

Abstract
Objective:
To demonstrate the three-dimensional (3D) orthodontic force systems of three commercial closing T-loop archwires using a new method and to quantify the force systems of the T-loop archwires.
Materials and Methods:
An orthodontic force tester (OFT) and a custom-made dentoform were developed to measure force systems. The system simulated the clinical environment for an orthodontic patient requiring space closure, which included measurement of three force components along, and three moment components about, three clinically defined axes on two target teeth. The archwires were attached to the dentoform and were activated following a standard clinical procedure. The resulting force system was measured using the OFT.
Results:
The force systems of the T-loops on the teeth were 3D. Activation in one direction resulted in force and moment components in other directions (side effects). The six force and moment components as well as the moment-to-force ratios in the clinically defined coordinate system were quantified.
Conclusions:
The commercial archwires do not provide force systems for pure translation. Quantification of the force system is critical for the selection and design of optimal orthodontic appliances.
Keywords: Orthodontic force system, Biomechanics
INTRODUCTION
The control of orthodontic movement relies on the ability to quantify and manipulate the force system, specifically the moment-to-force ratio (M/F). Small differences in M/F can produce different clinical results.1,2 The inability to control the orthodontic force system can result in undesirable tooth movement, which reduces overall treatment efficiency.
However, quantification of the force system delivered by a continuous closing loop archwire has only been studied on a limited basis. Various experimental or computational studies3–8 have been performed on the force systems. These studies4–6 have concluded that the force system is multifactorial and can be adjusted, and a 3D analysis is needed to study the force system of an archwire.8 However, they have not contributed much to the understanding of the continuous closing archwires, because either the data were obtained with segmented appliances in a two-dimensional space or the archwires were tested under nonclinical conditions.4–6,9–11
A segmental wire provides force systems on two teeth that are equal in magnitude but opposite in direction. However, an archwire is commonly attached to more than two teeth. The force systems on the two teeth adjacent to the space are affected by constraints from their neighboring teeth; thus, the force systems from these two kinds of appliances are different. Furthermore, most previous studies5–7 fixed the appliance to the brackets rigidly, whereas ligature ties are currently used in clinical settings. The archwires are secured firmly—not rigidly—with stainless-steel or elastomeric ligature ties. Recent data10 clearly demonstrate that the force system of an appliance depends heavily on the ligation method. Therefore, the clinical ligation method needs to be simulated in order to accurately measure the force system.
Currently, archwire selection has not been based on the force system that the springs can deliver but rather on personal trial-and-error experience and preference. Quantification of the 3D force system with a continuous closing loop archwire will allow the clinician to make an informed decision when selecting the archwires. The objectives of this study were to describe the technology and to evaluate the force systems of the commercial T-loop archwires.
MATERIALS AND METHODS
An orthodontic force tester was developed.12 Together with a custom-made dentoform made of autopolymerizing acrylic (Duralay, Reliance Dental Mfg Co, Worth, Ill), treatment of a space closure after first premolar extractions and canine retractions was simulated (Figure 1). For this purpose, the system allowed attachment of a clinically used orthodontic appliance to the full dentoform, activation of the appliance following established procedures, and measurement of the force systems on target teeth to be moved or to serve as an anchor.
Figure 1.
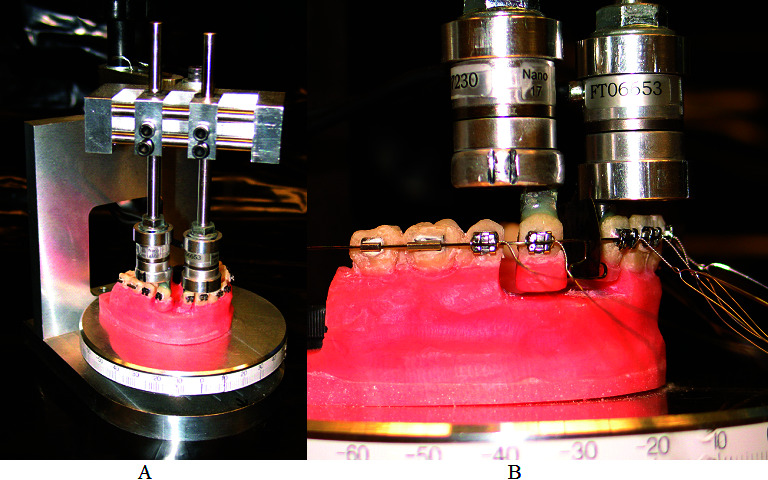
The orthodontic force tester used to measure three-dimensional (3D) load systems on the canine and incisor by a T-loop archwire. (A) Orthodontic force tester (OFT). (B) The T-loop archwire ligated to the brackets. The canine and lateral incisor were, respectively, separated from the rest of the typodont and attached to the load cells. The experimental setup allows simulation of the space closure cases.
