

Abstract
Background and aims
Internet gaming disorder (IGD) is associated with impaired inhibitory control and more impulsive decision-making. However, it remains unclear whether these associations are cross-sectional or predictive. We aimed to test the hypotheses that lower inhibitory control and more impulsive decision-making correlate with, are predicted by and predict more time spent on gaming and higher IGD severity.
Methods
A stratified convenience sample of 70 male participants (18–21 years) was recruited to achieve broad data variability for hours spent on gaming and IGD severity. In three annual assessments (T1, T2, T3), we measured gaming behaviour and IGD severity using the Video Game Dependency Scale (CSAS-II). Both gaming-related measures were correlates (T1), predictors (T2), or outcomes (T3) of inhibitory control and decision making, which were assessed at T2 using a go/no-go task and an intertemporal-choice task, respectively.
Results
Higher IGD severity at T1 predicted more impulsive decision-making at T2 (β = 0.45, 95% CI = 0.14–0.76). Lower inhibitory control at T2 predicted more hours spent on gaming at T3 (β = −0.13, 95% CI = −0.25 to −0.02). We found weak or no evidence for the other associations.
Discussion and conclusions
Lower inhibitory control predicts more time spent gaming, possibly due to insufficient top-down regulation of the behaviour. Impulsive decision-making is rather a consequence of IGD than a predictor, which may be due to altered reward learning. One-dimensional etiological assumptions about the relationship between neurocognitive impairments and IGD seem not to be appropriate for the complexity of the disorder.
Keywords: Internet gaming disorder, inhibitory control, decision-making, impulsivity, computer gaming
Introduction
Although impaired inhibitory control and impulsive decision-making are clearly associated with substance-related and addictive disorders (ADs; e.g. Brand et al., 2019; Goldstein & Volkow, 2011; Goschke, 2014; Redish, Jensen, & Johnson, 2008; van Holst, van den Brink, Veltman, & Goudriaan, 2010), it remains unclear whether these associations are cross-sectional or predictive. Internet gaming disorder (IGD) as a condition discussed as diagnostically and etiopathologically similar to other ADs such as gambling disorder has shown comparable neurocognitive impairments (Brand, Young, Laier, Wölfling, & Potenza, 2016; Fauth-Bühler & Mann, 2017; Petry et al., 2014). This study aimed to investigate whether lower inhibitory control and impulsive decision-making are only cross-sectionally associated with IGD or whether both neurocognitive impairments predict or are predicted by IGD.
Gaming has become a popular leisure activity worldwide, especially since the introduction of online multiplayer games, which combine social and competitive aspects (Nuyens et al., 2016). However, a meta-analysis of 33 worldwide studies has shown (using a conservative diagnostic approach) that about 3 % of all adolescents and young adults are diagnosed with IGD (Ferguson, Coulson, & Barnett, 2011). This estimate is consistent with recent research from Germany, where the current study was also conducted, which examined a representative sample of adolescents and estimated a prevalence of 3.5% (Wartberg, Kriston, & Thomasius, 2020). According to the eleventh revision of the International Classification of Diseases (ICD-11; World Health Organization, 2019), the clinical syndrome of IGD is characterised by a loss of behavioural control over gaming, an increased priority given to gaming over other interests and activities, and the continuation or escalation of gaming despite negative consequences. Substantial evidence for its clinical and public health relevance has led to the inclusion of IGD as a mental disorder in the ICD-11 and in Section 3 (‘Conditions for further study’) of the fifth revision of the Diagnostic and Statistical Manual of Mental Disorders (DSM 5; American Psychiatric Association (APA), 2013).
Given the rapid increase in Internet gaming, clarifying the underlying processes of IGD is important for developing effective intervention and prevention strategies. Several addiction models assume that dysfunctional changes in valuation systems and impaired cognitive control networks are two important mechanisms involved in ADs (e.g. Bickel et al., 2019; Goldstein & Volkow, 2011; Goschke, 2014; van Holst et al., 2010; Wiers, Gladwin, Hofmann, Salemink, & Ridderinkhof, 2013). As markers for these neurocognitive impairments, these studies focused on impulsive decision-making, i.e. the preference for immediate smaller rewards to the detriment of long-term rewards, and lower inhibitory control, i.e. a generally reduced ability to inhibit motor responses, both of which have been discussed as candidates for objective vulnerability markers of AD with and without substance use (Grant & Chamberlain, 2014). Accordingly, aetiological models of IGD and other behavioural addictions assume that lower inhibitory control and impulsive decision-making are also involved in the development and maintenance of IGD (Brand et al., 2019; Dong & Potenza, 2014). These assumptions are supported by previous cross-sectional case-control studies that show that IGD is associated with impaired task performance and/or functional alterations in brain regions in tasks measuring general inhibitory control, which are primarily go/no-go or stop-signal tasks (e.g. Irvine et al., 2013; Zheng et al., 2019; for meta-analyses of other studies see Argyriou, Davison, & Lee, 2017; Yao et al., 2017), and tasks measuring impulsive decision-making, which are primarily intertemporal choice paradigms (e.g. Irvine et al., 2013; Wang, Wu, Wang, et al., 2017; Wang, Wu, Zhou, et al., 2017; Zheng et al., 2019; for general overviews see Dong & Potenza, 2014; Fauth-Bühler & Mann, 2017; Şalvarlı & Griffiths, 2019).
Given the small number of longitudinal studies, it remains unclear whether lower general inhibitory control and more impulsive decision-making predict the course of IGD, are correlates of IGD, or whether IGD leads to neurocognitive changes that result impaired inhibitory control and decision-making. The I-PACE model assumes that IGD and other addictive behaviours develop as a consequence of interactions between predisposing variables, affective and cognitive responses to specific stimuli, and impaired executive functions, such as inhibitory control and decision-making (Brand et al., 2019). The cognitive-behavioural model of IGD by Dong and Potenza (2014) also includes inhibitory control and decision-making as two important domains that are altered in IGD. According to these models, lower general inhibitory control and more impulsive decision-making predict the development of IGD and are also symptoms during the course of IGD, which lead to unsuccessful attempts to control Internet gaming use. A generally lower inhibitory control may increase the risk for IGD and relapse because of an insufficient top-down regulation of attention, emotion and behaviour by long-term goals and an impaired ability to inhibit (cue-triggered) habitual, impulsive and reward-seeking responses (Brand et al., 2019; Dong & Potenza, 2014; Goschke, 2014). A generally increased impulsive decision-making may heighten the risk for IGD and relapse because immediate gratification by gaming is overvalued at the expense of long-term health, social and educational benefits (Brand et al., 2019; Dong & Potenza, 2014; Goschke, 2014). However, a lack of longitudinal studies on the relevance of inhibitory control and decision-making for the onset and course of IGD has been highlighted (Brand et al., 2019; Dong & Potenza, 2014). First evidence for a predictive relationship between impulsivity and later IGD was obtained from a longitudinal study in adolescents, which showed that heightened self-reported impulsivity is positively related to the current number and later progression of IGD symptoms (Gentile et al., 2011). Although there is some conceptual overlap between trait impulsivity, general inhibitory control and impulsive decision-making, there is strong evidence that these are subfacets of one construct or even distinct constructs (Aichert et al., 2012; Dick et al., 2010). Therefore, additional longitudinal studies using laboratory-based tasks to assess inhibitory control and impulsive decision making are needed to find out whether comparable predictive associations with IGD are evident.
