

Abstract
Objective
A clinical trial carried out in patients hospitalized for clinical and surgical conditions. This study evaluated the effectiveness of text messaging interventions (TM) versus telephone counseling (TC) to promote smoking cessation among hospitalized smokers in a middle-income country. Seven-day abstinence was measured during follow-up phone calls one month after discharge. The comparative cost of the two interventions considered the cost of calls, time spent on phone calls and sending SMS and cost of the professional involved in the approaches.
Results
Past 7-day tobacco abstinence was not statistically different between groups (30.5% in TM group and 26% in TC, p = 0.318). Costs were significantly lower in the TM group (U$9.28 × U$19.45- p < 0,001). Continuous abstinence was reported by 26% of TM participants and 24.5% of TC participants (p = 0.730). In the 3-month follow-up, 7-day abstinence was 23% in the TMI and 27% in the TC (p = 0.356) group. Continuous abstinence was reported by 20% of TM participants and 24% of TC participants (p = 0.334).
Trial registration: ClinicalTrials.gov ID: NCT03237949 Registred on: 30th May 2017.
Supplementary Information
The online version contains supplementary material available at 10.1186/s13104-022-06002-6.
Keywords: Patient discharge, Randomized trial, Smoking cessation, Text messaging
Introduction
Smoking is the leading cause of premature death worldwide [1, 2]. During hospital stays, when they were hospitalized for diagnosis and treatment of clinical and surgical conditions, patients must abstain from smoking, and they are particularly accessible and interested in receiving advice to quit [3–7]. Increased access to phones, cell phones, the internet, and the emergence of quitlines have made these strategies attractive vehicles for novel health interventions [8–15].
Brazil has one of the world’s most successful tobacco control programs, leading to a significant reduction in the prevalence of smoking in the last three decades (from more than 40% to less than 10% of the population). Brazil implemented numerous tobacco control policies including smoke-free air laws, marketing restrictions, graphic health warnings on cigarette packaging, national smoking cessation campaigns through the mass media, cigarette price increases and a national smoking cessation treatment program [16–19]. However, only a few hospitals in Brazil actually have a protocol to address smoking cessation with their patients [20–23].
Text messaging shows strong potential to extend care to hospitalized smokers in Brazil during the post-discharge period [3]. Text message interventions are effective for smoking cessation [24–26] and have a wide reach and low cost [24]. Most Brazilians- 86% of the population aged 10 years or over- are mobile phone users [27].
The present study is the first definitive randomized clinical trial to evaluate SMS for the post-discharge follow-up of smokers in Brazil. However, most smokers do not receive smoking cessation treatment when trying to quit [3]. Different from other countries, there is limited research investigating SMS to support smoking cessation among post-discharge patients in Brazil.
The objective of the present study was to evaluate the effectiveness and costs of a post-discharge text messaging (TM) versus telephone counseling (TC), for supporting cessation among hospitalized smokers in Brazil.
Main text
Methods
Design
The design a 1:1 ratio two-arm randomized controlled clinical trial of non-inferiority conducted with hospitalized smokers. The study was approved by the Hospital Ethics Committee Review Board/process number 2.868.112. The trial is registered in the Clinical Trials Registry (NCT03237949) and the Brazilian Clinical Trials Registry (RBR-8mgc3h). The study adheres to the CONSORT Guidelines.
Setting and participants
This study was conducted at a university hospital located in the city of Juiz de Fora in the southeastern part of Brazil. Smoking is prohibited in the hospital (tobacco-free campus) and patients had to remain abstinent throughout their stay. Patients were recruited from all units of a 159-bed public university hospital. Participants were involved in an initial pre-screening process using the Electronic Medical Record System (EMR) and then answered an in-person screening survey administered by the researcher team. In the first interview during hospitalization, eligible participants were consented and answered the baseline survey at bedside the day after hospitalization.
During the hospital stay and following discharge, the Interdisciplinary Center for Research and Intervention in Tobacco (CIPIT) provides tobacco treatment to all patients [28]. All patients also received a motivational approach during hospitalization and after discharge according to their allocation group.
Hospitalized smokers were eligible for inclusion on the study if they were aged ≥ 18 years, had smoked cigarettes within the past 30 days, had a cell phone, had received at least one text message in the past year. Participants were excluded if they were admitted to the intensive care, isolation rooms, were physically or cognitively unable to participate, or were incarcerated.
