

ABSTRACT
Background
Physician assistant/associates (PAs) are healthcare professionals whose roles expand universal access across many nations. PAs fill medical provider supply and demand gaps. Our paper reports a forecasting project to predict the likely census of PAs in the medical workforce spanning from 2020 to 2035.
Methods
Microsimulation modelling of the American PA workforce was performed using the number of clinically active PAs employed in 2020 as the baseline. Graduation rates and PA programme expansion were parameters used to predict annual growth; attrition estimates balanced the equation. Two models, one based on data from the US Bureau of Labor Statistics (BLS) and another based on National Commission on Certification of Physician Assistants (NCCPA) data were used to estimate future annual PA census numbers.
Results
As of 2020, the BLS estimated 125,280 PAs were in the medical workforce; the NCCPA estimate was 148,560 PAs in active practice. The BLS model predicted approximately 204,243 clinically active PAs by 2035; the NCCPA-based model predicted 214,248 PAs in clinical practice.
Conclusions
A PA predictive model based on four data sources projects that the 2035 census of clinically active PAs to be between 204,000 and 214,000: a growth rate of approximately 35%.
KEYWORDS: health workforce, physician associates, workforce modelling, predictive modelling, PA supply
Introduction
Americans are facing shortages in medical personnel due to two population stressors. One demand has been the growth of an ageing population that requires more human resources for health delivery services. With population growth comes the burden of chronic diseases and improved technology requiring frequent upgrading of skills and knowledge.1 The other is a physician and surgeon shortage due to restrictions on federally supported postgraduate training. The Association of American Medical Colleges predicts that medical service demand in the USA will grow faster than physician supply, leading to a projected physician shortage of between 54,100 and 139,000 by 2033. This means a primary care physician shortage of between 21,400 and 55,200, and a shortage of non-primary care specialty physicians of between 33,700 and 86,700.2 Compounding this supply and demand issue is that the number of annual medical care visits is increasing and, at the same time, the annual productivity of primary care providers is decreasing.3,4
The enactment of the Affordable Care Act (ACA) in 2010 was a policy to improve healthcare coverage for all citizens. One of the ACA provisions directed an increase in physician assistants (PAs; equivalent to physician associates in the UK) and advanced practice registered nurses (APRNs) in medical service delivery.5 We report on PAs, a growing provider presence in American medicine.6
The reason for developing a forecast model is to assist policymakers and health services researchers in anticipating shortages or surpluses. Patterns of employment behaviour and demographic trends are used to predict workforce imbalances. The prerequisites to a microsimulation model require understanding the dynamics of employment and the sources of the workforce supply. The first PA forecasting model was published in 2011 and predicted approximately 120,000 employed PAs by 2020. This was done by triangulating PA association data and patterns of attrition.7 The US Bureau of Labor Statistics (BLS) estimated 125,280 PAs were employed in 2020.8 This 1% difference is within the BLS relative statistical error rate of 1.7%.
A more recent PA forecasting model used a different set of information: PA licensure from 56 jurisdictions (50 states, District of Columbia and five territories). The model relied on the policy that all PAs had to have a state-based licence to practise medicine.9 In the 2014 model, which presumed employment data were more accurate at the decentralised state-based medical licensure level, the prediction was off compared with the BLS contemporary values. The 2014 study underestimated the 2020 employed PA population to be 108,000 (8% difference compared with the 2020 BLS data).
In both forecasting models, an upper and lower set of sensitivity analyses were applied to offer a range of estimates based on different assumptions. One strategy used a population-based method of accounting for the lower end and a PA programme growth method for the upper bound range.9 It appears that the population-based approach is a better predicting technique of projecting a PA census and is adopted here as the PA census forecasting method.