So far, it remains open whether lower inhibitory control and more impulsive decision-making are both simultaneously and predictively associated with IGD. In addition, a further hypothesis could be that lower inhibitory control and more impulsive decision-making may develop as a consequence of someone living mainly in the dynamic, high-frequent and immediately rewarding environment of Internet games. We addressed this open research question in a prospective-longitudinal study and complemented the study of Gentile et al. (2011) by assessing IGD severity before, simultaneously and after general inhibitory control and impulsive decision-making, which were measured with experimental tasks. In addition, we distinguished between IGD severity as an indicator of clinical severity and gaming time as an indicator of engagement, as they had been shown to be differently associated with inhibitory control and decision-making, with cross-sectional findings suggesting a stronger relationship with clinical severity (Amlung, Vedelago, Acker, Balodis, & MacKillop, 2017; Smith, Mattick, Jamadar, & Iredale, 2014) and first longitudinal evidence suggesting a stronger predictive relationship with engagement (Fernie et al., 2013; Gustavson et al., 2017; Kräplin, Joshanloo, et al., in revision; Nigg et al., 2006; Wilens et al., 2011).
In sum, three hypotheses were tested in the current study: (i) lower general inhibitory control and more impulsive decision-making are cross-sectionally associated with more time spent on gaming and a higher IGD severity (Hypothesis 1: simultaneous association), (ii) lower inhibitory control and more impulsive decision-making are retrospectively associated with earlier more time spent on gaming and a higher IGD severity (Hypothesis 2: retrospective association) and (iii) lower inhibitory control and more impulsive decision-making are predictively associated with later more time spent on gaming and a higher IGD severity (Hypothesis 3: predictive association).
Methods
Design
Data collection for this project was conducted from 2010 to 2014 at the Criminological Research Institute of Lower Saxony, Germany (KFN) and focused on the personality and clinical characteristics of a sample with different degrees of IGD severity and their development over time1. Thorough diagnostic interviews were carried out at three time points to assess axis I disorders according to DSM-IV, focussing on the stability of IGD and its relationship to social, psychopathological and personality factors. As cooperation between the KFN and the Technische Universität Dresden, Germany, two behavioural paradigms from our lab were implemented at the second time point of the survey to assess inhibitory control and decision-making (see Fig. 1). For the purpose of this paper, only the measures and data on IGD severity, gaming behaviour, inhibitory control and decision-making are described in detail.
Fig. 1.

Flow chart of the study with the recruitment phase and the three annual assessments (T1, T2, T3)
Participants and procedure
A convenience sample of 70 male participants aged between 18 and 21 years was recruited at baseline (Table 1). The educational level of the participants was comparable to the German average. The preferred games were (first-person) shooter games (e.g. Counter-Strike), massively multiplayer online role-playing games (MMORPG, e.g. World of Warcraft) and multiplayer online battle arena games (MOBA, e.g. League of Legends). Recruitment was carried out with flyers posted in vocational schools and universities, at support organizations and outpatient treatment centres for IGD, and with postings in gaming-related chatrooms. Interested participants took part in a paper-pencil or online screening, including a screening on IGD severity and gaming behaviour (n = 2,313). A total of 1,092 persons were available as potential interview partners, as many interested participants did not provide contact details or only partially completed the questionnaire. Stratified sampling was used to achieve broad data variability for IGD severity and number of hours spent on gaming: about one third each with (a) regular gaming time (1–4.5 hours/day) but without IGD, (b) increased gaming time (>4.5 h/day) and at risk for IGD and (c) increased gaming time and probable IGD (for IGD definition, see subsection ‘Measures’). Seventy participants were included and invited to three annual surveys (T1, T2, T3) to assess IGD severity, gaming behaviour and - for T2 only – decision-making and inhibitory control (Fig. 1). The dropout rate was low, as 87% of the participants at baseline took part again after two years.
Table 1.
Participant characteristics for each of the three annual assessments (T1, T2, T3)
| T1 | T2 | T3 | ||
| Baseline | FU 1 year | FU 2 years | ||
| n (all male) | n (%) | 70 | 64 (91%) | 61 (87%) |
| Age | Mean (SD) range | 18.90 (1.07) 18–21 | 20.27 (1.09) 19–22 | 21.28 (1.08) 20–23 |
| Abitura | n (%) | 16 (23%) | 20 (31 %) | 30 (49%) |
| Living in partnership | n (%) | 29 (41%) | 27 (44%) | 29 (48%) |
| Household with parents | n (%) | 30 (43%) | 22 (36%) | 17 (28%) |
| Most preferred games | ||||
| (First-person) Shooter | n (%) | 21 (30%) | 14 (20%) | 13 (19%) |
| MMORPG | 15 (21%) | 8 (11%) | 7 (10%) | |
| MOBA | 8 (11%) | 15 (21%) | 17 (25%) |
Note: SD = standard deviation; FU = Follow-up; MMORPGs = massively multiplayer online role-playing games; MOBA = multiplayer online battle arena; IGD = Internet gaming disorder.
aGerman university entrance qualification.
Measures
Gaming behaviour and IGD severity
IGD severity was assessed with the Video Game Dependency Scale (abbreviated as CSAS-II for the second version of the German ‘Computerspielabhängigkeitsskala’; Rehbein, Kleimann, & Mößle, 2010; for an overview see King, Haagsma, Delfabbro, Gradisar, & Griffiths, 2013). Participants were instructed to respond to 14 items based on their gaming behaviour within the last 12 months and rated each item on a four-point scale: 1 = strongly disagree, 2 = somewhat disagree, 3 = somewhat agree, 4 = strongly agree. The CSAS-II2 measures preoccupation, loss of control, conflicts, withdrawal symptoms and tolerance. This scale shows convergent validity with sleep difficulties, lower activity levels and suicidal thoughts and adequate criterion validity (r = 0.59) with self-reported gaming activity (Rehbein et al., 2010). The CSAS-II has a Cronbach's alpha of .92 and the items have a high item difficulty and a high discrimination value (Rehbein et al., 2010). Based on these previous results regarding the high internal consistency of the scale, we decided to use the total score of the CSAS-II as operationalization for IGD severity. The cut-off score for ‘at risk for IGD’ is a total score of 35 and for ‘probable IGD’ it is 42. The CSAS-II was used in the paper-pencil or online screening version at T12 and in the personal interviews at T2 and T3 to assess IGD severity over the last 12 months. In order to determine gaming time and the three most preferred games, questions on gaming behaviour were included in the personal interviews at T1, T2 and T3.