With 200 participants in each group, the study had 80% statistical power at an alpha of 0.05 to detect a 10% difference between groups in the proportion of participants who would quit smoking in the third month [3].
Randomization
A random allocation sequence was computer generated by the CDC Epi InfoTM7 platform. Participants were randomly assigned after the discharge, and the allocation order followed the discharge order (time and date).
Interventions
Text messaging
Patients randomized to TM received up to 30 text messages for 8–15 days after discharge. The number of messages sent after discharge was determined by the degree of motivation to maintain abstinence, reported by the patient while still hospitalized. The frequency and content of the messages varied depending on the participants’ motivation to quit. Patients abstinent or preparing to quit in the next 14 days received two messages/day over the course of 15 days. Patients not ready to quit received two messages/day over the course of 8 days following hospitalization.
The format and design of the text messages followed methods used in the pilot study [3]. Some messages were common to all patients and others were personalized based on information obtained in interviews during hospitalization. Bandura’s self-efficacy theory to design the content of text messages was used [29]. The study did not assess abstinence in the last 15 days but we used the intention to quit (or remain abstinent) in the next 30 days, collected in the baseline assessment, to customize the text message content. Participants abstinent or preparing to quit in the next 30 days received two messages per day for 15 days. Text messages were sent manually by a cell phone. Messaging was unidirectional-participants were unable to reply to messages.
Telephone counseling
In TC, participants received one weekly phone call for 4 weeks. Four attempts were made, on different days and times of the day, per week for each participant. Telephone counseling lasted approximately 15 to 30 min. The counseling approach addressed motivation, confidence, quitting history, environmental factors, trigger situations, coping strategies, medication use, relapse prevention and setting a quit date. This is the standard treatment given to all discharged patients, except in the intervention group (TM) during this study. The approaches were based on concepts of motivational interviewing and cognitive behavioral therapy. Each telephone counseling was designed to help patients develop an individualized plan to quit smoking or to remain abstinent. The approach was based on Motivational Interviewing (quote) and addressed behavioral and cognitive issues, including motivation, confidence, quitting history, environmental factors, trigger situations, coping strategies, medication use, relapse prevention and setting a quit date [30].
These approaches were based on previou pragmatic tobacco treatment research [3].
Measures
Measures included demographics and social class distribution [30]. The nicotine dependence was evaluated via Fagerström Test [32]. Withdrawal symptoms during hospitalization [33], tobacco use characteristics, readiness to quit [34], and nicotine replacement therapy during hospitalization were assessed. The Patient Health Questionnaire –4 (PHQ-4) and the Alcohol Use Disorder Identification Test (AUDIT-C) were used [35, 36].
The main outcome measure was self-reported 7 day point prevalence abstinence at 1 month post-randomization (“Did you smoke even a single puff in the last 7 days?”). Secondary outcomes included self-reported 30 days continued abstinence at 1-month post-randomization (“Did you smoke even a single puff in the last 30 days?), and biochemically verified abstinence at 3 months post-discharge. Exhaled carbon monoxide of ≤ 10 ppm was the cutoff for verification of abstinence [37].
To calculate costs, we analyzed the average time spent on interventions, the minute value of each intervention per participant, the amount paid to the telephone company, and the cost per minute worked by the healthcare professional, based on the federal employees’ salary scale. Costs were calculated in Brazilian Real and converted into dollars on January 7. 2020 (1 dollar = 4.08 Brazilian Real).
Analyses
Research Electronic Data Capture (REDCap) was used to enter the data. After descriptive statistics, the comparison of categorical variables was performed by chi-square and, for continuous variables with normal distribution, t-tests for independent samples. Nonparametric distribution variables were analyzed by Mann–Whitney. Subjects lost to follow-up were counted as smokers (intention to treat analysis—ITT).
A comparative assessment of intervention costs was performed using cost minimization, used to measure the cost difference between alternative interventions, when it is assumed that both have the same effectiveness [38].
