we were unable to account for changes in Medicaid status. Previous work has demonstrated minimal change in primary source-of-care for Medicaid recipients,43 yet health care use may have differed based on the timing of gaps in insurance. Fifth, although we incorporated many primary care variables into our analytic model, we lacked access to other important factors such as presenting symptoms, primary diagnosis, and objective respiratory markers, preventing corroboration of clinical status with clinician coding of asthma severity. The focus of this study was on setting-specific use of care, however, and there is evidence to suggest disparities in use persist despite equal distributions in asthma severity.44 Lastly, although this work advances the racial, ethnic, and language granularity needed to unravel asthma disparities, our lack of adequate sample sizes prevented study by other distinctions such as definition of a Black Latine group or other language subgroups; future work can expand this granularity.
Conclusions
This study shows disparate patterns of pediatric asthma-related health care use by race/ethnicity and language. Non-Hispanic Black children accessed clinics less for any reason and were more likely to use the ED for acute asthma care. In contrast, Spanish-preferring Latine children were more likely to access clinics in general and for acute exacerbations, which may explain their lower level of ED use. Understanding why Spanish-preferring Latine children access clinics more readily, and why Black children access clinics less regularly, is an important direction for further research.
Supplementary Material
{kind=link}
Acknowledgments
This research was funded by NIMHD and conducted with the ADVANCE Clinical Research Network. This network is led by OCHIN in partnership with Health Choice Network, Fenway Health, Oregon Health and Science University, and the Robert Graham Center HealthLandscape. ADVANCE is funded through the Patient Centered Outcomes Research Institute, contract number RI-CRN-2020-001.
Footnotes
Conflicts of interest: authors report none.
Funding support: National Institute on Minority Health and Health Disparities (NIMHD) R01MD011404; recipient: John Heintzman.
Disclaimer: NIMHD had no involvement in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
Previous presentation: An interactive live virtual oral presentation of this work, “Racial/Ethnic Disparities in Pediatric Asthma Exacerbations,” presented at the NAPCRG Annual Meeting; November 20-24, 2020; virtual meeting.
References
- 1.Centers for Disease Control and Prevention . Asthma prevalence. Published Oct 18, 2019. Accessed Aug 12, 2020. https://www.cdc.gov/asthma/data-visualizations/prevalence.htm
- 2.Centers for Disease Control and Prevention . Asthma attacks among people with current asthma, 2014–2017. Published Dec 4, 2019. Accessed Aug 12, 2020. https://www.cdc.gov/asthma/asthma_stats/attacks-current-asthma.htm
- 3.Loftus PA, Wise SK.. Epidemiology and economic burden of asthma. Int Forum Allergy Rhinol. 2015; 5(Suppl 1): S7–S10. 10.1002/alr.21547 [DOI] [PubMed] [Google Scholar]
- 4.Beck AF, Huang B, Simmons JM, et al. Role of financial and social hardships in asthma racial disparities. Pediatrics. 2014; 133(3): 431–439. 10.1542/peds.2013-2437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Soni A. Statistical Brief #434. The Five Most Costly Children’s Conditions, 2011: Estimates for U.S. Civilian Noninstitutionalized Children, Ages 0-17. Agency for Healthcare Research and Quality; 2014. Accessed Feb 27, 2020. https://www.ncbi.nlm.nih.gov/books/NBK476257 [PubMed] [Google Scholar]
- 6.Chamberlain JM, Teach SJ, Hayes KL, Badolato G, Goyal MK.. Practice pattern variation in the care of children with acute asthma. Acad Emerg Med. 2016; 23(2): 166–170. 10.1111/acem.12857 [DOI] [PubMed] [Google Scholar]
- 7.Ginde AA, Espinola JA, Camargo CA Jr.. Improved overall trends but persistent racial disparities in emergency department visits for acute asthma, 1993-2005. J Allergy Clin Immunol. 2008; 122(2): 313–318. 10.1016/j.jaci.2008.04.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhang Q, Lamichhane R, Diggs LA.. Disparities in emergency department visits in American children with asthma: 2006-2010. J Asthma. 2017; 54(7): 679–686. 10.1080/02770903.2016.1263315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sullivan PW, Ghushchyan V, Navaratnam P, et al. Exploring factors associated with health disparities in asthma and poorly controlled asthma among school-aged children in the U.S. J Asthma. 2020; 57(3): 271–285. 10.1080/02770903.2019.1571080 [DOI] [PubMed] [Google Scholar]