Inhibitory control
Lower inhibitory control was defined a reduced ability to inhibit motor responses. As a well-established paradigm to assess this construct, a go/no-go task was used. We applied a proven go/no-go task from our lab, for which basic task effects have already been confirmed Beck et al., 2016. In 300 trials, participants were instructed to respond as fast as possible to the letter ‘M’ (go trials), but to withhold their response to the letter ‘W’ (no-go trials). In 20% randomly selected trials, no-go stimuli were presented. After a fixation cross of 300 milliseconds (ms), the letters were presented for 150 ms at the centre of the screen. The intertrial interval varied randomly between 1,250 and 1,750 ms. Error rates and reaction times were combined to inverse efficiency scores (IES; Bruyer & Brysbaert, 2011) to account for individual differences in the balance of the speed-accuracy trade-off (Bogacz, Wagenmakers, Forstmann, & Nieuwenhuis, 2010). Reaction times for error trials and trials immediately following errors were excluded. Reaction times below 100 ms and deviating from the median by more than 3.32 median absolute deviations were also excluded (Wilcox & Keselman, 2003). Higher IES indicate lower inhibitory control, i.e. higher error rates and/or slower reaction times. For better interpretation, the IES were reversed so that higher scores always indicate higher inhibitory control (according to Wolff et al., 2016).
Impulsive decision-making
Impulsive decision-making was defined as the preference for immediate smaller rewards to the detriment of long-term rewards, which is also termed as higher delay-discounting or lower delay of gratification. To measure impulsive decision-making, we used an already validated intertemporal choice task from our lab Kräplin et al., 2014. In 192 trials, participants were instructed to choose between a smaller monetary gain delivered sooner and a larger monetary gain delivered later. The sooner/smaller gain was randomly selected from a pool of items with a mean value of 20 euros, a standard deviation of two euros, and a range between 17 and 23 euros. The value of the later/larger reward was obtained by increasing the sooner/smaller reward by 1, 3.5, 7, 12, 18, 27, 40, or 80%. The time delay for the sooner/smaller reward was either ‘now’, in 7, or in 14 days and the later/larger reward was additionally delayed by 1, 2, 3, 5, 7, 9, 12, or 15 days. All participants were instructed to respond to the hypothetical choices as if they were real choices. The values of the rewards and the time delays were systematically varied to determine the indifference points for each participant. These points represent the subjective equivalence between the immediate and delayed rewards. For each subject a hyperbolic function was fitted to the indifference points over the different delay intervals (Mazur, 1987). Our dependent variable was the extracted k parameter of each hyperbolic function. A higher k value indicates steeper discounting of a delayed reward and more impulsive decision-making.
Statistical analysis
The visual inspection of our data revealed that neither the IGD severity and gaming time nor the IES (go/no-go task) and k-values (intertemporal choice task) were normally distributed and that some participants showed extreme values in the task outcomes, which we did not want to exclude because they were plausible given our previous experience with these tasks in clinical and healthy samples (for data distributions, see Fig. S1 in the supplemental material). Therefore, we applied robust regression analyses for hypotheses testing, since robust estimates of the model parameters and standard errors have been strongly recommended for clinical and experimental data, which usually violate the assumptions of common statistical methods (Field & Wilcox, 2017). Robust regression also accounts for residuals with different variances and extreme values that would otherwise have a strong impact on results (narrowing the scope of a mean effect results). We tested three hypotheses: (i) lower general inhibitory control and more impulsive decision-making are cross-sectionally associated with more time spent on gaming and a higher IGD severity, (ii) lower inhibitory control and more impulsive decision-making are retrospectively associated with earlier more time spent on gaming and a higher IGD severity and (iii) lower inhibitory control and more impulsive decision-making are predictively associated with later more time spent on gaming and a higher IGD severity. Separate regression models were performed for each IGD measure, i.e. gaming time and IGD severity and each neurocognitive measure, i.e. inhibitory control (IES from the go/no-go task) and impulsive decision-making (k value from the intertemporal choice task, Fig. 2). Regression model 1 (M1) tested Hypotheses 1, i.e. the simultaneous association between gaming time or IGD severity at T2 and the IES or k values at T2. Regression model 2 (M2) tested Hypothesis 2, i.e. the retrospective association between gaming time or IGD severity time at T1 and the IES or k values at T2. It was important to control for gaming time or IGD severity at T2 to obtain the ‘pure’ retrospective relationships. Regression model 3 (M3) tested Hypothesis 3, i.e. the predictive association between the IES or k values at T2 and the gaming time or IGD severity at T3. Again, it was controlled for gaming time or IGD severity at T2 to obtain the pure predictive relationships. In all regression models we additionally controlled for age and school type at T2 (at the time of task performance), since lower age and lower school graduation are theoretically and empirically associated with lower general inhibitory control and more impulsive decision-making (Liu et al., 2019; Reimers, Maylor, Stewart, & Chater, 2009). Except for descriptive data, we report the z-standardized values for regression analysis results for better interpretation of results. All statistical analyses were conducted using Stata 15.1 (Stata Corp., 2019). Our hypotheses have not been pre-registered. For reasons of research transparency, the primary data and the Stata do files of the analyses can be downloaded from the Open Science Framework (OSF) under https://osf.io/3hp7k.
Fig. 2.
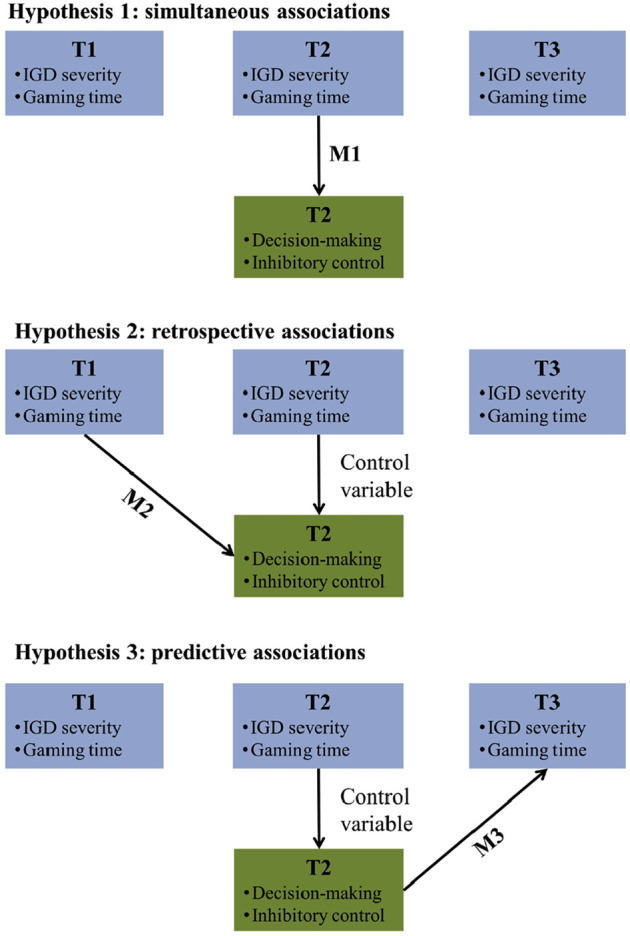
Schema of the study time points, predictors and outcomes according to the three hypotheses.
