

Key Points
Question
What is the efficacy and safety of tacrolimus vs intravenous cyclophosphamide (IVCY) as initial therapy for lupus nephritis (LN) among Chinese patients?
Findings
In this randomized clinical trial of 299 patients, the complete or partial kidney response rate was 83.0% with tacrolimus vs 75.0% with IVCY after 24 weeks of treatment, and tacrolimus was statistically noninferior to IVCY regarding response rate. The incidence and type of treatment-emergent adverse events reported were as expected in the patient population.
Meaning
These findings suggest that tacrolimus may be an alternative to IVCY as an initial therapy for LN.
This randomized clinical trial assesses the efficacy and safety of tacrolimus vs intravenous cyclophosphamide as an initial treatment for lupus nephritis in China.
Abstract
Importance
Lupus nephritis (LN) is typically treated with intravenous cyclophosphamide (IVCY), which is associated with serious adverse effects. Tacrolimus may be an alternative for initial treatment of LN; however, large-scale, randomized clinical studies of tacrolimus are lacking.
Objective
To assess efficacy and safety of tacrolimus vs IVCY as an initial therapy for LN in China.
Design, Setting, and Participants
This randomized (1:1), open-label, parallel-controlled, phase 3, noninferiority clinical trial recruited patients aged 18 to 60 years with systemic lupus erythematosus and LN class III, IV, V, III+V, or IV+V primarily from outpatient settings at 35 centers in China. Inclusion criteria included body mass index of 18.5 or greater to less than 27, 24-hour urine protein of 1.5 g or greater, and serum creatinine of less than 260 μmol/L. Of 505 patients screened, 191 failed screening (163 ineligible, 25 withdrawn consent, and 3 other reasons). Overall, 314 were randomized. The first patient was enrolled March 10, 2015, and the study finished September 13, 2018. The follow-up period was 24 weeks. Data were analyzed from December 2019 to March 2020.
Interventions
Oral tacrolimus (target trough level, 4-10 ng/mL) or IVCY for 24 weeks plus prednisone.
Main Outcomes and Measures
Complete or partial response rate at week 24 (prespecified).
Results
A total of 314 patients were randomized (158 [50.3%] to tacrolimus and 156 [49.7%] to IVCY). Overall, 299 patients (95.2%) were treated (tacrolimus group, 157 [52.5%]; IVCY group, 142 [47.5%]). Baseline demographic and clinical characteristics were generally similar between groups (mean [SD] age, 34.2 [9.5] years; 262 [87.6%] female). Tacrolimus was found to be noninferior to IVCY for LN response at week 24. There was a complete or partial response rate of 83.0% (117 of 141 patients) in the tacrolimus group and 75.0% (93 of 124 patients) in the IVCY group (difference, 7.1%; 2-sided 95% CI, −2.7% to 16.9%; lower limit of 95% CI greater than −15%). At week 24, least-square mean change in Systemic Lupus Erythematosus Disease Activity Index score was −8.6 with tacrolimus and −6.4 with IVCY (difference, −2.2; 95% CI, −3.1 to −1.3). Changes in other immune parameters and kidney function were generally similar between groups. Serious treatment-emergent adverse events (TEAEs) were reported in 29 patients in the tacrolimus group (18.5%) and 35 patients in the IVCY group (24.6%). Most common serious study drug-related TEAEs were infections (14 [8.9%] and 23 [16.2%], respectively). Seven patients in each group withdrew due to AEs.
Conclusions and Relevance
In this study, oral tacrolimus appeared noninferior to IVCY for initial therapy of active LN, with a more favorable safety profile than IVCY. Tacrolimus may be an alternative to IVCY as initial therapy for LN.
Trial Registration
ClinicalTrials.gov Identifier: NCT02457221
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease, with an estimated prevalence in China of 30 to 50 per 100 000 population.1 Kidney involvement in SLE has implications for disease management and prognosis. As many as 60% of patients with SLE develop lupus nephritis (LN).1,2,3 LN is associated with substantial morbidity and mortality3,4 and is an important cause of chronic kidney disease and kidney failure in Asia.5,6 The goal of treatment is to preserve kidney function and limit progression to end-stage kidney disease, thus preventing the need for dialysis and transplantation.3,7 Combination therapy with high-dose corticosteroids and intravenous cyclophosphamide (IVCY) is an established initial therapy among patients with LN.7,8,9,10 However, CY is cytotoxic, and serious adverse effects have been observed during long-term treatment, including premature ovarian failure.11,12
The calcineurin inhibitor (CNI) tacrolimus may be considered an alternative to IVCY for initial treatment of LN.7,8,9,10 Tacrolimus hinders T-cell activation, thereby suppressing autoantibody production and preventing long-term kidney damage.13 In addition to attenuating glomerular deposition of immune complexes, tacrolimus may have direct protective effects on podocytes, including stabilization of the actin cytoskeleton and inhibition of podocyte apoptosis, which could contribute to preservation of kidney function in patients with LN.14 Tacrolimus may also be steroid-sparing,15,16 which could reduce the adverse effect burden.
Significantly reduced LN disease activity index was observed in patients treated with tacrolimus over 28 weeks in a placebo-controlled phase 3 study in Japan.17 Studies have also shown that initial therapy with tacrolimus plus corticosteroids is at least as effective and well-tolerated as IVCY for LN.18,19,20,21 Indeed, a recent network meta-analysis found CNIs, alone or in combination with mycophenolate mofetil (MMF), to be more effective than IVCY for inducing response in patients with LN, with similar or lower treatment toxic effects.22 However, large-scale, randomized clinical studies of initial therapy with tacrolimus vs IVCY are lacking. We report results of a phase 3 study undertaken to evaluate the efficacy and safety of tacrolimus vs IVCY in combination with corticosteroids as initial therapy for LN in Chinese patients.
Methods
This report follows the Consolidated Standards of Reporting Trials (CONSORT) guideline for reporting of randomized trials. The study protocol is included in Supplement 1.