The orthodontic force tester consisted of two load cells (Multi-axis force/torque Nano17, ATI Industrial Automation, Apex, NC). The force range of each load cell was 0–20 N, with a ±0.025 N resolution, and the moment range was 0–100 N-mm, with a ±0.003 N-mm resolution. These ranges are adequate because commonly used clinical force and moment fall into the load cell's range with proper resolutions.13,14 The load cells were able to measure three force and three moment components simultaneously.
The dentoform was fixed to a platform (Figure 1). The target teeth (left canine and left lateral incisor) were attached to the load cells and were then separated from the dentoform. In this way, their original positions and orientations with respect to the remainder of the dentoform were maintained. The design ensured that the boundary condition of the lab model was the same as that in the clinic.
The load cells were aligned with the clinically used coordinate system, the origin of which was at the center of the bracket. The x-axis was directed buccally (normal to the crown and pointing toward the cheek), the y-axis distally (tangent to the crown and pointing toward the molar), and the z-axis apically (perpendicular to the x–y plane and pointing toward the root). The definition was good for only the left quadrant of the maxilla teeth. The dentoform base was parallel to the bracket slots, which allowed the occlusogingival (OG) axes of the target teeth to be parallel to the z axis. The transducers were further positioned so that buccolingual (BL) and mesiodistal (MD) axes of each target tooth corresponded to the x and y axes, respectively. The directions (OG, BL, and MD) are clinical terms to describe tooth displacements.
The T-loop closing archwires (0.016 × 0.022-inch Stainless Steel Natural Form Arch, Oscar Inc, Fishers, Ind) in interloop distances of 38 mm, 42 mm, and 46 mm were tested. The 42-mm T-loop closing archwire (TL42) positioned the T-loop in the middle of the interbracket distance of the lateral incisor and canine brackets. The 38-mm (TL38) and the 46-mm (TL46) archwires positioned the T-loop 2 mm anterior and 2 mm posterior to the middle of the interbracket distance, respectively.
Three measurements were made for each archwire. The OFT was zeroed before placing the closing loops. An archwire was placed on the dentoform, with the vertical legs separated by a 0.05-mm metal shim to maintain a consistent baseline. The closing loop archwire was secured to each bracket with 0.010-inch stainless-steel ligature wires (Figure 1). Crimpable stops were secured distal to the second molar tubes bilaterally. The resulting orthodontic force system (Fx, Fy, Fz, Mx, My, and Mz) on the tooth was measured as the baseline. The closing loops were activated using 1-mm and 2-mm shims between the crimpable stop and the molar tubes bilaterally. Measurements were made after all activations.
To assess variation due to operating errors, such as variation of ligature tie tightness, activation level, and wire shape, etc, experiments on each type of archwire were repeated on five wires with the same specifications. The average and standard deviation were computed to statistically determine the load components and their variations. A two-way full-factorial analysis of variance model was used to assess the effect of activation amount (1 mm or 2 mm) and location of the T-loop on the resulting forces and moments. A separate analysis was performed for each tooth sensor. A significance level of .05 was used to test all hypotheses.
RESULTS
The six load components were measured for both the left maxillary lateral incisor and the canine. T-loop archwires corresponding to three loop locations (TL38, TL42, and TL46) were evaluated. The force and moment components corresponding to 1-mm and 2-mm activations and their standard deviations are shown in Figures 2 and 3, respectively. The positive Fx was directed buccally. That component was responsible for a buccal (if it was positive) or lingual (if it was negative) crown tipping (first-order tipping). Similarly, the positive Fy was directed distally. That component caused a mesial (if it was negative) or distal (if it was positive) crown tipping (second-order tipping). The positive Fz was directed apically (toward the root). This component resulted in an intrusion (if it was positive) or extrusion (if it was negative) (Figure 2). The moment components were responsible for tooth rotations about the corresponding coordinate axes. The moment about the x-axis, Mx, created a second-order rotation. The positive Mx rotated the crown distally. The moments about the y-axis, My, caused a first-order rotation. The positive My rotated the crown lingually. Similarly, the moments about the z-axis, Mz, created a third-order rotation. The positive Mz caused distal-crown-in rotation (Figure 3).
Figure 2.
