

Abstract
Homicide is a leading cause of death among women who are pregnant and up to one year postpartum in the United States. Most incidents are perpetrated by an intimate partner with a firearm. Some states have implemented laws that prohibit firearm possession by perpetrators of domestic violence and, in some instances, include explicit statutory language mandating relinquishment of firearms once a person has become prohibited from possessing them. We examined the impact of these policies on state-level rates of homicide among pregnant and postpartum women during the period 2011–19. We found that state laws prohibiting possession of firearms and requiring relinquishment of firearms by people convicted of domestic violence–related misdemeanors were associated with substantial reductions in homicide of pregnant and postpartum women. State policy makers should consider further strengthening domestic violence–related firearm regulations and their enforcement to prevent homicide of pregnant and postpartum women.
Homicide is one of the leading causes of death during and after pregnancy in the US, a finding that has been documented for decades in populations drawn from single cities,1,2 states,3–10 and subnational jurisdictions.9–13 Reports examining pregnancy-associated homicide (homicide of a woman while pregnant or within one year from the end of pregnancy) consistently find that a majority of these homicides are committed by an intimate partner,14 and most involve firearms.2,8,11,13 These conditions mirror incidences of intimate partner homicide more broadly (those involving all women regardless of pregnancy status), where the majority involve firearms15 and where a gun in the home has been shown to be a key factor in the escalation of nonfatal spousal abuse to homicide.16,17
Multiple studies confirm that women who are pregnant or within one year postpartum are at elevated risk for homicide compared with other women of reproductive age.9,10,18,19 Pregnancy may add stress in vulnerable relationships, and abuse may start or escalate during pregnancy and postpartum.8,20,21 Not only does the perinatal period appear to increase the likelihood of experiencing domestic violence,22 but injuries inflicted on pregnant and postpartum women also are more likely to be fatal.23
To supplement federal law, some states have banned possession of firearms by people convicted of domestic violence misdemeanors or under final domestic violence restraining orders. Such laws are often, although not always, coupled with policies that provide statutory authorization for their enforcement by explicitly requiring people who have become banned from possessing firearms to relinquish any in their possession to law enforcement or authorized gun dealers.24
A small number of studies have begun to document the impact of these state laws on rates of intimate partner homicide. Carolina Diez and colleagues25 found a 14 percent reduction in states that prohibit people subject to domestic violence–related restraining orders from possessing firearms and that require them to relinquish firearms in their possession. Older work has found smaller and inconsistent associations26,27 but suggests that effectiveness in reducing intimate partner–involved homicides depends on which provisions of the law are in place and how they are enforced.28
Given that homicide is one of the leading causes of death among perinatal women, this study focused specifically on the impact of state firearm possession and relinquishment laws on homicide in pregnant or postpartum women. These women represent a uniquely vulnerable population, and there is currently no evidence on the effectiveness of state firearm policies in reducing pregnancy-associated homicide. Such evidence may inform efforts to prevent maternal mortality.
In this study we applied a difference-in-differences research design to the most recently available data on pregnancy-associated homicide from all fifty US states to test our hypothesis that domestic violence–related firearm possession bans and relinquishment laws are associated with reductions in pregnancy-associated homicide.
Study Data And Methods
POPULATION AND DATA
We used data from the National Center for Health Statistics (NCHS) 2011–19 restricted-use mortality files, which include death records for every decedent residing in the United States. Beginning in 2003 a pregnancy checkbox was included on the standard certificate of death for enhanced surveillance of maternal death. The checkbox allows certifiers to identify the decedent as pregnant, within forty-two days from the end of pregnancy, or within forty-three days to one year from the end of pregnancy at the time of death. In 2011 (the first year of outcome measurement in this study) thirty-seven states had implemented the pregnancy checkbox. By 2018 every state and Washington, D.C., had done so. This analysis included data from all fifty states beginning in 2011 or the first full year of pregnancy checkbox implementation (see online appendix exhibit A1).29 Washington, D.C., was excluded because of missing data on relevant covariates.
OUTCOME
Pregnancy-associated homicide is defined as the homicide of a woman who is pregnant or within one year from the end of pregnancy at the time of her death. Our dependent variable of interest was the annual state-level pregnancy-associated homicide ratio (deaths per 100,000 live births) during the period 2011–19. We identified cases as any record with a pregnancy status checkbox indicating that the decedent was pregnant or up to one year postpartum at the time of her death and with an underlying cause of death International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), code for assault (X85–Y09) or manner of death indicating homicide. The annual number of live births in each state (the denominator) was aggregated from the NCHS restricted-use natality files from the period 2011–19. We also identified a subgroup of pregnancy-associated homicides—those involving firearms (ICD-10 codes X93—X95)–and estimated annual pregnancy-associated firearm homicide ratios per 100,000 live births in every state with data available during the period 2011–19.