Results
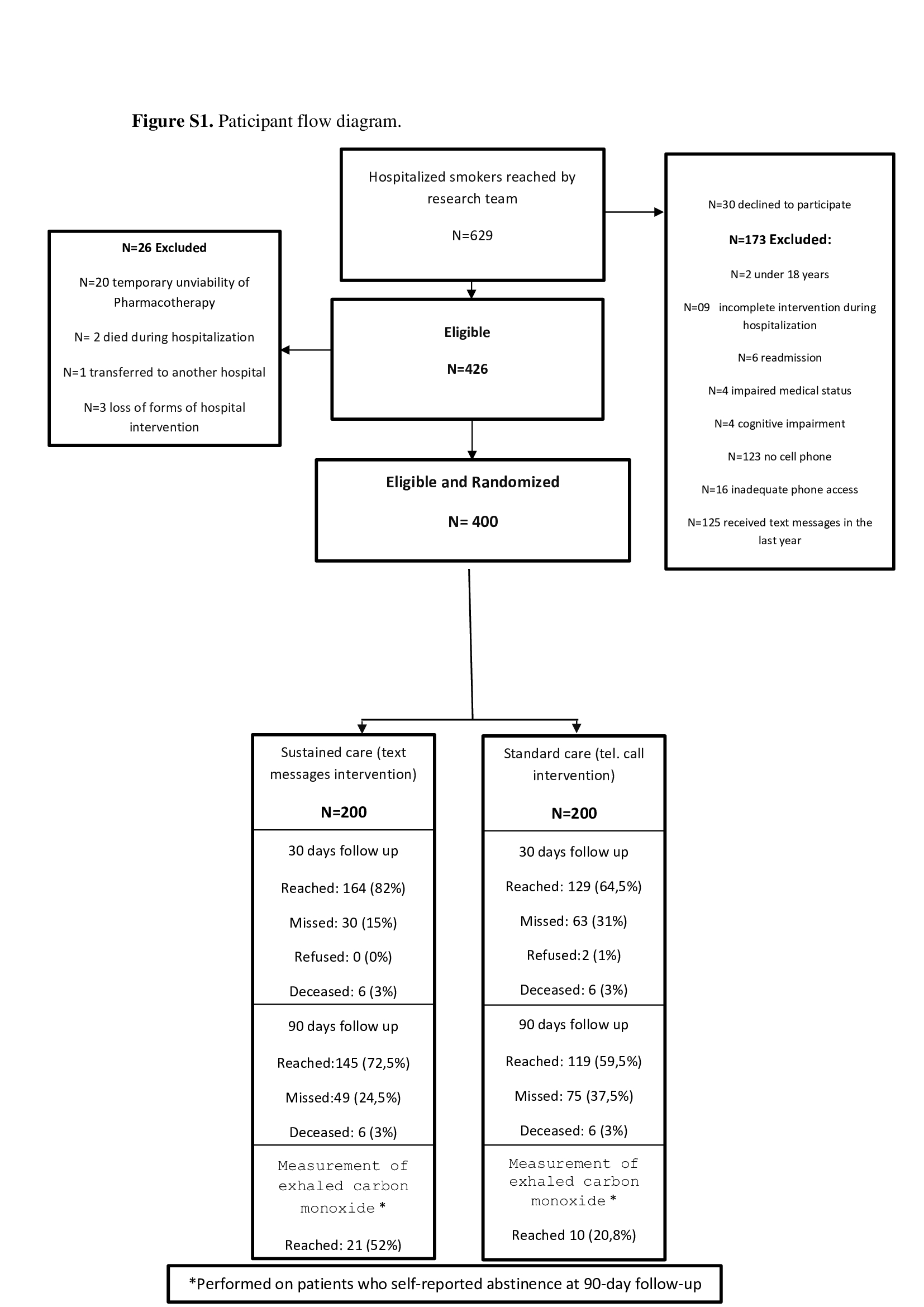
Participants were recruited from May 2017 to January 2019. Of 629 individuals identified as smokers, after evaluating exclusion criteria, 400 participants were randomized and allocated to the study groups. Some interruptions occurred due to the worsening of the medical condition of the patients or for the performance of complementary exams at the time of the approach (Figure S1).
Participant characteristics
Randomization led to similar groups for all baseline characteristics, except for the age of tobacco initiation (Table 1).
Table 1.
