

Abstract
Objective:
To compare the rates of retraction down an archwire of maxillary canine teeth when bracketed with a self-ligating bracket was used on one side and a conventional bracket on the other.
Materials and Methods:
In 43 patients requiring maxillary premolar extraction, a self-ligating bracket (Damon3, SmartClip) was used on the maxillary canine on one side and a conventional bracket (Victory Series) on the other. The teeth were retracted down a 0.018-inch stainless steel archwire, using a medium Sentalloy retraction spring (150 g). The rates of retraction were analyzed using a paired t-test.
Results:
The mean movement per 28 days for the conventional bracket was 1.17 mm. For the Damon bracket it was 0.9 mm and for the SmartClip bracket it was 1.10 mm. The differences between the conventional and self-ligating brackets were statistically significant: paired t-test, SmartClip, P < .0043; Damon3, P < .0001).
Conclusion:
The retraction rate is faster with the conventional bracket, probably because of the narrower bracket width of the self-ligating brackets.
Keywords: Canine retraction, Self-ligating, Edgewise brackets
INTRODUCTION
Orthodontists, when moving a tooth down a wire, have to contend with biologic barriers and mechanical phenomena. Three of the mechanical phenomena are currently of interest because of the marketing of self-ligating brackets that are said to reduce resistance to sliding: friction, binding, and notching. These collectively determine the resistance to sliding a wire through a bracket or a bracket along a wire.
Friction is the resistance force between objects that oppose movement.1 It is always exerted in a direction opposing movement between the two surfaces. Friction is not a fundamental force, it cannot be calculated from fundamental principles; it must be calculated empirically. In contrast, moments or binding can be calculated using fundamental principles, eg, a binding force that equals the moment of a couple (MC) can be calculated using the equation MC = F/D.
Friction is the result of chemical bonding between surfaces. Surface area does not affect friction because as surface area increases, the force per unit area decreases (not to be confused with traction where surface area is important). On a microscopic scale, even highly polished surfaces of orthodontic brackets and wires are irregular, and the true area of physical contact is determined by asperities (Figure 1).2
Figure 1.

Wire-bracket interface. The surface is not smooth, but irregular. The areas of contact between the wire surface and bracket surface is determined by asperities.
In clinical orthodontics, we are dealing with a quasistatic thermodynamic process, which means the movements are very slow and fairly close to static equilibrium. Kusy and Whitley3 defined resistance to sliding (RS) as a combination of three components: friction (FR), binding (BI), and notching (NO):
FR, static or kinetic, is due to the contact forces between the wire, brackets, and ligatures;
BI is created as soon as the tooth begins to move and the wire contacts the edge of the bracket; and
NO occurs when permanent deformation of the wire occurs at the wire-bracket corner interface (Figure 2). Tooth movement stops as a notch in the wire catches on the bracket or when the binding angle increases to a point (θz) that plastic deformation occurs. Movement resumes only after the notch is released.
Figure 2.

Notching occurring when the wire catches due to deformation of the wire, ie, contact of a notch in the wire against the edge of the bracket: or, when binding reaches an angle in which plastic deformation occurs (θ > θz). When binding becomes sufficient to cause notching, sliding mechanics cease.
Consequently, RS = FR + BI, or RS = NO because sliding stops when NO begins. This equation can be applied to the passive and active stages of tooth movement in a laboratory setting. The passive stage of movement is when the contact angle (θ) between the archwire and bracket slot is less than the critical angle (θc) (Figure 3A) before the wire touches the corner of the bracket, and resistance to sliding is due only to friction.4 The passive stage really exists only in laboratory settings because as soon as a tooth moves in response to a force against its crown, it tips until the wire touches the corner of a bracket. In a laboratory setting, the investigator can stabilize the wire-bracket system in a fixed position, so the bracket does not tip and the wire does not flex (Figure 3B); ie, the wire-bracket system can be positioned so it does not have any forces whatsoever on it as the wire passes through the bracket. This never happens in clinical orthodontics because the wire actually touches the bracket as soon as tooth movement begins. The active stage is defined as any angle above θc (Figure 3C).