EXPOSURE
This study evaluated two primary types of firearm laws related to domestic violence: prohibition of firearm possession by people convicted of a domestic violence-related misdemeanor, and prohibition of firearm possession by people subject to a domestic violence–related restraining order. We also evaluated the joint effect of these laws both with and without the presence of laws requiring the relinquishment of firearms among people prohibited from possessing them. We included relinquishment laws beginning in the first full year they were in effect. We lagged homicides by one year so that our models estimated associations between state law status in a given year and pregnancy-associated homicide in the subsequent year.26 Therefore, law status data covered 2010–18.
COVARIATES
All models included state and year fixed effects to control for geographic differences and secular trends. Additional state-level covariates were identified a priori as relevant to risk for homicide and maternal health outcomes and included annual estimates from the period 2010–18. Economic indicators obtained from the Census Bureau’s American Community Survey included the proportion of the state population living below the federal poverty level, median household income, and the Gini index of income inequality.
We controlled for temporal changes in homicide by including the annual stranger homicide rate (cases in which the perpetrator and victim are unknown to each other) and data available from the Federal Bureau of Investigation’s (FBI’s) Supplementary Homicide Reports,30 as well as the rate of firearm-involved homicide in the total population (deaths per 100,000 population) in the prior year. Given the absence of nationally representative data on firearm ownership in every state, we used a proxy indicator of gun ownership developed and validated by Michael Siegel and colleagues,31 which combines the number of paid permit hunting licenses per capita (from the US Fish and Wildlife Service)32 and the percentage of suicides involving firearms (from the Centers for Disease Control and Prevention’s Web-based Injury Statistics Query and Reporting System).33 Because risk for pregnancy-associated homicide differs by age and by race and ethnicity,9,18,34,35 we adjusted for differences in the demographic characteristics of the maternal population across states by including the percentage of births to non-Hispanic White women, non-Hispanic Black women, and Hispanic women and the percentage of births by maternal age. Maternal racial and ethnic groups were identified by self-reported race and ethnicity data from birth records. Finally, we included an annual policy indicator for whether the state Medicaid program covered family planning to capture women’s access to pregnancy prevention resources.36
STATISTICAL ANALYSIS
Descriptive statistics compared characteristics between states that never had a law in place and those that implemented at least one law (either a possession law or a relinquishment law) at some point during 2010–18. We fit multivariable linear difference-in-differences models to estimate changes in state-specific pregnancy-associated homicide ratios (deaths per 100,000 live births) associated with implementation of the firearm law or laws. We further explored the added impact of relinquishment laws coupled with prohibition laws by comparing states having a prohibition law alone with states having both prohibition and relinquishment laws. Each model was weighted by the number of live births by states and outcome years represented in the regression. Standard errors were clustered at the state level to control for potential serial correlation. Results include beta coefficients from both crude models (controlled only for state and year) and fully adjusted models (controlled for state, year, and all covariates).
Two states (Florida and Alabama) did not provide data to the FBI’s Supplementary Homicide Reports for some or all of the years included in this study and therefore were dropped from models that included the stranger homicide rate covariate. Because of this and other known issues with the Supplementary Homicide Reports data,37 we conducted a sensitivity analysis that refit the fully adjusted model, using the total homicide rate (available from the FBI’s Uniform Crime Reporting Program38 in every state for every year) instead of the stranger homicide rate.
Valid inference using difference-in-differences analysis requires parallel trends between treatment and control groups in the absence of the policy that was implemented. We tested this using event study models. In these models we replaced the single treatment indicator variable with relative time effects: three or more years before the policy change, two years before the policy change, the year of the policy change, and one, two, or three or more years after the policy change. We regressed the outcome variable on these time effect policy variables (omitting the year before the policy change, as is standard in event studies to avoid perfect collinearity)39 and all other covariates. If the estimates on the pretreatment time variables were statistically insignificant, we took this as evidence of parallel pre trends.
Finally, we used a placebo test to evaluate the robustness of our findings by examining the association between the firearm policies and deaths due to pneumonia in the fully adjusted model. This model would be able to detect changes that may affect general mortality through channels other than firearm laws, such as changes in the health system or access to that health system. As there is no reason to suppose a relationship between pneumonia deaths and firearm restriction laws, a well-specified difference-in-differences model should not return a statistically significant result. Data on state pneumonia mortality rates (deaths per 100,000 population) were identified using ICD-10 codes for underlying cause of death40 and aggregated from annual mortality files. Difference-in-differences analyses were conducted in SAS, version 9.4, and event study graphs were constructed in Stata, version 15.
LIMITATIONS
Our study had several limitations. Two are related to the reliance on vital records as the sole source of national data on violent maternal death. First, death records are extremely limited in detail on victims’ characteristics and circumstances surrounding the death. Without information on circumstances, we were unable to restrict our analysis to only those pregnancy-associated homicides that involved intimate partner violence. Second, although death records are an increasingly accurate source of information on maternal death, given the implementation of the pregnancy checkbox, there may be probable under-ascertainment of pregnancy-associated homicides–for example, in cases where the pregnancy is in its early weeks or where the woman is not in custody of her infant. In addition, a substantial proportion of female decedents of reproductive age have records with unknown pregnancy status. For these reasons, our estimates of pregnancy-associated homicide prevalence may be conservative reflections of the true magnitude.