Study Design and Participants
This randomized, open-label, parallel-controlled, multicenter, phase 3 noninferiority study was undertaken at 35 centers in China (2 centers did not enroll patients). The study was approved by the independent ethics committee or institutional review board at each site and was conducted in accordance with the International Conference on Harmonisation guideline on Good Clinical Practice and applicable local laws and regulations. Written informed consent was obtained from patients prior to study participation.
Patients were recruited primarily from outpatient settings based on eligibility and willingness to participate. Eligible patients were aged 18 to 60 years (body mass index [calculated as weight in kilograms divided by height in meters squared] ≥18.5 but <27) with SLE (according to American Rheumatism Association Diagnostic Criteria and proven by kidney biopsy within 24 weeks before enrollment)23 and were categorized as LN class III, IV, V, III+V, or IV+V (International Society of Nephrology/Renal Pathology Society classification).24 Patients were also required to have 24-hour proteinuria of 1.5 g or greater and serum creatinine (SCr) levels less than 260 μmol/L (to convert to milligrams per deciliter, divide by 88.4). Exclusion criteria are listed in eTable 1 in Supplement 2. The first patient was enrolled on March 10, 2015; the study finished on September 13, 2018.
Randomization and Treatment
Eligible patients were randomized (1:1) via a centralized randomization system using interactive response technology to treatment with tacrolimus or IVCY for 24 weeks. Randomization was stratified according to LN class (III, IV, V, III+V, or IV+V). All patients received intravenous methylprednisolone pulse therapy (0.5 g/d for 3 days) prior to starting study treatment, followed by oral prednisone (initiated at 0.8 mg/kg/d [maximum dose 45 mg/d] for 4 weeks, then tapered by 5 mg/d every 2 weeks to 20 mg/d, then by 2.5 mg/d every 2 weeks to a maintenance dose of 10 mg/d, which was then maintained in both groups until 24 weeks). Oral tacrolimus was initiated at a dose of 4 mg/d, administered in 2 divided doses; dose adjustments were permitted after day 14 to maintain tacrolimus trough levels of 4 to 10 ng/mL. The starting dose of IVCY was 0.75 g/m2 body surface area (BSA); thereafter, the target was 0.5 to 1.0 g/m2 BSA every 4 weeks, with dose adjustments of 0.25 g/m2 permitted to maintain white blood cell (WBC) count above 2500 to 4000 cells/μL (to convert to cells × 109 per liter, multiply by 0.001). IVCY treatment could be suspended because of adverse events or other specific conditions at the investigator’s discretion.
Outcomes
Patients were assessed at visits at weeks 1, 2, 4, 8, 12, 16, 20, and 24. The primary efficacy end point was the proportion of patients who achieved a response (complete or partial) at week 24. Complete response was defined as proteinuria of less than 0.5 g per 24 hours, serum albumin of 3.5 g/dL or greater (to convert to grams per liter, multiply by 10), and stable kidney function (ie, SCr in the reference range or an increase of ≤15% from baseline). Partial response was defined as proteinuria of less than 3.5 g per 24 hours and decreased by more than 50% from baseline, serum albumin of 3.0 g/dL or greater, and stable kidney function. Secondary efficacy assessments included Systemic Lupus Erythematosus–Disease Activity Index (SLEDAI) score, immune parameters (serum complement C3 and C4, and anti-double-stranded DNA [dsDNA] antibodies), and kidney function (24-hour proteinuria, serum albumin and SCr levels, and estimated glomerular filtration rate [eGFR, based on Chronic Kidney Disease Epidemiology Collaboration formula]). Unless otherwise stated, values are expressed as means and SDs.
Treatment-emergent adverse events (TEAEs) were summarized by preferred terms (Medical Dictionary for Regulatory Activities, version 17.0). TEAEs were considered serious if they resulted in death, were life-threatening, required hospitalization or prolongation of existing hospitalization, resulted in persistent or significant disability or incapacity, or resulted in congenital anomaly or birth defect.
Statistical Analysis
The sample size was based on the results of a randomized, placebo-controlled, phase 3 study of tacrolimus for LN in Japan,17 in which the response rates were 2.9% and 46.4% in the placebo and tacrolimus groups, respectively (data on file). Tacrolimus was assumed to have the same efficacy as IVCY (namely, a treatment effect of 43.5%), and the noninferiority margin was therefore set at 15% to ensure that tacrolimus would retain at least two-thirds of the expected effect of IVCY. Previous studies have shown response rates of 70% to 100% in patients with LN receiving tacrolimus or IVCY initial therapy19,20; the response rate for tacrolimus and IVCY in this study was therefore assumed to be 80%. It was estimated that 125 patients per group would yield 80% power to show noninferiority; planned enrollment was 294 patients, allowing for 15% attrition.
Safety was assessed in all randomized patients who received at least 1 dose of study drug. Efficacy was assessed according to a modified intention-to-treat approach. The full analysis set (FAS) included all patients from the safety population with any efficacy data. However, given that use of the FAS tends to favor a noninferiority conclusion, efficacy was assessed in the per-protocol set (PPS), comprising patients from the FAS with at least 12 weeks (ie, 85 ± 5 days) of follow-up (including early withdrawals due to lack of efficacy), who were compliant with medication (taking 80%-120% of required number of tablets) and had no major protocol deviations.
The Cochran-Mantel-Haenszel test was used for the primary efficacy analysis, with adjustment for baseline stratification by LN class. For the primary end point, noninferiority was concluded if the lower limit of the 95% CI of the difference in response rate between tacrolimus and IVCY was greater than −15%. To confirm robustness of the primary analysis and assess consistency of the primary efficacy outcome among subpopulations, sensitivity and subgroup analyses of the primary end point were undertaken (eTable 2 in Supplement 2). Sensitivity analyses of response rate were carried out for the FAS (last observation carried forward) and for the FAS/PPS based on response assessment in week 24 and response derived from laboratory test data. Subgroup analyses were performed for the primary end point according to sex, baseline BSA, LN class and duration, and SLEDAI score.
