

Abstract
Background Total hip arthroplasty (THA) presents as an excellent treatment for the osteoarthritic hip, demonstrating good survival rates. However, aseptic loosening and infection are the main causes of operative revision. The methods used in revision surgery are non-modular or modular THA implants. In addition to the abovementioned revision reasons for THA, this treatment could be associated with the possibility of femoral stem fracture, especially in the modular system. The topic of material failure has been focused on in the public media. The question arises as to how such media reports correlate with the published literature. The observed mentioned number of cases concerning a femoral stem fracture vary between one single case and up to 18.5% within a clinical study, thus presenting an inhomogeneous data situation with a large span. The specific aim of this systematic review is to establish facts and clarify the number of unforeseen events of a femoral stem fracture based on peer review articles and registry data. This clarification is important to us, as these media reports have led to uncertainty among patients.
Methods A systematic review was performed in accordance with the PRISMA statement. Peer review articles in English and German, presenting original articles, meta-analyses, or case reports, were searched from the turn of the millennium up to December 2019. Only articles that reported a femoral stem component fracture, with content of clinical data as well as register data, were included. Relevant papers published after the defined research time frame were taken into account within the discussion.
Results In total, 218 fractures of a femoral stem (141 primary and 77 revision THA) component could be identified within the selected literature. Most cases of a femoral stem fracture occurred in the modular THA implants compared to the non-modular stems. Regarding revision THA, in summary, 77 implants, presenting 23 non-modular and 54 modular implants, failed by means of femoral stem fracture. A review of 11 National Joint Registries shows a revision rate between 0.04 and 0.05% in only 2 registers according to the specific subject of a femoral stem fracture. For the remaining 9 registers, however, detailed information is lacking and only nonspecific information such as a generic “implant failure” or “other reason” (which can cover a multitude of causes) is supplied.
Conclusion A femoral stem fracture presents a devastating complication for the patient, the surgeon as well as for the manufacturer of the implant. Modular THA implants play an increasingly valuable role concerning restoration of individual anatomy in modern THA revision surgery, especially within complex cases. Regarding revision procedures, data suggests a lower risk of femoral stem fracture for modular implants compared to primary procedures, while the risk of fracture for non-modular implants seems to increase during revision. Ultimately, it cannot be proven whether this is actually applicable, since the absolute number of implanted prosthesis systems is not known. Various implant-, patient-, and surgeon-related factors may lead to these reported femoral stem fractures. However, this systematic review suggests that this is, in general, a rare complication.
Key words: femoral stem, stem fracture, systematic review, total hip arthroplasty, revision hip arthroplasty
Zusammenfassung
Einleitung Die Hüftendoprothetik stellt eine ausgezeichnete Behandlungsoption der Hüftgelenksarthrose dar und weist gute Langzeitüberlebensraten der Implantate auf. Aseptische Lockerungen und Infektionen sind die Hauptursachen für eine Revision des primären Hüftgelenkersatzes. Die in der Revisionschirurgie verwendeten Implantatkonzepte sind als nicht modulare oder modulares Hüftendoprothesensystem verfügbar. Neben den genannten Revisionsgründen wird in der modularen Revisionsendoprothetik vereinzelt über gebrochene, femorale Schaftkomponenten berichtet. Das Thema des Materialversagens in der Endoprothetik ist in Fokus der Medien gerückt. Es stellt sich die Frage, wie solche Medienberichte mit der veröffentlichten Literatur korreliert. Die genannten Fallzahlen femoraler Schaftbrüche variieren von Einzelfällen bis zu 18,5% in klinischen Studien. Ziel der Arbeit ist es, Daten aus der Literatur und Registern zu sammeln, um eine möglichst realitätsnahe Frakturrate für die femorale Schaftkomponente zu ermitteln. Die Klärung der Sachlage ist wichtig, da derartige Medienberichte zur Verunsicherung der Patienten führen.
Material und Methode Gemäß den PRISMA-Richtlinien wurde eine systematische Literaturrecherche durchgeführt. Peer-Review-Artikel in englischer und deutscher Sprache wurden im Zeitraum Januar 2000 bis Dezember 2019 recherchiert. Neben Registerdaten wurden nur wissenschaftliche Artikel mit klinischen Daten, die unterschiedliche femorale Schaftbrüche abhandelten, eingeschlossen. Relevante Beiträge, die nach dem definierten Recherchezeitraum veröffentlicht wurden, sind in der Diskussion dieser Arbeit berücksichtigt.
Ergebnisse Insgesamt konnten 218 Frakturen femoralen Schaftkomponenten (141 primäre und 77 Revisionsendoprothesensysteme) gezählt werden. Die meisten Schaftbrüche traten bei modularen Systemen auf. Bei den 77 Revisionsendoprothesensystemen brachen anteilig 23 nicht-modulare und 54 unterschiedliche modulare Implantate. Die Durchsicht von insgesamt 11 Endoprothesenregistern ergab, dass in nur 2 Registern die Revisionsrate aufgrund femoralen Schaftbrüche beschrieben wurde, die zwischen 0,04% und 0,05% lag. Bei den verbleibenden 9 Registern fehlen detaillierte Angaben. Hier werden nur unspezifische Informationen angegeben, wie z. B. ein allgemeines „Implantatversagen“ (das eine Vielzahl von Implantatkomponenten umfassen kann) oder solche Ereignisse werden unspezifizierend unter der Kategorie „anderer Revisionsgrund“ subsummiert.
Diskussion Der femorale Schaftbruch stellt für den Patienten, den Chirurgen und den Implantathersteller eine gravierende Komplikation dar. Modulare Systeme spielen in der modernen Hüftrevisionschirurgie, insbesondere in komplexen Situationen, eine immer wertvollere Rolle. Die modulare Revisions-Hüftendoprothetik scheint ausweislich der vorgelegten Analyse ein geringeres Risiko für einen femoralen Schaftbruch im Vergleich zu modularen Systemen in der Primärversorgung aufzuweisen, während das Frakturrisiko beim nicht modularen Implantat in der Revisionsendoprothetik einen erhöhten Absolutwert zeigte. Ob dies tatsächlich zutreffend ist, kann letztendlich nicht belegt werden, da die absoluten Zahlen der implantierten Prothesensysteme nicht bekannt sind. Unterschiedlichste implantat-, patienten- und chirurgisch-assoziierte Faktoren können zum femoralen Schaftbruchs führen. Die Daten dieser systematischen Literaturrecherche zeigen jedoch, dass der femoralen Schaftbruch eine eher selten auftretende Komplikation ist.
Schlüsselwörter: femorale Schaft, Schaftbruch, systematisches Review, Hüftendoprothetik, Hüftrevision
Introduction
Since its introduction in the 1960s, modern total hip arthroplasty (THA) has been shown to be an excellent and reliable treatment for the osteoarthritic hip 1 . Survival rates for THA of 95% after 10 and 80% after 25 years are reported 2 . Case numbers of THA treatment have increased. For example, within the Swedish Hip Arthroplasty Registry (SHAR), the number of primary THAs has more than doubled from 1995 to 2017 3 . In summary, THA surgery has the potential to be put forward as “the operation of the century” 4 .
However, long-term survival of THA is a multifactorial issue. It can be influenced by three factors, which may have a unilateral or reciprocal effect on the long-term outcome of THA treatment. First, the patient (i.e., age, body mass index, health status, activity level), second, the surgeon or applied surgical technique (i.e., experience, approach, technique), and third, the implant itself (i.e., cementless or cemented THA, design, materials, modularity, bearing surface, ball head size) are influencing factors 1 . A greater economic burden of 52% for THA revision surgery in comparison with total knee arthroplasty is reported 5 . The SAHR identifies aseptic loosening or osteolysis and infection as well as dislocation presenting as the top three reasons for revision of primary THA. The number of revisions following primary THA has increased by up to 50% from 1995 to 2017. In the case of a re-revision, the cause is most likely to be the same as the one for the first revision 3 .
THA revision surgery presents a more challenging treatment for the surgeon in comparison with primary THA. Each revision surgery is accompanied by a loss of bone substance as well as bone stock quality due to stress shielding and/or bone cement failure, which is different in each patient. For a revision of failed primary THAs, different implant systems based on different concepts are available nowadays on the market. Usually, the stem of a THA revision system is cementless and distally anchored via press-fit within its surrounding bone 6 . Two concepts or “philosophies” of femoral stem design in THA revision surgery do exist: the non-modular stem versus modular stem design. However, both concepts are distinguishable through a longer stem compared to the primary THAs, which is necessary to enable the mentioned distal press-fit anchoring of the femoral implant.
