

Abstract
Objective:
To test the null hypothesis that surface treatment has no influence on the micro-shear bond strength between orthodontic composite resin cement and ceramics (feldspathic porcelain).
Materials and Methods:
Circular specimens of feldspathic porcelain were fabricated and randomly divided into six groups: (1) no treatment; (2) treatment with a mixture of acidic primer and silane agent for 20 seconds; (3) etching with 9.5% hydrofluoric acid; (4) etching with 9.5% hydrofluoric acid and coating with a mixture of acidic primer and silane agent for 20 seconds; (5) airborne-particle abrasion with 50-μm aluminum oxide; and (6) airborne-particle abrasion and coating with a mixture of acidic primer and silane agent for 20 seconds. The porcelain disks were then bonded to resin cylinders with composite resin cement. A micro-shear bond test was carried out to measure the bond strength. Moreover, each ceramic surface was observed morphologically by scanning electron microscopy. One-way analysis of covariance was used to compare the groups for differences in micro-shear bond strength.
Results:
The mean micro-shear bond strength varied as a function of surface treatment. It ranged from 3.7 to 20.8 MPa. The highest values for micro-shear bond strength were found when the surface was acid-etched with hydrofluoric acid and coated with silane. On the other hand, the control group (no treatment) had significantly lower micro-shear bond strength than all the other groups.
Conclusion:
The null hypothesis that the surface treatment has no influence on the micro-shear bond strength of orthodontic composite resin was rejected. The bond strength between ceramics and orthodontic resin cement is affected by the ceramic surface treatment. The bond failure was of the adhesive type, except with the hydrofluoric acid + silane group, where it was a cohesive bond failure.
Keywords: Orthodontic resin, Cementation, Surface treatment, Shear bond strength, Acid etching, Abrasion
INTRODUCTION
Dental ceramics have increasingly become the material of choice for achieving natural-looking restorations that can substitute for destroyed or missing anterior teeth.1,2 These materials have desirable characteristics, such as chemical stability, biocompatibility, high compressive strength, and a coefficient of thermal expansion that is similar to that of natural tooth structure, thereby producing more natural restorations.
According to the NHANES III data, the frequency of malocclusion in adults in the United States is around 50%.3 The prevalence of malocclusion in Western European adults is between 40% and 76%.4 Data from previous research indicate that the prevalence of malocclusion in adults is equal to or greater than that of children and adolescents.5 With the increase in adult orthodontic treatment comes the need to find a reliable method for bonding orthodontic brackets onto metal or ceramic restorations. Over the past few years, a number of mechanical and chemical retention systems have been developed to achieve satisfactory bond strength between adhesives and ceramics. Organosilane coupling agents have been reported to increase the bond strength of composite resin to porcelain.6 It has even been reported that airborne-particle abrasion (APA) and acid etching with hydrofluoric acid (HF) increase the surface area of ceramic surfaces and create an irregular topography that enhances the potential for micromechanical retention of the adhesive cement. However, HF has been found to be harmful and can irritate the soft tissues; therefore, clinicians should be cautious when using it in the oral cavity.
Few studies have reported on the bond strength of orthodontic composite resin to feldspathic porcelain. Moreover, the micro-shear bond strength (MSBS) of orthodontic composite resins to most porcelain surfaces has been reported to be inadequate. Therefore, the purpose of this in vitro study was to compare the MSBS of orthodontic composite resin bonded to a feldspathic porcelain disk prepared by six different surface treatments and to ascertain whether surface treatment has any significant effect on the overall shear bond strength. Additionally, the conditioned surfaces were evaluated by scanning electron microscopy (SEM). The null hypothesis was that different surface treatment methods have no significant influence on the MSBS of the orthodontic composite resin.
MATERIALS AND METHODS
Bonding Procedure
Thirty-seven circular specimens (6 mm in diameter and 4 mm in thickness) of feldspathic porcelain were divided into six different groups according to the surface treatment. Group 1 included seven circular specimens, whereas the other groups were made up of six circular specimens (Table 1).
Table 1.
Surface Treatments Applied to Each Group of Disks