Secondary efficacy end points were intended to provide supportive evidence relating to the primary objective and hence were assessed without adjustment for multiple comparisons. They were compared between groups by analysis of covariance, with treatment group, baseline value, and stratification factor (pathological type) as fixed effects. Missing data for response were imputed by last observation carried forward. All statistical tests were 2-sided, with a significance level of .05; associated P values are intended to be read descriptively. Analyses were performed using SAS version 9.4 (SAS Institute). Data were analyzed from December 2019 to March 2020.
Results
Patients
Patient disposition is summarized in Figure 1. Of the 505 patients screened, 314 (158 [50.3%] in tacrolimus group; 156 [49.7%] in IVCY group) were randomized, and 299 received study treatment (157 [52.5%] in tacrolimus group; 142 [47.5%] in IVCY group). Baseline demographic and clinical characteristics were generally similar between the 2 groups (Table 1). Patients were predominantly female (262 [87.6%]), had a mean (SD) age of 34.2 (9.5) years (range, 18-58 years), and predominantly had LN class IV (122 [40.8%]) or class IV+V (85 [28.4%]). The PPS included 265 patients (141 [53.2%] in the tacrolimus group; 124 [46.8%] in the IVCY group). Overall, 263 patients completed the study (141 [53.6%] in the tacrolimus group; 122 [46.4%] in the IVCY group). The most common reasons for discontinuation were adverse events (7 patients in each group) and withdrawal of consent (1 patient in tacrolimus group and 6 patients in IVCY group).
Figure 1. Study Flowchart.

IVCY indicates intravenous cyclophosphamide; FAS, full analysis set; PPS, per-protocol set; SAF, safety set.
aPPS comprised patients from the FAS with at least 12 weeks (85 ± 5 days) of follow-up (including early withdrawals due to lack of efficacy) who were compliant with medication (taking 80%-120% of required number of tablets) and had no major protocol deviations.
Table 1. Patient Demographics and Baseline Clinical Characteristics in the Full Analysis Set.
| Parameter | Participants by treatment group, mean (SD) | ||
|---|---|---|---|
| Tacrolimus (n = 157) | IVCY (n = 142) | Total (N = 299) | |
| Age, y | 34.3 (9.6) | 34.1 (9.4) | 34.2 (9.5) |
| Female, No. (%) | 138 (87.9) | 124 (87.3) | 262 (87.6) |
| Male, No. (%) | 19 (12.1) | 18 (12.7) | 37 (12.4) |
| BSA, m2 | 1.6 (0.1) | 1.6 (0.1) | 1.6 (0.1) |
| BMI | 22.3 (2.5) | 22.5 (2.4) | 22.4 (2.5) |
| Duration of LN, mean (SD) [range] y | 1.4 (3.3) [0.0-17.8] | 1.5 (4.0) [0.1-25.2] | 1.4 (3.7) [0.0-25.2] |
| Pathological type, No. (%) | |||
| III | 8 (5.1) | 8 (5.6) | 16 (5.4) |
| IV | 64 (40.8) | 58 (40.8) | 122 (40.8) |
| V | 22 (14.0) | 20 (14.1) | 42 (14.0) |
| III+V | 17 (10.8) | 17 (12.0) | 34 (11.4) |
| IV+V | 46 (29.3) | 39 (27.5) | 85 (28.4) |
| SLEDAI score | 11.9 (5.6) | 12.6 (5.1) | 12.3 (5.3) |
| ESR, mm/h | 36.3 (28.0) | 33.3 (25.0) | 34.8 (26.6) |
| Anti-dsDNA antibody positive, No. (%) | 84 (53.5) | 91 (64.1) | 175 (58.5) |
| Anti-dsDNA antibody, IU/mL | 275.0 (467.6) | 288.3 (358.4) | 281.3 (424.0) |
| C3, g/L | 0.62 (0.30) | 0.60 (0.25) | 0.61 (0.28) |
| C4, g/L | 0.12 (0.07) | 0.11 (0.06) | 0.11 (0.07) |
| Kidney biopsy activity index scorea | 7.8 (3.9) | 7.6 (3.8) | 7.7 (3.9) |
| Kidney biopsy chronicity index scoreb | 2.5 (1.3) | 2.5 (1.3) | 2.5 (1.3) |
| 24-hour urine protein, mg | 5805.7 (3538.3) | 5347.9 (3441.5) | 5588.3 (3494.3) |
| Serum albumin, g/dL | 2.3 (0.7) | 2.4 (0.7) | 2.4 (0.7) |
| SCr, μmol/L | 75.8 (39.2) | 70.8 (35.0) | 73.4 (37.3) |
| SCr >132.6 μmol/L, No. (%) | 13 (8.3) | 9 (6.3) | 22 (7.4) |
| eGFR, mL/min/1.73 m2 | 99.4 (33.4) | 103.4 (30.6) | 101.3 (32.1) |
| eGFR<60 mL/min/1.73 m2, No. (%) | 25 (15.9) | 16 (11.3) | 41 (13.7) |
| Concomitant ACEi/ARB use, No. (%) | |||
| ACEi | 19 (12.1) | 16 (11.3) | 35 (11.7) |
| ARB | 55 (35.0) | 52 (36.6) | 107 (35.8) |
Abbreviations: ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); BSA, body surface area; C3, complement C3; C4, complement C4; dsDNA, double-stranded DNA; eGFR, estimated glomerular filtration rate; ESR, erythrocyte sedimentation rate; IVCY, intravenous cyclophosphamide; LN, lupus nephritis; SCr, serum creatinine; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index.
SI conversion factors: To convert serum albumin to grams per liter, multiply by 10; SCr to milligrams per deciliter, divide by 88.4.
Based on available data: 150 and 131 for the tacrolimus and IVCY groups, respectively (281 total).
Based on available data: 116 and 93 for the tacrolimus and IVCY groups, respectively (209 total).
Treatment
Mean medication compliance was 99% in both treatment groups (eTable 3 in Supplement 2). Mean duration of exposure was similar in both groups (159.6 vs 153.5 days, respectively). Mean (SD) blood concentration of tacrolimus throughout the study was 5.3 (2.0) ng/mL (<4 ng/mL in 43 patients [27.4%]; 4-10 ng/mL in 109 [69.4%]; and >10 ng/mL in 3 [1.9%]). There was no notable difference in daily dosage or total dosage of oral prednisone between the 2 groups.