Third, substantial variation exists in the provisions of state firearm possession and relinquishment laws, but our modeling did not account for the variation. For example, some laws include provisions covering people under ex parte restraining orders, evidence of previous use of a firearm in a domestic violence incident, time limits by which mandatory relinquishment must occur, and search and seizure for banned firearms.24 Certain provisions may make possession and relinquishment laws more or less effective in preventing pregnancy-associated homicide. Fourth, our study lacked sufficient power to stratify analyses by maternal race and ethnicity, but future work in this area is urgently needed given the disproportionate experience of pregnancy-associated homicide among Black women.34,35,41 Finally, the difference-in-differences approach accounted for time-invariant state-level features, and we controlled for a rigorous set of additional factors that may influence risk for pregnancy-associated homicide. Still, the possibility of residual confounding by unobserved time-varying factors remains.
Study Results
Sixteen states never had either type of firearm prohibition law in effect during 2010–18, whereas twenty-three states had at least one law in effect (either type of prohibition, with or without the paired relinquishment law) during the same period (exhibit 1 and appendix exhibit A1).28 The remaining eleven states implemented at least one law (either a prohibition law with or without a relinquishment law, or a relinquishment law to support an existing prohibition law) at some point during 2010–18.
EXHIBIT 1. Status of state domestic violence–related firearm laws in the US, 2010–18.
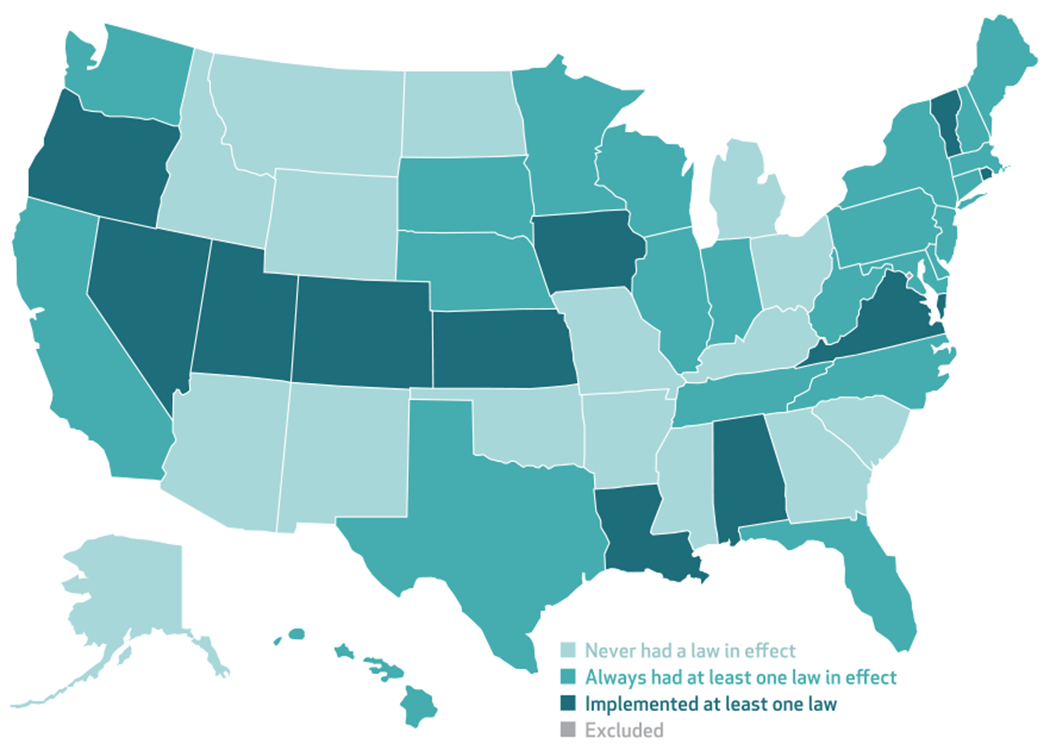
SOURCE Authors’ analysis of state legislation dates in all fifty states from legal review. NOTES Laws include prohibited possession by people convicted of a domestic violence misdemeanor, required relinquishment of firearms in possession by people convicted of a domestic violence misdemeanor, prohibited possession by people under domestic violence restraining orders, and required relinquishment of firearms in possession by people under domestic violence restraining orders. Washington, D.C., was excluded because of missing data on relevant covariates.
Pregnancy-associated homicide mortality across all state-year observations was 2.87 deaths per 100,000 live births; when we limited the observations to pregnancy-associated homicides involving firearms, the rate was 1.81 deaths per 100,000 live births (exhibit 2). Pregnancy-associated homicide ratios averaged 2.31 deaths per 100,000 live births in states that ever had at least one firearm prohibition law in effect during 2010–18 compared with 3.97 deaths per 100,000 live births in states that never had a law in effect. Economic conditions were generally better in states that ever had a firearm prohibition law.