Note: M = Robust regression models for hypotheses testing
Ethics
The study procedures were carried out in accordance with the Declaration of Helsinki. The Ethics Committee of the German Society for Psychology (DGPs) approved the study (Reference number ‘Moessle122010’). All participants were informed about the study and all provided written informed consent.
Results
Internet gaming disorder
Descriptive data for IGD severity and gaming hours are shown in Table 2. Over time, there was an overall significant decrease in IGD severity (F(1.65, 100.04) = 75.73, P < 0.001), which was significant for the post-hoc contrasts between T1 and T2 (t = −7.53, P < 0.001) and between T2 and T3 (t = −12.16, P < 0.001). There was also a significant overall decrease in hours spent gaming (F(1.60, 97.07) = 13.07, P < 0.001) and the post-hoc contrasts showed significant differences between T1 and T2 (t = −2.62, P = 0.01) and between T2 and T3 (t = −5.11, P < 0.001). While 16 participants (22%) were screened as probable having an IGD according to the CSAS-II at T1, 2 were positively screened at T2 and 0 at T3.
Table 2.
Descriptive data of the study variables by time points
| T1 | T2 | T3 | ||
| Baseline | FU 1 year | FU 2 years | ||
| n (all male) | n (%) | 70 | 64 (91%) | 61 (87%) |
| IGD severitya | Mean (SD) range | 34.14 (8.45) 19–51 | 25.84 (7.16) 14–43 | 20.75 (5.60) 14–38 |
| Hours spent on gaming per day | Mean (SD) range | 4.21 (3.11) 0–14b | 3.39 (2.22) 0–10 | 2.40 (2.06) 0–9 |
| General inhibitory control in go/no-go task | ||||
| Inverse efficiency score (milliseconds) | Mean (SD) | – | 447.74 (131.62) | – |
| Impulsive decision-making in intertemporal choice task | ||||
| k value | Mean (SD) | – | 0.06 (0.04) | – |
Note: SD = standard deviation; FU = Follow-up; IGD Internet gaming disorder.
aMeasured with the Video Game Dependency Scale (CSAS-II). The CSAS-II sum scores (see subsection Measures) range from 14 to 56, cut-off >35 for ‘at risk for IGD’, cut-off > 42 for ‘probable IGD’.
bFor T1, it should be noted that the CSAS-II was measured within the paper-pencil or online screening while the gaming time was measured in the personal interview, which took place on average eight weeks later (range from 1 to 24 weeks). The (current) gaming time from the interview may therefore contradict the IGD severity from the CSAS-IIs, e.g. if someone has successfully restricted the gaming time in the meantime. This is no issue for our analyses, because separate analyses were performed for gaming time and IGD severity.
Inhibitory control
Descriptive data for the go/no-go task are shown in Table 2. The mean false alarm rate was 19% (SD = 18%) and the mean go-reaction time was 344.33 ms (SD = 53.73ms). The results of the hypotheses testing for inhibitory control are shown in Fig. 3. Further details for the robust regression models can be found in the supplemental material (Table S1; results of the ordinary linear regression are shown in Table S2). The robust regression model 3 (M3) revealed a significant prospective association between lower inhibitory control at T2 and more hours spent on gaming one year later at T3 (β = −0.13, P = 0.03). The confidence interval was closely to 0, which suggests small associations (95%CI = −0.25–0.02). There were no other significant associations. In summary, we found evidence that lower inhibitory control is predictively associated with an increased amount of time spent on gaming after one year.
Fig. 3.

Overview of the results for the three (independent) robust regression models (M1 to M3) to test the associations between (A) IGD severity or (B) gaming time across the three annual assessments (T1 to T3) and inhibitory control at T2.
Note. Predictors and outcomes were both z-standardized, yielding standardized regression coefficients that have the same range as correlations. Bold numbers indicate significant associations at P < 0.05.
IGD = Internet gaming disorder; CI = 95% confidence interval.
Decision-making
Descriptive data for the intertemporal choice task are shown in Table 2. The mean ratio of sooner/smaller choices was 40.15% (SD = 23.26%). Results of the hypotheses testing for decision-making are shown in Fig. 4. Detailed results of the robust regression models can be found in the supplemental material (Table S1; results of the ordinary linear regression are shown in Table S2). The robust regression model 1 (M1) revealed a significant retrospective association between increased IGD severity at T1 and steeper delay discounting one year later at T2 (β = 0.45, P = 0.03). The confidence interval for this association suggested small to large associations (95%CI = 0.14–0.76). There were no other significant associations. In summary, we found evidence that more impulsive decision-making is retrospectively associated with more IGD symptoms one year ago.
Fig. 4.

Overview of the results for the three (independent) robust regression models (M1 to M3) to test the association between (A) IGD severity or (B) gaming hours over the three annual assessments (T1 to T3) and impulsive decision-making at T2.
Note. Predictors and outcomes were both z-standardized, yielding standardized regression coefficients that have the same range as correlations. Bold numbers indicate a significant association at P <0.05.
IGD = Internet gaming disorder; CI = 95% confidence interval.
Discussion
As one of few studies with a prospective longitudinal design, we tested whether lower general inhibitory control and more impulsive decision-making are simultaneously, retrospectively and prospectively associated with more time spent on gaming and a higher IGD severity. We found evidence that lower general inhibitory control is predictively associated with more gaming behaviour one year later and that more impulsive decision-making is retrospectively associated with a higher IGD severity one year ago. However, we found only weak or no evidence for the other associations.