Since the 2014 study, a third data source has been added: certified PAs who report they are clinically active in the National Commission on Certification of Physician Assistants (NCCPA) database.10 This database is in a constant state of change as PAs log their continuing medical education hours and refine their role and status.11
Methods
A workforce asset model was constructed to forecast the annual supply of new PAs from 2021 to 2035. Historical PA graduation data from 2014 to 2020 was obtained from the Physician Assistant Education Association (PAEA). The workforce models use contemporaneous numbers (ie PAs) and new inflows (annual cohorts), we then subtracted the estimated number of clinicians who will leave clinical practice sometime during their career.
Information from the Accreditation Review Commission on Education for the Physician Assistant (ARC-PA) regarding new PA programme applications and the annual number of certified PAs from the NCCPA provide variables in this equation. Retirement estimates were obtained from the NCCPA (unpublished data). Concurrently, the BLS annual result estimates PA employment growth for the next 10 years to 2031 at 31% and is based on annual employer surveys. These models are predicated on a career span of an annual PA cohort that approaches 50% attrition by year 30, and less than 1% are clinically active by 40 years (NCCPA; unpublished data). The annual number of PAs graduating each year has been trending up since 2000.
Data sources
The number of PAs in clinical practice is derived from the BLS PA employment statistics, which queries employers and not from self-reported surveys. PA education programmes are the source of graduates for the American system. Essential PA data systems are shown in Table 1.
Table 1.
Data sources for physician assistant predictive modelling
| Data | Attributes | Limitations |
|---|---|---|
| Accreditation Review Commission on Education for the Physician Assistant (ARC-PA) | Accredits PA programmes, active and in development, and periodically evaluates them. All potential PA programmes must apply for and be granted provisional accreditation before inaugurating a class. |
Lengthy application process and historically trended around 10–12 new programmes per year. Personal communication is required for more specific data. |
| US Bureau of Labor Statistics (BLS) | A survey of PA employers across all health service industries is published annually. Estimates growth for 12 years. |
Does not collect data on self-employed PAs in the five US territories or overseas. Historical data on employed PAs began in 2001. |
| National Commission on Certification of Physician Assistants (NCCPA) | Nationally certifies all PAs who want to work clinically in the USA. Administers a recertification examination. Approximately 92% of all certified PAs input data triennially. |
Self-reported data, including intent to retire. Personal communication is required for data. |
| Physician Assistant Education Association (PAEA) | Annually surveys all PA programmes for attrition and graduation rates and calculates the average number of graduates. The 2020 completion rate was 100%. | Dependent on a faculty member in each programme to complete the survey. |
PA = physician assistant.
PA education growth
PA supply is predicated on the number of graduates from accredited PA programmes; which was 282 programmes in 2021.12 Not all programmes had a graduating class due to recent accreditation or delays due to the COVID-19 pandemic from 2020. The estimated lag time from provisional accreditation (approval to enrol students) to a graduation cohort is 3 years on average. The mean number of graduates per programme is 45 (a constant since 2010; PAEA, 2020). Demand in the educational pipeline appears strong with over 23,000 unique applicants annually for 11,000 available first-year seats (personal communication, PAEA, 2022). The average annual number of new programmes is conservatively estimated at 10. At least 260 programmes had a graduating class in 2021, and 40 new programme applicants have requested provisional accreditation.12
Clinically active PAs
A clinically active PA holds a state medical licence whether employed within the state or in a federal agency.13 To be initially licensed to practise medicine, a PA must pass the PA National Certification Examination (PANCE), administered by the NCCPA. Historically, the eventual PANCE pass rate is 99% (personal communication, S Maudlin, 2019). This 1% loss of clinical employment is factored into the annual attrition rate of a cohort. The NCCPA estimates that 95% of the 157,000 certified PAs were clinically active in 2021 based on self-reported status (approximately 149,000; personal communication, NCCPA, 2021).
Baseline data for PA forecasting
At the end of 2020, there were 127,560 PAs who had entered their triennial data in the NCCPA PA Professional Profile (PAPP). Of these, 105,699 PAs responded to the question assessing intentions to retire in the following 5 years (82% response rate). Also, as of the end of 2020, 5.8% of certified PAs indicated that they plan to retire from the PA workforce in the following 5 years (unpublished data).