- 10.Qin X, Zahran HS, Malilay J.. Asthma-related emergency department (ED) visits and post-ED visit hospital and critical care admissions, National Hospital Ambulatory Medical Care Survey, 2010-2015. J Asthma. 2021; 58(5): 656–672. 10.1080/02770903.2020.1713149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fitzpatrick AM, Gillespie SE, Mauger DT, et al. Racial disparities in asthma-related health care use in the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol. 2019; 143(6): 2052–2061. 10.1016/j.jaci.2018.11.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Beck AF, Huang B, Auger KA, Ryan PH, Chen C, Kahn RS.. Explaining racial disparities in child asthma readmission using a causal inference approach. JAMA Pediatr. 2016; 170(7): 695–703. 10.1001/jamapediatrics.2016.0269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Marino M, Angier H, Valenzuela S, et al. Medicaid coverage accuracy in electronic health records. Prev Med Rep. 2018; 11: 297–304. 10.1016/j.pmedr.2018.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Heintzman J, Bailey SR, Hoopes MJ, et al. Agreement of Medicaid claims and electronic health records for assessing preventive care quality among adults. J Am Med Inform Assoc. 2014; 21(4): 720–724. 10.1136/amiajnl-2013-002333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Heintzman J, Marino M, Hoopes M, et al. Supporting health insurance expansion: do electronic health records have valid insurance verification and enrollment data? J Am Med Inform Assoc. 2015; 22(4): 909–913. 10.1093/jamia/ocv033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Eschbach K, Ostir GV, Patel KV, Markides KS, Goodwin JS.. Neighborhood context and mortality among older Mexican Americans: is there a barrio advantage? Am J Public Health. 2004; 94(10): 1807–1812. 10.2105/ajph.94.10.1807 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kaplan MS, Marks G.. Adverse effects of acculturation: psychological distress among Mexican American young adults. Soc Sci Med. 1990; 31(12): 1313–1319. 10.1016/0277-9536(90)90070-9 [DOI] [PubMed] [Google Scholar]
- 18.National Heart Lung and Blood Institute . Asthma care quick reference: diagnosing and managing asthma. Published Jun 2002. Updated Sep 2012. Accessed Aug 12, 2020. https://www.nhlbi.nih.gov/sites/default/files/media/docs/asthma_qrg_0_0.pdf
- 19.Dougherty RH, Fahy JV.. Acute exacerbations of asthma: epidemiology, biology and the exacerbation-prone phenotype. Clin Exp Allergy. 2009; 39(2): 193–202. 10.1111/j.1365-2222.2008.03157.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fu L-S, Tsai M-C.. Asthma exacerbation in children: a practical review. Pediatr Neonatol. 2014; 55(2): 83–91. 10.1016/j.pedneo.2013.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nath JB, Hsia RY.. Children’s emergency department use for asthma, 2001-2010. Acad Pediatr. 2015; 15(2): 225–230. 10.1016/j.acap.2014.10.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hasegawa K, Stoll SJ, Ahn J, Kysia RF, Sullivan AF, Camargo CA Jr.. Association of insurance status with severity and management in ED patients with asthma exacerbation. West J Emerg Med. 2016; 17(1): 22–27. 10.5811/westjem.2015.11.28715 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lawson CC, Carroll K, Gonzalez R, Priolo C, Apter AJ, Rhodes KV.. “No other choice”: reasons for emergency department utilization among urban adults with acute asthma. Acad Emerg Med. 2014; 21(1): 1–8. 10.1111/acem.12285 [DOI] [PubMed] [Google Scholar]
- 24.Trivedi M, Fung V, Kharbanda EO, et al. Racial disparities in family-provider interactions for pediatric asthma care. J Asthma. 2018; 55(4): 424–429. 10.1080/02770903.2017.1337790 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.National Association of Community Health Centers . Health center funding. Accessed Aug 21, 2020. https://www.nachc.org/focus-areas/policy-matters/health-center-funding/
- 26.Flores G, Tomany-Korman SC.. Racial and ethnic disparities in medical and dental health, access to care, and use of services in US children. Pediatrics. 2008; 121(2): e286–e298. 10.1542/peds.2007-1243 [DOI] [PubMed] [Google Scholar]
- 27.US Department of Health and Human Services, Office of Minority Health . Asthma and African Americans. Accessed Apr 30, 2021. https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=15