Baseline characteristics of study participants by treatment group
| Variables | Standard care (control) |
Sustained care (intervention) | p |
|---|---|---|---|
| M (SD) | M (SD) | ||
| Age (years) | 45.97 (12.58) | 45.45 (12.92) | 0.701 |
| Age at smoking initiation | 18.70 (16.35) | 16.09 (7.40) | 0.001 |
| Md (IR) | Md (IR) | ||
| Importance of quitting (0–10) | 10 (0) | 10 (0) | 0.844 |
| Confidence to quit (0–10) | 7 (5) | 8 (5) | 0.273 |
| Withdrawal scale (0–4) | 3 (4) | 3 (4) | 0.303 |
| N (%) | N (%) | ||
| Male | 102 (51.3) | 94 (47.2) | 0.422 |
| Ethnoracial group (self-declared) | 0.511 | ||
| White | 67 (36.2) | 62 (33.0) | |
| Black, grayish-brown/indigenous | 118 (63.8) | 126 (67.0) | |
| Education level | 0.201 | ||
| 0–4 years | 5 (2.6) | 1 (0.5) | |
| 5–8 years | 78 (40.4) | 75 (38.1) | |
| More than 9 years | 110 (57) | 121 (61.4) | |
| Married or whit a partner | 61 (33) | 58 (32.2) | 0.878 |
| SES1—average household income in dollars/month2 | 0.228 | ||
| SES A (USD 5.058) | 1 (0.5) | 0.0 (0.0) | |
| SES B1(USD 2.241) | 2 (1.0) | 1.0 (0.5) | |
| SES B2 (USD 1.175) | 43 (21.1) | 30 (15.0) | |
| SES C1 (USD 655) | 112 (56.3) | 110 (55.0) | |
| SES C2 (USD 393) | 42 (21.1) | 58 (29.0) | |
| SES D + E (USD 186) | 0 (0.0) | 1.0 (0.5) | |
| Cigarettes/day | 0.165 | ||
| < 10 | 81 (40.5) | 94 (47.3) | |
| 11–20 | 72 (36.0) | 83 (41.7) | |
| > 21 | 47 (23.5) | 22 (11.0) | |
| Time to first cigarette of the day | 0.264 | ||
| After 60 min | 34 (17.3) | 52 (26.4) | |
| Between 31 and 60 min | 24 (12.2) | 19 (9.6) | |
| Between 6 and 30 min | 61 (31.0) | 43 (21.8) | |
| The first 5 min | 78 (39.5) | 83 (42.2) | |
| Nicotine dependence3 ≥ 5 | 168 (84.0) | 179 (89.5) | 0.105 |
| Quit attempts in past year | 69 (34.5) | 87 (43.5) | 0.065 |
| Life use quit medication | 0.742 | ||
| NRT | 32 (16.1) | 34 (16.9) | |
| Bupropion | 15 (4.6) | 15 (7.5) | |
| Champix or Varenicline | 2 (1.0) | 0 (0.0) | |
| Commitment to quitting | 0.711 | ||
| Plan to stay quit | 118 (62.8) | 125 (64.4) | |
| Plan to try to stay quit | 25 (13.3) | 27 (13.9) | |
| Plan to reduce smoking | 34 (18.1) | 28 (14.4) | |
| Plan not to quit | 11 (5.9) | 14 (7.2) | |
| Current depressive symptoms4 | 88 (56.1) | 88 (55.3) | 0.900 |
| Current anxiety symptoms5 | 96 (72.2) | 98 (76.6) | 0.418 |
| Mild to Severe Risk of alcohol abuse6 | 133 (66.5) | 123 (61.5) | 0.298 |
| NRT during hospitalization | 188 (94.0) | 190 (95.0) | 0.661 |
| Any smoking-cessation treatment | 23 (13.9) | 26 (20.5) | 0.133 |
| Any smoking-cessation counseling | 57 (34.8) | 37 (29.6) | 0.354 |
| Interest in receiving medication | 170 (89.9) | 171 (91.9) | 0.503 |
M Mean, SD Standard deviation, Md Median, IR Interquartile range, SES Social economic stratum, NRT Nicotine replacement therapy
1Assessed via Brazilian criteria and social class distribution (ABEP 2016)
21 real = 4.129 dollars, december 09, 2019
3Assessed via Fagerström test for nicotine dependence
4,5Assessed via patient health questionnaire 4 item (PHQ-4)
6Assessed via alcohol use disorder identification test (AUDIT-C)
The proportion of participants reached for follow-up was 73.25% (n = 293) at 30 days post-discharge and 66% (n = 264) at 90 days post-discharge.
Abstinence at 1 and 3 months after discharge
Self-reported, 7 day point prevalence abstinence rates were not statistically different between groups at 1 month post-discharge using an ITT analysis (p = 0.318). Similarly, 30 day continuous abstinence was not significantly different between groups (p = 0.730), however the number of cigarettes per day smoked was fewer in the TM group (p < 0,036). Quit rates were also not significantly different at 3-month follow-up (Table 2).
Table 2.