Figure 3.

(A) Passive stage of orthodontic tooth movement when the contact angle, θ, is less than the critical angle, θc. In the passive stage, the wire does not touch the edges. (B) In an experimental design, the wire can be stabilized so it does not move, and the wire can be stabilized so it cannot flex. The wire can actually be positioned so there are no forces whatsoever on the bracket-wire interface. This, however, never happens in clinical orthodontics. (C) This represents the active stage of orthodontic tooth movement when θ is more than θc, and the wires start to contact the corners of the bracket and binding starts.
Kusy reported the effect of binding and notching in the late 1990s. Articolo and Kusy5 concluded that the binding influence increased as the second-order angulation increased, which is in agreement with Nicolls and others.6–11 Articolo and Kusy further reported that “RS becomes dependent on BI very quickly, after the initiation of the active configuration.” “In fact BI was calculated to be at least 80% of RS at θ = 7° for all couples, and as much as 99% at θ = 13° for one couple (SS-SC).” Friction was hardly an influence.
In 2002, Thorstenson and Kusy12,13 reported two studies that investigated the effect of second-order angulation (binding) on self-ligating brackets. Both studies basically had the same conclusion. “RS increased proportionally with the second-order angulation”12 and the binding was “independent of bracket design.”13 Figure 4 shows the results when only friction is involved. Figure 5 shows the data for binding. Thorstenson14 concluded that “binding does not appear to be affected by ligation method,” ie, binding was the same with conventional and self-ligating brackets.
Figure 4.
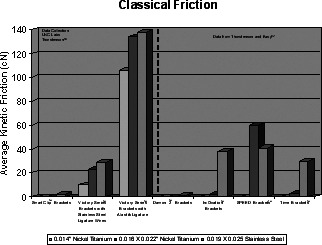
Classical friction results when only friction is involved.
Figure 5.
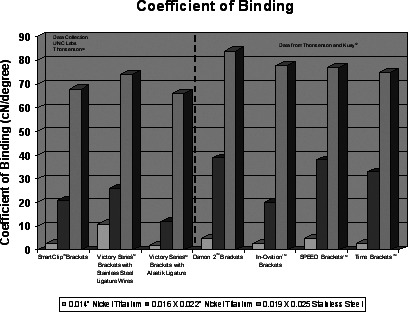
Coefficient of binding data.
These laboratory reports do not support advertising claims of faster tooth movement with self-ligating brackets. The goal of this clinical study was to compare the velocity of canine retraction with self-ligating brackets to conventional brackets.
MATERIALS AND METHODS
A sample size of 43 patients was used in this investigation (21 Damon3, 22 SmartClip, 43 conventional Victory Series).
The inclusion criteria for the study were as follows:
Class II malocclusion with proclined maxillary incisors or crowding, or Class I malocclusion with proclined maxillary and mandibular teeth;
treatment plan for extraction of maxillary first premolars and retraction of maxillary canines; and
excellent periodontal health.
All patients who met the inclusion criteria were entered into the study. Their demographic characteristics are shown in Table 1.
Table 1.
Demographic Characteristics of Sample

Each patient had a 0.022-inch slot conventional bracket placed on one canine and a 0.022-inch slot Damon3 or SmartClip bracket placed on the other, with the left or right side for the self-ligating bracket chosen using a randomization sequence. The molars were banded with Victory Series bands, and a transpalatal arch was placed. All remaining teeth were bracketed with Victory Series brackets. The arches were leveled and aligned before commencing canine retraction.
The canines were retracted using a GAC Sentalloy retraction spring (150 g). The conventional canine bracket was tied in with a stainless steel ligature. The retraction springs were attached to the bracket attachments. The SmartClip and Victory Series brackets have the attachments manufactured to the bracket, and the Damon3 attachment is manually placed and crimped to the bracket. Intra-arch mechanics were used and the canines were retracted down a 0.018-inch stainless steel wire. Patients were seen every 4 weeks (28 days).