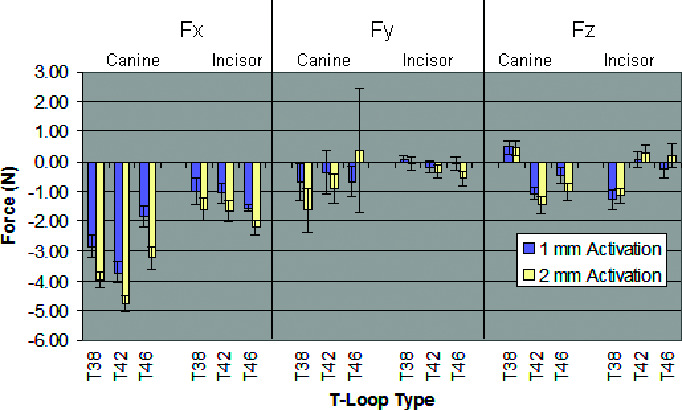
Three force components of the three T-loops on the canine and lateral incisor corresponding to 1 mm and 2 mm of activations.
Figure 3.
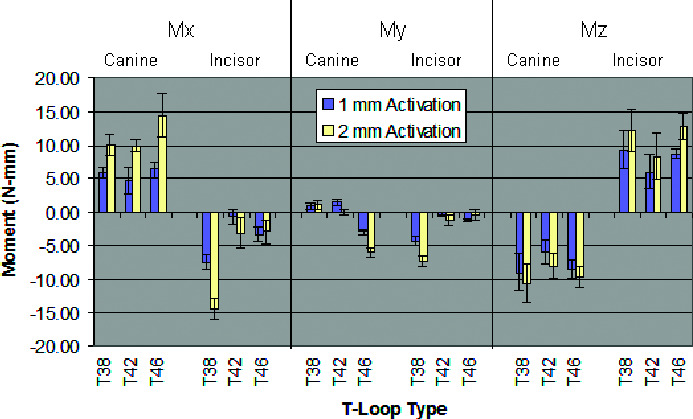
Three moment components of the three T-loops on the canine and lateral incisor corresponding to 1 mm and 2 mm of activations.
The activation of the spring in the distal direction resulted in force and moment components in all three directions. For all the loops, Fx was negative (against the crown) for all three archwires (TL38, TL42, and TL46). The force increases linearly with the activation (Figure 2). The force was higher on the lateral incisor. Fy was low (less than 0.6 N), primarily on the incisor side. The force component on the canine side was negative (directed mesially) at 1-mm and 2-mm activations. The magnitude increased linearly with the activation for the TL38 and TL42 cases (Figure 2). In the z direction, the sign of Fz was controlled by the loop location. For all the wires, the force components on the two target teeth had different signs. Mx was positive on the canine and negative on the incisor (Figure 3). However, the sign of My depends on the loop location. For example, My on the canine was positive for the TL38 and TL42 wires and negative for TL48. Finally, Mz was negative on the canine and positive on the incisor (Figure 3).
The location of the T-loop had a significant effect on all of the forces and moments except for the Fy force on the canine tooth (Figures 2 and 3). The amount of activation also had a significant effect on all of the outcomes except, again, for the Fy force on the canine tooth. The two-way analysis of variance additionally assessed if there was a multiplicative effect between the T-loop location and the amount of activation. In the case of the Mx moment on the incisor and the My moment on both the canine and incisor teeth, there was a significant interaction between location and activation.
DISCUSSION
As a result of ligation there were initial values for all the load components corresponding to the zero activation. These values were small compared to the corresponding components at 1-mm and 2-mm activations. Since zero activation is not used clinically, the associated force values are not reported here.
There were variations in the measured force and moment components (Figures 2 and 3). The variations were primarily due to the following inevitable factors: forces for tightening the stainless-steel ligature wire, archwire shape, and activations. These factors were accounted for in the statistical evaluations. The variations were, in general, small with respect to the means. Large variations on Fy and Mx occurred for the TL46 wires, especially corresponding to the 2-mm activation. This was because the loop was too close to the canine bracket at the level of activation, such that the loop interfered with the bracket and resulted in an unstable force system. This loop location and activation must be discouraged clinically, because an unstable force system may result in an unpredictable tooth displacement.
Clinical control of tooth displacement is determined by the design or selection of appropriate appliances, which requires knowledge of M/F ratios in all three directions.15 Furthermore, the magnitude of the force needs to be restricted within a certain range for the best clinical effects.13 For the first time, all six components of the force systems of the three archwires were quantified experimentally. The force increased linearly with the activation. Each type of archwire had a distinct force system. Activation in the distal direction results in force and moment components in both BL and OG directions, which may cause undesired tooth displacement components. These unwanted components are side effects that need to be eliminated.