Over the three assessment time points of our study, we found strong evidence for an overall decrease in time spent on gaming and IGD severity. This is in line with previous studies showing a high rate of spontaneous remission in the natural course of IGD and raises the important question of which factors contribute to the course of IGD (Ko, Yen, Yen, Lin, & Yang, 2007; Lau, Wu, Gross, Cheng, & Lau, 2017; Wartberg & Lindenberg, 2020). In line with our hypothesis, we found evidence that a lower general inhibitory control is predictively associated with more time spent on gaming one year later, but there was weak or no evidence that inhibitory control is associated with the past or current gaming time or IGD severity. Impaired general inhibitory control may play a more important role in unsuccessful attempts to control or stop the gaming behaviour than in the reduction of IGD symptoms. This underlines the assumption of several models on ADs that over the course (in our specific case) of IGD behavioural control by general inhibitory mechanisms becomes more difficult and individuals are less able to inhibit desires and reward-seeking behaviour, which results in more habitual and impulsive gaming (e.g. Brand et al., 2019; Dong & Potenza, 2014; Goldstein & Volkow, 2011; Goschke, 2014). This assumption is further supported by results from previous longitudinal studies that consistently found evidence that lower cognitive control abilities predict the amount of substance use and substance-related problems, but found weak evidence for predictive associations with substance-related AD symptoms (Fernie et al., 2013; Gustavson et al., 2017; Kräplin, Joshanloo, et al., in revision; Nigg et al., 2006; Wilens et al., 2011). In contrast to these studies on the course of substance-related ADs, one of few longitudinal studies on the course of IGD showed that heightened trait impulsivity was positively associated with the progression of IGD symptoms (Gentile et al., 2011). However, there is strong evidence that trait impulsivity and general inhibitory control are subfacets of one construct or even distinct constructs (Aichert et al., 2012; Dick et al., 2010). In contrast to general inhibitory control, self-reported trait impulsivity may also include a self-evaluation of one''s current gaming behaviour, which is probably the best predictor for future gaming behaviour. Concerning cross-sectional evidence of the association between lower inhibitory control and IGD, a meta-analysis found overall medium group differences between participants with IGD and healthy controls in tasks measuring response inhibition (Argyriou et al., 2017). These studies were based on case-control designs that compared performance between IGD patients or participants who were positively screened for IGD and healthy controls in response inhibition tasks. Compared to these studies, we were interested in linear associations between inhibitory control and the natural course of IGD severity and the amount of gaming time. We also observed an overall decrease of IGD severity and gaming hours over time, with 22% of cases screened positive for IGD at baseline compared to zero cases after three years. The linear association between general inhibitory control and IGD may be stronger in individuals above a clinically meaningful threshold, which would explain the stronger effects in previous case-control studies compared to our study. Another aspect to be discussed is that we investigated general response inhibition using a behavioural task without game-related contexts. According to the I-PACE model, stimulus-specific inhibitory control may be more important than general inhibition abilities in the later stages of addiction processes (Brand et al., 2019). General inhibitory control might be important for the amount of time spent on gaming itself, while context-specific inhibitory control is more important when conflicts between a cue-triggered desire to game and superordinate goals such as academic achievements or social roles are involved (Brand et al., 2019).
Regarding decision-making, results revealed evidence that IGD severity is associated with a later steeper delay discounting, whereas weak or no evidence was found for associations with the current or later IGD severity or gaming time. These results are consistent with a longitudinal study from our lab that showed evidence that delay discounting rather predicts substance-related symptoms than behavioural addiction symptoms after one year (Kräplin et al., 2020). To the best of our knowledge, we conducted the first study that assessed IGD severity prior to decision-making. Our results contribute to aetiological models by showing that IGD may change the decision-making tendencies of individuals. This has so far not been explicitly mentioned in aetiological models on ADs without substance use but in models on substance-related ADs, where this change has already been discussed as possible mechanism of progression (De Wit, 2009). In addition to the long-term sequelae of substance use on decision-making, our results suggest that also behavioural addictions such as IGD are associated with more dysfunctional changes in reward-based learning that lead to a general overvaluation of immediate rewards (Everitt & Robbins, 2016) and/or an attenuated valuation of anticipated long-term rewards (Krönke et al., 2020). Although no substance use and thus no neurotoxic effects on the brain are involved in IGD, changes in reward processing could occur as a consequence of conditioning within the often immediately rewarding environments of Internet games (Fauth-Bühler & Mann, 2017). However, we did not investigate our participants before the development of their IGD symptoms. Therefore, impulsive decision-making may be both a predisposing risk factor for the onset of IGD and may also worsen over time as the disorder develops (Dong & Potenza, 2014; Fineberg et al., 2014).
Limitations
At the time of the initial study planning and implementation, there were no established criteria for the diagnosis of IGD. Therefore, we used the CSAS-II, a reliable and valid instrument to assess IGD severity (Rehbein et al., 2010). However, compared to a later adaptation of the CSAS-II (CSAS; Rehbein, Kliem, Baier, Mößle, & Petry, 2015), our version did not cover all nine DSM-5 criteria for IGD (escape adverse moods is missing). In addition, for six participants at T1 one item was missing in the total CSAS score (the ‘withdrawal’ item). It may therefore be that we overlooked certain aspects of IGD severity and underestimated associations. Regarding our IGD measures, it should also be mentioned that we assessed the current gaming time in comparison to the IGD severity that we assessed over the past 12 months. Associations may be stronger for a time-point measure than for a cumulative measure over several months, which involve a larger measurement error. Moreover, our recruitment strategy may have led to a selection bias. For example, persons with more impulsive decision-making might not have been attracted by a study with long interviews, where incentives were given at the end. Another specific characteristic of our sample is that it includes only male participants from Germany. Although young men are the population with the highest prevalence rates of IGD (Mentzoni et al., 2011; Rehbein et al., 2010), it may still be important to investigate gender differences. In addition, the generalisability of our results across cultures remains open. Another observation in our sample was that we had 22% positively screened clinical cases with IGD at baseline, but no cases at the 3-years follow-up. It might be the case that the intensive clinical interviews had some interventional character and therefore symptoms decreased over time. However, since the participants started in late adolescence and ended in early adulthood after three years, the explanation of ‘maturing out’ is more likely, i.e. that role transitions (e.g. partnership, employment and starting a family) and changed consumption motives are associated with a decrease in addictive use (e.g. Lee, Ellingson, & Sher, 2015; Littlefield, Sher, & Wood, 2010). Further sources of bias could be unconsidered confounders (common causes) that may underlie both inhibitory control or decision-making and IGD severity such as neuroendophenotypes (Robbins et al. 2012).
Conclusions
We found evidence in young men (i) that lower general inhibitory control is more likely to be a predictor of later prolonged time spent gaming than of later higher IGD severity and (ii) that more impulsive decision-making is more likely to be consequence of higher IGD severity than a predictor. One-dimensional etiological assumptions about IGD (e.g. lower inhibitory control as cause of IGD) seem not to be appropriate for the complexity of the disorder. Even with follow-ups over three years, we may not have fully captured the circular relationship between lower inhibitory control or impulsive decision making and IGD or gaming. Moreover, the revealed associations were small to medium-sized, suggesting that lower inhibitory control and impulsive decision-making are certainly only two of many intra-individual factors in the course of IGD that need to be considered in interaction with other factors such as cue-reactivity, reward processing, error monitoring, or emotion regulation (Brand et al., 2019; Dong & Potenza, 2014; Goschke, 2014). Further studies are needed that assess inhibitory control and decision-making prior to the onset of IGD and that use interventions to investigate whether a causal relationship exists (Goudriaan, 2020; Verdejo-García, Alcázar-Córcoles, & Albein-Urios, 2019).