Group 1: Specimens were not given any additional surface treatment (control).
Group 2: Specimens were treated with a mixture of acidic primer and silane coupling agent (Kuraray Co, Osaka, Japan) for 20 seconds.
Group 3: Specimens were treated with 9.5% HF (Ultradent, South Jordan, Utah) for 60 seconds (according to the manufacturer's instructions). Subsequently, the specimens were washed with tap water for 1 minute, ultrasonically cleaned in a water bath for 10 minutes, and air dried.
Group 4: Similar to group 3, the specimens were etched with 9.5% HF (Ultradent). After etching, the specimens were washed under tap water for 1 minute, ultrasonically cleaned in a water bath for 10 minutes, and air dried. After air drying, a mixture of acidic primer and silane agent (Kuraray Co) was applied to the ceramic surface for 20 seconds.
Group 5: Specimens were treated with APA with 50-μm aluminum oxide for 5 seconds at 4 bar pressure. Because the distance of the abrasion tip from the ceramic surface can affect surface topography, it was maintained at a fixed distance of 4 mm for all specimens. Following ABA, the specimens were washed with tap water for 1 minute, ultrasonically cleaned in a water bath for 10 minutes, and air dried.
Group 6: Specimens were treated with APA with 50-μm aluminum oxide for 5 seconds at 4-bar pressure, with the distance of the tip from the ceramic surface kept at 4 mm. The specimens were then washed with tap water for 1 minute, ultrasonically cleaned in a water bath for 10 minutes, and air dried. After air drying, a mixture of acidic primer and silane agent (Kuraray Co) was applied to the surfaces for 20 seconds.
To prepare the orthodontic adhesive (Transbond Light Cure Adhesives, 3M Unitek, Monrovia, Calif) for cementation, adhesive was directly used to fill an iris that was cut from microbore Tygon tubing (TYG-030, Small Parts Inc, Miami Lakes, Fla) with internal diameter and height of approximately 1 mm and 0.5 mm, respectively (Figures 1 and 2). The Tygon tubing containing the composite resin was put on the ceramic surface and light-cured for 40 seconds. In this manner, each ceramic surface was bonded at four different locations with the resin cylinders. The assembly of porcelain plus composite resin was stored at room temperature (23°C ± 2°C) for 1 hour prior to removal of the Tygon tubing. Subsequently, the specimens were immersed in water at 37°C for 24 hours before testing for MSBS. The bonding procedures were carried out by the same operator in accordance with the manufacturers' instructions.
Figure 1.

Formation of resin cylinders on ceramic surfaces.
Figure 2.

Sketch depicting the bond strength testing procedure.
Micro-Shear Bond Testing
Before the test, all porcelain/resin cylinder interfaces were checked under an optical microscope at 20× (Olympus, Tokyo, Japan) for bonding defects. Any cylinders that showed apparent interfacial gaps, bubbles, or any other defects were excluded and replaced by other cylinders. The assembly of the round porcelain disk and the composite resin was attached to the testing device using cyanoacrylate adhesive (Superbond, Loctite, Hunt Valley, Md), which in turn was placed in a universal testing machine (MTS Sine Tech Re New 1123, MTS Systems Corp, Eden Prairie, Minn) for shear bond testing (Figure 2). An edge of stainless steel, 0.5 mm in thickness, was fixed on the superior part of the universal testing machine and was gently adapted against the ceramic/resin cement interface. A shear force was applied to each specimen at a crosshead speed of 0.5 mm/min until failure occurred.
Two specimens from each group were gold coated with a sputter coater (Balzers-SCD 050, Balzers Union Aktiengeselischaft Fuürstentun, Liechtenstein) for 180 seconds at 40 mA and they were examined using SEM (LEO 435 VP, Cambridge, England) at 20 Kv by the same operator (Figures 3 and 4).
Figure 3.
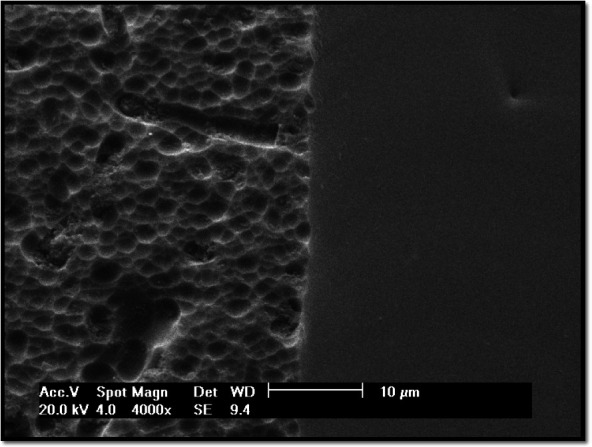
Comparison of HF-treated ceramic with a glazed (control) ceramic under SEM.
Figure 4.
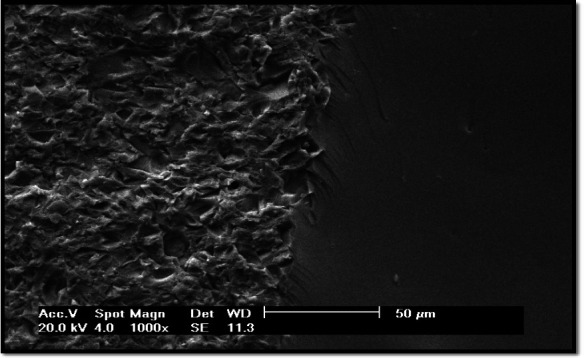
Comparison of APA ceramic with a glazed ceramic under SEM.
Statistical Methods
One-way analysis of variance was used to compare the groups for differences in failure strength. Because the failure strength measurements were not normally distributed, a transformation of the data (natural logarithm) was used for the analyses to satisfy the analysis of variance assumptions.
RESULTS
The results are shown in Tables 2 and 3 and Figure 5. The MSBS values ranged from a minimum of 0.7 MPa for the control group to a maximum of 35.5 MPa for the HF/silane-treated group. The mean MSBS was 20.8 MPa for the HF/silane-treated group. The control had significantly lower mean MSBS (P < .01) than all other groups. Silane had a significantly different mean MSBS than HF (P = .0187), APA (P < .0001), APA/silane-treated (P < .0001), and HF/silane-treated (P < .0001). The HF-treated specimens had significantly lower mean MSBS than APA/silane-treated (P < .0191) and HF/silane-treated (P < .0001) disks and a marginally lower mean MSBS than APA specimens. APA and APA/silane-treated disks had significantly lower failure stress than did HF/silane-treated disks (P = .0006 and P = .006, respectively).
Table 2.
Micro-Shear Bond Strength of Different Groups