Modularity within THA revision surgery provides many advantages to surgeons and patients. Advantages of modularity in hip revision surgery include improved intraoperative flexibility in complex cases, the opportunity of an individual adjustment of the leg length, femoral antetorsion, offset, and an individual so-called “fit and fill” at the metaphyseal and diaphyseal femur, which results in good implant-to-bone contact as well as an improvement of proximal stabilisation and bone regeneration. Furthermore, it offers the opportunity of an isolated exchange of the proximal femoral implant segment without removing the entire femoral implant. Modular cup components enable individual reconstruction of the hip rotation centre 7 . An increasing trend of cementless modular revision stems is observable in revision surgery after primary THA 8 .
Modular THA revision systems are associated with increasing implant costs, the risk of fretting corrosion, implant loosening or osteolysis, implant dissociation, and implant breakage 9 , 10 , 11 , 12 . However, a proper surgical technique respecting the instructions for use are essential for the performance of modular THA revision systems 7 . The topic of implant stem fracture is reported only occasionally within the current literature 13 , 14 , 15 . Implant stem fracture within THA, especially with modular systems, is based on various fracture mechanisms 16 . “Implant fracture” can refer to a breakage of the femoral stem or its modular junctions (if available) or ball head as well as the acetabular cup or its insert.
One associated disadvantage of modular revision stems is the parameter of force transmission between both modular parts (if a proper surgical technique/implant setup technique is missing), which is associated with a higher risk of junction fracture because of fretting corrosion processes 9 , 10 , 11 , 17 . Another reason for the modular junction fracture described in the literature is the lack of medial bone support around the proximal THA component with simultaneous firm osteointegration of the distal shaft component almost up to the modular junction level 9 , 18 . The risks mentioned are not only caused by the THA design, but also by the intraoperative application by the surgeon 19 . In addition, patientʼs body weight and activity play an important role in the breakage of modular THA components 9 , 20 . From a surgical aspect, component safety of THA is not a given if user error occurs due to non-observance of the manufacturerʼs instruction for use and specifications of the respective implant. Also their off-label use (e.g., BioBall Adapter System; Merete GmbH, Berlin, Germany), and contamination in the area of the morse taper junction by organic material such as blood, tissue, bone, etc., are common 19 .
The reported fracture rate for modular THA is inhomogeneous and ranges from case reports of a single patient 18 at over 1.4% (1 of 72 cases) 11 , up to 18.5% (5 of 27 cases) 10 , 17 for modular revision stems within a clinical trial. A review by Fink 16 resulted in 24 cases. The most recent publication from the year 2020 reported, for the first time, data regarding the number of units in a single type of Implant sold in conjunction with its number of failures 19 . Their systematic classification registered a total of 113 femoral shaft fractures (out of a total of 37 600 implants sold). National Joint Registries report implant fracture (failure) rates from 0.6 to 10.0% 3 , 21 . However, these percentages are related to the reason for revision of the primary THA only. The types of revision THA systems are not considered and detailed information concerning the kind of failure is lacking (i.e., fracture ball head, stem component, etc.).
Heck et al. 22 did the last detailed review investigating implant component failure in THA. Out of a total of 64 483 collated metallic femoral components, a stem fracture was reported in 172 cases. This means a failure rate of 27 per 10 000 cases. However, information regarding the design or type of system is lacking. The highest failure rates given, 45 and 24 cases, resulted out of different THA designs from two different implant manufacturers, respectively.
The discussion about implant safety and how to substantiate it for market approval is not really a new debate 22 . Rather, it has been the subject of political and scientific debate in recent years 23 due to the public media discussion in November 2018 about the “implant files” story that focused on breast implant surgery, cardiac valve failures, and THA systems (addressing breakage of primary modular systems and metal ion release of hip resurfacing and large diameter ball heads). It is necessary to elucidate this issue by a systematic review, based on facts found in the scientific literature as well as from data in available registers.
Objectives of this systematic review:
Reporting the fracture rate for femoral stem components after primary implantation and for revision THA surgery of the hip joint by using the literature and registers.
Identification of the breakage area and cause of the femoral stem fracture.
Which implantation systems are affected and could be associated with a higher risk? Non-modular or modular THA stem components?
Material and Methods
Our systematic review of femoral stem fractures is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocols 24 .
Literature search
A literature search was performed using the following bibliographies: PubMed, Medline, and the Cochrane Database depending on the available access rights. Articles were searched from the turn of the millennium up to December 2019. These databases continued to be viewed from this end date and relevant papers that were published after the defined research time frame were taken into account within the discussion. Articles in English and German presenting original articles, meta-analyses, or case reports were considered for this review. The search strategy consisted of the following components, each defined by a combination of controlled vocabulary and free text terms:
Search strategy (A)
Fatigue fracture AND modular THA AND revision NOT periprosthetic.
Failure AND modular AND revision NOT periprosthetic.
Failure AND modular AND revision AND THA NOT periprosthetic.
Search strategy (B) using MeSH-Terms
Arthroplasty, Replacement, Hip[Mesh] AND fatigue fracture AND modular THA AND revision NOT periprosthetic.
Arthroplasty, Replacement, Hip[Mesh] AND failure AND modular AND revision NOT periprosthetic.
Arthroplasty, Replacement, Hip[Mesh] AND failure AND modular AND revision AND THA NOT periprosthetic.
The initial screening for article inclusion or exclusion based on the title and abstract of the resulting articles was performed by M. S. When information regarding femoral stem component fractures within the abstract was insufficient or if there was any doubt, the studies were nevertheless considered. In addition, further publications were found by reviewing literature lists of already included publications (cross-referencing).
The available full text of the eligible studies was evaluated by M. S., with F. S. and R. F. consulting when necessary.
Inclusion and exclusion criteria
Journal (with peer a review process) articles with content of clinical data (out of clinical trials or case reports) as well as data from different registries (newest available report) were included in this systematic review. Eligible manuscripts were selected if they gave an account of (a) revision THA and/or (b) primary THA. Only articles that reported a fracture of the femoral stem component were included.
Articles about fractures of the femoral ball head, acetabular cup component, or insert were excluded as well as articles regarding periprosthetic fractures and fractures of the femoral neck of the femur bone. Further exclusion criteria were non-clinical studies, animal studies, and experimental or phantom model investigations.
Data extraction
Data out of the included articles was extracted by M. S. Histograms were extracted or calculated from the included articles.
Data synthesis and analysis
Due to the large number of terms used in the literature to describe the assemblies of a THA as well as the fact that an exact localisation of each individual fracture was not explicitly described in the literature, a specific nomenclature was defined for the presented results of this review ( Fig. 1 ). Failure of femoral stem components was categorised according to the three possible regions of implant fracture: the (i) proximal, (ii) intermediate, and (iii) distal part of the femoral stem component.
Fig. 1.
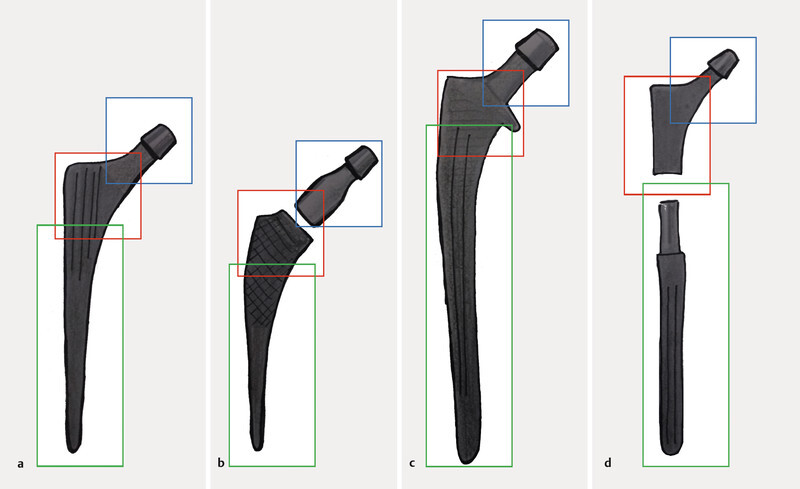
Applied nomenclature of femoral stem components. Stems were categorised according to a monobloc primary, b modular primary, c monobloc revision, and d modular revision THA systems. Each femoral stem design was subcategorised according to the region of the fracture – proximal (blue), intermediate (red), and distal (green) parts.
Femoral stem components were categorised according their indication (primary or revision) and system design specification (non-modular or modular), resulting in four investigated study groups:
Primary THA non-modular stem.
Primary THA modular stem.
Revision THA non-modular stem.
Revision THA modular stem.
To avoid a potential effect of publication bias, results of this systematic review on femoral stem component fractures will be compared to the results found in the registries and in the single past review of Heck et al. 22 . This will take place in the discussion section.