Funding sources
The overall project was funded by the Ministry for Science and Culture of Lower Saxony, Germany. Research published in this paper was supported by a grant from the Deutsche Forschungsgemeinschaft (DFG) for the Collaborative Research Centre 940 (project number 178833530). Open Access was funded by the Publication Fund of the Technische Universität Dresden, Germany.
Authors' contribution
FR and TM designed the overall project and, together with EMK, the dissertation project in which the data for the presented study were collected. EMK recruited the participants and conducted the data collection. AK, GB and TG conceptualised the sub-study for this article. SS programmed the behavioural tasks for the study and supported data analysis. AK carried out the literature search, analysed the data and wrote the first draft of the manuscript. TM supported the data exchange and analysis. All authors contributed substantially to the revision and final approval of the manuscript.
Conflict of interest
Anja Kräplin, Stefan Scherbaum, Eva-Maria Kraft, Florian Rehbein, Thomas Goschke and Thomas Mößle have no conflicts of interests to declare. Gerhard Bühringer has received unrestricted research grants from the Bavarian State Ministry of Finance (regulatory authority for and operator of the state gambling monopoly), via the Bavarian State Ministry of the Environment and Public Health, the German Federal Ministry of Economics and Technology (regulatory authority for the commercial gambling industry) and from public and private gambling providers.
Supplementary Material
Footnotes
Data collection was part of the dissertation project of Dr Eva-Maria Kraft, which was part of the project ‘Computerspiel-und Internetabhängigkeit: Diagnostik, Ätiopathogenese, Therapie und Prävention’ [Computer game and internet addiction: diagnostics, aetiopathogenesis, therapy and prevention] at the KFN. Hypotheses and data analyses for this paper were independent of the dissertation project.
Please note that for six participants (from the first assessed school), one item of the CSAS-II was missing for the calculation of the total score (‘withdrawal’ item) due to a mistake of the experimenter.
References
- Aichert, D. S., Wöstmann, N. M., Costa, A., Macare, C., Wenig, J. R., Möller, H.-J., et al. (2012). Associations between trait impulsivity and prepotent response inhibition. Journal of Clinical and Experimental Neuropsychology, 34(10), 1016–1032. 10.1080/13803395.2012.706261. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association (APA) . (2013). Diagnostic and statistical manual of mental disorders (DSM-5®) (5th ed.). Washington, DC: American Psychiatric Association. [Google Scholar]
- Amlung, M., Vedelago, L., Acker, J., Balodis, I., & MacKillop, J. (2017). Steep delay discounting and addictive behavior: A meta-analysis of continuous associations. Addiction, 112(1), 51–62. 10.1111/add.13535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Argyriou, E., Davison, C. B., & Lee, T. T. (2017). Response inhibition and Internet gaming disorder: A meta-analysis. Addictive Behaviors, 71, 54–60. 10.1016/j.addbeh.2017.02.026. [DOI] [PubMed] [Google Scholar]
- Beck, S. M., Ruge, H., Schindler, C., Burkart, M., Miller, R., Kirschbaum, C., & Goschke, T. (2016). Effects of Ginkgo biloba extract EGb 761® on cognitive control functions, mental activity of the prefrontal cortex and stress reactivity in elderly adults with subjective memory impairment – a randomized double-blind placebo-controlled trial. Human Psychopharmacology: Clinical and Experimental, 31(3), 227–242. 10.1002/hup.2534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel, W. K., Athamneh, L. N., Basso, J. C., Mellis, A. M., DeHart, W. B., Craft, W. H.et al. (2019). Excessive discounting of delayed reinforcers as a trans-disease process. Current Opinion in Psychology, 30, 59–64. 10.1016/j.copsyc.2019.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogacz, R., Wagenmakers, E.-J., Forstmann, B. U., & Nieuwenhuis, S. (2010). The neural basis of the speed–accuracy tradeoff. Trends in Neurosciences, 33(1), 10–16. 10.1016/j.tins.2009.09.002. [DOI] [PubMed] [Google Scholar]
- Brand, M., Wegmann, E., Stark, R., Müller, A., Wölfling, K., Robbins, T. W., et al. (2019). The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neuroscience & Biobehavioral Reviews, 104, 1–10. 10.1016/j.neubiorev.2019.06.032. [DOI] [PubMed] [Google Scholar]
- Brand, M., Young, K. S., Laier, C., Wölfling, K., & Potenza, M. N. (2016). Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model. Neuroscience & Biobehavioral Reviews, 71, 252–266. 10.1016/j.neubiorev.2016.08.033. [DOI] [PubMed] [Google Scholar]
- Bruyer, R., & Brysbaert, M. (2011). Combining speed and accuracy in cognitive psychology: Is the inverse efficiency score (IES) a better dependent variable than the mean reaction time (RT) and the percentage of errors (PE)? Psychologica Belgica, 51(1), 5–13. 10.5334/pb-51-1-5. [DOI] [Google Scholar]
- Stata Corp . (2019). Stata statistical software: Release 15.1 Stata Corporation. [Google Scholar]
- De Wit, H. (2009). Impulsivity as a determinant and consequence of drug use: A review of underlying processes. Addiction Biology, 14(1), 22–31. 10.1111/j.1369-1600.2008.00129.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dick, D. M., Smith, G., Olausson, P., Mitchell, S. H., Leeman, R. F., O'Malley, S. S., et al. (2010). Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addiction Biology, 15(2), 217–226. 10.1111/j.1369-1600.2009.00190.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dong, G., & Potenza, M. N. (2014). A cognitive-behavioral model of Internet gaming disorder: Theoretical underpinnings and clinical implications. Journal of Psychiatric Research, 58, 7–11. 10.1016/j.jpsychires.2014.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Everitt, B. J., & Robbins, T. W. (2016). Drug addiction: Updating actions to habits to compulsions ten years on. Annual Review of Psychology, 67(1), 23–50. 10.1146/annurev-psych-122414-033457. [DOI] [PubMed] [Google Scholar]
- Fauth-Bühler, M., & Mann, K. (2017). Neurobiological correlates of internet gaming disorder: Similarities to pathological gambling. Addictive Behaviors, 64, 349–356. 10.1016/j.addbeh.2015.11.004. [DOI] [PubMed] [Google Scholar]
- Ferguson, C. J., Coulson, M., & Barnett, J. (2011). A meta-analysis of pathological gaming prevalence and comorbidity with mental health, academic and social problems. Journal of Psychiatric Research, 45(12), 1573–1578. 10.1016/j.jpsychires.2011.09.005. [DOI] [PubMed] [Google Scholar]