Response Rate
Tacrolimus was noninferior to IVCY for response of LN at week 24 (Table 2). At 24 weeks, the rate of complete response was 70 (49.6%) and 45 (36.3%) and the rate of partial response was 47 (33.3%) and 48 (38.7%) in the tacrolimus and IVCY groups, respectively. The rate of complete or partial response was 83.0% (117 patients) with tacrolimus and 75.0% (93 patients) with IVCY (difference between groups, 7.1%; 2-sided 95% CI, −2.7% to 16.9%; lower limit of the 95% CI greater than −15%). Sensitivity analyses confirmed robustness of the primary analysis (eTable 4 in Supplement 2). Response rates were numerically higher in the tacrolimus group than in the IVCY group when split by sex, BSA at baseline, duration of LN, SLEDAI score at baseline (data not shown), and pathological type of LN (except in patients with type IV+V disease) (eTable 5 in Supplement 2). In patients with type V disease, the response rate at week 24 was 68.4% in the tacrolimus group (13 patients) vs 44.4% in the IVCY group (8 patients; difference between groups, 24.0%; 2-sided 95% CI, −7.3% to 49.6%).
Table 2. Response Rate at Week 24 in the Per-Protocol Set.
| Parameter | Participants by treatment group, No. (%) | % Difference between tacrolimus and IVCY groups, (95% CI) | |
|---|---|---|---|
| Tacrolimus (n = 141) | IVCY (n = 124) | ||
| Complete response | 70 (49.6) | 45 (36.3) | NA |
| Partial response | 47 (33.3) | 48 (38.7) | NA |
| Response rate | 117 (83.0) | 93 (75.0) | 7.1 (−2.7 to 16.9) |
Abbreviations: IVCY, intravenous cyclophosphamide; NA, not applicable.
SLEDAI Score
Mean SLEDAI score decreased in both groups over the study period (eFigure 1 in Supplement 2), was less than 10 in both groups at week 4, and was less than 4 in the tacrolimus group at week 24. At week 12, least-square mean (LSM) change in SLEDAI score was −6.7 with tacrolimus and −5.7 with IVCY (LSM difference, −1.0; 95% CI, −1.8 to −0.1; P = .02). At week 24, LSM change in SLEDAI score was −8.6 with tacrolimus and −6.4 with IVCY (LSM difference, −2.2; 95% CI, −3.1 to −1.3; P < .001).
Immune Parameters
No significant differences were seen between groups in mean change from baseline to week 24 for serum C3 and C4 (eFigure 2 in Supplement 2). Mean C3 levels returned to reference range (0.9-1.8 g/L) from week 4 in the tacrolimus group and week 12 in the IVCY group; mean C4 levels were within the reference range (0.1-0 4 g/L) in both groups throughout the study. Anti-dsDNA antibody converted from positive to negative by week 24 in 37 patients (26.2%) and 26 patients (21.0%) in the tacrolimus and IVCY groups, respectively (P = .33).
Kidney Function
Tacrolimus was associated with significant improvement in mean 24-hour proteinuria vs IVCY (Figure 2A). LSM reductions in 24-hour proteinuria from baseline were significantly greater with tacrolimus vs IVCY at all visits from week 4 onwards (P < .001). At week 24, LSM change in 24-hour proteinuria from baseline was −4534.8 mg and −3632.5 mg in the tacrolimus and IVCY groups, respectively (LSM difference, −902.3 mg; 95% CI, −1382.2 to −422.3 mg; P < .001). Mean change from baseline to week 24 in serum albumin was similar between groups (Figure 2B). Differences in mean SCr level (Figure 2C) and eGFR were seen between the 2 groups over the study period but remained within the reference range in both groups at all visits (eTable 6 in Supplement 2). At week 24, LSM change in SCr level from baseline was 10.2 μmol/L with tacrolimus and −5.6 μmol/L with IVCY (LSM difference, 15.9 μmol/L; 95% CI, 6.7 to 25.1 μmol/L; P < .001). Doubling of SCr level from baseline within 24 weeks occurred in 9 patients in the tacrolimus group (4 patients outside the reference creatinine range) and none in the IVCY group. LSM change in eGFR from baseline at week 24 was −8.8 mL/min/1.73 m2 with tacrolimus and 4.3 mL/min/1.73 m2 with IVCY (LSM difference, −13.1 mL/min/1.73 m2; 95% CI, −17.9 to −8.4 mL/min/1.73 m2; P < .001).
Figure 2. Mean Change From Baseline to Week 24 for 24-Hour Urine Protein, Serum Albumin Level, and Serum Creatinine Level in the Per-Protocol Set.