Abstinence at follow up post-discharge by treatment group
| Variables | Sustained care (Intervention) N (%) |
Standard care (Control) N (%) |
p |
|---|---|---|---|
| Follow-up 30 (missing = smoking)1 | |||
| Abstinences for the past 7 days | 61 (30.5) | 52 (26.0) | 0.318 |
| Abstinences for the past 30 days | 52 (26.0) | 49 (24.5) | 0.730 |
| Follow-up 90 (missing = smoking) | |||
| Abstinences for the past 7 days | 46 (23.0) | 54 (27.0) | 0.356 |
| Abstinences for the past 90 days | 40 (20.0) | 48 (24.0) | 0.334 |
| Abstinences verified by measurement of exhaled carbon monoxide2 | 20 (95.2) n = 21 | 8 (80.0) n = 10 | 0.160 |
| M (SD) | M (SD) | ||
| Number of cigarettes per day in non-abstinent participants at follow-up 30 | 9.99 (15.033) | 13.91 (14.859) | 0.036 |
| Number of cigarettes per day in non-abstinent participants at follow-up 90 | 10.04 (14.997) | 12.51 (12.421) | 0.131 |
M Mean, SD Standard deviation
1Subjects lost to follow-up were counted as smokers (intention to treat analysis—ITT)
2Participants were characterized as abstinent if their results were ≤ 10 ppm
Cost analysis
Costs were significantly lower in the TM group compared to the TC group. Cost results can be seen in Table 3.
Table 3.
Cost analysis by strategies of counseling post-discharge
| Analysis | Text messages interventions | Telephone calls | p |
|---|---|---|---|
| Quantity per patient | 14 a 30 | 4 | |
| Monthly cost of telephone company |
R$ 22.50 U$5.51 |
R$ 69.90 U$17.13 |
p < 0,001 |
| Average time | 1 message- 0.5 min | 1 call- 4.7 min | |
| Average number of retries per approach | 1 | 3.15 | |
| Time spent on unsuccessful attempts per patient | 0 min | 8 min | |
| Health worker’s minute value 1 |
R$ 0.77 U$ 0.18 |
R$ 0.77 U$ 0.18 |
|
| Average time per patient | 7/15 minutes2 | 26.8 minutes3 | |
| Total cost per patient |
R$ 5.39 / R$ 11.55 U$ 1.32/2.83 |
R$ 20.63 U$ 5.06 |
p < 0.001 |
| Cost total per group (200 participants) | R$ 2.310.00 | R$ 4.126.00 | |
| Cost per abstinent participant in last 7 days with 30 days of follow-up |
(61 participants) R$ 37.87 U$9.28 |
(52 participants) R$ 79.34 U$19,45 |
p < 0.001 |
1According to Table of Salaries of Civil Federal Civil Servants of Jan 2019 –Education Technicians Category E (undergraduate level)
2Referring to 15 messages for the least motivated group and 30 messages for the group motivated for cessation
3Sum of call times completed, and average spent on unsuccessful attempts per patient
Discussion
This was the first fully-powered study to compare the effectiveness of text messaging versus telephone counseling for post-discharge smoking cessation treatment. Both led to a high prevalence of self-reported smoking abstinence. Cost analysis found that text messaging intervention was half as expensive as phone calls.
A recent meta-analysis included 26 clinical trials and concluded that there is moderate evidence that text messages increase cessation rates by approximately 50% when compared to support for smoking cessation [26].
In the last decades, there has been a great advance in the use of communication technologies in health care. This phenomenon contributed to the emergence of innovative health behavior change interventions [24] and several strategies have been studied to help hospitalized smokers to quit [11, 12, 15].
Behavior change interventions sent by text messages are becoming increasingly popular, the possibility of reaching many people when performing interventions without personal contact reduces costs and allows access to people who are reluctant to have direct contact [24, 25, 39, 40].
Text messages have been used in Brazil for approximately 30 years, but the strategy, despite offering great advantages in the health area, is still little explored for this purpose. Despite the Brazilian tobacco control program reaching a significant number of people, through actions of the Unified Health System (SUS), the country’s free public health system, communication technologies such as SMS are still not used by the program. Text messaging strategies are promising especially for low/middle-income countries where proactive telephone counseling is not available for free and quitline services are not structured. Future studies should address the effectiveness of automated messaging systems, evaluate ways to promote better interactivity with the participants, and determine the intensity of the approach to deliver the best results.
Limitations
Loss of follow up is an important limitation of longitudinal studies. In this study, there were significantly fewer reached for follow up in the standard care (TC) group than in the TM group. Other limitations are the loss of interactivity due to the lack of actions aimed at possible participants’ responses to messages (unidirectional messaging) and the unavailability of an automated messaging system.