All changes in the amount of retraction were measured intra-orally by the investigator using a flexible millimeter ruler. The amount of retraction was measured from the maxillary dental midline to the mesial of the canine. Each measurement was made four times and the results averaged. The measurements were made to the one-half millimeter.
The rate of retraction of the canines was defined as the distance traveled divided by the time interval needed for closure of the extraction space. The amount of retraction was measured at each appointment during space closure, but the only measurement used in this study was the distance traveled divided by the number of 28-day intervals until one of the canines was in the proper position; ie, the finish date for the retraction was when the extraction space was closed on one side (Figure 6).
Figure 6.

(A) Maxillary right canine retracted using GAC retraction spring (150 g). Canine in final position (SmartClip). (B) Maxillary right canine in final position (Damon). (C) Maxillary canine is retracted with conventional bracket (Victory Series).
A paired t-test was used to compare the retraction rates of the conventional bracket to those of the Damon3 and SmartClip bracket.
RESULTS
The amount of movement between appointments (28 days) for the three bracket types is shown in Table 2. The rate of movement for the conventional bracket side was greater than that for either of the self-ligating brackets, with the SmartClip bracket faster than the Damon3 bracket. Although the mean differences at successive appointments were small, the difference between the conventional bracket and both the self-ligating brackets was statistically significant on a paired t-test: SmartClip, P < .0043; Damon3, P < .0001.
Table 2.
Rate of Movement by Bracket Type

The average movement per 28 days was 0.27 mm faster with the conventional brackets than with the Damon bracket; it is statistically significant (P < .0001). The movement per 28 days was 0.07 mm faster with the conventional bracket than with the SmartClip bracket; this was also statistically significant (P < .0043). When the self-ligating brackets were combined and compared with the conventional bracket, the average movement per 28 days was 0.17 mm faster with the conventional; this was statistically significant (P < .0001). Although these average differences were small, they were statistically significant.
DISCUSSION
In comparing these results with those of other studies of the rate of tooth movement, several points described below should be considered.
Rate of Movement in This Study of Sliding Compared with Other Types of Tooth Movement
The properties that influence resistance to sliding are of great interest in the orthodontic community because lower resistance to sliding could lead to increased efficiency and possibly shorter treatment times. The force levels, size of the wire, and geometry of the bracket could have an impact on the efficiency of tooth movement.
Many studies of the relationship of force to tooth movement used closing loops. Although this does not directly compare to sliding mechanics, it provides some insight into the effect of force magnitude on the rate of tooth movement and the pattern of typical tooth movement. Boester and Johnston15 used sectional closing loops to retract canines in extraction situations using force levels of 60, 150, 240, and 330 g. Their objective was to study the rate of tooth movement at various force levels. Maxillary canine retraction was 0.8 mm/month for 60 g, 1.3 mm/month for 150 g, 0.8 mm/month for 240 g, and 1 mm/month for 330 g of force. They concluded that “space closure proceeds equally rapidly at forces ranging from five (possibly less) to eleven ounces. In this range, bone resorption, per se, appears to be occurring at a minimal rate and accordingly, may constitute the rate limiting factor.” Iwasaki et al.16 used sectional closing loops to retract canines and studied the velocity of tooth movement using force levels of 18 g and 60 g. When he used 60 g of force to retract canines, the velocity averaged 1.27 mm/month. With 18 g of force, the velocity was 0.87 mm/month, although there was quite a bit of individual variation. They concluded that “cell biology and metabolic factors must account for the variability in tooth movement.” From all three of these reports, it seems clear that once a level of force sufficient to produce a biologic response is present, the rate of tooth movement is a function of the biology, not the force magnitude.