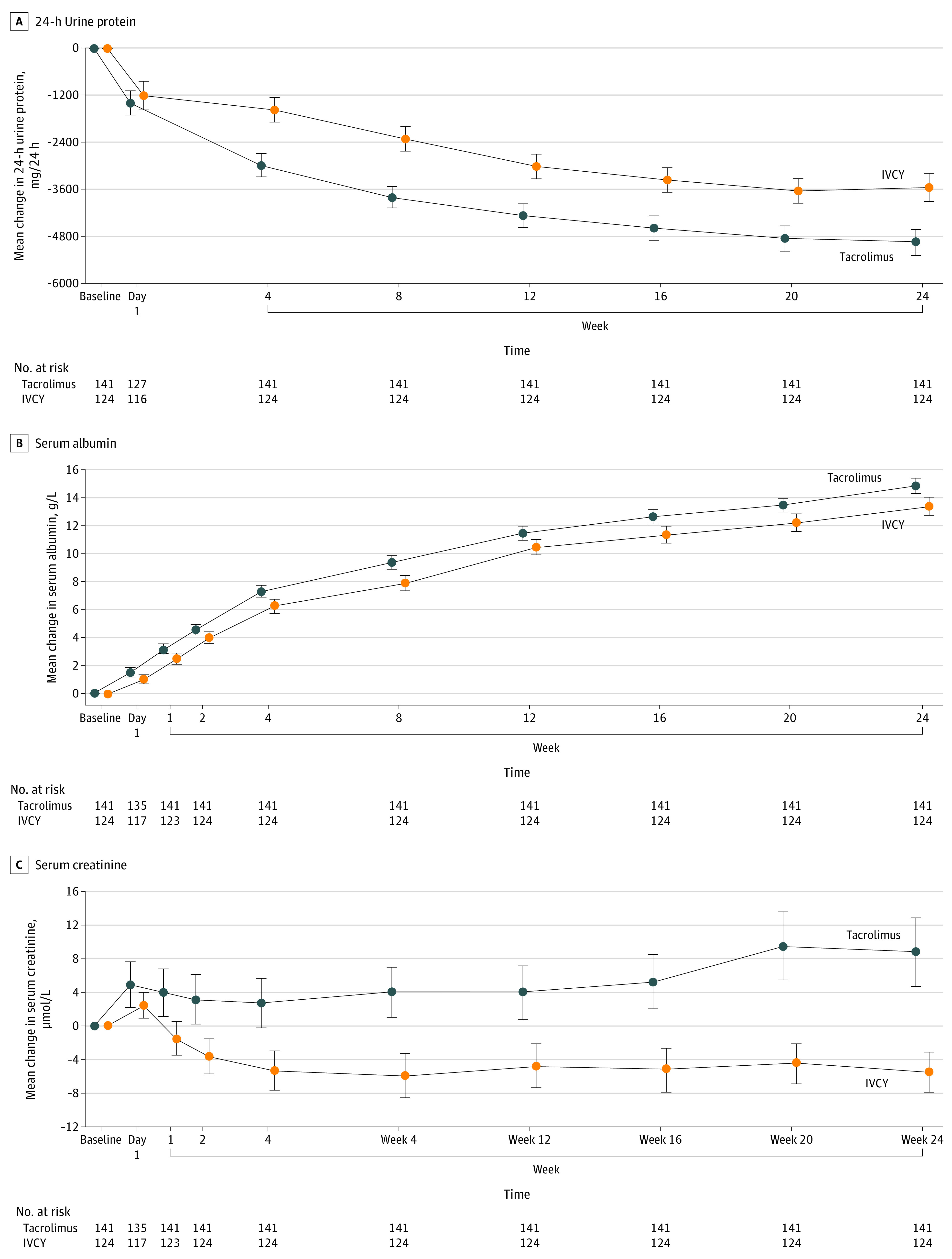
IVCY indicates intravenous cyclophosphamide. Whiskers indicate SEs. To convert serum albumin to grams per liter, multiply by 10; serum creatinine to milligrams per deciliter, divide by 88.4.
Safety
A similar proportion of patients experienced TEAEs in both groups (Table 3). Most (>70%) TEAEs were mild or moderate in severity. The most common study drug-related TEAEs were upper respiratory tract infection (37 [23.6%]) and diarrhea (16 [10.2%]) in the tacrolimus group, and upper respiratory tract infection (40 [28.2%]), nausea (34 [23.9%]), vomiting (33 [23.2%]), alopecia (17 [12.0%]), and decreased WBC count (16 [11.3%]) in the IVCY group. Serious TEAEs were reported in 29 patients (18.5%) in the tacrolimus group and 35 patient (24.6%) in the IVCY group. The proportion of patients with serious TEAEs considered to be study drug–related was numerically lower in the tacrolimus group than in the IVCY group (18 [11.5%] vs 30 [21.1%]). The most common serious study drug–related TEAE was infection (mainly lung and upper respiratory tract infections), reported in 14 patients (8.9%) and 23 patients (16.2%) in the tacrolimus and IVCY groups, respectively. Three TEAEs resulted in 2 deaths (1 in the tacrolimus group due to varicella; 1 in the IVCY group due to septic shock and pneumonia), both considered treatment-related.
Table 3. Summary of Patients Experiencing TEAEs Over the 24-Week Study Period in the Safety Population.
| TEAE parameter | Participants in safety population, No. (%) | |
|---|---|---|
| Tacrolimus (n = 157) | IVCY (n = 142) | |
| Any TEAE | 145 (92.4) | 136 (95.8) |
| TEAE related to study drug | 118 (75.2) | 120 (84.5) |
| Study drug–related TEAES reported in ≥5% of patients in either groupa | ||
| Abdominal distension | 6 (3.8) | 8 (5.6) |
| Alopecia | 5 (3.2) | 17 (12.0) |
| Bronchitis | 8 (5.1) | 10 (7.0) |
| Cough | 11 (7.0) | 7 (4.9) |
| Diarrhea | 16 (10.2) | 2 (1.4) |
| Granulocytopenia | 0 | 9 (6.3) |
| Headache | 4 (2.5) | 8 (5.6) |
| Herpes zoster | 4 (2.5) | 14 (9.9) |
| Hyperuricemia | 13 (8.3) | 5 (3.5) |
| Leukopenia | 0 | 12 (8.5) |
| Hepatic function abnormal | 8 (5.1) | 10 (7.0) |
| Hypokalemia | 3 (1.9) | 8 (5.6) |
| Lung infection | 8 (5.1) | 11 (7.7) |
| Nausea | 4 (2.5) | 34 (23.9) |
| Tremor | 15 (9.6) | 2 (1.4) |
| Upper respiratory tract infection | 37 (23.6) | 40 (28.2) |
| Urinary tract infection | 9 (5.7) | 6 (4.2) |
| Vomiting | 2 (1.3) | 33 (23.2) |
| WBC count decreased | 2 (1.3) | 16 (11.3) |
| Any serious TEAE | 29 (18.5) | 35 (24.6) |
| Any serious TEAE related to study drug | 18 (11.5) | 30 (21.1) |
| Serious study drug–related TEAEs reported by >1 patient in either groupb | ||
| Infections and infestations | ||
| Any | 14 (8.9) | 23 (16.2) |
| Lung infection | 5 (3.2) | 10 (7.0) |
| Upper respiratory tract infection | 3 (1.9) | 4 (2.8) |
| Pneumonia | 2 (1.3) | 2 (1.4) |
| Bronchitis | 2 (1.3) | 1 (0.7) |
| Pulmonary tuberculosis | 0 | 2 (1.4) |
| Blood and lymphatic system disorders | ||
| Any | 0 | 4 (2.8) |
| Granulocytopenia | 0 | 2 (1.4) |
| Gastrointestinal disorders | 1 (0.6) | 2 (1.4) |
| General disorders and administration site conditions | ||
| Any | 0 | 2 (1.4) |
| Pyrexia | 0 | 2 (1.4) |
| Respiratory, thoracic, and mediastinal disorders | 2 (1.3) | 0 |
| Any TEAE leading to early withdrawal | 19 (12.1) | 16 (11.3) |
| TEAE related to study drug leading to early withdrawal | 16 (10.2) | 13 (9.2) |
| Any serious TEAE leading to early withdrawal | 11 (7.0) | 9 (6.3) |
| Any serious TEAE related to study drug leading to early withdrawal | 9 (5.7) | 7 (4.9) |
| Any TEAE leading to death | 1 (0.6) | 1 (0.7) |
Abbreviations: IVCY, intravenous cyclophosphamide; TEAE, treatment-emergent adverse event; WBC, white blood cell.