Results
The initial literature research resulted in 755 (search strategy A) and 496 (search strategy B) identified journal articles in PubMed/Medline ( Fig. 2 ). The used key words combination Fatigue fracture AND modular AND revision AND hip NOT periprosthetic resulted in 25 articles, Failure AND modular AND revision NOT periprosthetic in 634 articles, and failure AND modular AND revision AND THA NOT periprosthetic in 96 articles for search strategy A. Used MeSH Terms Arthroplasty, Replacement, Hip[Mesh] AND fatigue fracture AND modular THA AND revision NOT periprosthetic resulted in 3 articles, Arthroplasty, Replacement, Hip[Mesh] AND failure AND modular AND revision NOT periprosthetic in 393 articles, and Arthroplasty, Replacement, Hip[Mesh] AND failure AND modular AND revision AND THA NOT periprosthetic in 100 articles.
Fig. 2.
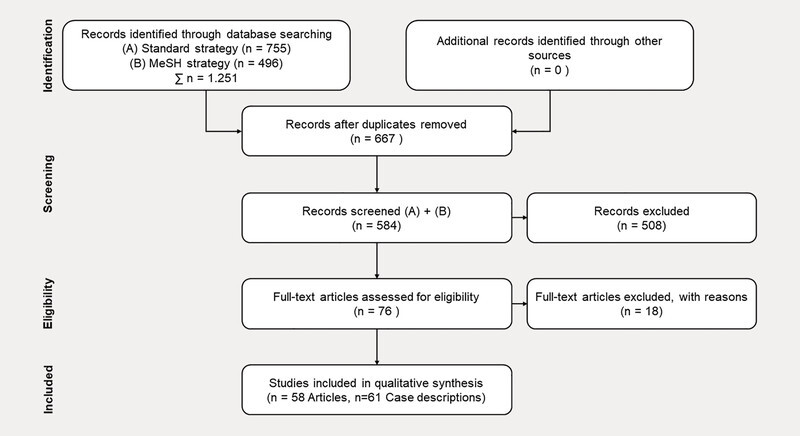
Flow chart selection of case seriesʼ and cohort studies for systematic review of femoral stem fractures following the PRISMA protocol.
After abstract review (screening), according to inclusion/exclusion criteria, a remaining 76 full text journal articles proved to be suitable. No article was excluded because of available access rights. Of these articles, a total of 18 articles were excluded, as they had different elimination criteria. Thus, 61 case descriptions in 58 publications (articles) were included qualitatively and quantitatively. The remaining articles focused on case descriptions of THA revision surgery (n = 29) and primary THA (n = 32).
To summarise: 51 articles with 5 or less cases of femoral stem fractures were found. Additionally, there were 7 articles found with 5 cases or more, up to a maximum of 67 cases, of femoral stem fractures 13 , 25 , 26 , 27 , 28 , 29 , 30 .
It should be mentioned, that 18 publications with a total of 121 reported fractures are included in this review, presenting articles by industrial partners, or those with some partial industry participation within the published investigation.
Complete data set
A total of 218 fractures (141 cases in primary THA and 77 cases in revision THA) of a femoral stem component were documented in the selected literature ( Fig. 3 ). Most cases of a femoral stem fracture occurred in primary as well as revision THA using modular implant systems. Within the primary THA group, 12 stem components were of a non-modular stem and 129 were of a modular THA system design. Regarding the revision THA group, 23 non-modular stem implants and 54 modular implants failed by means of femoral stem fracture. Especially for the proximal part of the femoral stem, the data suggests that modular stems fractured more often during primary THA interventions (106 cases) than during revisions (5 cases).
Fig. 3.
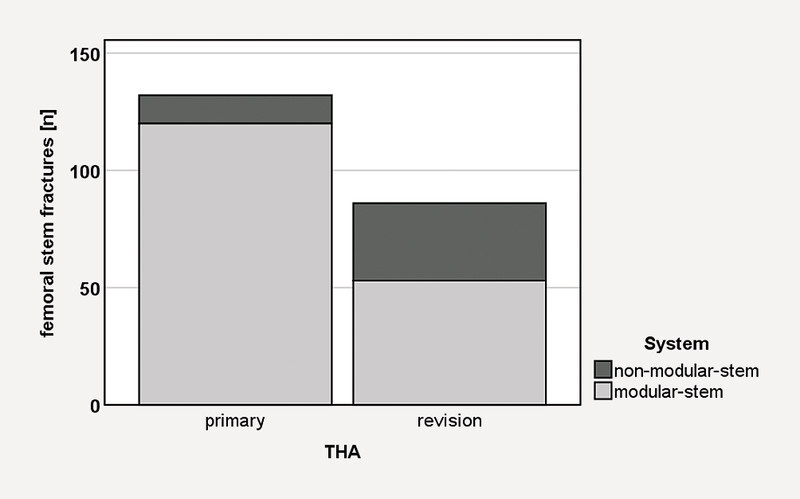
Number of published femoral stem fractures for primary and revision THA, categorised according monobloc (dark grey) and modular systems (grey).
For non-modular stem systems, this trend seems to be contrary. More fractures exist for revision THA implants (18 cases) than for primary interventions (4 cases) ( Fig. 4 ). It has to be emphasised that this data is based on published cases without any knowledge of absolute values (sold numbers of implants, complication rate, etc.).
Fig. 4.
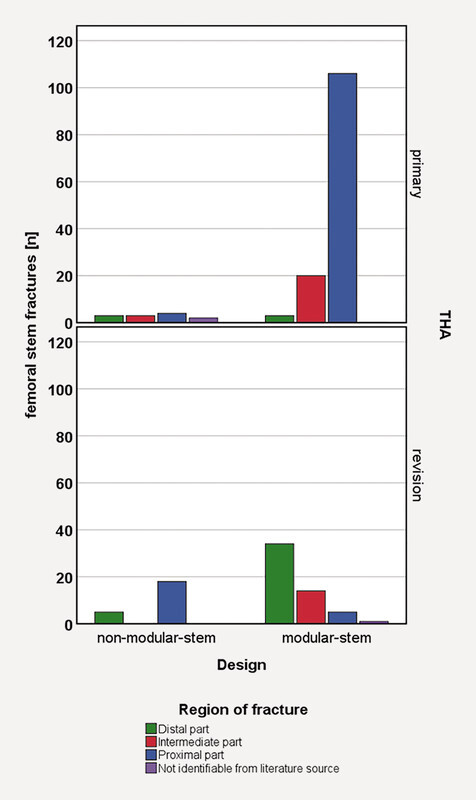
Number of femoral stem fractures classified according to the region of the fracture for monobloc and modular THA designs. Proximal (blue), intermediate (red), and distal (green) parts of a THA system – not identifiable from the literature source (lilac).
Forty-five femoral stem implants cracked in the distal part, 37 in the intermediate part, and 133 in the proximal part ( Fig. 4 ). In only three cases was the fracture level not explicitly stated, thus a categorisation according to the specific nomenclature ( Fig. 1 ) of this review was not possible.
The respected reasons for implant failure have been taken from the identified articles and are partly not fact-based assumptions of the authors ( Table 1 ). In summary, a total of 52 cases of a femoral stem fracture were attributed to the implant (i.e., design influences or metallurgical properties, laser engraving, etc.) 18 , 25 , 26 , 27 , 28 , 31 , 32 , 33 , 34 , 35 , 36 , 37 , 38 , 39 , 40 , 41 , 30 cases to the surgeon (i.e., electrocautery contact to the implant, incorrect handling of implant, etc.) 30 , 42 , 43 , 44 , 45 , 46 , 47 , 48 , 49 , 50 , 51 , 52 , 53 , 54 , 55 , and 22 cases to the patient (i.e., bone loss, tissue reaction, BMI, trauma) 9 , 17 , 56 – 65 . One hundred and ten cases resulted out of a mixture of the three given causes for failure 13 , 15 , 29 , 66 , 67 , 68 , 69 , 70 , 71 , 72 , 73 , 74 , 75 . However, for four cases, the reason is unknown and not given within the reference 18 , 76 , 77 . A detailed analysis of implant-related factors indicates 24 cases related to stem fracture (initiated by crack, friction, corrosion, etc.) are due to design influences, 17 cases due to the manufacturing process, e.g., laser engraving, and 11 cases due to metallurgical properties.