Supplementary Information
{kind=link}
Additional file 1: Figure S1. Participant flow diagram.
Acknowledgements
The authors thank the employees of the Brazilian Company of Hospital Services EBSERH and UFJF, as well as the students and residents of the University Hospital for their participation in data collection and assistance in performing the test.
Abbreviations
- TM
Text messaging
- TC
Telephone counseling
- CIPIT
Interdisciplinary center for research and intervention in tobacco
- CDC
Center disease control
- PHQ-4
Patient health questionnaire–4
- AUDIT-C
Alcohol use disorder identification test
- REDCap
Research electronic data capture
- ITT
Intention to treat analysis
- M
Mean
- SD
Standard deviation
- Md
Median
- IR
Interquartile range
- SES
Social economic stratum
- NRT
Nicotine replacement therapy
- ppm
Particles per million
Authors’ contributions
LMA: conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, software, validation, writing-original draft. TMR: conceptualization, writing-review & editing. EC: conceptualization, data curation, formal analysis, investigation, methodology, software, validation, writing-review & editing. KPR: conceptualization, methodology, writing-review & editing. ROA: investigation, resources, software, visualization, writing-original draft. IOL: investigation, resources, software, writing-original draft. ACDADM: investigation, resources, writing-original draft. ICGL: conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, software, validation, writing-review & editing. All authors read and approved the final manuscript.
Funding
This work was supported by Coordination for the Improvement of Higher Education Personnel of Brazil (CAPES) process number: 88881.361525/2019-01, Federal University of Juiz de Fora and the National Council for Scientific and Technological Development (CNPQ), process number: 303229;2019-5.
Availability of data and materials
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
The study was approved by the Hospital Ethics Committee Review Board/process number 2.868.112 and all participants signed informed consent. Participants were not reimbursed for participation, as this is not permitted under Brazilian law. The trial is registered in the Clinical Trials Registry (NCT03237949) and the Brazilian Clinical Trials Registry (RBR-8mgc3h).
Consent for publication
Not applicable.
Competing interests
The authors declared no competing interest in the subject matter or materials discussed in this article.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Ekpu VU, Brown AK. The economic impact of smoking and of reducing smoking prevalence: review of evidence. Tob Use Insights. 2015;8(1):1–35. doi: 10.4137/TUI.S15628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jha P, Ramasundarahettige C, Landsman V, Rostron B, Thun M, Anderson RN, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–350. doi: 10.1056/NEJMsa1211128. [DOI] [PubMed] [Google Scholar]
- 3.Cruvinel E, Richter KP, Colugnati F, Ronzani TM. An experimental feasibility study of a hybrid telephone counseling/text messaging intervention for post-discharge cessation support among hospitalized smokers in Brazil. Nicotine Tob Res. 2019;21(12):1700–1705. doi: 10.1093/ntr/nty165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rigotti NA, Clair C, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database Syst Rev. 2012;12(1):1–86. doi: 10.1002/14651858.CD001837.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Reid ZZ, Regan S, Kelley JH, Streck JN, Ylioja T, Tindle HA, et al. Comparative effectiveness of post-discharge strategies for hospitalized smokers: study protocol for the helping HAND 2 randomized controlled trial. BMC Public Health. 2015;15(1):1–12. doi: 10.1186/s12889-015-1484-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rigotti NA, Arnsten JH, McKool KM, Wood-Reid KM, Pasternak RC, Singer DE. Efficacy of a smoking cessation program for hospital patients. Arch Intern Med. 1997;157(22):2653–2660. doi: 10.1001/archinte.1997.00440430135016. [DOI] [PubMed] [Google Scholar]
- 7.Richter KP, Faseru B, Mussulman LM, Ellerbeck EF, Shireman TI, Hunt JJ, et al. Using warm handoffs to link hospitalized smokers with tobacco treatment after discharge: study protocol of a randomized controlled trial. Trials. 2012;13(127):1–11. doi: 10.1186/1745-6215-13-127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abu-Hasaballah K, James A, Aseltine RH. Lessons and pitfalls of interactive voice response in medical research. Contemp Clin Trials. 2007;28(5):593–602. doi: 10.1016/j.cct.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 9.Cummins S, Zhu SH, Gamst A, Kirby C, Brandstein K, Klonoff C, et al. Nicotine patches and quitline counseling to help hospitalized smokers stay quit: study protocol for a randomized controlled trial. Trials. 2012;13(128):1–9. doi: 10.1186/1745-6215-13-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Buller DB, Borland R, Bettinghaus EP, Shane JH, Zimmerman DE. Randomized trial of a smartphone mobile application compared to text messaging to support smoking cessation. Telemed e-Health. 2014;20(3):206–214. doi: 10.1089/tmj.2013.0169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Harrington KF, Kim Y-I, Chen M, Ramachandran R, Pisu M, Sadasivan RS, et al. Web-Based intervention for transitioning smokers from inpatient to outpatient care: an RCT. Am J Prev Med. 2016;51(4):620–629. doi: 10.1016/j.amepre.2016.04.008. [DOI] [PubMed] [Google Scholar]