TEAEs were recorded using Medical Dictionary for Regulatory Activities preferred terms and are listed alphabetically.
Serious TEAEs were recorded using Medical Dictionary for Regulatory Activities system organ class and preferred terms and are listed alphabetically.
Discussion
To our knowledge, this is the first large-scale, randomized clinical trial to assess the safety and efficacy of tacrolimus vs IVCY in patients with LN. Results show initial therapy with tacrolimus to be noninferior to IVCY regarding response rate after 24 weeks of treatment (83.0% vs 75.0% in the tacrolimus and IVCY groups, respectively). Results of this study are consistent with those of previous small-scale studies of tacrolimus vs IVCY for initial treatment of LN, although findings should be compared with caution due to differences in patient populations, primary end point definitions, and treatment dosing regimens between studies.18,19,20,21 The response rate with tacrolimus in the present study (83.0%) is also aligned with that reported in a randomized clinical trial undertaken to compare the efficacy of tacrolimus vs MMF as LN initial therapy (overall response rate at 6 months, 89% in the tacrolimus group vs 80% in the MMF group).25 In another Chinese study, Liu et al26 investigated the efficacy and safety of combined therapy with tacrolimus (4 mg/d) and MMF (1 g/d) vs IVCY (initiated at 0.75 g/m2 BSA and then adjusted to 0.5-1.0 g/m2 BSA) as initial therapy for adult patients with LN class III, IV, V, III+V, or IV+V disease. The complete or partial response rates at 6 months were 83.5% vs 63.0%, respectively.26 However, caution should be exercised when comparing data from our study with those from the study by Liu et al,26 as patients in the tacrolimus group from our study did not receive MMF.
Notably, tacrolimus demonstrated a clinically meaningful improvement in SLEDAI score vs IVCY from week 12. Tacrolimus was also associated with a clinically meaningful improvement in 24-hour proteinuria compared with IVCY, which may suggest a more favorable long-term kidney outcome in patients with LN.27,28 This is consistent with findings from other studies, in which more rapid reduction in proteinuria was seen in patients with LN who received therapy with tacrolimus vs with IVCY.19,20 These findings suggest that kidney response may be more rapidly achieved during initial therapy with tacrolimus than IVCY.
In this study, after 24 weeks’ treatment, the LSM change from baseline in SCr level was higher in the tacrolimus group than in the IVCY group (10.2 vs −5.6 μmol/L). However, this change was not clinically relevant. As might be expected, the mean SCr level was elevated in the tacrolimus group throughout the study, but it did not exceed 15% of the mean baseline level, remaining within the reference range across visits. This elevation in SCr level is not thought to be caused by lupus disease but may be related to tacrolimus treatment, given that similar trends have been observed in previous studies. For example, in the 28-week study by Miyasaka et al,17 median creatinine clearance decreased from 101.4 mL/min at baseline to 78.2 mL/min at the final assessment in the tacrolimus group, while baseline and final creatinine clearance were similar in the placebo group. Furthermore, Szeto et al29 reported lower (although not statistically significantly lower) eGFR after 24 weeks of tacrolimus treatment vs control. The effect of tacrolimus on SCr level may be influenced by drug dose and blood concentration. As the target trough concentration of tacrolimus in our study was 4 to 10 ng/mL and the mean (SD) tacrolimus trough concentration was 5.3 (2.0) ng/mL, these data remind clinicians to monitor kidney function even within normal drug concentration ranges. Since this was a 24-week study, long-term follow-up is needed to further evaluate the effect of tacrolimus on SCr levels in patients with LN.
It is known that different kidney pathological types of LN respond differentially to drug therapy. In this study, except for class IV+V LN, the response rate in the tacrolimus group was numerically higher than that in the IVCY group for all other pathological classes , especially class V LN, which had a response rate of 68.4%. This is consistent with findings from the study by Mok et al,25 in which patients with class V LN who received tacrolimus as initial therapy had a higher response rate at 6 months than those treated with MMF (100% vs 75%).25 These results highlight the beneficial effects of tacrolimus on membranous LN, which should be further elucidated in future large-sample, multicenter studies.
Most patients in both treatment groups experienced TEAEs, but the majority were mild or moderate in severity. No unexpected safety findings were reported, and the incidence and type of TEAEs observed was expected in the patient population. Of note, the proportion of patients in whom infection was reported as a study drug–related serious TEAE was numerically lower in the tacrolimus group (8.9%) than in the IVCY group (16.2%). Although not assessed in this study, the potential for longer term treatment-related adverse effects should be considered when selecting the most appropriate initial therapy in patients with LN. In this context, the apparent lack of ovarian toxic effects with tacrolimus is an advantage over IVCY, which has been shown to be associated with an increased risk of premature ovarian failure in patients with SLE.11,12 However, whether tacrolimus is associated with long-term kidney toxic effects in LN—as has been suggested in transplantation—may also be a consideration.30,31 Long-term follow-up of Chinese patients with LN is needed in the future to evaluate the long-term effect of CNIs on kidney function.