Sensitivity analysis
Sensitivity analyses were incorporated to explore the influence of uncertainty in the variables and assumptions used for estimating the projected numbers. Each sensitivity analysis was used with programme growth and different annual attrition rates. Data were analysed using MS Excel and IBM SPSS.
The estimates of a future PA workforce size were conservatively based on 10 new programmes per year for 4 years. As the capacity for programme growth is increasingly constrained by clinical sites, the number of new programmes was arbitrarily tapered after 2024.14 Based on consensus with PA educators, the taper was set at five programmes per year for 3 years, then four programmes per year for 2 years, then three programs per year for 3 years, then two programs per year for 2 years and then one programme per year afterwards. The lag time from the day a new programme begins classes to graduation averages 36 months (24–40 months). As of 2021, a total of 40 programmes had applied to ARC-PA for accreditation status.15
Attrition
The definition of attrition is any PA departing a clinical practice role. Departures from clinical practice were based on historical information from prior predictive models that included retirement, career breaks and death. The annual attrition of 5% PAs from clinical status was selected based on published models of PAs, physicians, nurses, some medical and surgical specialties, and NCCPA data.2,16–18
Exiting the clinical labour force occurs across 40 years, with an estimated half of a cohort vacated by year 30 and all by year 40.19,20
Assumptions
Assumptions for this predictive model are shown in Table 2. The data include existing programmes, new programmes likely to grow in the third decade, programme numbers and characteristics. The assumptions result from combined replies from experts, health workforce economists, PA academics and education leaders for their opinions. We used median numbers when given a range.
Table 2.
Key assumptions underpinning the simulation model of clinically active physician assistants through to 2035
| Variable | Key assumption |
|---|---|
| New graduates | Domestic graduates only. Mean age 28 years. |
| Attrition from clinical activity as a PA | Includes PANCE failures (1%), retirement, administration, academic career, death, emigration and other reasons departing US clinical practice. |
| New PA programmes | The net number of PA programmes requesting accreditation at the end of 2021 was 40. From the time of provisional accreditation by ARC-PA to a graduation cohort averages 36 months (range 30–42). Growth of PA programmes is predicated on adding 10 at first, then five per year from 2026 to 2028, four per year for the following 2 years, three per year for the following 3 years, and two per year for 2034 and 2035. |
| Existing PA programmes | The number of PA programmes with a graduating class at the end of 2020 was 260. The mean programme length is 27 months (range 18–36). A historical steady state of 45 graduates (mean) per year is maintained. |
| Full-time status | Defined as 32+ hours per week worked clinically. Remains stable at 85% of all clinically active PAs. |
| Other | N/A |
ARC-PA = Accreditation Review Commission on Education for the Physician Assistant; PA = physician assistant; PANCE = Physician Assistant National Certification Examination.
Formula
The equation that underlies the conceptual projection is:
nPAT,X,Y = nPAT,X – nOUTT,X,Y + nINT,X,Y + εT,X,Y
ε = projection error; nIN = number of inflows; nOUT = number of outflows; nPA = number of PAs; T = target year; X = projection horizon; Y = base period.
The total estimated supply of future PAs (nPAT,X,Y) is calculated using the PA census in the launch year (nPAT,X), minus the estimated outflow (nOUTT,X,Y), plus the estimated inflow (nINT,X,Y) of PAs in the years between launch and target year (T – X → T), based on a specific base period (T – X – Y → T – Y).
Results
Two PA predictive models were created. The first calculation draws on the BLS 2000–2020 historical numbers. The BLS identifies employers of PAs and calculates their employment each year. Data on PAs have been collected and published since 2000 (Fig 1). Each year the BLS predicts the employment rate for the following 10 years. The prediction was for a 31% growth from 2020 to 2030 and a relative statistical error of 1.4% (BLS, 2021). These annual BLS estimates are calculated with data collected from employers in all industry sectors, metropolitan and non-metropolitan areas, and states and the District of Columbia. It does not include employers of PAs in the five US territories or employed outside continental US healthcare. The embedded ‘expert modeller’ in SPSS selects the best fitting exponential smoothing or Autoregressive Integrated Moving Average (ARIMA) model. This expert modeller was used to project the number of clinically active PAs in 2021–2035 and a 75% confidence interval. The model predicted there would be 204,243 clinically active PAs by 2035, with an upper bound of 242,826 and a lower bound of 165,660 (Fig 1).