Table 3.
Differences in Micro-Shear Bond Strength Between Groups

Figure 5.

Graph depicting MSBS values of different groups.
APA and APA/silane-treated disks (P = .469) were not significantly different from each other. It was also noted the bond failures for all the specimens, except for the HF/silane group, were of the adhesive type, whereas the HF/silane specimens revealed a cohesive type of bond failure (Figures 6 and 7).
Figure 6.
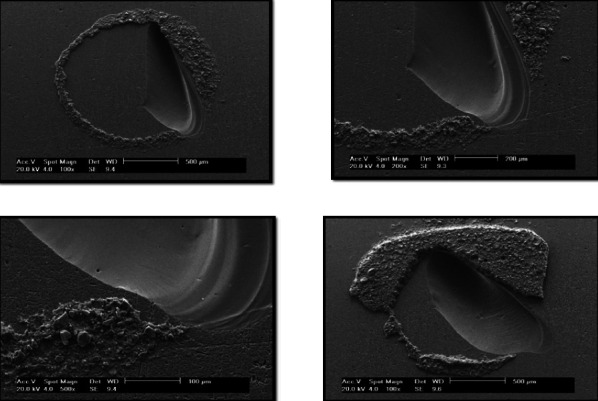
HF/silane-treated specimen under SEM.
Figure 7.
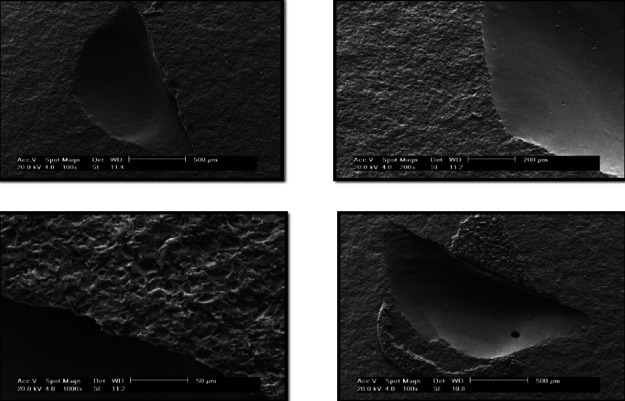
APA/silane-treated specimen under SEM.
DISCUSSION
The null hypothesis of this study—that surface treatment of feldspathic porcelain has no influence on the MSBS of the orthodontic composite resin—was rejected. The results showed that the MSBS varied as a function of surface treatment. Adequate bond strength between a metal bracket and enamel is in the range of 6 to 8 MPa.7 Except for the control group, all the mean values of MSBS between composite resin and feldspathic ceramic were either within or above the optimal range.
The previous literature has suggested the effectiveness of silane coupling agents in establishing a bond between resin and a ceramic surface.6 Acid catalysis increases the bond strength of adhesive cement to ceramics treated with silane because of the initiation and formation of a siloxane bond between the silane coupling agent and the ceramic surface. The current research confirms this finding, where ceramic treated with a mixture of acidic primer and silane showed a significantly greater MSBS than control ceramic samples that were left untreated; similarly, HF/silane and APA/silane treatment of ceramic resulted in a significantly greater MSBS than treatment with HF and APA alone, respectively.
In all the groups except HF/silane, adhesive failures between the porcelain and composite resin were seen. Adhesive failures at the porcelain/composite interface are preferred to avoid porcelain fractures during debonding. It has been reported that if the composite/porcelain bond strength is above 13 MPa, cohesive failure is seen in the porcelain; however, in the present study, although the APA group (13.5 MPa) and the APA/silane group (14.3 MPa) had a mean MSBS slightly higher than 13 MPa, adhesive failure was observed between the porcelain and the composite resin.8 The HF/silane group had a mean MSBS (20.8 MPa) that was significantly higher than all the other groups and showed a cohesive failure in the porcelain. This finding indicates that clinicians should be extremely cautious when using the HF/silane method to prepare porcelain, because debonding may result in a fracture or a crack in the porcelain surface.
In the present study tests of MSBS were performed between an orthodontic adhesive and feldspathic porcelain. This methodology involved small bonding surface areas and a uniform distribution of stress; when compared to the micro-tensile bond test, trimming of the sample after the bonding procedure is not necessary. Aside from this, preparing specimens for this test is easy and multiple samples can easily be made, even using brittle materials. Although Shimada et al.9 used a thin wire (diameter of 0.20 mm) looped around the resin cylinder to carry out MSBS testing, a pilot experiment indicated no difference in using a wire or a stainless steel edge.