EXHIBIT 2.
State characteristics by domestic violence–related firearm prohibition law status, 2010–18
| Characteristics | All observations, mean (N = 418) | Ever had firearm prohibition law, mean (n = 278) | Never had firearm prohibition law, mean (n = 140) |
|---|---|---|---|
| Pregnancy-associated homicide ratio | 2.87 | 2.31 | 3.97 |
|
| |||
| Pregnancy-associated firearm homicide ratio | 1.81 | 1.34 | 2.75 |
|
| |||
| Gini index of income inequalitya | 46.32 | 46.44 | 46.09 |
|
| |||
| Population below federal poverty level (%) | 14.29 | 13.39 | 16.09 |
|
| |||
| Median household income ($) | 55,598 | 58,611 | 49,615 |
|
| |||
| Gun ownership (%) | 35.59 | 31.06 | 44.28 |
|
| |||
| Stranger homicide rate | 0.45 | 0.48 | 0.41 |
|
| |||
| Firearm homicide rate | 3.70 | 3.42 | 4.25 |
|
| |||
| Maternal population race and ethnicity (%) | |||
| Non-Hispanic Black | 13.13 | 13.06 | 13.27 |
| Hispanic | 16.00 | 17.22 | 13.58 |
| Non-Hispanic White | 61.40 | 60.10 | 63.99 |
|
| |||
| Maternal population age, years (%) | |||
| 10–19 | 6.53 | 5.81 | 7.96 |
| 20–29 | 52.07 | 49.72 | 56.73 |
| 30–39 | 38.71 | 41.46 | 33.27 |
| 40–49 | 2.68 | 3.00 | 2.04 |
|
| |||
| No. of live births | 78,134 | 89,686 | 55,196 |
|
| |||
| Medicaid family planning waiver (%) | 49 | 48 | 52 |
SOURCE Authors’ analysis of data on all fifty states from the National Center for Health Statistics, the Census Bureau’s American Community Survey, the US Fish and Wildlife Service, the Centers for Disease Control and Prevention, and legal review. NOTES Pregnancy-associated homicide ratios are for 2011–19 and calculated as deaths per 100,000 live births. Stranger and firearm homicide rates are calculated as deaths per 100,000 population.
Higher values indicate greater inequality.
We found no evidence of nonparallel pre trends for pregnancy-associated homicide rates in general (appendix exhibit A2) or with firearms specifically (exhibit 3).28 The coefficients on the pre period event time indicators (two years before and three or more years before) were small and statistically insignificant, meaning that there were no detectable differences in outcome trends between treatment and control groups before policy implementation. The coefficients on postimplementation indicators (zero, one, two, and three or more years after implementation) were always negative, indicating that these laws may have some lasting protective effect.
EXHIBIT 3. Relative impacts of firearm prohibition laws on pregnancy-associated homicide involving firearms in the US, 2011–19.
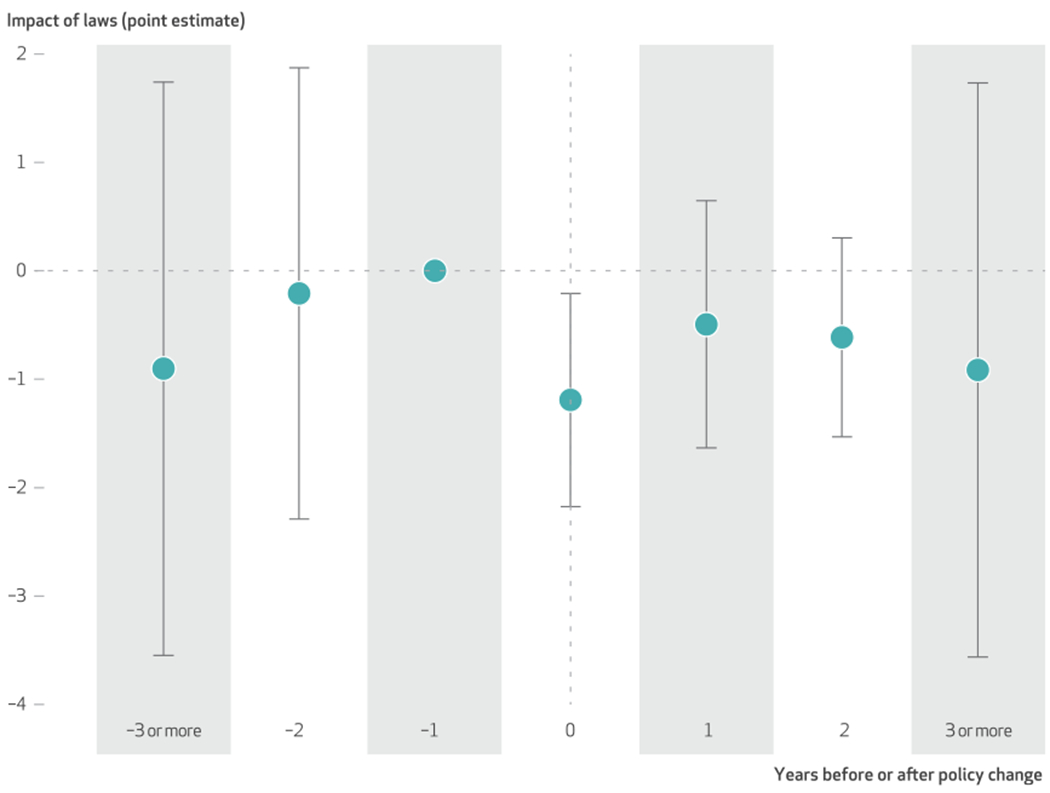
SOURCE Authors’ analysis of pregnancy-associated homicide mortality data on all fifty states from the National Center for Health Statistics and state legislation dates from legal review. NOTES Exhibit shows relative time impacts of state laws that require relinquishment of firearms when a person is convicted of a domestic violence–related misdemeanor on pregnancy-associated homicide involving firearms (deaths per 100,000 live births). One year before the policy change (−1 on the x-axis label) is the reference year. All data are from a single regression where the omitted category is the year before each state passes the legislation. Point estimates from a single regression are shown as dots, and 95% confidence intervals based on Huber-White cluster-robust standard errors at the state level are shown as whiskers.