Understanding of the 3D force system influences the clinical decision of choosing the appliances. For all of the loops, the dominant force component was Fx. Compressive Fx against the crown was observed for all three archwires (TL38, TL42, and TL46). The force was higher on the lateral incisor. It reached 5 N with 2-mm activation. Consequently, a large moment My would be needed if translation was required. Distal force, Fy, was low primarily on the incisor side, which would not be sufficient for its distal movement. The mesial force was on the canine side. The force component reached 1.6 N at 2-mm activation for TL38, meaning the posterior segment would be protracted. In the OG direction, the forces on the two target teeth had different signs when an archwire was activated, meaning if one tooth was extruded, then the other one was intruded. The TL38 wire extruded the incisor and intruded the canine, while the TL42 wire showed the opposite, meaning selection of loop location could adjust the force component (Figure 2). The dominant moment component was Mx. Positive Mx on the canine rotates the crown distally, which counters the tipping created by a mesially directed Fy. Negative Mx on the incisor balances the moment created by distally directed Fy. The TL38 wire created the largest Mx on the lateral incisor, while the TL46 wire generated the largest Mx on the canine, meaning the component is sensitive to the loop location. The Mx/Fy controlled the translation or tipping in the MD direction. The low Fy on the incisor contributed to a large Mx/Fy (see Table 1). In the BL direction, a negative My on the incisor counters the moment created by the negative Fx, meaning that only a positive My/Fx may reduce the tipping caused by Fx, and a negative ratio will enhance the lingual crown tipping. Although most My/Fx were positive, their values were low, which means they were not sufficient to translate the teeth (Table 1). Finally, Mz from the three archwires was high, which created a high Mz/Fy as a result of low Fy. This would produce a distal-crown-out rotation for the canine and a mesial-crown-out rotation for the lateral incisor (Figure 3). This knowledge helps one to select appliances for a clinical need, which will not be possible without the quantification of the 3D force system.
Table 1.
Moment-to-Force (M/F) Ratios of the Three Types (TL38, TL42, TL46) of T-Loop Archwires. Values Presented Are the Average M/F Ratios. N = 5 in All Cases

The measured 3D force system confirmed some of the conclusions from previous two-dimensional studies and revealed new information on coupling effects. When a T-loop is placed eccentrically in the space to be closed, the moment, Mx, is higher on the tooth closer to the loop (Figure 3), confirming the conclusion made by Burstone and Koenig.16 In this study, coupling effects were quantified when the loop was activated distal to the molars. A large force, Fx, in BL direction was generated against the crown, causing the teeth to tip crown-in. If the desired tooth displacement was translation, there was not enough correction moment, My (low My/Fx), causing tipping (Table 1). The intrusion/extrusion force, Fz, would also occur depending on the loop locations. Placing the loop mesially (TL38) would extrude the incisor and intrude the canine, while placing the loop in the middle (TL42) or distally (TL46) showed an opposite effect (Figure 2). Thus, adjusting the loop location could be used as a method to control intrusion and extrusion. The force in the MD direction, Fy, was generally small on the incisor side. Large Fy would be needed if the incisor was prescribed to be translated distally. An understanding of coupling effects is important for estimating potentially unwanted displacement, which cannot be quantified in two-dimensional models. The results demonstrated that the 3D force systems would need to be quantified so that they could be manipulated quantitatively in order to control tooth displacement and to reduce undesirable side effects.
It is beneficial for clinicians to use an appliance with predictable clinical outcomes. This kind of appliance will result in fewer side effects and fewer office visits, which greatly benefits both the orthodontist and the patient. For example, the TL42 at a 2-mm activation produced a ratio of −10.9 mm for Mx/Fy and a ratio of 0 for My/Fx (see Table 1). If a desired M/F ratio for translating the tooth is 8 for Mx/Fy and My/Fx, then the force system would overcorrect the tipping in the MD direction and tip the canine crown-in in the BL direction. If the desired tooth movement is translation, which is a common requirement for space closure, the archwire does not meet that requirement. However, the M/F can be adjusted to the target values by introducing gable angles,6 different loop locations, and activations.4 Future studies should be conducted to investigate the effects of the gable bends on the force system.
CONCLUSIONS
The proposed method can quantify 3D force systems of an archwire under a simulated clinical condition.