- 28.Nguyen TT, Vable AM, Glymour MM, Nuru-Jeter A.. Trends for reported discrimination in health care in a national sample of older adults with chronic conditions. J Gen Intern Med. 2018; 33(3): 291–297. 10.1007/s11606-017-4209-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bleich SN, Findling MG, Casey LS, et al. Discrimination in the United States: experiences of black Americans. Health Serv Res. 2019; 54(Suppl 2): 1399–1408. 10.1111/1475-6773.13220 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Shavers VL, Fagan P, Jones D, et al. The state of research on racial/ethnic discrimination in the receipt of health care. Am J Public Health. 2012; 102(5): 953–966. 10.2105/AJPH.2012.300773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ma A, Sanchez A, Ma M.. The impact of patient-provider race/ethnicity concordance on provider visits: updated evidence from the Medical Expenditure Panel Survey. J Racial Ethn Health Disparities. 2019; 6(5): 1011–1020. 10.1007/s40615-019-00602-y [DOI] [PubMed] [Google Scholar]
- 32.Saha S, Taggart SH, Komaromy M, Bindman AB.. Do patients choose physicians of their own race? Health Aff (Millwood). 2000; 19(4): 76–83. 10.1377/hlthaff.19.4.76 [DOI] [PubMed] [Google Scholar]
- 33.Association of American Medical Colleges . Figure 18. Percentage of all active physicians by race/ethnicity, 2018. Accessed Aug 21, 2020. https://www.aamc.org/data-reports/workforce/interactive-data/figure-18-percentage-all-active-physicians-race/ethnicity-2018
- 34.López-Cevallos DF, Lee J, Donlan W.. Fear of deportation is not associated with medical or dental care use among Mexican-origin farmworkers served by a federally-qualified health center—faith-based partnership: an exploratory study. J Immigr Minor Health. 2014; 16(4): 706–711. 10.1007/s10903-013-9845-1 [DOI] [PubMed] [Google Scholar]
- 35.DeVoe J, Angier H, Likumahuwa S, et al. Use of qualitative methods and user-centered design to develop customized health information technology tools within federally qualified health centers to keep children insured. J Ambul Care Manage. 2014; 37(2): 148–154. 10.1097/JAC.0000000000000016 [DOI] [PubMed] [Google Scholar]
- 36.42 U.S. Code §254b – Health centers. Legal Information Institute. Accessed Jan 20, 2021. https://www.law.cornell.edu/uscode/text/42/254b [Google Scholar]
- 37.Rader F, Elashoff RM, Niknezhad S, Victor RG.. Differential treatment of hypertension by primary care providers and hypertension specialists in a barber-based intervention trial to control hypertension in Black men. Am J Cardiol. 2013; 112(9): 1421–1426. 10.1016/j.amjcard.2013.07.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Victor RG, Ravenell JE, Freeman A, et al. Effectiveness of a barber-based intervention for improving hypertension control in black men: the BARBER-1 study: a cluster randomized trial. Arch Intern Med. 2011; 171(4): 342–350. 10.1001/archinternmed.2010.390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Gaston-Johansson F, Hill-Briggs F, Oguntomilade L, Bradley V, Mason P.. Patient perspectives on disparities in healthcare from African-American, Asian, Hispanic, and Native American samples including a secondary analysis of the Institute of Medicine focus group data. J Natl Black Nurses Assoc. 2007; 18(2): 43–52. [PubMed] [Google Scholar]
- 40.Ortega AN, Fang H, Perez VH, et al. Health care access, use of services, and experiences among undocumented Mexicans and other Latinos. Arch Intern Med. 2007; 167(21): 2354–2360. 10.1001/archinte.167.21.2354 [DOI] [PubMed] [Google Scholar]
- 41.O’Malley JP, O’Keeffe-Rosetti M, Lowe RA, et al. Health care utilization rates after Oregon’s 2008 Medicaid expansion: within-group and between-group differences over time among new, returning, and continuously insured enrollees. Med Care. 2016; 54(11): 984–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Health Resources & Services Administration . National Health Center Program Uniform Data System (UDS) Awardee Data. Accessed Jan 20, 2021. https://data.hrsa.gov/tools/data-reporting/program-data/national
- 43.Huguet N, Kaufmann J, O’Malley J, et al. Using electronic health records in longitudinal studies: estimating patient attrition. Med Care. 2020; 58(Suppl 6, Suppl 1): S46–S52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mitchell SJ, Bilderback AL, Okelo SO.. Racial disparities in asthma morbidity among pediatric patients seeking asthma specialist care. Acad Pediatr. 2016; 16(1): 64–67. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.