In the crude difference-in-differences model, firearm prohibition coupled with relinquishment for both people convicted of a domestic violence–related misdemeanor and people under domestic violence restraining orders were associated with significant reductions in pregnancy-associated homicide (exhibit 4). In the fully adjusted model, states that had both prohibited firearm possession and required firearm relinquishment by people convicted of a domestic violence-related misdemeanor experienced 3.74 fewer deaths per 100,000 live births than would have been expected in the absence of either law. The relinquishment law was associated with 1.17 fewer deaths per 100,000 live births compared with the prohibition law alone. After adjustments, we did not find significant associations related to the prohibition law with or without the relinquishment law for people under domestic violence restraining orders. Patterns of association were similar for the subset of pregnancy-associated homicides that involved firearms, but results were not statistically significant.
EXHIBIT 4.
Associations between US state firearm prohibition laws (2010–18) and pregnancy-associated homicide in the year after policy implementation (2011–19)
| Crude modela |
Adjusted modelb |
||||
|---|---|---|---|---|---|
| Firearm laws | No. of observations | Pregnancy-associated homicide | No. of observations | Pregnancy-associated homicide | Firearm pregnancy-associated homicide |
| Prohibition of firearm possession by people convicted of domestic violence misdemeanorc | |||||
| Relinquishment not required | 356 | −1.57 | 311 | −1.37 | −1.24 |
| Relinquishment required | 338 | −2.33*** | 295 | −3.74** | −2.48* |
|
| |||||
| Prohibition of firearm possession by people subject to domestic violence–related restraining orderc | |||||
| Relinquishment not required | 318 | −0.61 | 278 | −0.58 | −0.59 |
| Relinquishment required | 380 | −1.30*** | 340 | −1.24* | −0.70 |
|
| |||||
| Prohibition and relinquishment by people convicted of a domestic violence misdemeanord | 210 | −0.79* | 184 | −1.17** | −0.68* |
|
| |||||
| Prohibition and relinquishment by people subject to a domestic violence–related restraining orderd | 206 | −0.87** | 172 | 0.13 | −0.56 |
SOURCE Authors’ analysis of data on all fifty states from the National Center for Health Statistics, the Census Bureau’s American Community Survey, the US Fish and Wildlife Service, the Centers for Disease Control and Prevention, and legal review. NOTE Pregnancy-associated homicide mortality is deaths per 100,000 live births.
Includes state and year fixed effects only.
Includes state, year, gun homicide and stranger homicide rates, state Medicaid family planning waiver, median household income, income inequality, poverty, gun ownership, and percent of births by maternal race and ethnicity and age during policy implementation year.
Reference group is state-years without this law.
Reference group is state-years with the possession prohibition law but no relinquishment law.
p < 0.10
p < 0.05
p < 0.01
Results did not differ substantially in models that adjusted for the total homicide rate instead of the stranger homicide rate, yielding an additional three to twelve observations across models (data not shown). Finally, the placebo tests examining the relationship between firearm prohibition and relinquishment laws and pneumonia mortality resulted in coefficients that were not statistically significant (all p > 0.05), as expected (appendix exhibit A3).28
Discussion
This analysis of state laws governing firearm prohibition and relinquishment related to domestic violence from the period 2010–18 suggests that they may be an effective intervention for the prevention of pregnancy-associated homicide. We identified two salient findings in particular. First, we found that state laws prohibiting possession of firearms and requiring relinquishment of firearms in possession by people convicted of domestic violence–related misdemeanors were associated with substantial reductions in pregnancy-associated homicides. The association between pregnancy-associated homicide and firearm prohibition laws for people under domestic violence restraining orders were in a similar direction, but smaller in magnitude and not statistically significant after adjustments.