Because this is an in vitro study, extrapolation of the current findings to the clinical situation must be done with caution. Furthermore, in clinical situations, the bonds between the composite resin and porcelain are influenced by additional oral environmental factors, eg, saliva, forces of mastication, type of stress being applied, etc. Nevertheless, these in vitro studies can be used to compare mean MSBS values of different composite resins and thus can suggest clinical usage. Further research with other composite resins and ceramics is indicated to effectively compare the mean MSBS values of different composite resins.
CONCLUSIONS
The mean MSBS varied as the function of surface treatments. The mean MSBS values were between 3.7 and 20.8 MPa and were adequate for all groups except for the control group.
The HF/silane-treated group had a significantly greater MSBS than all the other groups. The MSBS values were greatest for HF/silane-treated, followed by APA/silane-treated, APA, HF-treated, silane-treated, and the control group.
The MSBS values of the APA specimens and the APA/silane-treated specimens were not significantly different from each other.
A silane coupling agent effectively increased the mean MSBS between orthodontic adhesive and feldspathic porcelain.
REFERENCES
- 1.Heydecke G, Thomason J. M, Lund J. P, Feine J. S. The impact of conventional and implant supported prostheses on social and sexual activities in edentulous adults. Results from a randomized trial 2 months after treatment. J Dent. 2005;33:649–657. doi: 10.1016/j.jdent.2005.01.003. [DOI] [PubMed] [Google Scholar]
- 2.Raptis N. V, Michalakis K. X, Hirayama H. Optical behavior of current ceramic systems. Int J Periodontics Restorative Dent. 2006;26:31–41. [PubMed] [Google Scholar]
- 3.Proffit W. R, Fields H. W, Jr, Moray L. J. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998;13:97–106. [PubMed] [Google Scholar]
- 4.Salonen L, Mohlin B, Gotzlinger B, Hellden L. Need and demand for orthodontic treatment in an adult Swedish population. Eur J Orthod. 1992;14:359–368. doi: 10.1093/ejo/14.5.359. [DOI] [PubMed] [Google Scholar]
- 5.McLain J. B, Proffitt W. R. Oral health status in the United States: prevalence of malocclusion. J Dent Educ. 1985;49:386–397. [PubMed] [Google Scholar]
- 6.Lacy A. M, LaLuz J, Watanabe L. G, Dellinges M. Effect of porcelain surface treatment on the bond to composite. J Prosthet Dent. 1988;60:288–291. doi: 10.1016/0022-3913(88)90270-3. [DOI] [PubMed] [Google Scholar]
- 7.Oliver B. M, Dujovne A. R. Shear strength of APC brackets bonded to extracted teeth. A pilot study. Orthod Cyber J. http://www.oc-j.com/issue2/liver2a.htm. Accessed on June 19, 2009. [Google Scholar]
- 8.Piascik J. R, Swift E. J, Thompson J. Y, Grego S, Stoner B. R. Surface modification for enhanced silanation of zirconia ceramics. Dent Mater. 2009;25:1116–1121. doi: 10.1016/j.dental.2009.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shimada Y, Yamaguchi S, Tagami J. Micro-shear bond strength of dual-cured resin cement to glass ceramics. Dent Mater. 2002;18:380–388. doi: 10.1016/s0109-5641(01)00054-9. [DOI] [PubMed] [Google Scholar]