Overall, the findings from our study are encouraging for use of tacrolimus as LN initial therapy in clinical practice. Although long-term data are limited, tacrolimus was also recently shown to be effective and well tolerated as maintenance therapy over a period of 5 years in a large population of patients with LN in real-world clinical settings in Japan.32
Limitations
This study has limitations, including the open-label design and the short duration of follow-up (24 weeks). Furthermore, it was not designed to assess whether tacrolimus can be steroid sparing and mitigate the adverse effects associated with long-term steroid treatment. In addition, subgroup analyses should be interpreted with caution because of the small number of patients in some groups. Furthermore, only Chinese patients were included, which may limit application of the findings to non-Asian populations. However, the study population can be considered representative of the general population of patients with LN, as it predominantly comprised women of child-bearing age.
Conclusions
In this study, initial therapy with oral tacrolimus in combination with corticosteroids appears to be effective and have a more favorable safety profile in Chinese patients with LN. Our findings add to the increasing evidence supporting a role for tacrolimus as an alternative to IVCY for initial therapy of LN.18,19,20,21,22,25
Trial Protocol and Statistical Analysis Plan
eTable 1. Study Exclusion Criteria
eTable 2. Sensitivity and Subgroup Analyses of the Primary Efficacy End Point
eTable 3. Study Drug Compliance and Exposure (Safety Population)
eTable 4. Results of Sensitivity Analyses of Response Rate at Week 24
eTable 5. Subgroup Analyses: Response Rate by Different Pathological Types of LN at Week 24
eTable 6. Mean SCr Level and Mean Change from Baseline to Week 24
eFigure 1. Mean (SE) Change from Baseline to Week 24 in SLEDAI Score
eFigure 2. Mean (SE) Change from Baseline to Week 24 in Serum C3 and Serum C4
Data Sharing Statement
References
- 1.Osio-Salido E, Manapat-Reyes H. Epidemiology of systemic lupus erythematosus in Asia. Lupus. 2010;19(12):1365-1373. doi: 10.1177/0961203310374305 [DOI] [PubMed] [Google Scholar]
- 2.Mok CC. Epidemiology and survival of systemic lupus erythematosus in Hong Kong Chinese. Lupus. 2011;20(7):767-771. doi: 10.1177/0961203310388447 [DOI] [PubMed] [Google Scholar]
- 3.Almaani S, Meara A, Rovin BH. Update on lupus nephritis. Clin J Am Soc Nephrol. 2017;12(5):825-835. doi: 10.2215/CJN.05780616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Saxena R, Mahajan T, Mohan C. Lupus nephritis: current update. Arthritis Res Ther. 2011;13(5):240. doi: 10.1186/ar3378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mok CC, Kwok RCL, Yip PSF. Effect of renal disease on the standardized mortality ratio and life expectancy of patients with systemic lupus erythematosus. Arthritis Rheum. 2013;65(8):2154-2160. doi: 10.1002/art.38006 [DOI] [PubMed] [Google Scholar]
- 6.Sui M, Ye X, Ma J, et al. Epidemiology and risk factors for chronic kidney disease in Chinese patients with biopsy-proven lupus nephritis. Intern Med J. 2015;45(11):1167-1172. doi: 10.1111/imj.12840 [DOI] [PubMed] [Google Scholar]
- 7.Fanouriakis A, Kostopoulou M, Cheema K, et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis. 2020;79(6):713-723. doi: 10.1136/annrheumdis-2020-216924 [DOI] [PubMed] [Google Scholar]
- 8.Hahn BH, McMahon MA, Wilkinson A, et al. ; American College of Rheumatology . American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res (Hoboken). 2012;64(6):797-808. doi: 10.1002/acr.21664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rovin BH, Caster DJ, Cattran DC, et al. ; Conference Participants . Management and treatment of glomerular diseases (part 2): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;95(2):281-295. doi: 10.1016/j.kint.2018.11.008 [DOI] [PubMed] [Google Scholar]
- 10.Mok CC, Yap DYH, Navarra SV, et al. ; Asian Lupus Nephritis Network (ALNN) . Overview of lupus nephritis management guidelines and perspective from Asia. Nephrology (Carlton). 2014;19(1):11-20. doi: 10.1111/nep.12136 [DOI] [PubMed] [Google Scholar]
- 11.Harward LE, Mitchell K, Pieper C, Copland S, Criscione-Schreiber LG, Clowse MEB. The impact of cyclophosphamide on menstruation and pregnancy in women with rheumatologic disease. Lupus. 2013;22(1):81-86. doi: 10.1177/0961203312468624 [DOI] [PubMed] [Google Scholar]
- 12.Ceccarelli F, Orefice V, Perrone G, et al. Premature ovarian failure in patients affected by systemic lupus erythematosus: a cross-sectional study. Clin Exp Rheumatol. 2020;38(3):450-454. [PubMed] [Google Scholar]
- 13.Mok CC. Calcineurin inhibitors in systemic lupus erythematosus. Best Pract Res Clin Rheumatol. 2017;31(3):429-438. doi: 10.1016/j.berh.2017.09.010 [DOI] [PubMed] [Google Scholar]
- 14.Liao R, Liu Q, Zheng Z, et al. Tacrolimus protects podocytes from injury in lupus nephritis partly by stabilizing the cytoskeleton and inhibiting podocyte apoptosis. PLoS One. 2015;10(7):e0132724. doi: 10.1371/journal.pone.0132724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Borrows R, Loucaidou M, Van Tromp J, et al. Steroid sparing with tacrolimus and mycophenolate mofetil in renal transplantation. Am J Transplant. 2004;4(11):1845-1851. doi: 10.1111/j.1600-6143.2004.00583.x [DOI] [PubMed] [Google Scholar]