The next studies investigated sliding mechanics. Paulson et al.17 measured canine retraction using sliding mechanics down a 0.016-inch wire. The retraction force was 50 g to 100 g. His sample averaged 1.08 mm/month, but individual velocities ranged from 0.7 mm/month to 2.4 mm/month. Huffman and Way18 did an vivo study to determine the amount of movement, rate of movement, and amount of tipping when retracting a canine down a 0.016-inch wire and a 0.020-inch wire using sliding mechanics. They used 200 g of force to retract the canine. The velocities were 1.37 mm/month when retracting down the 0.016-inch wire and 1.20 mm/month with the 0.020-inch wire. The difference was not significant. Sonis et al.19 used energy chains and latex thread to retract canines down a 0.016 × 0.022 inch archwire. The initial forces were 250–400 g. The mean velocity of tooth movement calculated over a 3-week period was 1.28 mm for elastic threads and 1.51 mm for the elastic chains. They concluded that “all the materials tested produced approximately equal amounts of tooth movement.”
Based on the above studies, it seems reasonable to have used 150 g of force when retracting canines along an undersized wire in this study.
Other Studies of Self-ligating vs Conventional Brackets
Advocates of self-ligating brackets recommend their bracket based on light forces, less friction, low moments, and consequentially more efficient (faster) tooth movement. Is there any evidence that these purported advantages are real?
Miles et al.20 compared the effectiveness of Damon and conventional twin brackets during initial alignment. This was a clinical trial using 60 consecutive patients in a split-mouth design. The irregularity index was measured at three times; original baseline, 10 weeks, and 20 weeks. The conventional bracket achieved a better irregularity index score at both 10 and 20 weeks. The authors reported that the difference in alignment could be due to the fact that the Damon bracket does not engage the initial wires and allows 8.5° of rotational play when compared with the conventional bracket. The second wire, a 0.016 × 0.025 inch archwire, was not fully engaged either. They surmised that the degree of rotational play involved in the Damon bracket attributed to the better alignment of the conventional bracket. Miles21 also compared SmartClip self-ligating brackets to conventional brackets and concluded that there was no difference in reducing crowding. Scott et al.22 did a randomized clinical trial comparing clinical effectiveness on mandibular tooth alignment comparing conventional brackets with Damon brackets and concluded that there was no difference in reducing crowding.
Pandis et al.23 compared the magnitude of moments generated during a laboratory-simulated rotational correction of teeth using three different brackets: Orthos 2, Damon2, and In-Ovation R. They found the highest moments were generated using the Damon bracket, and the conventional brackets generated the lowest moments. Thorstenson and Kusy12,14 also found Damon brackets to have higher binding forces (second-order angulation) compared with conventional brackets.
These studies comparing self-ligating brackets with conventional brackets all point to the same conclusion as this study, ie, ligation type makes little difference in initial alignment or space closure.
Bracket Geometry as a Factor in Resistance to Sliding
Hamdan and Rock,24 who investigated different combinations of torque and tip, reported that every 4-degree increase in bracket tip produced a significant increase in resistance to sliding. “RS was significantly increased by tip and torque separately and in combination, although tip was the more powerful influence.”
The amount of tip at the point of wire contact with the corner of a bracket is a function of bracket width. The Damon bracket is 2.67 mm wide, the SmartClip is 2.79 mm wide, and the Victory Series bracket is 3.81 mm wide. When a force is placed on the canine (or any other) bracket to move it down the archwire, a moment of force is created (MF). To counter the MF, a moment of a couple is created (MC). The MC is equal to the forces at the edges of the brackets times the width of the bracket. The maximum bending moment (MBM) when a tooth is moved down an archwire is MBM = (FWX)/L (Figure 7).
Figure 7.
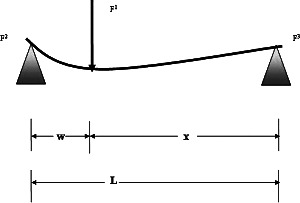
The beam illustration demonstrates the position of the maximum bending moment (MBM). The maximum bending moment is MBM = (FWX)/L.