All three commonly used T-loop archwires produce 3D force systems. The force systems are tooth specific and dependent on loop location.
Significant coupling effects occur when a distal activation is applied; these effects need to be quantified in order to control the unwanted side effects.
The commercial archwires do not provide force systems for pure translation.
Quantification of the force system is critical for the selection and design of optimal orthodontic appliances.
Acknowledgments
The study was supported by grant NIH-NIDCR R41-DE017025.
REFERENCES
- 1.Smith R. J, Burstone C. J. Mechanics of tooth movement. Am J Orthod. 1984;85:294–307. doi: 10.1016/0002-9416(84)90187-8. [DOI] [PubMed] [Google Scholar]
- 2.Gjessing P. Controlled retraction of maxillary incisors. Am J Orthod Dentofacial Orthop. 1992;101:120–131. doi: 10.1016/0889-5406(92)70003-S. [DOI] [PubMed] [Google Scholar]
- 3.Braun S, Garcia J. L. The gable bend revisited. Am J Orthod Dentofacial Orthop. 2002;122:523–527. doi: 10.1067/mod.2002.126727. [DOI] [PubMed] [Google Scholar]
- 4.Chen J, Bulucea I, Katona T. R, Ofner S. Complete orthodontic load systems on teeth in a continuous full archwire: the role of triangular loop position. Am J Orthod Dentofacial Orthop. 2007;132:e141–e148. doi: 10.1016/j.ajodo.2006.10.016. [DOI] [PubMed] [Google Scholar]
- 5.Chen J, Markham D. L, Katona T. R. Effects of T-loop geometry on its forces and moments. Angle Orthod. 2000;70:48–51. doi: 10.1043/0003-3219(2000)070<0048:EOTLGO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Katona T. R, Le Y. P, Chen J. The effects of first- and second-order gable bends on forces and moments generated by triangular loops. Am J Orthod Dentofacial Orthop. 2006;129:54–59. doi: 10.1016/j.ajodo.2004.10.009. [DOI] [PubMed] [Google Scholar]
- 7.Kuhlberg A. J, Burstone C. J. T-loop position and anchorage control. Am J Orthod Dentofacial Orthop. 1997;112:12–18. doi: 10.1016/s0889-5406(97)70268-3. [DOI] [PubMed] [Google Scholar]
- 8.Isaacson R. J, Lindauer S. J, Conley P. Responses of 3-dimensional arch wires to vertical v-bends: comparisons with existing 2-dimensional data in the lateral view. Semin Orthod. 1995;1:57–63. doi: 10.1016/s1073-8746(95)80090-5. [DOI] [PubMed] [Google Scholar]
- 9.Lisniewska-Machorowska B, Cannon J, Williams S, Bantleon H. P. Evaluation of force systems from a “free-end” force system. Am J Orthod Dentofacial Orthop. 2008;133(6):791. e1–10. doi: 10.1016/j.ajodo.2007.11.022. [DOI] [PubMed] [Google Scholar]
- 10.Gregg J, Chen J. The Effect of Wire Fixation Methods on the Measured Force Systems of a TLoop Orthodontics Spring AAO Meeting. Philadelphia, Penn: American Association of Orthodontists; 1997. [Google Scholar]
- 11.Raboud D, Faulkner G, Lipsett B, Haberstock D. Three-dimensional force systems from vertically activated orthodontic loops [erratum appears in Am J Orthod Dentofacial Orthop 2001;120(1):80] Am J Orthod Dentofacial Orthop. 2001;119:21–29. doi: 10.1067/mod.2001.110810. [DOI] [PubMed] [Google Scholar]
- 12.Chen J. Apparatus and method for measuring orthodontic force applied by an orthodontic appliance (US Patient No. 6,120,287) USA, 2000. [Google Scholar]
- 13.Proffit W. Contemporary Orthodontics. St Louis, Mo: Mosby, Inc; 2000. [Google Scholar]
- 14.Ren Y, Maltha J. C, Kuijpers-Jagtman A. M. Optimum force magnitude for orthodontic tooth movement: a systematic literature review. Angle Orthod. 2003;73:86–92. doi: 10.1043/0003-3219(2003)073<0086:OFMFOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Nanda R. S. Biomechanics in Clinical Orthodontics. Philadelphia, Penn: WB Saunders Company; 1996. [Google Scholar]
- 16.Burstone C. J, Koenig H. A. Optimizing anterior and canine retraction. Am J Orthod. 1976;70:1–19. doi: 10.1016/0002-9416(76)90257-8. [DOI] [PubMed] [Google Scholar]