- Fernie, G., Peeters, M., Gullo, M. J., Christiansen, P., Cole, J. C., Sumnall, H., et al. (2013). Multiple behavioural impulsivity tasks predict prospective alcohol involvement in adolescents. Addiction, 108(11), 1916–1923. 10.1111/add.12283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field, A. P., & Wilcox, R. R. (2017). Robust statistical methods: A primer for clinical psychology and experimental psychopathology researchers. Behaviour Research and Therapy, 98, 19–38. 10.1016/j.brat.2017.05.013. [DOI] [PubMed] [Google Scholar]
- Fineberg, N. A., Chamberlain, S. R., Goudriaan, A. E., Stein, D. J., Vanderschuren, L. J. M. J., Gillan, C. M., et al. (2014). New developments in human neurocognition: Clinical, genetic, and brain imaging correlates of impulsivity and compulsivity. CNS Spectrums, 19(1), 69–89. 10.1017/S1092852913000801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gentile, D. A., Choo, H., Liau, A., Sim, T., Li, D., Fung, D., et al. (2011). Pathological video game use among youths: A two-year longitudinal study. Pediatrics, 127(2), e319–e329. 10.1542/peds.2010-1353. [DOI] [PubMed] [Google Scholar]
- Goldstein, R. Z., & Volkow, N. D. (2011). Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nature Reviews Neuroscience, 12(11), 652–669. 10.1038/nrn3119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goschke, T. (2014). Dysfunctions of decision-making and cognitive control as transdiagnostic mechanisms of mental disorders: Advances, gaps, and needs in current research. International Journal of Methods in Psychiatric Research, 23(S1), 41–57. 10.1002/mpr.1410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goudriaan, A. E. (2020). Integrating neurocognition from bench to bedside in gambling disorder: From neurocognitive to translational studies. Current Opinion in Behavioral Sciences, 31, 83–88. 10.1016/j.cobeha.2019.12.012. [DOI] [Google Scholar]
- Grant, J. E., & Chamberlain, S. R. (2014). Impulsive action and impulsive choice across substance and behavioral addictions: Cause or consequence? Addictive Behaviors, 39(11), 1632–1639. 10.1016/j.addbeh.2014.04.022. [DOI] [PubMed] [Google Scholar]
- Gustavson, D. E., Stallings, M. C., Corley, R. P., Miyake, A., Hewitt, J. K., & Friedman, N. P. (2017). Executive functions and substance use: Relations in late adolescence and early adulthood. Journal of Abnormal Psychology, 126(2), 257–270. 10.1037/abn0000250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Holst, R. J., van den Brink, W., Veltman, D. J., & Goudriaan, A. E. (2010). Why gamblers fail to win: A review of cognitive and neuroimaging findings in pathological gambling. Neuroscience & Biobehavioral Reviews, 34, 87–107. 10.1016/j.neubiorev.2009.07.007. [DOI] [PubMed] [Google Scholar]
- Irvine, M. A., Worbe, Y., Bolton, S., Harrison, N. A., Bullmore, E. T., & Voon, V. (2013). Impaired decisional impulsivity in pathological videogamers. PloS One, 8(10), e75914. 10.1371/journal.pone.0075914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King, D. L., Haagsma, M. C., Delfabbro, P. H., Gradisar, M., & Griffiths, M. D. (2013). Toward a consensus definition of pathological video-gaming: A systematic review of psychometric assessment tools. Clinical Psychology Review, 33(3), 331–342. 10.1016/j.cpr.2013.01.002. [DOI] [PubMed] [Google Scholar]
- Ko, C.-H., Yen, J.-Y., Yen, C.-F., Lin, H.-C., & Yang, M.-J. (2007). Factors predictive for incidence and remission of Internet addiction in young adolescents: A prospective study. CyberPsychology and Behavior, 10(4), 545–551. 10.1089/cpb.2007.9992. [DOI] [PubMed] [Google Scholar]
- Kräplin, A., Dshemuchadse, M., Scherbaum, S., Behrendt, S., Goschke, T., & Bühringer, G. (2014). Dysfunctional decision-making in pathological gambling: pattern specificity and the role of impulsivity. Psychiatry Research, 215(3), 675–682. 10.1016/j.psychres.2013.12.041. [DOI] [PubMed] [Google Scholar]
- Kräplin, A., Höfler, M., Pooseh, S., Wolff, M., Krönke, K.-M., Goschke, T., et al. (2020). Impulsive decision-making predicts the course of substance-related and addictive disorders. Psychopharmacology, 237(9), 2709–2724. 10.1007/s00213-020-05567-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kräplin, A., Joshanloo, M., Wolff, M., Krönke, K.-M., Bühringer, G., Goschke, T., & Smolka, M. N. (2020). Latent executive functioning in substance-related and addictive disorders: Cross-sectional and longitudinal relations. Addiction. (in revision). [Google Scholar]
- Krönke, K.-M., Wolff, M., Mohr, H., Kräplin, A., Smolka, M. N., Bühringer, G., et al. (2020). Predicting real-life self-control from brain activity encoding the value of anticipated future outcomes. Psychological Science, 31(3), 268–279. 10.1177/0956797619896357. [DOI] [PubMed] [Google Scholar]
- Lau, J. T. F., Wu, A. M. S., Gross, D. L., Cheng, K.-M., & Lau, M. M. C. (2017). Is Internet addiction transitory or persistent? Incidence and prospective predictors of remission of Internet addiction among Chinese secondary school students. Addictive Behaviors, 74, 55–62. 10.1016/j.addbeh.2017.05.034. [DOI] [PubMed] [Google Scholar]
- Lee, M. R., Ellingson, J. M., & Sher, K. J. (2015). Integrating social-contextual and intrapersonal mechanisms of "maturing out": Joint influences of familial-role transitions and personality maturation on problem-drinking reductions. Alcoholism: Clinical and Experimental Research, 39(9), 1775–1787. 10.1111/acer.12816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littlefield, A. K., Sher, K. J., & Wood, P. K. (2010). Do changes in drinking motives mediate the relation between personality change and "maturing out" of problem drinking? Journal of Abnormal Psychology, 119(1), 93–105. 10.1037/a0017512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Y., van den Wildenberg, W. P. M., de Graaf, Y., Ames, S. L., Baldacchino, A., Ragnhild, B., et al. (2019). Is (poly-) substance use associated with impaired inhibitory control? A mega-analysis controlling for confounders. Neuroscience & Biobehavioral Reviews, 105, 288–304. 10.1016/j.neubiorev.2019.07.006. [DOI] [PubMed] [Google Scholar]
- Mazur, J. E. (1987). An adjusting procedure for studying delayed reinforcement. In Commons M. L., Mazur J.E., Nevin J.A., & Rachlin H. (Eds.), Quantitative analyses of behavior: The effect of delay and of intervening events on reinforcement value (5th ed., pp. 55–73). Hillsdale, NJ: Lawrence ErlbaumAssociates, Inc. [Google Scholar]