To evaluate the effect the bracket width has on tooth movement down an archwire, we need to algebraically rearrange MC = FW to F = MC/W. Substituting the equation into the maximum binding moment gives us:
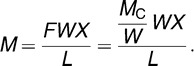 |
Substituting (L−W) for X gives us:
 |
which shows us that as the W (width) of the bracket increases, the maximum bending moment decreases. Consequently, a narrower bracket generates higher moments (higher forces at the edges) than a wider bracket. These increased forces could increase resistance to sliding. This concept already is incorporated into standard texts of orthodontics25 that advocate wider brackets for better sliding mechanics due to the decreased contact angle.
In this study, the average movement per 28 days was faster on the side being treated with the conventional bracket than on the side being treated with the self-ligating bracket. Although this is a statistically significant difference, clinically it probably would not matter. Even though bracket geometry, particularly bracket width, influences resistance to sliding, it still is important to keep in mind the limiting factor in the rate of tooth movement appears to be more the biologic response to the force than mechanical aspects of the orthodontic appliance.
CONCLUSION
Canine retraction by sliding the tooth along an undersized archwire tends to be faster with conventional than self-ligating brackets, probably because the narrower self-ligating brackets lead to greater elastic binding and resistance to sliding is much more determined by this than by friction.
Acknowledgments
I would like to thank Dr William R. Proffit for editorial assistance.
REFERENCES
- 1.Blau J. P. Tribology and Its Nomenclature in Friction and Wear Transitions of Materials. Park Ridge, NJ: Noyes Publications; 1989. [Google Scholar]
- 2.Jastrebski Z. B. The Nature and Properties of Engineering Materials 3rd ed. New York, NY: Wiley; 1987. [Google Scholar]
- 3.Kusy R. P, Whitley J. Q. Influence of archwire and bracket dimensions on sliding mechanics: derivations and determinations of the critical contact angles for binding. Eur J Orthod. 1999;21:199–208. doi: 10.1093/ejo/21.2.199. [DOI] [PubMed] [Google Scholar]
- 4.Kusy R. P. Ongoing innovations in biomechanics and materials for the new millennium. Angle Orthod. 2000;70:366–376. doi: 10.1043/0003-3219(2000)070<0366:OIIBAM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Articolo L. C, Kusy R. P. Influence of angulation on the resistance to sliding in fixed appliances. Am J Orthod Dentofacial Orthop. 1999;115:39–51. doi: 10.1016/S0889-5406(99)70314-8. [DOI] [PubMed] [Google Scholar]
- 6.Nicolls J. Frictional forces in fixed orthodontic appliances. Dent Pract. 1968;18:362–366. [PubMed] [Google Scholar]
- 7.Peterson L, Spencer and Andeasen G. F. Comparison of frictional resistance of Nitinol and stainless steel wires in edgewise brackets. Quint Inter Digest. 1982;13:563–571. [PubMed] [Google Scholar]
- 8.Frank C. A, Nikolai R. J. A comparative study of frictional resistance between orthodontic bracket and archwire. Am J Orthod. 1980;78:593–609. doi: 10.1016/0002-9416(80)90199-2. [DOI] [PubMed] [Google Scholar]
- 9.Andeasen G. F, Quevedo F. R. Evaluation of frictional forces in the 0.022 × 0.028 edgewise bracket in vitro. J Biomech. 1970;3:151–160. doi: 10.1016/0021-9290(70)90002-3. [DOI] [PubMed] [Google Scholar]
- 10.Sims A. P, Waters N. E, Birnie D. J. A comparison of the forces required to produce tooth movement ex vivo through three types of pre-adjusted brackets when subjected to determined tip or torque values. Br J Orthod. 1994;21:367–373. doi: 10.1179/bjo.21.4.367. [DOI] [PubMed] [Google Scholar]