Fig 1.
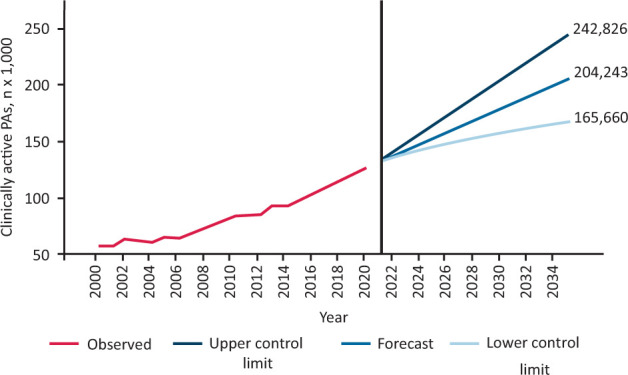
US Bureau of Labor Statistics physician assistant growth, 2000 to 2035. PA = physician assistant.
Fig 2.

Physician assistant programme growth, 1991 to 2035. PA = physician assistant.
PA stock and flow with programme growth and annual attrition: 5% 2012 to 2035
Our projected supply of PAs in clinical practice is based on the addition of 10 new programmes per year in 2022, 2023, 2024, 2025; five per year in 2026, 2027 and 2028; four per year in 2029 and 2030; three per year in 2031, 2032 and 2033; and two per year in 2034 and 2035 (Fig 2). Based on trend data, the model assumes each year, one programme will close or merge with another one.12 The historical average of 45 graduates per programme per year remains constant. A 5% annual attrition rate was factored in. All graduates are retired from clinical practice by year 40.
Estimated percentage of PAs clinically active in the workforce: after 40 years
In estimating the attrition rate, the model is steady from year 1 to year 10 at 5%, with approximately 95% of PAs clinically active through to year 20, followed by a decline to 50% of PAs clinically active at year 30. Subsequently, there is a steep decline reaching 90% attrition at year 35 and 100% by year 40 (Fig 3). In the absence of longitudinal PA career information, our model draws on the work by Auerbach and colleagues forecasting the nursing workforce and physician retirement patterns.16,21 There is some evidence that a large percentage of PAs may remain in the medical workforce for more than 30 years because they have the capacity to change roles to meet new career opportunities.19,22
Fig 3.
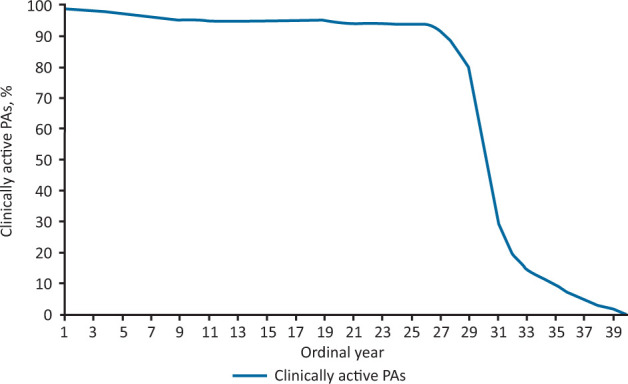
Estimated percentage of physician assistants that are clinically active in the workforce over 40 years. PA = physician assistant.