Table 1 Identified reasons for femoral stem fracture.
| Fracture reason | Cases | Primary THA | Revision THA | Literatur | ||
|---|---|---|---|---|---|---|
| Σ | Non-modular stem | Modular stem | Non-modular stem | Modular stem | ||
| Remark: Sources 18 , 66 , 73 are listed twice for case description. Source 18 reported implant-related reasons for fractures and one case was unclear. Sources 66 and 73 reported case descriptions for column primary and revision THA. | ||||||
| Implant related | ||||||
| Design influences, undersizing, bending moment initiation, geometry | 24 | 0 | 13 | 2 | 9 | 18 , 27 , 28 , 31 , 32 , 36 , 37 , 38 , 39 , 40 |
| Manufacturing process, e.g., laser engraving | 17 | 1 | 0 | 16 | 0 | 25 , 33 |
| Metallurgical properties | 11 | 4 | 0 | 0 | 7 | 26 , 34 , 35 , 41 |
| Surgeon related | ||||||
| Electrocautery contact to the implant, incorrect handling of implant, etc. | 14 | 3 | 1 | 0 | 10 | 30 , 42 , 43 , 44 , 53 |
| Contamination of surface properties | 16 | 1 | 11 | 0 | 4 | 46 , 47 , 48 , 49 , 50 , 51 , 52 , 54 , 55 |
| Patient related | ||||||
| Bone loss, tissue reaction, BMI, trauma | 22 | 1 | 3 | 5 | 13 | 9 , 17 , 56 , 57 , 58 , 59 , 60 , 61 , 62 , 63 , 64 , 65 |
| Combination of all | ||||||
| Implant, surgeon, and patient related | 110 | 0 | 100 | 10 | 13 , 15 , 29 , 66 , 67 , 68 , 69 , 70 , 71 , 72 , 73 , 74 , 75 | |
| Other | ||||||
| unknown | 4 | 2 | 1 | 0 | 1 | 18 , 76 , 77 |
| Σ | 218 | 12 | 129 | 23 | 54 | 58 articles 61 case descriptions |
Subanalysis of THA revision implant systems
In the revision THA non-modular stem group, 23 stem fractures were localised in 18 cases at the proximal end and in 5 cases at the distal end of the femoral stem ( Fig. 4 ). This trend was reversed for the reported 54 femoral stem fractures within the modular revision THA group, while 34 stems were broken at the distal part and 5 at the proximal part. Additionally, in this group, there was a breakage of the stem in its intermediate part in 14 cases and in 1 case, the region of the femoral stem fracture could not be deduced.
For modular THA systems, there were 25 articles with a case series of 5 or less femoral stem fractures. A case series of 6 stem fractures was published by Lakstein et al. 27 and Benoist et al. 26 for a modular THA revision system. Merini et al. 25 reported on 16 fractures for a non-modular stem THA revision system.
Registry Data
A total of 11 National Joint Arthroplasty Registries were included ( Table 2 ). Relevant information could be identified in only eight registries. Detailed information on femoral stem fractures was only available from the SHAR and the Australian Orthopaedic Association National Joint Replacement Registry (AOANJR) 3 , 12 .
Table 2 Register data reporting the number of revision cases after primary THA related to implant fracture.
| Register | Type of femoral component failure | THA | ||||||
|---|---|---|---|---|---|---|---|---|
| Fracture clearly stated | Failure general | No. primary | No. revisions after primary | |||||
| Stem | Neck | General not specified |
Cases | Overall fracture (failure) rate | Cases | Fracture (failure) rate | ||
| Exchangeable | Fixed | Fracture incl. | ||||||
| [n] | [n] | [n] | [n] | [n] | [%] | [n] | [%] | |
| Remark: n. i. = not identifiable; n. c. = not to be calculated; *the values were recalculated using the data published within the registers. **Addition of cases published within the registers. Data source: 112 taken from a Table HT15 & b HT27, 23 taken from c Table 8.3.4 & d Table 8.3.6, 379 taken from e Table 3.17 & f Table 3.7, 478 taken from g Table 2 & h Table 12, 580 taken from i Table 2 & j Table 3, 621 taken from k Table page 52, 782 taken from l Table 5 & m Table 10 (include primary and revisions), 881 taken from n Table 12.1 & °Table 10.1, 984 taken from p Table „Revision hips“ page 21 & q Table „All hip arthroplasty“ page 14, 1085 taken from r Table „Number of Primary THA and revision Arthroplasties …“ page 21 & s Table „Cumulative revision percentages of cemented …“ page 39/„Cumulative revision percentages of cemented …“ page 40, 1186 taken from t Figure 31 & u Figure 12. | ||||||||
| Australia 1 | a 163 | b 26 | b 137 | n. i. | b 386 101 | *0.04 | a 14 533 | a 1.1 |
| Sweden 2 | c 140 | n. i. | n. i. | n. i. | c 278 287 | c 0.05 | d 24 447 | *0.6 |
| UK 3 | n. i. | n. i. | n. i. | e,** 3787 | f 1 091 892 | *0.30 | e 115 777 | *3.3 |
| Germany 4 | n. i. | n. i. | n. i. | *329 | g 140 871 | *0.20 | g 16 453 | h 2.0 |
| Norway 5 | n. i. | n. i. | n. i. | j 403 | i, *203 232 | *0.20 | j, *46 921 | *0.9 |
| Italy 6 | n. i. | n. i. | n. i. | k 383 | k 81 530 | k 0,50 | k 3814 | k 10.0 |
| USA-MARCQI 7 | n. i. | n. i. | n. i. | l 64 | m 87 765 | *0,07 | *1461 | l 4.4 |
| Danmark 8 | n. i. | n. i. | n. i. | n 1021 | ° 182 737 | *0,56 | n 21 418 | n 4.7 |
| New Zealand 9 | n. i. | n. i. | n. i. | n. i. | q 137 341 | n. c. | p 19 582 | n. c. |
| Dutch 10 | n. i. | n. i. | n. i. | n. i. | s 247 633 | n. c. | r, *2509 | n. c. |
| USA 11 | n. i. | n. i. | n. i. | n. i. | u 405 346 | n. c. | t 10 188 | n. c. |
| Σ | 303 | 26 | 137 | 5987 | 3 242 735 | 277 103 | ||
| Σ without New Zealand, Dutch, USA | 303 | 26 | 137 | 5987 | 2 452 415 | 244 824 | ||
The AOANJR reports classified the cases into fractures of the femoral stem, of the ball heads, as well as for the acetabular cup and liners, respectively. The number of documented femoral stem fractures at 163 cases was the highest type of implant fracture rate compared to that of 45 femoral ball heads, 92 acetabular cups, and 131 liner fractures. The revision rate due to stem fractures in a total of 386 101 primary THAs was 0.04% 12 .
In the SHAR, 172 revised THAs are described to be as a result of “implant fracture”. One hundred and forty cases (0.6% of all revisions) referred to a femoral stem fracture in the period of time from 1999 to 2017 ( Table 2 ). Accordingly, from a total of 278 287 primary hip arthroplasty failures (reported within the registries), this resulted in a 0.05% revision rate. However, the exact number is not known, because these 140 cases were based on the assumption “ … if the stem of the hip prosthesis is revised as a result of an implant fracture, then it is highly probable that it is a case of a stem fracture …” 3 . Kärrholm et al. 3 note that the reported cases of a femoral stem fracture “ … could involve a slight overestimation” as a result of the abovementioned analysis approach.
For the remaining registries, no detailed information concerning the type of implant failure (i.e., stem, ball head, cup or liner) was published 21 , 78 , 79 , 80 , 81 , 82 . Implant or component failure of 0.9% was recorded in the Norwegian Register 80 , and up to 10.0% in the Register for Emilia-Romagna Region (RIPO) 21 . This resulted in a calculated fracture rate ranging from 0.2% 78 up to 0.5% 21 in a worst case scenario ( Table 2 ).
Also, in the Canadian Joint Replacement Register (CJRR), there was no specific information regarding the type of implant fracture available. Implant fracture (let alone itʼs type) was not recorded in a separate category, rather it was listed cumulatively under the blanket term “Remaining reasons for revision” and was found to be between 7.3 and 28.0% depending on the gender and age of the patient group 83 . However, the term “Remaining reasons for revision” included in its category, next to an implant fracture event, other types of events such as bearing wear, osteolysis, pain of unknown origin, implant dissociation, acetabular erosion, leg length discrepancy, and stiffness.
The Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI) reports “component fracture/failure” for THA, in summary, at 4.4% and gives individual numbers classified by THA systems. Within this classification, a total number of implantation procedures as well as the number of surgeons performing these surgical procedures is given. But, a detailed description of which part/component of the THA system fractures is also missing in the MARQI 82 .
To complete the review of the registries, it should be noted that the New Zealand Joint Registry 84 , the Dutch Arthroplasty Register 85 , and the American Joint Replacement Registry (AJRR) 86 do not provide specific details about implant fractures. This event may be listed under “other events”, which in contrast to CJRR, is not explicitly specified. In its annual report, the AJRR addresses the potential danger of a hip fracture in modular hip stems, but does not cover it with case numbers from the register. Only the case numbers of operated modular systems are shown 86 .