- 16.Li X, Li H, Chen J, et al. Tacrolimus as a steroid-sparing agent for adults with steroid-dependent minimal change nephrotic syndrome. Nephrol Dial Transplant. 2008;23(6):1919-1925. doi: 10.1093/ndt/gfm637 [DOI] [PubMed] [Google Scholar]
- 17.Miyasaka N, Kawai S, Hashimoto H. Efficacy and safety of tacrolimus for lupus nephritis: a placebo-controlled double-blind multicenter study. Mod Rheumatol. 2009;19(6):606-615. doi: 10.3109/s10165-009-0218-5 [DOI] [PubMed] [Google Scholar]
- 18.Mok CC, Tong KH, To CH, Siu YP, Au TC. Tacrolimus for induction therapy of diffuse proliferative lupus nephritis: an open-labeled pilot study. Kidney Int. 2005;68(2):813-817. doi: 10.1111/j.1523-1755.2005.00461.x [DOI] [PubMed] [Google Scholar]
- 19.Chen W, Tang X, Liu Q, et al. Short-term outcomes of induction therapy with tacrolimus versus cyclophosphamide for active lupus nephritis: a multicenter randomized clinical trial. Am J Kidney Dis. 2011;57(2):235-244. doi: 10.1053/j.ajkd.2010.08.036 [DOI] [PubMed] [Google Scholar]
- 20.Li X, Ren H, Zhang Q, et al. Mycophenolate mofetil or tacrolimus compared with intravenous cyclophosphamide in the induction treatment for active lupus nephritis. Nephrol Dial Transplant. 2012;27(4):1467-1472. doi: 10.1093/ndt/gfr484 [DOI] [PubMed] [Google Scholar]
- 21.Wang S, Li X, Qu L, et al. Tacrolimus versus cyclophosphamide as treatment for diffuse proliferative or membranous lupus nephritis: a non-randomized prospective cohort study. Lupus. 2012;21(9):1025-1035. doi: 10.1177/0961203312448105 [DOI] [PubMed] [Google Scholar]
- 22.Palmer SC, Tunnicliffe DJ, Singh-Grewal D, et al. Induction and maintenance immunosuppression treatment of proliferative lupus nephritis: a network meta-analysis of randomized trials. Am J Kidney Dis. 2017;70(3):324-336. doi: 10.1053/j.ajkd.2016.12.008 [DOI] [PubMed] [Google Scholar]
- 23.Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. doi: 10.1002/art.1780400928 [DOI] [PubMed] [Google Scholar]
- 24.Weening JJ, D’Agati VD, Schwartz MM, et al. ; International Society of Nephrology Working Group on the Classification of Lupus Nephritis; Renal Pathology Society Working Group on the Classification of Lupus Nephritis . The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004;65(2):521-530. doi: 10.1111/j.1523-1755.2004.00443.x [DOI] [PubMed] [Google Scholar]
- 25.Mok CC, Ying KY, Yim CW, et al. Tacrolimus versus mycophenolate mofetil for induction therapy of lupus nephritis: a randomised controlled trial and long-term follow-up. Ann Rheum Dis. 2016;75(1):30-36. doi: 10.1136/annrheumdis-2014-206456 [DOI] [PubMed] [Google Scholar]
- 26.Liu Z, Zhang H, Liu Z, et al. Multitarget therapy for induction treatment of lupus nephritis: a randomized trial. Ann Intern Med. 2015;162(1):18-26. doi: 10.7326/M14-1030 [DOI] [PubMed] [Google Scholar]
- 27.Korbet SM, Lewis EJ; Collaborative Study Group . Severe lupus nephritis: the predictive value of a ≥ 50% reduction in proteinuria at 6 months. Nephrol Dial Transplant. 2013;28(9):2313-2318. doi: 10.1093/ndt/gft201 [DOI] [PubMed] [Google Scholar]
- 28.Parodis I, Tamirou F, Houssiau FA. Prediction of prognosis and renal outcome in lupus nephritis. Lupus Sci Med. 2020;7(1):e000389. doi: 10.1136/lupus-2020-000389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Szeto C-C, Kwan BC-H, Lai FM-M, et al. Tacrolimus for the treatment of systemic lupus erythematosus with pure class V nephritis. Rheumatology (Oxford). 2008;47(11):1678-1681. doi: 10.1093/rheumatology/ken335 [DOI] [PubMed] [Google Scholar]
- 30.Okamoto M, Akioka K, Ushigome H, et al. Ten-year protocol biopsy findings of renal allografts in the calcineurin inhibitor era. Clin Transplant. 2006;20(suppl 15):16-19. doi: 10.1111/j.1399-0012.2006.00544.x [DOI] [PubMed] [Google Scholar]
- 31.Karolin A, Genitsch V, Sidler D. Calcineurin inhibitor toxicity in solid organ transplantation. Pharmacology. 2021;106(7-8):347-355. doi: 10.1159/000515933 [DOI] [PubMed] [Google Scholar]
- 32.Takeuchi T, Wakasugi N, Uno S, Makino H. Long-term safety and effectiveness of tacrolimus in lupus nephritis patients: 5-year interim post-marketing surveillance study in Japan (TRUST). J Rheumatol. 2021;48(1):74-81. doi: 10.3899/jrheum.191008 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol and Statistical Analysis Plan
eTable 1. Study Exclusion Criteria
eTable 2. Sensitivity and Subgroup Analyses of the Primary Efficacy End Point
eTable 3. Study Drug Compliance and Exposure (Safety Population)
eTable 4. Results of Sensitivity Analyses of Response Rate at Week 24
eTable 5. Subgroup Analyses: Response Rate by Different Pathological Types of LN at Week 24
eTable 6. Mean SCr Level and Mean Change from Baseline to Week 24
eFigure 1. Mean (SE) Change from Baseline to Week 24 in SLEDAI Score
eFigure 2. Mean (SE) Change from Baseline to Week 24 in Serum C3 and Serum C4
Data Sharing Statement