The second calculation is based on the NCCPA 2012–2020 historical numbers. The NCCPA collects data by surveying certified PAs. Certification by the NCCPA is a requirement for licensure by all US states. The NCCPA produces annual reports on the number of PAs in active clinical practice and asks certificate holders to indicate their practice status; 95% of all certificate holders report that they are in active practice (personal communication, NCCPA, 2021). The base number of PAs in active clinical practice as of 2021 was 149,000 (95% of the overall estimate of 157,000). Using programme growth and 5% annual attrition, we projected the number of clinically active PAs in 2021–2035 and a 75% confidence interval. The model predicts 214,248 clinically active PAs by 2035, with an upper bound of 254,955 and a lower bound of 171,541 (Fig 4).
Fig 4.

Physician assistant stock and flow with programme growth and 5% annual attrition, 2012 to 2035. PA = physician assistant.
Discussion
The US PA labour supply has experienced a sustained growth phase mainly due to educational programme expansion.23 Supply appears roughly in balance with marketplace demand as PA wages continue to rise ahead of inflation.8,24
Workforce estimations of the projected numbers of available healthcare providers with reasonable accuracy are helpful to employers and policymakers. Since the USA lacks central government regulation of graduation rates of American medical workers, estimating the calibre of the workforce depends on calculators of labour activity. Our modelling showed that the overall supply of clinically active PAs is likely to increase to over 200,000 by 2035. This is in line with other estimates that predicts 183,991 PAs by 2030 and only a 1% growth of physicians.6
Retention in the PA workforce is predicted to remain at the current level for several reasons. PAs are in increasing demand and job satisfaction is generally considered high.25 The value of a PA employee is their cost-effectiveness, which endears them to employers and governments.26 PAs appear to respond to market forces, and at least half change to another specialty throughout their careers.27 The ability to change specialties suggests mobility, adaptability and an occupational characteristic that may contribute to retention.
Furthermore, procedural-based specialties coupled with physician shortages tend to attract PAs. This may be due to high salaries associated with labour-intensive specialties.28 Finally, traditional retirement patterns are changing, and bridging strategies to remain at least partially involved in one's career into their 70s is rising.
PAs contribute to medical care delivery and influence the gap between the supply and demand of physicians.2 This is especially true in primary care, where team-based care is growing.29,30 In total, PA contributions improve access to care in the USA and globally. The utilisation of PAs as medical and surgical providers in hospitals and vertically integrated health systems represents significant US workforce trends. Employment of these providers in multispecialty practice sites, specialty practices and health systems offering a health plan and participating in a Medicare accountable care organisation increases.31
Limitations
Predictive models depend on variables, parameters and estimates that can differ among researchers and health workforce analysts. What a PA reports as clinically active and actual activity has not been assessed, and thus self-reported data remains a weak link variable. A 2013 Dutch study on predictive modelling using a 5- and 10-year back-tested strategy of physicians illustrated that 10-year projections are less reliable than those for shorter periods.32 Predictive models can gain usefulness when understanding the supply and demand effect from technology, a growing and ageing population, declining birth rate, economic perturbations, sustainability of chronic disease, and increasing efficiency in service delivery are accounted for. Forecasting trends in demand for various types of healthcare providers will be the next challenge.
The utilisation of PAs as providers in hospitals and vertically integrated health systems represent significant workforce trends in the USA. Employment in hospitals, multispecialty practice sites, specialty practices and health systems offering a health plan and participating in a Medicare accountable care organisation is increasing. We acknowledge that forecasts are vulnerable in several areas, including the adequacy of model documentation, the frequency of evaluative information on model validity and data quality. Our model did not allow for us to predict excess or shortage per the 69 different medical and surgical specialties that employ PAs. The COVID-19 pandemic of 2020–onwards illustrated that medical and surgical personnel adaptability was key to meeting supply and demand issues. Additional limitations include the inability to adjust the data to fit part-time employment.33
As with any modelling exercise, these projections depend on the parameters and estimates used. While the rate of attrition in the models may be subject to some margin of error, on the other hand, the value gained is by using differing forecasting scenarios. Adding retirement goals of a representative group of clinically active PAs could provide insight into occupational stability. We also considered other externalities in our estimate of attrition, such as professional burnout and a pandemic effect.34 We wait for more details about these phenomena before adding variables.