- Mentzoni, R. A., Brunborg, G. S., Molde, H., Myrseth, H., Skouverøe, K. J. M., Hetland, J., et al. (2011). Problematic video game use: Estimated prevalence and associations with mental and physical health. Cyberpsychology, Behavior, and Social Networking, 14(10), 591–596. 10.1089/cyber.2010.0260. [DOI] [PubMed] [Google Scholar]
- Nigg, J. T., Wong, M. M., Martel, M. M., Jester, J. M., Puttler, L. I., Glass, J. M., et al. (2006). Poor response inhibition as a predictor of problem drinking and illicit drug use in adolescents at risk for alcoholism and other substance use disorders. Journal of the American Academy of Child and Adolescent Psychiatry, 45(4), 468–475. 10.1097/01.chi.0000199028.76452.a9. [DOI] [PubMed] [Google Scholar]
- Nuyens, F., Deleuze, J., Maurage, P., Griffiths, M. D., Kuss, D. J., & Billieux, J. (2016). Impulsivity in multiplayer online battle arena gamers: Preliminary results on experimental and self-report measures. Journal of Behavioral Addictions, 5(2), 351–356. 10.1556/2006.5.2016.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petry, N. M., Rehbein, F., Gentile, D. A., Lemmens, J. S., Rumpf, H.-J., Mößle, T., et al. (2014). An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction, 109(9), 1399–1406. 10.1111/add.12457. [DOI] [PubMed] [Google Scholar]
- Redish, A. D., Jensen, S., & Johnson, A. (2008). A unified framework for addiction: Vulnerabilities in the decision process. Behavioral and Brain Sciences, 31, 415–487. 10.1017/S0140525X0800472X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rehbein, F., Kleimann, M., & Mößle, T. (2010). Prevalence and risk factors of video game dependency in adolescence: Results of a German nationwide survey. Cyberpsychology, Behavior, and Social Networking, 13(3), 269–277. 10.1089/cyber.2009.0227. [DOI] [PubMed] [Google Scholar]
- Rehbein, F., Kliem, S., Baier, D., Mößle, T., & Petry, N. M. (2015). Prevalence of internet gaming disorder in German adolescents: Diagnostic contribution of the nine DSM-5 criteria in a state-wide representative sample. Addiction, 110(5), 842–851. 10.1111/add.12849. [DOI] [PubMed] [Google Scholar]
- Reimers, S., Maylor, E. A., Stewart, N., & Chater, N. (2009). Associations between a one-shot delay discounting measure and age, income, education and real-world impulsive behavior. Personality and Individual Differences, 47(8), 973–978. 10.1016/j.paid.2009.07.026. [DOI] [Google Scholar]
- Şalvarlı, Ş. İ., & Griffiths, M. D. (2019). The association between Internet gaming disorder and impulsivity: A systematic review of literature. International Journal of Mental Health and Addiction. 10.1007/s11469-019-00126-w. [DOI] [Google Scholar]
- Smith, J. L., Mattick, R. P., Jamadar, S. D., & Iredale, J. M. (2014). Deficits in behavioural inhibition in substance abuse and addiction: A meta-analysis. Drug and Alcohol Dependence, 145, 1–33. 10.1016/j.drugalcdep.2014.08.009. [DOI] [PubMed] [Google Scholar]
- Verdejo-García, A., Alcázar-Córcoles, M. A., & Albein-Urios, N. (2019). Neuropsychological interventions for decision-making in addiction: A systematic review. Neuropsychology Review, 29(1), 79–92. 10.1007/s11065-018-9384-6. [DOI] [PubMed] [Google Scholar]
- Wang, Y., Wu, L., Wang, L., Zhang, Y., Du, X., & Dong, G. (2017). Impaired decision-making and impulse control in Internet gaming addicts: Evidence from the comparison with recreational Internet game users. Addiction Biology, 22(6), 1610–1621. 10.1111/adb.12458. [DOI] [PubMed] [Google Scholar]
- Wang, Y., Wu, L., Zhou, H., Lin, X., Zhang, Y., Du, X., et al. (2017). Impaired executive control and reward circuit in Internet gaming addicts under a delay discounting task: Independent component analysis. European Archives of Psychiatry and Clinical Neuroscience, 267(3), 245–255. 10.1007/s00406-016-0721-6. [DOI] [PubMed] [Google Scholar]
- Wartberg, L., Kriston, L., & Thomasius, R. (2020). Internet gaming disorder and problematic social media use in a representative sample of German adolescents: Prevalence estimates, comorbid depressive symptoms and related psychosocial aspects. Computers in Human Behavior, 103, 31-36. 10.1016/j.chb.2019.09.014. [DOI] [Google Scholar]
- Wartberg, L., & Lindenberg, K. (2020). Predictors of spontaneous remission of problematic Internet use in adolescence: A one-year follow-up study. International Journal of Environmental Research and Public Health, 17(2), 448. 10.3390/ijerph17020448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wiers, R. W., Gladwin, T. E., Hofmann, W., Salemink, E., & Ridderinkhof, K. R. (2013). Cognitive bias modification and cognitive control training in addiction and related psychopathology: Mechanisms, clinical perspectives, and ways forward. Clinical Psychological Science, 1(2), 192–212. 10.1177/2167702612466547. [DOI] [Google Scholar]
- Wilcox, R. R., & Keselman, H. J. (2003). Modern robust data analysis methods: Measures of central tendency. Psychological Methods, 8(3), 254–274. 10.1037/1082-989X.8.3.254. [DOI] [PubMed] [Google Scholar]
- Wilens, T. E., Martelon, M., Fried, R., Petty, C., Bateman, C., & Biederman, J. (2011). Do executive function deficits predict later substance use disorders among adolescents and young adults? Journal of the American Academy of Child & Adolescent Psychiatry, 50(2), 141–149. 10.1016/j.jaac.2010.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolff, M., Krönke, K.-M., Venz, J., Kräplin, A., Bühringer, G., Smolka, M. N., et al. (2016). Action versus state orientation moderates the impact of executive functioning on real-life self-control. Journal of Experimental Psychology: General, 145(12), 1635–1653. 10.1037/xge0000229. [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2019). ICD-11: International classification of diseases 11th revision. Retrieved from https://icd.who.int/browse11/l-m/en. [Google Scholar]
- Yao, Y.-W., Liu, L., Ma, S.-S., Shi, X.-H., Zhou, N., Zhang, J.-T., et al. (2017). Functional and structural neural alterations in Internet gaming disorder: A systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews, 83, 313–324. 10.1016/j.neubiorev.2017.10.029. [DOI] [PubMed] [Google Scholar]
- Zheng, H., Hu, Y., Wang, Z., Wang, M., Du, X., & Dong, G. (2019). Meta-analyses of the functional neural alterations in subjects with Internet gaming disorder: Similarities and differences across different paradigms. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 94, 109656. 10.1016/j.pnpbp.2019.109656. [DOI] [PubMed] [Google Scholar]