Previous studies exploring the impact of laws that restrict firearm access among domestic violence offenders have focused on states’ rates of intimate partner homicide (which may include cases of pregnancy-associated homicide).25,26 These studies find that laws directed at people under domestic violence restraining orders are associated with the largest reductions in intimate partner homicide; this is less true for laws targeting people convicted of domestic violence misdemeanors. Given the rarity of our outcome and the number of state-year observations, our analysis may have been insufficiently powered to detect a similarly significant association with restraining order laws. After inclusion of a robust set of covariates, significance was marginal (p = 0.05). It may also be the case that for the prevention of pregnancy-associated homicide, certain provisions of domestic violence restraining orders are most effective24 (such as covering ex parte orders—those issued without the opposing party present—or restricting firearm purchases),25 and our policy indicator did not capture that variance. In addition, unlike domestic violence convictions, domestic violence restraining orders require initiation by victims. If pregnant and postpartum women are less likely to engage the civil justice system than other women, prohibition and relinquishment laws would reach fewer perpetrators of violence against perinatal women than they would perpetrators of violence against other women.
Second, our results indicate that the effectiveness of firearm prohibition laws in preventing pregnancy-associated homicide is only apparent when those laws are coupled with a relinquishment law. In states where enforcement of prohibition among people convicted of domestic violence misdemeanors was not explicitly addressed in statutory language, there was no significant reduction in pregnancy-associated homicide. This is consistent with previous research on intimate partners, a group that may include pregnant and postpartum women, which shows that laws prohibiting firearm possession alone may be ineffective at removing firearms from violent offenders and preventing firearm violence against intimate partners.24,28 Beyond mandatory relinquishment by people prohibited from possession, there is a continuum of provisions that may strengthen firearm dispossession from courts specifying the relinquishment process, requiring proof of relinquishment, noncompliance penalties, and court-ordered search and seizure.24 Future work should attempt to identify ways to strengthen relinquishment laws.
Our results were not statistically significant in the analysis limited to cases of pregnancy-associated homicide that involved firearms. Although effect estimates were similar in magnitude to and consistent in direction with the models that included all cases of pregnancy-associated homicide, broad, imprecise confidence intervals suggest insufficient power to explore subgroups within an already relatively rare outcome. Cases of pregnancy-associated homicide involving firearms are included in the total pregnancy-associated homicide models, which show that firearm prohibition and relinquishment laws for people convicted of domestic violence significantly reduce pregnancy-associated homicide rates. Furthermore, previous evidence finds that abusers who own guns inflict more severe abuse.42 Prohibited possession and required relinquishment laws targeting people convicted of domestic violence misdemeanors and people under domestic violence restraining orders have both been associated with lower odds of nonfatal injuries.43 As such, the implications of removing firearms from people prohibited from having them extend beyond the prevention of gun violence to include the prevention of violence perpetrated by other means as well.
Conclusion
An increasing number of state Maternal Mortality Review Committees are beginning to expand their capacity to identify and review violent maternal deaths for the purposes of making systems- and policy-level recommendations for prevention.44 In this analysis we found that state laws that prohibit firearm possession by perpetrators of domestic violence and that explicitly require relinquishment of firearms in possession are a promising intervention to reduce pregnancy-associated homicide. Further strengthening of domestic violence–related firearm regulations and their enforcement should be an urgent priority to prevent homicide of pregnant and postpartum women in the US. ■
Supplementary Material
Acknowledgments
Maeve Wallace and Dovile Vilda were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant No. R01HD096070-03S1). All authors are supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant No. R01 HD096070). The funding source had no involvement in the conduct of the research or preparation of the article. Its contents are solely the responsibility of the authors and do not necessarily represent the official position of the National Institutes of Health. The authors acknowledge Yixue Shao and Kate Babineau for their assistance with data visualization.
Contributor Information
Maeve E. Wallace, Department of Social, Behavioral, and Population Sciences, Tulane University School of Public Health and Tropical Medicine, in New Orleans, Louisiana.
Dovile Vilda, Department of Social, Behavioral, and Population Sciences, Tulane University School of Public Health and Tropical Medicine.
Katherine P. Theall, Department of Social, Behavioral, and Population Sciences, Tulane University School of Public Health and Tropical Medicine.
Charles Stoecker, Department of Health Policy and Management, Tulane University School of Public Health and Tropical Medicine.