Discussion
The systematic review of femoral stem fractures in THA ultimately resulted in 185 cases. In general, a fracture series of five or less cases was reported. In summary, only five journal articles could be identified that dealt with a femoral stem fracture of more than five cases 13 , 25 , 26 , 27 , 28 .
It is conspicuous with regard to the event of a femoral stem fracture, the two companies named at positions 1 and 2 with the highest number of cases according to Heck et al. 22 still hold the top two positions (with regards to the number of femoral stem fractures) circa 25 years later. However, only the pole position has changed between the two companies. The described case numbers of 172 femoral stem fractures of Heck et al. 22 match the reported data within this systematic review of 218 cases.
Modular THA systems reveal more stem fractures than non-modular stem systems. The exact location of the stem fracture could not always be reliably determined from the papers. The reasons for stem breakage were not always described based on facts. A detailed retrieval analysis of each fracture case with the help of the entire biomechanical and material sciences tool kit is a mandatory requirement. However, case reports in general can only deliver analysis results by methods that are available on site.
It seems to be that the proximal part of modular THA revision systems, in comparison to non-modular stem systems, is probably due to the fact that the surgeon can react more flexibly to individual patient conditions during the operation (especially in complex cases) and thus the biomechanical conditions can be optimally restored. Modular prostheses are therefore indispensable during revision, with a lower risk of fracture compared to primary procedures, while the risk of fracture for non-modular stem prostheses increases during revision. To give a clear statement, knowledge of the absolute values (number of implants sold, number of procedures, full list of serious adverse events for the individual product, etc.) for each available THA revision system is necessary. Remember, the data presented here is based on published cases without any knowledge of these absolute values.
To avoid a potential effect of publication bias on the event of a femoral stem component fracture, a look inside common registries was done to compare given stem fracture rates with the results of this review. Registries providing detailed information about femoral stem fractures indicate similar case numbers.
The AOANJR provides the most detailed overview on the subject of implant fracture with a reported revision rate of 0.04% 12 . Within this report, a fracture classification considering femoral ball head, acetabular insert, the femoral stem, and its modular junctions (if available) as well as fracture of the acetabular cup components was given. The implant fracture rate of the remaining registries had a worst case of 0.5% ( Table 2 ). However, as given within AOANJR or SHAR, a lack of information exists about the type of fracture event, exact region of the fracture, as well as the type of component that failed. Because of the lack of details concerning fracture region and/or component, it is impossible to compare data among the various registries in detail. Some registries are too small and unable to investigate the rare event of a THA component fracture 87 . This may explain why the listing of this event is not kept separately. To study a rare event, a merging of databases between the registries would be useful and recommendable. This would require an equal structure of primary data as well as a detailed description of the event “fracture”, as fulfilled in the AOANJR.
The given data, depending on the individual THA system design, as well as the abovementioned registries do not, in general, indicate the exact type of reported implant fracture (ball head, insert, stem …) 78 , 79 . This fact explains why a comparison and/or an assessment of a real fracture rate presents such a challenge. Furthermore, it must be mentioned that an initial look within publicly available literature databases, such as PubMed or within registries, showed a trend of a huge number of “hits” with regards to the term “fracture”. The term fracture is used in many different contexts. However, appropriate care must be taken when referencing corresponding case numbers on the topic of “fracture” to avoid a misinterpretation according to an assessment of the real fracture rate.
The latest available publication adressing the “femoral stem fracture” topic reports on a realistic fracture rate, described by absolute values for a specific THA revision system 19 . This paper was published outside the time (December 2019) necessary for its inclusion within this review. With regard to the reported fracture rate of 0.3% (113 fractures/37 600 sold systems) of the modular stem system (MRP-TITAN, PETER BREHM GmbH, Weisendorf, Germany) published by Krüger et al. 19 , it should be noted that these authors had access to the manufacturerʼs incident database and present no Key Opinion leaders or Design Surgeons or have any relation to this company as a customer or for financial reasons. According to the authorsʼ knowledge, this is a first-time event, which requires a high degree of trust of the Krüger et al. group 19 on the one hand, and, on the other hand, this demonstrates absolute transparency and commitment to the topic of implant safety by the manufacturer.
Of course, there is a number of unrecorded reported cases within this incident database, which is due to a lack of feedback from operating clinics. In order to keep the number of unrecorded cases as small as possible, the legal obligation to report such serious adverse events is to be observed (i.e., EU – MDR (EU) 2017/745 or FDA – 21CFR803).
A limitation of this systematic review is that it presented data based on available published cases in the English and German languages. It is possible that further articles are available in other languages besides the abovementioned ones. Furthermore, a realistic fracture rate is not possible to report within this review, because detailed information of absolute values for specific THA revision systems is lacking. Register data also does not allow for a clear determination of a fracture rate, since here the data is neither uniform nor prepared to the necessary extent required by the initial research question.
Conclusion
According to the outcome of the review by Heck et al. 22 in 1995, mechanical stem failure is still reported 25 years later as a rare and unusual complication within the registry data as well as within the literature 3 , 9 , 22 .
In comparison to the available number of, in total, 14 885 156 hip replacements between 2000 to 2017 reported by the Organisation for Economic Cooperation and Development (OECD) 88 ( Fig. 5 ), the number of reported stem fracture cases within the literature as well as fracture rates by registries seems to be neglected. Eleven registers supplied a sum total of 3 242 735 observed primary THAs. After excluding cases of the 3 registers reporting no fracture, in total, 2 452 415 observed primary THAs and 6453 cases could be identified as receiving revision surgery according to an overall unspecified classification of an implant failure. This results in an overall fracture rate of 0.26%. However, 303 cases representing the total number of cases from AOANJR or SHAR could be assigned to the event of femoral stem fracture, which still represents a slight overestimation of real cases.
Fig. 5.
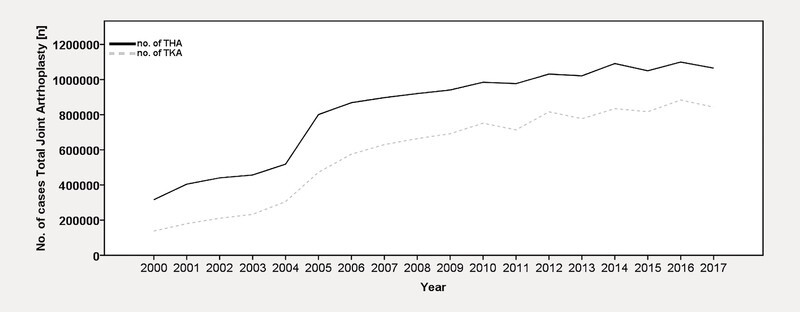
Reported numbers of THA (black line) and TKA (grey dotted line) replacements between 2000 and 2017. Plotted data taken from OECD 88 .
Compared to the probability of an aircraft crash, which is reported as 2.6 crashes out of 1 million departures 89 , the risk of a femoral stem fracture is equal to 2.6 revisions out of 1 million primary THAs.
For the purposes of data analysis, based on the given sources, there is an important caveat to remember. Namely, that the reported cases included multiple types of implant complications and not just that of a femoral stem fracture. However, the calculation is based on the given numbers by analysed registers. This means that this data also does not allow, on the one hand, a clear determination of a fracture rate for the above discussed reasons (data is not uniform, etc.) and, on the other hand, the absolute numbers are unknown. The calculated number of 2.6 revisions out of 1 million primary THAs portrays only a part of the puzzle, because the calculated number is based on only 8 registers.
However, on the one hand, a femoral stem fracture is rare complication, but on the other hand, it presents a devastating complication for the patient, surgeon, and manufacturer of the implant. Each fracture is one too many and its reason must be worked out in detail for every single case. It is important to remember that all implants are subject to failure. Therefore, it is necessary to recognise implant design limits in high-risk patients when deciding on a stem modularity. It is necessary to understand and recognise the problem in order to be able to counteract the problem with the appropriate method, such as additional instruction for use, modified inclusion or exclusion criteria for patients, and so on. Finally, a statement to improve the reporting of implant fractures within registers, studies, or case reports is given by the authors. Uniform terminology or a standard classification proposal is mandatory to define the location/area as well as the reason for the implant fracture in a standardised manner. This creates more transparency, and results from studies and registers can be compared with each other more easily.
Footnotes
Conflict of Interest The authors declare that they have no conflict of interest.