Conclusion
Predictive models based on two data sources projected the supply of PAs in the actively practising medical workforce in the USA from 2020–2035 approximately ranged from 204,000 to 214,000 assuming a growth rate of 35%. This new and refined information informs policymakers, workforce regulators, health systems and employers regarding the growing presence of the American PA. These estimates depend on a continuing demand for medical care services and continuing employment opportunities. Graduation rates of PAs are likely to slow due to limited clinical training sites. Under current assumptions, and barring significant changes in attrition, the number of clinically active PAs will increase by one-third over the next 15 years. Medical workforce analysts rely on PAs to provide medical services along with APRNs and physicians. Health policy makers believe that PAs are a needed component of the medical workforce to mitigate the growing doctor shortage.
Acknowledgement
We are indebted to Bettie Coplan, Robert Jarski and Mirela Bruza for their review and critique of earlier versions of this article.
References
- 1.World Health Organization . Framing the health workforce agenda for the Sustainable Development Goals: biennium report 2016–2017: WHO health workforce. WHO, 2017. https://apps.who.int/iris/handle/10665/272600 [Accessed 25 October 2021]. [Google Scholar]
- 2.IHS Markit . The complexities of physician supply and demand: projections from 2019 to 2034. Association of American Medical Colleges, 2019. [Google Scholar]
- 3.Hedden L, Barer ML, Cardiff K, et al. The implications of the feminization of the primary care physician workforce on service supply: a systematic review. Hum Resour Health 2014;12:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ahmed ST, Mahtta D, Rehman H, et al. Association between frequency of primary care provider visits and evidence-based statin prescribing and statin adherence: Findings from the Veterans Affairs system. Am Heart J 2020;221:9–18. [DOI] [PubMed] [Google Scholar]
- 5.Blumenthal D, Collins SR, Fowler EJ. The Affordable Care Act at 10 years — its coverage and access provisions. N Engl J Med 2020;382:963–9. [DOI] [PubMed] [Google Scholar]
- 6.Auerbach DI, Staiger DO, Buerhaus PI. Growing ranks of advanced practice clinicians — implications for the physician workforce. N Engl J Med 2018;378:2358–60. [DOI] [PubMed] [Google Scholar]
- 7.Hooker RS, Cawley JF, Everett CM. Predictive modeling the physician assistant supply: 2010-2025. Public Health Rep 2011;126:708–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.US Bureau of Labor Statistics . May 2020 National Occupational Employment and Wage Estimates. BLS, 2020. www.bls.gov/oes/current/oes_nat.htm#00-0000 [Accessed 25 October 2021]. [Google Scholar]
- 9.Hooker RS, Muchow AN. Supply of physician assistants: 2013-2026. J Am Acad PAs 2014;27:39–45. [DOI] [PubMed] [Google Scholar]
- 10.National Commission on Certification of Physician Assistants . Statistical profile of certified PAs. NCCPA, 2020. www.nccpa.net/wp-content/uploads/2021/07/Statistical-Profile-of-Certified-PAs-2020.pdf [Google Scholar]
- 11.Barnhill GC, Dallas AD, Mauldin SG, Hooker RS. PA practice analysis: Multidisciplinary tasks, knowledge, and skills. JAAPA 2018;31:34–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Accreditation Review Commission on Education for the Physician Assistant . Accredited programs. ARC-PA. www.arc-pa.org/accreditation/accredited-programs [Accessed 25 October 2021]. [Google Scholar]
- 13.Smith NE, Kozikowski A, Hooker RS. Physician assistants employed by the Federal Government. Mil Med 2020;185:e649–55. [DOI] [PubMed] [Google Scholar]
- 14.American Association of Medical Colleges . Clinical training sites: joint report of the 2013 multi-discipline clerkship/clinical training site survey. AAMC, 2014. [Google Scholar]