NOTES
- 1.Fildes J, Reed L, Jones N, Martin M, Barrett J. Trauma: the leading cause of maternal death. J Trauma. 1992;32(5):643–5. [PubMed] [Google Scholar]
- 2.Dannenberg AL, Carter DM, Lawson HW, Ashton DM, Dorfman SF, Graham EH. Homicide and other injuries as causes of maternal death in New York City, 1987 through 1991. Am J Obstet Gynecol. 1995;172(5):1557–64. [DOI] [PubMed] [Google Scholar]
- 3.Parsons LH, Harper MA. Violent maternal deaths in North Carolina. Obstet Gynecol. 1999;94(6):990–3. [DOI] [PubMed] [Google Scholar]
- 4.Harper M, Parsons L. Maternal deaths due to homicide and other injuries in North Carolina: 1992–1994. Obstet Gynecol. 1997;90(6):920–3. [DOI] [PubMed] [Google Scholar]
- 5.Sachs BP, Brown DA, Driscoll SG, Schulman E, Acker D, Ransil BJ, et al. Maternal mortality in Massachusetts. Trends and prevention. N Engl J Med. 1987;316(11):667–72. [DOI] [PubMed] [Google Scholar]
- 6.Horon IL, Cheng D. Enhanced surveillance for pregnancy-associated mortality—Maryland, 1993–1998. JAMA. 2001;285(11):1455–9. [DOI] [PubMed] [Google Scholar]
- 7.Jocums SB, Berg CJ, Entman SS, Mitchell EF Jr. Postdelivery mortality in Tennessee, 1989–1991. Obstet Gynecol. 1998;91(5 Pt 1):766–70. [DOI] [PubMed] [Google Scholar]
- 8.Cheng D, Horon IL. Intimate-partner homicide among pregnant and postpartum women. Obstet Gynecol. 2010;115(6):1181–6. [DOI] [PubMed] [Google Scholar]
- 9.Wallace ME, Crear-Perry J, Mehta PK, Theall KP. Homicide during pregnancy and the postpartum period in Louisiana, 2016–2017. JAMA Pediatr. 2020;174(4):387–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Koch AR, Rosenberg D, Geller SE, Illinois Department of Public Health Maternal Mortality Review Committee Working Group. Higher risk of homicide among pregnant and postpartum females aged 10–29 years in Illinois, 2002–2011. Obstet Gynecol. 2016;128(3):440–6. [DOI] [PubMed] [Google Scholar]
- 11.Chang J, Berg CJ, Saltzman LE, Herndon J. Homicide: a leading cause of injury deaths among pregnant and postpartum women in the United States, 1991–1999. Am J Public Health. 2005;95(3):471–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Palladino CL, Singh V, Campbell J, Flynn H, Gold KJ. Homicide and suicide during the perinatal period: findings from the National Violent Death Reporting System. Obstet Gynecol. 2011;118(5):1056–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wallace ME, Friar N, Herwehe J, Theall KP. Violence as a direct cause of and indirect contributor to maternal death. J Womens Health (Larchmt). 2020;29(8):1032–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Campbell J, Matoff-Stepp S, Velez ML, Cox HH, Laughon K. Pregnancy-associated deaths from homicide, suicide, and drug overdose: review of research and the intersection with intimate partner violence. J Womens Health (Larchmt). 2021;30(2):236–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fox JA, Fridel EE. Gender differences in patterns and trends in U.S. homicide, 1976–2015. Violence Gend. 2017;4(2):37–43. [Google Scholar]
- 16.Bailey JE, Kellermann AL, Somes GW, Banton JG, Rivara FP, Rushforth NP. Risk factors for violent death of women in the home. Arch Intern Med. 1997;157(7):777–82. [PubMed] [Google Scholar]
- 17.Spencer CM, Stith SM. Risk factors for male perpetration and female victimization of intimate partner homicide: a meta-analysis. Trauma Violence Abuse. 2020;21(3):527–40. [DOI] [PubMed] [Google Scholar]
- 18.Wallace ME, Hoyert D, Williams C, Mendola P. Pregnancy-associated homicide and suicide in 37 US states with enhanced pregnancy surveillance. Am J Obstet Gynecol. 2016;215(3):364.e1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Austin AE, Vladutiu CJ, Jones-Vessey KA, Norwood TS, Proescholdbell SK, Menard MK. Improved ascertainment of pregnancy-associated suicides and homicides in North Carolina. Am J Prev Med. 2016;51(5, Suppl 3):S234–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Campbell J, Garcia-Moreno C, Sharps P. Abuse during pregnancy in industrialized and developing countries. Violence Against Women. 2004;10(7):770–89. [Google Scholar]
- 21.Stewart DE, Vigod SN, MacMillan HL, Chandra PS, Han A, Rondon MB, et al. Current reports on perinatal intimate partner violence. Curr Psychiatry Rep. 2017;19(5):26. [DOI] [PubMed] [Google Scholar]
- 22.Campbell JC, editor. Empowering survivors of abuse: health care for battered women and their children. Thousand Oaks (CA): Sage Publications; 1998. [Google Scholar]
- 23.Deshpande NA, Kucirka LM, Smith RN, Oxford CM. Pregnant trauma victims experience nearly 2-fold higher mortality compared to their nonpregnant counterparts. Am J Obstet Gynecol. 2017;217(5):590.e1–9. [DOI] [PubMed] [Google Scholar]
- 24.Zeoli AM, Frattaroli S, Roskam K, Herrera AK. Removing firearms from those prohibited from possession by domestic violence restraining orders: a survey and analysis of state laws. Trauma Violence Abuse. 2019;20(1):114–25. [DOI] [PubMed] [Google Scholar]
- 25.Díez C, Kurland RP, Rothman EF, Bair-Merritt M, Fleegler E, Xuan Z, et al. State intimate partner violence-related firearm laws and intimate partner homicide rates in the United States, 1991 to 2015. Ann Intern Med. 2017;167(8):536–43. [DOI] [PubMed] [Google Scholar]
- 26.Vigdor ER, Mercy JA. Do laws restricting access to firearms by domestic violence offenders prevent intimate partner homicide? Eval Rev. 2006;30(3):313–46. [DOI] [PubMed] [Google Scholar]
- 27.Bridges FS, Tatum KM, Kunselman JC. Domestic violence statutes and rates of intimate partner and family homicide: a research note. Crim Justice Policy Rev. 2008;19(1):117–30. [Google Scholar]
- 28.Zeoli AM, Malinski R, Turchan B. Risks and targeted interventions: firearms in intimate partner violence. Epidemiol Rev. 2016;38(1):125–39. [DOI] [PubMed] [Google Scholar]
- 29.To access the appendix, click on the Details tab of the article online.