- 11.Ogata R. H, Nanda R. S, Duncanson M. G, Jr, Sinha P. K, Currier G. F. Frictional resistances in stainless steel bracket-wire combinations with effects of vertical deflections. Am J Orthod Dentofacial Orthop. 1996;109:535–542. doi: 10.1016/s0889-5406(96)70139-7. [DOI] [PubMed] [Google Scholar]
- 12.Thorstenson B. S, Kusy R. P. Effect of archwire size and material on the resistance to sliding of self-ligating brackets with second-order angulation in the dry state. Am J Orthod Dentofacial Orthop. 2002;122:295–305. doi: 10.1067/mod.2002.126156. [DOI] [PubMed] [Google Scholar]
- 13.Thorstenson B. S, Kusy R. P. Comparison to resistance to sliding between different self-ligating brackets with second-order angulation in the dry and saliva states. Am J Orthod Dentofacial Orthop. 2002;121:472–482. doi: 10.1067/mod.2002.121562. [DOI] [PubMed] [Google Scholar]
- 14.Thorstenson G. A. Orthodontic Perspectives Vol XII No 1. Monrovia, CA: 3M Unitek; 2005. SmartClip self-ligating brackets frictional study; pp. 8–11. [Google Scholar]
- 15.Boester C. H, Johnston L. E. A clinical investigation of the concepts of differential and optimum force in canine retraction. Angle Orthod. 1974;44:113–119. doi: 10.1043/0003-3219(1974)044<0113:ACIOTC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Iwasaki L. R, Haack J. E, Nickel J. C, Morton J. Human tooth movement in response to continuous stress of low magnitude. Am J Orthod Dentofacial Orthop. 2000;117:175–183. doi: 10.1016/s0889-5406(00)70229-0. [DOI] [PubMed] [Google Scholar]
- 17.Paulson R. C, Speidel T. M, Isaacson R. J. A laminagraphic study of cuspid retraction versus molar anchorage loss. Angle Orthod. 1970;40:20–27. doi: 10.1043/0003-3219(1970)040<0020:ALSOCR>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Huffman J. D, Way D. C. A clinical evaluation of tooth movement along arch wires of two different sizes. Am J Orthod. 1983;83:453–459. [PubMed] [Google Scholar]
- 19.Sonis A. L, Van der Plas E, Gianelly A. A comparison of elastomeric auxiliaries versus elastic thread on premolar extraction site closure: an in vivo study. Am J Orthod. 1986;89:73–78. doi: 10.1016/0002-9416(86)90115-6. [DOI] [PubMed] [Google Scholar]
- 20.Miles P. G, Weyant R. J, Rustveld L. A clinical trial of Damon2 vs conventional twin brackets during initial alignment. Angle Orthod. 2006;76:480–485. doi: 10.1043/0003-3219(2006)076[0480:ACTODV]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Miles P. G. SmartClip versus conventional brackets for initial alignment: is there a difference? Aust Orthod J. 2005;21:123–127. [PubMed] [Google Scholar]
- 22.Scott P, DiBiase A. S. T, Sherriff M, Coburne M. T. Alignment efficiency of Damon3 self-ligating and conventional orthodontic bracket systems: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2008;134:470–471. doi: 10.1016/j.ajodo.2008.04.018. [DOI] [PubMed] [Google Scholar]
- 23.Pandis N, Eliades T, Partowi S, Bourauel C. Moments generated during simulated rotational correction with self-ligating and conventional brackets. Angle Orthod. 2008;78:1030–1034. doi: 10.2319/110307-516.1. [DOI] [PubMed] [Google Scholar]
- 24.Hamdan A, Rock P. The effect of different combinations of tip and torque on archwire/bracket friction. Eur J Orthod. 2008;30:508–514. doi: 10.1093/ejo/cjn017. [DOI] [PubMed] [Google Scholar]
- 25.Proffit W. R. Mechanical principles in orthodontic force control. In: Proffit W. R, Fields H. W, Sarver D. H, editors. Contemporary Orthodontics 4th ed. St Louis, Mo: Elsevier; 207. p. 376. [Google Scholar]