- 12.Rigotti NA, Tindle HA, Regan S, Levy DE, Chang Y, Carpenter KM, et al. A post-discharge smoking-cessation intervention for hospital patients. Am J Prev Med. 2016;51(4):597–608. doi: 10.1016/j.amepre.2016.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Richter KP, Faseru B, Shireman TI, Mussulman LM, Nazir N, Bush T, et al. Warm handoff versus fax referral for linking hospitalized smokers to quitlines. Am J Prev Med. 2016;51(4):587–596. doi: 10.1016/j.amepre.2016.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fellows JL, Mularski RA, Leo MC, Bentz CJ, Waiwaiole LA, Francisco MC, et al. Referring hospitalized smokers to outpatient quit services: a randomized trial: a randomized trial. Am J Prev Med. 2016;51(4):609–619. doi: 10.1016/j.amepre.2016.06.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sherman SE, Link AR, Rogers ES, Krebs P, Ladapo JA, Shelley DR, et al. Smoking-cessation interventions for urban hospital patients: a randomized comparative effectiveness trial. Am J Prev Med. 2016;51(4):566–577. doi: 10.1016/j.amepre.2016.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brazilian Ministry of Health. Strategies for the care of the person with chronic disease: the care of the person who smokes. Brasília: Health Care Department Primary Care Department. 2015; 1(40):1–154. http://189.28.128.100/dab/docs/portaldab/publicacoes/caderno_40.pdf
- 17.Lee K, Chagas LC, Novotny TE. Brazil and the framework convention on tobacco control: global health diplomacy as soft power. PLoS Med. 2010;7(4):1–6. doi: 10.1371/journal.pmed.1000232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Levy D, de Almeida LM, Szklo A. The Brazil simsmoke policy simulation model: the effect of strong tobacco control policies on smoking prevalence and smoking-attributable deaths in a middle income nation. PLoS Med. 2012;9(11):1–13. doi: 10.1371/journal.pmed.1001336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shibuya K, Ciecierski C, Guindon E, Bettcher DW, Evans DB, Murray CJL. WHO framework convention on tobacco control: Development of an evidence based global public health treaty. Br Med J. 2003;327(7407):154–157. doi: 10.1136/bmj.327.7407.154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Garcia T, dos Andrade SAS, Biral AT, Bertani AL, de Caram LMO, Cezare TJ, et al. Evaluation of smoking cessation treatment initiated during hospitalization in patients with heart disease or respiratory disease. J Bras Pneumol. 2018;44(1):42–48. doi: 10.1590/S1806-37562017000000026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.de Azevedo RCS, Mauro MLF, Lima DD, Gaspar KC, da Silva VF, Botega NJ. General hospital admission as an opportunity for smoking-cessation strategies: a clinical trial in Brazil. Gen Hosp Psychiatry. 2010;32(6):599–606. doi: 10.1016/j.genhosppsych.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 22.de Abreu Perez C, Pinheiro T, Bialous S, Cunha V, Maria Cavalcante T. Disque Saúde Pare de Fumar no Brasil: uma Fonte de Informação a mais para a População. Brazilian J Cancerol. 2011;57(3):337–344. doi: 10.32635/2176-9745.RBC.2011v57n3.668. [DOI] [Google Scholar]
- 23.Matkin W, Ordóñez-Mena JM, Hartmann-Boyce J. Telephone counselling for smoking cessation. Cochrane Database Syst Rev. 2019;2019(5):1–163. doi: 10.1002/14651858.CD002850.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Spohr SA, Nandy R, Gandhiraj D, Vemulapalli A, Anne S, Walters ST. Efficacy of SMS text message interventions for smoking cessation: a meta-analysis. J Subst Abuse Treat. 2015;56:1–10. doi: 10.1016/j.jsat.2015.01.011. [DOI] [PubMed] [Google Scholar]
- 25.Scott-Sheldon LAJ, Lantini R, Jennings EG, Thind H, Rosen RK, Salmoirago B, et al. Text messaging-based interventions for smoking cessation: a systematic review and meta-analysis. JMIR mHealth uHealth. 2016;4(2):e49. doi: 10.2196/mhealth.5436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Whittaker R, McRobbie H, Bullen C, Rodgers A, Gu Y, Dobson R. Mobile phone text messaging and app-based interventions for smoking cessation. Cochrane Database Syst Rev. 2019;1(1):1–87. doi: 10.1002/14651858.CD006611.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Barbosa AF. Survey on the Use of Information and Communication Technologies in Brazilian Households - ICT Households 2015. São Paulo: Brazilian Internet Steering Committee; 2015. https://www.cetic.br/media/docs/publicacoes/2/TIC_Domicilios_2014_livro_eletronico.pdf. Accessed 28 Oct 2019.