- 30.Federal Bureau of Investigation. 2019 crime in the United States: expanded homicide [Internet]. Washington (DC): FBI; [cited 2021 Aug 2]. Available from: https://ucr.fbi.gov/crime-in-the-u.s/2019/crime-in-the-u.s.-2019/topic-pages/expanded-homicide [Google Scholar]
- 31.Siegel M, Ross CS, King C 3rd. A new proxy measure for state-level gun ownership in studies of firearm injury prevention. Inj Prev. 2014;20(3):204–7. [DOI] [PubMed] [Google Scholar]
- 32.US Fish and Wildlife Service. Historical hunting license data [Internet]. Washington (DC): Fish and Wildlife Service; [cited 2021 Aug 2]. Available from: https://www.fws.gov/wsfrprograms/subpages/licenseinfo/hunting.htm [Google Scholar]
- 33.Centers for Disease Control and Prevention. WISQARS—Web-based Injury Statistics Query and Reporting System [Internet]. Atlanta (GA): CDC; [cited 2021 Aug 2]. Available from: ahttps://www.cdc.gov/injury/wisqars/index.html [Google Scholar]
- 34.Kivisto AJ, Mills S, Elwood LS. Racial disparities in pregnancy-associated intimate partner homicide. J Interpers Violence. 2021. Feb 2. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 35.Morrison PK, Pallatino C, Fusco RA, Kenkre T, Chang J, Krans EE. Pregnant victims of intimate partner homicide in the National Violent Death Reporting System Database, 2003–2014: a descriptive analysis. J Interpers Violence. 2020. Jul 26. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 36.Guttmacher Institute. Medicaid family planning eligibility expansions [Internet] New York (NY): Guttmacher Institute; 2021. Jul 1 [cited 2021 Aug 2]. Available from: https://www.guttmacher.org/state-policy/explore/medicaid-family-planning-eligibility-expansions [Google Scholar]
- 37.Pizarro JM, Zeoli AM. An assessment of the quality of homicide data in the Supplementary Homicide Reports: a research note. Justice Q. 2013;30(4):711–31. [Google Scholar]
- 38.Federal Bureau of Investigation. Uniform Crime Reporting Program [Internet]. Washington (DC): FBI; [cited 2021 Aug 2]. Available from: https://www.fbi.gov/services/cjis/ucr [Google Scholar]
- 39.Borusyak K, Jaravel X (Princeton University, Princeton, NJ: ). Revisiting event study designs. SSRN [preprint on the Internet]. 2017. May 8 [cited 2021 Aug 20]. Available from: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2826228 [Google Scholar]
- 40.Smithee RB, Markus TM, Soda E, Grijalva CG, Xing W, Shang N, et al. Pneumonia hospitalization coding changes associated with transition from the 9th to 10th revision of International Classification of Diseases. Health Serv Res Manag Epidemiol. 2020. Jul 24. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wallin MA, Holliday CN, Zeoli AM. The association of federal and state-level firearm restriction policies with intimate partner homicide: a reanalysis by race of the victim. J Interpers Violence. 2021. Jun 18. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 42.McFarlane J, Soeken K, Campbell J, Parker B, Reel S, Silva C. Severity of abuse to pregnant women and associated gun access of the perpetrator. Public Health Nurs. 1998;15(3):201–6. [DOI] [PubMed] [Google Scholar]
- 43.Willie TC, Kershaw T, Perler R, Caplon A, Katague M, Sullivan TP. Associations between state intimate partner violence–related firearm policies and injuries among women and men who experience intimate partner violence. Inj Epidemiol. 2021;8(1):8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Koch AR, Geller SE. Addressing maternal deaths due to violence: the Illinois experience. Am J Obstet Gynecol. 2017;217(5):556.e1–6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.