References
- 1.Karachalios T, Komnos G, Koutalos A. Total hip arthroplasty: Survival and modes of failure. doi:10.1302/2058-5241.3.170068. EFORT Open Rev. 2018;3:232–239. doi: 10.1302/2058-5241.3.170068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pivec R, Johnson A J, Mears S C. Hip arthroplasty. doi:10.1016/s0140-6736(12)60607-2. The Lancet. 2012;380:1768–1777. doi: 10.1016/S0140-6736(12)60607-2. [DOI] [PubMed] [Google Scholar]
- 3.Kärrholm J, Mohaddes M, Odin D.Swedish Hip Arthroplasty Register – Annual Report 2017 2018. Accessed March 12, 2019 at:https://registercentrum.blob.core.windows.net/shpr/r/Eng_Arsrapport_2017_Hoftprotes_final-Syx2fJPhMN.pdf
- 4.Learmonth I D, Young C, Rorabeck C. The operation of the century: total hip replacement. doi:10.1016/s0140-6736(07)60457-7. The Lancet. 2007;370:1508–1519. doi: 10.1016/S0140-6736(07)60457-7. [DOI] [PubMed] [Google Scholar]
- 5.Bozic K J, Kamath A F, Ong K. Comparative Epidemiology of Revision Arthroplasty: Failed THA Poses Greater Clinical and Economic Burdens Than Failed TKA. doi:10.1007/s11999-014-4078-8. Clin Orthop Relat Res. 2015;473:2131–2138. doi: 10.1007/s11999-014-4078-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schuh A, Werber S, Holzwarth U. Cementless modular hip revision arthroplasty using the MRP Titan Revision Stem: outcome of 79 hips after an average of 4 yearsʼ follow-up. doi:10.1007/s00402-004-0656-7. Arch Orthop Trauma Surg. 2004;124:306–309. doi: 10.1007/s00402-004-0656-7. [DOI] [PubMed] [Google Scholar]
- 7.Thümler P, Forst R, Zeiler G. Heidelberg: Springer; 2005. Modulare Revisionsendoprothetik des Hüftgelenks. [Google Scholar]
- 8.Wirtz D C, Gravius S, Ascherl R. Uncemented femoral revision arthroplasty using a modular tapered, fluted titanium stem: 5- to 16-year results of 163 cases. doi:10.3109/17453674.2014.958809. Acta Orthop. 2014;85:562–569. doi: 10.3109/17453674.2014.958809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fink B, Urbansky K, Schuster P. Mid term results with the curved modular tapered, fluted titanium Revitan stem in revision hip replacement. doi:10.1302/0301-620X.96B7.33280. Bone Joint J. 2014;96-B:889–895. doi: 10.1302/0301-620X.96B7.33280. [DOI] [PubMed] [Google Scholar]
- 10.Konan S, Garbuz D S, Masri B A. Modular tapered titanium stems in revision arthroplasty of the hip: The Risk and Causes of Stem Fracture. doi:10.1302/0301-620X.98B1.36442. Bone Joint J. 2016;98-B:50–53. doi: 10.1302/0301-620X.98B1.36442. [DOI] [PubMed] [Google Scholar]
- 11.Lakstein D, Backstein D, Safir O. Revision total hip arthroplasty with a porous-coated modular stem: 5 to 10 years follow-up. doi:10.1007/s11999-009-0937-0. Clin Orthop Relat Res. 2010;468:1310–1315. doi: 10.1007/s11999-009-0937-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Australian Orthopaedic Association National Joint Replacement Registry (AOAJR) 2019 Annual Report – Hip, Knee & Shoulder Arthroplasty 2019. Accessed September 16, 2019 at:https://aoanjrr.sahmri.com/documents/10180/668596/Hip,+Knee+&+Shoulder+Arthroplasty/c287d2a3-22df-a3bb-37a2-91e6c00bfcf0
- 13.Grupp T M, Weik T, Bloemer W. Modular titanium alloy neck adapter failures in hip replacement–failure mode analysis and influence of implant material. doi:10.1186/1471-2474-11-3. BMC Musculoskelet Disord. 2010;11:3. doi: 10.1186/1471-2474-11-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Krull A, Morlock M M, Bishop N E. Factors influencing taper failure of modular revision hip stems. doi:10.1016/j.medengphy.2018.02.001. Med Eng Phys. 2018;54:65–73. doi: 10.1016/j.medengphy.2018.02.001. [DOI] [PubMed] [Google Scholar]
- 15.Bicanic G, Crnogaca K, Delimar D. A simple new technique for the removal of fractured femoral stems: a case report. doi:10.1186/1752-1947-8-151. J Med Case Rep. 2014;8:151. doi: 10.1186/1752-1947-8-151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fink B. What can the surgeon do to reduce the risk of junction breakage in modular revision stems? doi:10.1016/j.artd.2018.03.002. Arthroplast Today. 2018;4:306–309. doi: 10.1016/j.artd.2018.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Van Houwelingen A P, Duncan C P, Masri B A. High survival of modular tapered stems for proximal femoral bone defects at 5 to 10 years followup. doi:10.1007/s11999-012-2552-8. Clin Orthop Relat Res. 2013;471:454–462. doi: 10.1007/s11999-012-2552-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rueckl K, Sculco P K, Berliner J. Fracture risk of tapered modular revision stems: a failure analysis. doi:10.1016/j.artd.2017.11.002. Arthroplast Today. 2018;4:300–305. doi: 10.1016/j.artd.2017.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Krüger D R, Guenther K P, Deml M C. Mechanical failure of 113 uncemented modular revision femoral components. doi:10.1302/0301-620X.102B5. Bone Joint J. 2020;102:573–579. doi: 10.1302/0301-620X.102B5.BJJ-2019-1333.R2. [DOI] [PubMed] [Google Scholar]
- 20.Mertl P, Dehl M. Femoral stem modularity. doi:10.1016/j.otsr.2019.05.019. Orthop Traumatol Surg Res. 2020;106:S35–S42. doi: 10.1016/j.otsr.2019.05.019. [DOI] [PubMed] [Google Scholar]
- 21.Regional Register of Orthopaedic Prosthetic Implantology (R.I.P.O.) Overall Data Hip, Knee and Shoulder Arthroplasty in Emilia-Romagna Region (Italy) 2000–2017 2019. Accessed August 8, 2019 at:http://ripo.cineca.it/authzssl/pdf/report_eng_2017.pdf
- 22.Heck D A, Partridge C M, Reuben J D. Prosthetic component failures in hip arthroplasty surgery. doi:10.1016/s0883-5403(05)80199-8. J Arthroplasty. 1995;10:575–580. doi: 10.1016/s0883-5403(05)80199-8. [DOI] [PubMed] [Google Scholar]
- 23.Malchau H, Bragdon C R, Muratoglu O K. The stepwise introduction of innovation into orthopedic surgery: the next level of dilemmas. doi:10.1016/j.arth.2010.08.007. J Arthroplasty. 2011;26:825–831. doi: 10.1016/j.arth.2010.08.007. [DOI] [PubMed] [Google Scholar]
- 24.Liberati A, Altman D G, Tetzlaff J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. doi:10.1371/journal.pmed.1000100. PLoS Med. 2009;6:e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Merini A, Viste A, Desmarchelier R. Cementless Corail femoral stems with laser neck etching: Long-term survival, rupture rate and risk factors in 295 stems. doi:10.1016/j.otsr.2015.10.009. Orthop Traumatol Surg Res. 2016;102:71–76. doi: 10.1016/j.otsr.2015.10.009. [DOI] [PubMed] [Google Scholar]
- 26.Benoist J, Lambotte J C, Polard J L. High rate of fracture in the cementless modular Extreme (Mark I) femoral prosthesis in revision total hip arthroplasty: 33 cases at more than 5 yearsʼ follow-up. doi:10.1016/j.otsr.2013.08.007. Orthop Traumatol Surg Res. 2013;99:915–921. doi: 10.1016/j.otsr.2013.08.007. [DOI] [PubMed] [Google Scholar]
- 27.Lakstein D, Eliaz N, Levi O. Fracture of cementless femoral stems at the mid-stem junction in modular revision hip arthroplasty systems. doi:10.2106/JBJS.I.01589. J Bone Joint Surg Am. 2011;93:57–65. doi: 10.2106/JBJS.I.01589. [DOI] [PubMed] [Google Scholar]