- 15.Physician Assistant Education Association . Program report 35: By the numbers: data from the 2019 program survey. PAEA, 2020. https://paeaonline.org/wp-content/uploads/imported-files/program-report35-20201014.pdf [Google Scholar]
- 16.Auerbach DI, Chattopadhyay A, Zangaro G. Improving nursing workforce forecasts: comparative analysis of the cohort supply model and the health workforce simulation model. Nurs Econ 2017;35:283–326. [Google Scholar]
- 17.Coombs J, Hooker RS, Brunisholz K. Physician assistants and their intent to retire. Am J Manag Care 2013;19:e256–62. [PubMed] [Google Scholar]
- 18.Dill MJ, Hirsch GB. The Association of American Medical Colleges’ local area physician workforce modeling project. Acad Med 2021;96:1393–400. [DOI] [PubMed] [Google Scholar]
- 19.Hooker RS, Ramos C, Daly RP, Fang R. The characteristics of clinically active older physician assistants. JAAPA 2012;25:48,50,52–3. [DOI] [PubMed] [Google Scholar]
- 20.Coombs JM, Hooker RS, Brunisholz KD. What do we know about retired physician assistants? A preliminary study. JAAPA 2013;26:44–8. [DOI] [PubMed] [Google Scholar]
- 21.Rittenhouse DR, Mertz E, Keane D, et al. No Exit: An Evaluation of Measures of Physician Attrition. HSR Health Serv Res 2010;39:1571–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hooker RS, Cawley JF, Leinweber W. Career flexibility of physician assistants and the potential for more primary care. Health Aff (Millwood) 2010;29:880–6. [DOI] [PubMed] [Google Scholar]
- 23.Cawley JF, Jones PE, Miller AA, Orcutt VL. Expansion of physician assistant education. J Physician Assist Educ 2016;27:170–5. [DOI] [PubMed] [Google Scholar]
- 24.Quella A, Brock DM, Hooker RS. Physician assistant wages and employment, 2000-2025. JAAPA 2015;28:56–8,60–3. [DOI] [PubMed] [Google Scholar]
- 25.Hooker RS, Kuilman L, Everett CM. Physician assistant job satisfaction: a narrative review of empirical research. J Physician Assist Educ 2015;26:176–86. [DOI] [PubMed] [Google Scholar]
- 26.van den Brink GTWJ, Hooker RS, van Vaught AJ, Vermeulen H, Laurant MGH. The cost effectiveness of physician assistants/associates: a systematic review of international evidence. PLOS One 2021;16:e0259183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Quella AK, Hooker RS, Zobitz JM. Retention and change in PAs’ first years of employment. JAAPA 2021;34:40–3. [DOI] [PubMed] [Google Scholar]
- 28.American Academy of Physician Assistants . 2020 AAPA salary report. AAPA, 2020. [Google Scholar]
- 29.White R, Keahey D, Luck M, Dehn RW. Primary care workforce paradox: A physician shortage and a PA and NP surplus. JAAPA 2021;34:39–42. [DOI] [PubMed] [Google Scholar]
- 30.Pany MJ, Chen L, Sheridan B, Huckman RS. Provider teams outperform solo providers in managing chronic diseases and could improve the value of care. Health Aff Proj Hope 2021;40:435–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Jones D, Furukawa MF, Machta R, Bierman AS, Rich E. Employment of advanced practice clinicians in vertically integrated health systems reflects larger trends toward consolidation. Mathematica, 2021. www.mathematica.org/publications/employment-of-advanced-practice-clinicians-in-vertically-integrated-health-systems-reflects-larger [Accessed 25 October 2021]. [Google Scholar]
- 32.Van Greuningen M, Batenburg RS, Van der Velden LF. The accuracy of general practitioner workforce projections. Hum Resour Health 2013;11:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.American Academy of Physician Assistants . COVID-19 and the PA workforce: trends and implications. AAPA, 2020. [Google Scholar]
- 34.Essary AC, Bernard KS, Coplan B, et al. Burnout and job and career satisfaction in the physician assistant profession: a review of the literature. NAM Perspect 2018. [Google Scholar]