- 28.Brazilian Ministry of Health, National Cancer Institute - INCA. Approach and Treatment of Smokers: Consensus 2001. Rio de Janeiro: Prevention and Surveillance Coordination - CONPREV. 2001;1(1):1–38. https://www.inca.gov.br/sites/ufu.sti.inca.local/files//media/document//tratamento-consenso.pdf
- 29.Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Adv Behav Res Ther. 1978;1(4):139–161. doi: 10.1016/0146-6402(78)90002-4. [DOI] [PubMed] [Google Scholar]
- 30.Rollnick S, Butler CC, Kinnersley P, Gregory J, Mash B. Motivational interviewing. BMJ. 2010;340:c1900–c1900. doi: 10.1136/bmj.c1900. [DOI] [PubMed] [Google Scholar]
- 31.Kamakura W, Mazzon JA. Critérios De Estratificação E Comparação De Classificadores Socioeconômicos No Brasil. Rev Adm Empres. 2016;56(1):55–70. doi: 10.1590/s0034-759020160106. [DOI] [Google Scholar]
- 32.Fagerstrom K-O, Schneider NG. Measuring nicotine dependence: a review of the fagerstrom tolerance questionnaire. J Behav Med. 1989;12(2):159–182. doi: 10.1007/BF00846549. [DOI] [PubMed] [Google Scholar]
- 33.Hughes JR, Hatsukami D. Signs and symptoms of tobacco withdrawal. Arch Gen Psychiatry. 1986;43(3):289–294. doi: 10.1001/archpsyc.1986.01800030107013. [DOI] [PubMed] [Google Scholar]
- 34.DiClemente CC, Schlundt D, Gemmell L. Readiness and stages of change in addiction treatment. Am J Addict. 2004;13(2):103–19. doi: 10.1080/10550490490435777. [DOI] [PubMed] [Google Scholar]
- 35.Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the patient health questionnaire-4 (PHQ-4) in the general population. J Affect Disord. 2010;122(1–2):86–95. doi: 10.1016/j.jad.2009.06.019. [DOI] [PubMed] [Google Scholar]
- 36.(ACQUIP) for the ACQIP. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA. The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Arch Intern Med. 1998;158(16):1789–1795. doi: 10.1001/archinte.158.16.1789. [DOI] [PubMed] [Google Scholar]
- 37.SRNT Subcommittee on Biochemical Verification Biochemical verification of tobacco use and cessation. Nicotine Tob Res. 2002;4(2):149–159. doi: 10.1080/14622200210123581. [DOI] [PubMed] [Google Scholar]
- 38.Higgins AM, Harris AH. health economic methods: cost-minimization, cost-effectiveness, cost-utility, and cost-benefit evaluations. Crit Care Clin. 2012;28(1):11–24. doi: 10.1016/j.ccc.2011.10.002. [DOI] [PubMed] [Google Scholar]
- 39.Irvine L, Falconer DW, Jones C, Ricketts IW, Williams B, Crombie IK. Can text messages reach the parts other process measures cannot reach: an evaluation of a behavior change intervention delivered by mobile phone? PLoS ONE. 2012;7(12):1–7. doi: 10.1371/journal.pone.0052621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Suffoletto B. Text message behavioral interventions: From here to where? Curr Opin Psychol. 2016;9:16–21. doi: 10.1016/j.copsyc.2015.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Figure S1. Participant flow diagram.
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.