- 28.Pour A E, Borden R, Murayama T. High Risk of Failure With Bimodular Femoral Components in THA. doi:10.1007/s11999-015-4542-0. Clin Orthop Relat Res. 2016;474:146–153. doi: 10.1007/s11999-015-4542-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kovac S, Mavcic B, Kotnik M. What Factors Are Associated With Neck Fracture in One Commonly Used Bimodular THA Design? A Multicenter, Nationwide Study in Slovenia. doi:10.1097/CORR.0000000000000646. Clin Orthop Relat Res. 2019;477:1324–1332. doi: 10.1097/CORR.0000000000000646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Richards C J, Duncan C P, Masri B A. Femoral revision hip arthroplasty: a comparison of two stem designs. doi:10.1007/s11999-009-1145-7. Clin Orthop Relat Res. 2010;468:491–496. doi: 10.1007/s11999-009-1145-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yoshimoto K, Nakashima Y, Nakamura A. Neck fracture of femoral stems with a sharp slot at the neck: biomechanical analysis. doi:10.1007/s00776-015-0745-1. J Orthop Sci. 2015;20:881–887. doi: 10.1007/s00776-015-0745-1. [DOI] [PubMed] [Google Scholar]
- 32.Zajc J, Predan J, Gubeljak N. Modular femoral neck failure after revision of a total hip arthroplasty: a finite element analysis. doi:10.1007/s00590-018-2314-8. Eur J Orthop Surg Traumatol. 2019;29:717–723. doi: 10.1007/s00590-018-2314-8. [DOI] [PubMed] [Google Scholar]
- 33.Jang B, Kanawati A, Brazil D. Laser etching causing fatigue fracture at the neck-shoulder junction of an uncemented femoral stem: A case report. doi:10.1016/j.jor.2013.04.007. J Orthop. 2013;10:95–98. doi: 10.1016/j.jor.2013.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Peterson J R, Wright T M, Wellman S S. Fracture of the neck of an uncemented femoral component unrelated to trunnion corrosion. doi:10.1016/j.artd.2019.01.006. Arthroplast Today. 2019;5:52–56. doi: 10.1016/j.artd.2019.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Raj D, Coupe B D, Keene G S. Stem fracture of a collarless, polished, double-taper cemented femoral prosthesis: a case report. Acta Orthop Belg. 2008;74:697–699. [PubMed] [Google Scholar]
- 36.Dangles C J, Altstetter C J. Failure of the modular neck in a total hip arthroplasty. doi:10.1016/j.arth.2009.07.015. J Arthroplasty. 2010;25:1.169E8–1.169E10. doi: 10.1016/j.arth.2009.07.015. [DOI] [PubMed] [Google Scholar]
- 37.Mehran N, North T, Laker M. Failure of a modular hip implant at the stem-sleeve interface. doi:10.3928/01477447-20130624-33. Orthopedics. 2013;36:e978–981. doi: 10.3928/01477447-20130624-33. [DOI] [PubMed] [Google Scholar]
- 38.Paliwal M, Gordon Allan D, Filip P. Failure analysis of three uncemented titanium-alloy modular total hip stems. doi:10.1016/j.engfailanal.2010.02.011 Eng Fail Anal. 2010;17:1230–1238. [Google Scholar]
- 39.Skendzel J G, Blaha J D, Urquhart A G. Total hip arthroplasty modular neck failure. doi:10.1016/j.arth.2010.03.011. J Arthroplasty. 2011;26:3380–e4. doi: 10.1016/j.arth.2010.03.011. [DOI] [PubMed] [Google Scholar]
- 40.Waly F, Abduljabbar F H, Gascoyne T. Stem-Sleeve Junction Failure of a Modular Femoral Hip System: a Retrieval Analysis. doi:10.1007/s11420-015-9455-7. HSS J. 2015;11:285–290. doi: 10.1007/s11420-015-9455-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Harvie P, Haroon M, Henderson N. Fracture of the hydroxyapatite-ceramic-coated JRI-Furlong femoral component: body mass index and implications for selection of the implant. doi:10.1302/0301-620X.89B6.18680. J Bone Joint Surg Br. 2007;89:742–745. doi: 10.1302/0301-620X.89B6.18680. [DOI] [PubMed] [Google Scholar]
- 42.Herold F, Eijer H. Fracture of a Femoral Revision Stem following a Technical Failure. doi:10.1155/2018/9691627. Case Rep Orthop. 2018;2018:9.691627E6. doi: 10.1155/2018/9691627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Huber G, Weik T, Morlock M M. [Damage to a hip endoprosthesis caused by high-frequency electrocautery] doi:10.1007/s00132-009-1442-6. Orthopade. 2009;38:622–625. doi: 10.1007/s00132-009-1442-6. [DOI] [PubMed] [Google Scholar]
- 44.Konrads C, Wente M N, Plitz W. [Damage to implants due to high-frequency electrocautery: analysis of four fractured hip endoprostheses shafts] doi:10.1007/s00132-014-3023-6. Orthopade. 2014;43:1106–1110. doi: 10.1007/s00132-014-3023-6. [DOI] [PubMed] [Google Scholar]
- 45.Sonntag R, Gibmeier J, Pulvermacher S. Electrocautery Damage Can Reduce Implant Fatigue Strength: Cases and in Vitro Investigation. doi:10.2106/JBJS.18.00259. J Bone Joint Surg Am. 2019;101:868–878. doi: 10.2106/JBJS.18.00259. [DOI] [PubMed] [Google Scholar]
- 46.Cameron H, McTighe T. Experience with Modular Necks for Cemented Total Hip Arthroplasty. doi:10.15438/rr.6.1.132 ReconRev. 2016;6:31–36. [Google Scholar]
- 47.Fokter S K, Molicnik A, Kavalar R. Why do some titanium-alloy total hip arthroplasty modular necks fail? doi:10.1016/j.jmbbm.2016.12.012. J Mech Behav Biomed Mater. 2017;69:107–114. doi: 10.1016/j.jmbbm.2016.12.012. [DOI] [PubMed] [Google Scholar]
- 48.Parisi T, Burroughs B, Kwon Y M. Modular hip implant fracture at the stem-sleeve interface. doi:10.3928/01477447-20150305-91. Orthopedics. 2015;38:e234–e239. doi: 10.3928/01477447-20150305-91. [DOI] [PubMed] [Google Scholar]
- 49.Ryniewicz A M, Bojko Ł, Ryniewicz A. Identification of the cause of the stem neck fracture in the hip joint endoprosthesis. doi:10.1515/ijame-2018-0013 Int J Appl Mech Eng. 2018;23:223–234. [Google Scholar]
- 50.Schuh A, Kachler W, Sesselmann S. Fracture of the cone of a morse taper junction in revision arthroplasty of the hip. doi:10.15761/gmt.1000107 Glob Med Therap. 2018;1:2–4. [Google Scholar]
- 51.Wang Q, Parry M, Masri B A. Failure mechanisms in CoCrMo modular femoral stems for revision total hip arthroplasty. doi:10.1002/jbm.b.33693. J Biomed Mater Res B Appl Biomater. 2017;105:1525–1535. doi: 10.1002/jbm.b.33693. [DOI] [PubMed] [Google Scholar]
- 52.Wodecki P, Sabbah D, Kermarrec G. New type of hip arthroplasty failure related to modular femoral components: breakage at the neck-stem junction. doi:10.1016/j.otsr.2013.02.010. Orthop Traumatol Surg Res. 2013;99:741–744. doi: 10.1016/j.otsr.2013.02.010. [DOI] [PubMed] [Google Scholar]
- 53.Wilson D A, Dunbar M J, Amirault J D. Early failure of a modular femoral neck total hip arthroplasty component: a case report. doi:10.2106/JBJS.I.01107. J Bone Joint Surg Am. 2010;92:1514–1517. doi: 10.2106/JBJS.I.01107. [DOI] [PubMed] [Google Scholar]
- 54.Atwood S A, Patten E W, Bozic K J. Corrosion-induced fracture of a double-modular hip prosthesis: a case report. doi:10.2106/JBJS.I.00980. J Bone Joint Surg Am. 2010;92:1522–1525. doi: 10.2106/JBJS.I.00980. [DOI] [PubMed] [Google Scholar]
- 55.Patel A, Bliss J, Calfee R P. Modular femoral stem-sleeve junction failure after primary total hip arthroplasty. doi:10.1016/j.arth.2008.09.006. J Arthroplasty. 2009;24:11430–1.143E8. doi: 10.1016/j.arth.2008.09.006. [DOI] [PubMed] [Google Scholar]
- 56.Hernandez A, Gargallo-Margarit A, Barro V. Fracture of the Modular Neck in Total Hip Arthroplasty. doi:10.1155/2015/591509. Case Rep Orthop. 2015;2015:591509. doi: 10.1155/2015/591509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lichtinger T K, Lahner M, von Engelhardt L V. Früher Ermüdungsbruch am Prothesenhals einer konventionellen zementfreien Hüftendoprothese. doi:10.3238/oup.2015.0197-0199 OUP. 2015;4:197–199. [Google Scholar]
- 58.Zhu L, He R. Non-contemporaneous bilateral stem fractures occurring after staged bilateral hip revision using extensively porous-coated cylindrical femoral stems: a case report. doi:10.1186/s12891-019-2489-0. BMC Musculoskelet Disord. 2019;20:112. doi: 10.1186/s12891-019-2489-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Uchiyama K, Yamamoto T, Moriya M. Early fracture of the modular neck of a MODULUS femoral stem. doi:10.1016/j.artd.2016.09.004. Arthroplast Today. 2017;3:93–98. doi: 10.1016/j.artd.2016.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Busch C A, Charles M N, Haydon C M. Fractures of distally-fixed femoral stems after revision arthroplasty. doi:10.1302/0301-620X.87B10.16528. J Bone Joint Surg Br. 2005;87:1333–1336. doi: 10.1302/0301-620X.87B10.16528. [DOI] [PubMed] [Google Scholar]
- 61.Buttaro M A, Mayor M B, Van Citters D. Fatigue fracture of a proximally modular, distally tapered fluted implant with diaphyseal fixation. doi:10.1016/j.arth.2006.07.007. J Arthroplasty. 2007;22:780–783. doi: 10.1016/j.arth.2006.07.007. [DOI] [PubMed] [Google Scholar]
- 62.Klauser W, Bangert Y, Lubinus P. Medium-term follow-up of a modular tapered noncemented titanium stem in revision total hip arthroplasty: a single-surgeon experience. doi:10.1016/j.arth.2012.07.001. J Arthroplasty. 2013;28:84–89. doi: 10.1016/j.arth.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 63.Silverton C D, Jacobs J J, Devitt J W. Midterm results of a femoral stem with a modular neck design: clinical outcomes and metal ion analysis. doi:10.1016/j.arth.2014.04.039. J Arthroplasty. 2014;29:1768–1773. doi: 10.1016/j.arth.2014.04.039. [DOI] [PubMed] [Google Scholar]
- 64.Riesgo A M, Hochfelder J P, Adler E M. Survivorship and Complications of Revision Total Hip Arthroplasty with a Mid-Modular Femoral Stem. doi:10.1016/j.arth.2015.06.037. J Arthroplasty. 2015;30:2260–2263. doi: 10.1016/j.arth.2015.06.037. [DOI] [PubMed] [Google Scholar]
- 65.Mimura T. A Case Report of Implant Fracture of Extensively Porous-Coated, Distally Fixated Cementless Long Stem: Detailed Course of Stem Bending Development. doi:10.1155/2015/895214. Case Rep Orthop. 2015;2015:895214. doi: 10.1155/2015/895214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Ceretti M, Falez F. Modular titanium alloy neck failure in total hip replacement: analysis of a relapse case. doi:10.1051/sicotj/2016009. SICOT J. 2016;2:20. doi: 10.1051/sicotj/2016009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Koch C N, Mateo L S, Kayiaros S. Spontaneous Fractures of a Modern Modular Uncemented Femoral Stem. doi:10.1007/s11420-016-9510-z. HSS J. 2016;12:250–254. doi: 10.1007/s11420-016-9510-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Menciere M L, Amouyel T, Taviaux J. Fracture of the cobalt-chromium modular femoral neck component in total hip arthroplasty. doi:10.1016/j.otsr.2014.03.027. Orthop Traumatol Surg Res. 2014;100:565–568. doi: 10.1016/j.otsr.2014.03.027. [DOI] [PubMed] [Google Scholar]
- 69.Nasr P J, Keene G S. Revision of a fractured uncemented revision stem using a custom designed punch and retrograde through-knee approach. doi:10.1155/2015/485729. Case Rep Orthop. 2015;2015:485729. doi: 10.1155/2015/485729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Norman P, Iyengar S, Svensson I. Fatigue fracture in dual modular revision total hip arthroplasty stems: failure analysis and computed tomography diagnostics in two cases. doi:10.1016/j.arth.2013.09.008. J Arthroplasty. 2014;29:850–855. doi: 10.1016/j.arth.2013.09.008. [DOI] [PubMed] [Google Scholar]
- 71.Efe T, Schmitt J. Analyses of prosthesis stem failures in noncemented modular hip revision prostheses. doi:10.1016/j.arth.2010.05.020. J Arthroplasty. 2011;26:6.65E9–6.65E14. doi: 10.1016/j.arth.2010.05.020. [DOI] [PubMed] [Google Scholar]
- 72.Ellman M B, Levine B R. Fracture of the modular femoral neck component in total hip arthroplasty. doi:10.1016/j.arth.2011.05.024. J Arthroplasty. 2013;28:1960–1.96E7. doi: 10.1016/j.arth.2011.05.024. [DOI] [PubMed] [Google Scholar]
- 73.Pearce S, Jenabzadeh A R, Walter W L. Spontaneous fracture of diaphyseal stem of S-ROM femoral prosthesis. doi:10.1136/bcr-2013-202813. BMJ Case Rep. 2014;2014:bcr-2013 –202813. doi: 10.1136/bcr-2013-202813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Wright G, Sporer S, Urban R. Fracture of a modular femoral neck after total hip arthroplasty: a case report. doi:10.2106/JBJS.I.01033. J Bone Joint Surg Am. 2010;92:1518–1521. doi: 10.2106/JBJS.I.01033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Frank R M, Biswas D, Levine B R. Fracture of a dual-modular femoral component at the stem–sleeve junction in a metal-on-metal total hip arthroplasty. Am J Orthop. 2014;43:E57–E60. [PubMed] [Google Scholar]
- 76.de Thomasson E, Conso C, Mazel C. A well-fixed femoral stem facing a failed acetabular component: to exchange or not? A 5- to 15-year follow-up study. doi:10.1016/j.otsr.2011.08.014. Orthop Traumatol Surg Res. 2012;98:24–29. doi: 10.1016/j.otsr.2011.08.014. [DOI] [PubMed] [Google Scholar]
- 77.Trieb K, Stadler N. A New Case of Fracture of a Modular Femoral Neck Device After a Total Hip Arthroplasty. Open Orthop J. 2015;9:126–128. doi: 10.2174/1874325001509010126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Grimberg A, Jansson V, Liebs T.Endoprothesenregister Deutschland (EPRD) – Jahresbericht 2017 2018. Accessed November 1, 2019 at:https://www.eprd.de/fileadmin/user_upload/Dateien/Publikationen/Berichte/EPRD-Jahresbericht_2017_Einzelseiten_Online-Version.pdf
- 79.National Joint Registry for England, Wales, Northern Ireland and the Isle of Man (NJR) 16th Annual Report 2019Accessed March 4, 2020 at:https://reports.njrcentre.org.uk/Portals/0/PDFdownloads/NJR 16th Annual Report 2019.pdf
- 80.Furnes O, Gjertsen J E, Hallan G.Norwegian Arthroplasty Register – Annual Report 2019. Accessed April 10, 2020 at:http://nrlweb.ihelse.net/eng/Rapporter/Report2019_english.pdf
- 81.Danish Hip Arthroplasty Register (DHR) Annual Report 2019 Accessed March 4, 2020 at:http://danskhoftealloplastikregister.dk/wp-content/uploads/2019/09/DHR-årsrapport-2019_til-offentliggørelse-1.pdf
- 82.Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI) 2019 Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI) Annual Report 2019. Accessed April 20, 2020 at:http://marcqi.org/dev/wp-content/uploads/2020/02/2019_AnnualReport_2-15-2020.pdf [DOI] [PMC free article] [PubMed]
- 83.Canadian Joint Replacement Registry (CJRR) Hip and Knee Replacements in Canada, 2017–2018: Annual Report 2019. Accessed April 6, 2020 at:https://secure.cihi.ca/free_products/cjrr-annual-report-2019-en-web.pdf
- 84.New Zealand Joint Registry (NZJR) Twenty Year Report – January 1999 To December 2018 2019. Accessed March 24, 2020 at:https://nzoa.org.nz/sites/default/files/DH8328_NZJR_2019_Report_v4_7Nov19.pdf
- 85.Dutch Arthroplasty Register (LROI) Online LROI Annual Report 2019 2019. Accessed April 6, 2020 at:https://www.lroi-report.nl/app/uploads/2020/10/PDF-Online-LROI-annual-report-2019-min.pdf
- 86.American Joint Replacement Registry (AJRR) Annual Report 2018 2018. Accessed January 28, 2020 at:http://connect.ajrr.net/2018-annual-report-download
- 87.Varnum C, Pedersen A B, Rolfson O. Impact of hip arthroplasty registers on orthopaedic practice and perspectives for the future. doi:10.1302/2058-5241.4.180091. EFORT Open Rev. 2019;4:368–376. doi: 10.1302/2058-5241.4.180091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.OECD OfECaD Health Care Utilisation: Surgical procedures 2019. Accessed October 9, 2019 at:https://stats.oecd.org/index.aspx?queryid=30167
- 89.ICAO State of Global Aviation Safety – ICAO Safety Report 2019 EditionAccessed March 20, 2020 at:https://www.icao.int/safety/Documents/ICAO_SR_2019_29082019.pdf